")
Back to Journals » Clinical Ophthalmology » Volume 17
Efficacy, Safety, and Durability of Brolucizumab: An 8-Month Post-Marketing Surveillance Analysis
Received 29 June 2023
Accepted for publication 13 September 2023
Published 20 September 2023 Volume 2023:17 Pages 2791—2802
DOI https://doi.org/10.2147/OPTH.S425709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Nicholas J Saba,1 Scott D Walter2
1Department of Ophthalmology, SUNY Downstate Medical Center, Brooklyn, NY, USA; 2Retina Consultants, PC, Hartford, CT, USA
Correspondence: Scott D Walter, Retina Consultants, PC, 43 Woodland Street, Hartford, CT, USA, 06105, Tel +1860-206-2237, Fax +1860-409-7803, Email [email protected]
Importance: Brolucizumab (Beovu®) is an anti-vascular endothelial growth factor (anti-VEGF) agent approved for the treatment of neovascular age-related macular degeneration (nvAMD). Brolucizumab was marketed for its noninferiority to aflibercept and its potential for greater durability. However, post-marketing utilization has been tempered by safety concerns.
Objective: We evaluate the visual and anatomic efficacy of brolucizumab, examine changes in treatment intervals after switching to brolucizumab, and estimate the incidence of drug-related adverse events in the real world.
Design, Setting, and Participants: This was a retrospective consecutive case series of 626 eyes (543 patients) with nvAMD treated with 1438 brolucizumab injections at a single retina practice between 10/1/2019 and 5/15/2020.
Main Outcomes and Measures: Changes in visual acuity (VA); anatomic outcomes assessed by optical coherence tomography (OCT) including central subfield thickness (CST), macular volume (MV), presence of intraretinal fluid (IRF), subretinal fluid (SRF), and serous pigment epithelial detachment (sPED) on foveal line scans; treatment intervals before and after receiving brolucizumab; and the incidence of brolucizumab-related adverse events.
Results: The majority of eyes (N = 531, 89.7%) had received prior anti-VEGF therapy with aflibercept, ranibizumab, and/or bevacizumab. VA improved in treatment-naïve eyes (+3.7 letters, p = 0.04), and was maintained in previously treated eyes. There were significant improvements in all anatomic outcomes in both groups (p < 0.001). We observed a 4.8% incidence of intraocular inflammation (IOI) and a 0.6% incidence of retinal vasculitis. The average treatment interval increased from 6.3 to 6.8 weeks (p = 0.001).
Conclusions and Relevance: Brolucizumab treatment was associated with VA improvement in naïve eyes and maintenance of VA in previously treated eyes. Switching to brolucizumab was associated with improved anatomic outcomes and extended treatment intervals in most eyes. We observed a similar incidence of IOI and a lower incidence of retinal vasculitis compared to the Safety Review Committee’s analysis of HAWK and HARRIER.
Keywords: Beovu, brolucizumab, anti-VEGF, intraocular inflammation, retinal vasculitis
Introduction
Brolucizumab (Beovu®) is a low molecular weight humanized antibody fragment developed by Novartis (Cambridge, MA) as a vascular endothelial growth factor (VEGF) inhibitor.1 Registered Phase III clinical trials HAWK (NCT02307682) and HARRIER (NCT02434329) showed brolucizumab was associated with gains in visual acuity (VA) that were statistically noninferior to aflibercept for treatment-naïve patients with active choroidal neovascularization secondary to neovascular age-related macular degeneration (nvAMD). Brolucizumab received FDA approval on October 8th, 2019 for the treatment of nvAMD in the US.2 The recommended dosage regimen is 6 mg/0.05 mL via intravitreal injection (IVI) monthly for the first 3 doses, then once every 8–12 weeks.1
The majority of patients in HAWK (55.6% in the 6mg arm) and HARRIER (51.0%) were maintained on treatment intervals of 12 weeks, suggesting the potential for enhanced durability relative to aflibercept. In addition, brolucizumab showed more favorable anatomic outcomes relative to aflibercept. Intraretinal fluid (IRF) and subretinal fluid (SRF) were eliminated in more brolucizumab-treated eyes vs aflibercept-treated eyes. Greater central subfield thickness (CST) reductions from the baseline were observed with brolucizumab vs aflibercept.2
The original publication of the phase III clinical trial results stated that no serious ocular adverse events (AE) occurred in >1% of eyes.2 While there was a higher rate of uveitis (2.2%) and iritis (2.2%) observed in eyes treated with 6mg of brolucizumab (versus 0.3% and 0% with aflibercept) in HAWK, the corresponding rates of these inflammatory events in HARRIER were <1% in both arms.2 Approximately 90% of the IOI events were graded as mild-to-moderate, treated topically with corticosteroids and/or antibiotics, and resolved with no sequelae.2 Although there were 3 reported cases of retinal vascular occlusion, no cases of retinal vasculitis were originally reported in either trial.2
However, early post-marketing surveillance data raised new safety concerns about the prevalence and severity of ocular AEs with brolucizumab. In February 2020, the American Society of Retinal Specialists (ASRS) Research and Safety in Therapeutics (ReST) committee alerted ASRS members about incident reports of occlusive and nonocclusive retinal vasculitis in patients treated with brolucizumab.3 A subsequent report by the ASRS ReST committee detailed more information about the demographics, clinical features, and outcomes of these events.4,5 A number of cases illustrating the spectrum of brolucizumab-associated retinal vasculitis were subsequently reported in the peer-reviewed literature, including several with profound vision loss.6–8 A Safety Review Committee (SRC) formed by Novartis conducted an unmasked post-hoc review of all investigator-reported cases of IOI, retinal vascular occlusions, and endophthalmitis in the HAWK and HARRIER studies.9 The SRC found higher incidences of both retinal vasculitis and retinal vascular occlusion than originally reported by the investigators. In the combined HAWK/HARRIER study populations, the SRC found that 3.3% of eyes had retinal vasculitis (36 of 1088) and 2.1% of eyes had IOI with retinal vasculitis and a retinal vascular occlusion (23 of 1088 eyes).9 In June 2020, the FDA label was updated with a new warning that “retinal vasculitis and/or retinal vascular occlusion, typically in the presence of IOI, have been reported with the use of [brolucizumab]”.
