Back to Journals » Patient Preference and Adherence » Volume 16
Listen to Me! – A Mixed-Methods Study of Thoughts and Attitudes Towards Participation in Pulmonary Telerehabilitation Among People with Severe and Very Severe COPD Who Declined Participation in Pulmonary Rehabilitation
Authors Skibdal KM, Emme C ![]() , Hansen H
, Hansen H ![]()
Received 1 July 2022
Accepted for publication 5 October 2022
Published 18 October 2022 Volume 2022:16 Pages 2781—2798
DOI https://doi.org/10.2147/PPA.S380832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Kira Marie Skibdal,1 Christina Emme,2 Henrik Hansen3
1Department of Physical and Occupational Therapy, University Hospital Amager-Hvidovre Hospital, Hvidovre, Denmark; 2Department of Quality and Education, University Hospital Bispebjerg-Frederiksberg, Copenhagen, Denmark; 3Respiratory Research Unit and Department of Respiratory Medicine, University Hospital Amager Hvidovre Hospital, Hvidovre, Denmark
Correspondence: Henrik Hansen, Email [email protected]
Introduction: Pulmonary rehabilitation (PR) is a key standard treatment for people with chronic obstructive pulmonary disease (COPD) with documented effect on symptom relief, improved physical function, and quality of life. However, referral, uptake and adherence rates remain low. Pulmonary telerehabilitation (PTR) is a safe and effective alternative to conventional PR. This study explores associations, thoughts and attitudes towards PTR in patients with COPD who decline referral to outpatient hospital-based routine PR.
Methods: A mixed-methods study with integration of survey data (n=84) and semi-structured interviews (n=9).
Results: We found a significant association between belief of effect of PTR and willingness to participate. Increasing age was significantly associated with reduced odds of daily use of central processing unit (CPU) or tablet. One-third of the participants were undecided about potential participation in PTR. Qualitative findings highlight that participants perceived participating in PTR as more convenient and had preferences for individualized, supervised, and monitored rehabilitation.
Conclusion: Those willing to participate in a PTR program believed in the benefits, were comfortable with technological devices, had preferences for exercising at home, and saw opportunities in the social setting. Future PTR programs should include monitoring, preferably managed by a familiar health care professional (HCP).
Keywords: COPD, pulmonary rehabilitation, pulmonary telerehabilitation, Theoretical Domains Framework
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by shortness of breath, functional limitations, and reduced mental capacity.1 The illness is progressive and a leading cause of morbidity and mortality.2 COPD patients experience twice as many hospitalizations as the rest of the population and COPD is the third leading cause of death worldwide.2–4
Pulmonary rehabilitation (PR) has a documented effect on reducing dyspnea, and on improving activity levels, walking distance, and quality of life (QoL) in people with COPD.5–7 Further, PR reduces hospitalizations.6 PR programs are delivered both as hospital- and community-based programs, where patients attend supervised exercise at weekly basis to achieve optimal benefits. However, referral to and participation in PR is very low and drop-out rates are high, especially in the target population in this study, consisting of patients with severe and very severe COPD. Thus, 55% of the patients with severe and very severe COPD, decline participation.8,9 Barriers such as transportation difficulties, distance to the community and hospital settings, lack of physical and mental resources are reported as reasons for not attending PR.10,11
To eliminate specifically the transportation barriers, pulmonary rehabilitation can be offered as pulmonary telerehabilitation (PTR), which is home-based supervised rehabilitation through an Information and Communication Technology solution (ICT) e.g. tablets and smartphones.12 Several studies comparing PR to PTR have found that COPD patients attending PTR achieve the same effects on walking capacity, respiratory symptoms, QoL, physical capacity, and muscle strength as those attending PR.9,13–15 Only one study which compared supervised PR with home-based exercise with weekly telephone follow-up did not find the same improvement in walking capacity.16 Furthermore, PTR is a safe alternative to PR and reduces the risk of hospitalization when compared with usual care.17
An Australian survey with patients attending PR found that willingness to participate in PTR was associated with regular use of a computer or tablet.11 In addition, the participants who self-rated their technology skills as good were significantly younger and had a higher FEV1 than those who were not willing to participate in PTR.11 A qualitative study has investigated the patient perspective among patients with COPD who have undergone PTR and found that PTR had a positive impact on physical fitness, breathing and mood. Furthermore, the participants valued the flexibility and the convenience of the programme.18 These findings, however, do not include the thoughts and perspective of the proportion of patients who decline participation in outpatient PR programs, and little is known about the preferences for PTR among PR non-attenders. Therefore, the present study focuses specifically on this group. Thoughts, experience, and perspectives of PTR in this specific group is key in order to design and deliver PTR to a wider range of patients with COPD, particularly if PTR is to be considered as an extended offer specifically to those who live remotely and to those who lack energy and resources to join a conventional outpatient PR program. The perspective from the non-attenders can help clinicians design individualized flexible rehabilitation programs and potentially promote referral, uptake, adherence, and completion rates in PTR programs. The healthcare professionals’ (HCP) perspective towards delivering PTR, including barriers and enablers, has been explored in a qualitative study using the Theoretical Domains Framework (TDF).19,20 Especially attention towards involvement of the HCP in the decision process and sufficient education and skill training is essential to support the implementation of PTR in clinical practice.21–23 Lewis et al examined the feasibility of delivering PTR to patients with chronic respiratory disease during the COVID-19 pandemic and both healthcare professionals and patients found it acceptable and feasible.24
To our knowledge, no previous studies have investigated how patients with COPD who decline PR perceive participating in PTR. Therefore, this study aimed to explore associations, thoughts and attitudes towards PTR among COPD patients who decline participation in PR and to identify their imagined barriers and enablers towards hypothetical participation in PTR.
Materials and Methods
Study Design
This study is a mixed-methods study with a convergent parallel design for the purpose of complementarity, in order to develop a broader understanding of the research area. The quantitative and qualitative studies were conducted simultaneously, analyzed separately and subsequently merged to address facets of the same phenomenon.25–27
The study was conducted from February 2020 to December 2021. The design included surveys and individual semi-structured interviews.
Participants
Participants were recruited after declining participation in PR at two university hospitals in the Capital Region of Denmark.
It was possible to recruit the required number of participants during the time period in between the two major waves of the COVID pandemic (2020 and 2021). During this time, there were no COVID restrictions in Denmark; hence, it was possible to recruit from an outpatient pool and the participants were able to attend the PR in person.
None of the patients recruited for this study stated COVID-19 as a reason to decline outpatient hospital-based routine PR. All participants were adults (>18 years), eligible for outpatient hospital-based routine PR in the Capital Region of Denmark, and had a clinical diagnosis of COPD defined as FEV1/FVC <0.70, FEV1 <55%, Medical Research Council (MRC) ≥2, and had not participated in PR within the past 12 months.2
The invitation to this study took place when patients declined participation in the conventional hospital-based PR programs when offered during routine consultations and when inclusion and none of the exclusion criteria were confirmed by the clinical staff (nurses or physicians). If a patient agreed to participate, a research nurse and physiotherapist invited the patient to a physical assessment and completion of patient-reported outcome measures and the purpose-designed survey.28
All participants completed a survey about reasons for declining PR and thoughts and attitudes towards participation in PTR. First, the participants for the qualitative study were selected based on the survey answers to obtain a heterogeneous group, including patients with both positive and negative preferences for physical activity and technology. Second, the participants were selected by age and whether they had previous experiences with PR. After finishing the survey, the nurse or physiotherapist making the assessments asked whether they wanted to participate in an in-depth interview. Those interested were subsequently contacted by telephone by KS to make the final agreement about date and place for interviews.
