Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Pulmonary Rehabilitation with Airway Clearance Techniques Improves Mucus Hypersecretion and Clinical Outcomes in COPD: A Retrospective Study
Authors Li H ![]() , Li M, Liu W, Wang D
, Li M, Liu W, Wang D
Received 28 November 2025
Accepted for publication 9 March 2026
Published 1 April 2026 Volume 2026:21 576128
DOI https://doi.org/10.2147/COPD.S576128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jill Ohar
Huiyan Li,1,2 Miao Li,2,3 Wei Liu,1,2 Danxin Wang2,3
1Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Hainan Medical University, Hainan Provincial Clinical Medical Center for Respiratory Diseases, Haikou, Hainan, People’s Republic of China; 2Key Laboratory of Emergency and Trauma of Ministry of Education, The First Affiliated Hospital, Hainan Medical University, Haikou, Hainan, People’s Republic of China; 3Nursing Department, The First Affiliated Hospital of Hainan Medical University, Haikou, Hainan, People’s Republic of China
Correspondence: Danxin Wang, Nursing Department, The First Affiliated Hospital of Hainan Medical University, No. 3, Xueyuan Road, Longhua District, Haikou, Hainan, People’s Republic of China, Email [email protected]
Objective: To evaluate the effects of a pulmonary rehabilitation (PR) program incorporating airway clearance techniques Active Cycle of Breathing Technique (ACBT) and Oscillatory Positive Expiratory Pressure (OPEP) on mucus hypersecretion, pulmonary function, and quality of life in patients with chronic obstructive pulmonary disease (COPD).
Methods: This single-center, retrospective observational study included 118 hospitalized patients with stable moderate COPD and sputum hypersecretion between April 2024 and July 2025. Patients received either PR combined with ACBT and OPEP (PR+ACBT/OPEP, n = 56) or conventional PR with basic breathing training (n = 62). Primary outcomes were sputum volume, sputum viscosity, and responder rate (≥ 20% viscosity reduction). Secondary outcomes included pulmonary function parameters, symptom burden assessed by the COPD Assessment Test (CAT) and modified Medical Research Council (mMRC) scale, and treatment adherence.
Results: Baseline characteristics were comparable between groups. Adherence was high in both groups, and no serious adverse events were observed. At discharge, the PR+ACBT/OPEP group demonstrated significantly greater reductions in sputum volume (− 6.8 mL; P < 0.001) and viscosity (− 46 mPa·s; P < 0.001) than controls, with a higher responder rate (69.6% vs. 29.0%). Improvements in pulmonary function were more pronounced in the PR+ACBT/OPEP group, including FEV1, FEV1%pred, and small-airway indices. Symptom burden was also reduced, with greater declines in CAT scores and a higher proportion of patients achieving the minimal clinically important difference. The mMRC grade improved in the PR+ACBT/OPEP group but remained unchanged in controls.
Conclusion: In this retrospective, single-center study, the integration of ACBT and OPEP into pulmonary rehabilitation was associated with improved mucus clearance, lung function parameters, and patient-reported outcomes in COPD patients with chronic sputum hypersecretion. These findings should be interpreted as exploratory and hypothesis-generating, supporting the potential role of airway clearance techniques within pulmonary rehabilitation and warranting confirmation in prospective, multicenter studies.
Keywords: COPD, pulmonary rehabilitation, mucus hypersecretion, airway clearance, Acapella, ACBT
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous condition characterized by persistent airflow limitation and a wide spectrum of clinical phenotypes, including emphysema-predominant disease, frequent exacerbators, chronic bronchitis, and patients with substantial comorbidity burden.1 While airflow obstruction and acute exacerbations remain the primary drivers of morbidity and mortality in COPD, a substantial subset of patients exhibit chronic mucus hypersecretion, most commonly associated with the chronic bronchitis phenotype.2 Epidemiological studies indicate that approximately 30–50% of patients with COPD report chronic cough and sputum production, although prevalence varies by disease severity, smoking history, and diagnostic criteria.2,3
In this subgroup, airway mucus hypersecretion plays an important pathophysiological role by promoting small-airway obstruction, impairing mucociliary clearance, and increasing susceptibility to infections and exacerbations. Excessive mucus production does not affect all patients with COPD but represents a clinically relevant trait associated with worse symptoms, accelerated lung function decline, and higher healthcare utilization. Although exacerbations are the strongest predictors of mortality in COPD, chronic mucus hypersecretion contributes to exacerbation risk and symptom burden, making it a meaningful therapeutic target within this specific phenotype.2
Neutrophil-driven inflammation contributes to mucus hypersecretion in COPD by promoting goblet cell expansion and increased MUC5AC expression, which has been linked to mucus plugging, lung function decline, and exacerbations.4 In contrast, altered MUC5B expression may further impair baseline mucus clearance,2,5,6 supporting the clinical relevance of targeting mucus dysregulation in selected COPD patients.7,8
Pulmonary rehabilitation (PR) is a cornerstone non-pharmacological intervention for COPD, designed to interrupt the cycle of worsening symptoms and functional decline.9 Comprehensive PR programs, combining supervised exercise training, airway clearance techniques, patient education, and self-management support, have consistently been shown to alleviate dyspnea, improve exercise capacity and health-related quality of life, and reduce hospitalization risk.9–12 Importantly, PR is considered one of the most cost-effective interventions in COPD, with benefits extending across all disease stages, particularly moderate-to-severe disease.
Recent trials indicate that combining Oscillatory Positive Expiratory Pressure Therapy (OPEP) devices such as Acapella® with the Active Cycle of Breathing Technique (ACBT) yields superior improvements in lung function, sputum clearance, and symptom relief compared with breathing techniques alone.13,14 Building on existing evidence, this study aimed to evaluate the clinical effects of a pulmonary rehabilitation program incorporating ACBT and OPEP in COPD,15–17 patients with chronic sputum hypersecretion, with a focus on mucus clearance, lung function, and patient-reported outcomes.
Previous studies have shown that airway clearance techniques, including ACBT and oscillatory positive expiratory pressure devices, can improve sputum expectoration and symptoms in selected COPD populations. However, much of the existing evidence is derived from small randomized trials, short-term interventions, or outpatient settings, and comparative data embedded within structured pulmonary rehabilitation programs remain limited. In particular, real-world observational evidence evaluating both clinical outcomes and biological markers of mucus hypersecretion during inpatient rehabilitation is scarce. To address this gap, the present study uses a retrospective, exploratory design to assess the association between airway clearance–focused pulmonary rehabilitation and clinical outcomes in COPD patients with chronic sputum hypersecretion.
Pulmonary rehabilitation is a cornerstone of COPD management and has consistently been shown to improve exercise tolerance and symptom control. However, the specific role of structured airway clearance techniques within pulmonary rehabilitation programs remains incompletely defined, particularly in patients with chronic sputum hypersecretion. Previous studies have reported improvements in sputum expectoration and symptom burden with ACBT and oscillatory positive expiratory pressure (OPEP) devices, yet most investigations have been limited to short-term outpatient settings or focused on isolated physiological endpoints. Emerging literature has highlighted the importance of mucus clearance in reducing airway obstruction and improving ventilation distribution in COPD, but real-world inpatient data integrating both clinical and biochemical markers remain scarce. Furthermore, comparative evaluations embedded within structured rehabilitation programs are limited, leaving uncertainty regarding the incremental contribution of airway clearance strategies beyond standard rehabilitation care. Therefore, there remains a need for observational evidence that simultaneously examines patient-centered outcomes and mucus-related biological markers within routine clinical practice. Addressing this gap may help refine rehabilitation strategies for the chronic bronchitis phenotype of COPD and inform the design of future prospective trials.
The aim of this study was to evaluate the effects of a pulmonary rehabilitation program incorporating ACBT and OPEP on mucus clearance and clinical outcomes in COPD patients with chronic sputum hypersecretion. Specifically, we assessed changes in sputum characteristics, pulmonary function, and symptom burden during hospitalization. In addition, mucin biomarkers were examined to explore potential biological correlates of clinical response. The overall objective was to determine the clinical relevance of integrating airway clearance techniques into pulmonary rehabilitation for this COPD phenotype.
Materials and Methods
Study Design
This study was a single-center, retrospective cohort study designed to evaluate the association between pulmonary rehabilitation (PR) strategies and airway mucus hypersecretion in patients with chronic obstructive pulmonary disease (COPD). All consecutive hospitalized patients with stable moderate COPD and documented sputum hypersecretion who met predefined inclusion and exclusion criteria during the study period were screened. Eligible patients were included without further selection. Group allocation was determined by routine clinical practice during hospitalization. The choice of rehabilitation strategy (PR+ACBT/OPEP vs. Conventional PR) depended on treating physician preference, availability of airway clearance devices, and individualized clinical judgment rather than randomization or study protocol. No allocation was performed by the investigators. Baseline comparability between groups reflects the use of uniform inclusion criteria and standard inpatient management protocols rather than deliberate stratified assignment.
Group allocation was therefore determined by routine clinical practice rather than randomization or investigator assignment, and all eligible patients meeting inclusion criteria during the study period were included to minimize selection bias. The protocol was approved by the Ethics Committee of the First Affiliated Hospital of Hainan Medical University, and written informed consent was waived due to the retrospective nature of the study.
