Back to Journals » Patient Related Outcome Measures » Volume 14
Qualitative Exploration in Exit Interviews of Changes Observed in Clinical Trials for Individuals with Autism Spectrum Disorder Without Intellectual Disability
Authors Chladek M ![]() , Burbridge C, Gibbons E, Willgoss T, Smith J, Clinch S
, Burbridge C, Gibbons E, Willgoss T, Smith J, Clinch S ![]()
Received 21 January 2023
Accepted for publication 26 October 2023
Published 21 November 2023 Volume 2023:14 Pages 313—335
DOI https://doi.org/10.2147/PROM.S385682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Michael Chladek,1 Claire Burbridge,2 Elizabeth Gibbons,2 Tom Willgoss,3 Janice Smith,4 Susanne Clinch3
1Clinical Outcome Assessments, Clinical Outcomes Solutions LLC, Chicago, IL, USA; 2Clinical Outcome Assessments, Clinical Outcomes Solutions Ltd, Folkestone, Kent, UK; 3Patient Centered Outcomes Research, Roche Products Ltd, Welwyn Garden City, Hertfordshire, UK; 4Global Development, Roche Products Ltd, Welwyn Garden City, Hertfordshire, UK
Correspondence: Susanne Clinch, Patient Centered Outcomes Research, Roche Products Ltd, 6 Falcon Way, Shire Park, Welwyn Garden City, AL71TW, UK, Email [email protected]
Purpose: To explore, from the perspective of Study Partners (SPs; eg, caregivers) of clinical trial participants with autism spectrum disorder (ASD), any changes experienced in socialization and communication over the clinical trial, how these changes manifested, and the impact these changes had on the autistic individual, the SP, and family. This helps interpret whether changes in trial outcomes were meaningful.
Patients and Methods: Interviews were conducted with the SPs of individuals with ASD, without intellectual disability, from 2 clinical trials: 86 children (aged 5– 12 years) or adolescents (aged 13– 17 years) who took part in the aV1ation trial (83.7% male), and 41 adults (aged 18+ years) who took part in the V1aduct trial (80.5% male). The primary endpoint for both trials was change from baseline in the VinelandTM-II two-domain composite, consisting of the mean of the Socialization and Communication domains. In these interviews the participants verbally indicated level of change for each of these key domains on 7-point change scales.
Results: Improvements in the Socialization domain enabled greater awareness of the feelings of others and allowed for stronger empathy and kindness. Improvements in the Communication domain allowed for the autistic individual to be better at listening and better at self-expression. Together, changes in these two domains, which were considered most important, allowed for richer, deeper relationships. Study Partners noted that improvements in these domains allowed for better integration within the family unit, decreased stress, and increased optimism about the autistic individual’s future.
Conclusions: The impacts of changes in either domain were synergistic, combining together to create positive experiences which in turn led to further positive impacts in other skills. These qualitative insights provide context to the changes that were observed during the clinical trial and captured using the VinelandTM-II, illustrating the meaning of these changes to the individuals with ASD without intellectual disability and their families, and the impact that they have on people’s everyday lives and overall health-related quality of life.
Keywords: Autism, VinelandTM-II, ASD, socialization, communication, meaningful change, qualitative, interview
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that often appears early on in childhood; it is characterized by difficulties in the core areas of social interaction and communication difficulties, as well as possible repetitive sensory-motor behaviors.1–3 Although ASD is heterogeneous and there is much variation among individuals, those with ASD may struggle with eye contact and following typical social conventions or the natural rhythm of conversations, or they may exhibit repetitive behaviors and have unusual or overly focused interests, among other experiences.4 Globally, the prevalence of ASD is between 1–2%; the US experiences a prevalence at the higher end of this range due to more accurate ASD diagnosis and treatment networks.5–7
Individuals with ASD have demonstrated significant impairments in social cognition8 (the ability to recognize and respond appropriately to social stimuli) and adaptive skills9 (the skills required to adapt in daily life), which are related to functional outcomes. Research in children and adolescents with ASD has shown that more severe ASD symptomatology is associated with poorer adaptive functioning.10 Other research has found the strongest predictor of adaptive functioning in children with ASD to be IQ, although the gap between IQ and adaptive skills was greater for those who were higher functioning and older children.9 Another recent study in children and adolescents with high functioning ASD showed that specific aspects of IQ are impacted. The high functioning ASD group had higher total IQ (and intelligence domains of verbal communication and perceptual reasoning) compared to neurotypical controls and 2 other groups with neurodevelopmental disorders (Specific Learning Disorders [SLD], and Attention Deficit/Hyperactivity Disorder [ADHD]),11 but lower working memory and processing speed compared to the neurotypical group. The high functioning ASD group also showed significant behavioral and emotional problems and greater parental distress compared to the neurotypical group.12
Difficulties can also vary by age. Children with ASD can have difficulty with social interactions, using language to communicate, or engaging in symbolic or imaginative play.13 A recent study of children with ASD found that younger children displayed more severe symptoms of ASD and that older children had better communication skills.10 As individuals with ASD enter adulthood, these symptoms can persist and change as individuals enter new life stages, often without the support services provided in schools when they were younger.14 While some adults who have ASD can live independently, others can require life-long support from family or caregivers. Adults with ASD can be significantly disadvantaged regarding employment, social relationships, physical and mental health, and health-related quality of life (HRQOL).15 Specifically, HRQOL tends to be pervasively lower for adults with ASD, and notably lower in domains capturing social relationships and social integration, when compared to neurotypical groups.16 There is also an interaction between symptoms in ASD as some, such as sleep disturbance, can independently affect cognition and learning.17
In addition to the difficulties faced by individuals with ASD, caregivers and family members may also experience impacts on their own HRQOL, such as increased stress.18 In one recent study of parents of adolescent and adult children with ASD, 40% reported having symptoms of clinical depression and reported a significantly lower quality of life compared to the normative average US population.19 In another study, 84% of primary and secondary caregivers reported experiencing problems in their relationship with their autistic child.20 When investigating the factors associated with impacts on parents and caregivers of adolescents and young adults with ASD and intellectual disability (ID), ASD severity, externalizing behaviors, medical comorbidity, and parent age were most predictive of the level of HRQOL.
A range of non-drug interventions, such as behavioral and occupational therapy, are the current standard of care for the core symptoms of ASD.21 Although the Food and Drug Administration (FDA) has approved the atypical antipsychotics risperidone and aripiprazole for irritability associated with ASD, thus far, no medication has proved effective for the socialization and communication difficulties of ASD.22 The European Medicines Agency has not approved any medications, even for irritability, in ASD. A recent public workshop held by the FDA on patients’ perspective on treatments for ASD stressed the need for drug interventions that would improve patients’ daily quality of life (QOL).23 To support the development of effective therapies focusing on the core difficulties of ASD, there is a need for a better understanding of what improvements and QOL impacts in the areas of socialization and communication look like and mean for individuals with ASD and their caregivers. The FDA is increasingly asking for qualitative data to contextualize and help interpret meaningful change on clinical trial endpoints.16
Recently, two multicenter, randomized, double-blind, 24-week, 2-arm, parallel group, placebo-controlled clinical trials were conducted to evaluate the efficacy and safety of balovaptan compared with placebo. One trial enrolled children and adolescents 5 to 17 years of age with ASD (Phase 2; NCT02901431; aV1ation)24 and the other trial enrolled adults with ASD (Phase 3; NCT03504917; V1aduct). In both trials, individuals with ASD had no ID (IQ≥70). While neither trial met their primary endpoint, a substantial placebo response was observed and the qualitative data from these exit interviews are helpful in understanding what kinds of changes in socialization and communication are important and how they impact people’s daily lives.
The primary efficacy endpoint in these trials was change from baseline on the Vineland™ Adaptive Behavior Scales, 2nd Edition (VinelandTM-II) two-domain composite score (VABS-2DC) – which consists of a semi-structured interview between an ASD clinician/therapist and a caregiver of the autistic individual, described here as a Study Partner (SP). The VinelandTM-II consists of 3 primary domains: Socialization, Communication, and Daily Living Skills. While it also assesses Maladaptive Behaviors and Motor Skills, these were not assessed as part of these studies. The VABS-2DC consists of the mean of the Socialization (VABS-S) and Communication (VABS-C) domains. These two domains assess the core symptoms of ASD. The VABS was chosen as an endpoint because it is the most common measure of adaptive behavior used in ASD.25 It was the measure used to evaluate adaptive functioning in the literature cited above,9,10,12 on the difficulties faced in ASD.
While work has been conducted to better understand the minimal clinically important differences on the VABS,25 there is little literature on what a change on the VABS means qualitatively for individuals with ASD and their families. Exit interviews provide an opportunity to explore any changes clinical trial participants (and their families) have observed over the course of the clinical trial and what impact those changes have had on their daily lives and HRQOL.
Aims/Objectives
The overall aim of the exit interviews during the aV1ation and V1aduct trials was to explore, from the SPs’ view, the changes experienced by individuals with ASD (without ID) over the course of the clinical trial. The focus of these changes was within the three domains of the VABS, and the meaningfulness of those changes. Although all three domains of the VABS were discussed with SPs, this manuscript will center on the changes and impacts associated with Socialization and Communication because they are core difficulties faced within ASD that make up the primary endpoint, the VABS-2DC. These changes and impacts were explored for three cohorts: children (aged 5–12 years), adolescents (aged 13–17 years), and adults (aged ≥18 years).
An additional aim of the exit interviews was to inform the interpretation of changes observed during the clinical trial on the VABS and, thus, to contextualize any perceived benefit of balovaptan with qualitative data. Exit interviews also aimed to explore the impact of changes, not only on the individuals with ASD (without ID), but also on their families or others close to them.
Methods
Recruitment for the interviews were conducted across sites in the USA (for aV1ation) as well as Canada, Spain and the UK (for V1aduct). As eligibility was determined at the point of enrollment into the clinical trials, no further inclusion or exclusion criteria were applied for the interviews beyond the SP having accompanied the trial participant to a majority of clinic visits (and therefore completed the VABS), completion of the Week 24 visit, and willingness to take part in the exit interview. A key criterion for inclusion in the clinical trials was that the individual with ASD have an IQ of ≥70.
Exit interviews were conducted by trained qualitative researchers as close as possible after the End of Trial visit (ie, Week 24), but within 4 weeks of completion of the End of Trial visit in the aV1ation and V1aduct trials. They were semi-structured and were conducted over the telephone with SPs, who were defined as individuals who accompanied the trial participant throughout the clinical trial and who were often the parent or guardian of the autistic individual. SPs were interviewed rather than trial participants themselves because of the age of the participants in aV1ation, because SPs were the primary observer whom clinicians interviewed for the VABS during the clinical trial, and because SPs were able to accurately reflect on the main observable concepts of socialization, communication, and daily living skills. Only one interview was conducted with each SP who consented to take part in the optional exit interviews.
