Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Real-World Disability Outcomes Among Patients Treated with Cariprazine vs Other Atypical Antipsychotics as Adjunctive Treatment for Major Depressive Disorder
Authors Masand PS, Parikh M, Ta JT, Wade SW, Haile F ![]() , Ripley S, Zanardo E, Spencer CS, Laliberté F, Nabulsi N
, Ripley S, Zanardo E, Spencer CS, Laliberté F, Nabulsi N ![]()
Received 6 March 2025
Accepted for publication 14 August 2025
Published 28 August 2025 Volume 2025:17 Pages 585—600
DOI https://doi.org/10.2147/CEOR.S522756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Prakash S Masand,1 Mousam Parikh,2 Jamie T Ta,2 Sally W Wade,3 Filmon Haile,2 Susannah Ripley,4 Enrico Zanardo,5 Colleen S Spencer,4 François Laliberté,4 Nadia Nabulsi2
1Duke-NUS, Singapore; 2AbbVie, North Chicago, IL, USA; 3Wade Outcomes Research and Consulting, Salt Lake City, UT, USA; 4Group d’analyse, SRI, Ltée, Montréal, QC, Canada; 5Analysis Group, Inc, Denver, CO, USA
Correspondence: Nadia Nabulsi, AbbVie, 1 North Waukegan Road, North Chicago, IL, 60064, USA, Tel +1 224-786-6489, Email [email protected]
Purpose: Major depressive disorder (MDD) is a disabling condition that may require adjunctive treatment with atypical antipsychotics (AAs). However, little is known about how different adjunctive AAs impact disability outcomes. This analysis compared disability events, days, and costs among patients with MDD before and after initiating adjunctive treatment with cariprazine, brexpiprazole, or aripiprazole, which all belong to a class of AAs known as dopamine partial agonists.
Patients and Methods: The MerativeTM MarketScan® Commercial Database and the Health and Productivity Management Database (1/1/2015-12/31/2022) were used to identify adults with MDD and ≥ 2 dispensings of cariprazine, brexpiprazole, or aripiprazole (first dispensing=index) adjunctive to antidepressant therapy. Baseline characteristics between cohorts were balanced using inverse probability of treatment weighting. Changes (post-index minus pre-index) in all-cause and mental health (MH)-related disability claim rates, days, and costs were compared for cariprazine vs brexpiprazole and cariprazine vs aripiprazole via a difference-in-difference analysis; 95% CIs were generated using nonparametric bootstrap procedures. P-values < 0.05 were considered statistically significant.
Results: In the cariprazine (n=224) vs brexpiprazole (n=643) analysis, the cariprazine cohort had significantly greater reductions in all-cause disability claims, days, and costs vs the brexpiprazole cohort (between-cohort difference: − 0.23 claims [P< 0.05], − 25.27 days [P< 0.001], −$4577.08 [P< 0.01], respectively). The cariprazine cohort also had a significantly greater reduction in MH-related disability days (− 12.07 [P< 0.05]); reductions in MH-related disability claims and mean costs vs brexpiprazole were similar. In the cariprazine (n=174) vs aripiprazole (n=2931) analysis, a significantly greater reduction for cariprazine vs aripiprazole was observed for all-cause and MH-related disability costs (all-cause: −$3275.91 [P< 0.01]; MH-related: −$2196.36 [P< 0.05]); reductions in all-cause and MH-related disability claims and days were similar.
Conclusion: In this real-world analysis of patients with MDD using AAs adjunctively to antidepressants, significantly greater reductions were observed in disability claims and days for cariprazine vs brexpiprazole and in disability costs for cariprazine vs aripiprazole. These results suggest that adjunctive cariprazine may have beneficial effects on disability outcomes for patients with MDD.
Plain Language Summary: Major depressive disorder (MDD) can lead to disability. Medications such as cariprazine, brexpiprazole, and aripiprazole can be used with antidepressants to treat MDD. This study compared the changes in disability outcomes in adults with MDD based on which of these medications they took with their antidepressant. Using insurance databases, we found patients with MDD using medications with antidepressants. We then looked at how disability outcomes changed from before to after starting treatment with different medications. We looked at disability events, or health events which required filing for disability. We also looked at the number of days on disability and the cost of disability. We compared before and after changes between cariprazine vs brexpiprazole and cariprazine vs aripiprazole. Compared with patients using brexpiprazole, patients using cariprazine had greater reductions in disability events, days, and costs. Patients using cariprazine vs brexpiprazole also had a greater reduction in disability days associated with mental health reasons specifically. Disability events and costs for mental health reasons were similar. For cariprazine vs aripiprazole, changes in disability events and days were similar. Changes in disability events and days for mental health-related reasons were also similar. Patients using cariprazine had a greater reduction in overall and mental health-related disability costs than patients using aripiprazole. Our results suggest that in patients with MDD, cariprazine with antidepressants had a greater benefit on disability outcomes than aripiprazole or brexpiprazole with antidepressants. This study was limited by the type of data available and smaller numbers of patients.
Keywords: cariprazine, major depressive disorder, disability, brexpiprazole, aripiprazole, adjunctive therapy
Introduction
Major depressive disorder (MDD) is a leading cause of disability worldwide,1 with results of the 2019 National Health and Wellness Survey showing that 8.8% of respondents with MDD reported short- or long-term disability relative to 1.7% of respondents without MDD.2 The negative effects of MDD are further reflected in its large, increasing economic burden. According to an analysis based on National Survey on Drug Use and Health estimates, the economic burden of MDD increased by 37.9% from $236.6 billion in 2010 to $333.7 billion in 2019 ($382.4 billion in 2023 US dollars [USD]).3,4 The largest contributor to the growing economic burden of MDD from 2010 to 2018 was the 73.2% observed increase in workplace costs, which includes costs related to disabilities. Because steady employment in individuals with mental illness has been associated with decreased outpatient service use and healthcare costs relative to patients without steady employment,5 decreased rates of disability may benefit not only patients but also payers. As >80% of adults with depression report difficulty with work and other daily activities owing to their symptoms,6 effective treatment is imperative to decreasing the personal and economic burden of the disease. However, despite the substantial economic burden and associated workplace costs attributable to MDD, disability outcomes have not been well studied in the MDD population.
The episodic or relapsing nature of MDD can contribute to its negative impact on patients, including function and disability.7–9 Because of this, the American Psychiatric Association recommends maintenance treatment with antidepressant therapy (ADT) for at least 4 months after successful treatment in the acute phase of the illness, with a longer duration of therapy recommended for patients who have a high risk of recurrent depressive episodes.10 However, ~50% of patients with MDD experience inadequate response to first-line ADT.11 For patients who do not respond to their initial ADT, 1 guideline-recommended treatment option is the addition of an atypical antipsychotic (AA) as an adjunct to ADT.10,12,13 Adjunctive treatment with AAs has demonstrated efficacy vs placebo for the treatment of MDD in meta-analyses of clinical trial data14,15 and has the benefit of allowing patients to remain on their initial ADT if they experienced a partial response.16–18 Additionally, the use of adjunctive AAs has been associated with decreased healthcare resource utilization and healthcare costs. For instance, a claims-based analysis of adults with MDD found that the initiation of adjunctive AA treatment was associated with significantly decreased rates of all-cause and MDD-related hospitalizations and emergency department (ED) visits in the 12 months following adjunctive AA initiation compared with the 12 months before initiation.19 Furthermore, another claims-based analysis of patients with MDD found that patients who initiated an AA as their first adjunctive therapy had significantly less healthcare resource utilization and lower total healthcare costs relative to patients who initiated an AA as their subsequent adjunctive therapy.20 These prior analyses suggest that early initiation of adjunctive AAs for appropriate patients may result in decreased healthcare resource utilization and healthcare costs.
Currently, there are several AAs approved by the US Food and Drug Administration (FDA) for the adjunctive treatment of MDD, including aripiprazole, brexpiprazole, and cariprazine, which are part of a class of AAs known as dopamine partial agonists. Dopamine partial agonists are of interest because they are generally well tolerated, cause little sedation, are prolactin sparing, and have a low risk of weight gain.21 Specifically, aripiprazole is a dopamine D2 and serotonin 5HT1A receptor partial agonist and serotonin 5HT2A receptor antagonist that was approved by the FDA for the adjunctive treatment of MDD in 2007.22 Brexpiprazole, which was approved for the adjunctive treatment of MDD in 2015, is a dopamine D2 and D3 receptor partial agonist that displays greater affinity for serotonin 5HT1A/5HT2A receptors and α1B-adrenergic receptors than aripiprazole.23 The latest AA approved in 2022 for the adjunctive treatment of MDD is cariprazine,24 which is a dopamine D3-preferring D3/D2 and serotonin 5-HT1A receptor partial agonist that has a longer half-life and higher relative affinity for the D3 receptor compared with aripiprazole and brexpiprazole.24,25 Although aripiprazole, brexpiprazole, and cariprazine have all demonstrated efficacy as dopamine partial agonists for the adjunctive treatments for MDD in clinical trial settings,26–28 little is known about how they compare in terms of their real-world effects on disability outcomes.