With growing uncertainty concerning the safety and efficacy of brolucizumab relative to other anti-VEGF agents, we set out to retrospectively analyze our practice’s initial post-marketing experience with brolucizumab during the first 8 months following FDA approval of the drug on October 7, 2019. Unlike the clinical trial population which enrolled only treatment-naïve eyes with nvAMD, our study population was mostly comprised of eyes switched from another anti-VEGF therapy (563/626 eyes, 89.9%). Typically, these patients were switched to brolucizumab for persistent fluid, or with the hope of achieving a longer treatment interval. As such, this was a nonrandom and highly selected population of NVAMD patients. However, we felt that this population was probably more representative of the nvAMD patients currently being treated with brolucizumab in the United States.
Our research questions included whether switching to brolucizumab was associated with changes in VA, improvement in anatomic outcomes, or increases in treatment interval; and whether the observed incidence of adverse events following IVI of brolucizumab was similar to the SRC analysis of the HAWK and HARRIER trials.
Methods
Study Design, Setting, and Subjects
This was a retrospective consecutive case series enrolling all patients with nvAMD who received IVIs of brolucizumab between 10/1/2019 and 5/15/2020 at the six offices of Retina Consultants, P.C., a private retina practice in Hartford County, Connecticut. Institutional review board approval was obtained for retrospective review from Hartford Hospital, which waived informed consent (IRB# HHC-2021-0134). Patient information was deidentified and protected by safeguards. This study followed the rules of the Health Insurance Portability and Accountability Act and adhered to the tenets of the Declaration of Helsinki. Potential subjects were identified using billing data for all anti-VEGF drug claims during the study period. A retrospective chart review was completed by N.J.S., and all data were anonymized for the analysis.
Data Collection
Snellen visual acuities (VAs) were recorded on the dates of the patient’s first and final brolucizumab IVIs during the study period. For patients who received only a single IVI of brolucizumab, final VA was recorded at the next office visit following the brolucizumab injection. Snellen VA was converted to approximate Early Treatment for Diabetic Retinopathy Study (ETDRS) letters for statistical analysis.10,11 Patients with VA of count fingers (CF) or worse were assigned an ETDRS letter score of 0.
Anatomic outcomes were assessed by spectral-domain optical coherence tomography (OCT). OCT images were acquired using the Spectralis imaging platform (Heidelberg Engineering Inc) with a horizontal raster scanning protocol and automated image registration for comparison between visits. In general, patients were imaged with OCT at every visit, but there were some reductions in scan frequency due to the onset of the COVID-19 pandemic during the study period. We chose to analyze the OCT images from the date of the initial IVI of brolucizumab and the second IVI of brolucizumab, or the first follow-up OCT image acquired thereafter. All OCT images were manually graded by N.J.S., and any equivocal images underwent a secondary review by S.D.W. Macular volume (MV) and CST measurements were generated by automated segmentation in Heidelberg Eye Explorer, and any images with gross segmentation errors were excluded from the analysis. The presence or absence of intraretinal fluid (IRF), subretinal fluid (SRF), and serous pigment epithelial detachment (sPED) was assessed on the foveal line scans only. Patients were excluded from the VA and anatomic outcome analysis if they had no follow-up visits within the study period. Patients were excluded from the analysis of anatomic outcomes if the OCT image quality was deemed too poor for analysis.
To analyze changes in treatment interval, we selected a subgroup of eyes that were previously treated with 3 or more anti-VEGF injections prior to initiation on brolucizumab treatment and then received 2 or more brolucizumab injections after switching. This subgroup was further stratified based on prior (pre-brolucizumab) treatment intervals of ≤4.0 weeks, 4.1–6.0 weeks, 6.1–8.0 weeks, and >8.0 weeks.
As part of our practice’s routine pharmacovigilance strategy, drug-related AEs are reported internally to our Compliance Officer and reported externally to the drug manufacturer and the ASRS ReST committee. For the purposes of this study, we defined “clinically significant” AEs as those which the treating clinician considered serious enough to warrant reporting. Other commonly occurring IVI-related complications, such as subconjunctival hemorrhage and ocular surface irritation following IVI, were not assessed in this study. We reviewed all anti-VEGF drug-related AE reports to the ASRS during the study period. The incidence of clinically significant AEs was calculated by dividing the number of AE reports attributed to brolucizumab by the total number of eyes receiving brolucizumab during the study period. The actual date of the AE diagnosis was determined by chart review, rather than the ASRS reporting date.
Statistical Analysis
A two-tailed, paired sample t-test was performed for continuous variables (ETDRS letters, CST, MV, treatment intervals), and the McNemar test with continuity correction was performed for categorical variables (IRF, SRF, sPED). A p-value <0.05 was considered significant.12–15 A Welch t-test was run to determine if there were differences in pre-brolucizumab visual acuity between naïve and switch eyes. Data analysis was performed using SPSS software, version 26 (IBM).
Results
Descriptive Analysis
A total of 1438 IVIs of brolucizumab were administered in 626 eyes of 543 patients during the study period. The median number of IVIs of brolucizumab per eye was 2 (range 1–8) with a mean of 2.3 (standard deviation [SD] 1.1) IVIs. One hundred and eighty-four eyes (29.4%) received a single dose of brolucizumab, 178 (28.4%) eyes received 2 brolucizumab injections, 180 (28.8%) eyes received 3 brolucizumab injections, 66 (10.5%) eyes received 4 brolucizumab injections, 16 (2.6%) eyes received 5 brolucizumab injections, 1 eye received 6 (0.2%) brolucizumab injections, and 1 eye received 8 (0.2%) brolucizumab injections. Right (320/626, 51.1%) and left (306/626, 48.9%) eyes were equally represented in the study sample. Eighty-three (83/626, 15.3%) patients received IVIs of brolucizumab in both eyes. The mean (SD) age was 80.8 (9.4) years on the date of the patients’ first brolucizumab injection. There was a slight female preponderance (325/543 patients, 59.9%) consistent with the typical demographics of nvAMD. The majority of the eyes treated with brolucizumab had received prior anti-VEGF therapy with aflibercept (493, 78.8%), ranibizumab (302, 48.2%), and/or bevacizumab (123, 19.6%). Only 10.1% (63/626) of the eyes were treatment naïve. The average interval between the first and second IVI of brolucizumab was 40.8 days (5.8 weeks) for previously treated eyes versus 32.8 days (4.7 weeks) for treatment-naïve eyes. Thirty-five (5.6%) eyes had no follow-up within the study period and were excluded from the study population; additional exclusion criteria were applied in subsequent analyses as described in the methods (Figure 1).
