Back to Journals » Patient Related Outcome Measures » Volume 14
Quantitative Global Survey Results of Acute Back Pain Sufferers Across Four Countries
Authors Maybaum N, Rios-Martinez S ![]() , Johnson M
, Johnson M
Received 22 November 2022
Accepted for publication 25 April 2023
Published 3 May 2023 Volume 2023:14 Pages 97—110
DOI https://doi.org/10.2147/PROM.S396674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Nadine Maybaum,1 Salvador Rios-Martinez,2 Martin Johnson3
1Haleon, Warren, NJ, USA; 2Internal Medicine Specialist Private Practice, Mexico City, Mexico; 3St Pancras Clinical Research, London, UK
Correspondence: Nadine Maybaum, Haleon, 184 Liberty Corner Road, Warren, NJ, 07059, USA, Tel +1 908 293-4000, Email [email protected]
Background: Surveys of back pain sufferers in the United States, China, Russia, and Germany were performed to better understand self-reported causes of acute nonspecific back pain and acute lower back pain among individuals engaging in sports and their preferred treatments.
Methods: In each country, 1000 participants were surveyed (Step 1) to identify a population of nonspecific acute back pain sufferers, understand pain and treatment characteristics, and generate profiles for individuals with long-lasting (≥ 7 days) acute lower back pain. Subsequently, 200 participants with acute lower back pain episodes (7– 21 days) and sports participation were identified in each country and completed surveys (Step 2) about sociodemographic, pain, treatment characteristics, and causes/triggers of long-lasting acute lower back pain episodes.
Results: In the United States, China, Russia, and Germany, respectively, 59%, 49%, 61%, and 63% of respondents reported ≥ 1 episode of nonspecific acute back pain in the previous 6 months. Average numbers of monthly nonspecific acute back pain episodes in the United States, Russia, Germany, and China were 2.5, 1.8, 1.3, and 0.8, respectively. Prevalence of acute lower back pain associated with sports/leisure activities ranged from 20% (Russia and Germany) to 46% (China). Onset of long-lasting acute lower back pain was between ages 30 and 33 years, limiting usual activities and reducing walking distance in 60% to 85% of respondents across all countries. Acute lower back pain started post-exercise within the first day for ≥ 75% of respondents. Most popular nonprescription and prescription treatments for acute lower back pain were creams/gels in Russia, creams/gels and oral painkillers in Germany, oral painkillers in the United States, and hot/cold patches in China.
Conclusion: These results help to better understand acute back pain triggers, features, and treatment preferences among sports participants in different countries. Further research is warranted to develop preventative strategies.
Trial Registration: Not applicable.
Keywords: lower back pain, surveys and questionnaires, acute pain, sports
Background
The global burden of back pain is substantial and is expected to increase as the world population ages, placing additional strains on health-care systems and economies.1–3 Back pain is a leading cause of physical suffering and is associated with a broad range of negative health and social effects.1 According to the Global Burden of Disease Study 2016, low back pain affects more than 500 million people and is the single leading cause of disability worldwide.4
A systematic review of back pain data from 54 countries found that lifetime prevalence is approximately 39%, occurring most often in people between 40 and 80 years of age.3 Back pain is one of the most frequent reasons people seek medical care, although care-seeking behaviors and treatment perceptions vary substantially between countries and regions based, in part, on cultural, demographic, and social characteristics.5,6 For example, in the United States (US), nearly two-thirds of adults will visit a health-care professional (HCP) because of back pain at some point during their lives, and Americans perceive physical therapy, chiropractic care, and prescription medications to be the most effective treatments.7 For comparison, in China, back pain is more common than in the US or Europe, and two-thirds of pain sufferers in China report using traditional Chinese medicine (eg, acupuncture) to treat back pain,8 some of whom also used Western-style pain management strategies.8
While the global burden of back pain is well established, the causes of, and the modifiable risk factors for, acute nonspecific back pain remain poorly understood.1,9,10 Certain regular activities such as recreational walking, vigorous gardening, and heavy housework have been associated with increased risk for back pain; however, contradictory findings have been reported on the associations between physical activity and back pain.11 It is particularly unclear whether participation in different types of sporting activities increases or decreases risk for developing back pain.12 Better understanding of these underlying causes of, and the modifiable risk factors for, back pain can help HCPs develop prevention and treatment strategies to better optimize patient care.10,12
Here, we report findings from 2 quantitative surveys performed to develop profiles of acute nonspecific back pain sufferers in 4 countries (the US, China, Germany, and Russia) with different cultural and sociodemographic perceptions of back pain. These surveys were designed to provide insight into the types of activities that result in or precede episodes of acute back pain lasting at least 7 days, with an emphasis on identifying sporting activities in each country that are most likely to be the trigger of back pain.
Methods
The global market and opinion research company Ipsos (Paris, France) was contracted to conduct a 2-step noninterventional questionnaire study in the US, China, Russia, and Germany. Ethics approval was not required by Haleon or Ipsos because this was a survey, and respondents had no contact with any type of health-care professional or product at any time in the process of the research. All participants provided informed consent through Ipsos Terms & Conditions at the time of study conduct in 2016.
Step 1
Participants in Step 1 were recruited via Ipsos panels in the US, Germany, Russia, and China. A total of 1000 participants in each of these 4 countries were surveyed to identify and understand self-diagnosed acute nonspecific back pain (includes upper, middle, and lower back pain) sufferers. The goals of the first step were to estimate the population size of acute nonspecific back pain sufferers who use over-the-counter medications to manage their pain, to understand the intensity and duration of back pain, and to identify the activities that trigger back pain. In this step, nationally representative samples of 1000 individuals in each country participated in ~7-minute surveys (survey questionnaire provided in the Supplementary Appendix) between March and May 2016. Quotas based on available census data for each country were applied with respect to categories of age, gender, and region to minimize bias stemming from over-representation of particular subgroups and to ensure that all categories carried similar weight to those of the national population.
Eligible participants must have experienced at least one episode of acute pain symptoms (generally lasting up to 7 days, with prolongation up to 30 days)13 in the upper back (including neck and shoulder), lower back, or middle back in the past 6 months. Participants were excluded if they experienced chronic back pain, defined as occurring for ≥12 weeks. Survey questions focused on acute nonspecific back pain triggers, types of treatments used, pain intensity (on an 11-point scale), duration of pain (in days/hours), and participation in sports or leisure activities. Index values were used to compare the profiles of long-lasting acute back pain sufferers identified in Step 1 with the profiles of the national representative population for each country. Index values were calculated by dividing the percentage of long-lasting acute back pain sufferers in the surveyed sample by the percentage obtained for the national representative population for each country. Index values >120 identified over-represented subpopulations among long-lasting back pain sufferers, which was used for recruitment and analysis of participants in Step 2. Further details and results from data analyses based on index values are provided in the Supplementary Appendix.
Step 2
The objective of Step 2 was to determine the profiles of participants experiencing long-lasting (≥7 days) acute lower back pain. Analyses from Step 1 were used to inform Step 2, which focused on a separate target population (200 survey participants per sport, at least 600 participants from each country) with long-lasting acute lower back pain (7–21 days) in the past 6 months who participated in each of the 3 key sport activities specific to each country (ie, the most common sport activities identified as being a main trigger for acute nonspecific lower back pain in that country). Participants from the US, Germany, and Russia were recruited via Ipsos panels; those from China were recruited via face-to-face encounters at sporting facilities (eg, Badminton clubs). In Step 2, participants completed a 15-minute survey (survey questionnaire provided in the Supplementary Appendix).