Survey
A purpose-designed survey was developed by the three authors KS (female physical therapist), CE (female nurse) and HH (male physical therapist).28 It contained 29 questions grouped in four themes: Knowledge of and reasons for declining PR (8 questions); Self-reported physical activity and functioning (6 questions); Knowledge and engagement with Information and Communication Technology (ICT) devices (5 questions); Attitudes and thoughts towards telerehabilitation (10 questions). The questions within the themes of Knowledge and engagement with Information and Communication Technology (ICT) devices and Attitudes and thoughts towards telerehabilitation (10 questions) were answered on a 5-point Likert score and included option of a neutral answer.
Telerehabilitation in the context of this study and the purpose-designed survey was defined as follows:
An offer where patients receive guidance in physical activity and exercise as well as information about their lung disease. It takes place either through a video connection on a computer, tablet, or smartphone, or by a telephone conversation, or a text message with a health professional at the hospital. The participants receive tele-rehabilitation in their own home. It can take place one-on-one or in a group with several participants who have a similar lung disease.16
The survey was pilot tested on five persons beforehand, all of whom were comparable to the eligible participants. Minor wording changes were made based on feedback to enhance understanding and comprehension of the questions.
The sample size calculation is based on an overall COPD population in Denmark of approximately 50,000 people with severe or very severe COPD. A confidence level of 95% with a margin of error (confidence interval) of 10% was chosen and resulted in a sample size of 97 participants.29 We anticipated a response rate of 100% since the survey was completed in continuation of a physical examination in which all patients participated (NCT04249388). The patient reported questionnaires and purpose-designed surveys were administered to all patients in the same order, and the patients filled out the questionnaires in an undisturbed room without interference from the rater. All patients received a brief, standardized instruction in how to complete the questionnaire.
Framework
The qualitative study was based on Theoretical Domains Framework (TDF). TDF was developed to simplify and integrate behavior change theories into a single framework.20 The framework was developed by an interdisciplinary group of health and implementation researchers who found consensus about how 33 theories related to behavior change could be categorized into domains, constructs, and labels. The latest validated TDF version from 2012, which was applied in this study, consists of 14 domains.19 TDF was beneficial for the purpose of this study as it is developed to assess enablers and barriers to implementation.
In this study, we used the framework for developing the interview guide. Furthermore, the results of the interviews were interpreted against the framework to identify barriers and enablers towards participation in PTR.
Interviews
The interview guide was developed by the authors and had a semi-structured design.30 The guide was divided into two main themes: Reasons for declining participation in PR, and thoughts and attitudes towards participating in PTR (see interview guide in Supplementary Table 1). For each theme, questions were based on the 14 domains of TDF and were designed to explore barriers and enablers regarding PR and PTR (see examples of interview questions in Table 1).
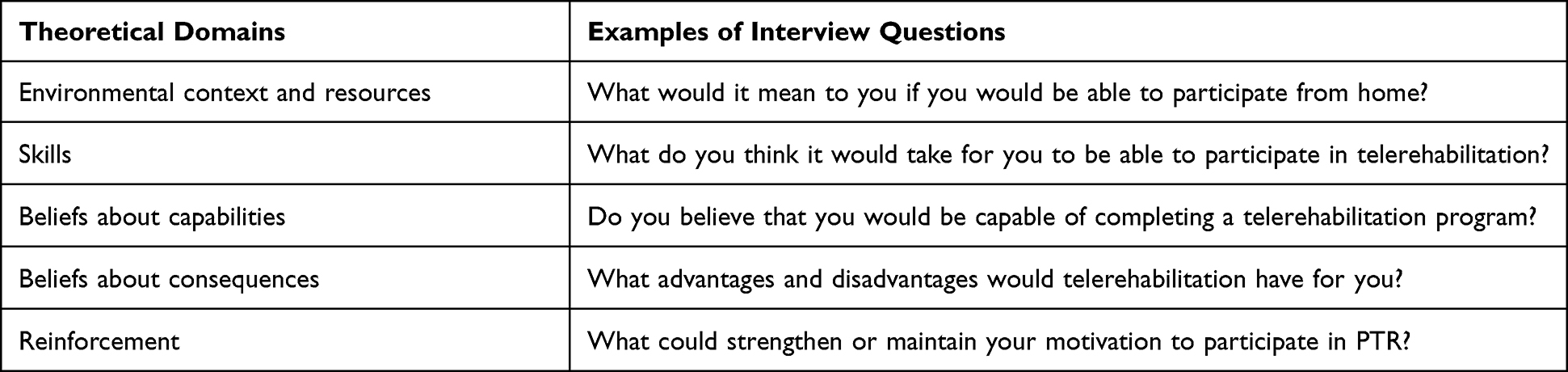 |
Table 1 Examples of Interviews Questions Related to the Domains in the Theoretical Domains Framework |
The interview guide was pilot tested on a male participant with a positive attitude towards physical activity, who confirmed the relevance of the questions, resulting in minor corrections of the interview guide. Recruitment for interview continued until triangulation of data ensured sufficient information power.31
In total, seven interviews took place in the participants’ own homes; one was conducted at the hospital and one online. The interviews lasted between 26 and 51 minutes with a mean duration of 37 minutes. The interviews were primarily conducted by KS with ongoing consensus discussions based on transcriptions or audio files with HH and CE. Four out of nine interviews were observed by either HH or CE, who asked supplementary questions during the interviews. All audiotaped interviews were transcribed shortly after the interviews by KS using the Express Scribe Transcription Software Pro version 9.11.32
Data Generation and Analysis
Data were collected simultaneously from surveys and interviews, analyzed separately and subsequently merged. Topics that emerge from the qualitative and quantitative data that supplement and support the same themes are presented under the same headings in order to substantiate and strengthen statements. Contradictory findings are presented to show different attitudes and thoughts within the same theme.25–27
Analysis of the Survey
Descriptive data are presented as mean ± SD (standard deviation), median (interquartile range (IQR)) or number (%). Data for each statement in the purpose-designed survey are expressed as mean ± SD, median (IQR) or number (%).” In questions where multiple responses are possible, the sum of percentages may be more than 100%. Multiple logistic regression analysis was used to assess the association between the variables for age, gender, educational level, comorbidities, and previous PR participation to the frequency in ‘use of technology device’, the ‘belief of benefit in pulmonary telerehabilitation analysis’, and ‘self-rated technical skill confidence’. A multinominal logistic regression analysis including the variables for age, gender, educational level, comorbidities, previous PR participation, ‘use of technology device’, ‘belief of benefit in pulmonary telerehabilitation analysis’ and ‘self-rated technical skill confidence’ was used to assess the association of being willing to participate in pulmonary telerehabilitation. Fisher’s exact test was used for analyses of categorical data. Data were analyzed using IBM SPSS version 26 (IBM Corp, Armonk, NY, USA) and p-values of less than 0.05 were considered statistically significant.
Analysis of the Interviews
The interviewers were aware of their own preconceptions in the meeting with the participants, which is why a hermeneutic approach is used to interpret and analyze the data.33,34
Initially, the transcripts were analyzed with a mainly deductive approach inspired by the thematic analysis to identify themes.35–37 The deductive analysis followed the six phases in the thematic analysis and was done iteratively. The researchers coded separately and subsequently discussed the coding and categorization process, interpretations, and information power. Agreement was found through discussion, nuances in interpretations were accommodated and resulted in a more complete analysis.
Thematic analysis:35–37
Phase 1–2: Familiarization of data and coding with a recognizable label referring to TDF domains.
Phase 3–5: Theme development, with a process of clustering codes to identify “higher-level” patterns in main themes and subthemes, then reviewing and refinement whether the placement of the codes is consistent with the themes, and last naming the themes in reference to what is the main essence of the theme.
