Back to Journals » Journal of Inflammation Research » Volume 19
Prognostic Value of the C-Reactive Protein–Albumin–Lymphocyte (CALLY) Index for In-Hospital Mortality in Spontaneous Intracerebral Hemorrhage: A Comparative Analysis with Hematoma Volume
Authors Yılmaz BÖ ![]() , Altunışık E, Dev Ş, Parlak S
, Altunışık E, Dev Ş, Parlak S
Received 24 February 2026
Accepted for publication 9 May 2026
Published 23 May 2026 Volume 2026:19 603872
DOI https://doi.org/10.2147/JIR.S603872
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Buket Özkara Yılmaz, Erman Altunışık, Şeyda Dev, Samet Parlak
Department of Neurology, Gaziantep City Hospital, Gaziantep, Turkey
Correspondence: Buket Özkara Yılmaz, Email [email protected]
Purpose: The C-reactive protein–albumin–lymphocyte (CALLY) index is a composite biomarker reflecting systemic inflammation, nutritional status, and immune response. Its role in predicting mortality in spontaneous intracerebral hemorrhage (ICH) remains unclear. This study aimed to evaluate the prognostic performance of the CALLY index for in-hospital mortality in patients with spontaneous ICH and to compare it with hematoma volume.
Methods: This retrospective study included 74 patients diagnosed with spontaneous intracerebral hemorrhage. Demographic, clinical, laboratory, and radiological data were analyzed. The CALLY index was calculated using admission serum albumin, C-reactive protein (CRP), and lymphocyte count. The predictive performance of the CALLY index and hematoma volume for in-hospital mortality was assessed using receiver operating characteristic (ROC) curve analysis. Optimal cutoff values were determined by the Youden index. The discriminative abilities of the models were compared using the DeLong test. Incremental prognostic value was evaluated using Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) analyses.
Results: In-hospital mortality occurred in 27% of the patients. CALLY index values were significantly lower in non-survivors compared to survivors (p=0.015), while hematoma volume was significantly higher in non-survivors (p=0.017). The CALLY index demonstrated moderate discriminative performance for predicting mortality (AUC: 0.668; p=0.015), with an optimal cutoff value of 0.36 (sensitivity 65%, specificity 69%). Hematoma volume also showed moderate predictive ability (AUC: 0.682; p=0.017), with an optimal cutoff value of 21 cc (sensitivity 70%, specificity 67%). No statistically significant difference was observed between the two models (ΔAUC=0.004; p=1.000). Reclassification analyses indicated minimal incremental prognostic contribution of the CALLY index (NRI=0.006; IDI=− 0.016).
Conclusion: Both the CALLY index and hematoma volume demonstrated moderate and comparable performance in predicting in-hospital mortality in spontaneous ICH. However, the CALLY index did not provide significant additional prognostic value beyond hematoma volume. Larger prospective studies are warranted to clarify the role of inflammation-based biomarkers in hemorrhagic stroke prognosis.
Keywords: spontaneous intracerebral hemorrhage, CALLY index, inflammation, hematoma volume, mortality
Introduction
Spontaneous intracerebral hemorrhage (ICH) is a severe form of stroke that accounts for approximately 10–15% of all stroke cases and is associated with high early mortality and substantial long-term disability.1 Despite advances in neurocritical care, outcomes remain poor in a considerable proportion of patients. Early prognostic assessment is therefore essential for risk stratification and clinical decision-making. Among established predictors, hematoma volume has consistently been identified as one of the strongest determinants of short-term mortality.2,3
Beyond the direct mechanical effects of the hematoma and increased intracranial pressure, secondary biological mechanisms contribute significantly to neurological deterioration. Experimental and clinical studies have demonstrated that inflammatory responses, including microglial activation, cytokine release, oxidative stress, and blood–brain barrier disruption, play a central role in perihematomal injury.4 Elevated inflammatory markers such as C-reactive protein (CRP) have been linked to neurological worsening,5 while low serum albumin levels have been associated with poor clinical outcomes and increased mortality.6 Albumin possesses antioxidant and anti-inflammatory properties and may exert neuroprotective effects.7 Furthermore, the interaction between inflammation and nutritional status during acute illness has been well documented.8 Inflammation-based indices, such as the neutrophil-to-lymphocyte ratio, have also been shown to predict hemorrhagic complications in cerebrovascular disease.9
While hematoma volume is a well-established structural predictor, there remains a need for easily accessible, bedside biomarkers that may reflect systemic physiological responses and complement imaging-based prognostic tools.