Prescreening
Participants were randomly selected according to their age, gender, and region; those who had completed an excessive number of prior surveys were excluded. Participants in Step 1 were prescreened using the WebCruiser14 online panel screening tool in the US, Germany, and Russia, and using an offline street intercept method in China. The purpose of the WebCruiser was to identify and then target the preselected special interest groups (back pain sufferers). If qualified, prescreened individuals were directed to the main screener/questionnaire. The surveys in Step 2 were conducted throughout multiple online panels in the US, Germany, and Russia, either Ipsos-owned or external, while they took place in public locations that reproduced similar online research conditions (eg, hall location, cyber-café) in China. Panelists were recruited via a double opt-in approach with standard quality checks, which included country validation via geographic internet protocol, mismatch detection between device settings and geographic location, anonymous proxy detection, detection of robots via Captcha code, detection of data anomalies and patterns, maintenance of Ipsos blacklist, and Real Answer® (Imperium; Shelton, CT, US) technology–based detection of pasted and robot answers. Strict panel usage rules were applied to avoid frequently interviewing the same people so as to prevent them from becoming too accustomed to a particular type of survey or product category. All surveys were conducted on auto-administrated mode. Step 2 survey questions focused on sociodemographic characteristics; perception of pain severity, frequency, and annoyance; types of treatments and combination treatments used; causes and triggers of long-lasting acute lower back pain episodes; and specific activities or occasions that generate or increase acute lower back pain (eg, a golf weekend).
Statistical Methods
Differences between countries and differences between sports/activities were analyzed using a 2-proportion Z test at a 5% significance level. Multiple comparisons were performed by comparing the numbers of respondents for each activity between every 2 columns for a particular country or between 2 countries, and by comparing the number of respondents within each column with the total number of respondents within a single country or across all 4 countries. All other statistics were descriptive.
Results
Step 1
Nationally representative surveys showed that roughly half to two-thirds of the population in each country suffered from acute nonspecific back pain in the past 6 months (US, 59%; China, 49%; Russia, 61%; and Germany, 63%). The majority of survey respondents from each country were employed full-time; the occupations of respondents ranged from physically demanding jobs (ie, plant-machine operators/assemblers) to sedentary jobs (ie, office workers) within each country. The average number of reported acute nonspecific back pain episodes per month was higher in the US (2.5) than in Russia (1.8), Germany (1.3), and China (0.8). Acute nonspecific back pain episodes lasted more than 7 days for one-quarter or more of respondents in the US (27%), Russia (25%), and Germany (28%), and for 16% of respondents in China. The percentage of acute nonspecific back pain–only (excluding shoulder and neck pain) episodes lasting more than 7 days was similar in the US (8.3%) and Germany (8%) and was less frequent in China (3%) and Russia (6%).
Overall, about two-thirds of acute nonspecific back pain episodes were attributed to or associated with regular daily activities (Figure 1) and about one-third with sporting activities. Self-reported causes of acute nonspecific back pain are summarized in Table 1. The most commonly self-reported regular activities causing acute nonspecific back pain were those associated with daily prolonged static posture, including sitting at a computer (15% to 32% across countries) and sitting at work (12% to 20%). Leisure activities that require bending or leaning for extended time periods were also reported causes of acute nonspecific back pain (eg, gardening [5% to 32%], home improvement projects [11% to 14%], and using a computer [7% to 25%]). Individual sport activities, such as gym workouts (17% to 26%) and running (6% to 16%) were reported to be the most likely causes of acute nonspecific back pain, and lack of professional supervision increased risk of injuries.