Because MDD is associated with a substantial impact on workplace productivity and functionality,29,30 evaluating the effects of different adjunctive AAs on disability outcomes is important to gain an overall understanding of the impacts of these medications. Although previous studies have shown a decreased rate of disability in patients with MDD treated with AAs adjunctive to ADTs,31,32 these previous clinical trials generally used patient-reported outcomes to evaluate disability such as the Sheehan Disability Scale. Conversely, claims-based analyses of disability data can provide a view of the real-world effects of medications on disability outcomes. However, little is known about the real-world implications of AAs on disability outcomes. A previous analysis of disability outcomes using claims data before and after cariprazine initiation found that rates of all-cause and mental health (MH)-related disability claims, days, and costs were significantly lower after cariprazine initiation compared with before cariprazine treatment.33 Nevertheless, the real-world disability outcomes associated with cariprazine compared with other adjunctive dopamine partial agonist AAs, as well as the costs associated with disability among various adjunctive AAs, remains unknown. Therefore, the goal of this analysis was to compare changes in all-cause and MH-related disability claims, days, and costs before and after treatment initiation with cariprazine vs brexpiprazole and cariprazine vs aripiprazole, among patients with MDD using AAs adjunctively to antidepressants.
Materials And Methods
Data Source and Study Design
This was a retrospective, observational cohort study using de-identified data from the MerativeTM MarketScan® Commercial Database and the Health and Productivity Management (HPM) Database (January 1, 2015, to December 31, 2022).34 The commercial database includes enrollment history and claims for medical and pharmacy services for patients from approximately 100 large-scale employers as well as several health plans. The HPM database includes integrated disability data for almost 3 million employees including enrollment in disability insurance plans and short- and long-term disability claims filed by patients with disability insurance, with data provided from employer payroll systems and disability case records by data contributors to the MarketScan Commercial Database. The data are fully linkable to the corresponding medical, pharmacy, and enrollment data for these employees. Details regarding the specific causes of disability are not available in the database, but disability claim records include medical diagnoses associated with the claim. All data are de-identified and compliant with the Health Insurance Portability and Accountability Act; therefore, no institutional review board was required.
The database was used to identify patients diagnosed with MDD who initiated adjunctive treatment with cariprazine, brexpiprazole, or aripiprazole, with the first dispensing defined as the index date (Figure 1). Patient demographics, clinical characteristics, and pre-index disability outcomes were evaluated during the baseline period, which spanned 12 months prior to the index date. Post-index disability outcomes were evaluated during the follow-up period, which was ≥30 days and lasted until the earliest date of the following: 1 year post-index, end of HPM or health insurance eligibility, diagnosis of schizophrenia or schizoaffective disorder, claim for a non-index AA, discontinuation of the index AA or ADT, or end of data availability.
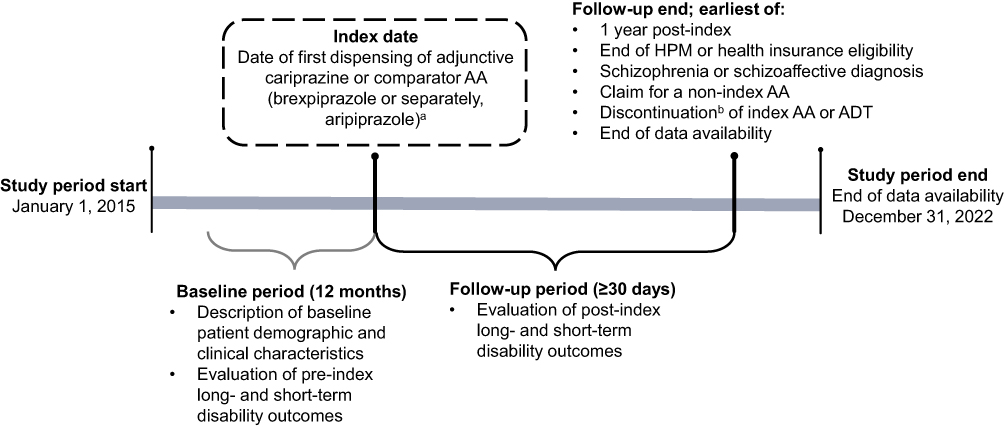 |
Figure 1 Study Design. Abbreviations: AA, atypical antipsychotic; ADT, antidepressant therapy; HPM, Health and Productivity Management. Notes: aPatients newly initiated on cariprazine or brexpiprazole were identified in the cariprazine vs brexpiprazole comparison (and similarly for the cariprazine vs aripiprazole comparison). bDiscontinuation was defined based on a gap of >90 days in days of supply between the end of a dispensing and the next fill or between the last dispensing and the end of the follow-up period. |
Study Population
The analysis included adults (≥18 years old) with ≥2 dispensings of cariprazine, brexpiprazole, or aripiprazole. Separate analyses were conducted to compare cariprazine vs brexpiprazole and cariprazine vs aripiprazole. Evidence of adjunctive therapy with the index AA was required, defined as ≥1 ADT prescription within 90 days before the index date and an overlap of ≥30 days of supply of 1 ADT and the index AA during the 90 days post-index (Supplementary Table 1). Patients were also required to have ≥30 days of follow-up after the index date and ≥12 months of continuous medical, pharmacy, and disability insurance coverage prior to the index date. The study included patients with a confirmed diagnosis of MDD within the 12 months before or on the index date, defined as ≥1 diagnosis in an inpatient setting or ≥2 diagnoses in an outpatient setting (Supplementary Table 2). Patients were excluded from the analysis if they had ≥1 diagnosis of bipolar I disorder, schizophrenia, or schizoaffective disorder during baseline or on the index date. In aiming to isolate our findings to the effects of the AAs of interest opposed to other treatments for major depressive disorder, patients were also excluded from the analysis if they had ≥1 dispensing for a non-index AA or mood stabilizer on the index date.
Study Outcomes
Outcomes included per patient-year (PPY) rates of all-cause and MH-related disability claims and days during baseline and follow-up. Between-cohort differences in means were used to compare the rates of claims and days PPY between adjunctive cariprazine vs adjunctive brexpiprazole and adjunctive cariprazine vs adjunctive aripiprazole. Disability claims and days were considered MH-related if the claim contained a primary or secondary MH diagnosis code. Disability days were measured as the total number of workdays spanned by all short- and long-term disability claims. All disability claims that started on or before the index date were considered baseline disability claims, whereas claims that started after the index date were considered follow-up disability claims.
In addition, all-cause and MH-related disability costs PPY during the baseline and follow-up period were evaluated, with between-cohort differences in means used to compare adjunctive cariprazine vs adjunctive brexpiprazole and adjunctive cariprazine vs adjunctive aripiprazole. When data were available, disability costs were measured using the costs reported on the disability case records. If the cost variable was missing, disability costs were estimated based on the number of short- and long-term disability days, median daily earnings rate (estimated using a median hourly wage of $22.26 based on the May 2022 National Occupational Employment and Wage Estimates for all occupations from the US Bureau of Labor Statistics),35 and earnings replacement rate while on disability. Based on data from the US Bureau of Labor Statistics, the earnings replacement rate was assumed to be 60%.36 Costs were adjusted to 2022 USD using the US hourly compensation price index.35 The imputation of missing or zero costs was performed separately for MH-related and non–MH-related costs; all-cause costs were then calculated as the sum of MH-related and non–MH-related costs, whether imputed or available.
Statistical Analysis
Patients were assigned to mutually exclusive cohorts based on their index AA, and 2 separate pairwise comparisons were evaluated: 1) adjunctive cariprazine vs adjunctive brexpiprazole and 2) adjunctive cariprazine vs adjunctive aripiprazole. Inverse probability of treatment weighting (IPTW) based on the propensity score was used to balance baseline characteristics between patients in the adjunctive cariprazine and adjunctive comparator AA cohorts (brexpiprazole or aripiprazole). Variables used in the propensity score included age at index date, sex, geographic region, year of index date, physician specialty around index date, baseline Quan-Charlson Comorbidity Index (CCI) score, baseline MDD severity, baseline MH-related therapy use, baseline other supportive therapy use, baseline all-cause healthcare resource utilization (hospitalizations, ED visits, outpatient visits), baseline all-cause medical costs, and baseline comorbidities. Comorbidities included in the propensity score were Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) and Elixhauser comorbidities with a standardized difference (std diff) >10% between unweighted AA cohorts and a prevalence in the cariprazine cohort ≥5%. The weight was trimmed at 99th percentile of the distribution.
Patient demographics and clinical characteristics were analyzed using descriptive statistics, including mean, SD, and median values for continuous variables and relative frequencies and proportions for categorical variables. Differences in baseline characteristics between the unweighted AA cohorts were analyzed using std diff; variables with a std diff >10% were considered imbalanced.
A difference-in-difference analysis using a doubly robust approach, in which baseline patient characteristics that remained imbalanced after IPTW were included as covariates in the regression model, was used to compare mean changes in disability outcomes from baseline between the cariprazine and comparator AA cohorts. Specifically, the weighted pre-post difference in PPY disability outcomes for cariprazine was compared with brexpiprazole and aripiprazole (separately) and variables that remained imbalanced after weighting were included as regressors. Generalized linear models with an identity link were used to model the differences between outcomes in pre- and post-AA initiation periods for all outcomes. Statistical significance was determined using P values and 95% CIs, which were calculated using nonparametric bootstrap procedures with 499 resamples. P values <0.05 were considered statistically significant.
