Back to Journals » Vascular Health and Risk Management » Volume 18
Prolonged Mechanical Ventilation Following Coronary Artery Bypass Graft in Santiago De Cali, Colombia
Authors Daza-Arana JE ![]() , Lozada-Ramos H
, Lozada-Ramos H ![]() , Ávila-Hernández DF, Ordoñez - Mora LT, Sánchez DP
, Ávila-Hernández DF, Ordoñez - Mora LT, Sánchez DP ![]()
Received 24 March 2022
Accepted for publication 24 August 2022
Published 30 September 2022 Volume 2022:18 Pages 767—781
DOI https://doi.org/10.2147/VHRM.S367108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Jorge Enrique Daza-Arana,1 Heiler Lozada-Ramos,2,3 Daniel Felipe Ávila-Hernández,1 Leidy Tatiana Ordoñez-Mora,1 Diana Patricia Sánchez1
1Physiotherapy Program, Universidad Santiago de Cali, Cali, Colombia; 2Medicine Program, Universidad Santiago de Cali, Cali, Colombia; 3Doctoral Program in Infectious Diseases, Universidad de Santander – UDES, Bucaramanga, Colombia
Correspondence: Jorge Enrique Daza-Arana, Physiotherapy Program, Universidad Santiago de Cali, Calle 5 No. 62-00 Pampalinda, Cali, Colombia, Tel +57 3108923676, Email [email protected]
Purpose: The purpose of this study was to describe factors associated with prolonged ventilatory support in subjects undergoing coronary artery bypass graft.
Patients and Methods: This was an analytical retrospective case–control study. Cases were defined as subjects requiring prolonged mechanical ventilation (> 48 hours) following isolated coronary artery bypass graft. Subjects older than 18 years who had undergone surgery were included, while subjects with missing clinical record data, subjects in coma or subjects with prior cardiac surgery were excluded. Variables were measured at the three time points surrounding surgery.
Results: A total of 204 cases and 408 controls were included. The final logistic model showed an association between prolonged mechanical ventilation and the following presurgical variables: chronic obstructive pulmonary disease (OR 1.85; 95% CI: 1.06– 3.23, p = 0.03) and chronic kidney disease (OR 1.90; 95% CI: − 3.31; p = 0.02). The associated transurgical variable was the use of intra-aortic balloon pump (OR 3.63; 95% CI: 1.73– 7.61, p = 0.00), and associated postsurgical variables were venous oxygen saturation < 60% (OR 2.00; 95% CI: 1.18– 3.40, p = 0.01), mediastinitis (OR 18.51; 95% CI: 4.06– 84.40, p = 0.00), inotrope use (OR 2.82; 95% CI: 1.77– 4.48, p = 0.00), pleural effusion requiring drainage (OR 3.57; 95% CI: 2.02– 6.32, p = 0.00) and delirium (OR 3.45; 95% CI: 1.91– 6.25, p = 0.00).
Conclusion: This study identifies factors associated with prolonged mechanical ventilation in subjects subject to coronary artery bypass graft over the presurgical, transurgical and postsurgical periods, identifying a new factor, delirium, for this type of population.
Keywords: coronary bypass, prolonged ventilatory support, risk factor, cardiac surgery, epidemiology
Introduction
Mechanical ventilation (MV) support is a therapeutic option since it provides vital support for the maintenance or substitution of the ventilatory function in subjects with different conditions, such as respiratory failure, and subjects subject to surgical procedures, such as coronary bypass or coronary artery bypass graft (CABG).1 The need for MV following this type of cardiovascular surgery results in subjects admission to intensive care units (ICUs). Respiratory support is generally removed within the first 24 hours, but some subjects may not recover immediately and may need prolonged mechanical ventilation (PMV), which is associated with different comorbidities or surgical and postsurgical complications.2
PMV is defined as any period in which patients require respiratory support for more than 21 days,3–5 although the cut-off point is controversial, and there is substantial variation in terms of terminology and defining criteria, which is why standardization of criteria is needed.6 According to the literature review, PMV in subjects subject to CABG can be defined by different ranges: >12 hours, >24 hours and >48 hours of ventilatory support.1,7,8 The latter was used for this study. PMV is considered a significant complication following cardiovascular surgery; even though its incidence levels are low, ranging from 2.9% to 8.6%,9–11 it is associated with higher morbidity and mortality rates, which is why it is still a relatively common issue.
Several studies have identified factors associated with PMV such as advanced age, left ventricular ejection fraction (LVEF) <30%, high score in the New York Heart Association (NYHA) functional classification, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), procedure duration and the performance of an emergency surgery.12–14 In addition, it is worth mentioning that PMV results in longer ICU stays, which increases the use of resources and health care costs.15
Identification of variables associated with PMV following CABG allows for the development of prevention and risk mitigation strategies aimed at reducing the adverse events of this condition and promoting early removal of the respiratory support. This results in a faster recovery and functional rehabilitation in a timelier manner.16 This study is the only of its kind in Colombia and it was conducted in a cardiovascular surgery reference center located in the Southwest region of the country with a 10-year observation period. Hence, the purpose of this research was to identify risk factors associated with PMV following CABG in Santiago de Cali, Colombia.
Patients and Methods
Subjects and Study Design
A retrospective case-control study was conducted in a high complexity healthcare institution in the city of Cali, Colombia. Subjects older than 18 years who had undergone isolated CABG from January 1 2006 and December 31 2015 were included. Subjects with missing clinical record data, subjects in coma or with prior cardiac surgery were excluded.
Cases were defined as adult subjects that had undergone CAGB and received invasive ventilatory support for more than 48 hours following surgery. Exposure variables were measured at the presurgical, transurgical and postsurgical time points. Data was collected from clinical records, clinical laboratory results, diagnostic imaging reports and perfusion and postsurgical follow-up records made by cardiovascular surgeons of the institution.
Sample size was estimated with a 95% safety level, α=0.05, and a 90% statistical potency, β=0.1, with a ratio of two controls per each PMV case. Sample sizes were estimated based on exposure values taking the study made by the US Society of Thoracic Surgeons (STS) as a reference.17 The exposure factor “being older than 75 years” resulted in a bigger sample size, with 204 cases and 408 controls, which were randomly selected from the database built by researchers, for which a simple random sampling was carried out using the EPIDAT 3.1 software; for this purpose included a total of 812 subjects. All the information about the people was processed during the period of time evaluated and included in this study for both the cases and the controls.
This study was conducted pursuant to the international recommendations for clinical research included in the Declaration of Helsinki. According to Resolution 8430 of 1993 issued by Ministerio de Salud de Colombia (Ministry of Health of Colombia), this study was classified as a risk-free research, since data was collected from secondary sources. Informed consent was not required as it was a retrospective study. This project was approved by the Research and Ethics and Bioethics Committee of the Faculty of Health “CEB-USC” (Minutes No. 01–2017) of the institution in which the study was conducted.
In this case-control study, biases were minimized as follows: The population at risk is often not defined. This situation in the study was handled properly since the population is framed in a surgical act. In this investigation, the cases and controls were selected from the cardiovascular surgery database of the reference institution, during the 10 years. It is difficult to ensure the comparability of rare risk factors. In the exploratory data analysis, the frequency of these factors was identified and exposed in the analysis of the information and results. They can frequently generate information biases, because the exposure in most cases is measured, reconstructed or quantified, after the development of the disease. In this study, when constituting the cases, the event of prolonged mechanical ventilation, this disadvantage was not presented, in addition to considering that they are incident cases. On the other hand, in the registry of the existence, dose, and time of exposure of the risk factors, a special study was made in the different sources of the clinical history to confirm the data, sources such as the daily registry of evolution, laboratory report, clinical records in physical and digitized media, and post-surgical control, which it had been observed that the institution had adequate content and quality of information.
Statistical Analysis
Concordance and statistical validation of the database, where data had been entered twice, were estimated, which allowed for the organization of data into a master database. This was followed by a descriptive analysis of the risk factors for the general population, as well as for cases and controls. This description was performed for qualitative data by distributing relative frequencies and ratios. For quantitative data, a numerical analysis of central tendency and dispersion measures was conducted.
Subsequently, the independent effect of exposure variables on the likelihood that predicted cases becoming actual cases was determined, with its respective 95% confidence interval. Bivariate case associations were then estimated, and each of the exposures of interest was calculated with a Chi² test.