In addition to the in-depth qualitative exploration of changes, SPs were asked to rank the 3 domains of communication, socialization and daily living skills in order of importance from 1 “most important” to 3 “least important” out of the 3. For analysis, the scores were reversed and summed so that higher scores for ranking indicated an overall higher rating of importance. Also, after discussing any changes noticed in each domain of the VABS, SPs were asked (during the interview) to rate their perceptions of the level of any change in that domain they had observed in the trial participant since the start of the clinical trial using a 7-point scale that was reflective of ratings of change used in the clinical trials (very much worse, much worse, minimally worse, no change, minimally improved, much improved, very much improved). If they indicated an improvement or worsening, they were also asked to indicate “yes” or “no” whether they considered this change to be meaningful. Study partners who reported “no change” were not asked if this was meaningful as the exit interviews focused on changes observed and the meaningfulness of these changes. These SP perceptions of meaningful change (SPPMC) ratings were obtained within the interviews for each VABS domain and for overall ASD. In interviews with SPs of adults in the V1aduct trial, SPPMC was also obtained for HRQOL. The response scale for the SPPMC items reflected those used in the Clinical Global Impression of Improvement (CGI-I) published by Busner and Targum in 2007 without the clinician focused descriptors to each response (eg, the response simply stated “very much improved” without any additional text) to be suitable for a non-clinical respondent, to avoid biasing the individual’s own interpretation of what this would mean, and to mirror the patient/caregiver impression of change items used within the clinical trials.26–28 These were thus based on validated change scales, though no validation was conducted specifically of the questions that were asked in the interviews.
The SPPMC was used to provide an additional quantitative indicator of magnitude of change. Quantitative data and SPPMC ratings were additionally used, alongside clinical trial anchors, in a mixed methods analysis to interpret and contextualize the estimation of meaningful change thresholds (MCTs) on the VABS-2DC. Such MCTs are reported separately,19 while the current paper focuses on the qualitative data analyzed for the 2 trials, describing if and how aspects of the individuals’ ASD changed throughout the trials.
All interviews were audio-recorded, transcribed, coded, and analyzed using NVivo v12.0. Quotes by SPs were given identification markers indicating the sex and age of the autistic individual for whom the SP was a study partner. For example, “SP/IwASD: M, 9” indicates a quotation from an SP about observations of a 9-year-old male individual with ASD (IwASD). Both SPs and interviewers were blinded to treatment allocation.
Thematic analysis of the qualitative data was conducted to identify what changes SPs had observed in clinical trial participants, the impact these changes had on daily life, and the importance of any changes experienced.29 Concepts were broadly analyzed within the domain/subdomain structure of the VABS. The qualitative data relating to the child and adolescent population from the aV1ation trial and the qualitative data from the adult population of the V1aduct trial were analyzed separately so that key themes of types of changes and their impacts were identified separately between the child/adolescent cohorts and the adult cohort. However, in this paper, findings are presented by domain for all groups together, with key differences across the cohorts discussed as relevant.
Results
Exit Interview Populations
Details of the exit interview and clinical trial populations are given in Table 1 and described below for both trials.
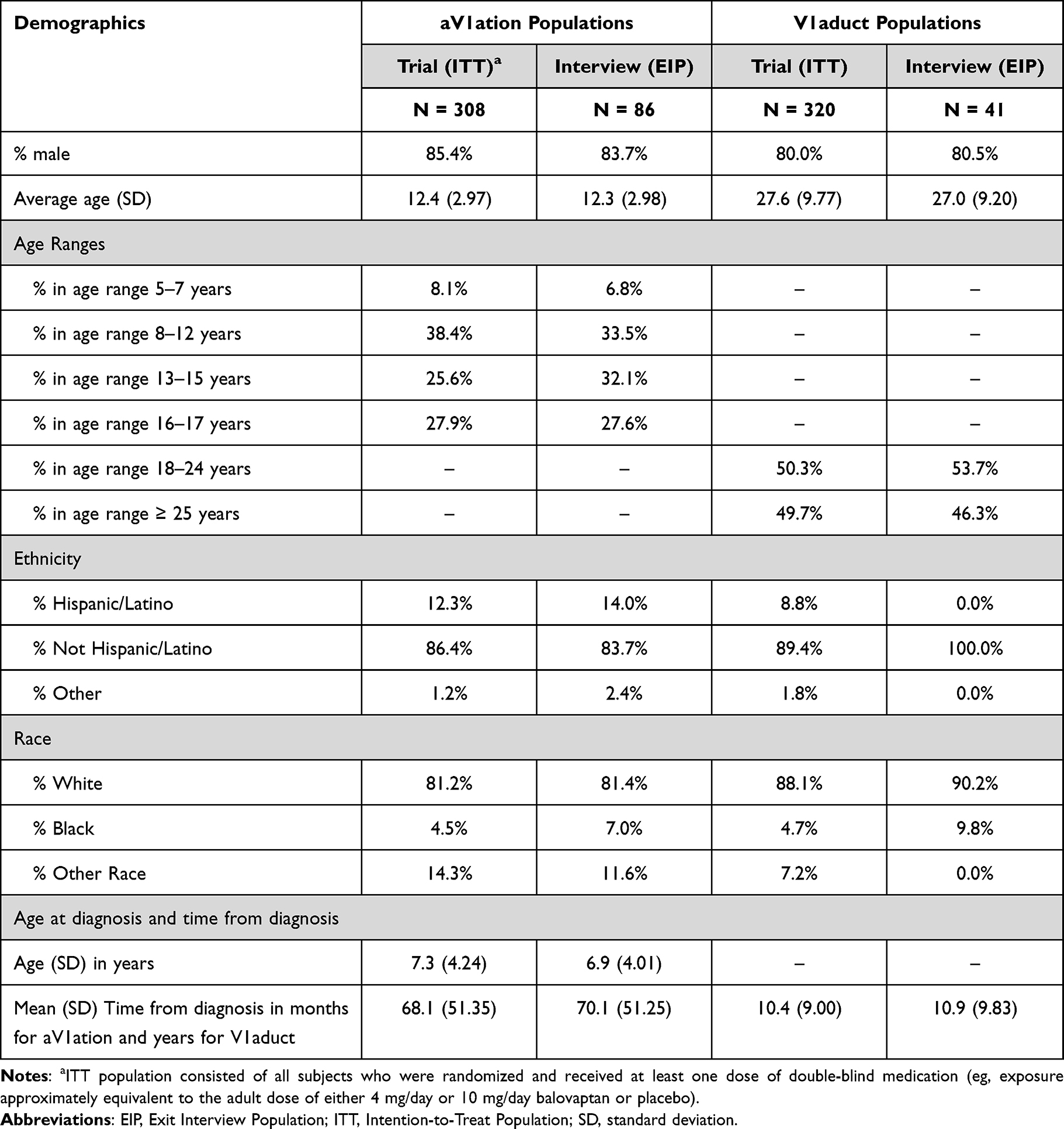 |
Table 1 Clinical Trial and Exit Interview Population Demographics |
aV1ation (Children and Adolescents)
Interviews were conducted with the SPs of 86 individuals with autism who took part in aV1ation (83.7% male, reflecting the predominance of ASD diagnosis in males and reflective of the proportion in the clinical trial). This Exit Interview Population (EIP) for aV1ation included 40 in the Child Cohort (aged 5–12 years), which had an average age of 9.6 years (SD=1.82) and 46 in the Adolescent Cohort (aged 13–17 years), which had an average age of 14.7 years (SD=1.32). The average age of individuals with autism in the total aV1ation EIP was 12.3 years (SD=2.98). Ethnicity, race, and time since diagnosis were all also highly reflective of the clinical trial population. Demographically, the EIP of aV1ation overall was similar to the larger intention-to-treat (ITT) population of the trial. See Table 1.
V1aduct (Adults)
Interviews were conducted with the SPs of 41 individuals with autism who took part in V1aduct (80.5% male; again reflecting the predominance of ASD diagnosis and proportion in the clinical trial). The age range within this EIP ranged from 18 to 51 years with an average of 27.0 years (SD = 9.20 years), and a split of approximately 50:50 between those aged 18 to 24 years of age and those aged 25 and over, reflecting the clinical trial population. Race and ethnicity within the EIP also reflected the major groups within the clinical trial, although not all groups in the trial were captured in the EIP. Average time since diagnosis was comparable with the clinical trial population. Demographically, the EIP of V1aduct overall was similar to the larger ITT population of the trial. See Table 1.
Importance of VinelandTM-II Domains
When SPs were asked in interviews to rank the three VinelandTM-II domains in order of importance, Socialization and Communication were the two most important domains to SPs across all age cohorts. Communication was rated as slightly more important than Socialization by SPs of children, though they were of almost equal importance; and for both adolescent and adult cohorts, SPs ranked Socialization as slightly more important than Communication. See Figure 1.
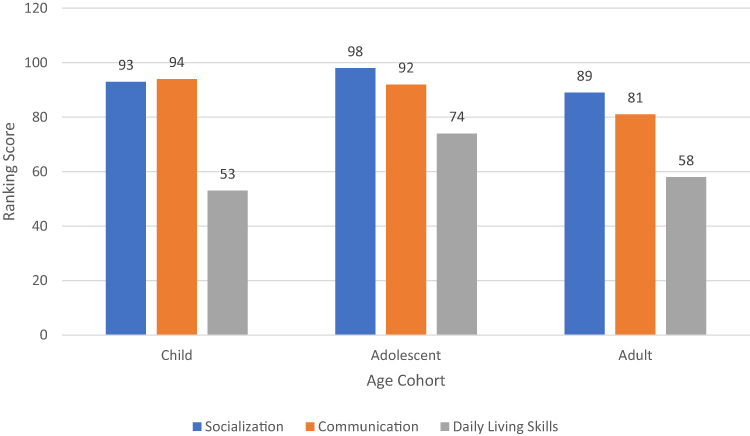 |
Figure 1 Rank of VABS-II domains in order of importance. |
Because SPs highlighted changes in the Socialization and Communication domains were the most important, and because they make up the VABS-2DC score, only these two domains are discussed in detail in the subsequent sections.
Socialization Skills
What Changes Were Experienced in Socialization During the Clinical Trial?