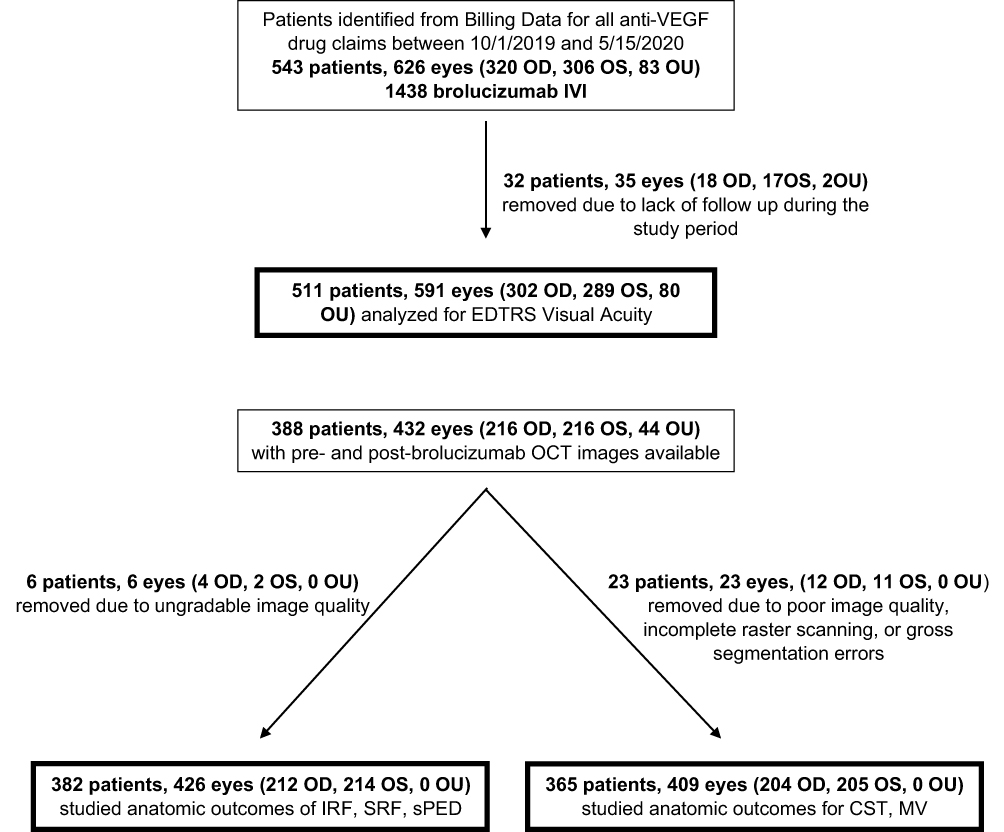 |
Figure 1 Flow diagram illustrating the application of inclusion/exclusion criteria and the resulting number of eyes available for the analysis of visual acuity and anatomic outcomes. |
Visual and Anatomic Outcomes
Visual and anatomic outcomes were analyzed in 3 groups (Table 1): treatment-naïve eyes (naïve, n = 61), previously treated eyes that were switched (switched, n = 530), and both groups combined (combined, n = 591). At initiation of brolucizumab treatment, VA was lower for naïve eyes versus switched eyes (mean difference of −8.1 ETDRS letters, p = 0.02, unpaired t-test). Among naïve eyes, there was an improvement in VA following treatment with brolucizumab (+3.7 ETDRS letters) (Table 1A). For switched eyes, there was no overall change in visual acuity (61.6 vs 61.1 EDTRS letters) (Table 1A); 214 (40.4%) eyes showed visual acuity improvement, 236 (44.5%) showed visual acuity deterioration, and 80 (15.1%) eyes had no change in visual acuity after receiving brolucizumab.
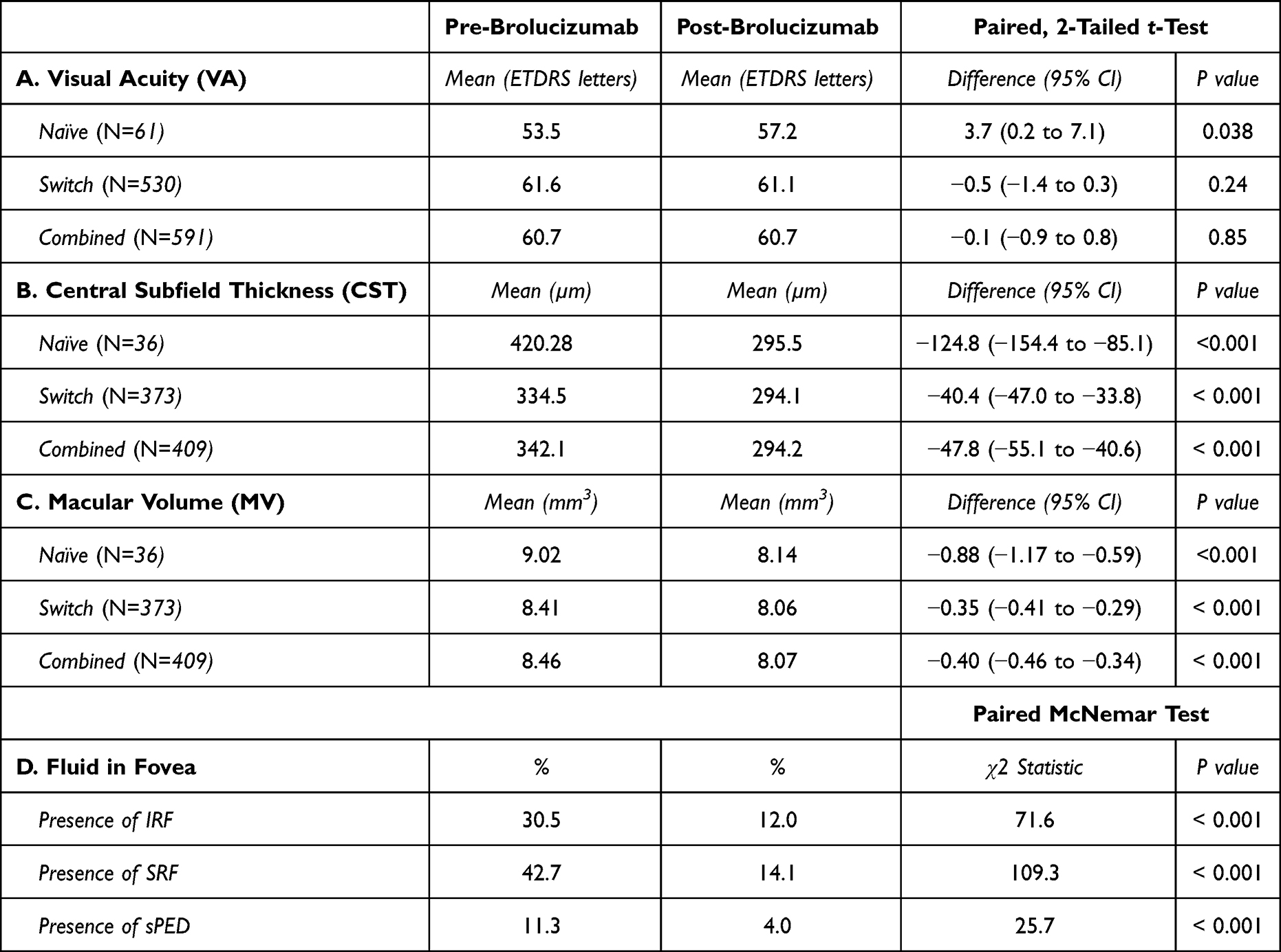 |
Table 1 Visual Acuity, Optical Coherence Tomography Anatomic Outcomes, and Fluid Reduction in Intraretinal Fluid (IRF), Subretinal Fluid (SRF), and Serous Retinal Pigmented Epithelial Detachment (sPED) Anatomic Variables After Brolucizumab Treatment |
Of the 432 eyes with pre- and post-brolucizumab OCT images available for analysis, 23 eyes (5.3%) were excluded due to poor image quality, incomplete raster scanning, or gross segmentation errors. A statistically significant decrease in CST occurred following the first IVI of brolucizumab (−47.8 µm; Table 1B). Central subfield thickness was decreased in 340 eyes (83.1%), increased in 66 eyes (16.1%), and unchanged in 3 eyes (0.7%). A statistically significant decrease in MV also occurred following the first IVI of brolucizumab (−0.40 mm3; Table 1C). Macular volume was decreased in 343 eyes (83.9%), increased in 63 eyes (15.4%), and unchanged in 3 eyes (0.7%). Treatment-naïve eyes demonstrated greater reductions in CST (−124.8 µm) and MV (−0.88 mm3) than switched eyes (−40.4 µm and −0.35 mm3 respectively) (Table 1C).
Fluid Resolution Analysis