Results
Adjunctive Cariprazine vs Adjunctive Brexpiprazole
A total of 867 patients were included in the adjunctive cariprazine vs adjunctive brexpiprazole analysis, with 224 patients in the cariprazine cohort and 643 patients in the brexpiprazole cohort. After IPTW, the average age was 45–46 years, 62%-64% of patients were female, and the majority (73%-77%) of patients had a comorbid anxiety disorder (Table 1; Supplementary Tables 3 and 4). The average length of follow-up in the weighted cariprazine and brexpiprazole cohorts was approximately 4 months.
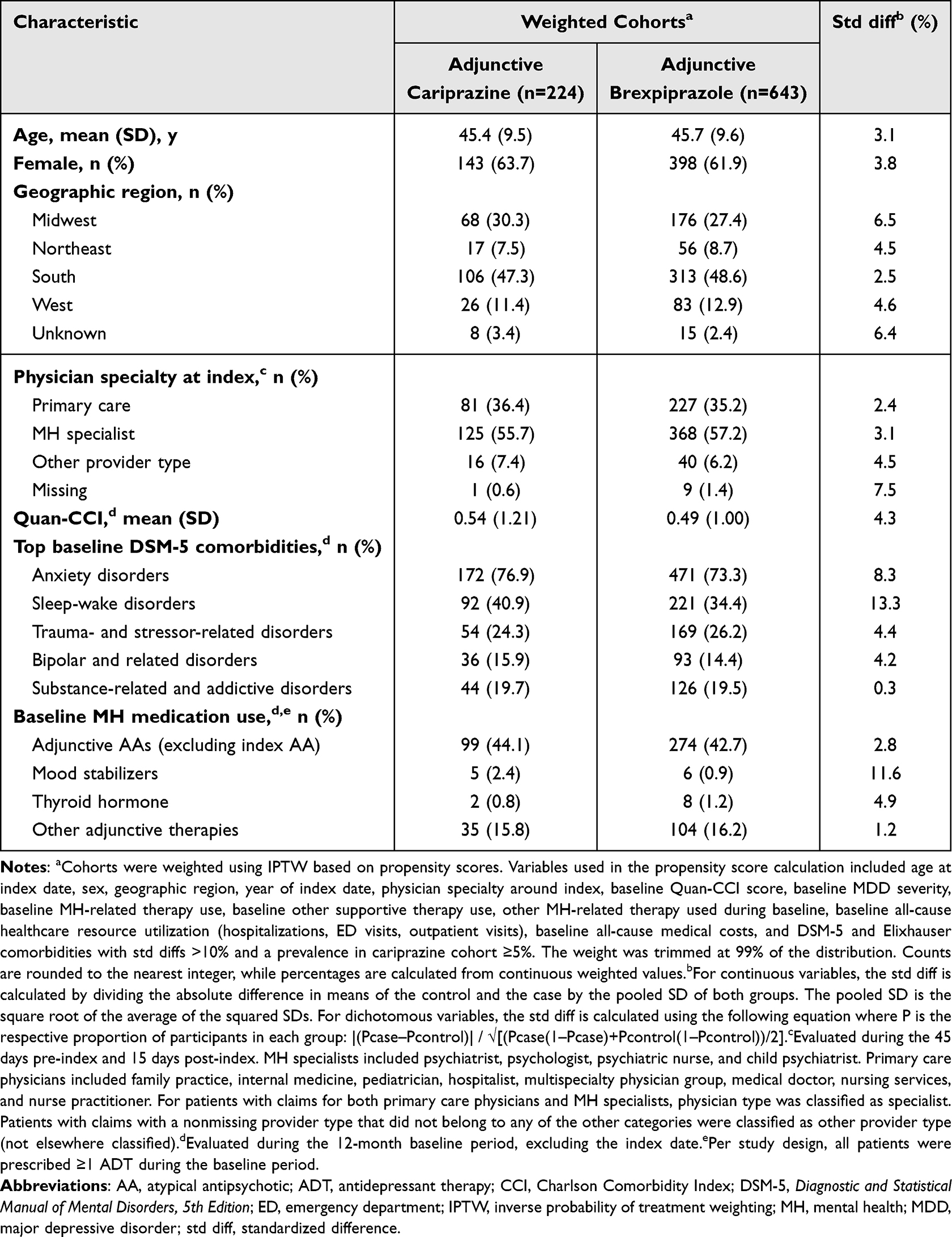 |
Table 1 Baseline Demographics and Clinical Characteristics: Adjunctive Cariprazine Vs Adjunctive Brexpiprazole |
For adjunctive cariprazine users, all-cause disability claims were 0.49 per patient-year (PPY) during the baseline period and 0.28 PPY during follow-up, while for adjunctive brexpiprazole users, all-cause disability claims were 0.44 PPY during the baseline period and 0.43 PPY during follow-up (Table 2); the reduction in all-cause disability claims was significantly greater in patients using adjunctive cariprazine compared with those using adjunctive brexpiprazole (adjusted between-cohort difference in means [95% CI]: −0.23 [−0.45, −0.02], P=0.028; Figure 2A). The rate of MH-related disability claims PPY in the adjunctive cariprazine cohort was 0.25 PPY during baseline and 0.10 PPY during follow-up, whereas the rate in the adjunctive brexpiprazole cohort was 0.21 PPY both before and after starting adjunctive treatment. However, the reduction in MH-related disability claims PPY was not significantly greater in the adjunctive cariprazine cohort relative to the adjunctive brexpiprazole cohort (−0.14 [−0.30, 0.01], P=0.068).
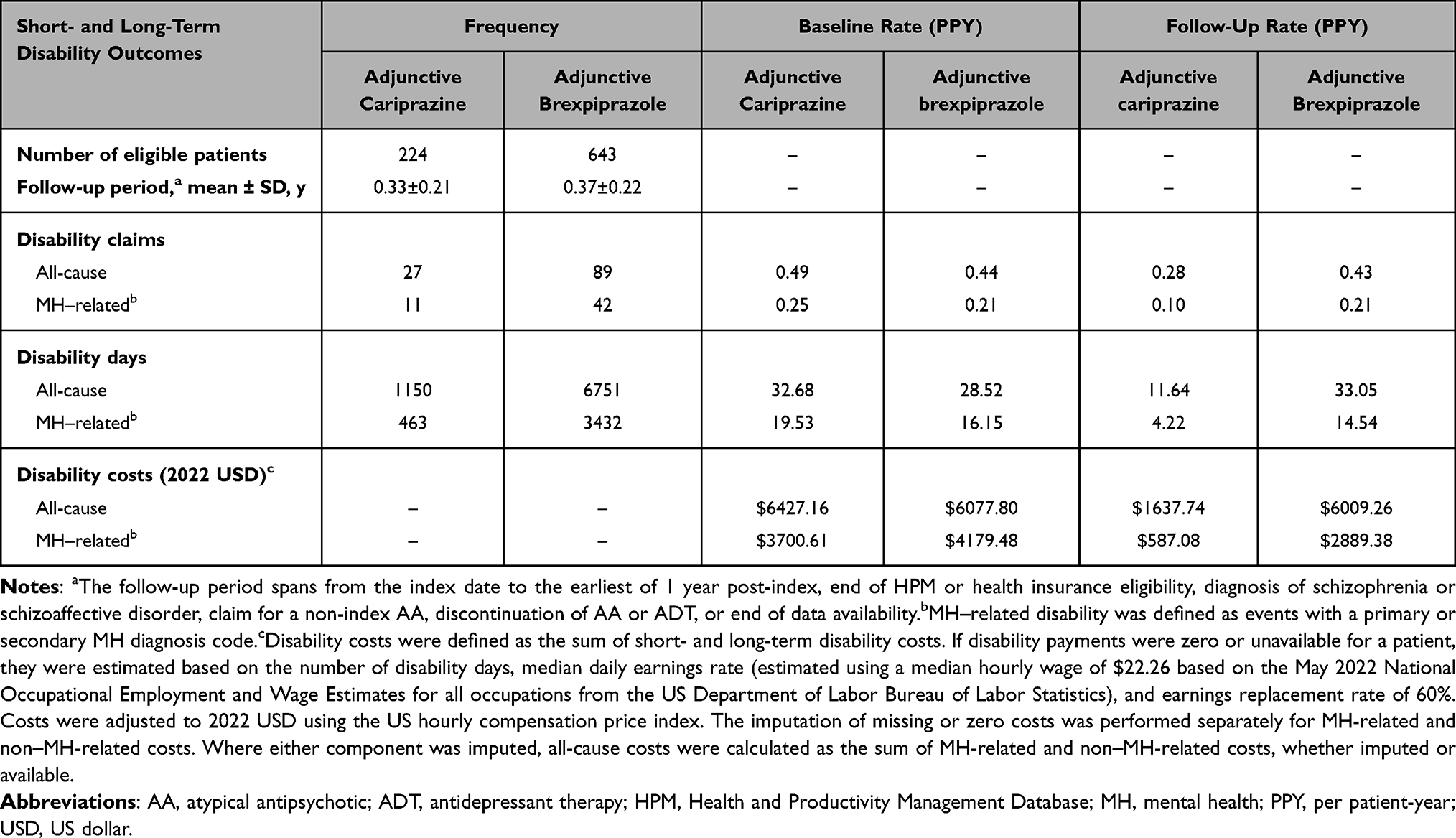 |
Table 2 Frequency and Rates of Short- and Long-Term Disability Outcomes: Adjunctive Cariprazine Vs Adjunctive Brexpiprazole |
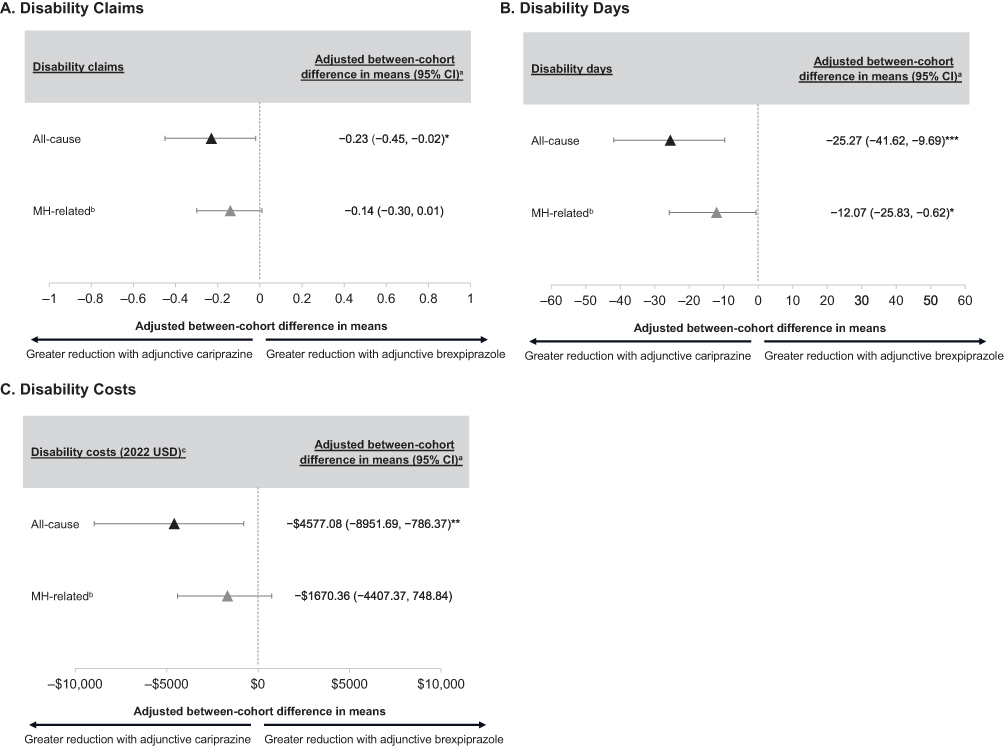 |
Figure 2 Adjusted Mean Between-Cohort Difference in Disability Outcomesa With Adjunctive Cariprazine vs Adjunctive Brexpiprazole (A) Disability Claims (B) Disability Days (C) Disability Costs. Abbreviations: AA, atypical antipsychotic; IPTW, inverse probability of treatment weighting; MH, mental health; PPY, per patient-year; USD, US dollar. Notes: *P<0.05, **P<0.01, ***P<0.001 vs adjunctive brexpiprazole.aThe difference-in-difference analysis evaluated the pre-post change in the outcome among patients treated with adjunctive cariprazine with the pre-post change in outcome among patients treated with the comparator AA (adjunctive brexpiprazole). Baseline patient characteristics that remained imbalanced after IPTW were included as covariates in the regression model. The estimate represents the absolute change in rates or mean costs PPY owing to being part of the cariprazine cohort.bMH-related disability outcomes were defined as claims with a primary or secondary MH diagnosis code.cDisability costs were defined as the sum of short- and long-term disability costs and inflated to 2022 USD using US hourly compensation price index. If disability payments were zero or unavailable for a patient, they were estimated based on the number of disability days, median hourly wage of $22.26, and earnings replacement rate of 60%. |