A variance analysis and a correlation coefficient were used for quantitative variables. After verifying the normality of the data through the Shapiro Wilk test, student’s t-test was used to test the hypothesis of differences between sample means. Variables for the construction of the final model were identified during this step. Strength of association was measured with odds ratio (OR), with a 0.05 significance level and a 95% confidence level. The criterion used to assign a non-exposure category was based on the literature review about factors associated with the study event and/or the categories of variables with lower PMV case occurrence (Figure 1).
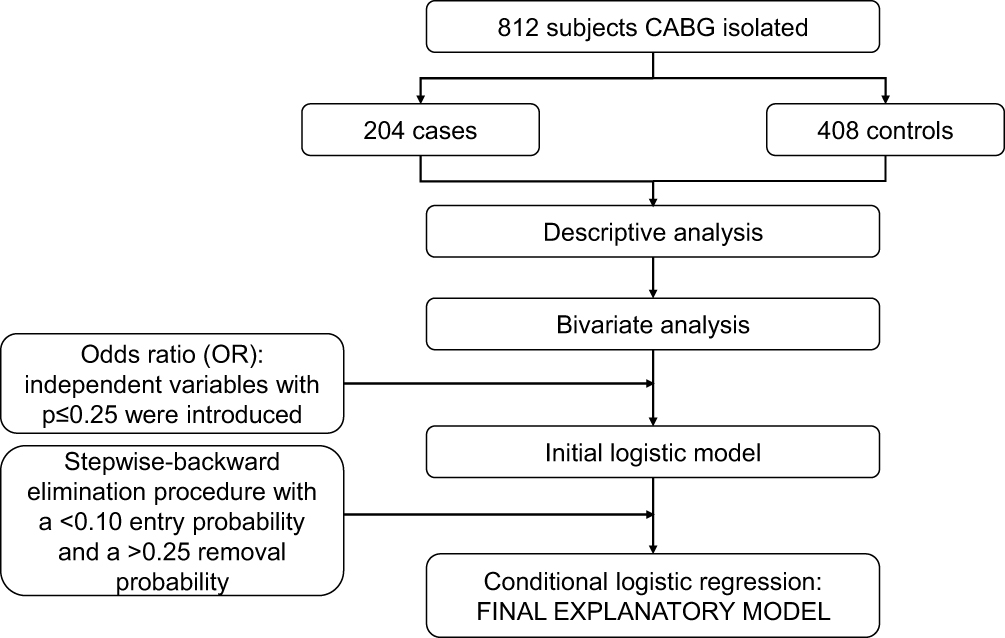 |
Figure 1 Statistical model. |
A multiple analysis was then conducted, which consisted of conditional logistic regression modeling. Based on statistical criteria, only independent variables with p≤0.25 in univariate models were introduced in the initial logistic model, through a stepwise-backward elimination procedure with a <0.10 entry probability and a >0.25 removal probability, resulting in the final explanatory model.
Confusion and interaction tests were conducted with variables from the adjusted model. The model was validated with the Hosmer-Lemeshow goodness of fit test and the likelihood ratio test. Data analysis was processed using STATA 16.0® statistical software.