Phase 6: Writing up, which involves compiling, developing, and editing analytic writing and choosing data extracts from across the dataset.
Merging of Data
The methodological triangulation of data, with a parallel convergent design, meant that completed analyses of both quantitative and qualitative data were merged and integrated in the final analysis.
The qualitative data were used to assess the validity of quantitative results and quantitative data helped generate the qualitative sample and explained findings from the interviews. The qualitative and quantitative data were weighted as equally significant. Sometimes the qualitative findings were essential for the emerged theme and sometimes the quantitative data defined the theme substantiated by qualitative interpretations and quotes25,27,38 (Supplementary Table 2).
All three researchers took part in the merging of data, discussing what findings emerged from each method were most important. Topics that complimented each other or showed variation were highlighted in the results section.
Ethics
The study was conducted in accordance with the ethical principles of the Helsinki Declaration.39 The Danish Data Protection Agency approved the research database (P-2019-730), and the General Data Protection Regulation was secured. Because the study was noninterventional, an ethical approval was not necessary according to Danish law.40 Prior to the survey and interviews, the aim of the study and the participants´ role was explained verbally and in writing. The participants who participated in interviews agreed to the interviews being audiotaped with anonymization and informed and written consent was obtained from all participants. Informed consent was obtained from all participants (survey and interviews) including approval for publication of anonymized responses.
Results
The data consisted of 84 completed surveys and nine individual semi-structured interviews. Eleven participants included for physical examination declined to complete the survey subsequently. Thus, we closed the survey collection with a response rate of 88% and a margin of error (confidence interval) of 10.7%. On the subsequent telephone call, six declined to participate in interviews due to personal circumstances or had regretted participation.
Participant characteristics are shown in Table 2. The participants had severely progressed airflow obstruction, a high burden of respiratory symptoms and/or exacerbations, and the majority presented ≥3 comorbidities. Forty percent were naïve to PR. The participants’ physical activity level (PAL) measured by steps/day (activePAL accelerometer) was classified as sedentary and physically inactive (<5000 steps/day),41 and 60% of the participants had frailty signs indicated by a short physical performance battery score of ≤8 points.
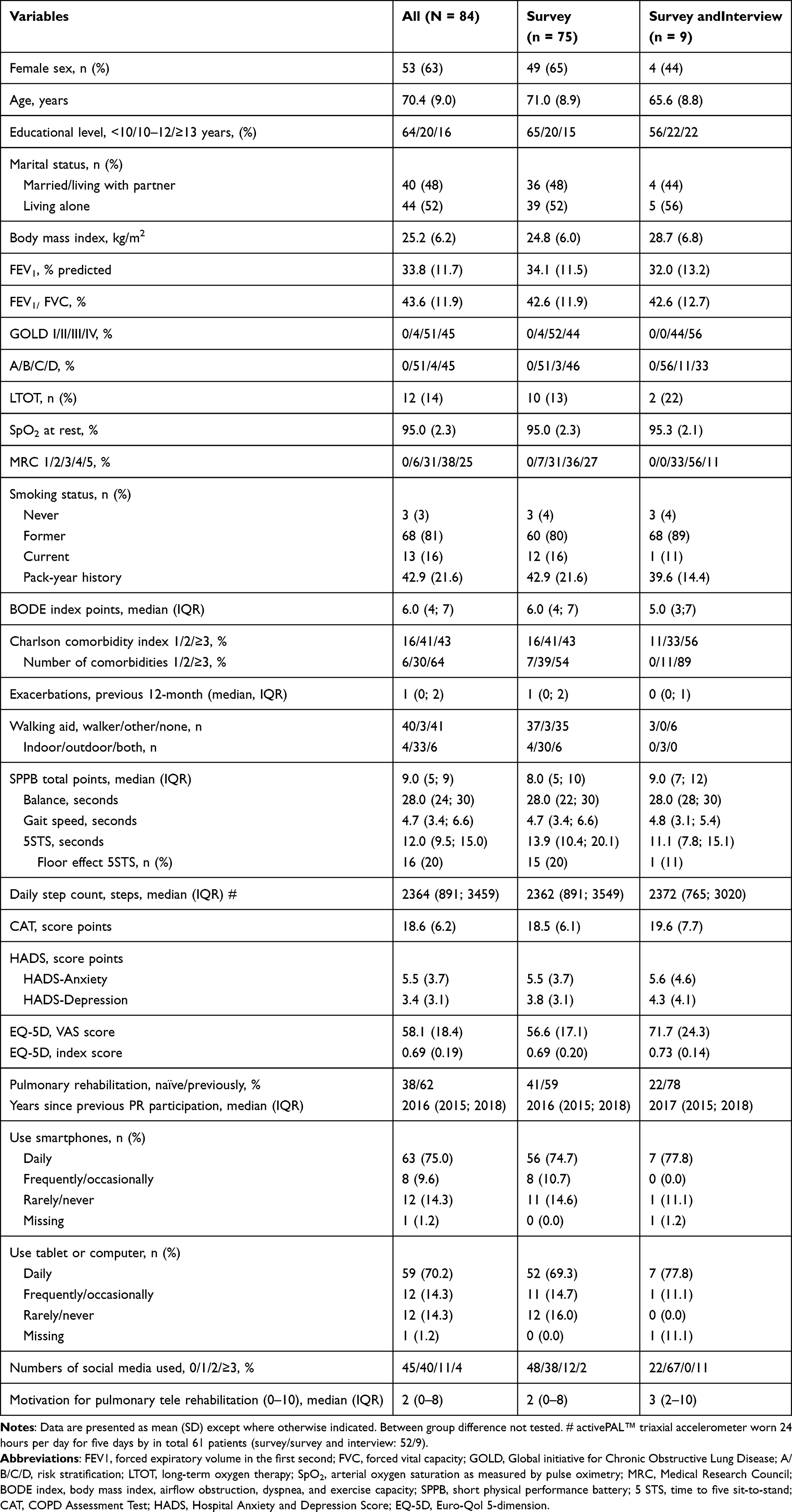 |
Table 2 Participants Characteristics |
The median motivation score was 2 on a numeric rating scale (NRS 0–10), whereas 32% of the participants had a motivational NRS score of ≥7 for PTR.
Reasons to Decline Pulmonary Rehabilitation
Survey data regarding reasons for declining PR, knowledge about PR, and recall of the referral situation can be seen in the Supplementary Materials (Supplementary Table 3). A statistically significant larger proportion of participants naïve to PR stated “not motivated/not relevant” compared to participants with previous PR experience (OR: 3.4 [95% CI: 1.1; 9.9], Fisher’s exact test, P=0.03). More participants with previous PR experience stated symptoms from COPD as a reason to decline PR. The proportion difference was statistically significant (OR: 5.8 [95% CI: 1.9; 17.5], Fisher’s exact test, P=0.001) (Supplementary Table 4). Interview data regarding the same subject are also available in Supplementary Material, presented with themes, subthemes, and citations referring to the themes (Supplementary Table 5).
Thoughts and Attitudes Towards Hypothetical Participation in Pulmonary Telerehabilitation
In the following, quantitative and qualitative data regarding potential participation in PTR are presented simultaneously referring to the same themes and headlines. Some themes and perspectives primarily emerged in the qualitative data and some have only been highlighted in the quantitative material. The qualitative themes which were found in the thematic analysis are as follows: 1) Convenience of participation and flexibility, 2) Beliefs of capabilities, 3) Willingness to participate in PTR and 4) Thoughts on and preferences for content in PTR (Supplementary Table 6). These four themes were subsequently merged with the quantitative findings and new themes and subthemes emerged. In the following section, mixed results are presented under new headlines in which the quantitative and qualitative results support each other (Table 3).