Participants
Patients admitted to the First and Second Wards of the Department of Respiratory Medicine, First Affiliated Hospital of Hainan Medical University, between April 2024 and July 2025 were retrospectively screened and included in this study (Figure 1).
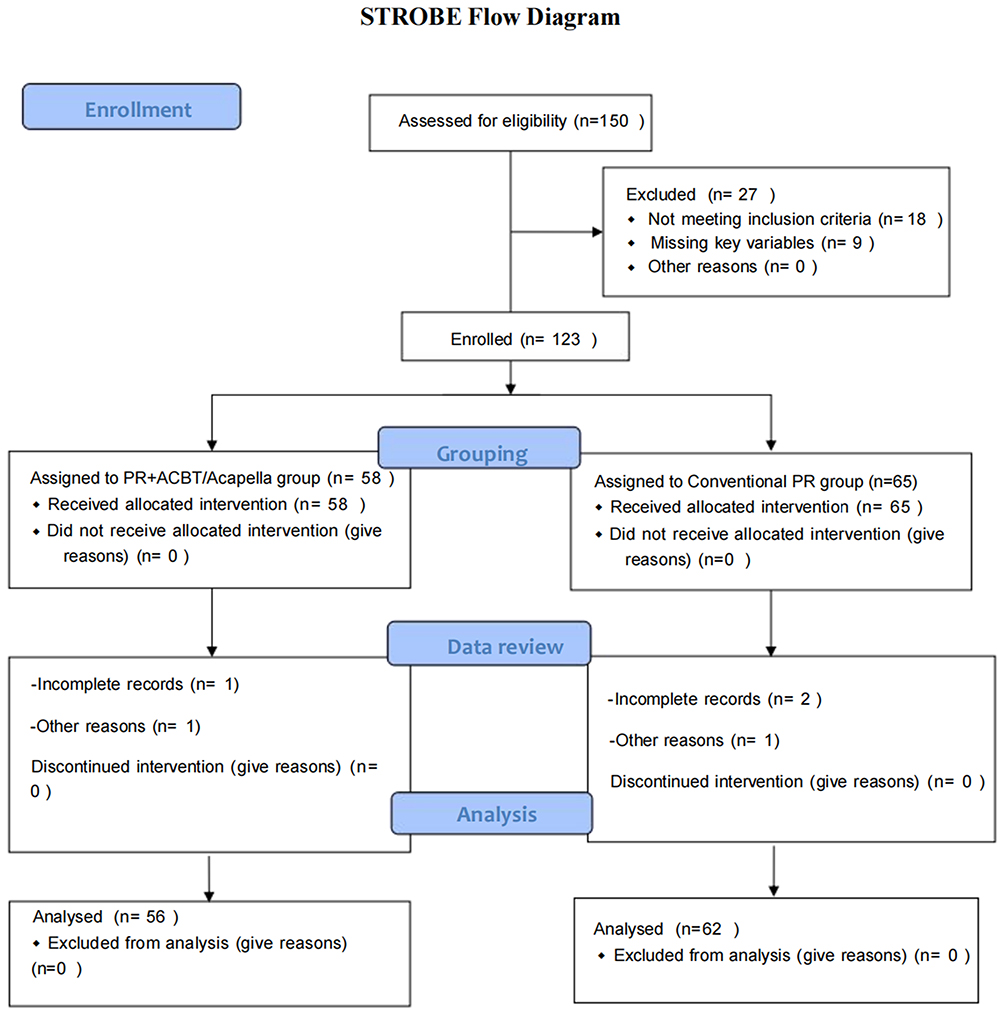 |
Figure 1 STROBE flow diagram of patient screening and inclusion. A total of 150 hospitalized patients with COPD were screened for eligibility. Of these, 27 were excluded (18 did not meet inclusion criteria, 9 had incomplete records). The remaining 123 eligible patients were retrospectively categorized according to the rehabilitation strategy received during hospitalization: 58 in the PR+ACBT/OPEP group and 65 in the Conventional PR group. During chart review, outcome data were incomplete for 2 patients in the PR+ACBT/OPEP group and 3 in the Conventional PR group; these cases were excluded from analysis. |
Inclusion criteria
- Hospitalized patients diagnosed with COPD according to the 2019 diagnostic guideline for COPD;
- Age between 40 and 80 years;
- Clinically stable COPD, GOLD stage II;
- Sputum viscosity grade II or III;
- Clear consciousness, stable vital signs, and able to cooperate with rehabilitation training;
Exclusion criteria
- Concomitant neuromuscular disease or end-stage malignancy;
- Other serious respiratory diseases (eg., bronchiectasis, pulmonary tuberculosis, bronchial asthma) or severe cardiovascular, cerebrovascular, hepatic, renal, or hematologic diseases;
- History of thoracoabdominal surgery, trauma, or chest drainage;
- Participation in other respiratory rehabilitation programs;
- Poor comprehension, or inability to perform rehabilitation techniques.
Withdrawal criteria
- Clinical deterioration during hospitalization that prevented continuation of the intervention;
- Patients with incomplete outcome records who could not be included in the final analysis.
Group Definition and Interventions
Eligible patients were retrospectively assigned into the PR+ACBT/Acapella group (n = 56) or Conventional PR group (n = 62) according to the actual rehabilitation strategy they had received during hospitalization.
Conventional PR Group (Usual Care + Basic Breathing Training)
In addition to routine medical therapy, patients performed pursed-lip breathing, diaphragmatic breathing, and effective coughing exercises (consisting of deep inspiration followed by a controlled, forceful cough to facilitate sputum expectoration) three times daily, for 10 minutes per session.
PR+ACBT/Acapella Group (Comprehensive PR Program)
Patients received a structured PR program comprising;Active Cycle of Breathing Technique (ACBT): Conducted under nursing supervision twice daily (~20 minutes per session). The sequence included breathing control (relaxation with ~2-second breath hold), thoracic expansion exercises (deep inspiration with slow expiration), and forced expiration techniques (huffing with sigh-like expiration), followed by effective coughing.
Oscillatory Positive Expiratory Pressure training (OPEP device duet): Performed three times daily, 20 sets per session. Before training, patients were educated on device principles and use. Exercises were performed in a seated or semi-recumbent position, beginning at a low-frequency resistance setting with an inspiratory: expiratory ratio of approximately 1:3–1:4. After each set, patients performed 2–3 cycles of huffing/effective coughing. Training continued until discharge or until termination criteria were met.
The study was conducted between April 2024 and July 2025, with patient follow-up limited to the hospitalization period, which varied based on individual clinical progress and discharge criteria. This timeframe is appropriate for evaluating short-term changes in symptoms, mucus-related outcomes, and functional measures but does not allow for conclusions regarding long-term clinical outcomes. This limitation should be considered when interpreting the results.
Termination Criteria for Training
Training was stopped immediately if ≥2 of the following occurred: heart rate >130 beats/min; respiratory rate >35 breaths/min; SpO2 <90%; systolic blood pressure <90 mmHg or >180 mmHg; altered consciousness, diaphoresis, agitation, or paradoxical breathing. The number of patients who temporarily interrupted or terminated training due to these criteria is reported in the Results section.
Outcomes and Data Collection
Pulmonary Function
FEV1, FVC, FEV1/FVC, maximal mid-expiratory flow (MMEF), and maximal expiratory flow (MEF) parameters were measured with a spirometer at baseline, after one week, and at discharge.
Sputum Measures
Sputum volume: Volume was collected in a graduated container at 1 hour and 24 hours post-intervention, with daily totals recorded by nursing staff.
Sputum viscosity: Viscosity was measured at constant temperature using an NDJ-1 viscometer (rotor No. 1, 6 rpm). Viscosity (mPa·s) was calculated as: dial reading × 10.
Health-Related Quality of Life
Symptom burden was assessed using the COPD Assessment Test (CAT), a validated instrument specifically designed to measure the impact of COPD on a patient’s health status and daily life, and the modified Medical Research Council (mMRC) dyspnea scale. The officially licensed Chinese version of the CAT was used in accordance with the copyright and trademark requirements of the CAT Development Steering Group, and the questionnaire was administered with all required trademark and copyright notices as specified by the copyright holder. The COPD Assessment Test (CAT) was administered at baseline, one week, and discharge.
Molecular Indicators
Peripheral venous blood samples were collected at baseline and at discharge. Serum was separated by centrifugation and stored at −80 °C until analysis. Serum concentrations of MUC5AC and MUC5B were quantified using commercially available enzyme-linked immunosorbent assay (ELISA) kits (MUC5AC ELISA kit, Cloud-Clone Corp., Houston, TX, USA; MUC5B ELISA kit, Cloud-Clone Corp., Houston, TX, USA) according to the manufacturers’ instructions. No sputum induction or sputum-based biomarker analysis was performed in this study.
Adverse Events
Events such as tachycardia, dyspnea, SpO2 decline, cough-induced symptoms, and device intolerance were recorded with details of onset, duration, and management.
Adherence Assessment
Daily completion rates were calculated. Nursing staff recorded patient engagement, independence in performing exercises, and reasons for withdrawal.
