Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Psychological Distress and Disordered Eating in Adults Attending an Obesity Outpatient Clinic
Authors Cyranka K, Zych Z, Cyganek K ![]() , Małecki MT, Styczeń K, Pietruś M
, Małecki MT, Styczeń K, Pietruś M ![]() , Dudek D, Klupa T, Matejko B
, Dudek D, Klupa T, Matejko B
Received 16 January 2026
Accepted for publication 27 May 2026
Published 8 June 2026 Volume 2026:19 594879
DOI https://doi.org/10.2147/DMSO.S594879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Donald McClain
Katarzyna Cyranka,1– 3 Zofia Zych,4 Katarzyna Cyganek,3,5 Maciej T Małecki,3,5 Krzysztof Styczeń,2,3 Martyna Pietruś,1,3 Dominika Dudek,2,3 Tomasz Klupa,3,6 Bartłomiej Matejko1,3,6
1Psychodiabetology Unit, Department of Metabolic Diseases, Jagiellonian University Medical College, Krakow, Poland; 2Department of Psychiatry, Jagiellonian University Medical College, Krakow, Poland; 3University Hospital in Krakow, Krakow, Poland; 4Student Scientific Association of Diabetology, Jagiellonian University Medical College, Krakow, Poland; 5Department of Metabolic Diseases, Jagiellonian University Medical College, Krakow, Poland; 6Center for Advanced Technologies in Diabetes, Department of Metabolic Diseases, Jagiellonian University Medical College, Krakow, Poland
Correspondence: Katarzyna Cyranka, Email [email protected]
Introduction: Obesity is recognized as a major global health challenge and is associated not only with metabolic complications but also with substantial psychological consequences. The bidirectional relationship between obesity and mental disorders—such as depression, anxiety, and maladaptive eating behaviors—plays a critical role in the development, maintenance, and treatment resistance of obesity. This study aimed to examine the psychological dimensions of obesity and to emphasize their clinical relevance in comprehensive obesity care.
Methods: The study was conducted between January and December 2024 at the Obesity Treatment Outpatient Clinic of the University Hospital in Krakow. Psychological parameters were assessed in 48 adults with obesity using standardized psychometric instruments, including the WHO-5 Well-Being Index, the Quick Inventory of Depressive Symptomatology (QIDS), the Eating Attitudes Test-26 (EAT-26), and the KO “O” Symptom Questionnaire.
Results: Moderate to very severe depressive symptoms were identified in 54.2% (n = 26) of participants, while 62.5% (n = 30) met the WHO-5 criteria for poor psychological well-being and reduced quality of life. An elevated risk of disordered eating behaviors was observed in 43.8% (n = 21) of the study population, with 14.6% (n = 7) meeting criteria indicative of a full eating disorder. Anxiety symptom severity was significantly associated with glycated hemoglobin (HbA1c) levels and percent body fat, highlighting links between emotional distress and metabolic regulation in individuals with obesity.
Conclusion: The results highlight the need for an integrated, multidisciplinary approach to obesity treatment that addresses both metabolic and psychological dimensions of the disease. Given the high prevalence of affective symptoms and disordered eating patterns, incorporating structured psychological and behavioral interventions—such as strategies targeting emotion regulation, eating behaviors, and adherence to medical, nutritional, and physical activity recommendations—should be considered an essential component of standard obesity care to improve both clinical outcomes and patient well-being.
Keywords: obesity, depression, anxiety, eating disorders, BMI
Introduction
Obesity is a complex, multifactorial chronic disease associated with numerous medical complications and progressive organ damage. Its consequences extend far beyond physical health, exerting a substantial impact on psychological functioning, emotional well-being, and overall quality of life. Recognized as a major public health challenge, obesity has reached epidemic proportions worldwide, with prevalence continuing to rise across all age groups. The current clinical paradigm is increasingly focusing on the critical role of overweight and obesity in the pathogenesis of metabolic dysregulation and its systemic complications. Excessive and ectopic adipose tissue distribution contributes to profound metabolic disturbances, ultimately leading to significant end-organ damage. Based on their metabolic profiles, individuals with a body mass index (BMI) exceeding 30 kg/m2 are categorized by the presence or absence of overt abnormalities as having either metabolically healthy obesity (MHO) or metabolically unhealthy obesity (MUO). MHO describes a phenotype in which excess adiposity - predominantly sequestered in the subcutaneous depot - is not associated with traditional metabolic sequelae, such as impaired glucose metabolism, type 2 diabetes, hypertension, dyslipidemia, or prothrombotic states. Nevertheless, these individuals remain at an elevated risk for cardiovascular disease and malignancy compared to their lean counterparts, albeit lower than those with the MUO phenotype. Contemporary frameworks now advocate for a transition beyond a BMI-centric diagnostic approach. These emerging standards underscore the necessity of integrating clinical parameters - specifically the waist-to-hip ratio (WHR) and the assessment of metabolic comorbidities - to facilitate a more precise diagnosis of preclinical versus clinical obesity.1,2
The pathogenesis of obesity results from a dynamic interplay of genetic, environmental, metabolic, psychological, behavioral, and iatrogenic factors. Among these determinants, emotional distress, disordered eating behaviors, and mental health disorders play a pivotal role in both the development and long-term persistence of obesity. The relationship between obesity and psychological health is inherently bidirectional: obesity increases vulnerability to mood and anxiety disorders, while these conditions may, in turn, promote weight gain through behavioral and physiological mechanisms such as emotional eating, reduced physical activity, impaired self-regulation, and neuroendocrine dysregulation.3,4
The association between obesity and depression is particularly well documented, especially in younger populations. A large meta-analysis5 demonstrated that obesity during childhood and adolescence significantly increases the risk of developing depression later in life. This relationship is mediated not only by biological mechanisms—including chronic low-grade inflammation and dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis—but also by psychosocial factors such as body image dissatisfaction, weight stigma, and social discrimination. Stigmatization frequently leads to diminished self-esteem, social withdrawal, and increased psychological distress, ultimately resulting in a marked reduction in quality of life.6,7
Beyond its psychological burden, obesity represents a major risk factor for metabolic disorders, particularly type 2 diabetes mellitus (T2DM). Excess body weight reduces the likelihood of achieving adequate glycemic control and increases the risk of chronic microvascular and macrovascular complications in both type 1 diabetes mellitus (T1DM) and T2DM.8–11 Visceral adiposity plays a central role in this process by promoting insulin resistance, systemic inflammation, and impaired glucose regulation—key mechanisms underlying the pathophysiology of T2DM.12 These complications, including cardiovascular disease, nephropathy, neuropathy, and retinopathy, substantially reduce life expectancy and further compromise quality of life.11,13 Furthermore, the interplay between obesity and its comorbidities extends beyond metabolic dysregulation to encompass a complex, bidirectional relationship with type 2 diabetes mellitus and psychological disorders.12,14 Importantly, individuals affected by both obesity and diabetes experience a disproportionately high psychological burden, with markedly elevated rates of anxiety and depressive symptoms compared with patients with either condition alone.12,14 The psychological impact of obesity—ranging from weight-related stigma to clinical depression and anxiety—often creates a self-perpetuating cycle that exacerbates metabolic decline.14 This synergistic interaction between metabolic impairment and psychological distress underscores the necessity of a multidisciplinary approach.