Results
When comparing the exposure frequencies of the variables from the presurgical period (Table 1), a trend could be observed towards a higher average age, history of heart failure (with preserved or reduced ejection fraction), COPD, CKD, peripheral vascular disease (PVD), pulmonary hypertension, vasodilator use and ventilatory support, as well as LVEF ≤35%, kidney function with creatinine ≥2.3 mg/dL and hemoglobin ≤12 g/dL and emergency surgery. Heart valve stenoses were not considered because they were only found in 5 subjects, and they were not severe.
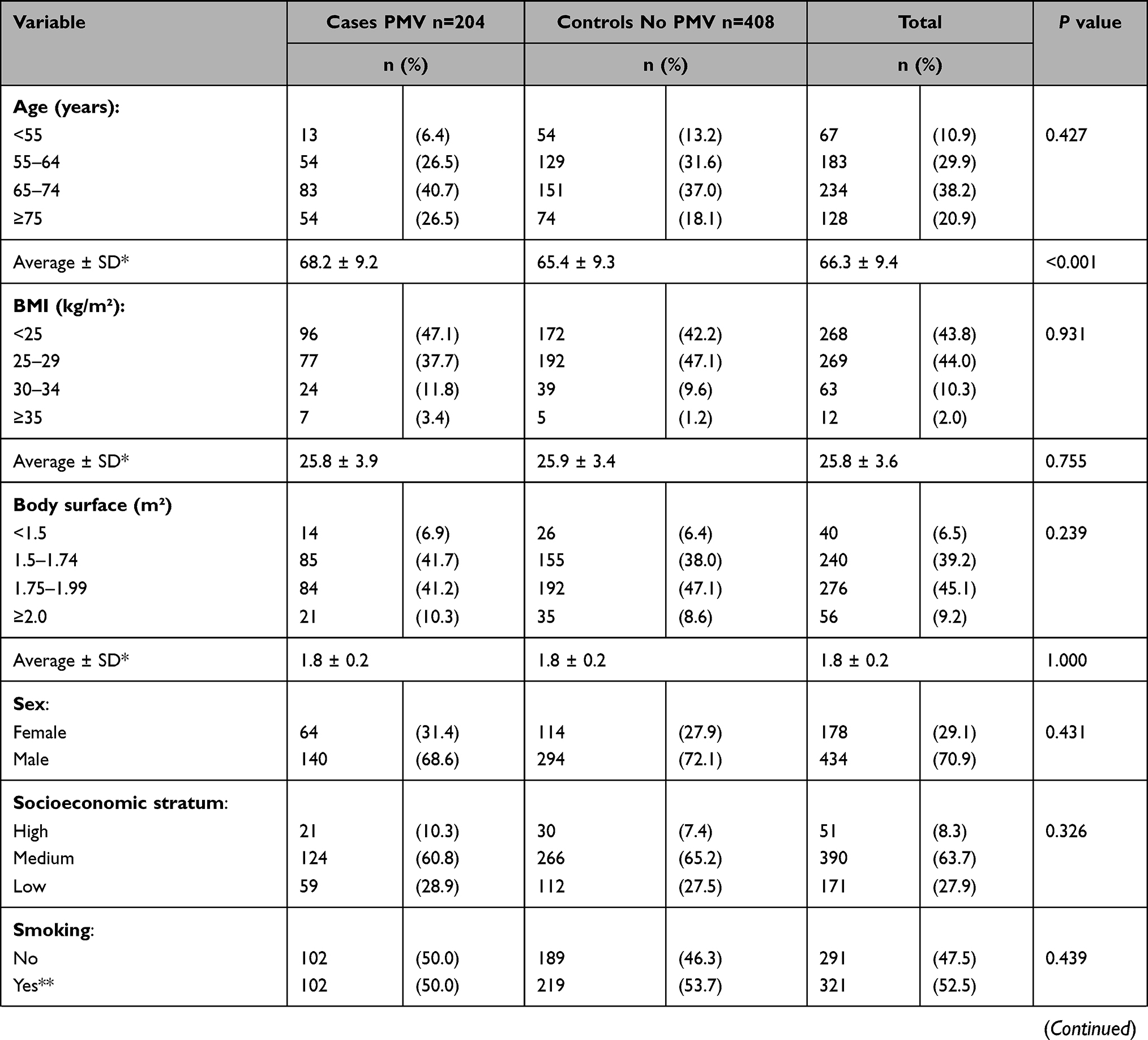 | 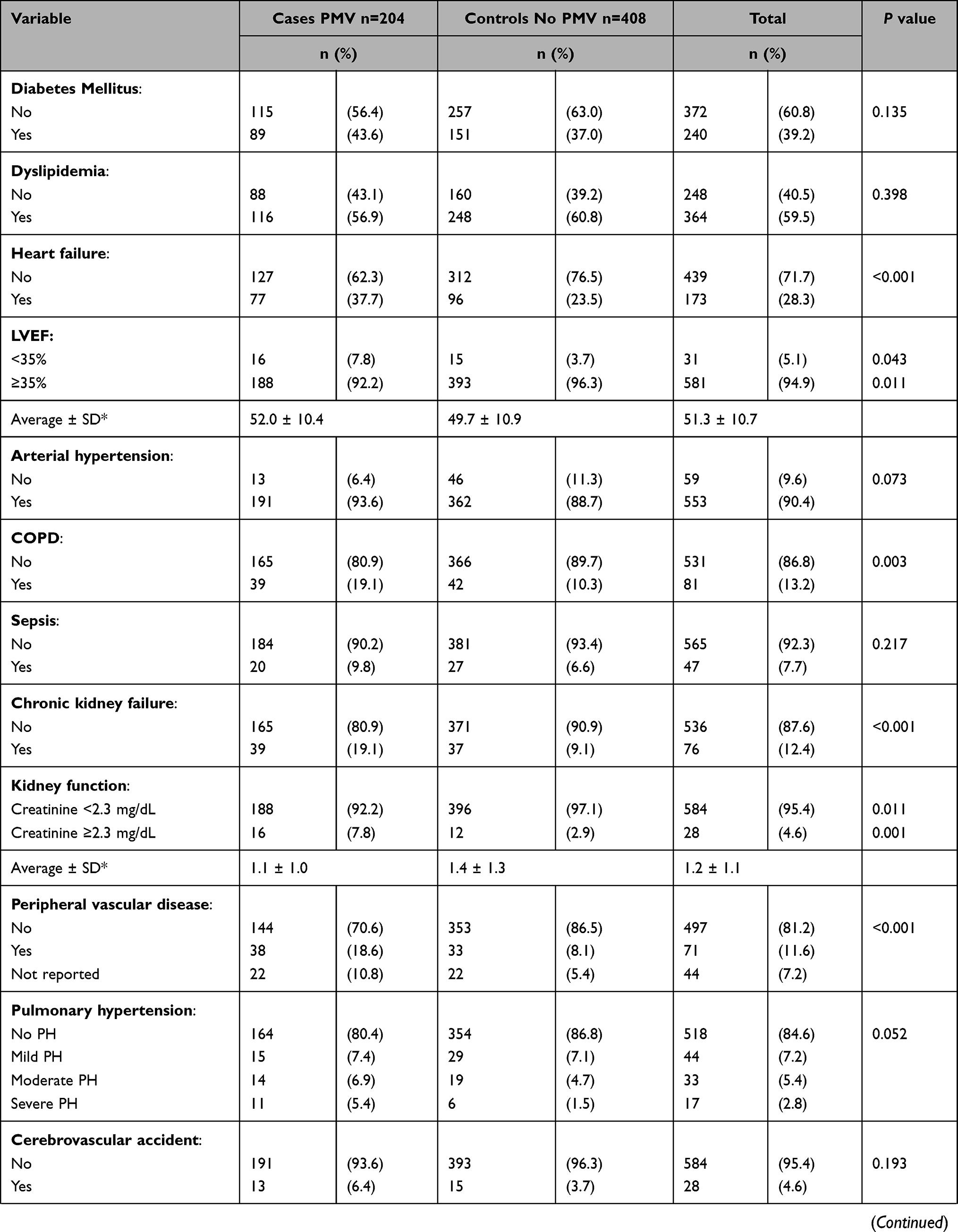 | 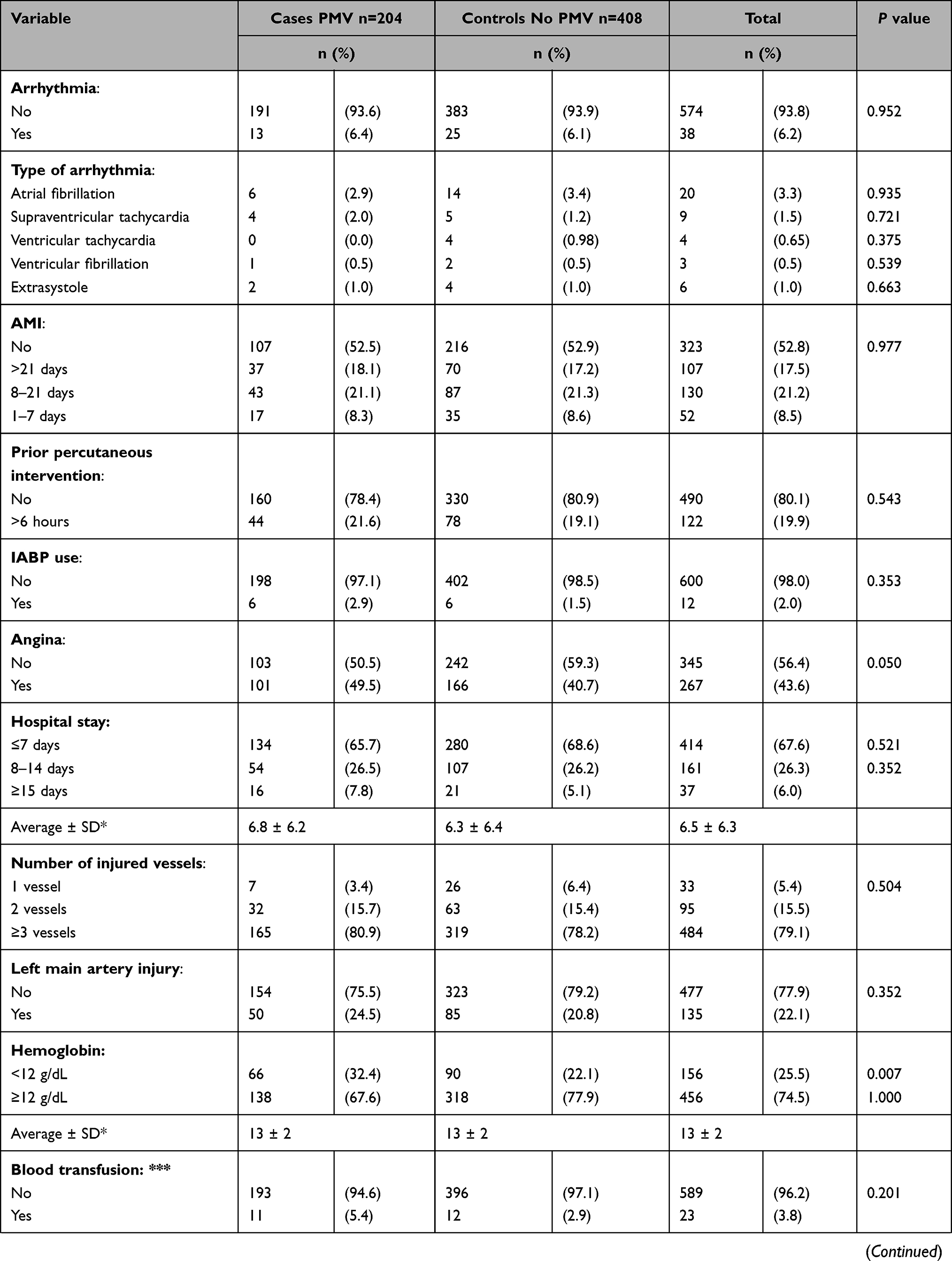 | 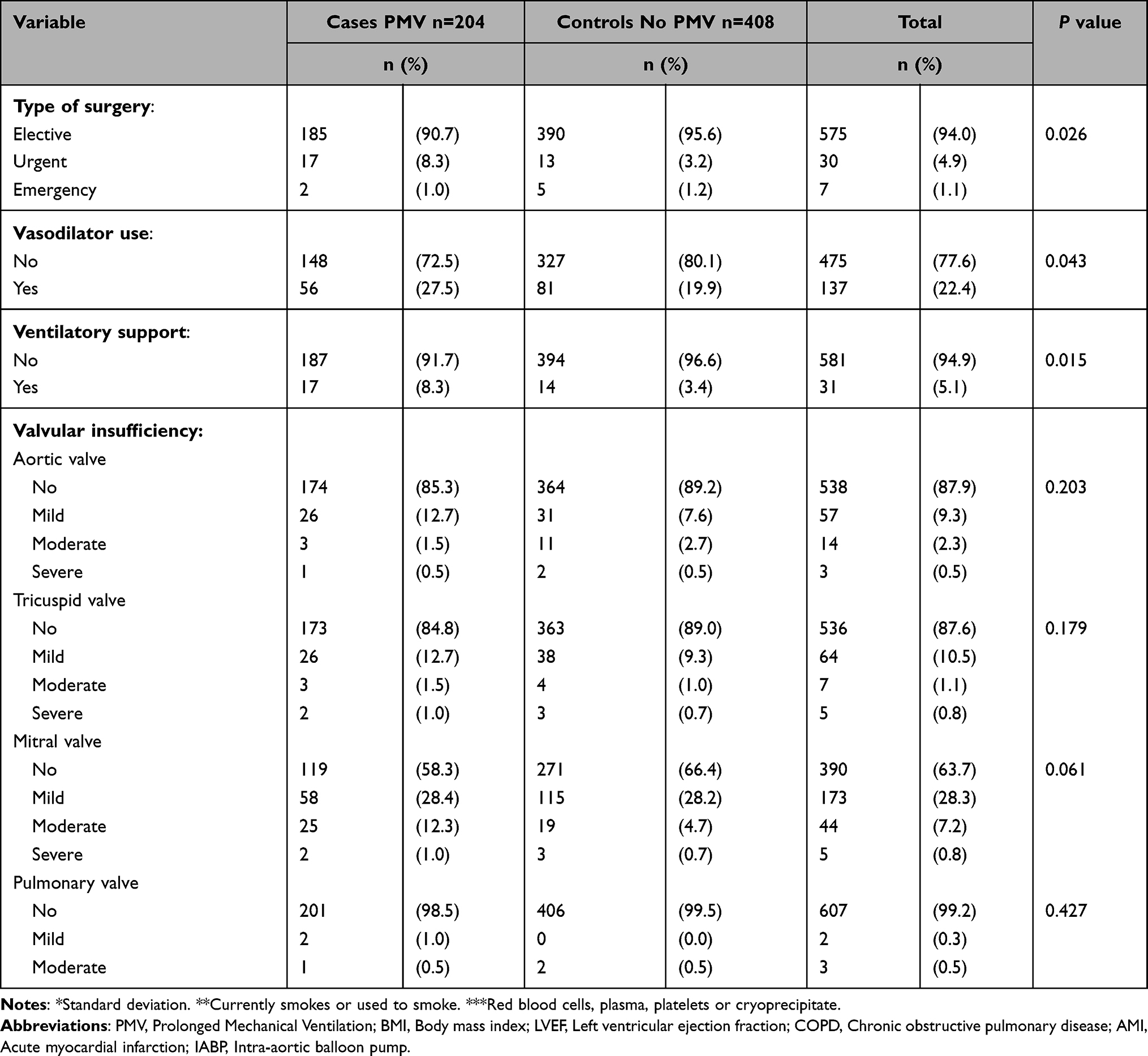 |
Table 1 Description of Presurgical Variables |
Regarding exposure factors during surgery (Table 2), subjects needing PMV showed significant differences between the average pump and ischemia times in extracorporeal circulation, higher rates of blood transfusion with ≥3 units of red blood cells, ≥2 units of plasma and ≥6 units of platelets, intra-aortic balloon pump (IABP) use, cardiogenic shock and need for vasopressor and inotropic agents.