To understand any changes in Socialization, SPs were asked to describe in detail any changes they noticed since starting the clinical trial in how the autistic individual interacted with others in interpersonal relationships, used their play and/or leisure/free time, and coped or adapted to different social situations (ie, the 3 subdomains of the VABS-S domain).
The majority of SPs for children and adolescents and about half of SPs for adults reported experiencing improvements in Socialization during the clinical trial (31/40 for the child cohort, 34/46 for adolescents, and 21/41 for adults), which included improvements across all 3 subdomains of Socialization. The remaining SPs reported no change except for two participants who reported a worsening (1 in each of the adolescent and adult cohorts), and 3 for whom their rating of change on the SPPMC was missing (1 adolescent and 2 adults). See Figure 2.
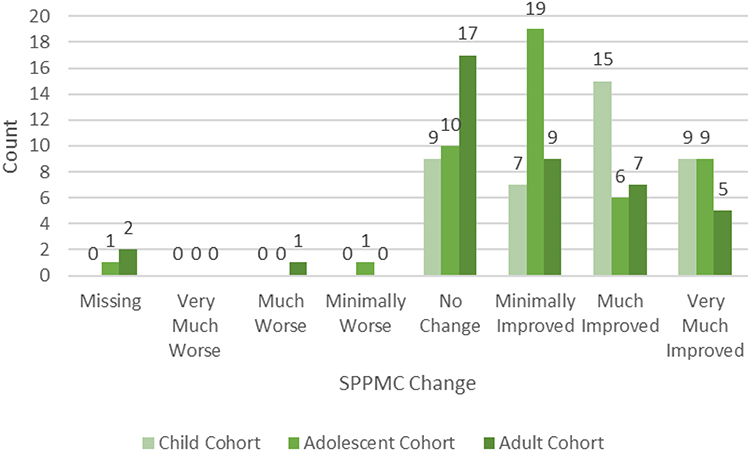 |
Figure 2 SPPMC changes in socialization. Abbreviation: SPPMC, Study Partners Perception of Meaningful Change. |
Across all three cohorts, the improvements in Socialization that were described by SPs reported allowed the autistic individual to have a greater awareness of the feelings of others, made them more empathetic and kinder, as well as being more open to different situations and engaging in interactions with others. These improvements were wide-ranging and noticeable within many types of social interactions, however, the precise interactions in which these benefits were observed often depended upon the age of the autistic individual. Importantly, all changes were mentioned spontaneously. See Table 2 for key themes of types of changes noticed by SPs.
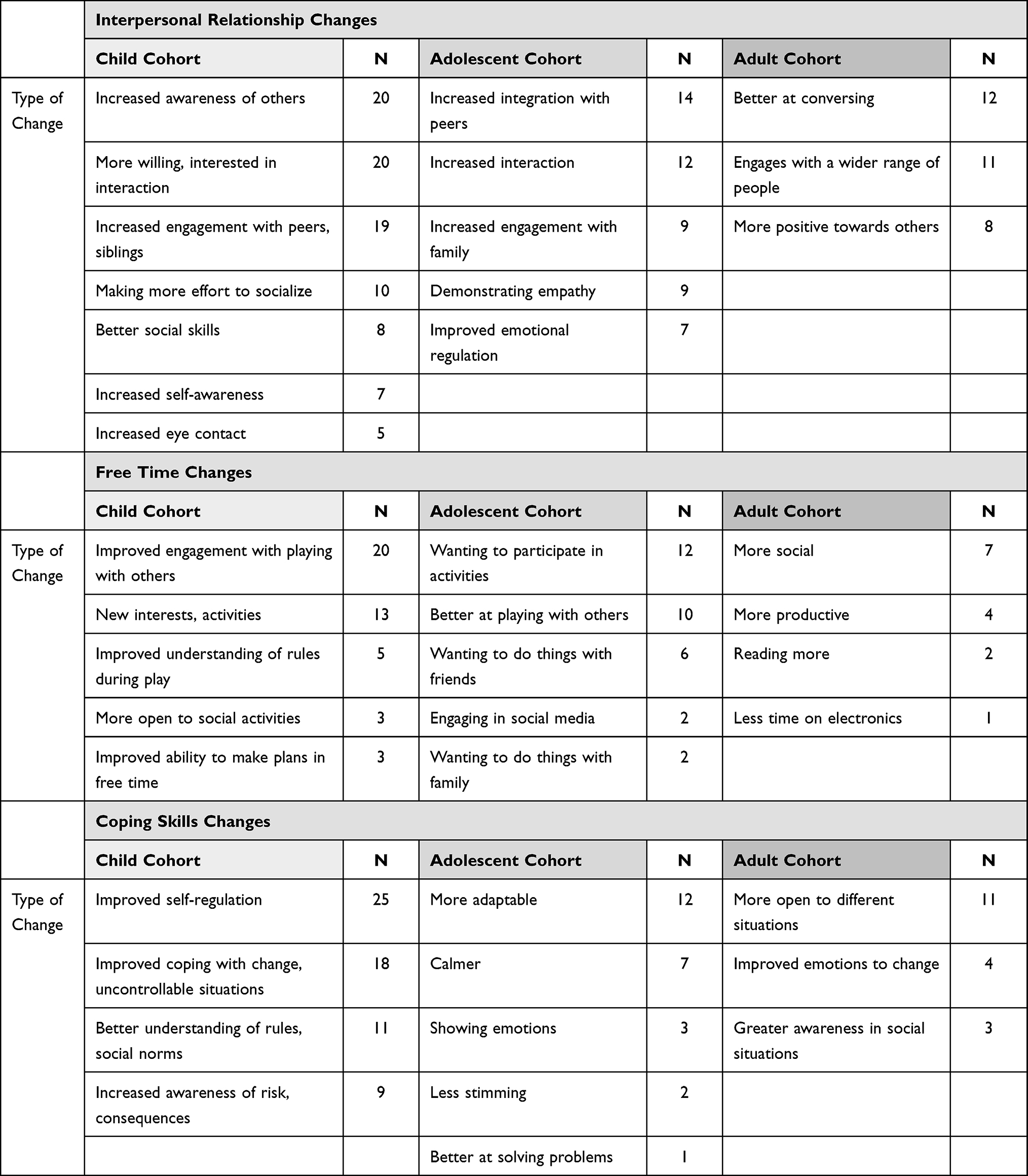 |
Table 2 Socialization Changes by VABS-S Subdomain |
Changes Observed in Interpersonal Relationships
When discussing interpersonal relationships, changes discussed by SPs focused on improving social skills, an increased willingness to engage, and more positive experiences in interpersonal relationships. While these broad changes were common across all cohorts, the exact nature of how these were observed or experienced reflected the typical life stage of the cohort.
In children, changes were noticed in aspects of development that are fundamental interpersonal skills, such as increased awareness of self and others as well as increased eye contact. For children, interpersonal skills often manifested as better conversational abilities. One SP noted,
He’s trying to be able to hold a conversation and find things that could be a commonality for conversation. He’s thought out better choices in friends at school, whether it’s at playtime or at lunch. He’s making an effort every day to go outside to play with a friend instead of shutting himself up in his room, and he’s been working hard, like I said, just getting along better with children in his own age group. [SP/IwASD: M, 10]
Children also displayed an awareness of others and their feelings,
I have seen an improvement. I’ve seen more of an awareness, I guess, he’s more aware of how other people think or feel and more sensitive to that. He used to just not be emotional, not really care if people were upset. He would say things like, ‘Well, I don’t really care about that.’ Now, he’s much more sensitive to when people are upset or when they’re sad, or when they’re hurting or angry. He seems to be able to distinguish those emotions better and able to empathize as well. [SP/IwASD: M, 9]
In adolescents, these changes in interpersonal relationships manifested as more positive feelings towards others and expanding their social circles. One SP noted,
Her interaction with her peers just really seemed to increase. It’s like she’s been more sociable with going up and talking to them on their, on her own without-without me, without mom or dad around or whatever. [SP/IwASD: F, 17]
Additionally, SPs reported that adolescents were engaged and sought out the company of others: “I noticed that after a couple of months, he was coming more out of his room, and actually he was like, Okay, what, family, what movie are we gonna watch?” Or, “Are we gonna go out and eat something”, or, “Are we gonna do something?” He was being more social about it.” [SP/IwASD: M, 15].
All reported the autistic individual being more willing to engage with others and demonstrating greater levels of engagement; in children, this was observed in playing with peers and siblings, in adolescents this focused primarily on interactions with the family and with adults, which represented engagement with a wider range of people. There were reports of better social skills in the children, increased integration with peers in adolescents, and adults were reported to be better at conversing.
For adults, too, willingness to engage in conversations with others was highlighted:
Well, she wasn’t able to, like, enjoy being around people before. Um, and she was actually very, uh, wary of having conversations with anybody. […] But now she’s participating in conversations instead of just trying to shy away or figuring out a way to get out of conversation. [SP/IwASD: F, 18]
Thus, the changes experienced in interpersonal relationships were common in theme, but reflective of the life stage of the individual.