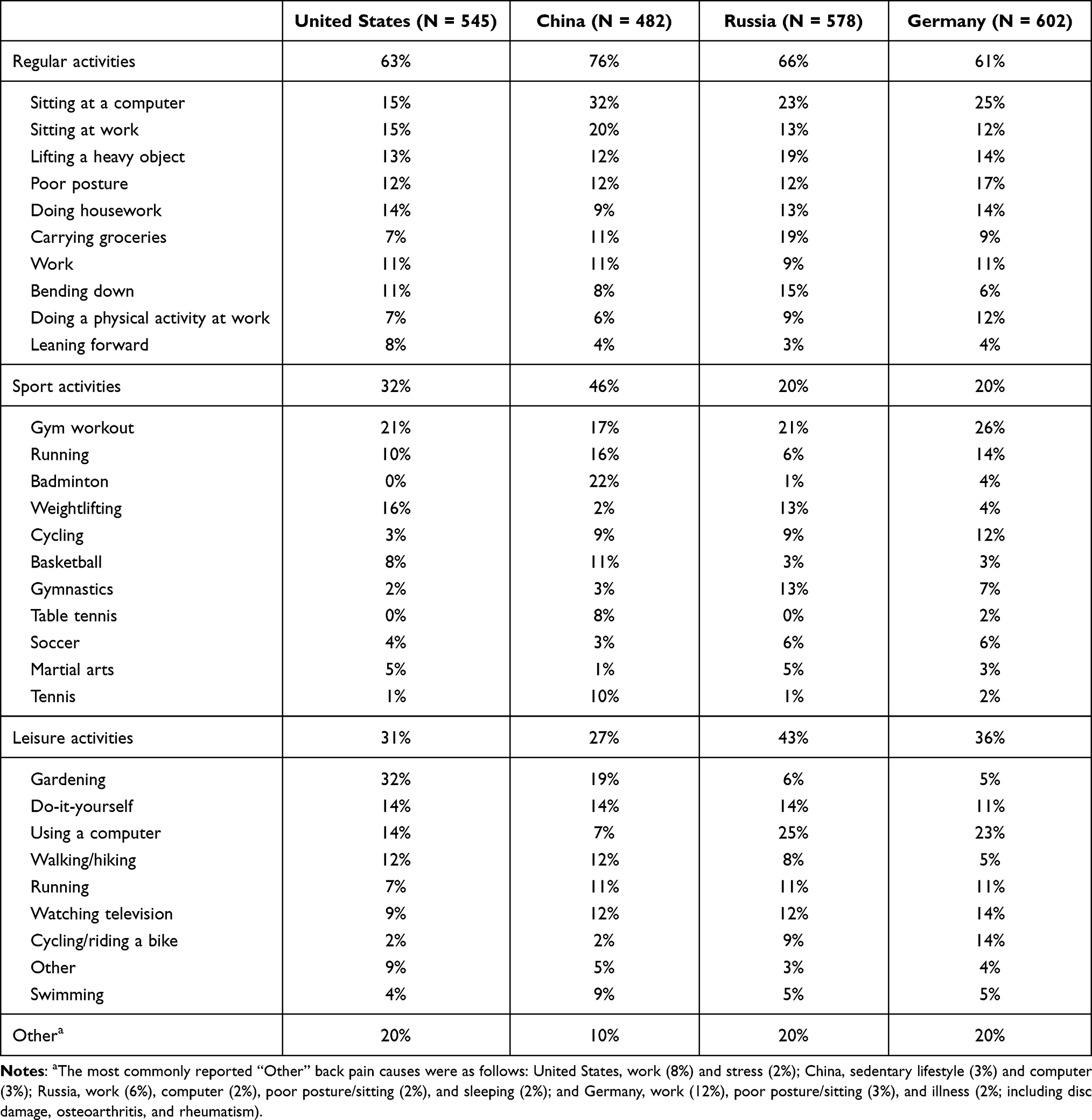 |
Table 1 Self-Reported Causes of Nonspecific Acute Back Pain Across Nationally Representative Population Samples |
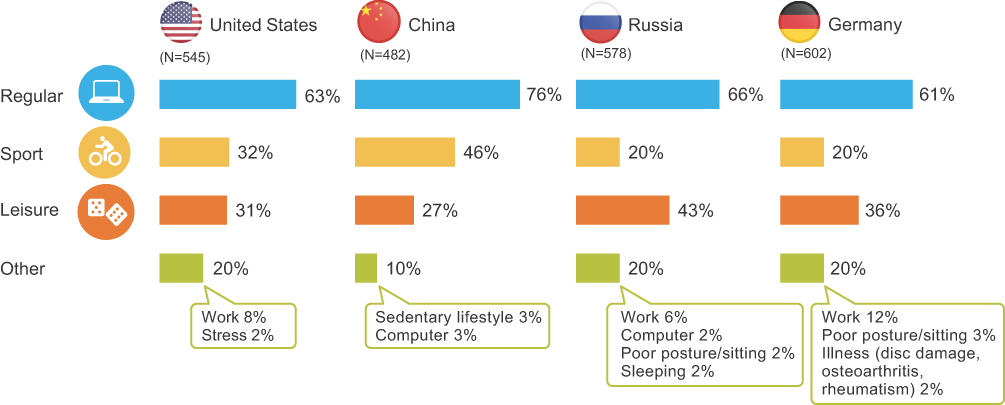 |
Figure 1 Most common causes of nonspecific acute back pain across 4 countries. |
Across all countries, most participants (85% to 86%) self-treat their acute back pain. Self-treatment with nonprescription (ie, over the counter) products was the most common method of treating acute back pain in the US (48%) and second most common in Russia (40%) and Germany (29%). In contrast, self-medication was infrequent in China (14%). Massage was the most common form of self-treatment in China (50%) and Russia (45%), and heat therapy was the most common self-treatment in Germany (36%). The most commonly used nonprescription products were oral painkillers in the US (87%), creams or gels in Russia (86%), and both oral painkillers (62%) and creams or gels (65%) in Germany. Overall, acute back pain sufferers were satisfied with the use of these analgesic products. The vast majority of users reported that they would definitely or probably use these products again (≥92% for oral painkillers and ≥88% for creams or gels).
More in-depth quantitative analyses of the survey results were used to develop sample profiles of acute back pain sufferers in each country based on gender, age, geographic region, employment status, occupation, household size, children in the household, ethnic background, type and intensity of acute back pain, likelihood of seeing an HCP versus self-treating, types of treatment used, type of HCP visited, and causes of lasting acute back pain. Detailed results of these analyses are provided in the Supplementary Material. Overall, these data provide a high-level overview of typical profiles of long-lasting acute back pain sufferers in each country (Figure 2).
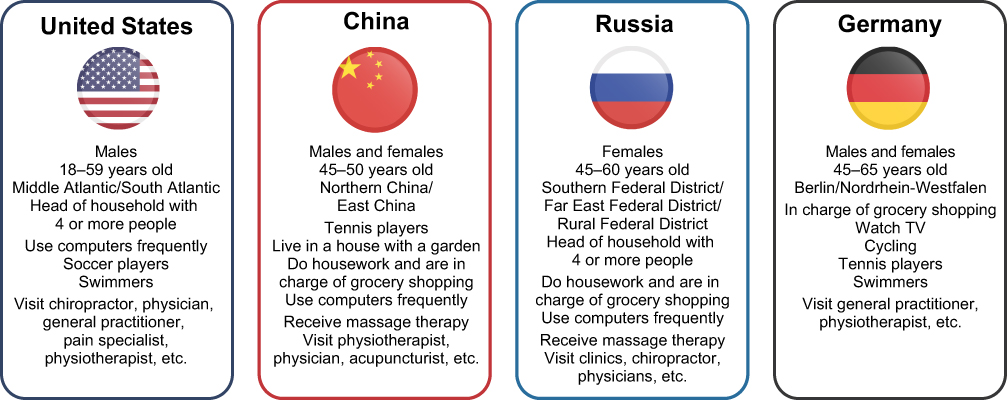 |
Figure 2 Characteristics of participants with acute long-lasting lower back pain across 4 countries. |
Step 2
Overall survey results in participants with long-lasting acute lower back pain across all 4 countries are summarized in Table 2. Among survey participants who engaged in key sport activities, onset of long-lasting acute lower back pain occurred between 30 and 33 years of age, and pain caused limitations in usual activities and reduced distances walked for 60% to 85% of acute lower back pain sufferers in all countries. For the most part, acute lower back pain started after, rather than during exercise, especially for respondents in China (93%). In all countries, onset of pain began within the first day of exercising for ≥75% of respondents, and most participants engaging in sports reported that rest alleviated their pain (≥76% of respondents). The types of treatments respondents reported using varied substantially by geography, but massage therapy was one of the most commonly used treatment in all countries (43% to 65%). In all countries, respondents were generally satisfied with the prescription and nonprescription treatments they used. For prescription treatments, the majority of participants engaging in sports indicated that they would use their preferred mode of treatment again (creams or gels [88% to 100%], muscle relaxants [91% to 100%], oral painkillers [83% to 97%], patches [86% to 96%], or injections [50% to 90%]). Similarly, most participants engaging in sports stated that they would use their preferred mode of nonprescription treatment again (creams or gels [90% to 97%], muscle relaxants [91% to 96%], oral painkillers [84% to 98%], or patches [87% to 96%]).