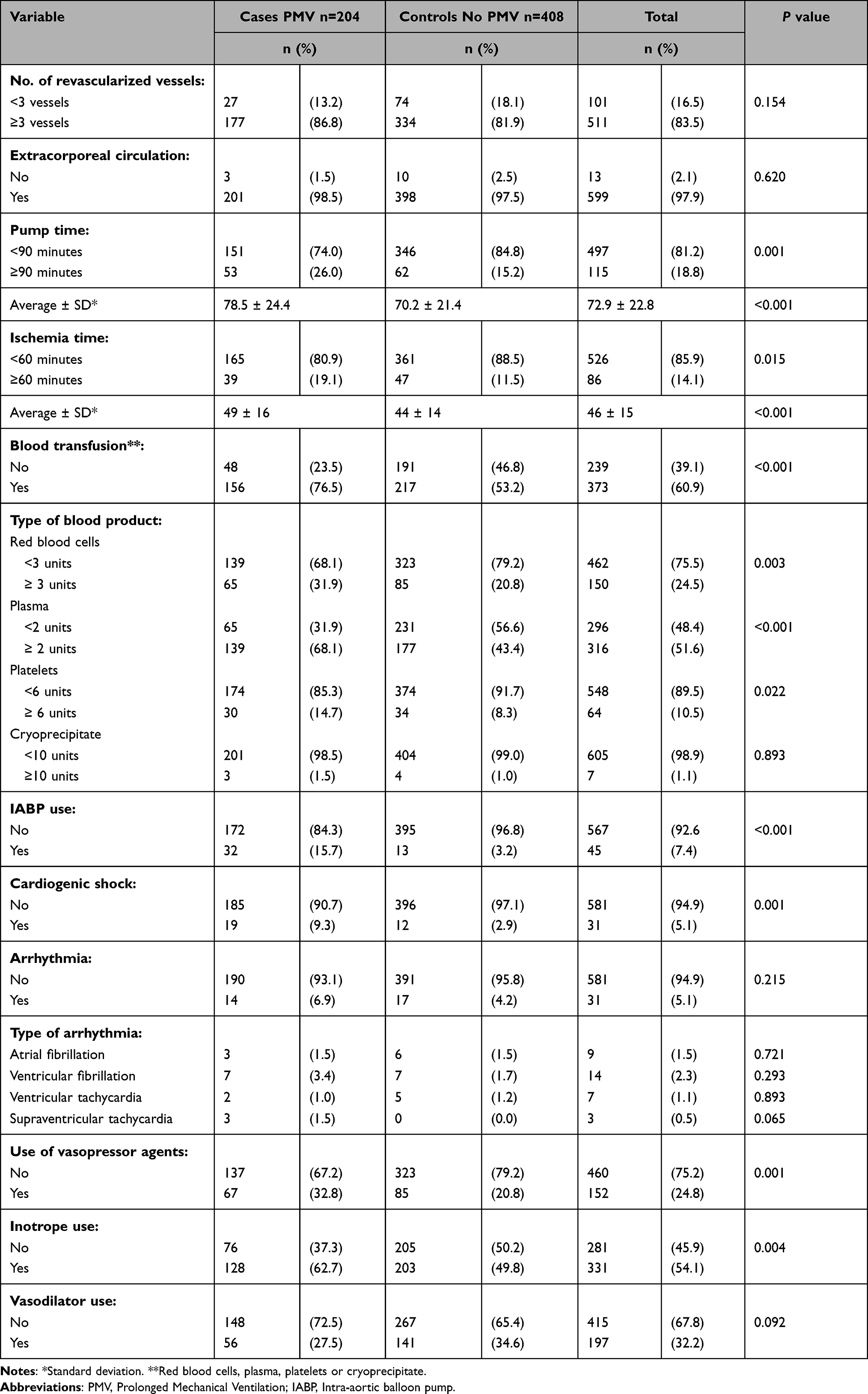 |
Table 2 Description of Transurgical Variables |
In the postsurgical period (Table 3), cases showed a higher frequency of ICU stays of >3 days, a higher need for blood transfusion with ≥3 units of red blood cells, ≥2 units of plasma, ≥6 units of platelets and ≥10 units of cryoprecipitate, need for vasopressor and inotropic agents, IABP use, presence of cardiogenic shock; arrhythmias such as atrial fibrillation and supraventricular tachycardia and venous oxygen saturation (SvO2) <60%. The majority of complications included surgical reintervention, pleural effusion requiring drainage, postsurgical bleeding, atelectasis, tracheal reintubation, pulmonary edema, delirium, bowel bleeding, sepsis, mediastinitis, coagulopathy, and acute kidney failure (definition of AKI Network) with and without dialysis (p<0.05).