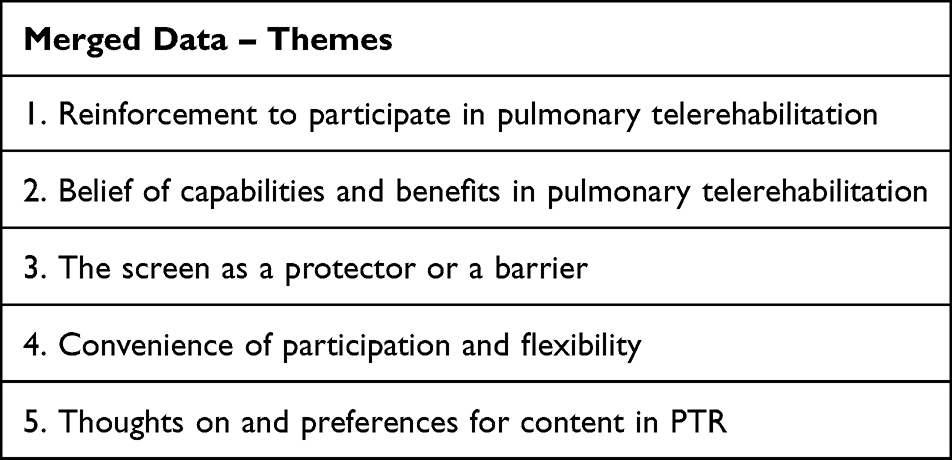 |
Table 3 Merged Data – Themes |
Reinforcement to Participate in Pulmonary Telerehabilitation
A total of 28% agreed or strongly agreed that they would be interested in participating in PTR, whereas 29% and 43% were undecided or not interested. Seventy percent agreed or strongly agreed that they would feel safe if initiating PTR at home.
In the multinomial regression model (Table 4), believing in the benefit from a PTR program was significantly associated with being willing to participate in PTR (OR: 12.69 [95% CI: 3.02; 53.22], p=0.0005) compared to the group not willing to participate in PTR. Daily use of tablet/CPU (Central Processing Unit) and smartphone was also strongly associated to willingness for PTR. There was no significant association related to the group of undecided patients’ willingness compared to those not interested. The model accounted for 39% (Nagelkerke R-square) of the variance in determining the odds of willingness to participate in PTR. A smaller proportion of those unwilling (73%) to participate in PTR compared to those interested in PTR (100%) used smartphones (p=0.043), Similar, a larger proportion (61% vs 31%) did not use a social media in those unwilling to PTR compared to those interested in PTR (p=0.006) (Supplementary Table 7).
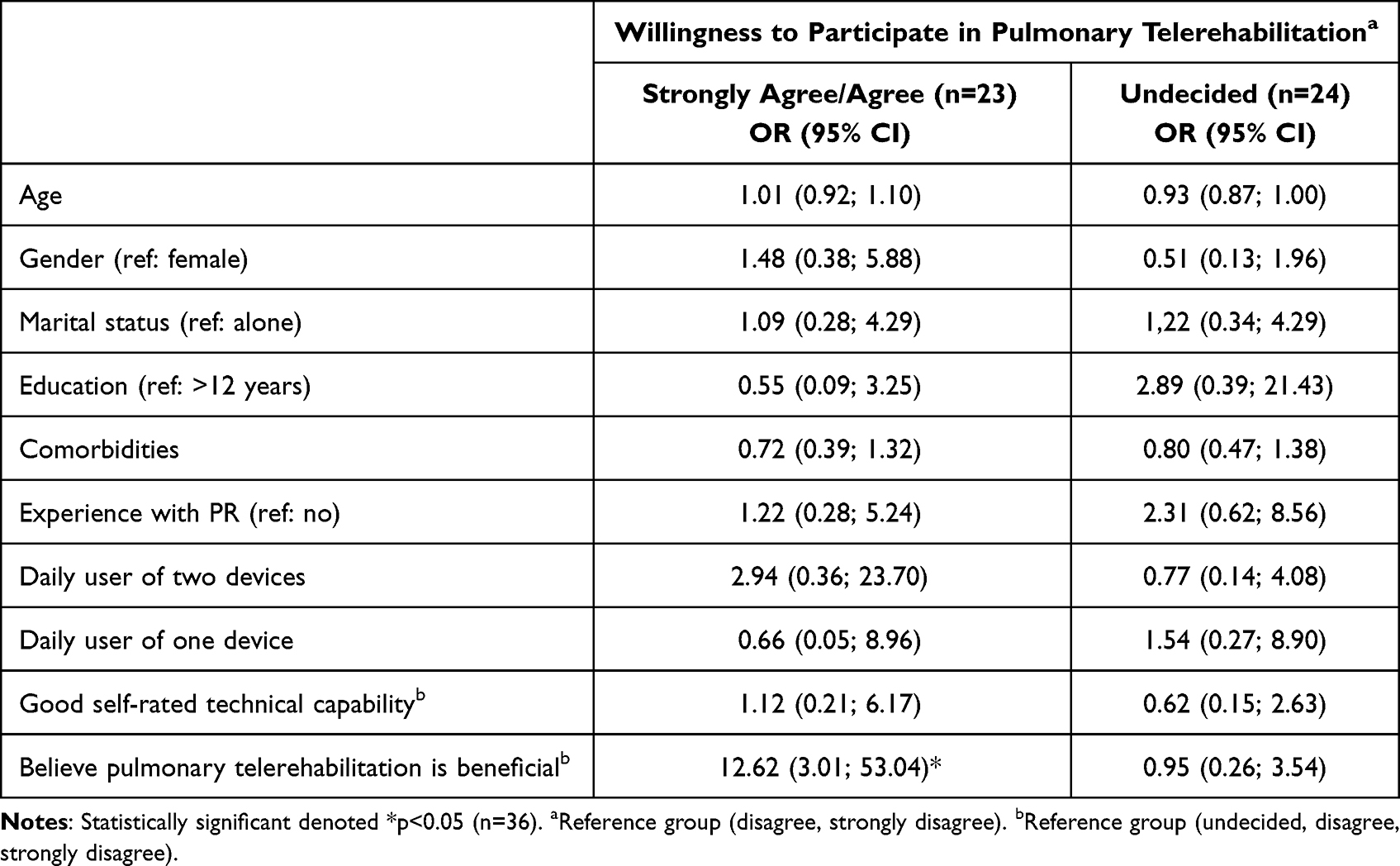 |
Table 4 Multinominal Logistic Regression |
The qualitative interviews highlight some of the factors which reinforce the participants’ willingness to participate in PTR, such as group vs individual setting and the perception of the screen.
Social Influences
Participants with positive preferences for PR found it beneficial that PTR takes place in groups and appeared optimistic about participation. They could see themselves sharing experiences about living with COPD – but were all doubtful whether it would be possible to achieve a close relationship over the screen.
No, I do not think it would be the same, I can´t imagine. But if we had a connection then you could perhaps invite and say: ‘Come over to my place – then vi can talk’. (woman #5, 70 years, PR naïve)
The participants did not expect the social needs to be met to the same extent via screen. However, the participants found that the content presented via virtual media may be as binding as attending in person. In addition, some could see themselves taking active part in the group, whereas others preferred to be passive members.
No, no, I could sit and talk with people, but if I sit in a group and someone asks me a question – I wouldn´t like that. (woman #2, 79 years, previously participated in PR).
Belief of Capabilities and Benefits in Pulmonary Telerehabilitation
A proportion of 42% (n=35) agreed or strongly agreed that PTR would be equally beneficial compared to outpatient hospital-based PR. Thirty-nine percent agreed or strongly agreed that they would benefit from participation. Neither gender, age, length of education, number of comorbidities nor previous PR participation was significantly associated to the belief of benefit in a PTR intervention (Table 5).
 |
Table 5 Multiple Logistic Regression |
The interviews highlighted that the participants’ beliefs about their capabilities and the consequences of PTR affect their attitudes towards telerehabilitation.