Of the 432 eyes with foveal OCT line scans available for analysis, 6 eyes (1.4%) were excluded due to ungradable image quality. The proportion of eyes with fluid in each of the intraretinal, subretinal, and sub-RPE compartments decreased following treatment with brolucizumab (Table 1D). The percentage of eyes with IRF in the fovea decreased from 30.5% (130/426) to 12.0% (51/426) following the first IVI of brolucizumab. The percentage of eyes with SRF in the fovea decreased from 42.7% (183/426) to 14.1% (60/426). The percentage of eyes with a sPED decreased from 11.3% (48/426) to 4.0% (17/426). A small number of eyes demonstrated a new occurrence of IRF (3 eyes, 0.7%), SRF (6 eyes, 1.4%), or sPED (2 eyes, 0.5%) in the fovea following the first IVI of brolucizumab. Representative pre- and post-treatment OCT images are shown in Figure 2.
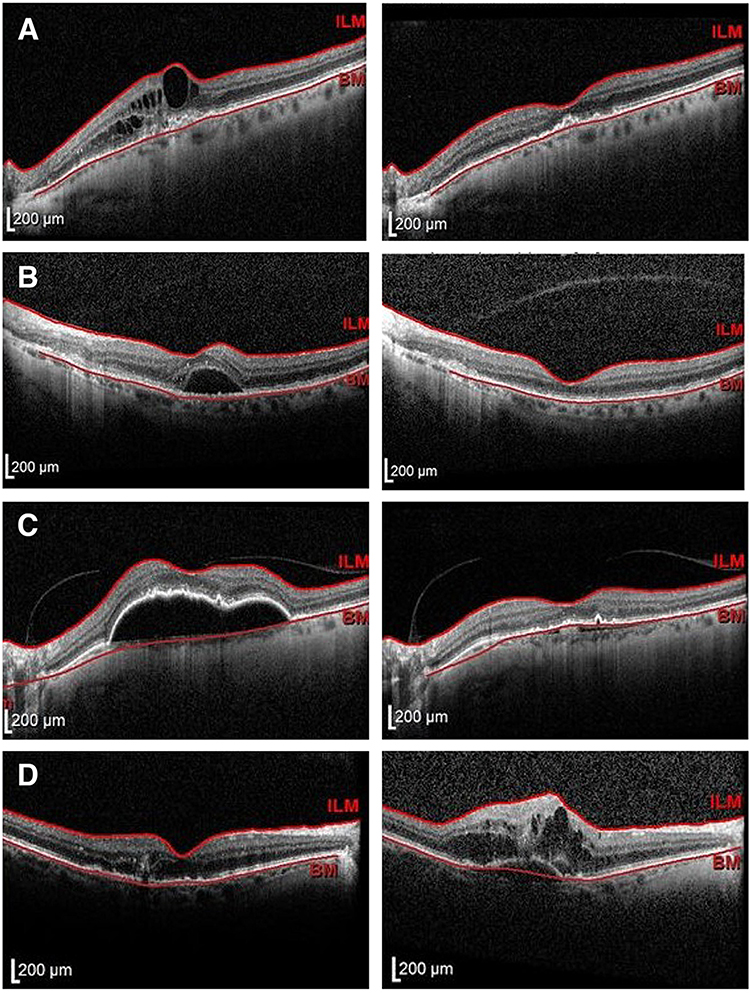 |
Figure 2 Representative OCT images of (A) intraretinal fluid, (B) subretinal fluid, and (C) serous pigment epithelial detachment resolution after brolucizumab treatment. (D) Paradoxical worsening of retinal fluid was occasionally observed following treatment with brolucizumab. |
Treatment Interval Analysis
Three hundred and eighty-five eyes (61.5% of the total study population) were included in the analysis of treatment intervals (Figure 3). The average treatment interval increased from 6.3 to 6.8 weeks (+0.5 weeks, p = 0.001, two tailed t-test) and the median treatment interval increased from 6 to 7 weeks. Patients with a prior treatment interval of ≤4 weeks achieved a significant increase in mean treatment interval from 3.8 to 5.9 weeks (+2.1 weeks, P < 0.001, paired t-test) with the median treatment interval increasing from 4 to 5 weeks. Patients with a prior treatment interval of 4.1 to 6 weeks also achieved a significant increase in treatment interval from 5.2 to 6.2 weeks (+1.0 weeks, P < 0.001) with the median increasing from 5 to 6 weeks. Patients with prior treatment intervals of 6.1 to 8.0 weeks maintained their treatment interval (7.3 prior vs 7.5 weeks after switching, P = 0.3). Moreover, patients with a prior treatment interval >8 weeks experienced a decrease in their average treatment interval from 9.9 to 7.6 weeks (−2.3 weeks, P < 0.001) with the median decreasing from 9 to 8 weeks.