Statistical Analysis
All analyses were performed using SPSS 22.0. Continuous variables were tested for normality. Normally distributed data were expressed as mean ± standard deviation and compared between groups using independent-samples t-tests; non-normally distributed data were reported as median (interquartile range) and compared with the Mann–Whitney U-test. Categorical variables were summarized as frequency (percentage) and compared using the χ2-test or Fisher’s exact test as appropriate.
For longitudinal outcomes measured at baseline (T0), week 1 (T1), and discharge (T2), linear mixed-effects models with random intercepts for subjects were applied to assess the effects of group, time, and group × time interaction, with adjustment for baseline values and prespecified covariates (eg., age, sex, BMI, smoking index). Binary outcomes (eg., responder rate for sputum viscosity, CAT MCID achievement) were analyzed using log-binomial or Poisson regression with robust variance to estimate relative risk (RR) and 95% confidence intervals. A two-sided P < 0.05 was considered statistically significant. Given the retrospective design and absence of a formal sample size calculation, all analyses were conducted on an exploratory basis and should be interpreted accordingly.
Results
Baseline Characteristics
To ensure the reliability of comparisons, baseline demographic and clinical variables were examined between groups. There were no statistically significant differences in demographic characteristics, including age, sex distribution, body mass index, smoking history, smoking index, or disease duration (P > 0.05). Similarly, pulmonary function measures (FEV1, FEV1%pred, FEV1/FVC), sputum volume and viscosity, CAT scores, mMRC grades, and serum levels of MUC5AC and MUC5B were comparable (P > 0.05) (Table 1). These findings confirm good baseline equivalence, strengthening the validity of subsequent outcome comparisons.
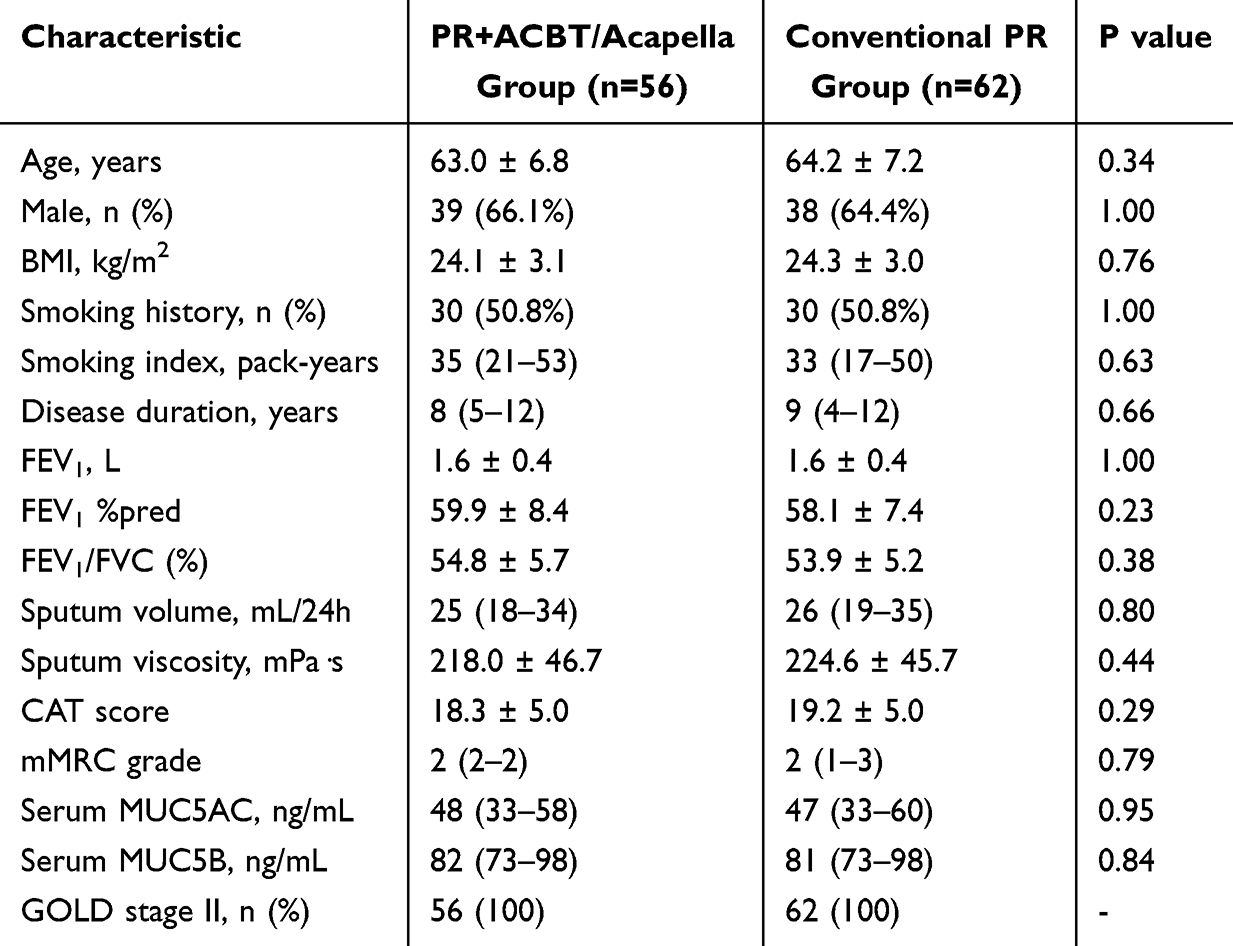 |
Table 1 Baseline Characteristics of the Study Population |
Intervention and Compliance
High adherence is crucial for evaluating the feasibility of a rehabilitation program. During hospitalization, patients in the PR+ACBT/OPEP group completed an average of 42.6 ± 8.3 training sessions, lasting 19.4 minutes per session, whereas the Conventional PR group completed 43.1 ± 7.9 sessions of shorter duration (9.8 minutes; P < 0.001). Both groups demonstrated high compliance, with 92.9% (52/56) of intervention patients and 79.0% (49/62) of controls achieving a completion rate ≥80% (P = 0.04).
Among intervention patients, the final OPEP resistance settings were level 1 in 21 (37.5%), level 2 in 27 (48.2%), and level 3 in 8 (14.3%). All levels were well tolerated, and no participant discontinued due to device-related discomfort. A minority of patients reported interruptions or reduced training intensity, most commonly from fatigue or dyspnea, with similar rates in both groups (interrupted training: 8.5% vs. 6.8%, P = 0.74; reduced intensity/shortened duration: 10.2% vs. 5.1%, P = 0.30; early discontinuation: 3.4% vs. 5.1%, P = 0.65) (Table 2). Taken together, these results demonstrate that the intervention program was well tolerated, feasible across different resistance levels, and associated with high patient adherence.
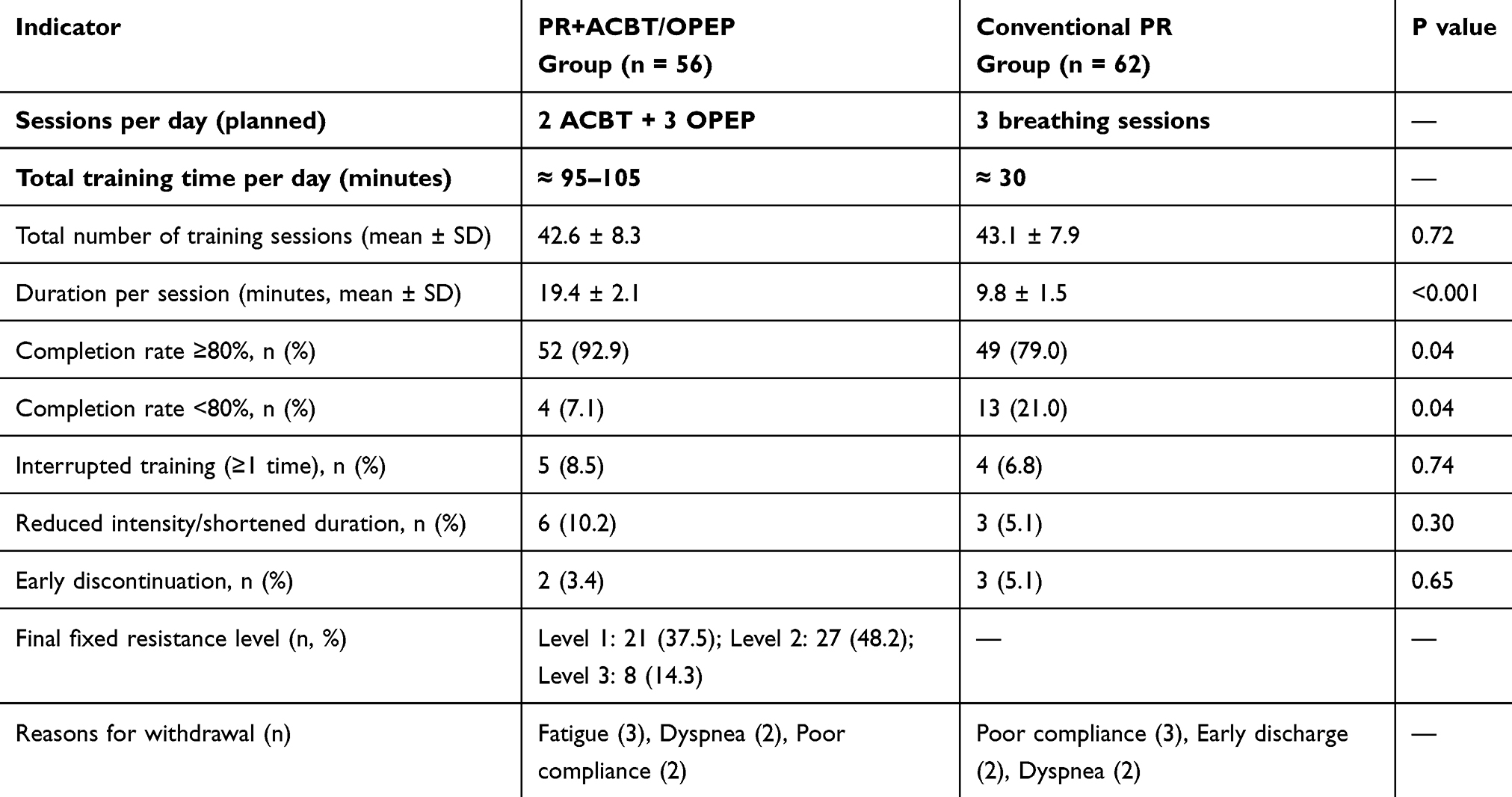 |
Table 2 Intervention Implementation and Compliance (n=118) |
Changes in Sputum Parameters Over Time
As mucus hypersecretion is a key clinical concern in COPD, sputum characteristics were tracked longitudinally. At baseline (T0), all included patients provided sufficient sputum samples for analysis. At T1 and T2, a small number of patients in both groups were unable to produce measurable sputum due to clinical improvement or minimal sputum production. These missing values were handled using linear mixed-effects models, which allow inclusion of all available data without requiring complete observations at every time point.