Disordered eating behaviors are highly prevalent among individuals with obesity and represent a major barrier to effective and sustained weight management. Conditions such as binge eating disorder (BED), emotional eating, and night eating syndrome (NES) are frequently observed and are often driven by underlying psychological distress.15,16 This close association underscores the necessity of integrating systematic psychological assessment with targeted behavioral interventions into standard obesity care. Cognitive-behavioral therapy (CBT) has demonstrated efficacy in reducing disordered eating behaviors, enhancing emotional regulation, and supporting long-term behavioral change, reinforcing the role of psychological care as a core component of obesity treatment.16
An additional psychological contributor to obesity is the persistence of nutritional misconceptions and dysfunctional relationships with food. Emotional eating, the use of food as a coping strategy for stress, and cycles of overly restrictive dieting undermine self-regulatory capacity and may contribute to hormonal dysregulation and the development of eating disorders.17,18 Effective treatment therefore requires the establishment of a strong therapeutic alliance, the application of individualized psychodietetic strategies, and behavioral interventions aimed at modifying dysfunctional beliefs, improving coping skills, and promoting sustainable eating patterns.19
Despite advances in pharmacological and surgical treatment options, long-term weight loss remains difficult to maintain. Conventional treatment approaches often fail to adequately address behavioral and psychological determinants of eating and activity patterns, resulting in high rates of weight regain.17,19 Both historical and contemporary perspectives highlight the central role of psychological and behavioral mechanisms in body weight regulation and eating behavior.
Given the complex interplay between obesity, mental health, metabolic dysfunction, and health-related behaviors, a comprehensive understanding of the psychological profile of individuals with obesity is essential for the development of effective, patient-centered treatment strategies. From a clinical perspective, psychological factors are closely intertwined with everyday health behaviors—such as eating patterns, physical activity, and treatment adherence—highlighting behavioral mechanisms as key mediators between emotional distress and metabolic outcomes. Therefore, this study aims to assess depressive and anxiety symptoms, disordered eating behaviors, and their associations with metabolic parameters in patients with obesity.
Study Objectives
In July 2024, a specialized Obesity Treatment Outpatient Clinic was established within the Department of Diabetology, Internal Medicine and Metabolic Diseases at the University Hospital in Kraków. The clinic operates as a comprehensive care center providing multidisciplinary medical and psychological management for individuals diagnosed with obesity. Each patient undergoes an in-depth evaluation conducted by a multidisciplinary team comprising an internist/diabetologist, dietitian, physiotherapist, and clinical psychologist. This integrated model enables a thorough diagnostic process and the formulation of individualized treatment recommendations addressing both medical and psychological needs. Eligibility for treatment was based on the BMI-based diagnostic criteria for obesity that were standard in routine clinical practice at the time of study design (BMI ≥ 30 kg/m2). The study was designed and conducted before publication of the 2025 Commission redefining clinical obesity; therefore, the cohort was not formally classified according to the newer preclinical/clinical obesity framework.
The primary objective of this study was to evaluate selected psychological parameters in patients attending the Obesity Treatment Outpatient Clinic. Specifically, the study aimed to assess:
- quality of life,
- depressive symptoms,
- anxiety levels,
- the presence of disordered eating behaviors.
Additionally, the study sought to examine associations between obesity severity, as reflected by BMI and body composition parameters, and psychological outcomes, exploring potential relationships between metabolic status and mental health indicators.
Studied Population
Data were collected from patients treated at the Obesity Treatment Outpatient Clinic between January and December 2024 and retrospectively analysed based on medical records obtained during routine clinical visits. All patients underwent a comprehensive diagnostic assessment, including anthropometric measurements (height, weight, waist and hip circumference), blood pressure evaluation, body composition analysis using the InBody 370S device, and standard laboratory testing. Supplementary data were obtained regarding medical and family history, sociodemographic characteristics, comorbidities, and current treatments.
Psychological assessments were conducted under the supervision of a clinical psychologist; however, participation in the psychological consultation was voluntary, and not all patients elected to undergo this evaluation. The final study group consisted of 48 patients. The mean age of the study population was 46.67 years (range: 19–75; SD = 13.86; median = 44.5). The sample consisted of 35 women (72.9%) and 13 men (27.1%).
All participants received multidisciplinary care, including nutritional education, physical activity counseling, psychological support, medical consultation, and appropriate pharmacotherapy. The psychological evaluation focused on affective symptoms and disordered eating patterns, assessed using validated psychometric instruments.
Methods
During the initial clinical visit, participants completed a battery of standardized psychological questionnaires in accordance with clinical guidelines for the mental health assessment of patients with obesity and diabetes. The selected instruments were chosen to capture psychological domains relevant to both clinical management and prognosis in obesity. Because this study was embedded in routine outpatient care, brief, validated self-report tools were prioritized to enable standardized screening across the whole cohort.
The following psychometric tools were used:
- WHO-5 Well-Being Index20 – a widely applied screening instrument assessing overall psychological well-being and depressive symptoms. A total score below 13, or a response of 0 or 1 to any item, indicates reduced quality of life and possible depression.