Changes Observed in Use of Free Time
The changes reported in use of free time often related to the autistic individual’s increased interpersonal skills and willingness to engage others. These changes also often aligned with the typical life stage of the autistic individual. In children, the changes in use of free time focused upon play; there was an improvement in understanding of rules during play, improved engagement in play with others, and reports of new interests and activities. For children, improvements in play allowed them to participate in reciprocal play with peers, which required cooperation and listening. When remarking on how their child interacted with others, one SP recalled,
I remember him having this unbelievable play date. He was at the park and he was drawing and his friend comes over and they’re drawing with chalk and the friend decides to make the Super Mario characters that they’re drawing come to life and they were playing Super Mario tag, and that was the first time I looked at [Son’s Name] and I was like, ‘Oh, my God.’ I’m like, not only is he playing with another friend, he’s following someone else’s plan. There’s reciprocity, he’s smiling looking back at the kid. [SP/IwASD: M, 8]
Study partners of adolescents also reported being better at playing with others and wanting to participate in activities more, including wanting to do things with friends and family. A more diverse range of interests, as well as increased participation in activities, were highlighted,
While taking the medication we noticed that he was open to, you know, going to the movies, going and playing baseball, um, riding a bike. Um, getting outside a little more and not constantly playing video games. [SP/IwASD: M, 14]
In adults, the focus was again on being more social and productive, with one SP noting,
Now he’s more interactive with others, ‘cause before it would just be immediate family members, and now he kind of goes outside of that. He’ll talk to other people now, more so than what he ever did before. [SP/IwASD: M, 22]
For some adults, changes in productivity meant a renewed focus on academics:
All of a sudden, he has started deciding that if he wants to make it in college, he’s gotta do this, that, and the other thing. And he’s going to stop watching TV, and he’s going to do extra study. He sits in his room in the morning when he gets up and he studies. [SP/IwASD: M, 43]
Improved sociability and productivity resulted in increased independence in these settings for adults:
Before he didn’t want to be in a group unless somebody was right there with him ‘cause he wouldn’t assert himself. Now he’s like ‘No mom I got it’ and I’m like okay, awesome. And to see the improvement from needing somebody to be there with him to be in a social situation ‘cause he always felt awkward. [SP/IwASD: M, 18]
Changes Observed in Coping Skills
There were common themes across cohorts raised in the discussion regarding improvements in coping skills. Across all cohorts, the most commonly reported changes experienced related to greater adaptability and improved emotional self-regulation in changing situations. Children were commonly reported to show a better understanding of rules and social norms as well as an awareness of risk and consequences. One SP noted that their child’s behavior was more appropriate in social settings and that they were not engaged in self-harm behaviors, which often scared the child’s peers:
So the one thing that the school has said that because he’s not self-harming, like he’s not banging his head anymore, kids are not freaked out. Last year… a lot of the kids wanted to stay away from him because he was self-harming himself. He literally would make his nose bleed. So the kids like kind of stayed away from him. That part has disappeared, so kids can approach him more, and they don’t freak him out as much. Where before, he didn’t care if people were freaked out about it, he would just do it. In other words, that has increased his social behavior. [SP/IwASD: M, 9]
Study partners of adolescents highlighted an improved ability to adapt and respond to change. One SP noted,
He was able to handle changes a little bit more, because he doesn’t usually do well when things change on him, he likes things the same, but he was able to deal with it a little bit better. [SP/IwASD: M, 13]
This improved adaptability was marked by an increase in calmness:
As the study went on, it’s like we realized that we didn’t have to remind her as much and also too, she was able to sit calmly and wait her turn instead of getting anxious and-and stuff. [SP/IwASD: F, 17]
Much like adolescents, SPs of adults also noted improvement in adaptability:
In changes of routine, so before he would get frustrated, really frustrated and go silent, um, if it was something he wanted to do, which was most of what we do and now he, um, I’m trying to think. He doesn’t get frustrated but we end up doing it anyway. He just, the way he is now is he expresses it kindly that he would rather not change what we’re supposed to do. [SP/IwASD: M, 51]
Adaptability in adults was often described alongside increased independence. Thus, while gains in coping skills were observed, the manifestation of these improvements varied depending on the age of the autistic individual.
What Did the Change in Socialization Mean for Individuals with ASD and Their Study Partner?
The overall impact of the changes in Socialization that were observed during the clinical trials were wide-ranging. Increased socialization led to a decrease in stress, and this was associated with improvements in family life. SPs of child and adolescents noted that they could achieve “peace” within the family unit and that individuals with ASD displayed more awareness of relationships. In turn, this awareness of others improved interactions and facilitated communication skills, leading to improved relationships with friends and family.
The changes observed in socialization skills were reported by SPs to have had a substantial positive impact on the autistic individual, the SP, and the larger family across all cohorts. Across all cohorts, SPs reported more positive relationships for the autistic individual; for the child cohort, this was mainly within the family, for adolescents this extended to friends, and adults were reported to have more interactions with a variety of others, as well as richer, deeper relationships more generally. See Tables 3 and 4 for the types of impacts noted by SPs because of improvements in the individual’s Socialization for each cohort.
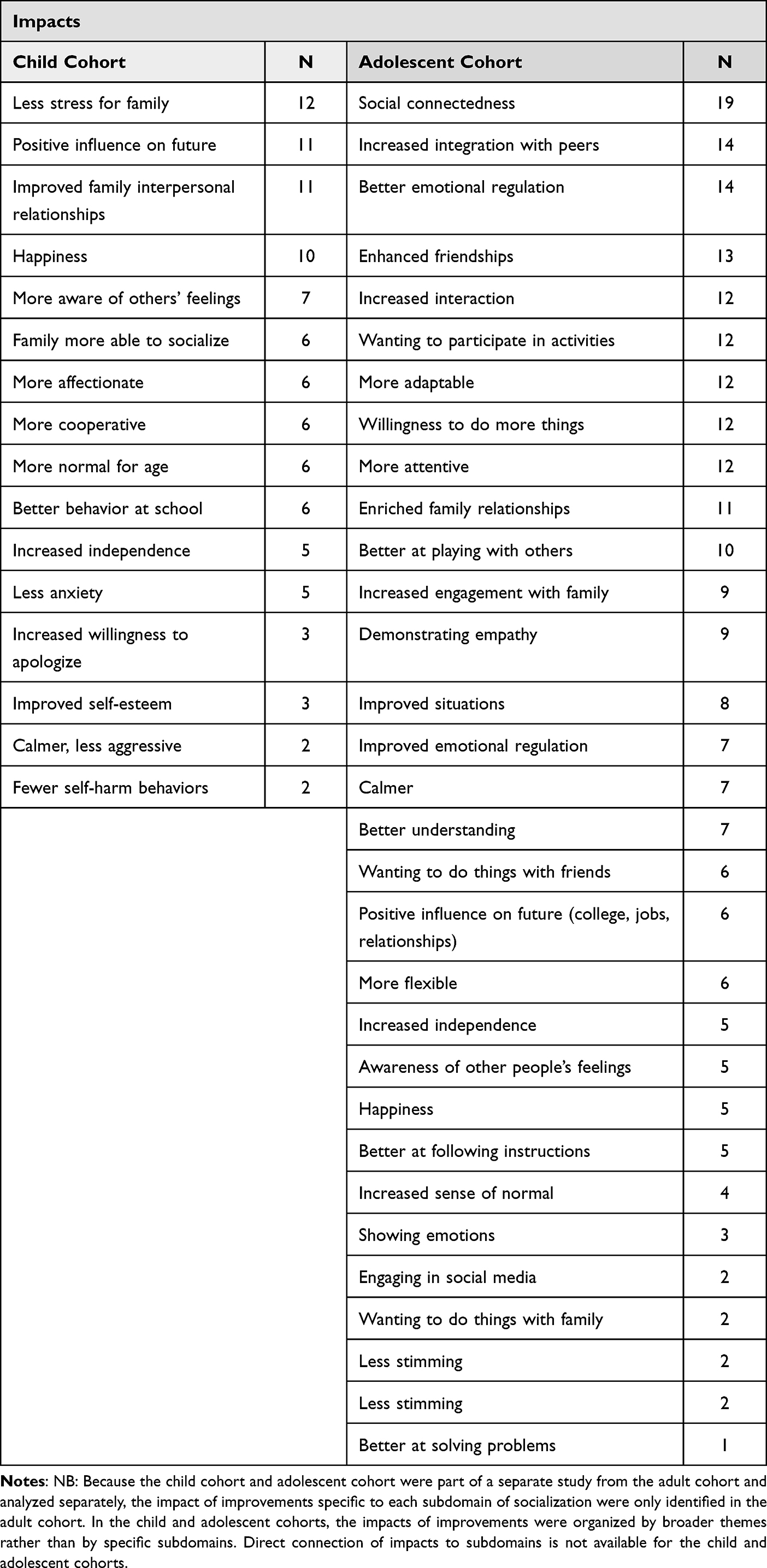 |
Table 3 Impacts of Socialization Changes – Child and Adolescent Cohorts |
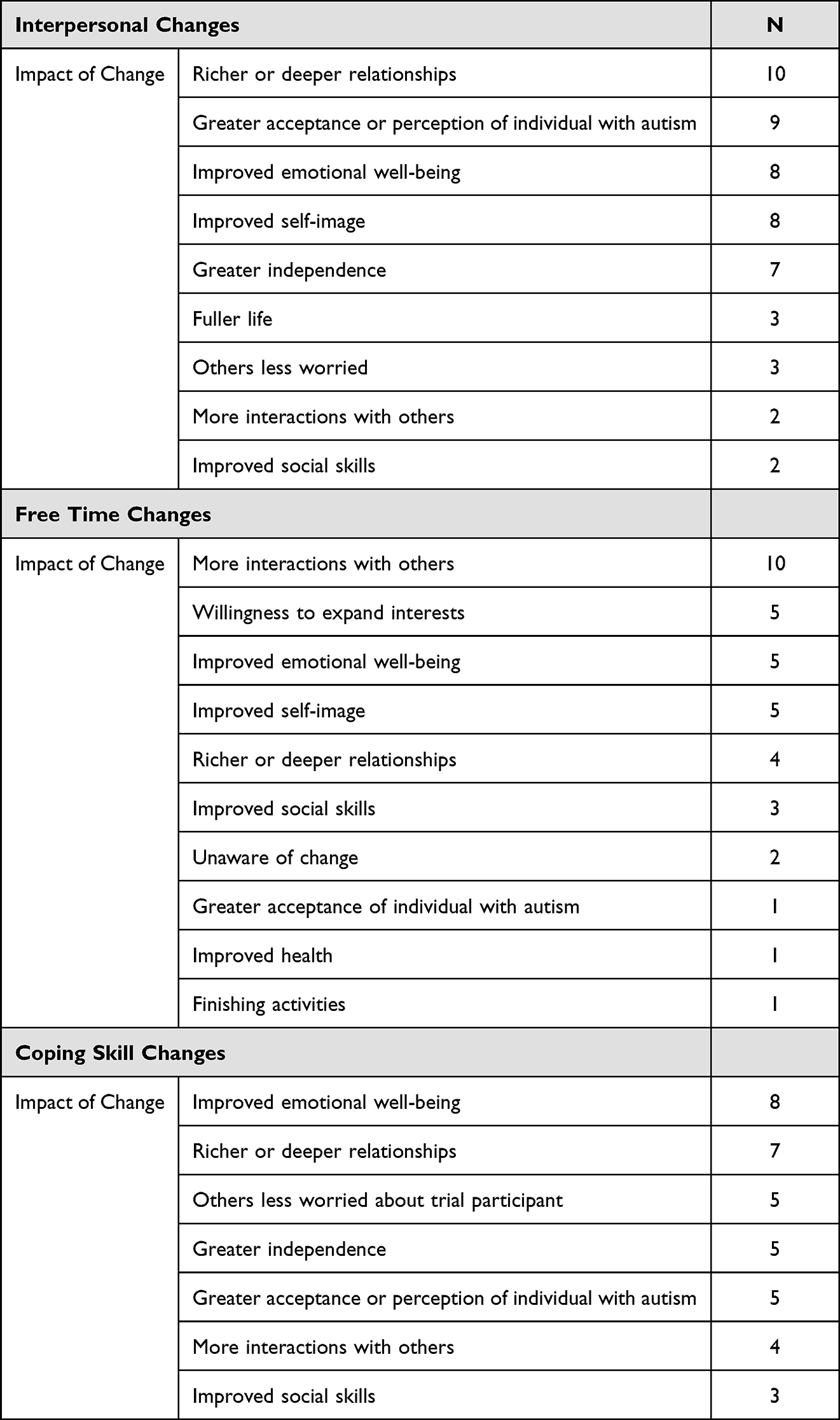 |
Table 4 Impacts of Socialization Changes – Adult Cohort |
In the child cohort, the changes in Socialization allowed the family to interact more with others, adolescents were also reported to be willing to do more things, and adults were reported to be more willing to expand their interests. Repeatedly, SPs highlighted a reduction of stress on the family unit,
A lot less stress, for us it’s more fun because we can actually go places and not always worry. Go out to dinner, go to the fair, stuff like that and he’s fine. [SP/IwASD: M, 8]
Behaviorally, those in the child cohort were reported to be more cooperative, better behaved at school, calmer and less aggressive,
It was so nice for it to not be a complete disaster every day, for her not to think it was the most horrible thing on earth. It was so nice for the first time in my life, to have her not have all these concerns and issues and, blow-ups because something was different or not how she wanted it. [SP/IwASD: F, 10]