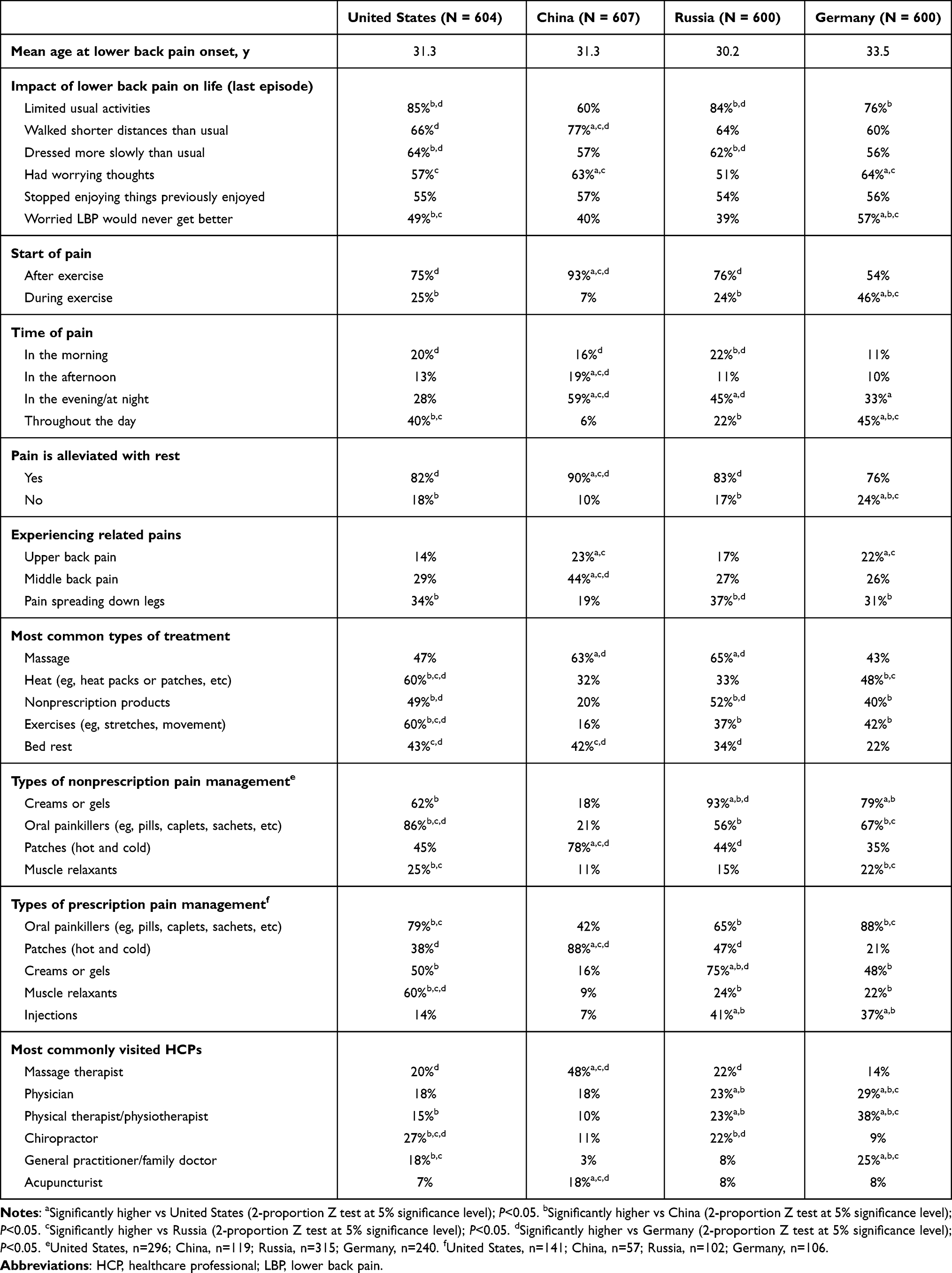 |
Table 2 Pain Profile and Treatment Characteristics of Participants with Acute Long-Lasting Lower Back Pain Engaging in Sports |
Key Results in Participants with Long-Lasting Acute Lower Back Pain in the US
The most common treatments reported in the US to treat long-lasting acute lower back pain were heat packs or patches (60%) and stretching exercises (60%). Respondents in the US preferred systemic oral prescription medications (79%) over any other prescription treatment modalities, but they were also amenable to using nonprescription topical therapies. They were generally more likely to use nonprescription topical gels or creams (62%) and systemic oral therapies (86%) to treat their long-lasting acute lower back pain than to use patches (45%) or muscle relaxants (25%). Respondents in the US who sought care from an HCP were most likely to consult chiropractors (27%), massage therapists (20%), physicians (ie, orthopedists, internists, rheumatologists; 18%), or general practitioners (18%) about their lower back pain (Table 2).
Overall, 85% of respondents in the US reported limiting their usual activities because of long-lasting acute lower back pain. Specific pain characteristics reported by respondents in the US when they engage in golf, gym workouts, and weightlifting are summarized in Table 3. Golfers had the highest proportion of individuals who always experience pain when practicing among the 3 sporting groups (32% vs 19% of gym-goers and 23% of weightlifters), and most golfers engage in their sport throughout the year (81%) and with one or more additional people (91%). Weightlifters had the highest proportion of individuals who reported experiencing significant pain among the 3 sporting groups (30% vs 27% of golfers and 17% of gym-goers), and most weightlifters exercise regularly throughout the year (88%) and at indoor facilities (96%). The proportions of gym-goers who always experienced pain while practicing and who experienced significant pain were the lowest among the 3 sporting groups although most exercised regularly throughout the year (92%). The most common equipment used by gym-goers included treadmills (52%), weight/resistance machines (52%), hand weights/dumbbells (48%), elliptical trainers (38%), and abdominal machines (36%). The most common activities for gym-goers included aerobics/step aerobics (28%), yoga (25%), circuit training (20%), and high-impact aerobics/body pump (16%). The most common causes of pain were attributed to wrong movements and repetitive movements among golfers (26% and 24%, respectively) and gym-goers (22% and 20%, respectively), and wrong posture and wrong movements among weightlifters (26% and 18%, respectively).