The C-reactive protein–albumin–lymphocyte (CALLY) index is a composite biomarker derived from routine laboratory parameters that integrates inflammatory burden, immune status, and nutritional condition. Initially introduced as a prognostic marker in oncological populations,10 the CALLY index has subsequently been investigated in acute ischemic stroke. Previous studies have reported associations between lower CALLY index values and hemorrhagic transformation as well as unfavorable functional outcomes.11 In patients undergoing endovascular therapy, the CALLY index has also been identified as an independent predictor of adverse clinical outcomes.12 Compared with single inflammatory markers such as CRP or neutrophil-to-lymphocyte ratio, the CALLY index integrates inflammatory burden, nutritional status, and immune response into a single composite parameter, potentially providing a more comprehensive reflection of systemic condition.
However, the prognostic role of the CALLY index in spontaneous intracerebral hemorrhage has not been clearly established. Given the recognized contribution of inflammatory mechanisms to hemorrhagic brain injury, a composite inflammation-based marker such as the CALLY index may provide additional prognostic insight. Nevertheless, its clinical value must be evaluated in relation to established structural predictors, particularly hematoma volume.
Therefore, the present study aimed to assess the prognostic performance of the CALLY index for predicting in-hospital mortality in patients with spontaneous intracerebral hemorrhage and to compare it directly with hematoma volume.
Methods
This retrospective observational cohort study was conducted at the Department of Neurology, Gaziantep City Hospital. Medical records of patients admitted with a diagnosis of spontaneous intracerebral hemorrhage were systematically reviewed. A total of 74 consecutive adult patients with radiologically confirmed spontaneous intraparenchymal hemorrhage were included in the analysis.
Patients were eligible if they were aged 18 years or older and had available admission laboratory parameters, including serum C-reactive protein (CRP), serum albumin, and absolute lymphocyte count. All laboratory measurements, including CRP, albumin, and lymphocyte count, were obtained within the first 24 hours of hospital admission. Patients with traumatic intracranial hemorrhage, subarachnoid hemorrhage, epidural or subdural hematoma were excluded. In addition, individuals with active infection, known malignancy, autoimmune or rheumatologic disease, chronic liver failure, advanced renal failure, or incomplete clinical or laboratory data were not included in the study. Patients with incomplete clinical or laboratory data were excluded from the analysis; therefore, no imputation method was applied.
Baseline demographic characteristics, comorbidities, admission vital signs, and neurological findings were recorded from electronic medical records. Neurological severity at admission was assessed using the National Institutes of Health Stroke Scale (NIHSS) and the Glasgow Coma Scale (GCS). Hematoma volume was calculated from the initial non-contrast cranial computed tomography (CT) scans using the ABC/2 method and expressed in milliliters (mL). Hematoma volume was calculated using the ABC/2 method by two independent neurologists blinded to clinical outcomes. In case of discrepancy, a consensus was reached.
Laboratory measurements obtained at admission included serum albumin (g/L), CRP (mg/L), and absolute lymphocyte count (×109/L). The C-reactive protein–albumin–lymphocyte (CALLY) index was computed using the following formula:
CALLY = (serum albumin × lymphocyte count) / (CRP × 10)
The primary endpoint of the study was in-hospital mortality. Patients were classified into survivor and non-survivor groups according to their discharge status.
To determine the independent prognostic value of the CALLY index, a multivariable logistic regression analysis was performed. Variables with p < 0.10 in univariate analysis and clinically relevant parameters (age, NIHSS, GCS, and hematoma volume) were included in the model. Multicollinearity was assessed using variance inflation factor (VIF), and variables with VIF > 5 were excluded from the final model.
The study was approved by the Gaziantep City Hospital Non-Interventional Clinical Research Ethics Committee (Decision date: December 17, 2025; Meeting No: 2025/376).Due to the retrospective design and use of anonymized patient data, the requirement for informed consent was waived by the ethics committee. All procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki. Patient confidentiality was strictly maintained throughout the study.
This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics version 25. Continuous variables were described as mean ± standard deviation, whereas categorical variables were summarized as counts and percentages. Distributional assumptions were assessed using skewness and kurtosis values.