Sputum volume and viscosity were comparable between groups at baseline (all P > 0.05). After one week of intervention, patients in the PR+ACBT/OPEP group showed significantly lower sputum volume and viscosity than those receiving conventional PR. By discharge, reductions in sputum volume were substantially greater in the PR+ACBT/OPEP group, with a significant group × time interaction confirmed by linear mixed-effects modeling (Table 3 and Figure 2A). Relative sputum volume reduction was markedly higher in the intervention group compared with controls. Similarly, sputum viscosity declined more prominently in the PR+ACBT/OPEP group over time, whereas only modest changes were observed in the Conventional PR group (Table 3 and Figure 2B). Group × time interaction analysis demonstrated a significant treatment effect. At discharge, relative viscosity reduction was considerably greater in the PR+ACBT/OPEP group than in controls. Using a predefined threshold of ≥20% viscosity reduction, a significantly higher proportion of patients in the PR+ACBT/OPEP group achieved responder status compared with the Conventional PR group (Table 3). Overall, incorporation of ACBT and OPEP into pulmonary rehabilitation was associated with greater improvements in sputum volume and viscosity.
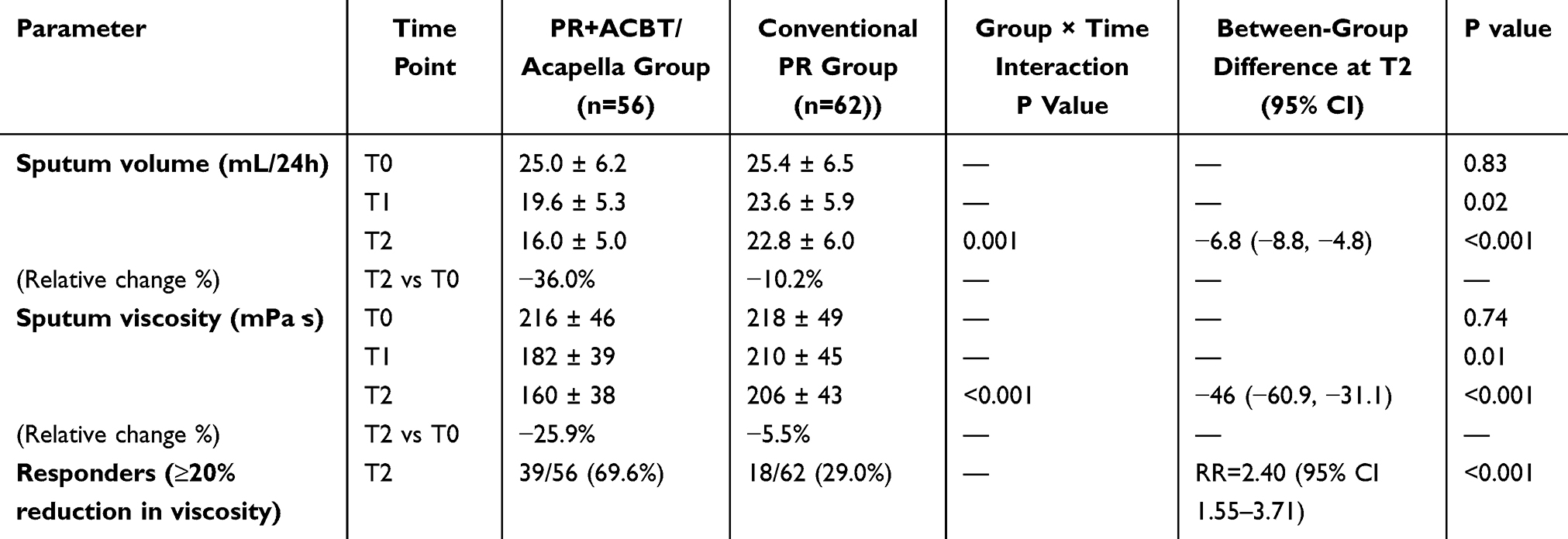 |
Table 3 Changes in Sputum Characteristics Over Time (n=118) |
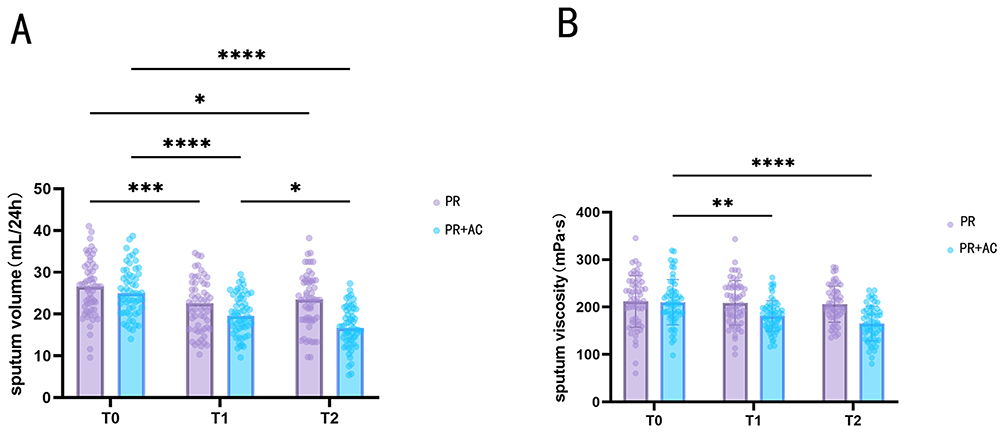 |
Figure 2 Changes in sputum characteristics over time between the PR+ACBT/OPEP and Conventional PR groups. (A) Daily sputum volume (mL/24 h) and (B) sputum viscosity (mPa·s) measured at baseline (T0), after 1 week of intervention (T1), and at discharge (T2). The primary comparison of interest is the between-group difference at discharge (T2). Each dot represents an individual patient, and horizontal bars indicate group means ± SD. Statistical analysis was performed using two-way ANOVA with group × time interaction, followed by post hoc tests. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. PR: conventional pulmonary rehabilitation (basic breathing exercises including pursed-lip breathing, diaphragmatic breathing, and effective coughing). PR+ACBT/OPEP: pulmonary rehabilitation combined with airway clearance techniques (ACBT and OPEP). |
Changes in Mucin Biomarkers (MUC5AC/MUC5B) Over Time
To explore potential biological mechanisms underlying clinical changes, mucin biomarkers were assessed. At baseline (T0), there were no significant differences between groups (P > 0.05) (Table 4). By discharge (T2), serum MUC5AC concentrations had decreased significantly in the PR+ACBT/OPEP group (38.2 ± 9.4 ng/mg protein) compared with controls (46.1 ± 10.1 ng/mg protein), with a mean difference of −7.9 ng/mg (95% CI −11.5 to −4.3; P < 0.001). In relative terms, this represented a 21.3% reduction in the PR+ACBT/OPEP group versus only 3.8% in controls (Figure 3A). Conversely, MUC5B increased in the PR+ACBT/OPEP group (82.1 ± 14.6 to 90.3 ± 13.9 ng/mg protein), whereas levels remained stable in controls (82.4 ± 15.0 ng/mg protein at T2). The between-group difference was +7.9 ng/mg (95% CI 3.5–12.3; P = 0.001) (Figure 3B). Exploratory analysis of the MUC5AC/MUC5B ratio revealed a significant decrease in the PR+ACBT/OPEP group (0.59 ± 0.11 to 0.42 ± 0.10), while values in the Conventional PR group remained stable (0.59 ± 0.12 to 0.56 ± 0.11). At T2, the between-group difference was −0.14 (95% CI −0.18 to −0.10; P < 0.001) (Figure 3C). These biomarker results suggest that the intervention not only reduced pathological overproduction of MUC5AC but also promoted relative increases in MUC5B, leading to a favorable shift in mucin balance consistent with improved mucus clearance.