- Quick Inventory of Depressive Symptomatology (QIDS)21 – a validated self-report measure assessing the severity of depressive symptoms. The questionnaire consists of 16 items rated on a 0–3 scale, with total scores categorized as:
- 0–5: no depression
- 6–10: mild depression
- 11–15: moderate depression
- 16–20: severe depression
- ≥21: very severe depression
- Eating Attitudes Test-26 (EAT-26)22 – a screening tool for identifying disordered eating behaviors, including binge eating, emotional eating, and restrictive eating patterns. The questionnaire comprises 26 items rated on a six-point scale, with total scores ≥20 indicating clinically significant eating pathology. We selected the EAT-26 as a brief and pragmatic screening instrument suitable for routine clinical assessment in an outpatient obesity setting; the aim of the present study was to identify the risk of maladaptive eating patterns rather than to establish a formal eating disorder diagnosis.
- KO “O” Symptom Questionnaire23 – developed by Aleksandrowicz, this instrument assesses neurotic and anxiety-related symptoms. Scores exceeding 200 in women and 180 in men indicate a high probability of an anxiety disorder.
Together, these assessments enabled a comprehensive characterization of participants’ psychological functioning and supported the exploration of associations between emotional distress, eating behaviors, and metabolic outcomes. Formal structured psychiatric interviews were not performed because the project had an observational, real-world design embedded in routine multidisciplinary care, and the psychological component was intended as standardized screening rather than diagnostic case ascertainment.
Statistical Methods
Clinical characteristics were summarized as mean ± standard deviation (SD) for normally distributed variables and as median with interquartile range (IQR) for non-normally distributed variables. Categorical variables were presented as counts and percentages.
Normality of distribution was assessed using the Shapiro–Wilk test. Comparisons between two independent groups were performed using the two-tailed Student’s t-test or Welch’s t-test for normally distributed variables, and the Mann–Whitney U-test for non-normally distributed variables. Comparisons among three groups were conducted using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test, as appropriate. Post hoc analyses were conducted using Tukey’s HSD test or pairwise t-tests with Bonferroni correction, as appropriate. Correlations between continuous variables were evaluated using Pearson’s or Spearman correlation coefficients, depending on data distribution. Associations between categorical variables were analyzed using the chi-square test. A two-sided p value < 0.05 was considered statistically significant.
All statistical analyses were performed using R software (version 4.4.2; R Foundation for Statistical Computing). Abbreviations used in the text are presented in Table 1.
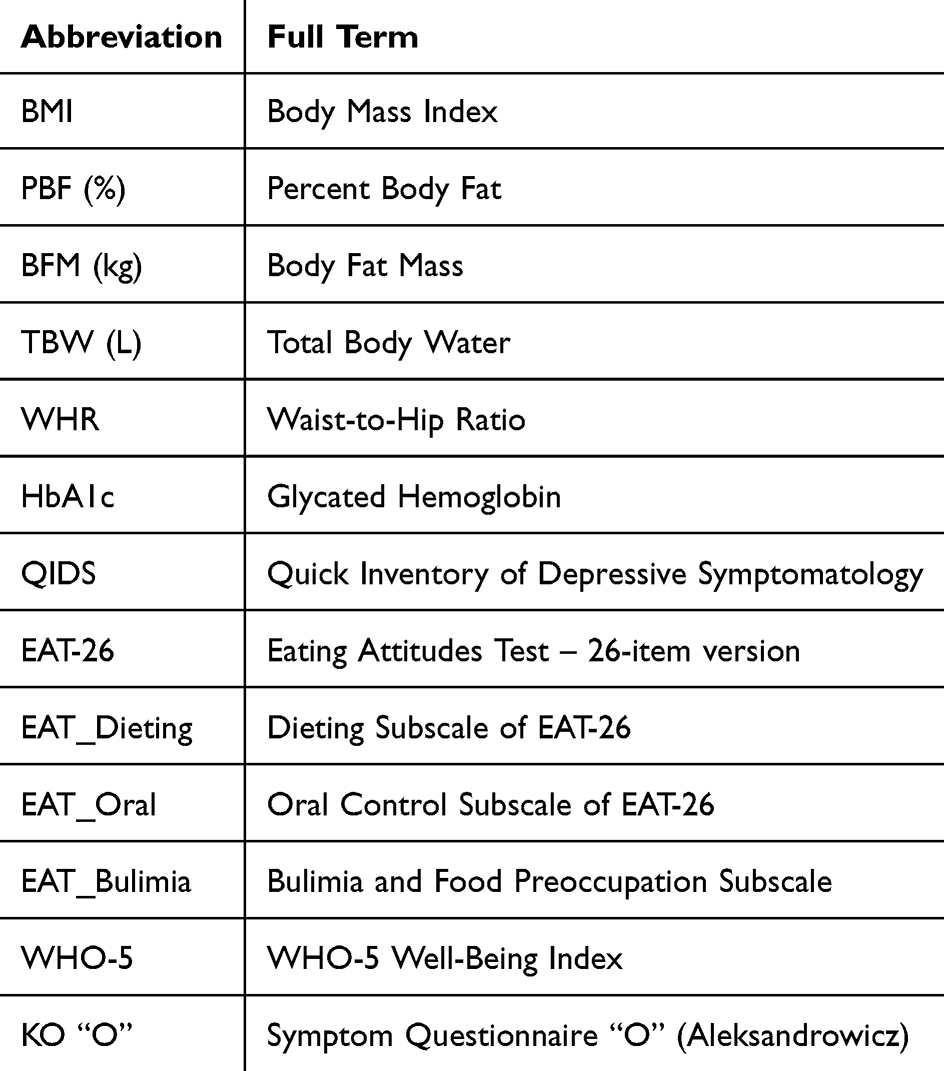 |
Table 1 Abbreviations Used in the Text |
Results
Demographic and Clinical Characteristics
The mean age of the study population was 46.67 years (range: 19–75; SD = 13.86; median = 44.5). The sample consisted of 35 women (72.9%) and 13 men (27.1%).
Regarding educational attainment, 19 participants (39.6%) reported higher education, 18 (37.5%) secondary education, 3 (6.3%) vocational secondary education, and 1 participant (2.1%) primary vocational training (Table 2).