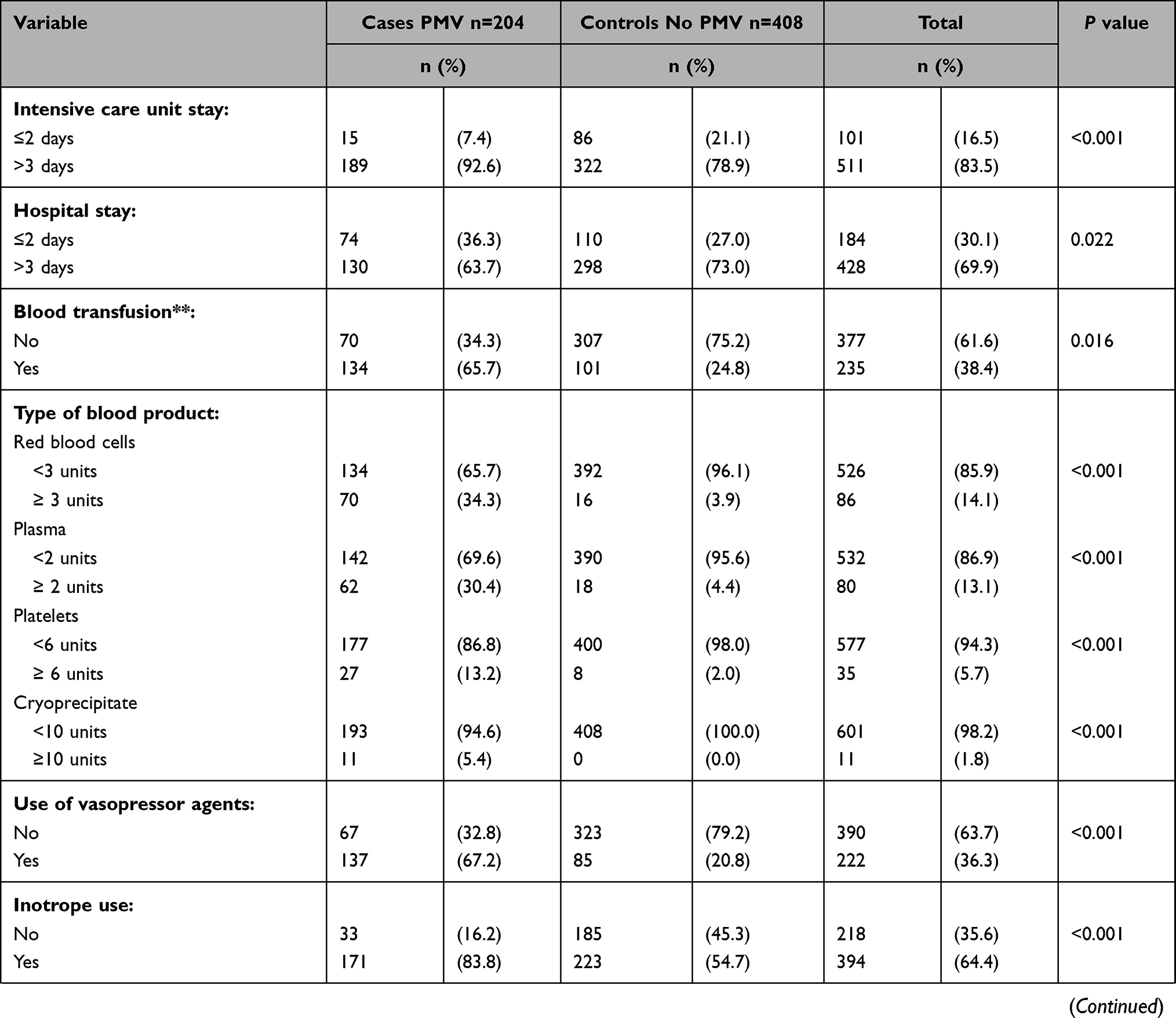 | 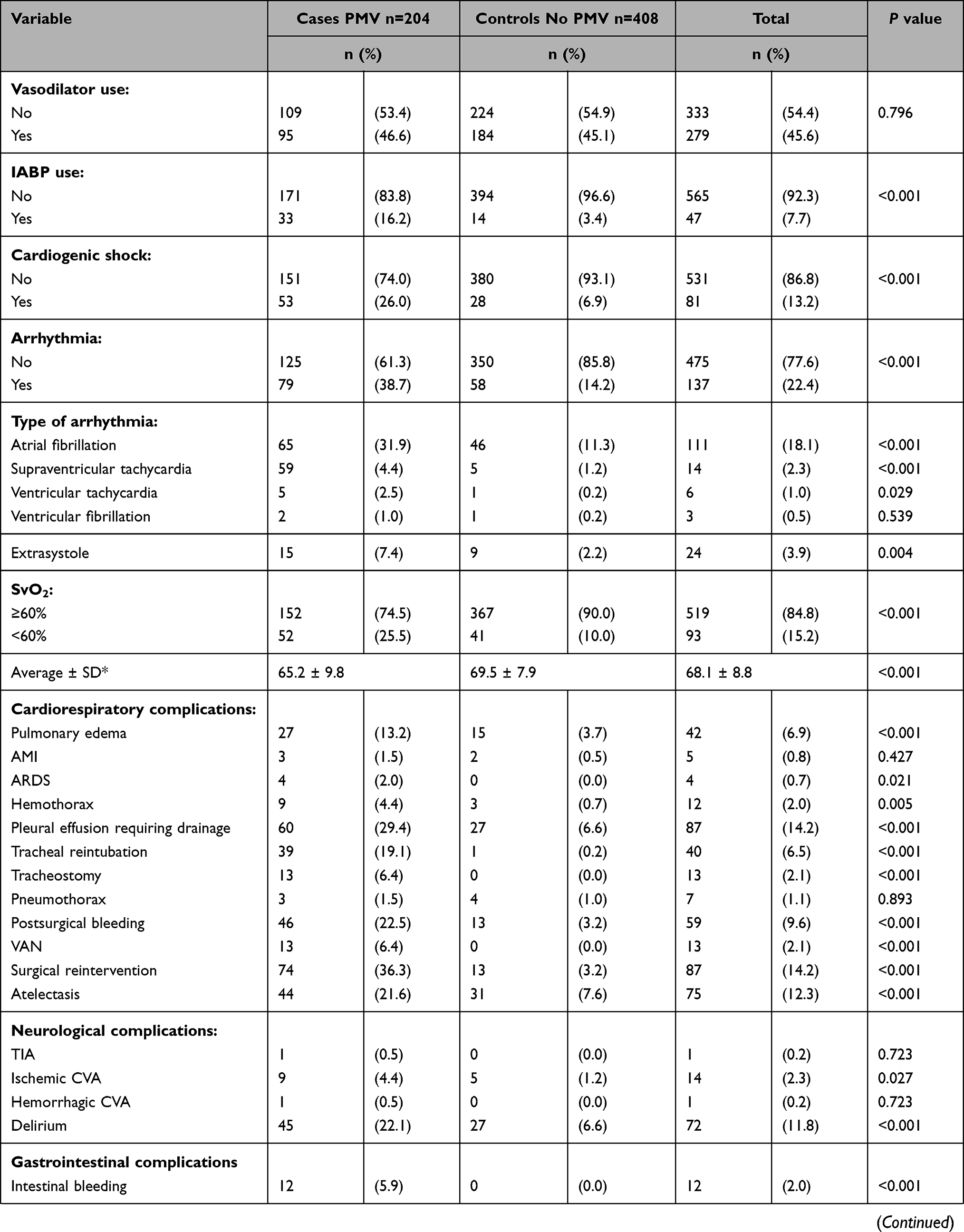 | 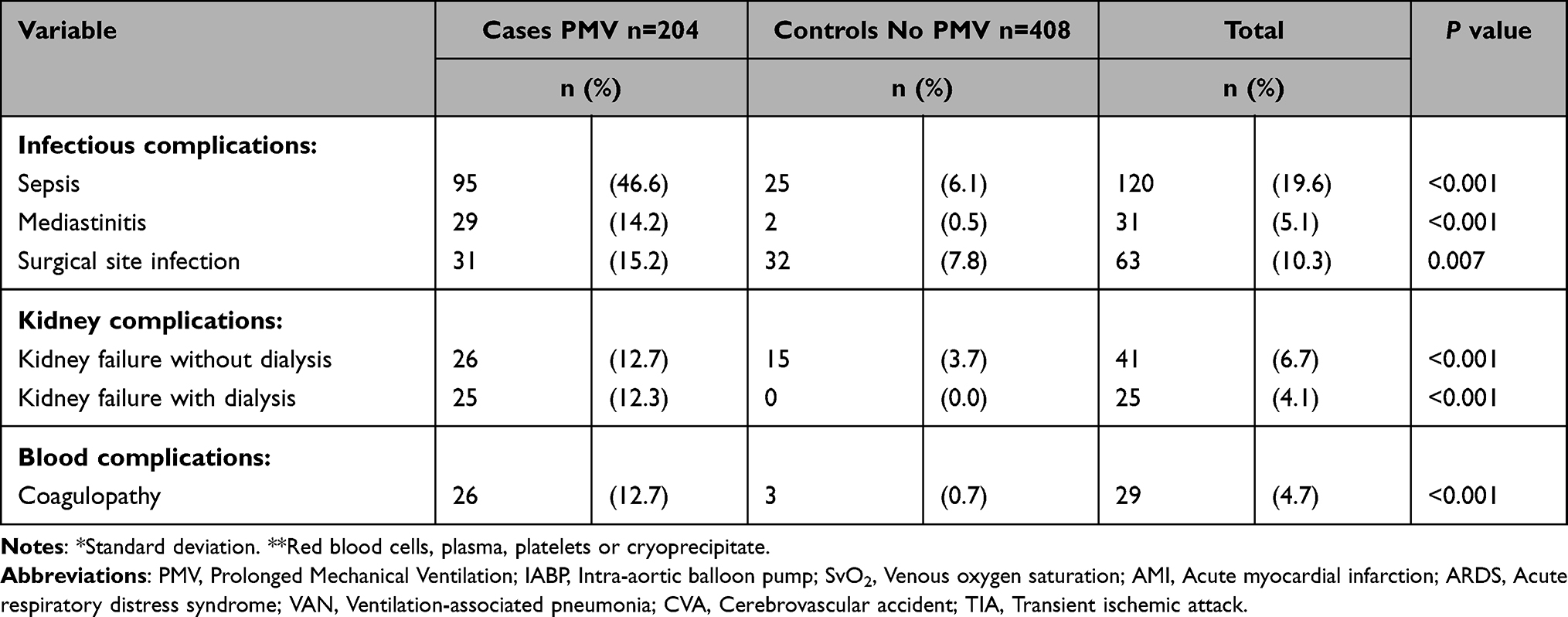 |
Table 3 Description of Postsurgical Variables |
Regarding hospital mortality (<30 days), it was more frequent among subjects receiving PMV as opposed to subjects in which ventilation was removed promptly (22.6% vs 6.1%). The main causes of death in the 46 subjects who died with PMV were sepsis (43.5%), cardiogenic shock (41.3%) and postsurgical bleeding (13%).