In the adjunctive cariprazine cohort, the rate of all-cause disability days was 32.68 PPY during the baseline period and 11.64 PPY during follow-up. In the adjunctive brexpiprazole cohort, the baseline rate was 28.52 PPY and the follow-up rate was 33.05 PPY. There was a statistically significantly greater reduction in all-cause disability days PPY for adjunctive cariprazine relative to adjunctive brexpiprazole (adjusted between-cohort difference in means [95% CI]: −25.27 [−41.62, −9.69], P<0.001; Figure 2B). Additionally, the rate of MH-related disability days PPY in the adjunctive cariprazine cohort was 19.53 PPY during the baseline period and 4.22 PPY during follow-up, while the rate in the adjunctive brexpiprazole cohort was 16.15 PPY during the baseline period and 14.54 PPY during follow-up; there was a statistically significantly greater reduction for adjunctive cariprazine relative to adjunctive brexpiprazole (−12.07 [−25.83, −0.62], P=0.032).
Among adjunctive cariprazine users, all-cause baseline disability costs (2022 USD) were $6427.16 PPY during the baseline period and $1637.74 PPY during follow-up. Among adjunctive brexpiprazole users, all-cause disability costs PPY were $6077.80 during baseline and $6009.26 during follow-up. A statistically significantly greater reduction in disability costs was observed for adjunctive cariprazine vs adjunctive brexpiprazole (adjusted between-cohort difference in means [95% CI]: −$4577.08[−8951.69, −786.37], P=0.004; Figure 2C). MH-related disability costs PPY for adjunctive cariprazine users were $3700.61 and $587.08 during baseline and follow-up, respectively, and for adjunctive brexpiprazole users were $4179.48 and $2889.38, respectively. The reduction estimate was similar for adjunctive cariprazine relative to adjunctive brexpiprazole (−$1670.36 [−4407.37, 748.84], P=0.20).
Adjunctive Cariprazine vs Adjunctive Aripiprazole
The adjunctive cariprazine vs adjunctive aripiprazole analysis included 3105 patients, with 174 patients included in the cariprazine cohort and 2931 patients included in the aripiprazole cohort. After IPTW, the average age was approximately 44 years old, 63%–64% of patients were female, 73%-75% of patients had a comorbid anxiety disorder, and the average length of follow-up was approximately 4 months (Table 3; Supplementary Tables 5 and 6).
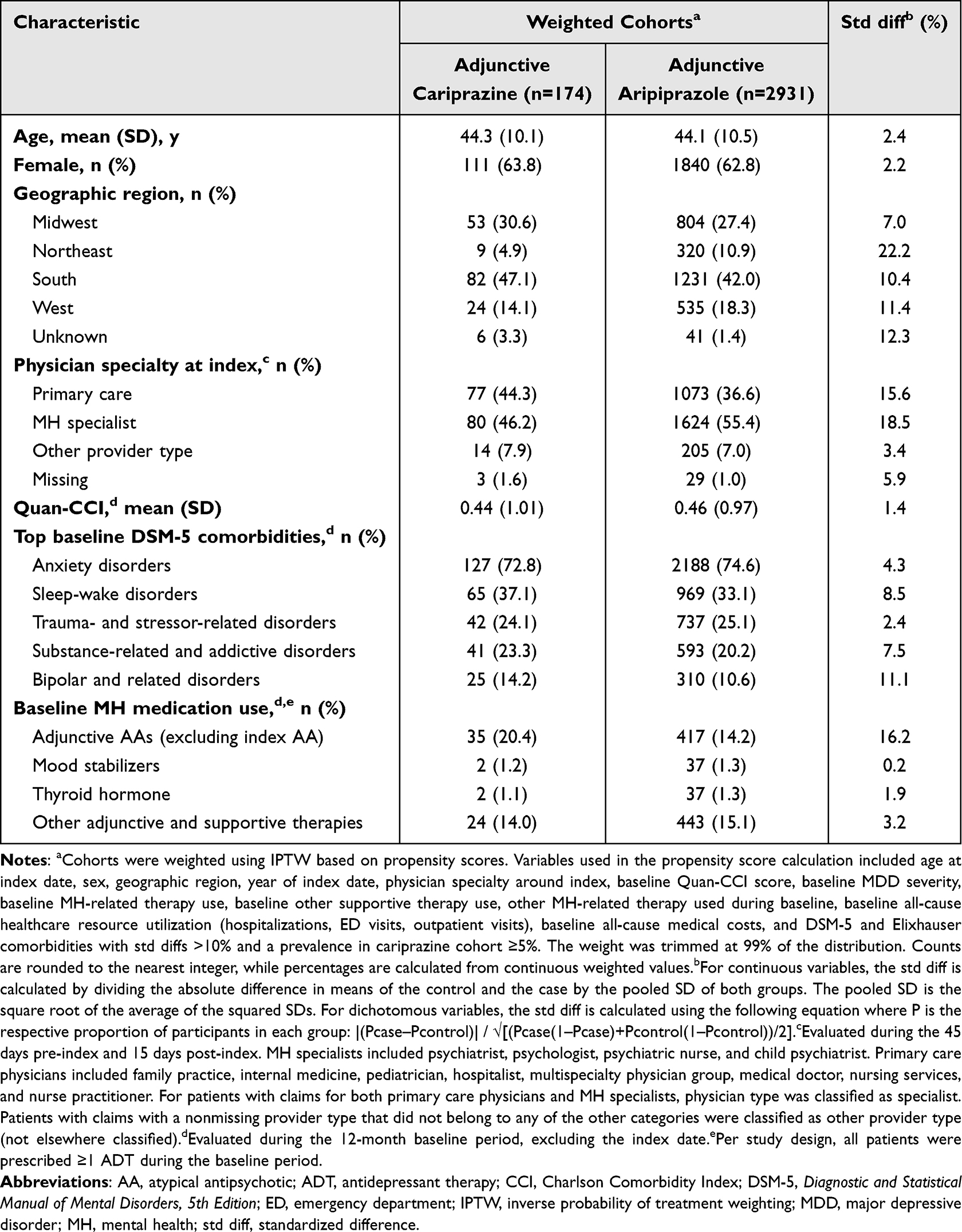 |
Table 3 Baseline Demographics and Clinical Characteristics: Adjunctive Cariprazine Vs Adjunctive Aripiprazole |
All-cause baseline disability claims were 0.51 PPY and 0.51 PPY for adjunctive cariprazine and adjunctive aripiprazole, respectively, and disability claims during follow-up were 0.42 PPY and 0.37 PPY, respectively (Table 4). Additionally, MH-related baseline disability claims were 0.26 PPY and 0.25 PPY for cariprazine and aripiprazole, respectively, and MH-related follow-up disability claims were 0.17 PPY and 0.18 PPY, respectively. The reductions in all-cause and MH-related disability claims were not significantly greater for adjunctive cariprazine relative to adjunctive aripiprazole (adjusted between-cohort difference in means [95% CI], all-cause: −0.11 [−0.30, 0.11], P=0.321; MH-related: −0.08 [−0.21, 0.07], P=0.2855; Figure 3A). Baseline all-cause disability days were 33.61 PPY for adjunctive cariprazine and 34.15 PPY for adjunctive aripiprazole, while follow-up disability days were 20.29 PPY and 25.15 PPY, respectively. Further, MH-related baseline and follow-up disability days were 20.72 PPY and 11.91 PPY for adjunctive cariprazine, respectively, and 20.13 PPY and 12.36 PPY for adjunctive aripiprazole, respectively. Similar to disability claims, the reductions in disability days were not significantly greater for adjunctive cariprazine compared with adjunctive aripiprazole (all-cause: −10.65 [−24.26, 0.75], P=0.072; −7.22 [−18.13, 2.40], P=0.144; Figure 3B).