 |
Figure 3 Frequency histogram showing the percentage of patients experiencing extended or reduced treatment intervals after switching to brolucizumab. This analysis was stratified according to the patient’s prior treatment interval immediately preceding the switch to brolucizumab. |
Incidence of Ocular Adverse Events
During the study period, a total of 1438 brolucizumab IVIs were performed across our practice (Figure 4). Thirty eyes (4.8%, 30/626) of 26 patients (4.8%, 26/543) treated with brolucizumab developed serious ocular AEs (Table 2) after receiving a median of 2 injections, yielding a 2.1% (30/1438) incidence on a per injection basis. All of the AEs were observed among switch eyes, such that the incidence of ocular AEs among switch eyes was 5.7% (30/530) on a per eye and 2.3% (30/1282) on a per injection basis. Of the 30 eyes that developed IOI secondary to brolucizumab injections, 2 (6.7%) eyes showed inflammatory cells in the anterior segment only, 10 (33.3%) eyes showed inflammatory cells in the vitreous only, and 16 (53.3%) eyes showed inflammatory signs in both the anterior and posterior segments. Retinal vasculitis was documented in 4 eyes of 3 patients, yielding an overall incidence of 0.6% on a per patient (3/543) and 0.6% on a per eye (4/626) basis. One patient with retinal vasculitis developed a partial arterial occlusion along a proximal segment of the inferotemporal branch retinal arteriole, leading to paracentral acute middle maculopathy (PAMM) involving the fovea. This patient had stable VA but reported “gray spots” near her central vision, which subsequently resolved. Another patient developed a central retinal artery occlusion (CRAO) resulting in permanent loss of 70 ETDRS letters. A case of presumed post-injection endophthalmitis occurred in 1 eye after the 5th injection of brolucizumab, however cultures did not yield any growth; of note, this patient had a previous history of endophthalmitis. One patient developed an erythematous periocular rash after the third IVI of brolucizumab; the rash was localized around the treated eye, but this patient did not demonstrate any evidence of IOI. The patient was evaluated by a dermatologist who attributed the rash to a drug-induced flare of the patient’s underlying rosacea. There were no other extraocular or systemic adverse events during the study period that were attributed to brolucizumab.
 |
Table 2 Adverse Events in 30 Eyes Treated with Brolucizumab and Subsequent Management |
 |
Figure 4 Frequency histogram depicting the number of intravitreal injections of brolucizumab administered and the number of reportable drug-related adverse events on a monthly basis. |
Discussion
In this analysis, we evaluated the efficacy, durability, and safety of brolucizumab among both treatment-naïve and previously treated nvAMD eyes in a real-world clinical practice. Recently published post-marketing surveillance studies of brolucizumab for nvAMD range from a small case series of 19 eyes to a large multicenter, retrospective study of 1098 eyes in the Czech Republic.16–43 To our knowledge, this series of 626 eyes treated with brolucizumab is the 2nd largest post-marketing surveillance study worldwide, and the largest single-center study worldwide.16
Study Limitations
As with any retrospective real-world study, our analysis does have some important limitations. Real-world VA measurements may be less accurate than the best-corrected VA measurements in clinical trials. Additionally, the conversion of Snellen VA to EDTRS letters may be inaccurate, particularly for patients with poorer VA (eg we assigned eyes with CF or worse vision an EDTRS letter score of 0, which limits the continuity of the variable). Grading of macular fluid was performed on foveal OCT line scans only, which likely underrepresents the presence of fluid in other parafoveal planes. We had a relatively short period of follow-up, and many patients who were treated with brolucizumab were switched to other anti-VEGF agents following the ReST committee announcement. Additionally, the onset of the COVID-19 pandemic may have disrupted patient follow-up during the study period.
Vision and Anatomy
HAWK and HARRIER demonstrated a significant VA improvement in treatment-naïve patients –gaining an average of 6.1 and 6.9 ETDRS letters at 48 weeks.2 While a minority of the patients in this series (10.1%) were treatment-naïve and the duration of follow-up was much shorter (median 4.9 wks), we also observed a significant improvement in VA (+3.7 letters) in this population. Although the VA gains observed in our study were lower, this difference is probably due to the treatment-naïve patients in our study receiving fewer injections (mean = 2.4 ±0.7; median = 2) than those in the clinical trials (4–6 injections). Our study population primarily included eyes previously treated with aflibercept, ranibizumab, and bevacizumab. Visual acuities before and after switching were similar, supporting the claim that brolucizumab is noninferior to other anti-VEGF therapies.
It has been hypothesized that brolucizumab is a more powerful drying agent than aflibercept.16,17,21,22,26,34–36,38–40,43 Although anatomic outcomes were not the primary endpoint of HAWK and HARRIER, brolucizumab-treated eyes showed significantly less fluid in the intraretinal, subretinal, and sub-RPE compartments at week 48.2 Our data confirmed that that brolucizumab is a powerful drying agent not only in treatment-naïve NVAMD eyes but also in previously treated eyes that were switched to brolucizumab. The superior anatomic outcomes may be due to the higher molar concentration of the drug and/or higher VEGF-binding affinity.1,44 Alternatively, patients who were considered for switching may have developed tachyphylaxis to their prior anti-VEGF therapy.