Different logistic models were developed based on the theoretical framework and according to statistical criteria in order to identify those variables whose statistical significance and theoretical importance allowed for the construction of the most parsimonious model. First, individual logistic models were built for each CABG stage and then the final model was developed. The presurgical model showed a statistically significant association and a higher PMV likelihood for subjects with history of CKD, PVD, COPD and heart failure.
The individual model for the transurgical stage showed pump time and IABP use as risk factors. The postsurgical model evidenced a significant association with the need for red blood cells transfusion, IABP use, SVO2 <60%, pulmonary edema, surgical reintervention, delirium and sepsis.
Once the final logistic model was built, 8 variables were included (Figure 1). The presurgical variables were COPD and CKD, the transurgical variable was IABP use and the postsurgical factors associated were SVO2<60% at ICU admission, mediastinitis, inotrope use, pleural effusion requiring drainage and delirium. The final model accounts for 23% of the variability of PMV following CABG (Pseudo R²).
Due to variations in raw and adjusted OR (Figure 2) values and based on theoretical clinical criteria, the presence of the effect modification was assessed. However, no statistical significance was found, nor any explanation for the variability of the event.
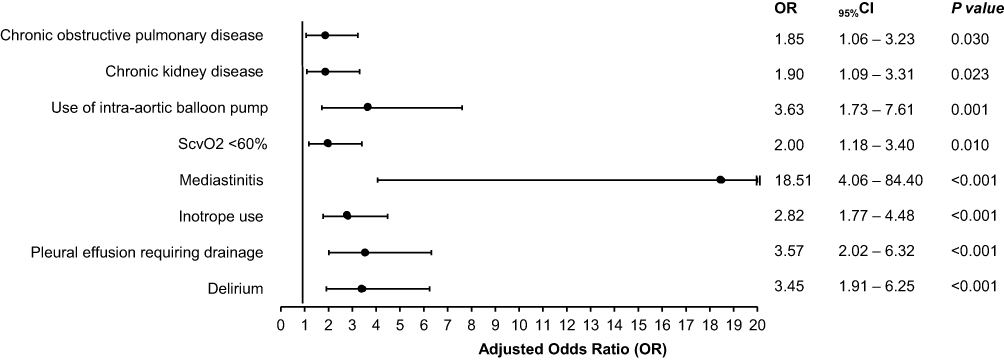 |
Figure 2 Forest plot final logistical model based on odds ratios (OR). |
The assessment of the final adjustment of the logistic regression model showed adequate data adjustment (Hosmer-Lemeshow) with a Chi2 of 33.82 (p=0.99). Model classification evidenced that the model had a 52.7% capacity to classify cases as cases (sensitivity) and 88.6% capacity to classify controls as controls (specificity). In other words, the model is highly capable of ruling out subjects unlikely to receive PMV. Cases predicted by the model had a 69.9% likelihood of becoming actual cases. Subjects unlikely to receive PMV according to the model had a 78.9% likelihood of becoming controls.
Discussion
Among the factors studied, the final logistic model included variables associated with the three surgical time points, such as history of COPD, CKD, IABP use during surgery, SVO2<60%, mediastinitis, inotrope use, pleural effusion requiring drainage and delirium.
A majority of COPD subjects subject to CABG were reported as needing mechanical ventilation for more than 48 hours or prolonged intubation, since there is a significant decrease of their vital capacity, total pulmonary capacity and functional residual capacity, which results in a proportionally higher mortality rate.18 In their study, Piotto et al1 described COPD as a strong predictor of PMV following CABG, with an OR of 2.65 (95% CI: 1.38–5.09, p=0.004). This is consistent with our study, in which COPD had an OR of 1.85 (95% CI: 1.06–3.23, p=0.030) and a statistically significant association.
CKD subjects are prone to present adverse results, and this variable was observed to be associated with critical conditions such as pulmonary edema, sepsis and metabolic dysfunction, which may result in prolonged intubations.19 This condition is also considered a PMV predictor following cardiac surgery. This study yielded relevant findings, with a significant association between CKD and PMV (OR 1.90, 95% CI: 1.09–3.31, p=0.023) regardless other risk factors. In addition, a higher frequency was observed (19.1%) for subjects needing prolonged respiratory support. Likewise, subjects with kidney injury following cardiac surgery have a high death probability. In the study performed by Fernández et al,2 a relatively small fraction (10–15%) of subjects admitted to the ICU following CABG required PMV, 72.8% of which reported CKD, resulting in a positive association (OR 2.14; 95% CI: 1.1–4.07, p= 0.027).
Similarly, Gumus et al11 found that this type of subjects had high mortality rates and a PMV frequency of 58.7%, and concluded that kidney injury is one of the most significant risk factors in this critical condition (OR 7.7, 95% CI: 1.3–47.6, p=0.00). On the other hand, Shirzad et al,20 reported a lower incidence (6.6%) of subjects with CKD requiring PMV following CABG (OR 5.65; 95% CI: 1.42–22.48, p=0.01).
Regarding IABP use, this was the only transurgical variable identified as a predictor of PMV in this study (OR 3.63, 95% CI: 1.73–7.61, p=0.001). In their study, Helena et al8 suggested that IABP use time is associated with prolonged ventilatory support following CABG, with an OR of 1.12 (95% CI: 0.96–1.31, p=0.001). It should be mentioned that the exact moment to remove MV following a CABG that required IABP use is still under debate. However, it is known that complications associated with MV —such as atelectasis, pneumothorax and pneumonia— are directly correlated with the duration of endotracheal intubation.21 The reporting frequency of these conditions was higher (p<0.05) in this study population.
IABP use is associated with PMV in subjects subject to CABG and other cardiovascular surgeries. Graziela et al22 assessed the efficacy of IABP in subjects undergoing high risk cardiac surgery, in which 47.8% of the IABP group required PMV, and no decrease in associated mortality and morbidity rates was observed. Moreover, Ranucci et al23 conducted a study with 110 subjects and observed a higher PMV frequency in subjects needing IABP cardiovascular support as opposed to those who did not need it (31% vs 27%). They also found incidence of other complications, such as acute kidney failure, surgical reintervention and cerebrovascular accident.
In the postsurgical stage, we found that SVO2 <60% was a predictive variable for PMV with an OR of 2.0 (95% CI: 1.18–3.40, p=0.010). We also found that average and standard deviation values were lower for cases than for controls (65.2 ± 9.8). There are several studies which evidence that low SvO2 levels are not associated with PMV. Greg et al24 concluded that SvO2 <70% at ICU admission following cardiac surgery was not associated with morbidity increase or the duration of mechanical ventilation. Conversely, Hitendra et al25 evidenced that hemodynamic, oximetric and laboratory alterations, including SvO2, were associated with a significantly prolonged need of mechanical ventilation and ICU stay.