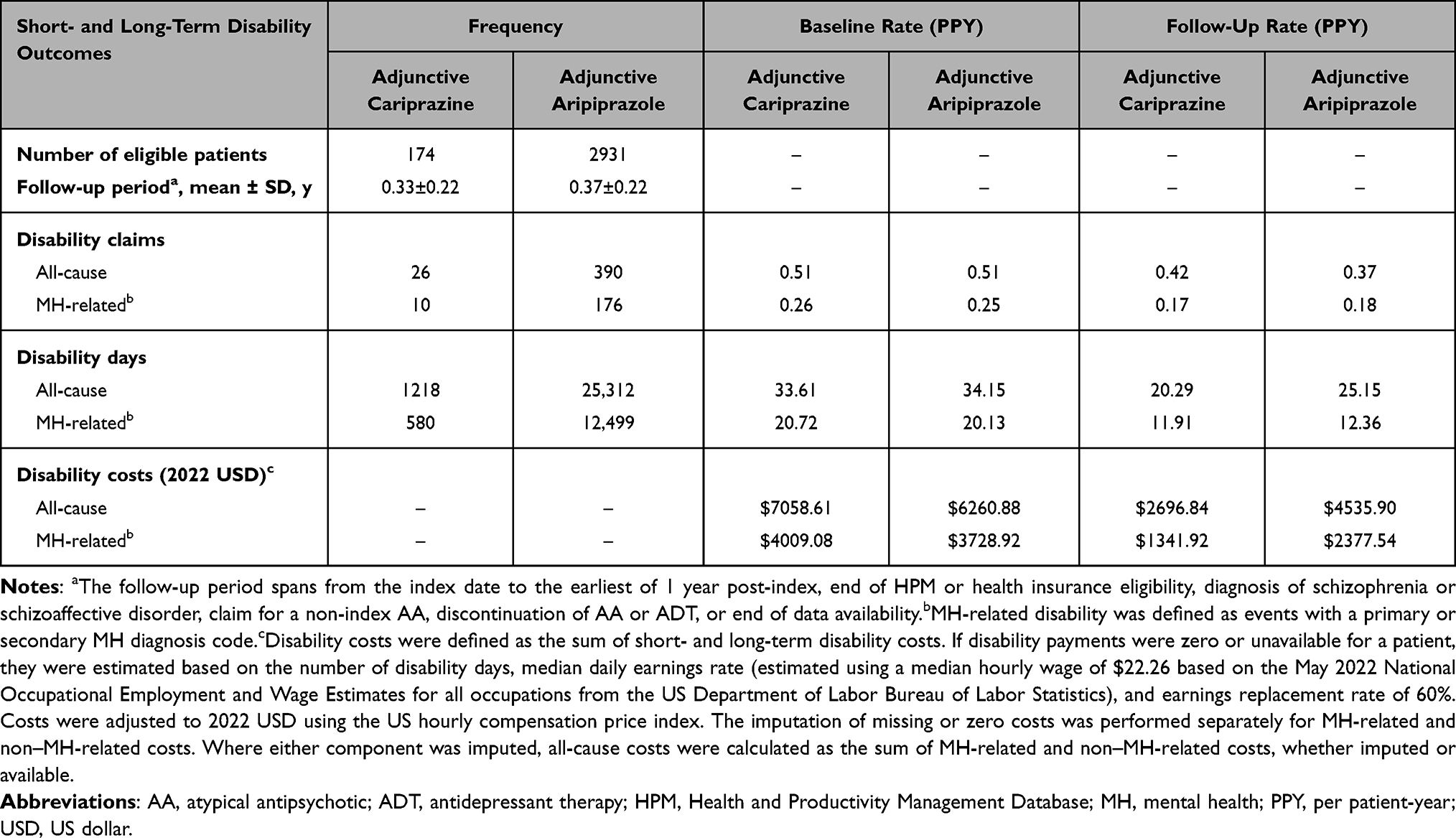 |
Table 4 Frequency and Rates of Short- and Long-Term Disability Outcomes: Adjunctive Cariprazine Vs Adjunctive Aripiprazole |
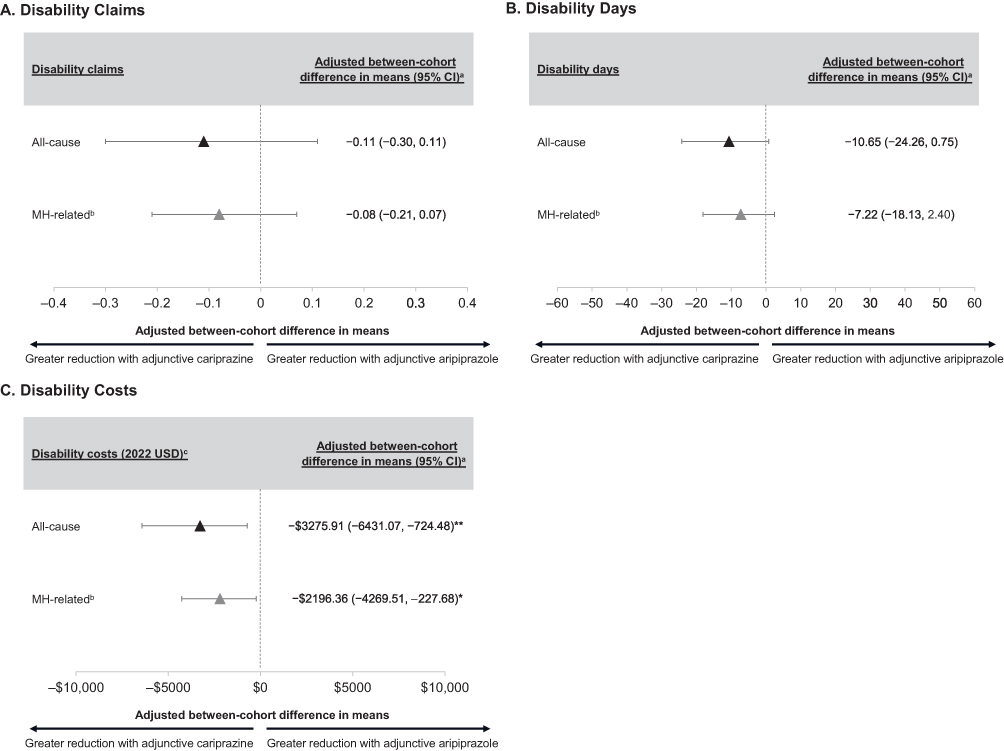 |
Figure 3 Adjusted Mean Between-Cohort Difference in Disability Outcomesa With Adjunctive Cariprazine vs Adjunctive Aripiprazole (A) Disability Claims (B) Disability Days (C) Disability Costs. Abbreviations: AA, atypical antipsychotic; IPTW, inverse probability of treatment weighting; MH, mental health; PPY, per patient-year; USD, US dollar. Notes: *P<0.05, **P<0.01 vs adjunctive aripiprazole.aThe difference-in-difference analysis evaluated the pre-post change in the outcome among patients treated with adjunctive cariprazine with the pre-post change in outcome among patients treated with the comparator AA (adjunctive aripiprazole). Baseline patient characteristics that remained imbalanced after IPTW were included as covariates in the regression model. The estimate represents the absolute change in rates or mean costs PPY owing to being part of the cariprazine cohort.bMH-related disability outcomes were defined as claims with a primary or secondary MH diagnosis code.cDisability costs were defined as the sum of short- and long-term disability costs and inflated to 2022 USD using US hourly compensation price index. If disability payments were zero or unavailable for a patient, they were estimated based on the number of disability days, median hourly wage of $22.26, and earnings replacement rate of 60%. |
Among adjunctive cariprazine users, all-cause disability costs were $7058.61 PPY during the baseline period and $2696.84 PPY during the follow-up period; among adjunctive aripiprazole users, baseline and follow-up costs were $6260.88 PPY and $4535.90 PPY, respectively. The reduction in all-cause disability costs PPY was statistically significantly greater with adjunctive cariprazine compared with adjunctive aripiprazole (adjusted between-cohort difference in means [95% CI]: −$3275.91 [−6431.07, −724.48], P=0.004; Figure 3C). Similarly, MH-related disability costs during baseline and follow-up were $4009.08 PPY and $1341.92 PPY for adjunctive cariprazine users, respectively, and $3728.92 PPY and $2377.54 PPY for adjunctive aripiprazole users, respectively. The reduction was statistically significantly greater with adjunctive cariprazine vs adjunctive aripiprazole (−$2196.36 [−4269.51, −227.68], P=0.028).