They had all experienced a decreased functional capacity over several years and appeared skeptical and pessimistic about new initiatives. This made the belief of positive effects difficult, but they still hoped for some improvements.
It has only been going one way (shows with the hands that it has declined). As I say to you, I hope it can remove some of my difficulties – and I have many. (man #2, 61 years, previously participated in PR)
The participants were aware of their own physical ability and were honest about their immediate expectations.
…I was down to 26% lung function…you can only concentrate on surviving until the next day. In that period, I couldn´t find the energy. I don´t think I would benefit from participating. (woman #1, 70 years, previously participated in PR)
Furthermore, it was important to the participants that their individual capabilities are matched in PTR, referring to both extent and demands for participation and technological skills.
Physical Challenges in Relation to Co-Morbidities
Just as participation in PR was hindered by comorbidities, some participants perceived their poor health to be a barrier to participation in PTR.
I´ve been a bit scared of certain things. I do not want to experience any more defeats. For example, I have not been riding a bicycle all year and almost not last year either. Because I fear that I´m not able to, and then I don´t want to try at all. (man #2, 61 years, previously participated in PR)
The fear of another defeat, when the body fails again, strengthened this participant in his doubt about whether PTR would match his needs. In addition, some described themselves as forgetful and had difficulties learning new things. The obligation to something new and unknown seemed frightening.
Beliefs of Capabilities Regarding Technical Skills
A majority of the survey respondents were daily users of a computer or tablet and smartphone, and more than 50% used the social media Facebook (Table 2). In the multiple logistic regression model, an increase of age was significantly associated with reduced odds of daily use of a CPU or tablet (OR: 0.89 [95% CI: 0.83; 0.96], p=0.003), while age was not associated with daily use of a smartphone (Table 5).
More than two-thirds (69%, n= 58) agreed or strongly agreed that they had the technical capability to participate in PTR. In the multiple logistic regression model (Table 5), an increase in age was significantly associated with reduced odds of the individual believing in one’s own technical abilities (OR: 0.92 [95% CI: 0.86; 0.98], p=0.007).
Most of the interview participants felt confident using technologies, were curious, and could recognize the potential in the use of technology, which reinforced their potential participation in PTR. It applied to participants in all ages and of both genders. However, one participant (83 years) had a very strong dislike against all technologies.
I´m not even going to start dealing with something like that. You know what, something like that with electronics and numbers. I simply can´t. I have never been able to. (woman #3, 80 years, previously participated in PR)
Some participants believed that technologies are necessary to be in contact with the outside world. But not all preferred this way of communication even though they felt confident using the technology.
Sometimes I´m talking with friends from Thailand over the screen.… It’s not optimal, so I might as well call them on the phone (man #2, 61 years, previously participated in PR)
The participants drew on earlier experiences with technologies when reflecting about possible participation in PTR. Some only had experiences with communication through screen not being guided to exercise training. Most participants did not know anything about PTR, and a short introduction did not seem to change their immediate assumptions.
I have seen some of it on the internet, but it wouldn´t work for me. (man #2, 61 years, previously participated in PR)
The Screen as a Protector or a Barrier
The screen was in general perceived as a barrier, but at the same time some of the patients described that they felt safe behind the screen. This perception was expressed as the screen having an enabling effect because of the physical and mental distance.
But it´s like when someone is sitting there (pointing on the dining room chair), I feel a certain pressure. That (pointing on the TV) on the other hand, I would not feel. It´s sounds crazy, I know. (woman #2, 79 years, previously participated in PR)
The participant perceived the screen as a shield that protected her against the pressure that she felt when a therapist was present, which strengthened her positive beliefs of PTR.
The skeptics believed that the screen would impede the interaction between people. They worried that the technical equipment would not work, which could affect communication negatively. They also believed that the distance between participants would reduce the positive results of PTR.
Feeling Supported and Looked After
The participants expressed a need to be supported in their exercises, and they wanted to be able to seek professional help with questions concerning their illness. They believed that they would feel encouraged to participate if they had scheduled appointments and knew that they would be supported.
So, no matter how serious it is, you will always laugh with her (referring to the nurse she talks to through a screen). It makes me feel safe, and I also know that others feel safe, because you always have someone to back you up. (woman #1, 70 years, previously participated in PR)
An alliance was created between the nurse and the participant, which strengthened the connection and commitment. The participants emphasized the importance of PTR being a forum where concerns could be addressed with relevant HCPs.
The survey also highlighted the participants’ immediate thoughts about whether participation in PTR at home would be safe or not. A majority of 70% agreed PTR performed in their own home would be safe, and only 6% disagreed or strongly disagreed.
Convenience of Participation and Flexibility
A proportion of 49% agreed that PTR would make it easier to participate in rehabilitation (compared to PR), 19% disagreed, while 32% were undecided. A majority of 80% agreed that PTR would be time saving and more flexible compared to outpatient PR in hospital and community settings.
In the interviews, the participants reflected on the convenience of exercising at home, and how tele-rehabilitation would affect their daily living.
Environmental Context
For some participants, rehabilitation in their own home would be attractive. They presumed that it would give them more energy if they should not be concerned about the transportation to and from the hospital. On the contrary, some participants imagined that too many disturbing elements in the home would hinder them from focusing on the screen.
I don´t know, I have no interest in it. I´m not going to stand in front of that (pointing on the television), it´s not going to work for me. Then you have to pee and then you want a cup of coffee – there will always be something that disturbs you. (man #2, 61 years, previously participated in PR)
Common to all participants was that the context must appeal to physical activity, and the HCPs must accommodate and support these beliefs to facilitate to participation in PTR.
PTR´s Impact on Daily Living
If the participants found exercising important, they seemed more willing to prioritize participation in PTR over daily chores and appeared more positive about making changes in the home.
My life is more important than dust and vacuuming. Well dear, no one will clean for you. Whether it´s going to be today or tomorrow, or the day after that, it doesn´t matter. I´m ready, it´s my life. (woman #4, 57 years, PR naïve)
A positive attitude and a strong belief in the effect of PTR was reinforced by the easy accessibility. If the participant doubted the effect, the consequences of making changes in the home would be too big and it could potentially lead to drop-out.
Thoughts on and Preferences for Content in PTR
A proportion of 40% preferred to exercise in groups (supervised) and only 28% preferred exercising alone without supervision. The most preferred content was physiological measurements which the participants were familiar with qua their control visits at the hospital (Figure 1).
 |
Figure 1 Preferred content for pulmonary telerehabilitation. |
The survey data on thoughts on the content of PTR were elaborated further in the interviews.
Extent of PTR (Time, Duration)
The participants were asked to what extent they saw themselves able to participate in PTR. Earlier experiences with exercise training, how much interruption in daily life they would accept, and what they saw themselves able to manage physically were important elements in the decision-making.
I think if you want to benefit from the exercises, you ought to participate at least twice a week, perhaps 3 times. How it could fit into my life, I don´t know, and how to find the energy, that I can´t figure out either. (woman #4, 57 years, PR naïve)
The participants responded from what is common knowledge about physical activity and what they knew from other contexts. The skepticism is interpreted as a doubt as to whether they can master what is expected from them.
Oral or Written Communication
According to the participants, PTR should include both conversations about specific topics related to COPD and physical activity. But the participant expressed that it must be separated, otherwise it would remove focus from the exercises. Several participants expressed concerns about the content of the conversation during PTR. Since the entire group are listening, they would prefer if the conversation did not get too personal.