Additionally, children were more aware of other’s feelings, more affectionate, and more willing to apologize. One SP noted, “He’s more spontaneously loving with us. Spontaneous hugs and spontaneous ‘I love you, mom’ and things like that.” [SP/IwASD: M,9] Because children were more aware of others, they were able to both participate in and enjoy play more,
He just kind of came up to me all of a sudden at home, he was playing with his sister. They were playing this superhero game and he’s like, ‘I used to feel anxious about pretend play, but now I know it’s fun.’ [SP/IwASD: M, 9]
Among the adolescents, individuals were reported to have better emotional regulation, understanding, and ability to follow instructions. These improvements allowed children to have richer interactions with their peers,
One of the teachers called him a social butterfly. I just about fell over. But the thing is, kids are listening to him. They, they want to. They used to be so mean to him. And, you know, he would try to say something and everybody would talk over him. And people are now looking to him. [SP/IwASD: M, 15]
Richer interactions with peers were seen as the gateway to acceptance by others,
See people being kind to him, and see him smiling and joining in and fitting in, gosh, I’d give just about anything for that. [SP/IwASD: M, 15]
Much like adolescents, SPs of adults reported richer, deeper relationships,
I think he’s finding that helpful too. He’s not feeling alone, isolated, and, um, I think that’s helping him, uh, feel more connected again also. [SP/IwASD: M, 26]
For SPs, witnessing the adult with ASD have more robust relationships relieved stress,
Well, for me, it’s like a huge weight has been lifted off my shoulders. Because social activities are genuinely crucial. So, the fact that he’s opening up to carry out some sort of activity, outside the house and with friends, well, that is a whole new world. […] It used to be unthinkable that my son would leave for three or four days to a countryside holiday with his friends. And however last August he’s been out for four days with his friends, I mean it’s a change I didn’t think I would see. [SP/IwASD: M, 22]
Across all cohorts, greater levels of independence were reported, improvements in happiness, self-esteem, and emotional well-being. The SPs reported less stress upon the family, less worry, and a more positive outlook for the future, whether it be the future education of adolescents or the ability to live an independent life without relying on the SP.
Communication Skills
What Changes Were Experienced in Communication During the Clinical Trial?
To understand changes in Communication, SPs were asked to describe in detail any changes they noticed since starting the clinical trial in expressive communication, receptive communication, and reading and writing skills (ie, the 3 subdomains of the VABS Communication domain).
The majority of SPs in the child and adolescent cohorts reported experiencing improvements in Communication during the clinical trial (33/40 for the child cohort, 28/46 for adolescents), and about half of the adult cohort (21/41), which included improvements across all 3 subdomains. The remaining SPs reported no change except for 3 who reported a worsening (1 in the child and 2 in the adult cohorts), and 4 for whom there was missing data on the rating of change on the SPPMC (2 adolescent and 2 adults) (see Figure 3).
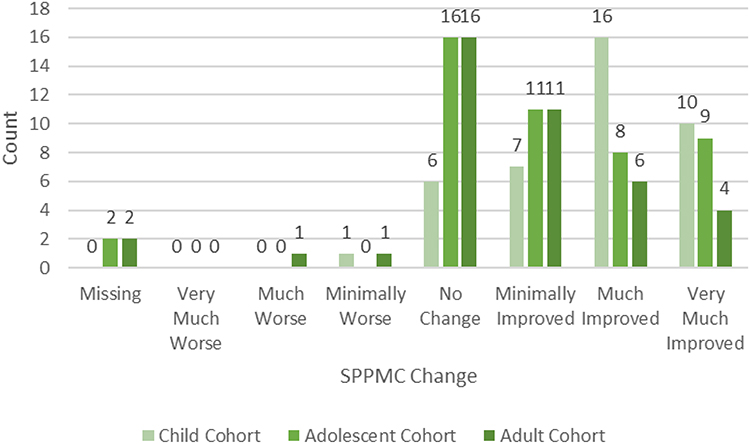 |
Figure 3 SPPMC changes in communication. Abbreviation: SPPMC, Study Partners Perception of Meaningful Change. |
Overall, individuals across all three cohorts saw improvements in their concentration within conversations and their ability to have longer and more articulate conversations. During interviews, SPs noted that the autistic individual paid more attention, was more expressive, and showed more interest in engaging in humor. See Table 5 for key themes of types of changes noticed by SPs.
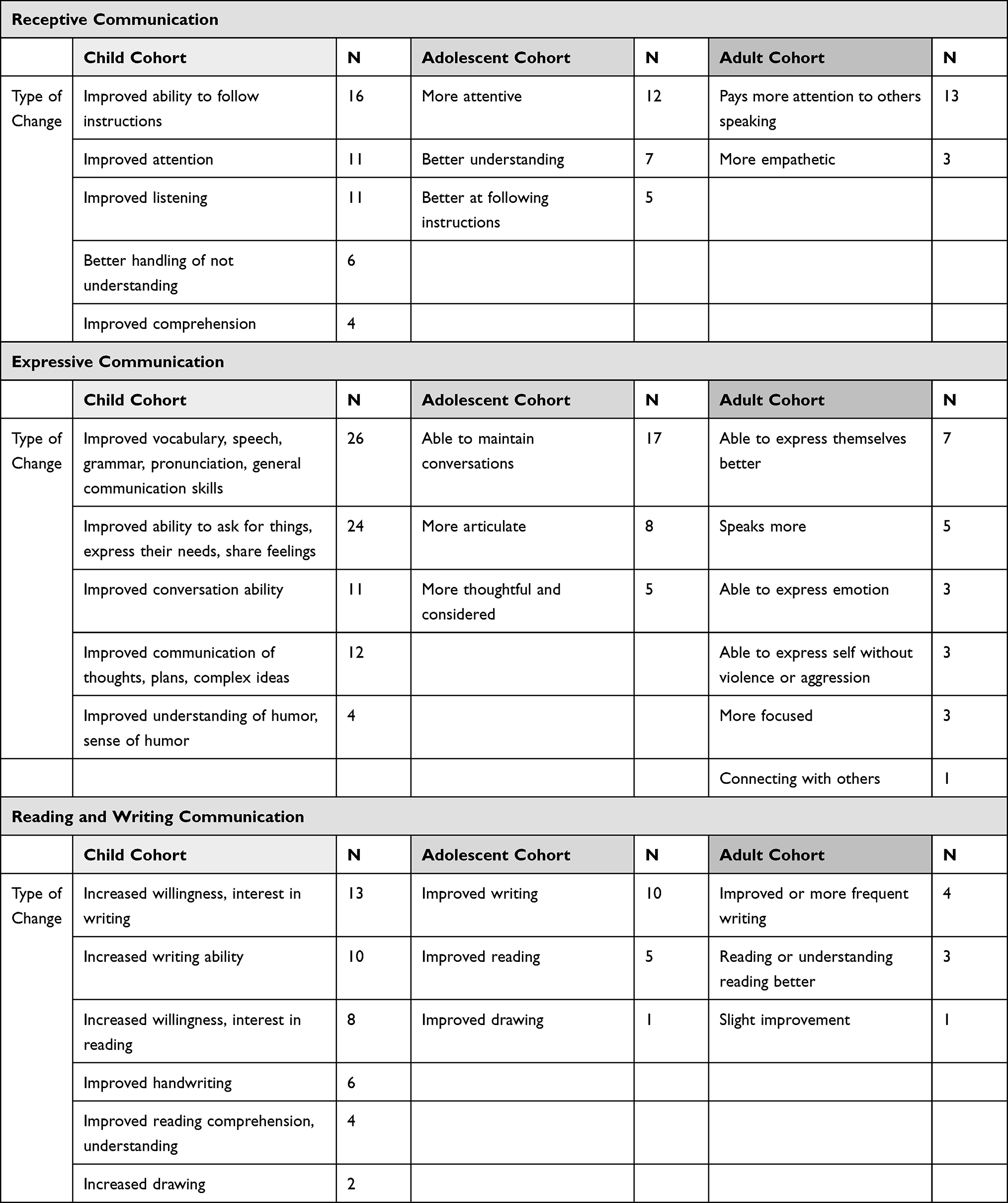 |
Table 5 Communication Changes by VABS-C Subdomain |
Changes Observed in Receptive Communication
Across all cohorts, an improved level of attention during communication was reported. Children and adolescents were reported to have a better understanding of communication. For children, better communication was two-fold: better listening and better spoken self-expression. When discussing the child’s listening, one SP noted,
She is trying to listen more. It doesn’t mean she’s going to do it all the time, but since she’s slowed down to listen more, when she does listen, she tends to do whatever was talked about, because she actually heard the whole thing instead of her version of it. [SP/IwASD: F, 11]
Improved self-expression in children was marked by better articulation of thoughts and feelings,
I believe that now he’s much more verbal and can more clearly communicate his thoughts and feelings than when he started. His vocabulary just has… it’s almost as if his thoughts are just more clear. Like the word’s always been there, but he seems to be able to put them together in a clearer, more expressive way. [SP/IwASD: M, 9]
Additionally, both children and adolescents were better or more able to follow instructions. One SP noted an improved ability to understand more complex or multi-step instructions,
While we still can’t give him complicated instructions, I have seen now we can give him two, sometimes three-part directions. Whereas before, it had to be one instruction at a time. [Child’s name], go brush your teeth. Now we can say, [Child’s name] go brush your teeth and then grab your jacket. [SP/IwASD: M, 7]
For adolescents, improved receptive communication meant the child did not have to receive instructions multiple times,
I said that he’s chiming into things. We were so used to him never listening and having to repeat myself over and over to him, almost like he’s in his own world. Yes, he listens a lot, lot more. [SP/IwASD: M, 15]
While children and adolescents showed improvements in listening skills, improvements in adults also included being able to be more empathetic when listening to others. This manifested as allowing others to finish their thought or statement without interruption and an increased ability to ask relevant questions of another person:
He lets people talk instead of end, uh, interrupting. Um, he asks questions. Um, well he does still interrupt me anyway. Um, but he, when he’s interrupting, he’s asking me questions relevant to what I’m saying instead of being critical, um, and pushing back on what I’m saying. So that’s an improvement. [SP/IwASD: M, 51]
Changes Observed in Expressive Communication
More specific changes in expressive communication were reported in children, as may be expected given their age and naturally still developing in their language abilities. Children were reported to show improvement in vocabulary, speech, grammar, and pronunciation. They were noted to have improvements in communication of thoughts, plans, and expressing complex ideas, as well as an understanding and awareness of humor. Several SPs highlighted the reciprocity that marked improved communication,
I’ve noticed since then that there’s been more interest in reciprocal conversation… Before, his conversations were very short, very direct, just basic facts, and to the point, and not really interested in a lengthy conversation or reciprocating. He would answer questions, he might ask a question here and there, but it was very short and direct. I’m noticing now that, when he does talk about things that interest him, he’s going into more detail. He’s asking a lot more questions [and is] very inquisitive about things that he’s interested in or wanting to know what other people think about things. So his level of interaction, I believe, on the conversation level has increased. [SP/IwASD: M, 9]