Discussion
Despite MDD being a leading cause of disability worldwide,1 little research has been conducted analyzing the effects of medications on real-world disability outcomes. Although previous clinical trials have evaluated disability outcomes in patients with MDD treated with adjunctive AAs using patient reported outcomes,31,32 this claims-based analysis used real-world medical and disability claims to evaluate the changes in disability outcomes before and after treatment with adjunctive cariprazine vs adjunctive brexpiprazole or adjunctive cariprazine vs adjunctive aripiprazole. Results demonstrated that adjunctive cariprazine was associated with significantly lower rates of disability claims and days relative to adjunctive brexpiprazole, while rates were similar for adjunctive cariprazine vs adjunctive aripiprazole. Further, adjunctive cariprazine was associated with significantly greater reductions in all-cause disability costs vs adjunctive brexpiprazole and both all-cause and MH-related disability costs vs adjunctive aripiprazole. These results underscore the extent to which adjunctive AA choice may have real-world implications on disability outcomes in patients with MDD.
The results of our analysis differed when comparing adjunctive cariprazine to adjunctive brexpiprazole and adjunctive cariprazine to adjunctive aripiprazole. In the cariprazine vs brexpiprazole analysis, greater reductions in favor of cariprazine were observed for all outcomes, with statistically significantly greater reductions in all-cause disability claims, days, and costs as well as statistically significantly greater reductions in MH-related disability days. In the cariprazine vs aripiprazole analysis, all-cause and MH-related costs showed a statistically significantly greater reduction in favor of cariprazine vs aripiprazole, while only numerically greater reductions in favor of cariprazine were observed for all other outcomes. The reason for the lack of statistical significance on all-cause and MH-related disability claims and days may be, in part, owing to the smaller cariprazine cohort sample size in the cariprazine vs aripiprazole comparison. The relatively small sample size paired with the rarity of the disability events may compound to generate estimates that do not reach statistical significance at the 0.05 threshold.
The results of the present analysis also showed that disability claims, days, and costs were descriptively lower after treatment with adjunctive cariprazine compared with before treatment in patients with MDD. These results are consistent with a previous claims-based study, which compared disability outcomes during cariprazine treatment with the 12 months prior to cariprazine treatment in patients with MDD, bipolar I disorder, or schizophrenia.33 The previous analysis found that patients treated with cariprazine had statistically significantly lower rates of all-cause and MH-related disability events and days during vs before cariprazine use. Disability-related costs were also significantly lower during cariprazine use than before the initiation of cariprazine. The present analysis supports previous findings and adds important context regarding how adjunctive cariprazine compares with other adjunctive AAs in reducing real-world disability outcomes and costs. Therefore, these results may be useful to clinicians, employers, payers, and other stakeholders when evaluating the choice of initial adjunctive AA treatment for patients with MDD.
Decreased rates of disability outcomes are important from a patient, provider, and societal prospective. From the patients’ perspective, being unable to work due to disability can result in not only financial strain due to lost income but also negatively impact their emotional well-being and may increase stress and further exacerbate symptoms.37 Conversely, steady employment has been shown to enhance self-esteem, improve quality of life, and reduce mental health service use.38 As mental health services emphasize a holistic approach rather than just the treatment of symptoms, treatments that can help to reduce disability outcomes are also valuable from a provider’s perspective.39 Further, because poor functioning is closely associated with disability,40 decreased disability claims and a decreased number of days on disability can be proxy indicators of improvement in a patient’s functional recovery. Therefore, treatments such as cariprazine, which reduce the disability burden for patients and the accompanying economic burden, are valuable from multiple perspectives.
Disability associated with MDD is complex and multifactorial.41,42 One major contributor is impairment in function, which often lags behind symptomatic recovery.43 Although the reasoning for the improvements in disability outcomes observed in this study is unknown and the timeframe was limited, the observed disability improvements may be related to cariprazine’s previously demonstrated efficacy on functional outcomes.44–46 For example, in a post hoc analysis of a Phase 3 clinical trial, patients with MDD who received adjunctive cariprazine 1.5 mg/d or 3 mg/d had significant improvements in the 12-item Short-Form version 2 Health Survey domains of social functioning and role limitations owing to emotional problems relative to patients receiving adjunctive placebo.46 Anhedonia, or the loss of interest or pleasure, is negatively correlated with function and may also play a role in the high rates of disability among patients with MDD.47 In another post hoc analysis of a phase 3 clinical trial evaluating cariprazine for the treatment of MDD, adjunctive cariprazine was associated with improvement in symptoms of depression and anhedonia in patients with moderate to severe anhedonia at baseline.48 Anxiety is also associated with disability and is highly comorbid with MDD,30 which is supported by the current study where >70% of patients in both the cariprazine vs brexpiprazole and cariprazine vs aripiprazole analyses had comorbid anxiety. Cariprazine has previously been shown to decrease anxiety symptoms, with a post hoc analysis of clinical trial data demonstrating that adjunctive cariprazine for the treatment of MDD reduced anxiety symptoms as measured by mean reductions in Hamilton Rating Scale for Depression Anxiety/Somatization scores and Hamilton Anxiety Rating Scale total scores relative to placebo.49 Although further studies are needed to confirm, the positive effects of cariprazine on a wide range of clinical symptoms may have contributed to the descriptively lower rates of disability outcomes and costs observed in this analysis. The efficacy cariprazine has demonstrated across multiple indications, coupled with the decreased disability burden observed in this real-world study, may be important considerations for prescribers when making clinical treatment decisions.
Although the underlying factors resulting in the differences in disability outcomes between cariprazine, brexpiprazole, and aripiprazole are unclear, the D3-preferring pharmacology of cariprazine may play a role given the broad efficacy of cariprazine across depressive and other associated symptoms. While cariprazine, brexpiprazole, and aripiprazole are all dopamine partial agonists, the receptor binding profiles of these compounds differ. Unlike aripiprazole and brexpiprazole, which have a higher affinity for dopamine D2 receptors than D3 receptors, cariprazine has a greater affinity for D3 over D2.22,24,50 D3 receptors are expressed in areas of the brain thought to be involved in the modulation of reward, mood and motivation.51 In preclinical rodent models, cariprazine was associated with anti-anhedonic and pro-cognitive effects, which were found to be mediated through the D3 receptor.52–55 These findings are further supported by clinical data, including the previously-mentioned analyses demonstrating effects of cariprazine on anxiety and anhedonia symptoms as well as other analyses showing cariprazine was associated with significant effects on cognitive symptoms in patients with bipolar I mania, bipolar I depression, and schizophrenia.56 For example, a post hoc analysis evaluating cariprazine and aripiprazole vs placebo in patients with schizophrenia found that cariprazine 3 mg/d was associated with significantly greater improvements vs placebo in cognitive outcomes measuring focused attention and sustained attention, while aripiprazole was not.56 However, the precise underlying factors resulting in differences in disability outcomes between these medications is unknown, and future research into the relationship between symptomatic improvement and improved disability outcomes is warranted.
Limitations
By using data from claims databases, this analysis was able to capture real-world outcomes of patients prescribed different adjunctive AAs; however, the results of this study are subject to limitations that are inherent to claims-based analyses. For example, claims data are vulnerable to omissions and coding errors, although it is not expected that this would affect one cohort more than another. Further, because Merative MarketScan is a commercial database and because disability claims were obtained from employers, results may have limited generalizability to those in the US population with no insurance coverage, with other types of insurance such as Medicaid or Medicare, or who are unemployed. It should also be noted that a pharmacy claim for a dispensed medication does not necessarily indicate that the medication was taken as prescribed, and medications not recorded in the claims data (ie, over-the-counter medications, drug samples, or medications received during an inpatient stay) were not captured in the analysis. Additionally, both the Merative MarketScan and HPM databases may undercount productivity loss because unreported absenteeism and presenteeism are not recorded by the employer and therefore are not included in the database; however, it is expected that this limitation would equally affect both cohorts. The HPM database also does not include specific causes of disability, though it includes diagnosis codes associated with the disability event. Additionally, although a doubly robust approach was used to account for potential between-cohort differences, the possibility of residual confounding remains. The results were also not adjusted for multiple comparisons, although correcting for multiple comparisons is a subject of debate and may reduce power and increase type II errors, contributing to publication bias.57,58 Moreover, we attempted to minimize bias by being intentionally inclusive in our covariate selection for the IPTW, but we acknowledge that residual confounding is always possible due to variables that are not available in claims data. It should also be noted that nonadherence is common in patients with MDD59 and difficult to account for in claims-based analyses; however, follow-up ended once patients discontinued their medication. Another limitation is the short follow-up periods for the patient cohorts in this dataset, which limit the results from being applied to long-term outcomes. Further, inherent to retrospective, observational studies, causality cannot be determined from these data; however, these types of studies are commonly used to evaluate disability outcomes in the real-world.60–62 Last, as cariprazine was not approved for the adjunctive use of MDD until December 2022, cariprazine was used off-label for the majority of the analysis, which may have resulted in the smaller samples sizes.