Durability
One potential clinical advantage of brolucizumab is the ability to treat patients at extended dosing intervals. In HAWK and HARRIER, brolucizumab-treated eyes received 3 monthly loading doses followed by an injection q12 weeks, and were interval adjusted to q8 weeks if disease activity was present.2 Brolucizumab was the first anti-VEGF drug FDA-approved with a label indicating efficacy up to q12 week dosing. Although the labelling studies for aflibercept only evaluated a treatment interval of 8 weeks,45 subsequent studies have demonstrated that some patients can be successfully extended and maintained at longer treatment intervals.46–49
Real-world experience with brolucizumab has shown extension of treatment intervals after switching, particularly in the handful of studies with longer-term follow-up.17,23,31,42 Our study showed a statistically significant but modest 0.5-week extension in average treatment interval after switching. Interestingly, patients with longer prior treatment intervals saw no durability benefit or even a detrimental effect on treatment interval. Our analysis likely underestimates the ultimate potential for interval extension after switching to brolucizumab, due to the relatively short length of follow-up. Additionally, some patients who were switched have been “re-loaded” with monthly injections of brolucizumab, skewing the data on treatment intervals.
When a new anti-VEGF drug is approved, patients currently on a q4-6 week dosing interval are often the first considered for switching.47 Therefore, we sought to evaluate the treatment dynamics after switching specifically among patients with shorter pre-brolucizumab treatment intervals. Patients with pre-brolucizumab treatment intervals ≤4 weeks were most likely to experience extended treatment intervals, followed by patients with intervals of q4-6 weeks. This result suggests that switching to brolucizumab may allow treatment interval extension in our most difficult to treat patients. However, there are some potential safety concerns about more frequent dosing with brolucizumab. The Phase 3a MERLIN study was designed to compare monthly brolucizumab versus monthly aflibercept in previously treated nvAMD eyes with persistent retinal fluid. Unfortunately, this study was terminated due to the higher incidence of IOI in eyes receiving brolucizumab 6 mg dosed q4 weeks.28
Safety
Post-marketing safety concerns raised by retina specialists and subsequently confirmed by the SRC have significantly curtailed the utilization of brolucizumab in the real world.3–8 According to the SRC’s post hoc analysis, the true incidence of IOI in HAWK and HARRIER was 4.6% (50 of 1088 eyes).9 The incidence of IOI in our real-world study was 4.8% (30 of 626 eyes), closely mirroring the trial results. The SRC analysis also showed a 3.3% incidence of retinal vasculitis, with concomitant retinal vascular occlusion in 2.1% of eyes. Our real-world experience identified retinal vasculitis in only 4 of 626 eyes, for an overall incidence of 0.6%. Interestingly, a large IRIS registry study also found a similar 0.6% incidence of retinal vasculitis in the US real-world experience with brolucizumab.29 The incidence of retinal vascular occlusion in our study was 0.3% (2 of 626 eyes), whereas the SRC analysis found an incidence of 2.1%.
There are several possible explanations why the observed incidence of IOI in our study was similar to the SRC, whereas the observed incidence of retinal vasculitis and retinal vascular occlusion was lower. Firstly, our study may have been “underpowered” to detect rare events as a result of our smaller sample size (626 vs 1088 eyes). However, this would not explain why a large, nationally representative sample of 10,654 eyes also demonstrated a retinal vasculitis incidence of 0.6%.29 Most eyes treated with brolucizumab in the real world were previously treated with other anti-VEGF agents.16,17,21–23,26,35,39–43 It is possible that previously treated eyes are equally susceptible to IOI but somehow less susceptible to retinal vasculitis than treatment-naïve eyes.
Our leading hypothesis is that the incidence of IOI often precedes the development of brolucizumab-associated retinal vasculitis. The median follow-up in our study was only 5.3 weeks versus 48 weeks in HAWK and HARRIER. Despite this very short length of follow-up, we immediately recognized IOI in 4.8% of our patients after a median of only 2 injections. This supports our hypothesis that the incidence of IOI often occurs early in the course of brolucizumab treatment. However, if retinal vasculitis and vascular occlusions occur later in eyes with IOI that are subjected to continued brolucizumab treatment, then real-world studies with shorter follow-up would suffer from “lead time bias”, resulting less frequent detection of later-term complications (ie retinal vasculitis and retinal vascular occlusion). Adding weight to our hypothesis, the early termination of the MERLIN study yielded a higher incidence of IOI (9.3%) and a lower incidence of retinal vasculitis (0.8%).28
Conclusion
Our real-world experience with brolucizumab largely confirmed the key findings of the HAWK and HARRIER trials. Treatment naïve patients showed significant improvements in vision and anatomy after initiating treatment with brolucizumab. Previously treated eyes maintained VA after switching to brolucizumab, supporting the claim of noninferiority to other anti-VEGF agents. Our analysis found that brolucizumab was highly effective in reducing fluid within all retinal compartments, even in previously treated nvAMD eyes. We found that patients may achieve extended dosing intervals shortly after switching to brolucizumab, especially those with prior treatment intervals <6 weeks. The incidence of IOI in our patient population closely mirrored the incidence seen in the SRC analysis of HAWK and HARRIER. We observed a lower incidence of retinal vasculitis and vascular occlusion, perhaps due to shorter follow-up, earlier recognition of IOI, and/or discontinuation of brolucizumab treatment. Given the relatively high incidence of IOI after a median of 2 injections, retina specialists should carefully examine the anterior and posterior segment for signs of inflammation prior to each subsequent brolucizumab injection.
Acknowledgments
The preliminary results of this analysis were presented at The Association for Research in Vision and Ophthalmology (ARVO) meeting in May 2021 and at the American Society of Retina Specialists (ASRS) meeting in October 2021. The poster’s abstract was published in “Poster Abstracts” in Investigative Ophthalmology & Visual Science June 2021, Vol.62: https://iovs.arvojournals.org/article.aspx?articleid=2774044
Funding
There is no funding to report.
Disclosure
Scott D. Walter is a speaker for Apellis, Bausch and Lomb, Genentech/Roche, Regeneron, and Spark Therapeutics; and a consultant for Allergan, Aura Biosciences, Bausch and Lomb, Castle Biosciences, Genentech/Roche, EyePoint Pharmaceuticals, Ideaya Biosciences, Lupin, Novartis, and Regeneron. Nicholas J. Saba reports no conflicts of interest for this work.