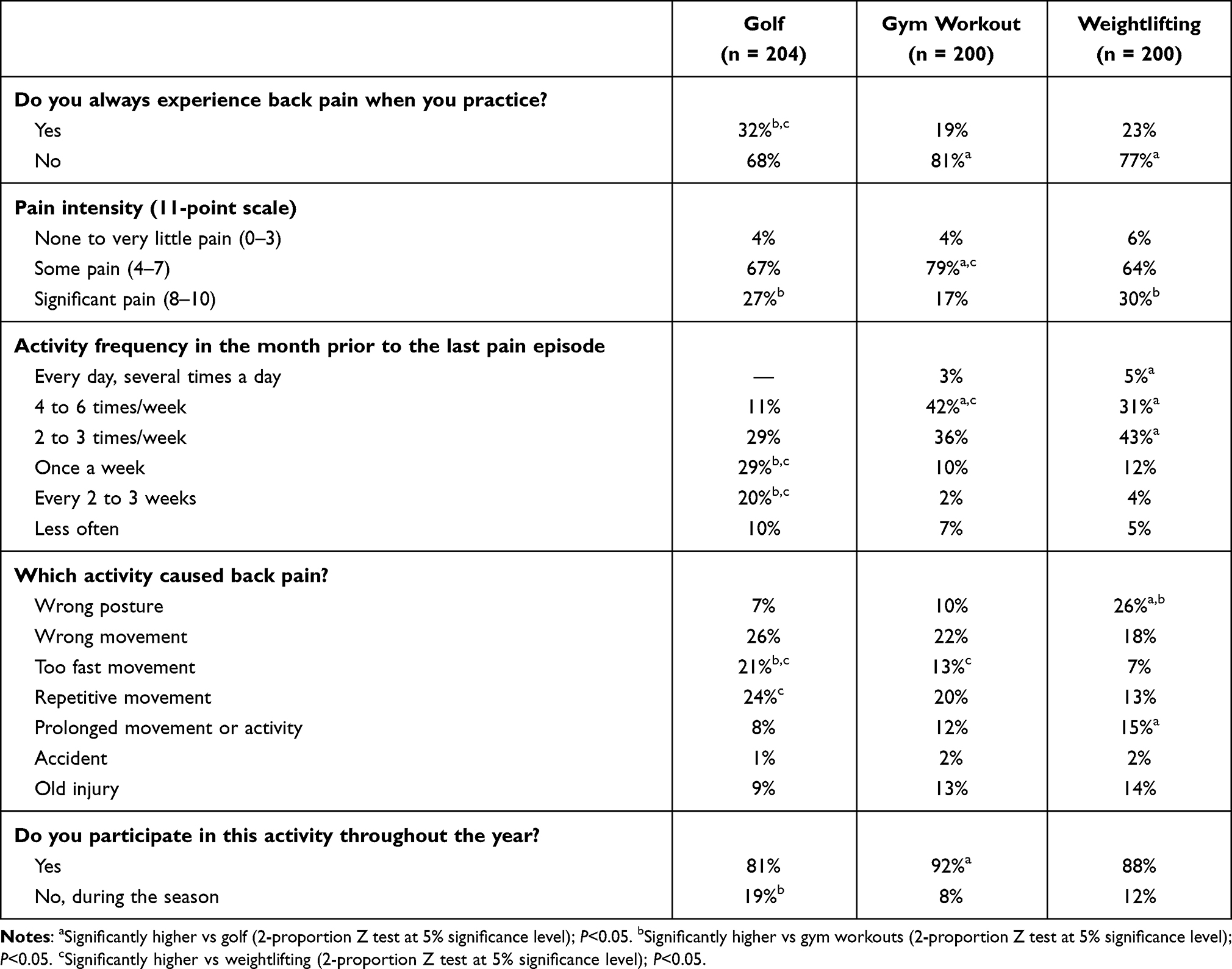 |
Table 3 Acute Lower Back Pain and Sports Activity Characteristics in the United States |
Key Results in Participants with Long-Lasting Acute Lower Back Pain in China
Long-lasting acute lower back pain sufferers in China showed a preference for traditional (nonmedical) treatments such as massage (63%), bed rest (42%), and acupuncture (14%) to manage their pain; if they reported using Western medicine, heat (32%) and cold patches (22%) were preferred (Table 2). Overall, 60% of respondents in China reported limiting their usual activities because of their lower back pain. Specific pain characteristics reported by back pain sufferers in China when engaging in badminton, basketball, and gym workouts are summarized in Table 4. More than two-thirds (69% to 73%) of respondents in China reported experiencing acute lower back pain each time they engage in their activity of choice. Gym-goers reported experiencing the most significant pain and generally exercising regularly throughout the whole year. The most common equipment used by gym-goers included treadmills (79%), abdominal machines (35%), and hand weights/dumbbells (34%). The most common activities for gym-goers included aerobics/step aerobics (41%), yoga (35%), circuit training (18%), and body boot camp (18%). Basketball players experienced acute lower back pain most often and throughout the whole year. For badminton players, movements made too quickly were the most common self-reported cause of acute lower back pain.
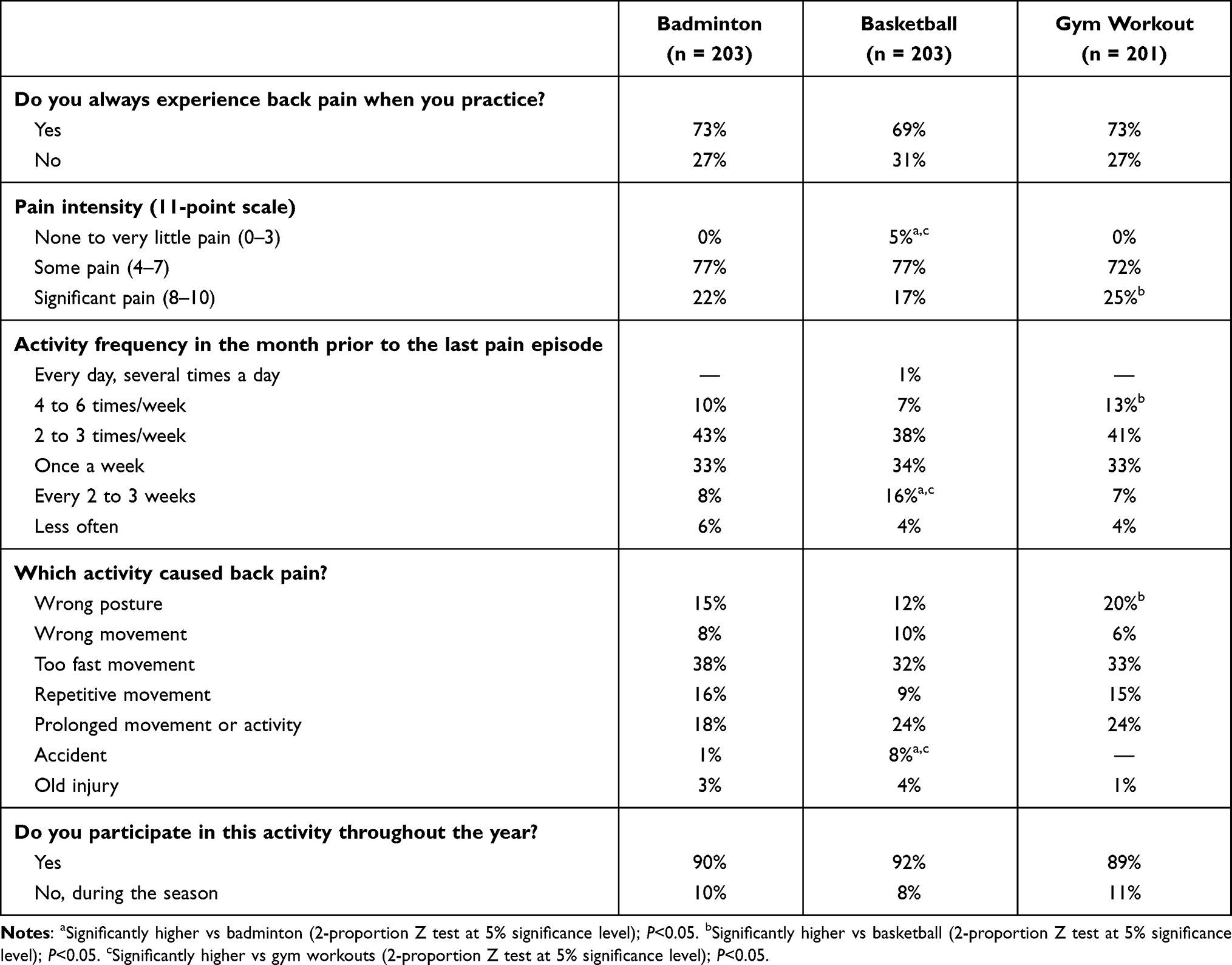 |
Table 4 Acute Lower Back Pain and Sports Activity Characteristics in China |
Key Results in Participants with Long-Lasting Acute Lower Back Pain in Russia
About a third of participants in Russia who suffer from long-lasting acute lower back pain also reported suffering from another form of back pain, with 1 in 4 citing pain spreading down the legs. Topical creams or gels were reported as the most commonly used type of nonprescription treatment, used by 93% of respondents in Russia. About half of participants also reported using systemic oral therapies (prescription, 65%; nonprescription, 56%) and hot or cold patches (prescription, 47%; nonprescription, 44%). Respondents in Russia showed a preference for seeking care from physical therapists (23%), physicians (23%), chiropractors (22%), or massage therapists (22%) to treat their lower back pain (Table 2).