Yes, we can talk, but if it takes too much time, and we all must sit for 20 minutes and talk about our lives, then it won’t make any sense. (man #1, 64 years, previously participated in PR)
The participants with previous experience with telemedicine saw advantages in the online written communication with an HCP. Being able to ask questions related to their COPD and cancel an appointment would promote participation.
It seemed important that the group would be homogeneous and that the individuals would have the same approach to e.g., life, technological skills, or similar functional level. Otherwise, it could be a barrier to participation.
It must be someone who is at the same level as me, not in terms of technological skills, but has the same lung function as me. Otherwise, it would not work for me. (woman #1, 70 years, previously participated in PR)
Discussion
In this study we explored thoughts and attitudes and identified perceived barriers and enablers towards participating in pulmonary telerehabilitation among patients with severely progressed COPD who declined referral to an outpatient hospital-based routine pulmonary rehabilitation program.
The main part of the participants had a low motivation or was undecided for participation in PTR which is supported by the qualitative findings. Their reserved thoughts and attitudes towards PTR are even more important to highlight in order to accommodate these barriers in future designs of PTR. We found a significant association between belief of effect of PTR and willingness to participate. Also, an increase of age was significantly associated with reduced odds of daily use of CPU or tablet. Most participants perceived participating in PTR convenient, due to easier access and minimal interruption of daily living, and had preferences for individualized, supervised and monitored rehabilitation. Thus, the individual’s preferences must be met in relation to preferences for physical activity, positive as well as negative attitudes, and social influences. Not being able to see themselves in the setting, hospital or exercising at home, may be a barrier for referral and participation. A novel aspect of this study was that PTR is considered just as binding as PR as long as it is supervised and there is a sense of social community.
To our knowledge, this is the first study to investigate thoughts and beliefs of PTR among patients with COPD who decline enrolment in conventional outpatient PR. In line with previous qualitative studies concerning COPD patients, the qualitative results from our study found that the patients request individualized rehabilitation protocols.42 Conversely, HCP and patients have different opinions about the context in which PTR is implemented. A majority of the participants agreed that PTR performed in their own home would be safe, which is in contrast to study findings among HCPs for whom safety and communication are central themes of concern.21
The included participants have different opinions about PTR. A few see technology as a barrier because they do not have the skills, for others technology is not appealing, whereas half of the participants believe that the technology enables participation because of its flexibility and easy access. The perception and acceptance may change over time as generations become more digitalized (digital natives), and the platforms continuously develop.
The strong association of daily use of tablet/CPU and smartphone and willingness to participate in PTR is consistent with the results from an Australian study by Seidman et al investigating technology engagement in patients participating in an outpatient PR program.11 Seidman and colleagues found a significant association between self-rated computer/technology skills and age <70 years and that a proportion of 40% were willing to use PTR.11 In our study, only 28% agreed or strongly agreed that they would be interested in participating in PTR. The association between self-rated skills and belief of effect and willingness to participate in PTR can be explained using the TDF where belief of capability and inherent skills are interpreted as enablers towards successful implementation of a health intervention.19,20 Another Australian study by Tsai et al evaluated satisfaction and experiences of an 8-week supervised PTR program.13 Participants reported that PTR is convenient, saves costs and is more flexible compared to physical attendance. Besides the important difference investigating people with and without capabilities to participate in and outpatient PR program, Australia and Denmark are geographically incomparable in terms of distance to the rehabilitation centers, which could be another plausible explanation for the different interest and willingness towards PTR.
Both the qualitative and quantitative data reveal that one-third of the group remain undecided about participation in PTR or have difficulty imagining the potential benefits. The qualitative statements reveal that not everyone has been able to form an opinion only based on a brief description of PTR. Thus, their immediate thoughts are affected by lack of knowledge. New models must be designed and tested with the aim to promote knowledge and understanding about the beneficial effects of PTR, ensuring that patients make decisions about participation on an informed basis.
Little is known on what overturns a patient’s decision from pro to con and vice versa in a referral situation to a PR program. Obviously, knowledge of methods and information to promote PTR is essential to increase referral and uptake for PTR programs and increase the overall utilization of PR programs.43,44
In addition, the COVID-19 period might have changed our digital behavior and the perspective on PTR, as communication through screen has been integrated into our way of communicating with the outside world and to maintain social contact. We might see new opportunities in delivering and receiving healthcare through a digital solution.
A study by Reicher et al has examined attitudes towards telemedicine during COVID-19 lockdown and willingness to use such services in the future.45 A majority stated they would continue using telemedicine in the future. Participants with chronic conditions were more likely to use these services, and specific attention should be directed to their needs. Preferences for visiting the clinic were negatively correlated with willingness to use telemedicine in the future.45 Polgar et al examined digital literacy amongst to cohorts of patients with COPD, just before the COVID-19 pandemic in 2020 and during the pandemic in 2021 and found that digital literacy was better among the 2021 cohort, but despite this no difference was seen in the proportion of patients choosing PTR.46 A qualitative study of provider’s shift to telerehabilitation during COVID-19 suggests that while telerehabilitation may not be appropriate in all patients, future healthcare interventions should be designed as a hybrid system of using both telerehabilitation and in-person visits as a way to advance the rehabilitation care continuum.47
Participants who decline PR are scarcely researched and their thoughts and attitudes towards PTR have not previously been explored, although PTR is intended for this group of patients. This study brings insights into barriers and enablers towards participation in PTR and provides suggestions for how HCP can meet the patients’ individual needs.
PTR is a relevant and attractive alternative to PR, in patients who are convinced of beneficial effect from a PTR program, see opportunities in exercising at home, have high self-rated technological skills, and when PTR includes the possibility of monitoring and a continuous dialogue with HCPs. Thus, PTR is not one solution only, and not suitable for all patients.
This study emphasizes that PTR should include disease monitoring, which is supported by a previous study.48 This is interpreted as a need that is otherwise met by the patients’ hospital visits with physical attendance. Interview participants expressed that close contact to an HCP with monitoring of their COPD provides a feeling of not being alone with the disease. The screen is perceived as both a barrier and a protector, the latter resulting in a feeling of being supported and looked after. These statements may positively affect coping strategies and commitment to PTR. Consistent with our findings, a study by Emme et al suggests that there is no difference between self-efficacy in COPD patients undergoing virtual admission, compared to conventional hospital admission49 and accordingly, communication by screen can be perceived as safe and equally supportive. Slevin et al explored the patient perspective on the potential benefits of digital health technology (DHT) for management of COPD. The study emphasized that DHT could enable the patients’ symptom management. Furthermore, interaction with the HCP could facilitate a personalized care.50 Both results substantiate our findings.
Nearly half of the participants believed that PR and PTR are equally beneficial, but PTR is considered to ease access, be more flexible and time saving compared to an outpatient PR program in hospital and community settings. Our findings are similar to those in a study by Shanmugasegaram et al, who explored barriers to home-based cardiac rehabilitation (CR) compared with an outpatient program. The study found that patients who perceived transport or distance to the rehabilitation center as a barrier had increased attendance and adherence rates if they were allocated to home-based CR. These patients were engaging in significantly more exercise 1-year post-hospitalization than their site-based counterparts. This is a group comparable to patients with COPD, and it is reasonable to assume that perceived barriers to rehabilitation are comparable.51
The qualitative data from our study have highlighted the importance of social influences in terms of support from HCP and preferences for group-based interventions. If the social needs are not fully met, it could lead to lack of engagement or motivation. Conversely, the social community facilitates motivation, maintains participation, and promotes commitment. A qualitative study from 2021, which has explored the commitment to CR, finds that the patient´s commitment increases when maintaining contact with the treatment team.52 The maintaining commitment is associated with positive consequences such as treatment adherence and the formation of healthy behaviors.