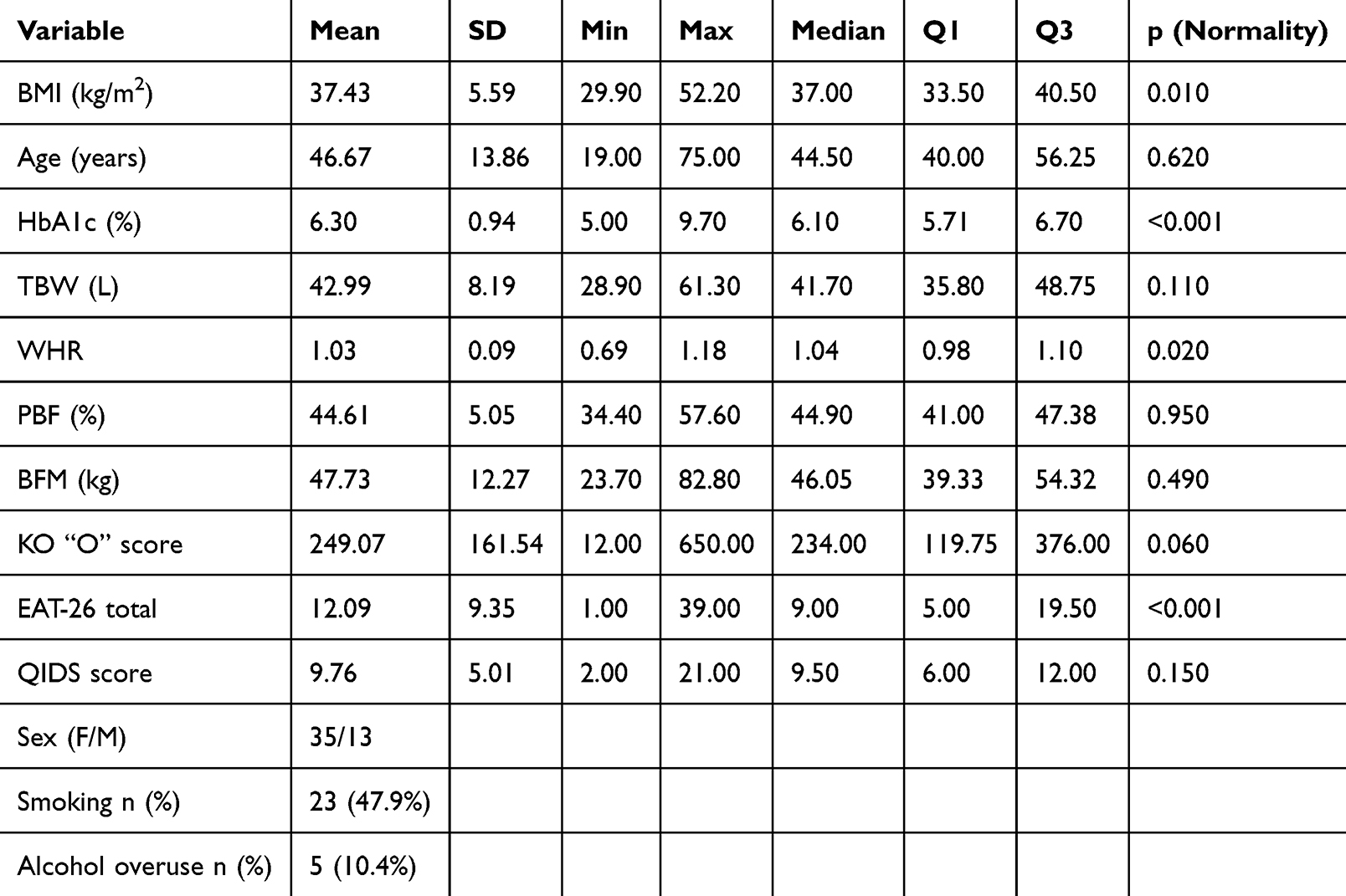 |
Table 2 Clinical and Demographic Characteristics of the Study Population (n = 48) |
The mean body mass index (BMI) was 37.4 kg/m2 (range: 29.9–52.2; SD = 5.59; median = 37.0). According to obesity classification, 19 participants (39.6%) were classified as having class I obesity, 15 (31.3%) class II obesity, and 14 (29.2%) class III obesity.
Type 2 diabetes mellitus or prediabetes was present in 31 participants (64.6%), while 17 individuals (35.4%) did not have either diagnosis.
Analysis of medical histories showed a high burden of obesity-related and other coexisting conditions. Hypothyroidism was documented in 22 participants (45.8%), while 1 participant (2.1%) had hyperthyroidism. Thirty-one participants (64.6%) had either type 2 diabetes or prediabetes, 42 (87.5%) had hypertension, and 46 (95.8%) were receiving statin therapy in relation to dyslipidemia. A history of cardiovascular disease was noted in 15 participants (31.3%), chronic kidney disease with an estimated glomerular filtration rate between 30 and 60 mL/min/1.73 m2 in 14 (29.2%), osteoarthritis in 7 (14.6%), non-alcoholic fatty liver disease in 5 (10.4%), obstructive sleep apnea in 4 (8.3%), and past malignant disease in remission in 5 (10.4%). One additional participant (2.1%) was undergoing diagnostic evaluation for suspected malignancy at the time of assessment. None of the participants was receiving chemotherapy during the study period. Because patients were cared for by different physicians, the detail and completeness of documentation regarding comorbidities varied across medical records.
With regard to pharmacotherapy, 8 participants (16.7%) were treated with liraglutide (Saxenda), 5 (10.4%) with oral semaglutide (Rybelsus), and 2 (4.2%) with weekly semaglutide (Ozempic). A small number of participants received other agents, including tirzepatide (Mounjaro) or dipeptidyl peptidase-4 (DPP-4) inhibitors. Most patients were treated with metformin and/or sodium–glucose cotransporter-2 (SGLT2) inhibitors.
Current or past smoking was reported by 23 participants (47.9%), while alcohol overuse was reported by 5 individuals (10.4%).