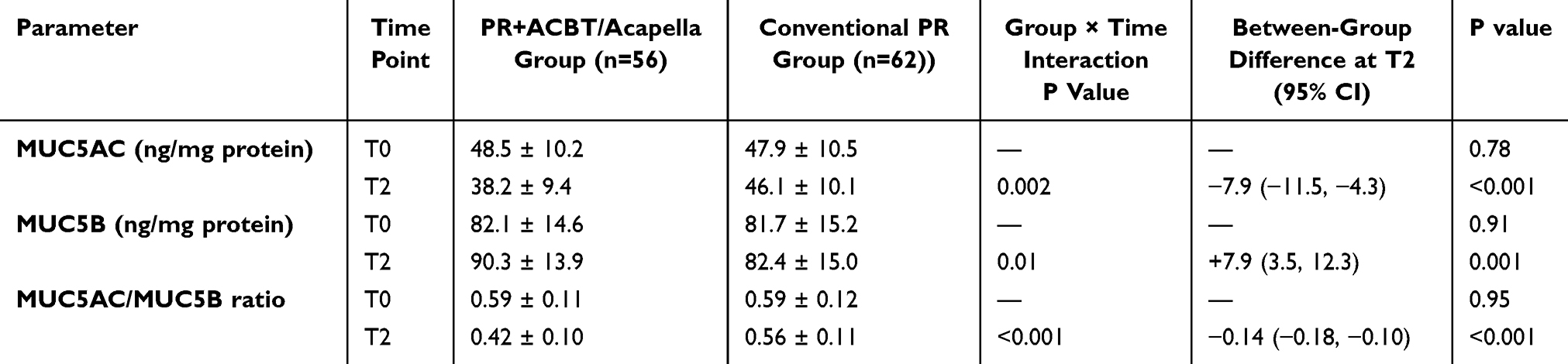 |
Table 4 Changes in Sputum Mucin Biomarkers Between Groups |
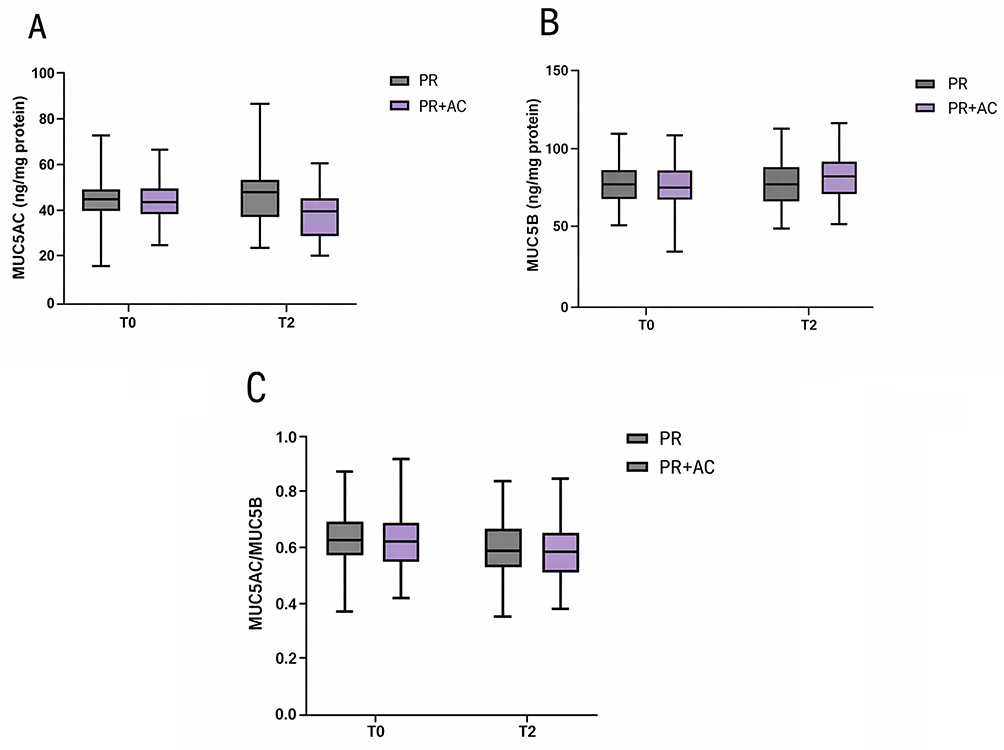 |
Figure 3 Changes in sputum mucin biomarkers from baseline (T0) to discharge (T2). (A-C) Sputum MUC5AC (A) and MUC5B (B) concentrations (ng/mg protein) and MUC5AC/MUC5B ratio (C) in the intervention and Conventional PR groups. Data are presented as box-and-whisker plots (median, interquartile range, and full range). Group comparisons were performed at each time point. P<0.05, P<0.01, P<0.001, P<0.0001. PR: conventional pulmonary rehabilitation (basic breathing exercises: pursed-lip, diaphragmatic breathing, effective cough). PR+AC: PR plus airway clearance techniques (ACBT and OPEP). |
Comparison of Pulmonary Function Improvement
Pulmonary function parameters were comparable between the PR+ACBT/OPEP and Conventional PR groups at baseline, including FEV1, FEV1%pred, FVC, FEV1/FVC, and small-airway indices (MMEF and MEF25–75%) (Table 5 and Figure 4A–F). After one week of intervention, early functional improvements were observed in the PR+ACBT/OPEP group. Small-airway indices showed significant between-group differences, with higher FEV1%pred, MMEF, and MEF25–75% compared with the Conventional PR group. In contrast, changes in FEV1 (L), FVC, and FEV1/FVC were modest and did not differ significantly between groups at this time point. By discharge, pulmonary function improvements became more evident. Patients receiving PR combined with ACBT and OPEP demonstrated significantly greater increases in FEV1 and FEV1%pred than controls, supported by significant group × time interaction effects. Improvements in FVC and FEV1/FVC remained limited and did not reach statistical significance between groups. Notably, small-airway function showed the most consistent and robust response to the intervention. At discharge, both MMEF and MEF25–75% were significantly higher in the PR+ACBT/OPEP group compared with the Conventional PR group, with sustained group × time interaction effects indicating a treatment-related benefit over time (Table 5, Figure 4E and F). Overall, these findings indicate that incorporation of ACBT and OPEP into pulmonary rehabilitation preferentially improved small-airway function and was associated with moderate but clinically meaningful gains in FEV1 and FEV1%pred by discharge.