Strengths and Limitations
The strength of this study was the triangulation of quantitative and qualitative data with the latter methodology allowing a greater depth of detail to emerge thoughts and attitudes towards potential participation in telerehabilitation, triangulated with a sufficient sample of survey respondents allowing more generalized findings.53,54
Ongoing consensus and dialogue in the research group concerning diversity of findings, seen from an exploratory approach, ensured that the study achieved sufficient information power, which enabled us to conduct a trustworthy thematic analysis and answer the research questions. The integration of two methods brings insights in to details which are otherwise not possible to obtain by using only one method.54 The interviews unfold details of the phenomenon and survey data can support the extent of the phenomenon. This way our study findings can be representative and generalizable to a larger population and in other settings.46
All patients declining PR were asked to participate to avoid selection bias. However, the inclusion of participants who declined PR but accepted participation in surveys and interviews is a selected group and might not reflect the thoughts and attitudes of the patients who also decline participation in research. However, the thoughts and attitudes of the interview participants were very diverse, why this might not have influenced the results of this study in any specific direction.
Implications for Clinical Practice
This study provides new insight into how patients with severe and very severe COPD think about potential participation in telerehabilitation as an alternative to conventional outpatient hospital-based PR.
This study focused on exploring thoughts and attitudes towards PTR among COPD patients who decline participation in hospital-based PR. Some of the findings of this study may be transferable to a community-based setting, but further research is needed.
The referral situation seems crucial for whether the patients believe they will benefit from the intervention they are offered (PR or PTR). In addition, non-specific factors, such as contact with a well-known and trusted HCP must be considered.
In order to make an informed decision about rehabilitation, the participants need information about content in PTR, and how their personal preferences are met. Finally, all clinicians should identify barriers, enablers, and preferences in any PR referral conversation as they might change over time.
Conclusion
Most participants were not motivated for participation in pulmonary telerehabilitation. Those most willing to participate believed in the benefit of pulmonary telerehabilitation, were comfortable with technological devices, had preferences for exercising at home, and saw opportunities in the social setting. Participants unable to attend an outpatient rehabilitation program were frequent users of smartphones, tablets, and Central Processing Units. However, one-third were undecided about potential participation in a pulmonary telerehabilitation program, why their needs and attitudes must be further elaborated. Healthcare professionals must be educated to identify barriers and enablers, create interest for pulmonary telerehabilitation programs and communicate in an understandable and equal manner.
The participants requested future pulmonary telerehabilitation programs to include monitoring, preferably managed by a familiar healthcare professional. Furthermore, the study emphasizes that the healthcare professionals should pay attention to the patients´ preferences for physical activity and social commitment. In addition, knowledge about patients’ belief in their own physical and technological capabilities and thoughts of possible effect may be helpful in assisting the patients in choosing the most suitable rehabilitation program.
Data Sharing Statement
The raw data are not available to the public according to rules of the Danish Data Protection Agency.
Ethics Approval and Informed Consent Statement
The Danish Data Protection Agency approved the research database (P-2019-730). Because the study is noninterventional, ethical approval was not necessary according to Danish law. Informed verbal and written consent were obtained from all subjects involved in the study.
Acknowledgments
We thank the patients who participated in this study. We also thank the Departments of Respiratory Medicine at Hvidovre and Bispebjerg University Hospital for their commitment and recruitment of patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Telemedical center Regional Capital Copenhagen (governmental funding) and TrygFonden.
Disclosure
HH received personal grants from the Telemedical center Regional Capital Copenhagen (governmental funding) and TrygFonden foundation (charitable funding). The grants cover expenses conducting the trial and salary for his postdoctoral employment. The authors report no other conflicts of interest in this work.
References
1. Sundhedsstyrelsen. Anbefalinger for tværsektorielle forløb for mennesker med KOL; 2017. Available from: https://www.sst.dk/da/udgivelser/2017/-/media/Udgivelser/2017/Anbefalinger-for-tværsektorielle-forløb-for-mennesker-med-KOL.ashx.
2. Augusti A, Beasley R, Celli BR, Chen R Global initiative for chronic obstructive pulmonary disease; 2020. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
3. Løkke A, Hilberg O, Tønnesen P, Ibsen R, Kjellberg J, Jennum P. Direct and indirect economic and health consequences of COPD in Denmark: a national register-based study: 1998–2010. BMJ Open. 2014;4(1):e004069. doi:10.1136/bmjopen-2013-004069
4. Sundshedsdatastyrelsen. Borgere med KOL – Kontaktforbrug i sundhedsvæsenet og medicinforbrug; 2016.
5. Spruit MA, Burtin C, De Boever P, et al. COPD and exercise: does it make a difference? Breathe. 2016;12(2):e38–e49. doi:10.1183/20734735.003916
6. Puhan MA, Gimeno‐Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016. doi:10.1002/14651858.CD005305.pub4
7. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Libr. 2015;2015(4):CD003793. doi:10.1002/14651858.cd003793.pub3
8. Bjoernshave B, Korsgaard J, Jensen C, Vinther Nielsen C. Participation in pulmonary rehabilitation in routine clinical practice: participation in pulmonary rehabilitation. Clin Respir J. 2011;5(4):235–244. doi:10.1111/j.1752-699X.2011.00237.x
9. Hansen H, Bieler T, Beyer N, et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: a randomised multicentre trial. Thorax. 2020;75(5):413–421. doi:10.1136/thoraxjnl-2019-214246
10. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756
11. Seidman Z, McNamara R, Wootton S, et al. People attending pulmonary rehabilitation demonstrate a substantial engagement with technology and willingness to use telerehabilitation: a survey. J Physiother. 2017;63(3):175–181. doi:10.1016/j.jphys.2017.05.010
12. Ambrosino N, Vagheggini G, Mazzoleni S, Vitacca M. Telemedicine in chronic obstructive pulmonary disease. Breathe. 2016;12(4):350–356. doi:10.1183/20734735.014616
13. Tsai LL, McNamara RJ, Moddel C, Alison JA, McKenzie DK, McKeough ZJ. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: the randomized controlled TeleR Study. Respirology. 2017;22(4):699–707. doi:10.1111/resp.12966
14. Vasilopoulou M, Papaioannou AI, Kaltsakas G, et al. Home-based maintenance tele-rehabilitation reduces the risk for acute exacerbations of COPD, hospitalisations and emergency department visits. Eur Respir J. 2017;49(5):1602129. doi:10.1183/13993003.02129-2016
15. Godtfredsen N, Frølich A, Bieler T, et al. 12-months follow-up of pulmonary tele-rehabilitation versus standard pulmonary rehabilitation: a multicentre randomised clinical trial in patients with severe COPD. Respir Med. 2020;172:106129. doi:10.1016/j.rmed.2020.106129
16. Nolan CM, Kaliaraju D, Jones SE, et al. Home versus outpatient pulmonary rehabilitation in COPD: a propensity-matched cohort study. Thorax. 2019;74(10):10. doi:10.1136/THORAXJNL-2018-212765
17. Cox NS, Cox NS, Dal Corso S, et al. Telerehabilitation for chronic respiratory disease. Cochrane Libr. 2021;2021(1):CD013040. doi:10.1002/14651858.CD013040.pub2
18. Lahham A, McDonald CF, Mahal A, et al. Home-based pulmonary rehabilitation for people with COPD: a qualitative study reporting the patient perspective. Chron Respir Dis. 2018;15(2):123–130. doi:10.1177/1479972317729050
19. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37. doi:10.1186/1748-5908-7-37
20. Michie S, Johnston M, Abraham C, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33. doi:10.1136/qshc.2004.011155
21. Damhus CS, Emme C, Hansen H. Barriers and enablers of COPD telerehabilitation - a frontline staff perspective. Int J Chron Obstruct Pulmon Dis. 2018;13:2473–2482. doi:10.2147/COPD.S167501
22. Slevin P, Kessie T, Cullen J, Butler MW, Donnelly SC, Caulfield B. Exploring the barriers and facilitators for the use of digital health technologies for the management of COPD: a qualitative study of clinician perceptions. QJM. 2020;113(3):163–172. doi:10.1093/QJMED/HCZ241
23. Alwashmi MF, Fitzpatrick B, Davis E, Gamble JM, Farrell J, Hawboldt J. Perceptions of health care providers regarding a mobile health intervention to manage chronic obstructive pulmonary disease: qualitative study. JMIR mHealth uHealth. 2019;7(6). doi:10.2196/13950
24. Lewis A, Knight E, Bland M, et al. Feasibility of an online platform delivery of pulmonary rehabilitation for individuals with chronic respiratory disease. BMJ Open Respir Res. 2021;8(1):e000880. doi:10.1136/BMJRESP-2021-000880
25. Gibson K. Mixed-methods research in sport and exercise - integrating qualitative research. In: Smith B, editors. Routledge Handb Qual Res Sport Exerc. 2017:382–396.
26. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134–2156. doi:10.1111/1475-6773.12117
27. Creswell JW, Clarke VLP. Choosing a mixed methods design. In: Designing and Conducting Mixed Methods Research. 2007:58–89.
28. Robson C, McCartan K. Psychological Methods” Research & Statistics. Real World Res. 2016;1;560.
29. Ryan TP. Sample Size Determination and Power.
30. Kvale S, Brinkmann S. Interview: Det Kvalitative Forskningsinterview Som Håndværk. 3. Hans Reitzels Forlag; 2015.
31. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
32. QSR International. NVivo Qualitative Data Analysis Software; 1999. Available from: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home?fbclid=IwAR1KzvQHW9oLB6tLf2lsk0s7SCiEQw1Ki60twke-YLDf71hd6dEiAV_fNls.
33. Smith B, Sparkes AC. Routledge Handbook of Qualitative Research in Sport and Exercise. Routledge; 2016.
34. Koch L, Vallgårda S. Forskningsmetoder i Folkesundhedsvidenskab. 3. udgave. Munksgaard; 2007.
35. Braun V, Weate P. Using thematic analysis in sport and exercise research. In: Smith B, editors. Routledge Handb Qual Res Sport Exerc. 2017:191–205.
36. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
37. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Heal. 2019;11(4):589–597. doi:10.1080/2159676x.2019.1628806
38. Braun F. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134–2156. doi:10.1111/1475-6773.12117
39. World Medical Association. No. WMA Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects. The World Medical Association; 2018.
40. Aeldreministeriet S. Komiteloven; 2003. Available from: https://www.retsinformation.dk/eli/lta/2003/402.
41. Demeyer H, Mohan D, Burtin C, et al. Objectively measured physical activity in patients with COPD: recommendations from an international task force on physical activity. Chronic Obstr Pulm Dis. 2021;8(4):528–550. doi:10.15326/JCOPDF.2021.0213
42. Janaudis-Ferreira T, Tansey CM, Harrison SL, et al. A Qualitative study to inform a more acceptable pulmonary rehabilitation program after acute exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2019;16(9):1158–1164. doi:10.1513/AnnalsATS.201812-854OC
43. Early F, Wellwood I, Kuhn I, et al. P212 Interventions to increase referral to and uptake of pulmonary rehabilitation programmes for people with chronic obstructive pulmonary disease (COPD): a systematic review. Thorax. 2016;71(Suppl3):A200–A201. doi:10.1136/thoraxjnl-2016-209333.355
44. Jones AW, Taylor A, Gowler H, O’Kelly N, Ghosh S, Bridle C. Systematic review of interventions to improve patient uptake and completion of pulmonary rehabilitation in COPD. ERJ Open Res. 2017;3(1):89. doi:10.1183/23120541.00089-2016
45. Reicher S, Sela T, Toren O. Using telemedicine during the COVID-19 pandemic: attitudes of adult health care consumers in Israel. Front Public Heal. 2021;9(May):1–11. doi:10.3389/fpubh.2021.653553
46. Polgar O, Patel S, Walsh JA, et al. Digital habits of pulmonary rehabilitation service-users following the COVID-19 pandemic. Chron Respir Dis. 2022;19:1–3. doi:10.1177/14799731221075647
47. Bhaskar SMM, Michel J, Walmore N, et al. Article 831762 2 Veterans Rural Health Resource Center-Salt Lake City (VRHRC-SLC), Office of Rural Health, Veterans Health Administration. World Journal of Clinical Cases. 2022;10(27):9602–9610. doi:10.3389/fpubh.2022.831762
48. Inskip JA, Lauscher HN, Li LC, et al. Patient and health care professional perspectives on using telehealth to deliver pulmonary rehabilitation. Chron Respir Dis. 2018;15(1):71–80. doi:10.1177/1479972317709643
49. Emme C, Mortensen EL, Rydahl-Hansen S, et al. The impact of virtual admission on self-efficacy in patients with chronic obstructive pulmonary disease - a randomised clinical trial. J Clin Nurs. 2014;23(21–22):3124–3137. doi:10.1111/jocn.12553
50. Slevin P, Kessie T, Cullen J, Butler MW, Donnelly SC, Caulfield B. Exploring the potential benefits of digital health technology for the management of COPD: a qualitative study of patient perceptions. ERJ Open Res. 2019;5(2):00239–2018. doi:10.1183/23120541.00239-2018
51. Shanmugasegaram S, Oh P, Reid RD, McCumber T, Grace SL. A comparison of barriers to use of home- versus site-based cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2013;33(5):297–302. doi:10.1097/HCR.0b013e31829b6e81
52. Mohebi S, Parham M, Sharifirad G, Gharlipour Z. Social support and self care behavior study. Int J Med. 2018:1–6. DOI:10.4103/jehp.jehp
53. Carter SM, Justifying Knowledge LM, Method J. Taking action: epistemologies, methodologies, and methods in qualitative research. Qual Health Res. 2007;17(10):1316–1328. doi:10.1177/1049732307306927
54. O’Cathain A, Murphy E, Nicholl J. The quality of mixed methods studies in health services research. J Health Serv Res Policy. 2008;13(2):92–98. doi:10.1258/JHSRP.2007.007074
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Singing on Symptoms in Stable COPD: A Systematic Review and Meta-Analysis
Fang X, Qiao Z, Yu X, Tian R, Liu K, Han W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2893-2904
Published Date: 14 November 2022
Exploring the Presence of Implicit Bias Amongst Healthcare Professionals Who Refer Individuals Living with COPD to Pulmonary Rehabilitation with a Specific Focus Upon Smoking and Exercise
Barradell AC, Robertson N, Houchen-Wolloff L, Singh SJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1287-1299
Published Date: 21 June 2023
Can Blood Biomarkers Be Used to Assess Oxidative Stress in COPD Patients After Pulmonary Rehabilitation
Beykumül A, Ersoy Y, Gülbaş G, Neselioglu S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2179-2186
Published Date: 5 October 2023
Advocating for Action: Exploring the Potential of Virtual Reality in Breathing Exercise – A Review of The Clinical Applications
Alhammad SA
Patient Preference and Adherence 2024, 18:695-707
Published Date: 19 March 2024
Delivery of Remote Pulmonary Rehabilitation: COVID-19 Service Evaluation in England
Ellis J, Gilworth G, Morgan T, Harris K, King N, White P
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:533-538
Published Date: 5 March 2025