Additionally, children were reported to be more able to ask for things, express their needs, share feelings, and have better conversational abilities. One SP noted that conversational abilities improved because the child with autism was not as frustrated while trying to communicate, which allowed her to be more successful,
Her willingness to try and communicate. I think it was so [important]. She would get overwhelmed and frustrated, and then, just sort of close down, and be done. Once she started having success, then the shutting happened a lot less often. That’s a benefit for everyone. If nobody understands you, what’s the point? If people are starting to understand you, there’s more benefit to it, and she’s happier that people are trying to understand her. [SP/IwASD: F, 10]
Similarly, adolescents and adults also were reported to be more able to express themselves and be more able to maintain conversations or speak more. One SP noted, “Now he’s having full-blown conversations, even about stuff that he’s not into.” [SP/IwASD: M, 15] An increase in ability to communicate also led to more enjoyment while conversing,
He ended up going and having a really good time and having a conversation with this guy that lasted at least half an hour or an hour or so, over you know, just stuff that he liked. So could have a back and forth conversation with someone about that certain topic that he liked. [SP/IwASD: M, 14]
Much like the child and adolescent cohorts, SPs of adults also reported adults being better able to express emotions and communicate their thoughts more clearly,
If he... now as opposed to before the study, sometimes he is able to explain back to me, um, details of the circumstance whether it’s something that needs to be done or something that has been done, um, he’s able to state back to me more readily what, whatever the communication piece is so that he can be like, ‘So, what you’re telling me is-’ and he’s understanding it so that I don’t have to be like, ‘No, that’s not it.’ [SP/IwASD: M, 36]
Importantly, SPs of adults noted that increased communication they witnessed was marked by decreased aggression. For example,
He would then get mad and just don’t say anything for a long period of time. Now he’s actually venting and saying more. You know, like I don’t know this, I don’t. He doesn’t like for you to discuss him when he’s not there. He doesn’t like that. [SP/IwASD: M, 25]
Changes Observed in Reading and Writing
Across all cohorts, SPs noted improvements in the autistic individual’s ability and interest in writing. Additionally, an increased ability and interest in writing and reading allowed for new or deeper modes of connecting with peers, although the modes differed by cohort. For children, writing notes in school to classmates allowed for increased connection with peers:
She’s been doing a lot of writing of letters to peers and inviting them to recess or lunch or just expressing thanks or that she hopes that they feel better or whatever the situation is. I think that’s helping her communicate more. [SP/IwASD: F, 7]
For adults, an increase in reading and writing signified increased communication with others through email or other digital message exchange:
He was always pretty good about writing. Um, he’s not communicating anymore wri- by writing, but he does more on the computer […] communications with emails and stuff like that. [SP/IwASD: M, 51]
Importantly, legibility increased for some, particularly adolescents:
Writing was very much improved. She was writing like a third grader. It was becoming very legible now. [SP/IwASD: F, 14]
Increased legibility may allow attempts at written communication to be more successful.
What Did the Change in Communication Mean for Individuals with ASD and Their Study Partner?
The impacts of improved communication for an autistic individual were far ranging and present within each age cohort. Overall, increased communication allowed for more effective and willing interaction. Study partners noted that the impact of improved communication was that the autistic individual genuinely seemed to find some pleasure in interactions. This allowed for the family unit to feel more relaxed and more highly functional. Study partners of adolescents and adults with ASD repeatedly noted how these communication improvements would positively impact both school and work for years to come, leading to greater independence with less reliance on the SP. Improved self-esteem and emotional well-being were consistently reported across all cohorts. Additionally, across all cohorts, SPs reported more positive relations, particularly within the family, such as less stress in the child and adolescent cohorts and a more positive outlook for the future of the autistic individual. A positive outlook for the future was often mentioned in conjunction with increased independence. See Tables 6 and 7 for the types of impacts noted by SPs because of improvements in the individual’s Communication for each cohort.
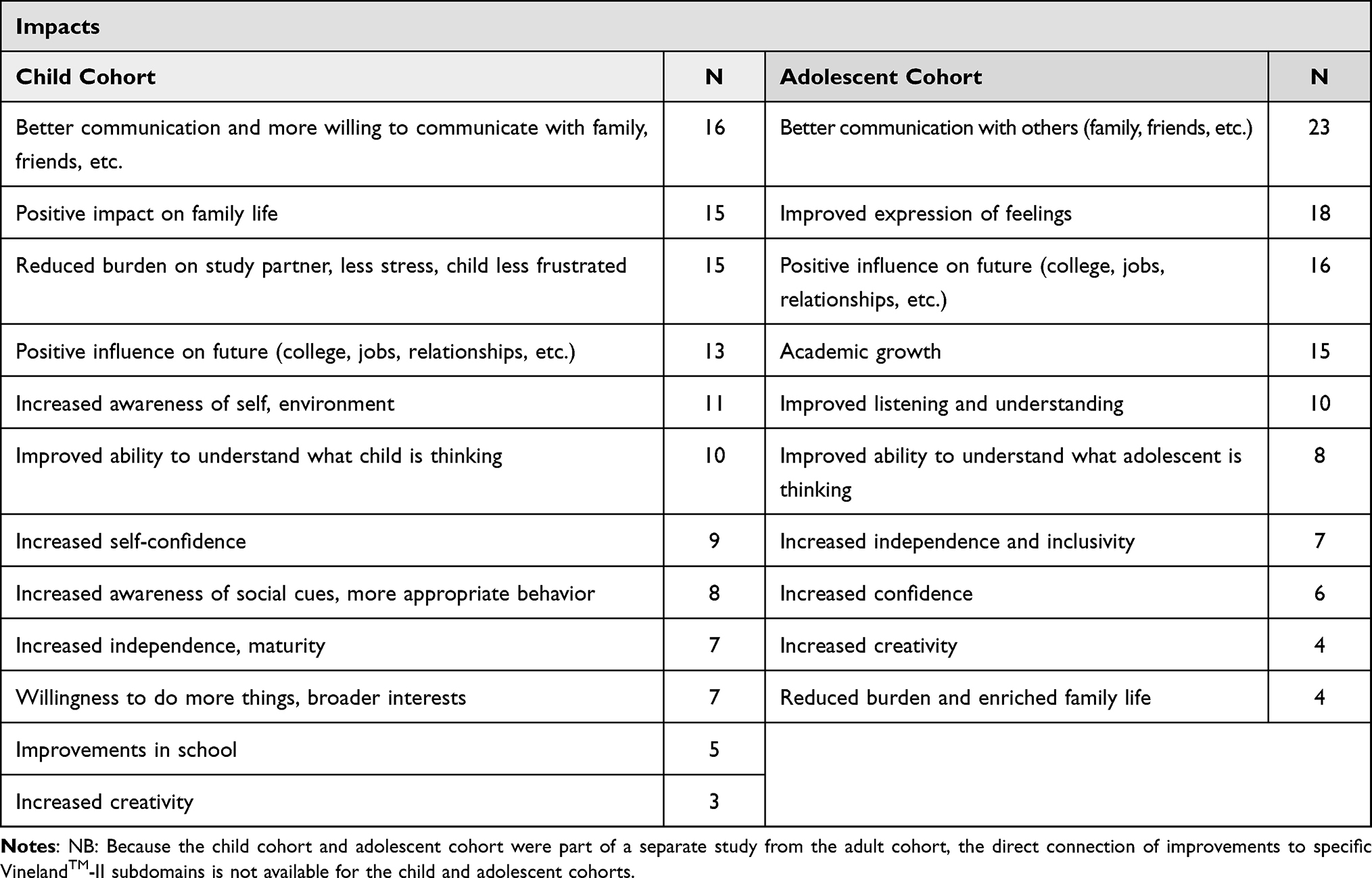 |
Table 6 Impacts of Communication Changes – Child and Adolescent Cohorts |
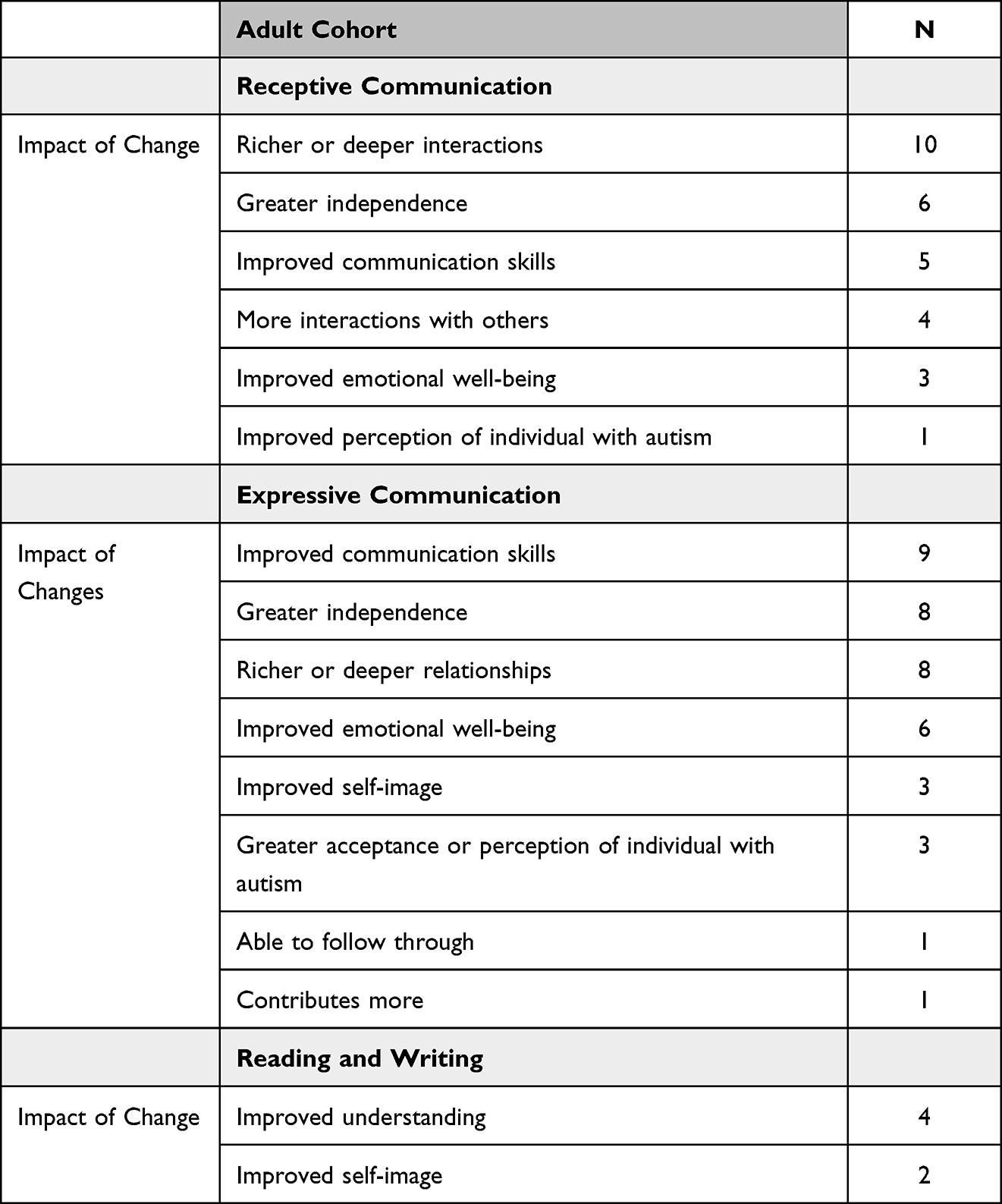 |
Table 7 Impacts of Communication Changes – Adult Cohort |
The impact of changes in Communication were similar to those of improved social skills. Individuals were better and more willing to communicate with family and friends, children showed increased awareness of social cues and more appropriate behavior, increased awareness of self, and improvements in school:
For me I think his future is better. Like the way he is at school, he’s getting good grades. Obviously he’s listening and understanding what the teacher’s telling him because he’s doing pretty well in certain things at school, like math and science and stuff like that. Geography, he’s amazing at, obviously. So stuff is getting through to him. I feel like that gives me hope for his future. [SP/IwASD: M, 8]
Study partners of adolescents also reported greater academic growth, and increased independence and inclusivity,
It’s a good thing, because it means he’s, going a little bit further academically, which opens up more doors, you know, in the future. [SP/IwASD: M, 13]
Importantly, SPs stated that this improvement manifested in a classroom setting,
I would say within two weeks, the teachers were all noticing a difference and they were emailing me, you know, commenting on how much better his behavior was and he was actually trying harder and seemed to be more concerned about his work and his grades, where prior to the medication he just, you know, he didn’t care. [SP/IwASD: M, 14]
For SPs of children and adolescents, educational attainment was linked to a brighter future for the autistic individual, which provided emotional relief.
The improvements in Communication also impacted the social lives of adolescents with SPs noting the adolescents’ ability to communicate reciprocally to be a good friend,
Well, I think it’s helped him with his friends. That he’s able to be more of a friend. A better friend, you know, to listen and be able to have an actual conversation instead of just kind of a one way, ‘Hey, this is what I want to talk about,’ kind of a thing. [SP/IwASD: M, 13]
Additionally, SPs noted that improvements in communication allowed the adolescent to be a more active and well-integrated member of the family,
Well, he just seems more, more of a part of the family. Like, he’s better bonded to us and, you know, like, when something happens in school, he can tell us exactly what his part was. [SP/IwASD: M, 14]
Many SPs who were parents of adolescents remarked that the family unit was better able to function, often with less stress and frustration:
That’s also pretty important, I think. You know, it definitely helps the way that we get along with each other and with him, to know that he is capable of give and take, and that we’re not always having to butt heads over, you know, his way or the highway kind of a thing. [SP/IwASD: M, 13]
Much like the adolescent cohort, for adults, improved communication was also marked by reciprocity in communication,
The con- The communications goes longer because he’s now communicating ideas that he’s responding to other people’s words better. […] For me it’s good because, um, we actually have conversations. It’s- it’s a two-way street, it’s not just a one-way street on a conversation now. [SP/IwASD: M, 42]
As is expected given the age of adult individuals with ASD, less emphasis was placed on academic achievement or success and instead SPs felt positive impacts in interpersonal relationships.
Discussion
The qualitative data from these interviews confirm that individuals with ASD without ID experience impairments in adaptive functioning, as captured by the VABS. This is consistent with other research in high functioning ASD.9,10,12 Socialization and Communication were rated as the most important domains across all cohorts. There was a slight tendency for SPs of younger children to rate Communication as more important than adolescents and adults, who tended to rate Socialization higher. This could be reflective of previous research showing that older children demonstrated better communication skills.10 However, the current findings suggest that it is not relevance that varied by age but, rather, the specific way in which impacts were experienced. The complexity and heterogeneity of ASD was also shown and the interaction between areas of challenge was identified by SPs. While Socialization and Communication were seen by SPs as the two most important domains within the VABS, across all cohorts, they were also seen as highly interrelated concepts, which has been described in previous research on ASD.30 For instance, SPs who reported improvements in the Communication domain often noted how such improved communication meant the individual could have deeper and more meaningful social relationships. Similarly, SPs who reported improvements in the Socialization domain often noted that such changes meant the individual could interact and communicate with others more often or more appropriately.
Improvements in socialization reported by SPs had a meaningful impact on the autistic individual themselves and those around them. Study partners described the person being able to engage with a wider range of people than they had before and that such interactions were often more positive. Improved social interactions included being able to make eye contact, which research has shown is especially relevant to the social difficulties of adults with ASD.31 Such improved social interactions meant that the autistic individual was more accepted or seen more positively by others around them, which SPs saw as contributing to the person’s increased self-esteem. More positive social interactions also indicated to SPs that the autistic individual could be more independent, especially important to SPs of children, adolescents, and younger adults who hoped improved social skills could lead to having a job or a better future. This is consistent with other research highlighting the importance of independence.14 Study partners also noted the importance of social improvements around being more open to different situations and different interests. Such improvement in being able to adapt to different social situations meant improved emotional well-being for the autistic individual, feeling happier and less frustrated in different social contexts.
Study partners who reported improvements in communication similarly indicated that these improvements had real impacts on the person’s life. One of the most commonly reported improvements related to communication was the autistic individual paying more attention to others speaking and not interrupting. This focus on being able to pay attention is understandable given that joint attention has been described as often lacking in individuals with ASD and key to being able to engage in social interactions.32 As with improvements in socialization, such improvement in being able to pay attention to others meant that the autistic individual could have richer interactions with others they were close to. Communication was also improved by the person being able to better express themselves, particularly in terms of being able to do so in more non-aggressive ways. Fewer SPs noted a change in the person’s reading and writing skills compared to other areas of communication. Furthermore, most of those SPs who observed no change in this area specified that reading/writing was not something they were particularly hoping or expecting to see change in, especially in the adult cohort. This suggests that when it comes to communication, SPs were most focused on improvements around verbal communication and interactions.
This is the first study to capture meaningful change in a broader population of individuals with ASD without ID, including adults, and explore how changes in ASD manifest and the impact of those changes. Ultimately, improvements in the Socialization domain enabled the person with ASD to have greater awareness of the feelings of others and develop more empathy and kindness. Improvements in the Communication domain allowed for the autistic individual to be better at listening and better at self-expression. Together, changes in these two domains allowed for richer, deeper relationships. Study Partners repeatedly mentioned that improvements in these domains allowed for better integration within the family unit, decreased stress, and increase optimism about the future of the autistic individual. Such changes could lead to tangible benefits in the everyday lives of individuals with ASD, according to SPs, including having larger social networks for support, better prospects for work or school, and greater independence, being able to live on their own and relying less on the SP or other family members for support including financial support. Greater independence was of particular importance to SPs in both cohorts, as concerns for the future in the child cohort but, in the adult cohort, SPs, who were growing older, worried about what would happen when they were no longer around to help the autistic individual. As one SP noted,
That means that there’s a lot more possibility that he can handle this on his own when I die. […] Because I was the one who was always fixing his problems before. Because he’s finding ways to connect to the world, that even if he needs help, he will go out and find people who are appropriate, who could help him. [SP/IwASD; M, 43]
Some limitations of this study should also be noted. There was a 4-week window for exit interviews and because of this, some SPs spoke about changes that happened after the end-of-trial rather than during the trial. However, these instances were few, and interviewers reminded SPs to focus on changes only observed during the trial. Additionally, while we found it valuable to conduct interviews with SPs rather than trial participants with ASD, it can be expected that the SP would focus on what is noticeable to them and there could be other changes experienced. It was not possible to gain information on how the autistic individual felt about any changes they had observed in themselves over the course of the trial, or any other changes they may have experienced. Additionally, this research was conducted in SPs of individuals with ASD without ID. Based on the research already discussed, the challenges experienced in adaptive functioning may be different for those with ID. The findings therefore can only be applied to those with ASD without ID.