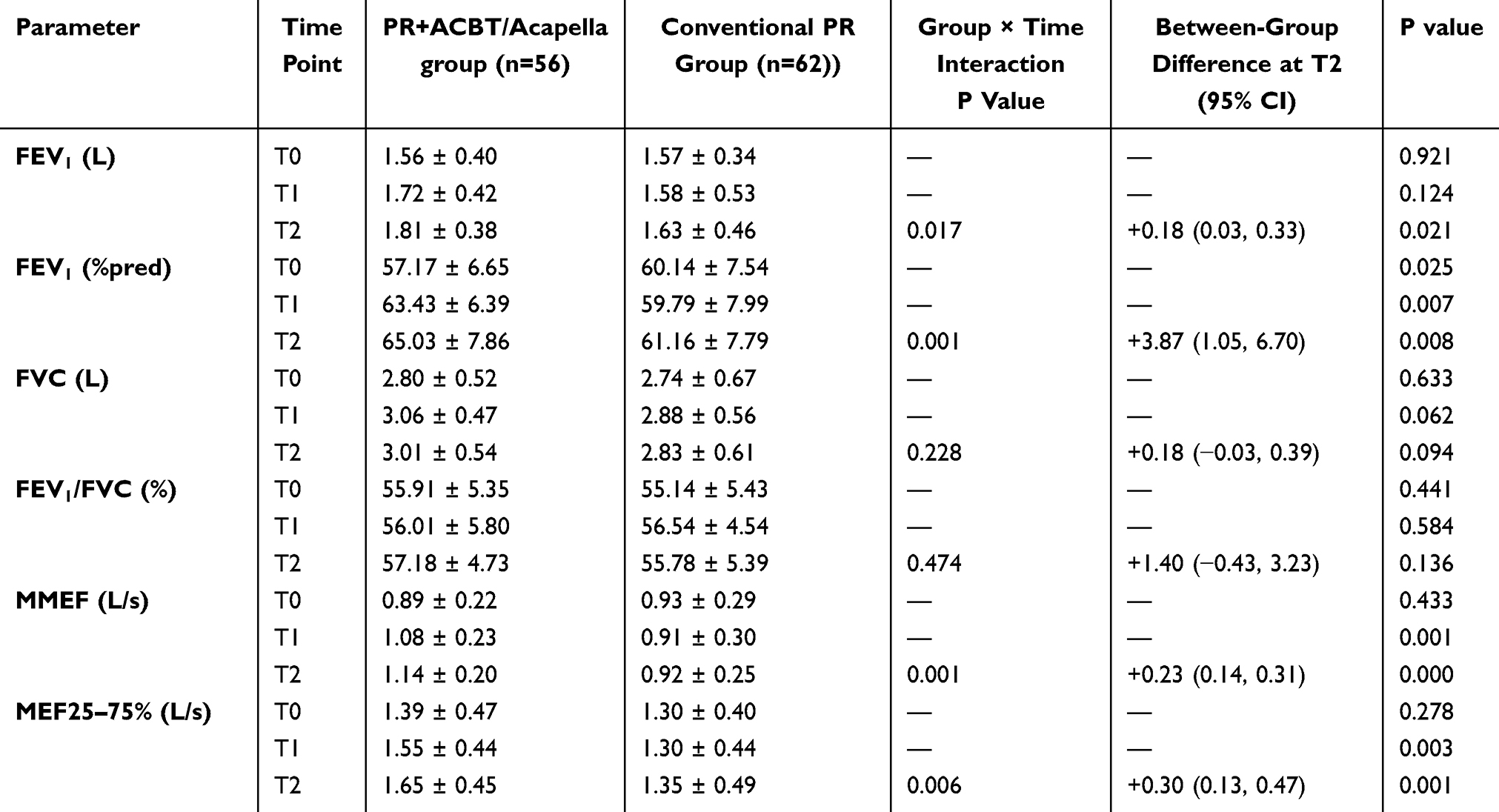 |
Table 5 Changes in Pulmonary Function Parameters Over Time |
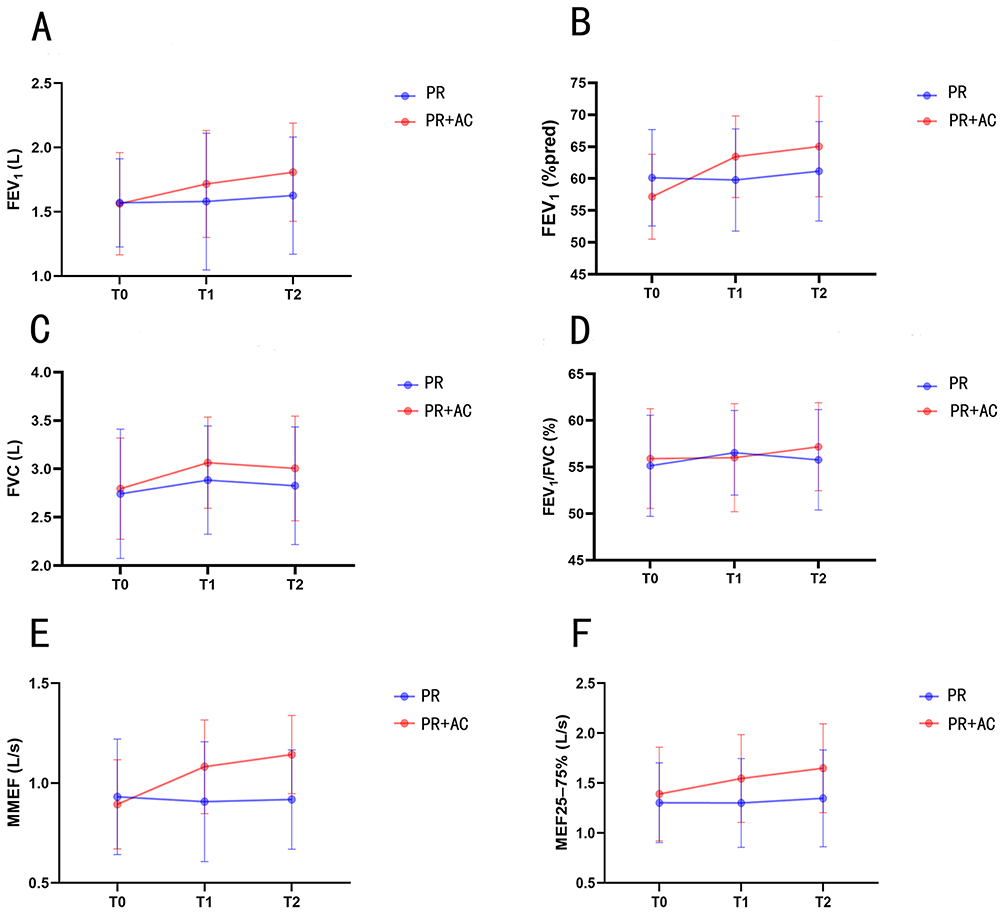 |
Figure 4 Changes in pulmonary function parameters over time between the PR+ACBT/OPEP and Conventional PR groups. (A) FEV1 (L), (B) FEV1 (% predicted), (C) FVC (L), (D) FEV1/FVC (%), (E) maximal mid-expiratory flow (MMEF, L/s), and (F) maximal expiratory flow between 25% and 75% of FVC (MEF25–75%, L/s), measured at baseline (T0), after 1 week of intervention (T1), and at discharge (T2). The primary comparison of interest is the between-group difference at discharge (T2), particularly for small-airway indices. Data are expressed as mean ± SD. PR: conventional pulmonary rehabilitation (basic breathing exercises including pursed-lip breathing, diaphragmatic breathing, and effective coughing). PR+ACBT/OPEP: pulmonary rehabilitation combined with airway clearance techniques (ACBT and OPEP). |
Comparison of Symptoms and Quality of Life
To evaluate patient-centered benefits, changes in symptom burden and quality of life were assessed using the CAT and mMRC scores. At baseline (T0), no significant differences were observed between groups (P > 0.05) (Table 6). By week one (T1), the PR+ACBT/OPEP group showed a significantly lower mean CAT score compared with controls (15.9 ± 4.1 vs. 18.2 ± 4.4; P = 0.01). At discharge (T2), CAT scores further declined to 14.0 ± 3.9 in the PR+ACBT/OPEP group, while controls remained higher at 17.6 ± 4.3. The between-group difference was −3.6 points (95% CI −5.0 to −2.2; P < 0.001), with a significant group × time interaction. Importantly, 67.9% (38/56) of intervention patients achieved the minimal clinically important difference (MCID; ≥2-point reduction), compared with 24.2% (15/62) of controls (RR = 2.81, 95% CI 1.71–4.62; P < 0.001) (Figure 5). Similarly, mMRC grades improved significantly in the PR+ACBT/OPEP group, decreasing from a baseline median of 2 (IQR 2–3) to 1 (IQR 1–2) at discharge, while the Conventional PR group remained unchanged at 2 (IQR 2–3). The difference between groups at T2 was statistically significant (P = 0.002). Together, these results demonstrate that structured airway clearance within PR not only improved physiological outcomes but also translated into meaningful reductions in symptom burden and enhanced quality of life for patients.