Overall, 84% of respondents in Russia reported limiting their usual activities because of their lower back pain. Most reported that they do not experience lower back pain when they engage in the most common sport activities of gym workouts (82%), running (73%), and weightlifting (68%; Table 5). However, runners and weightlifters were significantly more likely to experience lower back pain than gym-goers. Weightlifters experienced pain the most often and had the most significant pain. Runners were the least likely to experience significant lower back pain; the most common self-reported causes of their pain were prolonged activity, wrong posture, and rapid movement. Gym workouts caused pain for about 1 in 4 participants, most often because of wrong movements and prolonged activity. The most common equipment used by gym-goers included weight/resistance machines (55%), abdominal machines (53%), treadmills (44%), and squat machines (42%). The most common activities for gym-goers included high-impact aerobics/body pump (34%) and circuit training (28%).
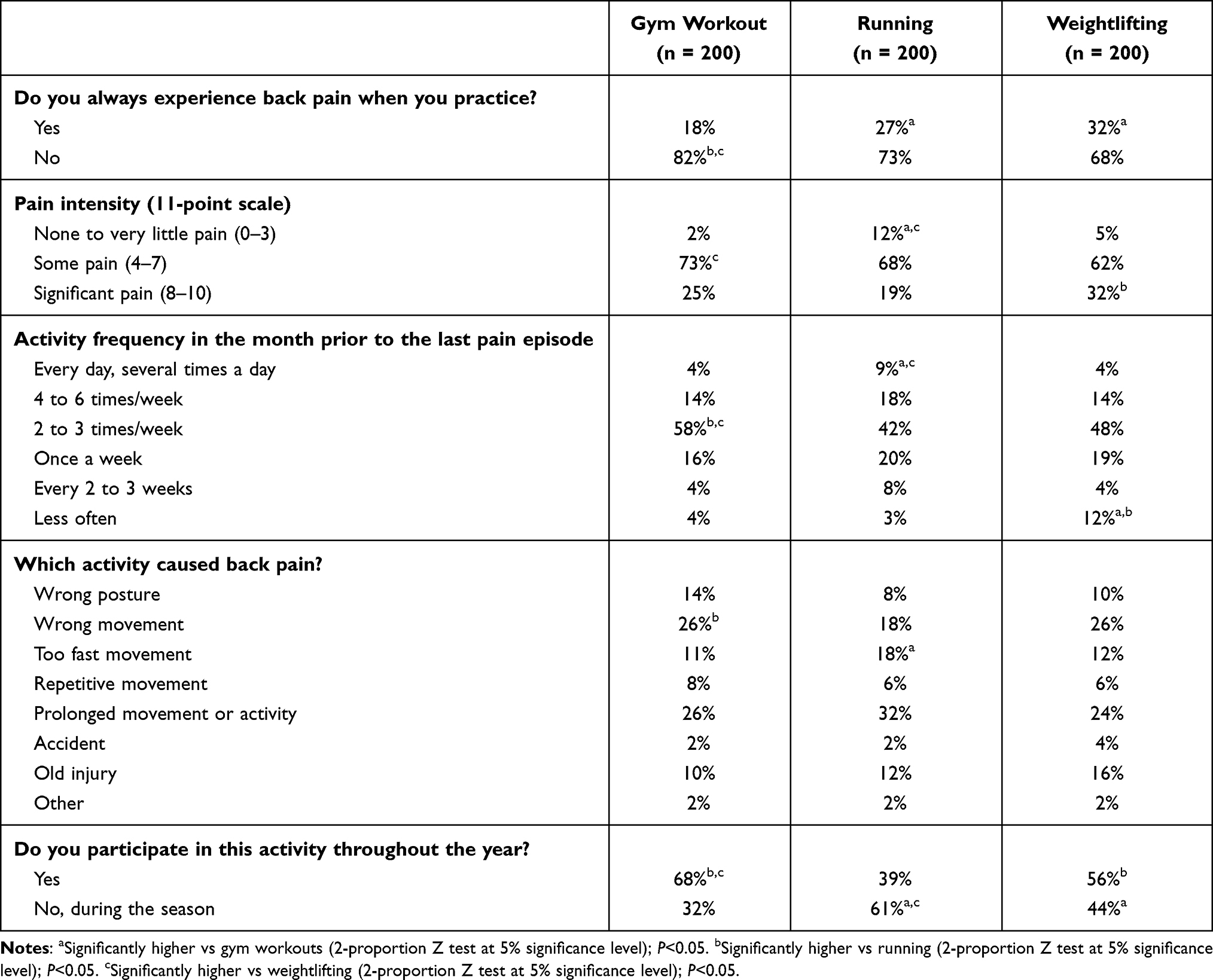 |
Table 5 Acute Lower Back Pain and Sports Activity Characteristics in Russia |
Key Results in Participants with Long-Lasting Acute Lower Back Pain in Germany
Long-lasting acute lower back pain sufferers in Germany reported treating their pain primarily using heat (48%) and massage therapy (43%), along with stretching and exercise (42%); their preferred nonprescription treatment was topical gels and creams (79%). Respondents in Germany who reported seeking care from an HCP were most likely to see a physiotherapist (38%), physician (29%), or general practitioner (25%; Table 2).
Overall, 76% of respondents in Germany reported limiting their usual activities because of their lower back pain. Approximately 4 out of 10 respondents in Germany reported experiencing lower back pain each time they practice their activity of choice (cycling, gym workouts, or running; Table 6). Runners experienced lower back pain most often and had the most significant pain, often caused by the wrong movement (27%) and prolonged activity (27%). Eight of 10 runners covered an average distance of ≤10 km per run, with nearly half running between 6 and 10 km. Cyclists experienced the least significant lower back pain; their pain was most often caused by incorrect posture (41%) and prolonged activity (22%). Cyclists typically used a road bike (50%) or a mountain bike (35%), and roughly 90% of cyclists in Germany usually cycled for less than 40 km on average, with the majority of cyclists covering a distance of 11 to 20 km. Gym-goers exercised the most regularly; 13% experienced significant lower back pain, most often caused by the wrong movement (48%). Gym-goers in Germany tended to participate in a variety of classes, most commonly circuit training (34%), as well as Zumba (16%), yoga (15%), spin/group cycling classes (14%), Pilates (14%), aerobics/step aerobics (13%), and high-impact aerobics/body pump (12%). Weight/resistance machines were the most popular type of workout equipment used (76%), followed by treadmills (55%), elliptical trainers (50%), hand weights/dumbbells (49%), and abdominal machines (49%).