Conclusion
Among patients with MDD, adjunctive cariprazine was associated with significantly lower rates of disability claims and days compared with adjunctive brexpiprazole. Adjunctive cariprazine was also associated with significantly greater reductions in all-cause disability costs relative to adjunctive brexpiprazole and significantly greater reductions in all-cause and MH-related costs relative to adjunctive aripiprazole. Overall, these real-world outcomes highlight the importance of adjunctive AA choice in mitigating the burden of disability and demonstrate that adjunctive cariprazine may be a useful treatment option in managing the real-world burden of disability in patients with MDD.
Abbreviations
AA, atypical antipsychotic; ADT, antidepressant therapy; CCI, Charlson Comorbidity Index; ED, emergency department; FDA, US Food and Drug Administration; HPM, Health and Productivity Management; IPTW, inverse probability of treatment weighting; MDD, major depressive disorder; MH, mental health; PPY, per patient-year; Std diff, standardized difference; USD, US dollars.
Data Sharing Statement
Data are not available owing to commercial restrictions.
Ethical Approval and Informed Consent
This study was exempt from ethics committee approval and institutional review because it is a retrospective analysis that used anonymized and de-identified data certified as fully compliant with US patient confidentiality requirements set forth in the Health Insurance Portability and Accountability Act of 1996. Allergan (prior to its acquisition by AbbVie) obtained permission to access and use the Merative MarketScan and Health and Productivity Management data used in the analysis through licensing agreements.
Acknowledgments
Medical writing support was provided by Samantha Watry, PharmD, from Citrus Health Group, Inc. (Chicago, IL) and funded by AbbVie.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
AbbVie funded this study and participated in the study design, research, analysis, data collection, interpretation of data, reviewing, and approval of the publication. No honoraria or payments were made for authorship.
Disclosure
P.S. Masand has served as a consultant for Abbvie, Intra-Cellular Therapies, Karuna Therapeutics, Neumora Therapeutics, and Neurocrine Biosciences; has served on speaker’s bureaus for AbbVie, BMS, Neurocrine Biosciences, and Vanda Pharmaceuticals; and has stock ownership in Relmada Therapeutics. M. Parikh, J. Ta, F. Haile, and N. Nabulsi are employees of AbbVie and may hold stock. S.W. Wade is a partner in Wade Outcomes Research and Consulting and a consultant for AbbVie. S. Ripley, E. Zanardo, C. Spencer, and F. Laliberté are employees of Analysis Group, which was funded by AbbVie to conduct the analyses. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva, Switzerland; 2017.
2. Culpepper L, Martin A, Nabulsi N, Parikh M. The humanistic and economic burden associated with major depressive disorder: a retrospective cross-sectional analysis. Adv Ther. 2024;41(5):1860–1884. doi:10.1007/s12325-024-02817-w
3. Greenberg PE, Fournier AA, Sisitsky T, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics. 2021;39(6):653–665. doi:10.1007/s40273-021-01019-4
4. Greenberg P, Chitnis A, Louie D, et al. The economic burden of adults with major depressive disorder in the United States. Adv Ther. 2023;40(10):4460–4479. doi:10.1007/s12325-023-02622-x
5. Bush PW, Drake RE, Xie H, McHugo GJ, Haslett WR. The long-term impact of employment on mental health service use and costs for persons with severe mental illness. Psychiatr Serv. 2009;60(8):1024–1031. doi:10.1176/ps.2009.60.8.1024
6. Brody DJ, Pratt LA, Hughes JP. Prevalence of depression among adults aged 20 and over: united States, 2013-2016. NCHS Data Brief. 2018(303):1–8.
7. Richards D. Prevalence and clinical course of depression: a review. Clin Psychol Rev. 2011;31(7):1117–1125. doi:10.1016/j.cpr.2011.07.004
8. Severe J, Greden JF, Reddy P. Consequences of recurrence of major depressive disorder: is stopping effective antidepressant medications ever safe? Focus. 2020;18(2):120–128. doi:10.1176/appi.focus.20200008
9. Moylan S, Maes M, Wray NR, Berk M. The neuroprogressive nature of major depressive disorder: pathways to disease evolution and resistance, and therapeutic implications. Mol Psychiatry. 2013;18(5):595–606. doi:10.1038/mp.2012.33
10. Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice Guideline for the Treatment of Patients with Major Depressive Disorder.
11. Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006;163(1):28–40. doi:10.1176/appi.ajp.163.1.28
12. Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. pharmacological treatments. Can J Psychiatry. 2016;61(9):540–560. doi:10.1177/0706743716659417
13. Patkar AA, Pae CU. Atypical antipsychotic augmentation strategies in the context of guideline-based care for the treatment of major depressive disorder. CNS Drugs. 2013;27(Suppl 1):S29–37. doi:10.1007/s40263-012-0031-0
14. Nelson JC, Papakostas GI. Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials. Am J Psychiatry. 2009;166(9):980–991. doi:10.1176/appi.ajp.2009.09030312
15. Papakostas GI, Shelton RC, Smith J, Fava M. Augmentation of antidepressants with atypical antipsychotic medications for treatment-resistant major depressive disorder: a meta-analysis. J Clin Psychiatry. 2007;68(6):826–831. doi:10.4088/JCP.v68n0602
16. Thase ME. Update on partial response in depression. J Clin Psychiatry. 2009;70(Suppl 6):4–9. doi:10.4088/JCP.8133su1c.01
17. Papakostas GI, Petersen TJ, Green C, et al. A description of next-step switching versus augmentation practices for outpatients with treatment-resistant major depressive disorder enrolled in an academic specialty clinic. Ann Clin Psychiatry. 2005;17(3):161–165. doi:10.1080/10401230591002129
18. Philip NS, Carpenter LL, Tyrka AR, Price LH. Pharmacologic approaches to treatment resistant depression: a re-examination for the modern era. Expert Opin Pharmacother. 2010;11(5):709–722. doi:10.1517/14656561003614781
19. Seetasith A, Greene M, Hartry A, Burudpakdee C. Changes in healthcare resource use and costs associated with early versus delayed initiation of atypical antipsychotic adjunctive treatment in major depressive disorder. J Med Econ. 2018;21(9):888–901. doi:10.1080/13696998.2018.1484373
20. Jain R, Laliberte F, Germain G, et al. Treatment patterns, health care resource utilization, and costs associated with use of atypical antipsychotics as first vs subsequent adjunctive treatment in major depressive disorder. J Manag Care Spec Pharm. 2023;29(8):896–906. doi:10.18553/jmcp.2023.29.8.896
21. Keks N, Hope J, Schwartz D, McLennan H, Copolov D, Meadows G. comparative tolerability of dopamine D2/3 receptor partial agonists for schizophrenia. CNS Drugs. 2020;34(5):473–507. doi:10.1007/s40263-020-00718-4
22. Otsuka Pharmaceutical Co. Abilify (Aripiprazole). full prescribing information. otsuka pharmaceutical co.; 2024.
23. Otsuka Pharmaceutical Co. Rexulti (brexpiprazole). full prescribing information. otsuka pharmaceutical co.2024.
24. AbbVie, Inc. VRAYLAR®. (Cariprazine).full Prescribing Information. AbbVie, Inc.; 2024.
25. Girgis RR, Slifstein M, D’Souza D, et al. Preferential binding to dopamine D3 over D2 receptors by cariprazine in patients with schizophrenia using PET with the D3/D2 receptor ligand [(11)C]-(+)-PHNO. Psychopharmacol. 2016;233(19–20):3503–3512. doi:10.1007/s00213-016-4382-y
26. Sachs GS, Yeung PP, Rekeda L, Khan A, Adams JL, Fava M. Adjunctive cariprazine for the treatment of patients with major depressive disorder: a randomized, double-blind, placebo-controlled phase 3 study. Am J Psychiatry. 2022;180(3):241–251. doi:10.1176/appi.ajp.20220504
27. Hobart M, Skuban A, Zhang P, et al. Efficacy and safety of flexibly dosed brexpiprazole for the adjunctive treatment of major depressive disorder: a randomized, active-referenced, placebo-controlled study. Curr Med Res Opin. 2018;34(4):633–642. doi:10.1080/03007995.2018.1430220
28. Berman RM, Marcus RN, Swanink R, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2007;68(6):843–853. doi:10.4088/JCP.v68n0604
29. Trivedi MH, Corey-Lisle PK, Guo Z, Lennox RD, Pikalov A, Kim E. Remission, response without remission, and nonresponse in major depressive disorder: impact on functioning. Int Clin Psychopharmacol. 2009;24(3):133–138. doi:10.1097/YIC.0b013e3283277614
30. Hendriks SM, Spijker J, Licht CM, et al. Long-term work disability and absenteeism in anxiety and depressive disorders. J Affect Disord. 2015;178:121–130. doi:10.1016/j.jad.2015.03.004
31. Kennedy SH, Lam RW, Rotzinger S, et al. Symptomatic and functional outcomes and early prediction of response to escitalopram monotherapy and sequential adjunctive aripiprazole therapy in patients with major depressive disorder: a CAN-BIND-1 report. J Clin Psychiatry. 2019;80(2). doi:10.4088/JCP.18m12202.