As for mediastinitis, it has been described as a condition related to prolonged ventilatory support, which can also increase mortality rates among these subjects.26 Charbonneau et al27 assessed and described the characteristics of a large cohort of subjects with postsurgical mediastinitis, particularly analyzing gram-negative bacteria. Mediastinitis occurred in 309 of these subjects (mean age 65 years), and a significant association with PMV was described (p=0.004). Gustavo et al28 conducted an analytical retrospective case-control study regarding the presence of mediastinitis, and built a predictive model for this condition using risk factors, which revealed a strong association with PMV (OR 2.66; 95% CI: 1.02–6.93, p=0.045). Our study is highly consistent with the studies above, since mediastinitis was considered a postsurgical predictor associated with PMV following CABG (OR 18.51; 95% CI: 4.06–84.40, p=<0.001).
The use of inotropic agents in subjects subject to CABG and staying in the ICU with invasive MV may improve myocardial contractility through diverse mechanisms and result in a quicker MV removal. However, it should be considered that each agent affects systemic and pulmonary vasculature in a different way, which may cause characteristic hemodynamic effects that are strongly associated with PMV following CABG or any cardiac surgery. In this study, inotrope use as a postsurgical variable was evidenced as a strong predictor for PMV following CABG (OR 2.82; 95% CI: 1.77–4.48, p=<0.001). Moreover, Umar et al29 conducted a retrospective analysis on 690 subjects subject to isolated emergency CABG surgery in a tertiary center in West Australia, in which IABP was used in 78 subjects (11.3%), and prolonged inotrope use was widely considered a postoperative secondary outcome (OR 6.11; 95% CI: 2.77–13.48, p= <0.001). An association with PMV was also found (OR 20.2; 95% CI: 8.24–49.74, p= <0.001).
Pleural effusion requiring drainage is a postsurgical variable of CABG and is a common complication, widely associated with PMV. Few studies reporting an association between pleural effusion and PMV following CABG or any other cardiac surgery have been found. Williams et al30 conducted a retrospective cohort study that assessed risk factors for pleural effusion requiring drainage following CABG, including 409 subjects, of which, 53 (12.9%) underwent this procedure. In these subjects, PMV following CABG was reported to be associated with pleural effusion requiring drainage (p=0.049). In our study, results of the final logistic model showed that pleural effusion requiring drainage is associated with PMV (OR 3.57; 95% CI: 2.02–6.32, p= ≪0.001).
Delirium is considered a neuropsychiatric complication after major surgery in elderly adults, which is frequently reported and which is prevalent among subjects subject to cardiac surgery.31 This condition occurs acutely after surgery and is characterized by fluctuant changes in consciousness, mental state, attention, feelings, cognition, memory, perception and diurnal cycle. It is considered as a strong postsurgical predictor associated with postsurgical PMV. Tania et al32 identified predictive factors of delirium in 501 subjects admitted to acute cardiac care units following transcatheter aortic valve replacement, resulting in an association between delirium and PMV (OR 18.86; 95% CI: 1.85–192.58, p=0.013). On the other hand, in a retrospective observational study including 2447 subjects subject to cardiac surgery, delirium was independently and strongly associated with a higher risk of PMV (OR 113.7; 95% CI: 99.7–127.7, p=0.00).33
Matthew et al34 conducted a retrospective cohort study which included 250 subjects undergoing cardiac surgery, in which PMV was identified as a triggering factor for delirium, as well as surgery duration, transfusion of blood products, conscious sedation and duration of ICU stay. Based on the above, these studies are highly consistent with our research, in which the multiple logistic model yielded a correlation between delirium and PMV (OR 3.45; 95% CI: 1.91–6.25, p=0.00). So far, few studies performed with subjects subject to CABG have identified this risk factor, such as the one conducted by Stransky et al,35 in which hypoactive delirium was evidenced as an independent predictor of PMV (OR 1.56; 95% CI: 1.25–1.92, p<0.01). Another example is the study conducted by Norkiene et al,36 who found an association between postsurgical delirium and PMV over time (9.2±3.1 vs 2.0±2.7 days, p=0.001).
Finally, regarding hospital mortality observed in subjects requiring PMV following surgery, 46 of 204 subjects died, representing 22.5%. The main causes of death included sepsis, cardiogenic shock and postsurgical bleeding. This is consistent with the study performed by Ibañez et al,37 in which 69% of subjects died due to cardiogenic and septic shock. Moreover, Fernández et al2 studied whether PMV is a predictor of mortality in subjects subject to cardiac surgery, in which the main causes of death were multiorgan failure and sepsis (50.3%).
This study has some limitations. The research was conducted on a specific population group with similar healthcare affiliation characteristics, so the “type of subject” factor could not be evaluated. The ethnic variable was reported in a low proportion of clinical records, so it had to be removed from the analysis. The final logistic regression model included presurgical, transurgical and postsurgical variables consistent with what has been reported in scientific literature. However, strongly associated factors such as age, sex and pump time were excluded from the model, possibly due to the sample size of this study. Based on the findings of this study, multicentric studies should be conducted throughout the country in order to reinforce the purposes of the research by using a sample size that allows for the assessment of a wider range of variables of interest.
Conclusion
The final logistic model included the presurgical variables chronic obstructive pulmonary disease and chronic kidney disease, the transurgical variable IABP use and the postsurgical variables oxygen venous saturation, mediastinitis, inotrope use, pleural effusion requiring drainage and delirium.
Delirium and pleural effusion requiring drainage were novel risk factors. Therefore, the research invites the intensive care team to carry out an early and adequate intervention of delirium in search of achieving timely ventilatory weaning.
Take Home
PWV variables associated with cardiovascular surgery (CABG) were identified, such as COPD, CKD, intraoperative IABP use, SVO2 <60%, mediastinitis, inotrope use, pleural effusion, and delirium, the latter being a new risk factor.
Acknowledgments
The authors would like to express their gratitude to the Research and Education Department of Clínica de Occidente, which allowed for the performance of the study, as well as to Universidad Santiago de Cali and its Research Group on Health and Movement for providing academic support to the research project (project code 442-621120-G07), internal call DGI-02 −2020.
Funding
This research has been funded by the General Research Directorate of Universidad Santiago de Cali under call No. 07-2021.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Piotto RF, Ferreira FB, Colósimo FC, Silva GS, Sousa AG, Braile DM. Independent predictors of prolonged mechanical ventilation after coronary artery bypass surgery. Rev Bras Cir Cardiovasc. 2012;27(4):520–528. doi:10.5935/1678-9741.20120093
2. Fernandez Z, Gordillo B, Banderas B, et al. Prolonged mechanical ventilation as a predictor of mortality after cardiac surgery. Respir Care. 2018;63(5):550–557. doi:10.4187/respcare.04915
3. Lone NI, Walsh TS. Prolonged mechanical ventilation in critically ill patients: epidemiology, outcomes and modelling the potential cost consequences of establishing a regional weaning unit. Crit Care. 2011;15(2):102. doi:10.1186/cc10117
4. Tobin MJ, Grant BJ, Duffner LA, Collins EG, Lanuza DM, Hoffman LA. Efecto de la presión de soporte versus la respiración sin ayuda a través de un collar de traqueotomía sobre la duración del destete en pacientes que requieren ventilación mecánica prolongada: un ensayo aleatorizado. JAMA. 2013;309(7):671–677. doi:10.1001/jama.2013.159