Psychological Characteristics of the Study Population
Psychological assessment showed a high burden of mental health symptoms in the study group. Moderate-to-very severe depressive symptoms were present in 16 participants (33.3%), while an additional 10 participants (20.8%) reported mild symptoms. Based on the WHO-5 Well-Being Index, 30 participants (62.5%) met criteria for poor psychological well-being. Elevated risk of disordered eating behaviors (EAT-26 score ≥20) was observed in 21 participants (43.8%), including 7 individuals (14.6%) with results indicative of a full eating disorder. More than half of both women and men exceeded the KO “O” threshold suggestive of clinically relevant anxiety or neurotic symptoms (Table 3).
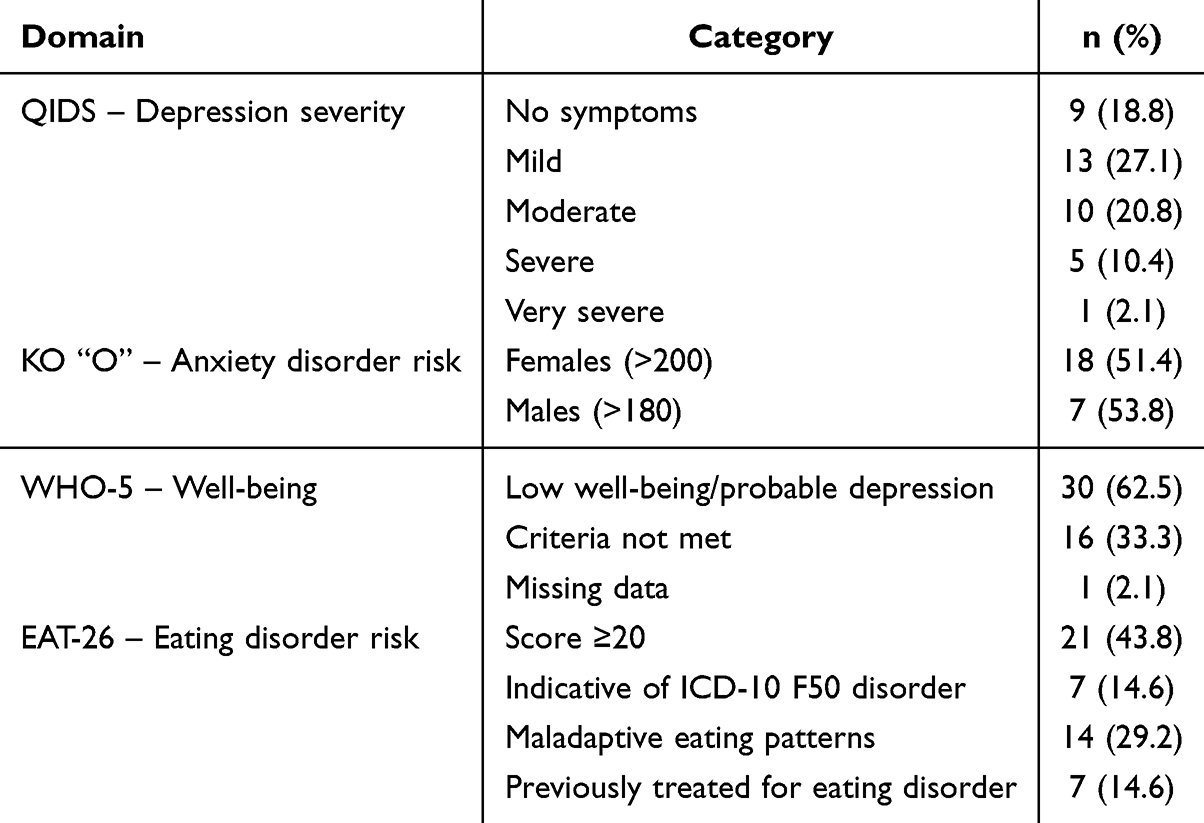 |
Table 3 Psychological Characteristics of the Study Population |
Gender Differences
Statistically significant gender differences were observed in selected eating behavior measures. Women demonstrated higher total EAT-26 scores and higher scores on the dieting and oral control subscales compared with men (Table 4). Differences in total EAT-26 scores across obesity classes are shown in Figure 1. No statistically significant gender differences were identified for depressive symptoms, anxiety severity, or quality of life measures.
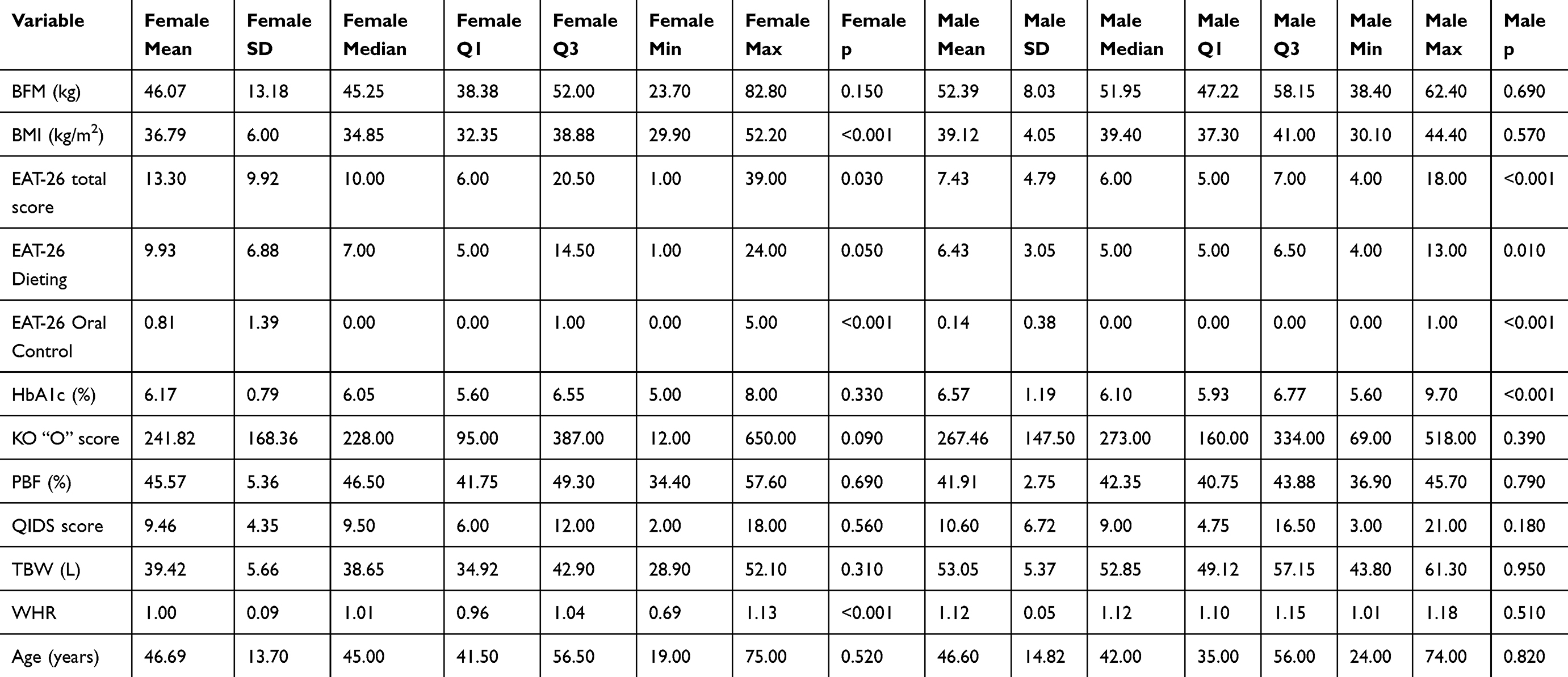 |
Table 4 Descriptive Statistics by Gender |
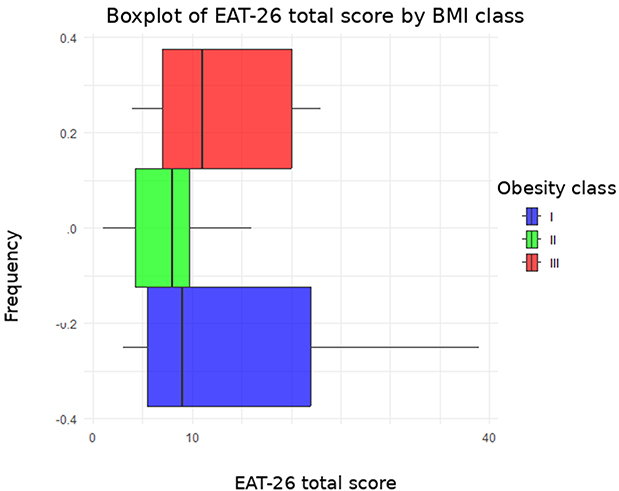 |
Figure 1 Differences in EAT-26 scores across obesity classes (I–III). The boxplot illustrates the distribution of total EAT-26 scores across obesity classes. Each box represents the interquartile range (IQR), with the median indicated by a horizontal line. Whiskers extend to values within 1.5 × IQR, and outliers are shown as individual data points. |
Associations Between Obesity Severity and Psychological Variables
No statistically significant linear correlations were observed between BMI and psychological variables when analyzed as continuous measures. However, group comparisons across obesity classes revealed differences in disordered eating patterns.
Although the overall one-way ANOVA indicated a marginally non-significant trend (p = 0.054), post hoc analyses demonstrated a statistically significant difference in total EAT-26 scores between participants with class I and class III obesity (p < 0.001). No significant associations were identified when psychological variables were analyzed using clinically relevant categorical cut-off scores (WHO-5, EAT-26, KO “O”, QIDS) (Table 5).
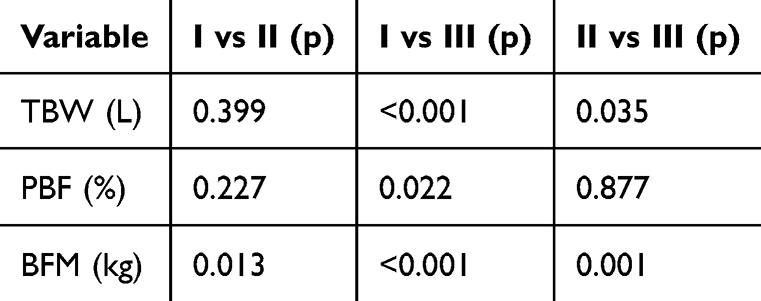 |