References
1. Markham A. Brolucizumab: first approval. Drugs. 2019;79(18):1997–2000. doi:10.1007/s40265-019-01231-9
2. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
3. Beovu update for ASRS members. American society of retina specialists; 2020. Available from: https://www.asrs.org/clinical/clinical-updates/960/Beovu-Update-for-ASRS-Members.
4. Witkin AJ, Hahn P, Murray TG. Occlusive retinal vasculitis following intravitreal brolucizumab: an ASRS research and safety in therapeutics (ReST) committee report. Retina Times; 2020. Available from: https://www.asrs.org/publications/retina-times/details/2929/oclusive-retinal-vasculitis-following-intravitreal-brolucizumab-an-asrs-research-and-safety-in-thera.
5. Witkin AJ, Hahn P, Murray TG. Occlusive retinal vasculitis following intravitreal brolucizumab: an ASRS research and safety in therapeutics (ReST) committee report. Retina Times. 2020;38(2):10–13.
6. Baumal CR, Spaide RF, Vajzovic L, et al. Retinal vasculitis and intraocular inflammation after intravitreal injection of brolucizumab. Ophthalmology. 2020;127(10):1345–1359. doi:10.1016/j.ophtha.2020.04.017
7. Haug SJ, Hien DL, Uludag G, et al. Retinal arterial occlusive vasculitis following intravitreal brolucizumab administration. Am J Ophthalmol Case Rep. 2020;18:100680. doi:10.1016/j.ajoc.2020.100680
8. Jain A, Chea S, Matsumiya W, et al. Severe vision loss secondary to retinal arteriolar occlusions after multiple intravitreal brolucizumab administrations. Am J Ophthalmol Case Rep. 2020;18:100687. doi:10.1016/j.ajoc.2020.100687
9. Monés J, Srivastava SK, Jaffe GJ, et al. Risk of inflammation, retinal vasculitis, and retinal occlusion-related events with brolucizumab: post hoc review of HAWK and HARRIER. Ophthalmology. 2020;S0161–6420(20):31075–31077. doi:10.1016/j.ophtha.2020.11.011
10. Gregori NZ, Feuer W, Rosenfeld PJ. Novel method for analyzing Snellen visual acuity measurements. Retina. 2010;30(7):1046–1050. doi:10.1097/IAE.0b013e3181d87e04
11. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including ‘counting fingers’, ‘hand movement’, ‘light perception’ and ‘no light perception’ and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2020;99:e963–e965. doi:10.1111/aos.14659
12. Edwards A. Note on “correction for continuity” in testing the significance of the difference between correlated proportions. Psychometrika. 1948;13(3):185–187. doi:10.1007/BF02289261
13. Hoffman JI. The incorrect use of chi-square analysis for paired data. Clin Exp Immunol. 1976;24(1):227–229.
14. McNEMAR Q. Note on the sampling error of the difference between correlated proportions or percentages. Psychometrika. 1947;12(2):153–157. doi:10.1007/BF02295996
15. Rasch D, Guiard V. The robustness of parametric statistical methods. Psychol Sci. 2004;46(2):175–208.
16. Stepanov A, Studnicka J, Veith M, et al. Incidence of adverse events after loading phase of the brolucizumab therapy of neovascular AMD: real-life Evidence in the Czech Republic. Eur J Ophthalmol. 2022:11206721221132619. doi:10.1177/11206721221132619
17. Abdin AD, Aljundi W, El Jawhari K, Suffo S, Weinstein I, Seitz B. First year real life experience with intravitreal brolucizumab for treatment of refractory neovascular age-related macular degeneration. Front Pharmacol. 2022;13:860784. doi:10.3389/fphar.2022.860784
18. Avaylon J, Lee S, Gallemore RP. Case series on initial responses to intravitreal brolucizumab in patients with recalcitrant chronic wet age-related macular degeneration. Int Med Case Rep J. 2020;13:145–152. doi:10.2147/IMCRJ.S252260
19. Awh CC, Davis EC, Thomas MK, Thomas AS. Short-term outcomes after interim treatment with brolucizumab: a retrospective case series of a single center experience. Retina. 2022;42(5):899–905. doi:10.1097/IAE.0000000000003418
20. Baumal CR, Bodaghi B, Singer M, et al. Expert opinion on management of intraocular inflammation, retinal vasculitis, and vascular occlusion after brolucizumab treatment. Ophthalmol Retina. 2021;5(6):519–527. doi:10.1016/j.oret.2020.09.020
21. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world experience: the BRAILLE study. Clin Ophthalmol. 2021;15:3787–3795. doi:10.2147/OPTH.S328160
22. Chakraborty D, Maiti A, Sheth JU, et al. Brolucizumab in neovascular age-related macular degeneration - Indian real-world Experience: the BRAILLE study - fifty-two-week outcomes. Clin Ophthalmol. 2022;16:4303–4313. doi:10.2147/OPTH.S395577
23. Coney JM, Zubricky R, Sinha SB, et al. Switching to brolucizumab: injection intervals and visual, anatomical and safety outcomes at 12 and 18 months in real-world eyes with neovascular age-related macular degeneration. Int J Retina Vitreous. 2023;9(1):8. doi:10.1186/s40942-023-00445-0
24. Corradetti G, Corvi F, Juhn A, Sadda SR. Short-term outcomes following treatment of recalcitrant cystoid macular edema secondary to radiation maculopathy using intravitreal brolucizumab. Am J Ophthalmol Case Rep. 2020;20:100981. doi:10.1016/j.ajoc.2020.100981
25. Enríquez AB, Baumal CR, Crane AM, et al. Early experience with brolucizumab treatment of neovascular age-related macular degeneration. JAMA Ophthalmol. 2021;139(4):441–448. doi:10.1001/jamaophthalmol.2020.7085
26. Giunta M, Gauvin Meunier LP, Nixon D, Steeves J, Noble J. Early Canadian real-world experience with brolucizumab in anti-vascular endothelial growth factor-experienced patients with neovascular age-related macular degeneration: a retrospective chart review. Clin Ophthalmol. 2022;16:2885–2894. doi:10.2147/OPTH.S376199