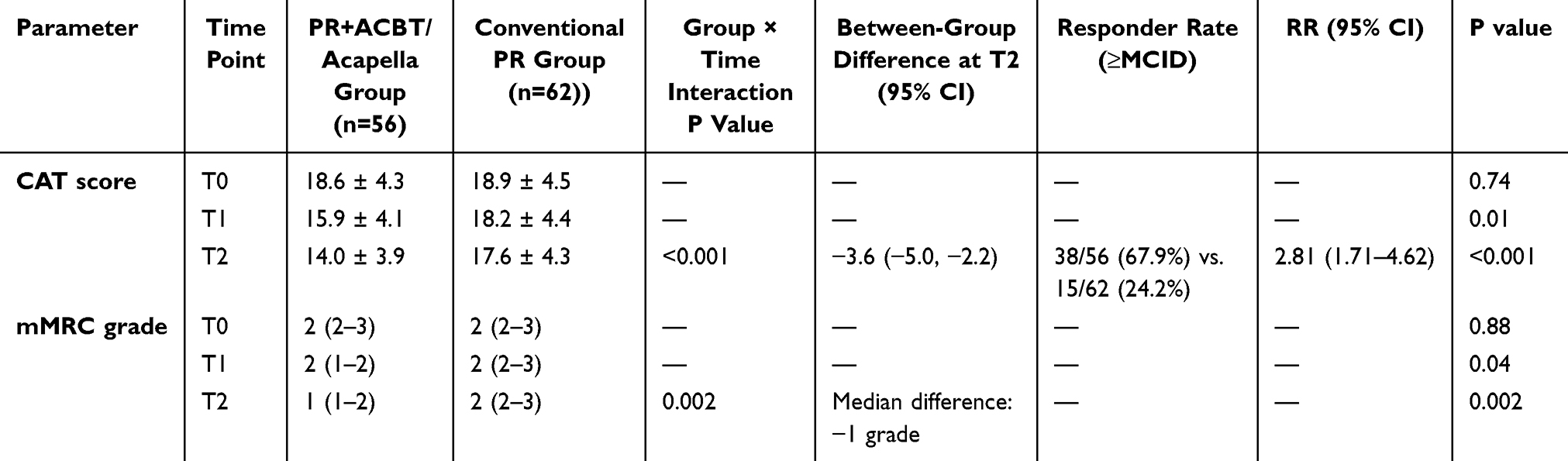 |
Table 6 Changes in CAT and mMRC Scores Over Time and Responder Rates |
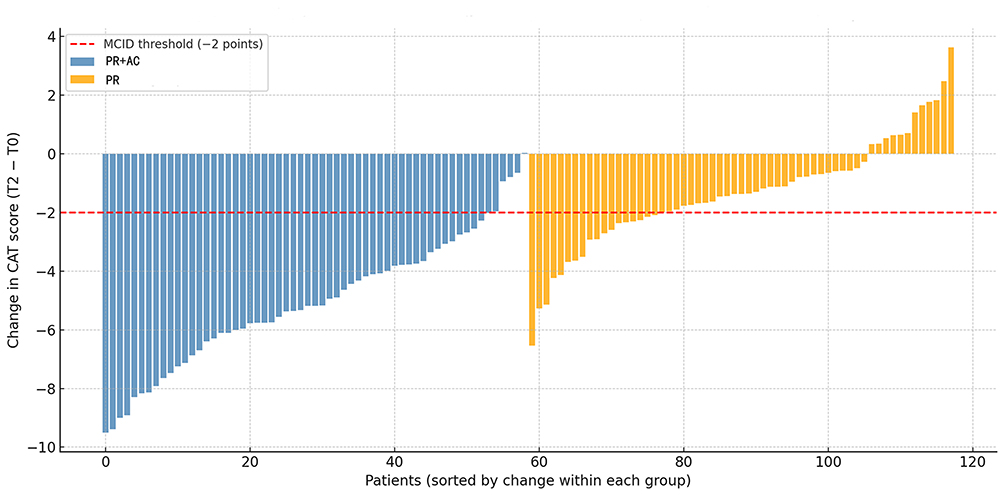 |
Figure 5 Individual changes in CAT score from baseline (T0) to discharge (T2). Each bar represents an individual patient, ranked by the magnitude of score change within each group. Blue bars indicate patients in the PR+ACBT/OPEP group, and Orange bars indicate those in the Conventional PR group. Negative values reflect improvement (reduction in CAT score). The dashed red horizontal line denotes the minimal clinically important difference (MCID) threshold of −2 points. A greater proportion of patients in the PR+ACBT/OPEP group achieved a clinically meaningful improvement compared with controls. PR: conventional pulmonary rehabilitation (basic breathing exercises: pursed-lip, diaphragmatic breathing, effective cough). PR+AC: PR plus airway clearance techniques (ACBT and OPEP). |
Discussion
This retrospective cohort study evaluated whether integrating airway clearance techniques (ACBT and OPEP) into pulmonary rehabilitation improves mucus clearance and clinical outcomes in COPD patients with chronic sputum hypersecretion. The findings directly correspond to the study objectives and are consistent with the results presented. Specifically, the intervention was associated with greater reductions in sputum volume and viscosity, improvements in pulmonary function particularly small-airway indices and clinically meaningful reductions in symptom burden compared with conventional pulmonary rehabilitation alone. These outcomes support the relevance of airway clearance–focused rehabilitation for this specific COPD phenotype, without extending conclusions beyond the observed data. Taken together, these findings provide real-world evidence suggesting that targeted airway clearance interventions can break the cycle of mucus retention, airway obstruction, and worsening symptoms, ultimately leading to better functional capacity and quality of life in this challenging COPD phenotype.18
The present findings are consistent with and further extend the existing body of evidence supporting the role of pulmonary rehabilitation in the management of COPD. A substantial number of studies have consistently demonstrated that pulmonary rehabilitation leads to significant improvements in exercise tolerance, reductions in dyspnea, and enhancements in health-related quality of life.19 In particular, prior work by Svenningsen et al showed that a three- to four-week program of daily oscillatory positive expiratory pressure therapy resulted in noticeably easier sputum expectoration, as assessed through patient-reported questionnaires. In addition, their study reported modest yet clinically meaningful improvements in forced vital capacity, six-minute walk distance, and St George’s Respiratory Questionnaire scores in COPD patients with sputum production, underscoring the multifaceted benefits of this intervention.19 Similarly, a recent randomized controlled trial13 assessed three months of OPEP device use in combination with standard care, including ACBT, in stable COPD patients with chronic phlegm production and demonstrated clinical benefit. However, clinical evidence specifically targeting patients with persistent mucus hypersecretion has remained limited. Prior studies suggested that OPEP improve mucus clearance and alleviate respiratory symptoms,2,4,20 but many of these trials lacked integration into a structured PR program and were primarily conducted in stable outpatients. By contrast, our retrospective analysis indicates that embedding ACBT and OPEP into a PR framework not only enhances mucus clearance but also translates into improvements in pulmonary function and symptom burden. Importantly, this study focused on a hospitalized population, which is more representative of patients with advanced disease and frequent exacerbations, thereby providing clinically relevant observations, though prospective studies are needed to confirm these findings.
The mechanisms underlying the observed improvements are likely multifactorial. ACBT facilitates mobilization of airway secretions from peripheral to central airways through controlled breathing, thoracic expansion, and forced expiration techniques, while OPEP provides expiratory resistance and oscillatory vibrations that reduce mucus viscosity and enhance expectoration. Together, these interventions promote airway patency and more homogeneous ventilation, consistent with the greater reductions in sputum volume and viscosity observed in the intervention group.21,22
Improvements in small-airway function indices (MMEF and MEF25–75%) provide physiological support for enhanced mucus clearance, as these measures are sensitive to peripheral airway obstruction. Reduced mucus plugging may lessen air-trapping and dynamic hyperinflation, contributing to improved FEV1,19,23,24 and reduced dyspnea. Importantly, these findings are most applicable to COPD patients with chronic sputum hypersecretion, typically associated with the chronic bronchitis phenotype. Other COPD phenotypes, such as emphysema-predominant disease or frequent exacerbators without prominent mucus production, may respond differently to airway clearance–focused rehabilitation, and this should be considered when interpreting the clinical applicability of the results.
Patients with chronic sputum hypersecretion typically experience a heavier symptom burden, more frequent exacerbations, and poorer long-term prognosis. Our findings suggest that structured airway clearance strategies, when systematically integrated into PR, may improve symptoms, enhance functional outcomes, and potentially reduce exacerbation risk and hospitalizations.25–27 From a healthcare systems perspective, such approaches may also offer cost-effective solutions for reducing COPD-related burden, particularly in settings where access to comprehensive PR remains limited. The simplicity, safety, and feasibility of both ACBT and OPEP further support their integration into clinical practice, even in resource-constrained environments.28
While pulmonary rehabilitation and airway clearance techniques have been evaluated previously in COPD, the present findings should be viewed primarily as confirmatory rather than conceptually novel. The added value of this study lies in providing real-world, inpatient observational data comparing ACBT combined with OPEP versus conventional rehabilitation within a structured program. By examining both clinical outcomes and mucus-related measures in routine practice, this study contributes practical evidence to inform rehabilitation strategies for COPD patients with chronic sputum hypersecretion.
Despite these encouraging results, several limitations must be acknowledged. First, this was a single-center, retrospective study with a modest sample size and no formal sample size justification, limiting statistical power for definitive comparisons. As such, all analyses should be interpreted as exploratory. Second, although multivariable and mixed-effects models were used to adjust for measured confounders, residual confounding inherent to observational designs cannot be excluded. These limitations restrict causal inference and highlight the need for prospective, adequately powered studies to confirm the observed associations. Larger multicenter trials are needed to confirm the generalizability of these results. Second, follow-up was restricted to the inpatient period, preventing assessment of long-term outcomes such as exacerbation frequency, readmission rates, or mortality. Third, although mucin biomarkers were evaluated, additional mechanistic endpoints, including inflammatory mediators, microbiome composition, and more detailed molecular profiles, were not investigated. Future studies incorporating these measures could provide deeper insights into the biological pathways by which airway clearance exerts clinical benefits. Finally, while adherence during hospitalization was high, long-term real-world adherence to PR-integrated airway clearance techniques remains uncertain and deserves further exploration. In addition, the retrospective design introduces inherent limitations, including possible selection bias and unmeasured confounding, which restrict causal inference.
Overall, these study provide incremental, practice-oriented evidence supporting the integration of airway clearance techniques into pulmonary rehabilitation for COPD patients with chronic sputum hypersecretion and may help inform the design of future prospective studies.
Conclusion
In summary, this retrospective, single-center study suggests that pulmonary rehabilitation incorporating airway clearance techniques (ACBT and OPEP) may be associated with short-term improvements in sputum characteristics, selected small-airway pulmonary function parameters, and reductions in COPD-related health status impact among hospitalized patients with chronic sputum hypersecretion. The observed reductions in sputum volume and viscosity, along with improvements in small-airway indices, are consistent with previously reported physiological effects of airway clearance strategies, while providing additional real-world inpatient data. Although these findings align with existing literature on airway clearance in COPD, the present study contributes observational evidence within a structured rehabilitation framework and integrates both clinical and biomarker assessments. The results should be interpreted as exploratory and hypothesis-generating rather than as proof of efficacy. Future multicenter, prospective, and randomized studies with longer follow-up are required to confirm these associations, determine their durability, and evaluate potential effects on exacerbation risk, hospitalization frequency, and long-term disease progression.