Comparisons between survivors and non-survivors were performed using the independent samples t-test or Mann–Whitney U-test, depending on data distribution. Categorical variables were analyzed using the chi-square test or Fisher’s exact test when appropriate.
The ability of the CALLY index and hematoma volume to predict in-hospital mortality was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the ROC curve (AUC) was calculated with 95% confidence intervals. Optimal threshold values were determined based on the maximum Youden index. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for each model.
Differences between AUCs were examined using the DeLong method. To explore whether the addition of the CALLY index improved predictive performance beyond hematoma volume, reclassification analyses were conducted using Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI). Correlations between continuous variables were assessed using Pearson or Spearman correlation coefficients as appropriate. A two-tailed p value < 0.05 was considered statistically significant.
Results
A total of 74 patients with spontaneous intracerebral hemorrhage were included in the study. Of these, 41 (55.4%) were male and 33 (44.6%) were female. In-hospital mortality occurred in 20 patients (27.0%). The mean CALLY index was 2.70. The overall mean age of the cohort was 60.51 ± 18.04 years. At admission, the mean NIHSS score was 10.35 ± 7.08 and the mean Glasgow Coma Scale (GCS) score was 10.67 ± 4.21. The mean length of hospital stay was 15.08 ± 14.71 days. The average hematoma volume was 31.86 ± 39.02 cc. The mean systolic blood pressure was 177.64 ± 36.06 mmHg and the mean diastolic blood pressure was 97.67 ± 16.99 mmHg. Hypertension was the most common comorbidity, present in 53 patients (71.6%), followed by diabetes mellitus in 31 (41.9%), hyperlipidemia in 35 (47.3%), coronary artery disease in 30 (40.5%), and previous stroke in 23 (31.1%). Nineteen patients (25.7%) were active smokers (Table 1).