Table 5 Post Hoc Comparisons Between Obesity Classes |
Psychological Symptoms and Metabolic Parameters
Anxiety symptom severity was positively correlated with percent body fat (ρ = 0.39, p = 0.01) and glycated hemoglobin (HbA1c) levels (ρ = 0.35, p = 0.02). No statistically significant correlations were observed between depressive symptom severity and metabolic parameters.
Discussion
The findings of this study corroborate existing evidence demonstrating a strong association between obesity and mental health disorders, particularly depression, anxiety, and maladaptive eating behaviors. The high prevalence of affective symptoms observed in this cohort underscores the clinical relevance of psychological distress as an integral component of obesity rather than a secondary or incidental feature. These results further support the bidirectional nature of the obesity–mental health relationship, whereby psychological difficulties may contribute to weight gain and may also be exacerbated by obesity-related biological, social, and behavioral factors.
Although linear correlations between BMI and psychological variables were not statistically significant, analyses stratified by obesity class suggested greater psychological vulnerability with increasing obesity severity. Participants with class III obesity presented with higher levels of disordered eating behaviors, indicating that severe obesity may be accompanied by more complex and entrenched behavioral patterns. This observation is consistent with the concept of obesity as a progressive condition in which psychological and behavioral complications may intensify over time. The high prevalence of comorbid conditions observed in this cohort further supports the conceptualization of obesity as a systemic disease affecting multiple organ systems rather than a condition defined solely by BMI.
Importantly, the associations observed in this study between anxiety symptom severity and metabolic parameters—particularly HbA1c and percent body fat—suggest that psychological factors may influence metabolic outcomes through behavioral and psychophysiological pathways. Potential mechanisms include emotional eating, reduced adherence to treatment recommendations, avoidance of physical activity, and stress-related neuroendocrine dysregulation. From a clinical perspective, these findings provide a rationale for integrating structured psychological and behavioral interventions into obesity treatment, not only to improve mental well-being but also to support metabolic stability.