Patient Data Statement
All patient case data on this study are confidential.
Abbreviations
ACBT, Active Cycle of Breathing Technique; CAT, COPD Assessment Test; CI, Confidence Interval; COPD, Chronic Obstructive Pulmonary Disease; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; IQR, Interquartile Range; LMM, Linear Mixed-Effects Model; MCID, Minimal Clinically Important Difference; MEF25–75%, Maximum Expiratory Flow between 25% and 75% of FVC; MMEF, Maximal Mid-Expiratory Flow; mMRC, Modified Medical Research Council (dyspnea scale); MUC5AC, Mucin 5AC; MUC5B, Mucin 5B; OPEP, Oscillatory Positive Expiratory Pressure Therapy; PR, Pulmonary Rehabilitation; RCT, Randomized Controlled Trial; RR, Relative Risk.
Data Sharing Statement
All data generated during the study is presented in the manuscript. Raw data files are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval for our study was granted by The Medical Committee of the First Affiliated Hospital of Hainan Medical University (2024-KYL-090). The trial was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Joint Project of Health and Medical Science and Technology Innovation in Hainan Province (WSJK2024QN036) and High-level Talents Program of the Natural Science Foundation of Hainan Province (823RC580).
Disclosure
The authors declare that there are no competing interests.
References
1. Fazleen A, Wilkinson T. Early COPD: current evidence for diagnosis and management. Ther Adv Respir Dis. 2020;141753466620942128.
2. Shah BK, Singh B. Mucus hypersecretion in chronic obstructive pulmonary disease and its treatment. Mediator Inflamm. 2023;2023:8840594.
3. Huang X, Guan W, Xiang B, et al. MUC5B regulates goblet cell differentiation and reduces inflammation in a murine COPD model. Respir Res. 2022;23(1):11. doi:10.1186/s12931-021-01920-8
4. Radicioni G, Ceppe A, Ford AA, et al. Airway mucin MUC5AC and MUC5B concentrations and the initiation and progression of chronic obstructive pulmonary disease: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2021;9(11):1241–16. doi:10.1016/S2213-2600(21)00079-5
5. Guo P, Li R, Piao TH, et al. Pathological mechanism and targeted drugs of COPD. Int J Chron Obstruct Pulmon Dis. 2022;171565–171575.
6. Negewo NA, Gibson PG, McDonald VM. COPD and its comorbidities: impact, measurement and mechanisms. Respirology. 2015;20(8):1160–1171. doi:10.1111/resp.12642
7. Vogelmeier CF, Román-Rodríguez M, Singh D, et al. Goals of COPD treatment: focus on symptoms and exacerbations. Respir Med. 2020;166:105938.
8. Donohue JF, Rheault T, MacDonald-Berko M, et al. Ensifentrine as a novel, inhaled treatment for patients with COPD. Int J Chron Obstruct Pulm Dis. 2023;18:1611–181622.
9. Zeng Y, Jiang F, Chen Y, et al. Exercise assessments and trainings of pulmonary rehabilitation in COPD: a literature review. Int J Chron Obstruct Pulmon Dis. 2018;13:2013–2023.
10. Hansen H, Bieler T, Beyer N, et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: a randomised multicentre trial. Thorax. 2020;75(5):413–421. doi:10.1136/thoraxjnl-2019-214246
11. Lamberton CE, Mosher CL. Review of the evidence for pulmonary rehabilitation in COPD: clinical benefits and cost-effectiveness. Respir Care. 2024;69(6):686–696. doi:10.4187/respcare.11541
12. Su MW, Ge LK, Yao XY, et al. Interoceptive abnormalities in COPD patients: their predictive role in anxiety and acute exacerbation of COPD. Medicine. 2025;104(27):e43023. doi:10.1097/MD.0000000000043023
13. Alghamdi SM, Alsulayyim AS, Alasmari AM. Oscillatory positive expiratory pressure therapy in COPD (O-COPD): a randomised controlled trial. Thorax. 2023;78(2):136–143. doi:10.1136/thorax-2022-219077
14. Alghamdi SM, Barker RE, Alsulayyim ASS. Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: a systematic review and meta-analysis. Thorax. 2020;75(10):855–863. doi:10.1136/thoraxjnl-2019-214360
15. Tse J, Wada K, Wang Y, et al. Impact of oscillating positive expiratory pressure device use on post-discharge hospitalizations: a retrospective cohort study comparing patients with copd or chronic bronchitis using the aerobika(®) and Acapella(®) devices. Toxicology. 2020;441:152527–152538. doi:10.1016/j.tox.2020.152527
16. Alghamdi SM, Alzahrani A, Alshahrani YM. Perception and clinical practice regarding mucus clearance devices with chronic obstructive pulmonary disease: a cross-sectional study of healthcare providers in Saudi Arabia. BMJ open. 2023;13(9):e074849. doi:10.1136/bmjopen-2023-074849
17. Morgan SE, Mosakowski S, Giles BL, et al. Variability in expiratory flow requirements among oscillatory positive expiratory pressure. Can J Respir Ther. 2019;567.
18. Shen M, Li Y, Ding X, et al. Effect of active cycle of breathing techniques in patients with chronic obstructive pulmonary disease: a systematic review of intervention. Eur J Phys Rehabil Med. 2020;56(5):625–632. doi:10.23736/S1973-9087.20.06144-4
19. Svenningsen S, Paulin GA, Sheikh K, et al. oscillatory positive expiratory pressure in chronic obstructive pulmonary disease. COPD. 2016;13(1):66–74. doi:10.3109/15412555.2015.1043523
20. Xia XX, Li CX, Guo HR. Association between oral microbiome diversity and chronic obstructive pulmonary disease in the US population. J Transl Med. 2025;23(1):557. doi:10.1186/s12967-025-06553-9
21. Demchuk AM, Chatburn RL. Performance characteristics of positive expiratory pressure devices. Respir Care. 2021;66(3):482–493. doi:10.4187/respcare.08150
22. McIlwaine M, Button B, Nevitt SJ. Positive expiratory pressure physiotherapy for airway clearance in people with cystic fibrosis. Cochrane Database Syst Rev. 2019;2019(11). doi:10.1002/14651858.CD003147.pub5
23. Svenningsen S, Guo F, McCormack DG, et al. Noncystic fibrosis bronchiectasis: regional abnormalities and response to airway clearance therapy using pulmonary functional magnetic resonance imaging. Acad Radiol. 2017;24(1):4–12. doi:10.1016/j.acra.2016.08.021
24. Sahardin SN, Jailaini MFM, Abeed NNN, et al. Impact of Aerobika(®) oscillating positive expiratory pressure in improving small airway resistance, lung function, symptoms and exercise capacity in chronic obstructive pulmonary disease. Front Med Lausanne. 2023;10:1202380.
25. Kesimer M, Ford AA, Ceppe A, et al. Airway mucin concentration as a marker of chronic bronchitis. N Engl J Med. 2017;377(10):911–922. doi:10.1056/NEJMoa1701632
26. Khoudigian-Sinani S, Kowal S, Suggett JA, et al. Cost-effectiveness of the Aerobika* oscillating positive expiratory pressure device in the management of COPD exacerbations. Int J Chron Obstruct Pulmon Dis. 2017;12:3065–123073.
27. Xia X, Xia K, Yao X. Factors influencing compliance with pulmonary rehabilitation in patients with stable COPD: a cross sectional study. Int J Chron Obstruct Pulmon Dis. 2025;20:895–20904.
28. Lahham A, Holland AE. The need for expanding pulmonary rehabilitation services. Life. 2021;11(11):1236. doi:10.3390/life11111236
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Listen to Me! – A Mixed-Methods Study of Thoughts and Attitudes Towards Participation in Pulmonary Telerehabilitation Among People with Severe and Very Severe COPD Who Declined Participation in Pulmonary Rehabilitation
Skibdal KM, Emme C, Hansen H
Patient Preference and Adherence 2022, 16:2781-2798
Published Date: 18 October 2022
Effect of Singing on Symptoms in Stable COPD: A Systematic Review and Meta-Analysis
Fang X, Qiao Z, Yu X, Tian R, Liu K, Han W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2893-2904
Published Date: 14 November 2022
Exploring the Presence of Implicit Bias Amongst Healthcare Professionals Who Refer Individuals Living with COPD to Pulmonary Rehabilitation with a Specific Focus Upon Smoking and Exercise
Barradell AC, Robertson N, Houchen-Wolloff L, Singh SJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1287-1299
Published Date: 21 June 2023
Can Blood Biomarkers Be Used to Assess Oxidative Stress in COPD Patients After Pulmonary Rehabilitation
Beykumül A, Ersoy Y, Gülbaş G, Neselioglu S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2179-2186
Published Date: 5 October 2023
Advocating for Action: Exploring the Potential of Virtual Reality in Breathing Exercise – A Review of The Clinical Applications
Alhammad SA
Patient Preference and Adherence 2024, 18:695-707
Published Date: 19 March 2024