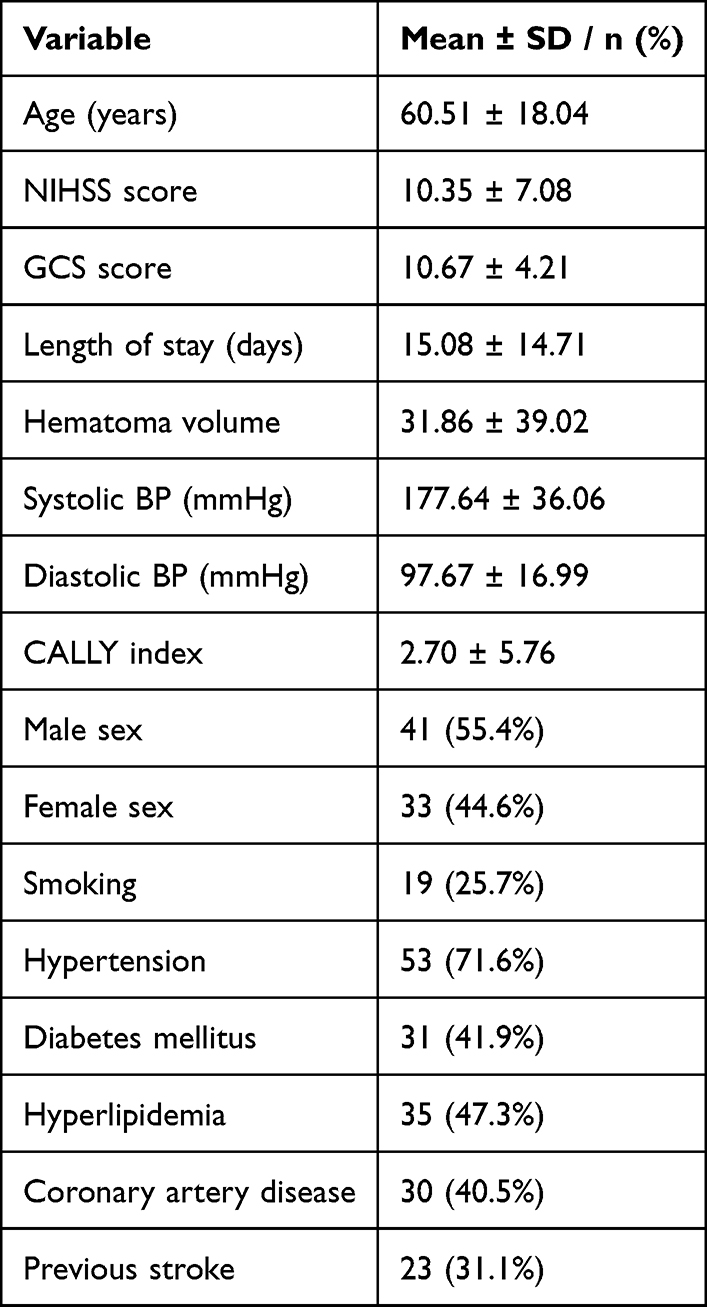 |
Table 1 Baseline Demographic and Clinical Characteristics |
When patients with in-hospital mortality were compared to survivors, no significant difference was observed in age (p = 0.883). However, neurological status at admission was significantly worse in non-survivors. The mean NIHSS score was higher in the non-survivor group (15.00 ± 5.61 vs 8.62 ± 6.83; p < 0.001), and the mean GCS score was significantly lower (5.95 ± 3.45 vs 12.42 ± 2.94; p < 0.001). Regarding hemodynamic parameters, systolic blood pressure did not differ significantly between groups (p = 0.228), whereas diastolic blood pressure was significantly higher in non-survivors (106.35 ± 17.30 vs 94.46 ± 15.85 mmHg; p = 0.007). CALLY index values were significantly lower in non-survivors compared to survivors (2.45 ± 7.30 vs 2.80 ± 5.15; p = 0.015). Hematoma volume was significantly greater in the non-survivor group (53.00 ± 54.20 cc vs 24.03 ± 28.51 cc; p = 0.017) (Table 2).
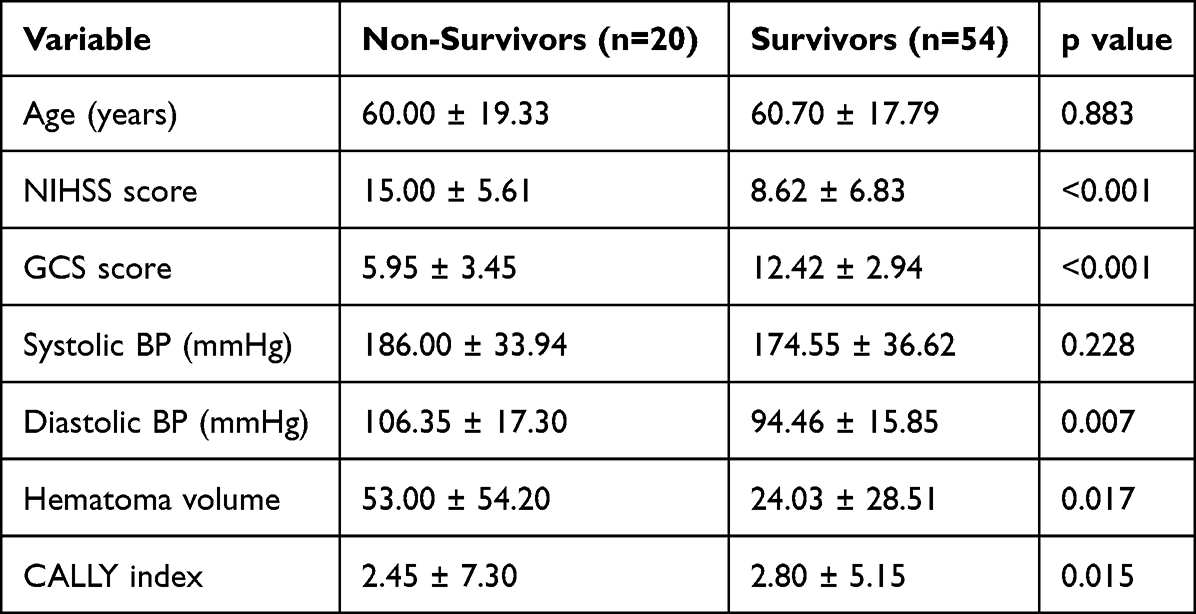 |
Table 2 Comparison of Clinical Parameters Between Non-Survivors and Survivors |
For the CALLY index, the optimal cutoff value was 0.36, yielding a sensitivity of 65%, specificity of 69%, positive predictive value (PPV) of 43%, and negative predictive value (NPV) of 84%. ROC curve analysis demonstrated that the CALLY index had moderate discriminative ability for predicting in-hospital mortality (AUC: 0.668; p = 0.015) (Figure 1). The overall performance metrics of the CALLY index and hematoma volume are presented in Table 3.