32. Fava M, Okame T, Matsushima Y, Perry P, Weiller E, Baker RA. Switching from inadequate adjunctive or combination treatment options to brexpiprazole adjunctive to antidepressant: an open-label study on the effects on depressive symptoms and cognitive and physical functioning. Int J Neuropsychopharmacol. 2017;20(1):22–30. doi:10.1093/ijnp/pyw087
33. Nabulsi N, Parikh M, Ta J, et al. The impact of cariprazine on short- and long-term disability among commercially insured patients.
34. Merative MMRD. 2022. Available from: https://www.merative.com/documents/merative-marketscan-research-databases.
35. May 2022 National Occupational Employment and Wage Estimates. US Bureau of Labor Statistics. 2022. Available from: https://www.bls.gov/oes/2022/may/oes_nat.htm#00-0000.
36. Monaco K. Disability insurance plans: trends in employee access and employer costs. Beyond the numbers: pay and benefits. U.S. Bureau of Labor Statistics. 2015.
37. Namkung EH, Carr D. the psychological consequences of disability over the life course: assessing the mediating role of perceived interpersonal discrimination. J Health Soc Behav. 2020;61(2):190–207. doi:10.1177/0022146520921371
38. Drake RE, Skinner JS, Bond GR, Goldman HH. Social security and mental illness: reducing disability with supported employment. Health Aff. 2009;28(3):761–770. doi:10.1377/hlthaff.28.3.761
39. Fukuura Y, Shigematsu Y. The work ability of people with mental illnesses: a conceptual analysis. Int J Environ Res Public Health. 2021;18(19):10172. doi:10.3390/ijerph181910172
40. Linden M. Definition and assessment of disability in mental disorders under the perspective of the International claSsification of Functioning disability and health (ICF). Behav Sci Law. 2017;35(2):124–134. doi:10.1002/bsl.2283
41. Peng R, Wang Y, Huang Y, et al. The association of depressive symptoms with disability among adults in China. J Affect Disord. 2022;296:189–197. doi:10.1016/j.jad.2021.09.030
42. Holma IA, Holma KM, Melartin TK, Rytsälä HJ, Isometsä ET. A 5-year prospective study of predictors for disability pension among patients with major depressive disorder. Acta Psychiatr Scand. 2012;125(4):325–334. doi:10.1111/j.1600-0447.2011.01785.x
43. Sheehan DV, Harnett-Sheehan K, Spann ME, Thompson HF, Prakash A. Assessing remission in major depressive disorder and generalized anxiety disorder clinical trials with the discan metric of the Sheehan disability scale. Int Clin Psychopharmacol. 2011;26(2):75–83. doi:10.1097/YIC.0b013e328341bb5f
44. Parikh M, Adams JL, Rekeda L, Yee T, Gleeson M, Nabulsi N. Impact of adjunctive cariprazine on quality of life in major depressive disorder: a post hoc analysis. In: Presented At: Psych Congress. Nashville, TN; 2023.
45. Vieta E, Calabrese JR, Whelan J, Tohen M, Earley WR. The efficacy of cariprazine on function in patients with bipolar depression: a post hoc analysis of a randomized controlled trial. Curr Med Res Opin. 2021;37(9):1635–1643. doi:10.1080/03007995.2021.1932446
46. Parikh M, Matthews-Hayes T, Adams JL, Kandukuri L, Yee T, Nabulsi N. Impact of adjunctive cariprazine on mental health–related quality of life in patients with major depressive disorder: a pooled post hoc analysis of clinical trial data.
47. Wong S, Le GH, Phan L, et al. Effects of anhedonia on health-related quality of life and functional outcomes in major depressive disorder: a systematic review and meta-analysis. J Affect Disord. 2024;356:684–698. doi:10.1016/j.jad.2024.04.086
48. McIntyre RS, Maletic V, Masand P, et al. Effect of adjunctive cariprazine on symptoms of anhedonia in patients with major depressive disorder.
49. Fava M, Masand PS, Maletic V, Chen C, Adams JL, Kerolous M. Efficacy of adjunctive cariprazine on anxiety symptoms in patients with major depressive disorder: post hoc analysis of a randomized placebo-controlled trial. J Clin Psychiatry. 2025;86(2):24m15506. doi:10.4088/JCP.24m15506
50. Otsuka Pharmaceutical Co. L. REXULTI (brexpiprazole). Full Prescribing Information. 2024.
51. Sokoloff P, Le Foll B. The dopamine D3 receptor, a quarter century later. Eur J Neurosci. 2017;45(1):2–19. doi:10.1111/ejn.13390
52. Duric V, Banasr M, Franklin T, et al. Cariprazine exhibits anxiolytic and dopamine D3 receptor-dependent antidepressant effects in the chronic stress model. Int J Neuropsychopharmacol. 2017;20(10):788–796. doi:10.1093/ijnp/pyx038
53. Zimnisky R, Chang G, Gyertyan I, Kiss B, Adham N, Schmauss C. Cariprazine, a dopamine D(3)-receptor-preferring partial agonist, blocks phencyclidine-induced impairments of working memory, attention set-shifting, and recognition memory in the mouse. Psychopharmacology. 2013;226(1):91–100. doi:10.1007/s00213-012-2896-5
54. Papp M, Gruca P, Lason-Tyburkiewicz M, Adham N, Kiss B, Gyertyan I. Attenuation of anhedonia by cariprazine in the chronic mild stress model of depression. Behav Pharmacol. 2014;25(5–6):567–574. doi:10.1097/FBP.0000000000000070
55. Gyertyan I, Saghy K, Kassai F, Kiss B, Szombathelyi Z. Anxiolytic-like activity in rat models of cariprazine (RGH-188), a dopamine d3 receptor preferring antipsychotic agent with d3/d2 receptor partial agonist activity.
56. McIntyre RS, Daniel DG, Vieta E, et al. The efficacy of cariprazine on cognition: a post hoc analysis from Phase II/III clinical trials in bipolar mania, bipolar depression, and schizophrenia. CNS Spectr. 2023;28(3):319–330. doi:10.1017/S109285292200013X
57. Saville DJ. Basic statistics and the inconsistency of multiple comparison procedures. Can J Exp Psychol. 2003;57(3):167–175. doi:10.1037/h0087423
58. Nakagawa S. A farewell to Bonferroni: the problems of low statistical power and publication bias. Behav Ecol. 2004;15(6):1044–1045. doi:10.1093/beheco/arh107
59. Lassen RH, Gonçalves W, Gherman B, et al. medication non-adherence in depression: a systematic review and metanalysis. Trends Psychiatry Psychother. 2024. doi:10.47626/2237-6089-2023-0680
60. Ivanova JI, Birnbaum HG, Kidolezi Y, Subramanian G, Khan SA, Stensland MD. Direct and indirect costs of employees with treatment-resistant and non-treatment-resistant major depressive disorder. Curr Med Res Opin. 2010;26(10):2475–2484. doi:10.1185/03007995.2010.517716
61. Gaspar FW, Wizner K, Morrison J, Dewa CS. The influence of antidepressant and psychotherapy treatment adherence on future work leaves for patients with major depressive disorder. BMC Psychiatry. 2020;20(1):320. doi:10.1186/s12888-020-02731-9
62. Jerry M, Arcona S, McMorrow D, Schwartz H, Princic N, Sasane R. Work loss and direct and indirect costs associated with parkinson’s disease. Clinicoecon Outcomes Res. 2023;15:309–319. doi:10.2147/CEOR.S398509
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Measuring Response to Adjunctive Therapy Among Individuals with Major Depressive Disorder
Forma F, Liberman JN, Rui P, Wiggins E, Ruetsch C
Neuropsychiatric Disease and Treatment 2022, 18:2467-2475
Published Date: 28 October 2022
Life Engagement Improvement Following Initiation of Brexpiprazole Treatment in Patients with MDD: A Naturalistic, Retrospective Real-World Study
Wee SN, Liman C, Waters HC, Houle CR, Renteria M, Mukherjee SS, Surendran S, Marcovici J, Brubaker M, Rasmussen Meehan S, de Jong-Laird A, Rush AJ, Sarkar J
ClinicoEconomics and Outcomes Research 2023, 15:195-208
Published Date: 18 March 2023
Efficacy and Clinical Relevance of Adjunctive Cariprazine Treatment in Patients with Major Depressive Disorder: Post Hoc Analyses from a Phase III Study
Papakostas GI, Masand PS, Clayton AH, Maletic V, Adams JL, Rekeda L, Singh MK, Kerolous M
Neuropsychiatric Disease and Treatment 2026, 22:561112
Published Date: 1 April 2026