Interpersonal psychotherapy (IPT) has been proposed as a potentially useful intervention in obesity management, particularly among individuals presenting with emotional eating or binge-eating symptoms. A systematic review by Toledo et al24 demonstrated that IPT can reduce binge-eating episodes and improve emotion regulation, thereby facilitating treatment engagement. At the same time, behavioral and psychological interventions in obesity are not interchangeable and should not be treated as a single uniform category. Depending on the clinical presentation, different interventions may target distinct problems, such as emotional eating, loss of control over eating, reduced self-regulation, low mood, anxiety, or difficulties adhering to medical, nutritional, and physical activity recommendations. Our findings support the need for individualized, multidisciplinary care models that match the psychological needs of patients to the most appropriate intervention targets.
The high prevalence of disordered eating behaviors identified in this study further supports the central role of behavioral mechanisms in obesity persistence. Consistent with previous observations,25 a substantial proportion of individuals with obesity demonstrate eating patterns linked to impulse dysregulation and emotion-focused coping. Elevated EAT-26 scores in our cohort indicate that binge eating, restrictive dieting, and loss of control over food intake represent key targets for intervention. Evidence-based psychotherapeutic approaches, particularly cognitive-behavioral therapy (CBT), may strengthen self-regulation, enhance emotion management, and reduce reliance on maladaptive eating behaviors, supporting long-term weight management.
Notably, EAT-26 scores across obesity classes showed greater heterogeneity and higher values in individuals with class III obesity. This finding underscores the psychological complexity of severe obesity and supports the need for stratified treatment approaches rather than uniform behavioral recommendations. Patients with more advanced obesity may require more intensive and individualized psychological interventions addressing entrenched behavioral patterns and emotional vulnerabilities.
Anxiety symptoms emerged as a clinically important factor affecting both quality of life and metabolic outcomes. In line with a prior meta-analysis,26 more than half of participants exceeded clinical thresholds for anxiety risk. Anxiety-related avoidance behaviors—such as reluctance to engage in physical activity, inconsistent healthcare utilization, or emotional withdrawal—may undermine treatment effectiveness, particularly in the context of weight stigma and fear of negative evaluation. As emphasized by Kolotkin et al,13 quality of life in obesity is shaped not only by physical limitations but also by internalized stigma, body dissatisfaction, and societal pressure.
Collectively, these findings reinforce the need for treatment models that move beyond traditional weight-loss paradigms focused solely on caloric restriction and physical activity.17 Effective obesity management should prioritize systematic psychological assessment, emotional resilience, behavioral self-regulation, and sustainable coping strategies as core therapeutic targets. Future research should focus not only on identifying obesity subtypes based on psychological and behavioral profiles but also on clarifying which intervention components are most effective for specific clinical presentations within multidisciplinary obesity care. These findings are also consistent with the emerging concept of obesity-related distress and obesity burnout, which highlights the disease-specific emotional burden associated with living with obesity and may help to better frame psychological difficulties observed in clinical practice.27
Pharmacological treatment of anxiety and depressive disorders may be necessary in a subset of patients with obesity.28 However, careful consideration of psychotropic medication profiles is essential, as certain agents may adversely affect body weight. Clinicians should preferentially select medications with neutral or weight-reducing effects (eg., fluoxetine, bupropion, agomelatine, moclobemide, vortioxetine) while avoiding agents associated with weight gain (eg., paroxetine, citalopram, clomipramine, amitriptyline, mianserin, mirtazapine, fluvoxamine). Particular caution is warranted when prescribing anxiolytics or sedative medications, including benzodiazepines, Z-drugs, and gabapentinoids (eg., pregabalin, gabapentin), which may exacerbate weight gain and negatively interact with behavioral patterns common in obesity, such as impulsivity, emotional dysregulation, and compulsive eating. Overall, these findings further underscore the need for integrated behavioral and psychiatric care in comprehensive obesity management.
Limitations
Several limitations should be acknowledged. First, the relatively small sample size and recruitment from a specialized obesity outpatient clinic may limit the generalizability of the findings and introduce selection bias, as many participants had experienced unsuccessful prior treatment attempts. Second, psychological assessments were based on self-report questionnaires, which may overestimate symptom prevalence. Nevertheless, self-report measures capture subjective distress and perceived functional impairment—central dimensions of psychological burden and quality of life in obesity. Third, the study was designed and conducted before publication of the 2025 clinical obesity framework. Consequently, participants were classified according to the BMI-based diagnostic approach used in routine clinical practice at that time, and the cohort was not formally reclassified according to the newer preclinical/clinical obesity model. Finally, the exploratory statistical approach and multiple testing warrant cautious interpretation of secondary associations, despite correction applied to post hoc comparisons.
Conclusions
This study supports growing evidence that psychological distress and disordered eating behaviors are highly prevalent among individuals with obesity and are associated with clinically relevant outcomes. Integrating psychological assessment and structured behavioral interventions into standard obesity care is essential to improve mental well-being and long-term treatment effectiveness. Recognizing obesity as a condition shaped by biological, psychological, and social factors is critical for developing personalized and sustainable treatment strategies.
Data Sharing Statement
The data supporting the findings of this study are not publicly available due to privacy and ethical restrictions but may be obtained from the corresponding author upon reasonable request.
Statement of Ethics
The study was approved by the Ethics Committee of the Jagiellonian University Medical College (approval no. 118.0043.1.111.2025). All procedures involving human participants were conducted in accordance with the ethical standards of the institutional and national research committees and with the principles of the 1964 Helsinki Declaration and its subsequent amendments. Written informed consent was obtained from all participants prior to study participation.
Author Contributions
Katarzyna Cyranka: Conceptualization, Investigation, Project administration, Writing – original draft, Writing – review & editing.
Zofia Zych: Formal analysis, Validation, Visualization, Writing – review & editing.
Maciej Małecki: Conceptualization, Writing – original draft, Writing – review & editing.
Katarzyna Cyganek: Investigation, Methodology, Writing – original draft, Writing – review & editing.
Krzysztof Styczeń: Interpretation of data, Writing – review & editing, Data curation & Formal analysis.