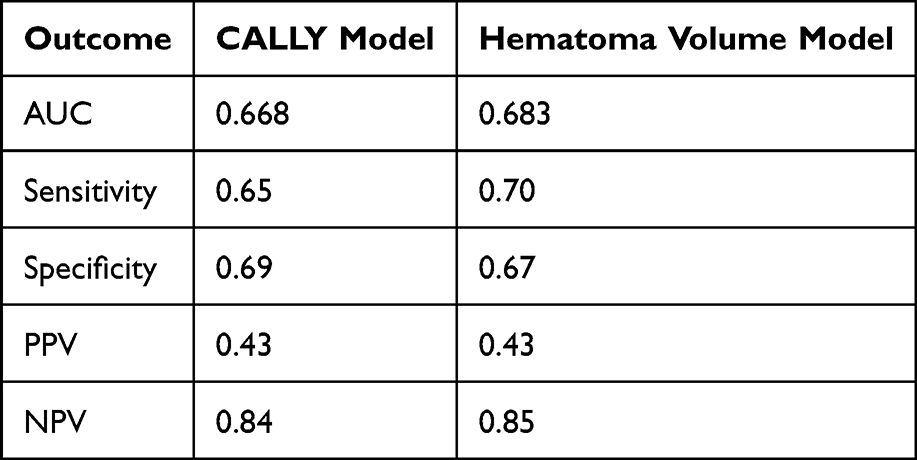 |
Table 3 Overall Performance Comparison of Mortality Prediction Models |
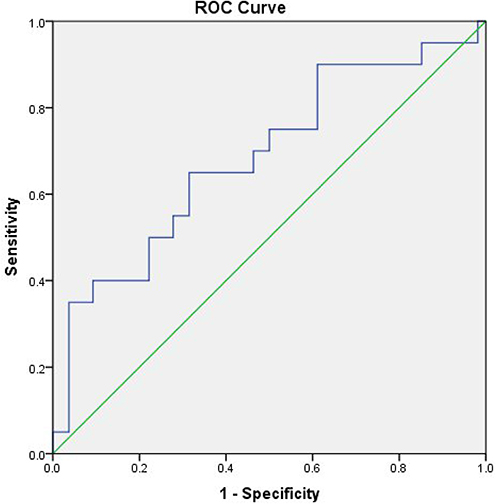 |
Figure 1 Receiver operating characteristic (ROC) curve of the C-reactive protein–albumin–lymphocyte (CALLY) index for predicting in-hospital mortality. The area under the curve (AUC) was 0.668 (p = 0.015), indicating moderate discriminative performance. The optimal cutoff value was 0.36, yielding a sensitivity of 65% and specificity of 69%. |
For hematoma volume, the optimal cutoff value was 21 cc, with a sensitivity of 70%, specificity of 67%, PPV of 43%, and NPV of 85%. ROC analysis indicated moderate discriminative performance (AUC: 0.682; p = 0.017) (Figure 2).
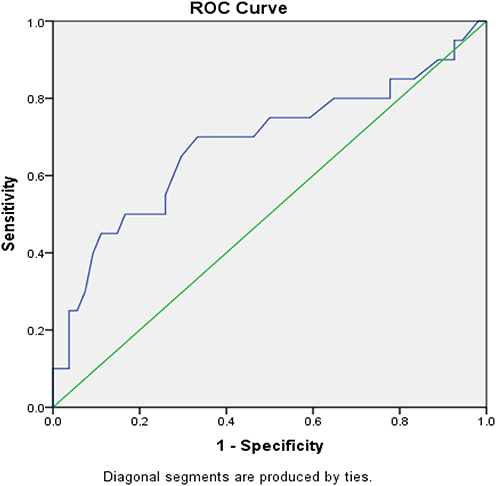 |
Figure 2 Receiver operating characteristic (ROC) curve of hematoma volume for predicting in-hospital mortality. The optimal cutoff value was 21 cc, yielding a sensitivity of 70% and specificity of 67%. The area under the curve (AUC) was 0.682 (p = 0.017), indicating moderate discriminative performance. |
Comparison of the two ROC curves using the DeLong test showed no statistically significant difference between the models (ΔAUC ≈ 0.004; p = 1.000), indicating comparable discriminative performance. Reclassification analysis demonstrated minimal incremental prognostic value of the CALLY index beyond hematoma volume (NRI = 0.006; IDI = −0.016).