Importantly, this manuscript describes the qualitative data on exploring the changes that were observed over the two clinical trials, and the impact that these changes had upon the autistic individual and their family. But this should be read in conjunction with the associated quantitative manuscript, which undertakes a quantitative analysis of meaningful change thresholds. Thus, to gain a full understanding of how individuals with ASD experience changes and the meaning of those changes, both quantitative and qualitative data must be examined together to understand the impact of changes. There is thus an associated manuscript presenting an exploration of meaningful change on the VABS-2DC using quantitative analysis to determine thresholds and qualitative data from these exit interviews to contextualize and interpret meaningful change. In the future, these insights can be used to support clinical trial design, and, thus, could support the development of future therapies for the core symptoms of ASD.
Conclusion
The impacts of changes in any domain were synergistic, combining together to create positive experiences which in turn led to further positive impacts in other skills. These qualitative insights provide context to the changes that were observed during the clinical trial and captured using the VABS, illustrating the meaning of these changes to the individuals with ASD and their families, and the impact that they have on people’s everyday lives and overall HRQOL.
Abbreviations
ASD, Autism spectrum disorder; COA, Clinical outcomes assessment; EIP, Exit interview population; FDA, Food and Drug Administration; HRQOL, Health-related quality of life; IwASD, Individual with autism spectrum disorder; ITT, Intention-to-treat; MCT, Meaningful change threshold; QOL, Quality of life; SD, Standard deviation; SP, Study Partner; SP/IwASD, Study Partner of an individual with autism spectrum disorder; SPPMC, Study Partner perception of meaningful change; VABS, Vineland-II Adaptive Behavior Scale; VABS-2DC, Vineland-II two domain composite; VABS-C, Vineland-II – Communication; VABS-S, Vineland-II – Socialization.
Ethics Approval and Consent to Participate
For both the aV1ation and V1aduct studies, approval by the Institutional Review Board and Ethics Approval were obtained before study initiation, as appropriate for each site, from an Institutional Review Board or Ethics Committee at each site provided in (supplementary materials). Both studies were conducted in full accordance with the principles of the Declaration of Helsinki and the International Council for Harmonization E6 guidelines for Good Clinical Practice, or the relevant laws and regulations of the country in which the research was done.
All participants and study partners in aV1ation and V1aduct gave written informed consent before enrollment.
Data Sharing Statement
Qualified researchers may request access to individual patient level data through the clinical study data request platform (https://vivli.org/). Further details on Roche’s criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here: (https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).
Acknowledgments
The planned methods of this paper were discussed at ISOQOL 2017. The methods and initial results from a small number of interviews on one VABS domain were shared as an illustrative example as part of a presentation in a symposium at ISOQOL 2020. A poster was presented highlighting the logistical issues with the conduct of exit interviews based on this study at ISPOR 2022. The methods of this study were presented as a presentation at INSAR 2022.
The authors would like to thank the participants and their families, and the study investigators and site staff for their contributions to the studies. Editorial services were provided by ArticulateScience and Emily Calderbank of Clinical Outcomes Solutions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by F. Hoffmann-La Roche Ltd. Additionally, F. Hoffmann-La Roche Ltd. provided funding for medical editorial assistance.
Disclosure
CB is an employee of Clinical Outcomes Solutions, a health research consultancy that was paid to conduct the work by Roche. MC and EG were employees of Clinical Outcomes Solutions at the time of the study. TW, JS, and SC are employees and shareholders of F. Hoffmann-La Roche Ltd. The authors report no other conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental DIsorders: DSM-5. 5th edn. Washington, DC: American Psychiatric Publishing; 2013.
2. Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. The Lancet. 2018;392(10146):508–520. doi:10.1016/S0140-6736(18)31129-2
3. Park HR, Lee JM, Moon HE, et al. A short review on the current understanding of autism spectrum disorders. Exp Neurobiol. 2016;25(1):1. doi:10.5607/en.2016.25.1.1
4. NIMH. Autism Spectrum Disorder. Available from: https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd/index.shtml.
5. Baxter AJ, Brugha T, Erskine HE, Scheurer RW, Vos T, Scott JG. The epidemiology and global burden of autism spectrum disorders. Psychol Med. 2015;45(3):601–613. doi:10.1017/S003329171400172X
6. Brugha TS, McManus S, Bankart J, et al. Epidemiology of autism spectrum disorders in adults in the community in England. Arch Gen Psychiatry. 2011;68(5):459–465. doi:10.1001/archgenpsychiatry.2011.38
7. Zablotsky B, Black LI, Maenner MJ, Schieve LA, Blumberg SJ. Estimated prevalence of autism and other developmental disabilities following questionnaire changes in the 2014 National Health Interview Survey; 2015.
8. Pastorino GMG, Operto FF, Padovano C, et al. Social cognition in neurodevelopmental disorders and epilepsy. Front Neurol. 2021;12:658823. doi:10.3389/fneur.2021.658823
9. Kanne SM, Gerber AJ, Quirmbach LM, Sparrow SS, Cicchetti DV, Saulnier CA. The role of adaptive behavior in autism spectrum disorders: implications for functional outcome. J Autism Dev Disord. 2011;41(8):1007–1018. doi:10.1007/s10803-010-1126-4
10. Operto FF, Pastorino GMG, Scuoppo C, et al. Adaptive behavior, emotional/behavioral problems and parental stress in children with autism spectrum disorder. Front Neurosci. 2021;15:751465. doi:10.3389/fnins.2021.751465
11. Wechsler D . Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV). Pearson. 2003.
12. Operto FF, Smirni D, Scuoppo C, et al. Neuropsychological profile, emotional/behavioral problems, and parental stress in children with neurodevelopmental disorders. Brain Sci. 2021;11(5):584. doi:10.3390/brainsci11050584
13. Johnson CP, Myers SM. Identification and evaluation of children with autism spectrum disorders. Pediatrics. 2007;120(5):1183–1215. doi:10.1542/peds.2007-2361
14. Thompson C, Bölte S, Falkmer T, Girdler S, Martinuzzi A. To be understood: transitioning to adult life for people with autism spectrum disorder. PLoS One. 2018;13(3):e0194758. doi:10.1371/journal.pone.0194758
15. Howlin P, Moss P. Adults with autism spectrum disorders. Can J Psychiatry. 2012;57(5):275–283. doi:10.1177/070674371205700502
16. Ayres M, Parr JR, Rodgers J, Mason D, Avery L, Flynn D. A systematic review of quality of life of adults on the autism spectrum. Autism. 2018;22(7):774–783. doi:10.1177/1362361317714988
17. Calhoun SL, Pearl AM, Fernandez-Mendoza J, Durica KC, Mayes SD, Murray MJ. Sleep disturbances increase the impact of working memory deficits on learning problems in adolescents with high-functioning Autism spectrum disorder. J Autism Dev Disord. 2020;50:1701–1713.
18. Lecavalier L, Leone S, Wiltz J. The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. J Intellect Disabil Res. 2006;50(3):172–183. doi:10.1111/j.1365-2788.2005.00732.x
19. Kuhlthau K, Payakachat N, Delahaye J, et al. Quality of life for parents of children with autism spectrum disorders. Res Autism Spectr Disord. 2014;8(10):1339–1350. doi:10.1016/j.rasd.2014.07.002
20. Ten Hoopen LW, de Nijs PF, Duvekot J, et al. Children with an autism spectrum disorder and their caregivers: capturing health-related and care-related quality of life. J Autism Dev Disord. 2020;50(1):263–277. doi:10.1007/s10803-019-04249-w
21. Goin-Kochel RP, Myers BJ, Mackintosh VH. Parental reports on the use of treatments and therapies for children with autism spectrum disorders. Res Autism Spectr Disord. 2007;1(3):195–209. doi:10.1016/j.rasd.2006.08.006
22. Goel R, Hong JS, Findling RL, Ji NY. An update on pharmacotherapy of autism spectrum disorder in children and adolescents. Int Rev Psychiatry. 2018;30(1):78–95. doi:10.1080/09540261.2018.1458706
23. FDA. The voice of the patient. A series of reports from the U.S. Food and Drug Administration’s patient-focused drug development initiative. Autism. Public meeting: May 4, 2017; January, 2018. Available from: https://www.fda.gov/media/111099/download.
24. Hollander E, Jacob S, Jou R, et al. Balovaptan vs placebo for social communication in childhood Autism spectrum disorder: a randomized clinical trial. JAMA Psychiatry. 2022;79(8):760–769.
25. Chatham C, Taylor K, Charman T, et al. Adaptive behavior in autism: minimal clinically important differences on the Vineland‐II. Autism Res. 2018;11(2):270–283. doi:10.1002/aur.1874
26. Rofail D, Acquadro C, Izquierdo C, Regnault A, Zarit SH. Cross-cultural adaptation of the Schizophrenia Caregiver Questionnaire (SCQ) and the Caregiver Global Impression (CaGI) Scales in 11 languages. Health Qual Life Outcomes. 2015;13(1):1–10. doi:10.1186/s12955-015-0264-y
27. Busner J, Targum S. As adapted from Spearing, et al. Psychiatry Res. 2007;1997(73):159–171.
28. Busner J, Targum S. As adapted from Kay, Stanley R. Positive and Negative Symptoms in Schizophrenia:Assessment and Research. Clinical and Experimental Psychiatry, Monograph No. 5. Brunner/Mazel, 1991; 2007.
29. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
30. Prelock PJ, Nelson NW. Language and communication in autism: an integrated view. Pediatric Clinics. 2012;59(1):129–145. doi:10.1016/j.pcl.2011.10.008
31. Auyeung B, Lombardo MV, Heinrichs M, et al. Oxytocin increases eye contact during a real-time, naturalistic social interaction in males with and without autism. Transl Psychiatry. 2015;5(2):e507. doi:10.1038/tp.2014.146
32. Llaneza DC, DeLuke SV, Batista M, Crawley JN, Christodulu KV, Frye CA. Communication, interventions, and scientific advances in autism: a commentary. Physiol Behav. 2010;100(3):268–276. doi:10.1016/j.physbeh.2010.01.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Quantitative and Qualitative Exploration of Meaningful Change on the Vineland Adaptive Behavior Scales (Vineland™-II) in Children and Adolescents with Autism Without Intellectual Disability Following Participation in a Clinical Trial
Clinch S, Hudgens S, Gibbons E, Willgoss T, Smith J, Polek E, Burbridge C
Patient Related Outcome Measures 2023, 14:337-354
Published Date: 20 November 2023
Male Partners’ Experiences with a Postpartum Haemorrhage Requiring Surgery: A Qualitative Study
Moen OSM, Dahl B
Journal of Multidisciplinary Healthcare 2026, 19:594311
Published Date: 21 April 2026