27. Hoshino J, Matsumoto H, Mukai R, Nakamura K, Akiyama H. Intravitreal aflibercept versus brolucizumab for treatment-naive neovascular age-related macular degeneration with type 1 macular neovascularization: comparison of short-term outcomes. Ophthalmologica. 2022;245(5):413–420. doi:10.1159/000526044
28. Khanani AM, Brown DM, Jaffe GJ, et al. MERLIN: phase 3a, multicenter, randomized, double-masked trial of brolucizumab in participants with nAMD and persistent retinal fluid. Ophthalmology. 2022;S0161–6420(22):334. doi:10.1016/j.ophtha.2022.04.028
29. Khanani AM, Zarbin MA, Barakat MR, et al. Safety outcomes of brolucizumab in neovascular age-related macular degeneration: results from the IRIS registry and komodo healthcare map. JAMA Ophthalmol. 2022;140(1):20–28. doi:10.1001/jamaophthalmol.2021.4585
30. Kim DJ, Jin KW, Han JM, et al. Short-term safety and efficacy of intravitreal brolucizumab injections for neovascular age-related macular degeneration: a multicenter retrospective real-world study. Ophthalmologica. 2023:1–11. doi:10.1159/000529410
31. Kitajima Y, Maruyama-Inoue M, Ikeda S, et al. Short-term outcomes of switching to brolucizumab in Japanese patients with neovascular age-related macular degeneration. Jpn J Ophthalmol. 2022;66(6):511–517. doi:10.1007/s10384-022-00940-1
32. Kulikov AN, Gazizova IR, Maltsev DS, Malafeeva AY, Vasilyev AS, Zhalimova VR. Kratkosrochnye dannye effektivnosti i bezopasnosti primeneniya preparata «Brolutsizumab» pri lechenii neovaskulyarnoi vozrastnoi makulyarnoi degeneratsii na territorii Rossiiskoi Federatsii [Short-term Efficacy and Safety of Brolucizumab for Neovascular Age-related Macular Degeneration in the Russian Federation]. Vestn Oftalmol. 2022;138(3):55–62. Russian. doi:10.17116/oftalma202213803155
33. Maruko I, Okada AA, Iida T, et al. Brolucizumab-related intraocular inflammation in Japanese patients with age-related macular degeneration: a short-term multicenter study. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2857–2859. doi:10.1007/s00417-021-05136-w
34. Matsumoto H, Hoshino J, Nakamura K, Akiyama H. Two-year outcomes of treat-and-extend regimen with intravitreal brolucizumab for treatment-naïve neovascular age-related macular degeneration with type 1 macular neovascularization. Sci Rep. 2023;13(1):3249. doi:10.1038/s41598-023-30146-5
35. Mehta N, Fong RD, Wilson M, et al. Real-world experience using intravitreal brolucizumab alone or in combination with aflibercept in the management of neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:657–665. doi:10.2147/OPTH.S399590
36. Montesel A, Bucolo C, Sallo FB, Eandi CM. Short-term efficacy and safety outcomes of brolucizumab in the real-life clinical practice. Front Pharmacol. 2021;12:720345. doi:10.3389/fphar.2021.720345
37. Mukai R, Matsumoto H, Akiyama H. Risk factors for emerging intraocular inflammation after intravitreal brolucizumab injection for age-related macular degeneration. PLoS One. 2021;16(12):e0259879. doi:10.1371/journal.pone.0259879
38. Murray JE, Gold AS, Latiff A, Murray TG. Brolucizumab: evaluation of compassionate use of a complex anti-VEGF therapy. Clin Ophthalmol. 2021;15:4731–4738. doi:10.2147/OPTH.S339393
39. Ota H, Takeuchi J, Nakano Y, et al. Switching from aflibercept to brolucizumab for the treatment of refractory neovascular age-related macular degeneration. Jpn J Ophthalmol. 2022;66(3):278–284. doi:10.1007/s10384-022-00908-1
40. Scupola A, Carlà MM, Boselli F, et al. Brolucizumab for wet age-related macular degeneration: one-year real-world experience from a tertiary center. Ophthalmologica. 2023;246:58–67. doi:10.1159/000529817
41. Sotani R, Matsumiya W, Kim KW, et al. Clinical features and associated factors of intraocular inflammation following intravitreal brolucizumab as switching therapy for neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2023:10.1007/s00417-023-06036–x. doi:10.1007/s00417-023-06036-x
42. Ueda-Consolvo T, Tanigichi A, Numata A, et al. Switching to brolucizumab from aflibercept in age-related macular degeneration with type 1 macular neovascularization and polypoidal choroidal vasculopathy: an 18-month follow-up study. Graefes Arch Clin Exp Ophthalmol. 2023;261(2):345–352. doi:10.1007/s00417-022-05793-5
43. Van Cleemput L, Peeters F, Jacob J. Brolucizumab for neovascular age-related macular degeneration (BEL Study). Clin Ophthalmol. 2023;17:1077–1085. doi:10.2147/OPTH.S402090
44. Tadayoni R, Sararols L, Weissgerber G, Verma R, Clemens A, Holz FG. Brolucizumab: a newly developed Anti-VEGF molecule for the treatment of neovascular age-related macular degeneration. Ophthalmologica. 2021;244:93–101. doi:10.1159/000513048
45. Heier JS, Brown DM, Chong V, et al. Intravitreal Aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
46. DeCroos FC, Reed D, Adam MK, et al. Treat-and-extend therapy using aflibercept for neovascular age-related macular degeneration: a prospective clinical trial. Am J Ophthalmol. 2017;180:142–150. doi:10.1016/j.ajo.2017.06.002
47. Hahn P. ASRS 2023 Preferences and Trends Membership Survey. Chicago, IL: American Society of Retina Specialists; 2023.
48. Khurana RN, Rahimy E, Joseph WA, et al. Extended (Every 12 Weeks or Longer) dosing interval with intravitreal aflibercept and ranibizumab in neovascular age-related macular degeneration: post hoc analysis of VIEW trials. Am J Ophthalmol. 2019;200:161–168. doi:10.1016/j.ajo.2019.01.005
49. Witkin AJ, Hahn P, Murray TG, et al. Occlusive retinal vasculitis following intravitreal brolucizumab. J Vitreoretin Dis. 2020;4(4):269–279. doi:10.1177/247412640930863
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.