Correlation analysis revealed no significant association between the CALLY index and length of hospital stay, hematoma volume, NIHSS score, or GCS score.
Multivariable logistic regression analysis was performed to identify independent predictors of in-hospital mortality. After adjustment for age, sex, NIHSS score, GCS score, hematoma volume, CALLY index, and systolic blood pressure, lower GCS score and higher hematoma volume remained independently associated with mortality.
An increase in GCS score was associated with a significant reduction in mortality risk (OR=0.323; 95% CI: 0.160–0.651; p=0.002). Similarly, higher hematoma volume was independently associated with increased mortality risk (OR=1.052; 95% CI: 1.001–1.105; p=0.046). The CALLY index did not retain independent statistical significance in the multivariable model (p=0.842) (Table 4).
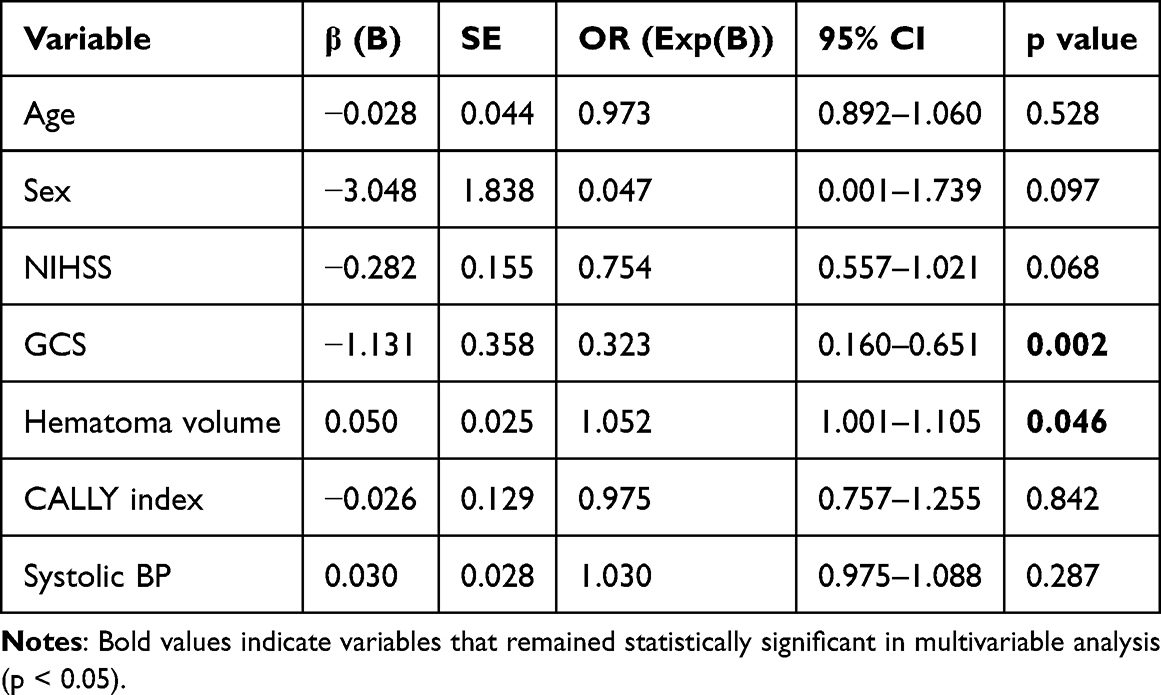 |
Table 4 Multivariable Logistic Regression Analysis for Predictors of in-Hospital Mortality |
Discussion
In the present study, we investigated the prognostic value of the C-reactive protein–albumin–lymphocyte (CALLY) index for predicting in-hospital mortality in patients with spontaneous intracerebral hemorrhage and directly compared its performance with hematoma volume. Our results demonstrated that both parameters exhibited moderate discriminative ability, and neither showed statistical superiority over the other.
Spontaneous intracerebral hemorrhage remains a major contributor to global stroke-related mortality and disability.1 Among the established determinants of early outcome, hematoma volume has consistently been identified as one of the strongest predictors of mortality.2,3 Larger hematoma size is associated with increased intracranial pressure, mass effect, and early neurological deterioration, thereby significantly influencing short-term prognosis. In line with previous evidence, we observed significantly greater hematoma volumes in non-survivors compared to survivors.