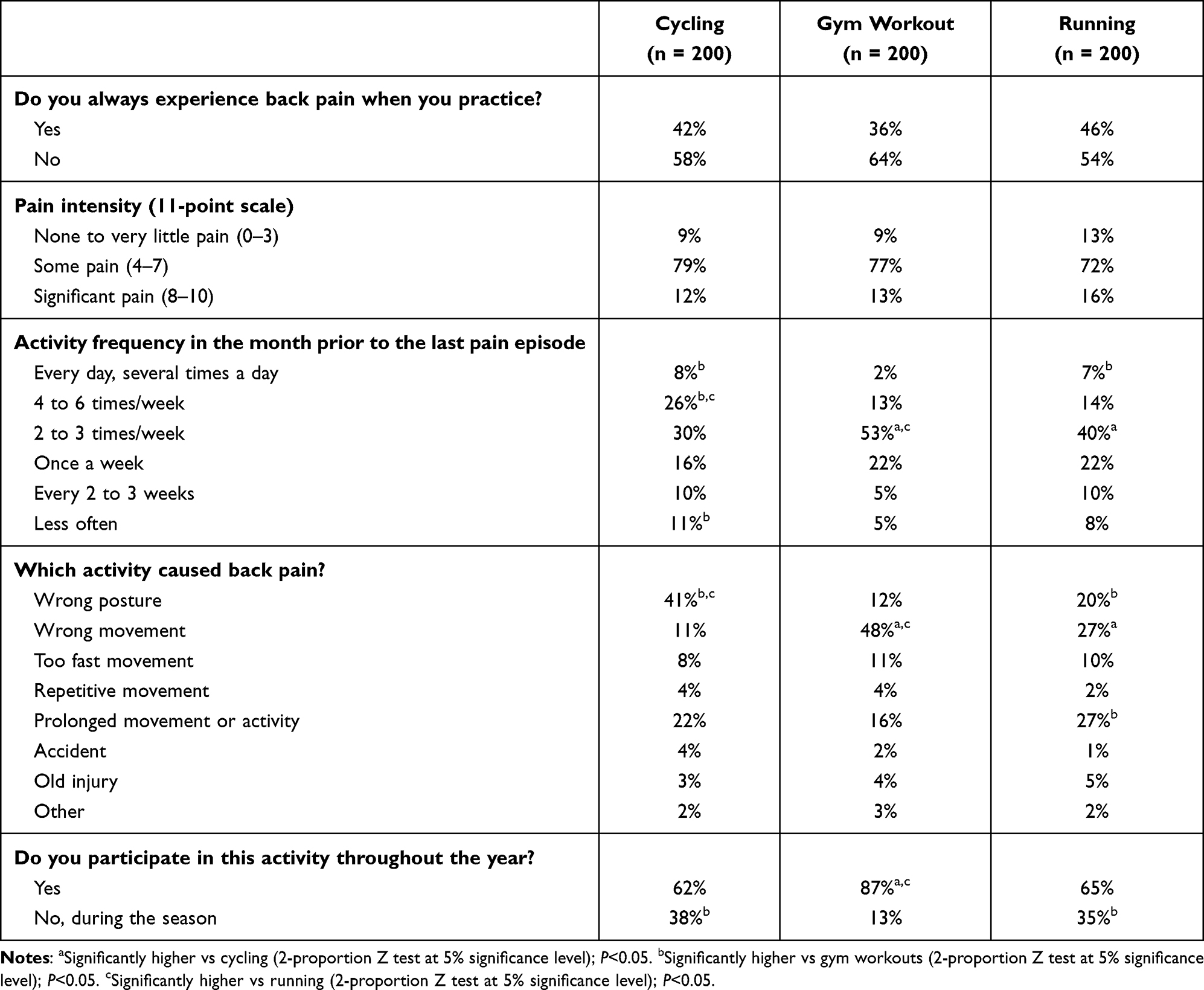 |
Table 6 Acute Lower Back Pain and Sports Activity Characteristics in Germany |
Discussion
In general populations around the world, the epidemiology of back pain has been well characterized; however, information is quite limited on the association between back pain and participation in sports activities.12 The current study investigated acute back pain epidemiology and treatment practices among individuals with acute long-lasting lower back pain engaging in sports in the US, China, Russia, and Germany in an effort to guide HCPs and potentially improve treatment outcomes.
While participants in all 4 countries reported that everyday activities, such as sitting at work, lifting heavy objects, poor posture, and doing housework, were the main causes of acute nonspecific back pain, sport and leisure activities were also commonly associated with acute nonspecific back pain. The prevalence of acute nonspecific back pain caused by sport and leisure activities varied across countries, ranging from 20% in Russia and Germany to 46% in China. Nonprescription (ie, over the counter) pain medications were the most common treatment for nonspecific acute back pain in the US, whereas massage therapy was the most common treatment in Russia and China and heat therapy was the most common treatment in Germany. The most commonly used nonprescription medications were oral painkillers in the US, creams or gels in Russia, and both oral painkillers and creams or gels in Germany.
Among long-lasting acute lower back pain sufferers, specific sporting activities most likely to precede or trigger acute lower back pain varied across countries. Gym workouts were associated with the highest incidence rates of acute lower back pain in all countries studied. Weightlifting was among the top 3 sports related to acute lower back pain in the US and Russia, and running was a leading trigger of acute lower back pain in Germany and Russia. Golf was a leading cause of acute lower back pain in the US, while badminton and basketball were among the top 3 sport-related causes of acute lower back pain in China, and cycling was a leading cause in Germany.
In-depth, country-specific profiling showed that sport-related acute lower back pain was significantly more likely to impact the usual activities of survey respondents in the US, Russia, and Germany compared with China. Respondents in China were significantly more likely to walk shorter distances because of acute lower back pain than respondents from the other countries. The most popular acute lower back pain treatment option was massage in China and Russia, while US respondents preferred heat therapy and stretching exercises; respondents in Germany preferred heat followed by massage, bed rest, and stretching exercises. The most popular nonprescription treatments for acute lower back pain were creams or gels in Russia and Germany, oral painkillers in the US, and hot or cold patches in China. The most popular prescription treatments were oral painkillers in the US and Germany, hot or cold patches in China, and creams or gels in Russia. These results may reflect the availability of different medications in each country. For example, some opioid analgesics are widely accessible in the US but are far less accessible in the other countries studied.15 Increased access to opioid analgesics in the US may be due to US pharmaceutical marketing and reimbursement practices, US health-care initiatives to increase pharmacologic treatment of pain, an abundant supply of opioid analgesics, and US patient perceptions of opioids as effective treatments.16
The methodology used in these surveys was specifically chosen to target individuals with acute lower back pain who engage in sporting activities. The Ipsos WebCruiser was utilized for prescreening participants using daily batches, allowing researchers to launch the main survey as soon as enough participants were identified. This methodology uses a syndicated approach based on the number of questions needed, not the incidence. While this methodology is robust and is commonly used to evaluate HCP and patient treatment behaviors, random screening may have been a better approach. However, a random screening approach would have been difficult, expensive, and time consuming to implement across 4 countries.