5. Tobin MJ. Principles and Practice of Mechanical Ventilation. In: Tercera Edición. Chicago: Illinois; 2013:175–176.
6. Rose L, McGinlay M, Amin R, et al. Variation in definition of prolonged mechanical ventilation. Respir Care. 2017;62(10):1324–1332. doi:10.4187/respcare.05485
7. Silva S, Consolim C, Rodrigues R, et al. Fluid overload after coronary artery bypass graft in patients on maintenance hemodialysis is associated with prolonged time on mechanical ventilation. BMC Anesthesiol. 2020;20(1):7–60. doi:10.1186/s12871-020-00971-6
8. Amaral H, Castilho L, Ragonete A, Sibinelli M, Dragosavac D. Factors associated with pulmonary dysfunction in patients undergoing coronary artery bypass graft surgery with use of intra-aortic balloon pump. Rev Port Cardiol. 2018;37(1):15–23. doi:10.1016/j.repc.2017.04.004
9. Saleh H, Shaw M, Al-Rawi O, et al. Outcomes and predictors of prolonged ventilation in patients undergoing elective coronary surgery. Interact Cardiovasc Thorac Surg. 2012;15(1):51–56. doi:10.1093/icvts/ivs076
10. Hsu H, Lai HC, Liu TJ. Factors causing prolonged mechanical ventilation and peri-operative morbidity after robot-assisted coronary artery bypass graft surgery. Heart Vessels. 2019;34(1):44–51. doi:10.1007/s00380-018-1221-6
11. Gumus F, Polat A, Yektas A, et al. Prolonged mechanical ventilation after CABG: risk factor analysis. J Cardiothorac Vasc Anesth. 2015;29(1):52–58. doi:10.1053/j.jvca.2014.09.002
12. Faritous Z, Aghdaie N, Yazdanian F, Azarfarin R, Dabbagh A. Perioperative risk factors for prolonged mechanical ventilation and tracheostomy in women undergoing coronary artery bypass graft with cardiopulmonary bypass. Saudi J Anaesth. 2011;5(2):167–169. doi:10.4103/1658-354X.82786
13. Totonchi Z, Baazm F, Chitsazan M, Seifi S. Predictors of Prolonged mechanical ventilation after open heart surgery. J Thorac Cardiovasc Surg. 2014;6(4):211–216. doi:10.15171/jcvtr.2014.014
14. Ji Q, Chi L, Mei Y, et al. Risk factors for late extubation after coronary artery bypass grafting. Heart Lung. 2010;39(4):275–282. doi:10.1016/j.hrtlng.2009.09.002
15. Natarajan K, Patil S, Lesley N, Ninan B. Predictors of prolonged mechanical ventilation after on-pump coronary artery bypass grafting. Ann Card Anaesth. 2006;9(1):31–36.
16. Oliveira E, Turquetto A, Tauil P, Junqueira L, Porto L. Risk factors for prolonged hospital stay after isolated coronary artery bypass grafting. Rev Bras Cir Cardiovasc. 2013;28(3):353–363. doi:10.5935/1678-9741.20130055
17. Shahian D, O’Brien S, Filardo G, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1--coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88(1):S2–22. doi:10.1016/j.athoracsur.2009.05.053
18. Ovalı C, Şahin A. Chronic Obstructive Pulmonary disease and off-pump coronary surgery. Ann Thorac Cardiovasc Surg. 2018;24(4):193–199. doi:10.5761/atcs.oa.17-00231
19. Zafrir B, Leviner D, Saliba W, Sharoni E. Prognostic interplay of chronic kidney disease, anemia, and diabetes in coronary bypass surgery. Ann Thorac Surg. 2021;111(1):94–101. doi:10.1016/j.athoracsur.2020.04.124
20. Shirzad M, Karimi A, Ahmadi S, Marzban M, Tazik M, Aramin H. Predictors and early outcome of prolonged mechanical ventilation in contemporary heart valve surgery. Monaldi Arch Chest Dis. 2010;74(1):22–27. doi:10.4081/monaldi.2010.276
21. Laizo A, Delgado F, Rocha G. Complicac¸ões que aumentam o tempo de permanência na unidade de terapia intensiva na cirurgia cardíaca. Rev Bras Cir Cardiovasc. 2010;25(2):71–166. doi:10.1590/S0102-76382010000200007
22. Rocha F, Almeida J, Landoni G, et al. Effect of a perioperative intra-aortic balloon pump in high-risk cardiac surgery patients: a randomized clinical trial. Crit Care Med. 2018;46(8):742–750. doi:10.1097/CCM.0000000000003185
23. Ranucci M, Castelvecchio S, Biondi A, et al. A randomized controlled trial of preoperative intra-aortic balloon pump in coronary patients with poor left ventricular function undergoing coronary artery bypass surgery. Crit Care Med. 2013;41(11):83–247. doi:10.1097/CCM.0b013e3182978dfc
24. Laine G, Hu B, Wang S, Thomas S, Reul G. Isolated high lactate or low central venous oxygen saturation after cardiac surgery and association with outcome. J Cardiothorac Vasc Anesth. 2013;27(6):1271–1276. doi:10.1053/j.jvca.2013.02.031
25. Kanzariya H, Pujara J, Keswani S, et al. Role of central venous - Arterial pCO2 difference in determining microcirculatory hypoperfusion in off-pump coronary artery bypass grafting surgery. Ann Card Anaesth. 2020;23(1):20–26. doi:10.4103/aca.ACA_48_19
26. Ang L, Veloria E, Evanina E, Smaldone A. Mediastinitis and blood transfusion in cardiac surgery: a systematic review. Heart Lung. 2012;41(3):255–263. doi:10.1016/j.hrtlng.2011.07.012
27. Charbonneau H, Maillet J, Faron M, et al. Mediastinitis due to Gram-negative bacteria is associated with increased mortality. Clin Microbiol Infect. 2014;20(3):197–202. doi:10.1111/1469-0691.12369
28. Gustavo B, Alfredo M, Rabassa-LópezCallejas MA, Lagomasino-Hidalgo ÁL, Chaljub-Bravo E, Barreto-Fiu EE. Naranjo U, Magda A. Rabassa L, Álvaro L, et al. Modelo predictivo de mediastinitis postoperatoria en cirugía cardiovascular. Cir Cardiov. 2019;26(6):277–282. doi:10.1016/j.circv.2019.09.003
29. Umar S, Nick S, Molly G, Kwok H, Warren P, Girish D. Preoperative intra-aortic balloon pumps in cardiac surgery: a propensity score analysis. Heart Lung Circ. 2021;30(5):758–764. doi:10.1016/j.hlc.2020.09.924
30. Williams M, Brookes J, Bannon P. Predictors of pleural effusion after coronary artery bypass surgery. Heart Lung Circ. 2021;30(1):54–55. doi:10.1016/j.hlc.2021.03.203
31. Lin Y, Chen J, Wang Z. Metaanálisis de factores que influyen en el delirio tras cirugía cardíaca. J Card Surg. 2012;27(4):481–492. doi:10.1111/j.1540-8191.2012.01472.x
32. Tania L, Francisco J, Angela M, et al. Impact of delirium in acute cardiac care unit after transcatheter aortic valve replacement. Int J Cardiol. 2021;330(2):164–170. doi:10.1016/j.ijcard.2021.01.053
33. Daryl J, George M, Johan M, et al. Predictors and outcomes of cardiac surgery-associated delirium. A Single Centre Retrospective Cohort Study Heart, Lung and Circulation. 2019;28(3):455–463.
34. Matthew D, Carolyn P, Katherine A, Thomas J, Paul P. Predisposing and precipitating factors associated with postoperative delirium in patients undergoing cardiac surgery at a veterans affairs medical center: a pilot retrospective analysis. J Cardiothorac Vasc Anesth. 2020;34(8):2103–2110.
35. Stransky M, Schmidt C, Ganslmeier P, et al. Hypoactive delirium after cardiac surgery as an independent risk factor for prolonged mechanical ventilation. J Cardiothorac Vasc Anesth. 2011;25(6):968–974. doi:10.1053/j.jvca.2011.05.004
36. Norkiene I, Ringaitiene D, Misiuriene I, et al. Incidence and precipitating factors of delirium after coronary artery bypass grafting. Scand Cardiovasc J. 2007;41(3):180–185. doi:10.1080/14017430701302490
37. Ibáñez J, Riera M, Ignacio J, et al. Risk factors of long-term survival after isolated coronary bypass graft surgery. Med balear. 2014;29(1):19–24.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence, General and Periodontal Risk Factors of Gastroesophageal Reflux Disease in China
Liu Z, Gao X, Liang L, Zhou X, Han X, Yang T, Huang K, Lin Y, Deng S, Wang Z, Wang C
Journal of Inflammation Research 2023, 16:235-244
Published Date: 17 January 2023
Emerging Prevalence and Clinical Features of Elizabethkingia meningoseptica Infection in Southwest China: A 9-Year Retrospective Study and Systematic Review
Ma S, Gong Y, Luo X, Peng Y, Zhang C, Zhang X, Hu X, Tang P, Yuan Z, Luo G, Li H
Infection and Drug Resistance 2023, 16:531-543
Published Date: 25 January 2023
The Prevalence and Risk Factors of Sexual Dysfunction in the Elderly in Southern China
Yu Z, Niu J, Wang C
International Journal of General Medicine 2024, 17:2355-2360
Published Date: 22 May 2024
Epidemiology and Risk Factors Characteristics of Alzheimer’s Disease in Southwestern China: A Cross-Sectional Study

Zhu Y, Liu H, He M, Xu Z, Sun L, Wu Z, Niu X, Huang S, Wang J, Ran X
Clinical Interventions in Aging 2025, 20:2685-2704
Published Date: 26 December 2025