Martyna Pietruś: Formal analysis, Investigation, Writing – review & editing.
Dominika Dudek: Supervision, Validation, Writing – review & editing.
Tomasz Klupa: Supervision, Conceptualization, Writing – review & editing.
Bartłomiej Matejko: Formal analysis, Supervision, Validation, Writing – review & editing.
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no external funding and was conducted using data collected during routine clinical practice at the University Hospital in Kraków.
Disclosure
The authors declare no conflicts of interest.
References
1. Cho YK, Lee YL, Pathogenesis JCH. Murine models, and clinical implications of metabolically healthy obesity. Int J Mol Sci. 2022;23:9614. doi:10.3390/ijms23179614
2. Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13:221–12. doi:10.1016/S2213-8587(24)00316-4
3. Segal Y, Gunturu S. Psychological issues associated with obesity. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. PMID:38753901.
4. Milaneschi Y, Simmons WK, van Rossum EFC, Penninx BW. Depression and obesity: evidence of shared biological mechanisms. Mol Psychiatry. 2019;24(1):18–33. PMID:29453413. doi:10.1038/s41380-018-0017-5
5. Quek YH, Tam WWS, Zhang MWB, RCM H. Exploring the association between childhood and adolescent obesity and depression: a meta-analysis. Obes Rev. 2017;18(7):742–754. PMID:28401646. doi:10.1111/obr.12535
6. Kolotkin RL, Andersen JR. A systematic review of reviews: exploring the relationship between obesity, weight loss and health-related quality of life. Clin Obes. 2017;7(5):273–289. doi:10.1111/cob.12203
7. Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 2010;67(3):220–229. doi:10.1001/archgenpsychiatry.2010.2
8. Mao Y, Gau JT, Jiang N. Obesity, metabolic health, and diabetic complications in people with type 1 diabetes. Endocrinol Diabetes Metab. 2025;8(1):e70017. PMID:39679900. doi:10.1002/edm2.70017
9. Koirala S, Sunnaa M, Bernier T, Oktay AA. The role of obesity as a cardiac disease risk factor in patients with type 2 diabetes. Curr Cardiol Rep. 2024;26(11):1309–1320. doi:10.1007/s11886-024-02129-z
10. Newson RS, Divino V, Boye KS, et al. Glycemic control and obesity among people with type 2 diabetes in Europe and Australia: a retrospective cohort analysis. Diabetes Ther. 2024;15(6):1435–1449. doi:10.1007/s13300-024-01583-w
11. Moosaie F, Ghaemi F, Mechanick JI, et al. Obesity and diabetic complications: a nationwide diabetes report. Prim Care Diabetes. 2022;16(3):422–429. doi:10.1016/j.pcd.2022.03.009
12. Baliou S, Apetroaei MM, Hatzidaki E, et al. The interplay between obesity and type 2 diabetes: common pathophysiological mechanisms contributing to telomere shortening. Life. 2025;15(6):873. doi:10.3390/life15060873
13. Kolotkin RL, Zunker C, Østbye T. Obesity and quality of life: a systematic review. Obes Rev. 2012;13(11):1039–1055.
14. El-hadidy GN, Basem Y, Mokhtar MM, et al. Obesity: genetic insights, therapeutic strategies, pharmacoeconomic impact, and psychosocial dimensions. Obesities. 2025;5:86. doi:10.3390/obesities5040086
15. Herpertz-Dahlmann B, Hebebrand J. Eating disorders and obesity. Child Adolesc Psychiatr Clin N Am. 2009;18(1):xvii–xix. doi:10.1016/j.chc.2008.09.001
16. Grilo CM. Psychological and behavioral treatments for binge-eating disorder. J Clin Psychiatry. 2017;78(Suppl 1):20–24. doi:10.4088/JCP.sh16003su1c.04
17. Baile JI. Why we are not effective in the treatment of obesity? The necessary contribution of psychology. Med Clin. 2019;152(2):72–74. doi:10.1016/j.medcli.2018.06.003
18. Brosin BW. The psychology of overeating. N Engl J Med. 1953;248(23):974–975. doi:10.1056/NEJM195306042482305
19. van de Riet A, Otte RS, Jager-Wittenaar H, et al. Dietitians’ perspectives on key components of successful obesity treatment. J Hum Nutr Diet. 2025;38(1):e13387. doi:10.1111/jhn.13387
20. Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: a systematic review. Psychother Psychosom. 2015;84(3):167–176. doi:10.1159/000376585
21. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-item Quick Inventory of Depressive Symptomatology (QIDS). Biol Psychiatry. 2003;54(5):573–583. doi:10.1016/S0006-3223(02)01866-8
22. Janahi S, Alkhater N, Bucheer A, et al. Reliability generalization meta-analysis of the EAT-26. Cureus. 2024;16(11):e73647. doi:10.7759/cureus.73647
23. Konop M, Sobański JA, Klasa K, et al. Neurotic symptoms profile in a day hospital patients with an anamnesis of head injury in the past. Psychiatr Pol. 2022;56(4):805–821. English, Polish. doi:10.12740/PP/OnlineFirst/133636
24. Toledo PR, Lotufo-Neto F, Verdeli H, et al. Interpersonal psychotherapy for treatment of obesity: a meta-analysis. J Affect Disord. 2023;320:319–329. doi:10.1016/j.jad.2022.09.070
25. Hudson JI, Hiripi E, HG P Jr, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. 2007;61(3):348–358. doi:10.1016/j.biopsych.2006.03.040
26. Amiri S, Behnezhad S. Obesity and anxiety symptoms: a systematic review and meta-analysis. Neuropsychiatr. 2019;33(2):72–89. doi:10.1007/s40211-019-0302-9
27. Cyranka K, Snoek FJ, Hermanns N, Ehrmann D, Klupa T. Obesity-related distress and obesity burnout: towards a conceptual framework for disease-specific emotional burden in obesity. Diabetes Obes Metab. 2026;28:3457–3461. doi:10.1111/dom.70549
28. Haleem DJ. Drug targets for obesity and depression: from serotonin to leptin. Curr Drug Targets. 2016;17(11):1282–1291. doi:10.2174/1389450117666151209123049
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025