Additionally, these surveys used social science methods, which differ from formal epidemiologic methods, restricting the statistical comparisons that could be performed. Additionally, selection bias based on the locations from which survey participants were recruited cannot be ruled out. For example, some elderly individuals in China and Russia were unable to participate because they did not have access to a computer and/or the internet. Selection bias also may have been introduced because respondents were not screened from a general representative population. However, this bias was minimized by applying quotas on selected representative criteria that were collected during Step 1 (eg, the acute lower back pain sufferers investigated during Step 2 were identified and profiled during Step 1 based on a national representative sample). The risk of causality bias is considered to be low because participants were asked to self-report the causality of the activity(ies) associated with each pain episode by temporal association (ie, pain was absent before the activity and appeared during or after performing the activity). Participants also reported the effects of stopping or repeating the trigger activity on acute back pain (data not shown). Participant’s self-reported causality is consistent with prospective studies, in which up to 20% of all sports injuries involve an injury to the lower back, with repetitive or high-impact activities and weightlifting affecting the lower back and rotation of the torso affecting the lumbar and thoracic spine.17
In a recent series of articles by the Lancet Low Back Pain Working Group, leading back pain experts highlighted the need for worldwide health-care initiatives to improve recognition of the growing burden of lower back pain and develop more effective strategies for prevention, treatment, and self-management.1,2,18 Widespread misconceptions about back pain causes and prognoses exist in the general population and among HCPs, and many accepted “high-quality” models of care still recommend outdated, ineffective, or even harmful treatment strategies.2 Global or country-specific health-care initiatives could be used in conjunction with the World Health Organization European Region action plan for the prevention and control of noncommunicable diseases, which identifies the importance of comprehensive musculoskeletal health initiatives.2 A promising initiative in the US is the use of financial incentives and organization support for HCPs to reduce patients’ requirements for work disability. Strategies to improve implementation of guideline recommendations, clinical systems/pathways for lower back pain, compensation and disability policies, integration of health and occupational interventions, as well as to change public beliefs and behaviors related to pain management are underway in Australia, Canada, Sweden, the Netherlands, Denmark, and the United Kingdom.18
Conclusions
Across all 4 countries surveyed, everyday activities were the main self-reported causes of acute nonspecific back pain, followed by sport and leisure activities. The most common sporting activities identified as triggers of acute lower back pain among long-lasting acute lower back pain sufferers were gym workouts (all 4 countries), weightlifting (US and Russia), golf (US), badminton (China), and cycling (Germany). Results from these surveys may enable HCPs and other professionals (eg, sports trainers) to better understand lower back pain triggers, features, and patient/client treatment preferences. Furthermore, these findings may ignite interest in conducting research on the causes and characteristics of sports/activity-related back pain aimed to deepen our understanding of the causes and preventive measures for lower back pain. As such, public health initiatives could be undertaken to improve lower back pain education and prevention. Observed differences between participants across different countries in this study highlight the need to consider national and regional patient profiles when developing lower back pain prevention and treatment plans.
Abbreviations
HCP, health-care professional; US, United States.
Data Sharing Statement
The aggregated data that support the findings of this survey are available upon reasonable request from Haleon S.A. Requests must include a research proposal describing the objectives of research and its benefits for patients accompanied by a sufficient description of statistical and publication plans. Each request will be reviewed on an individual basis by Haleon to assess the ability of the proposal to meet the proposed scientific objectives and relevance to patient care.
Ethics Approval and Informed Consent
Ethics approval was not applicable because this was a survey, and respondents had no contact with any type of health-care professional or product at any time in the process of the research. All participants provided informed consent through Ipsos Terms & Conditions provided at the time of study conduct in 2016.
Acknowledgments
Data management and statistical analyses were performed by Ipsos and were funded by Haleon. Medical writing assistance was provided by Peloton Advantage, LLC, an OPEN Health company, Parsippany, NJ, and was funded by Haleon.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or all areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This survey study was funded by Haleon (formerly GSK Consumer Healthcare), Warren, NJ.
Disclosure
Nadine Maybaum is an employee of Haleon (formerly GSK Consumer Healthcare), Warren, NJ, USA. Salvador Rios-Martinez was an employee of GSK Consumer Healthcare (now known as Haleon) at the time the research was conducted. Martin Johnson was a consultant for GSK Consumer Healthcare (now known as Haleon) and has given lectures and participated in advisory boards for Grünenthal, Mundipharma, Flynn Pharma, and Pfizer. Dr Johnson also reports personal fees from Medical Services Ltd, personal fees from St Pancras Clinical Research, outside the submitted work; and British Pain Society Council Member. RCGP Co-Opted from 2010-2012, 2022 – onwards; Honorary Secretary of the BPS Council, Oct 2012–May 2016; Vice President to the BPS Council, May 2016–May 2018; also Royal College of General Practitioners Representative for Chronic Pain 2011 onwards; Member of Pain Parliamentary Campaign Group since 2022. The authors report no other conflicts of interest in this work.
References
1. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
2. Buchbinder R, van Tulder M, Oberg B, et al. Low back pain: a call for action. Lancet. 2018;391(10137):2384–2388. doi:10.1016/S0140-6736(18)30488-4
3. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. doi:10.1002/art.34347
4. Vos T, Abajobir AA, Abate KH, et al.Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
5. Raspe H, Matthis C, Croft P, O’Neill T. Variation in back pain between countries: the example of Britain and Germany. Spine. 2004;29(9):1017–1021; discussion 1021. doi:10.1097/00007632-200405010-00013
6. Ferreira ML, Machado G, Latimer J, Maher C, Ferreira PH, Smeets RJ. Factors defining care-seeking in low back pain – a meta-analysis of population based surveys. Eur J Pain. 2010;14(7):747.e741–747. doi:10.1016/j.ejpain.2009.11.005
7. Gallup-Palmer College of chiropractic annual report: Americans’ perceptions of chiropractic; 2016. Available from: https://www.palmer.edu/uploadedFiles/Pages/Alumni/gallup-report-palmer-college-2016.pdf.
8. Volinn E, Yang B, He J, Sheng X, Ying J, Zuo Y. Do outcomes of acupuncture for back pain differ according to varying sociocultural contexts? The view from China. J Altern Complement Med. 2013;19(5):435–444. doi:10.1089/acm.2010.0786
9. Steffens D, Ferreira ML, Latimer J, et al. What triggers an episode of acute low back pain? A case-crossover study. Arthritis Care Res. 2015;67(3):403–410. doi:10.1002/acr.22533
10. Della Mora LS, Perruccio AV, Badley EM, Rampersaud YR. Differences among primary care patients with different mechanical patterns of low back pain: a cross-sectional investigation. BMJ Open. 2016;6(12):e013060. doi:10.1136/bmjopen-2016-013060
11. Junqueira DR, Ferreira ML, Refshauge K, et al. Heritability and lifestyle factors in chronic low back pain: results of the Australian twin low back pain study (The AUTBACK study). Eur J Pain. 2014;18(10):1410–1418. doi:10.1002/ejp.506
12. Trompeter K, Fett D, Platen P. Prevalence of back pain in sports: a systematic review of the literature. Sports Med. 2017;47(6):1183–1207. doi:10.1007/s40279-016-0645-3
13. Kent ML, Tighe PJ, Belfer I, et al. The ACTTION-APS-AAPM Pain Taxonomy (AAAPT) multidimensional approach to classifying acute pain conditions. Pain Med. 2017;18(5):947–958. doi:10.1093/pm/pnx019
14. WebCruisers product guide; 2020. Available from: http://iap.ipsos-interactive.com/webcruisers/download/product_guide.pdf.
15. International Narcotics Control Board. Narcotic Drugs. Estimated World Requirements for 2017. Statistics for 2015. New York, NY: United Nations; 2017.
16. Rummans TA, Burton MC, Dawson NL. How good intentions contributed to bad outcomes: the opioid crisis. Mayo Clin Proc. 2018;93(3):344–350. doi:10.1016/j.mayocp.2017.12.020
17. Zemková E, Kováčiková Z, Zapletalová L. Is there a relationship between workload and occurrence of back pain and back injuries in athletes? Front Physiol. 2020;11:894. doi:10.3389/fphys.2020.00894
18. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. doi:10.1016/S0140-6736(18)30489-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.