However, the clinical course of ICH cannot be explained solely by mechanical injury. Secondary biological mechanisms, particularly inflammatory cascades, contribute substantially to neurological deterioration following hemorrhage.4 Microglial activation, pro-inflammatory cytokine release, oxidative stress, and disruption of the blood–brain barrier are key components of perihematomal injury.4 Elevated CRP levels have been associated with worsening neurological status and poor clinical outcomes,5 while hypoalbuminemia has been linked to increased mortality in cerebrovascular disease.6 Albumin is known to possess antioxidant and anti-inflammatory properties and may exert protective effects in acute brain injury.7 Additionally, the interaction between systemic inflammation and nutritional status during acute illness has been well documented.8 Inflammation-based hematological indices, such as the neutrophil-to-lymphocyte ratio, have also been reported to predict hemorrhagic complications and unfavorable outcomes.9
The CALLY index integrates CRP, albumin, and lymphocyte count into a composite marker that reflects inflammatory burden, immune competence, and nutritional status. Initially introduced in oncological research as a prognostic indicator,10 the CALLY index has subsequently been evaluated in acute ischemic stroke. Lower CALLY index values have been associated with hemorrhagic transformation and unfavorable functional outcomes,11 and independent prognostic significance has been reported in patients undergoing endovascular therapy.12 These findings support the biological plausibility of the CALLY index as a marker of systemic inflammatory response in cerebrovascular disease.
In our cohort, the CALLY index demonstrated moderate predictive performance for in-hospital mortality but did not outperform hematoma volume. This finding may be explained by the dominant influence of structural injury in the early phase of ICH. While inflammatory processes undoubtedly contribute to secondary brain damage, hematoma volume remains the principal determinant of acute mortality. The limited incremental value observed in reclassification analyses further suggests that inflammation-based biomarkers may complement—but not replace—established structural predictors.
Another potential explanation for the absence of superiority of the CALLY index lies in the complexity of inflammatory dynamics in hemorrhagic stroke. Single time-point laboratory measurements may not fully capture the evolving inflammatory response. Serial assessment of inflammatory biomarkers might provide additional prognostic insight, an aspect that was not addressed in the present study.
Conclusion
In this study, we evaluated the prognostic performance of the C-reactive protein–albumin–lymphocyte (CALLY) index for predicting in-hospital mortality in patients with spontaneous intracerebral hemorrhage and compared it with hematoma volume. Both the CALLY index and hematoma volume demonstrated moderate discriminative ability for mortality prediction. However, no statistically significant difference was observed between the two models, and the incremental prognostic contribution of the CALLY index beyond hematoma volume was limited. These findings suggest that structural factors such as hematoma volume may play a major role in early mortality; however, this interpretation should be considered cautiously given the absence of multivariable adjustment.
Study Limitations
This study has several limitations. First, its retrospective and single-center design may introduce selection bias and limit the generalizability of the findings. Second, the relatively small sample size may have reduced the statistical power to detect subtle differences between models. In addition, long-term functional outcomes were not evaluated, and dynamic changes in the CALLY index were not assessed through serial measurements. These factors may have limited a more comprehensive understanding of the prognostic role of inflammation over time. Nevertheless, the limited number of studies investigating the CALLY index in spontaneous intracerebral hemorrhage supports the originality and clinical relevance of our findings. Importantly, multivariable analysis demonstrated that the CALLY index did not retain independent prognostic significance after adjustment for established clinical and radiological predictors.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Gaziantep City Hospital Non-Interventional Clinical Research Ethics Committee (Decision date: December 17, 2025; Meeting No: 2025/376).
Author Contributions
Buket Yılmaz: Conceptualization; Methodology; Investigation; Data Curation; Writing – Original Draft; Writing – Review & Editing; Supervision.
Erman Altunışık: Methodology; Formal Analysis; Validation; Writing – Review & Editing.
Şeyda Dev: Data Curation; Investigation; Validation; Writing – Review & Editing.
Samet Parlak: Data Curation; Investigation; Validation; Writing – Review & Editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declares that no financial support was received for this research.
Disclosure
The authors declare that there are no conflicts of interest related to this study.
References
1. Feigin VL, Norrving B, Mensah GA, et al. World stroke organization: global stroke fact sheet 2025. Int J Stroke. 2025;20(2):132–8. doi:10.1177/17474930241308142
2. Broderick JP, Brott T, Tomsick T, et al. Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke. 1993;24(7):987–993. doi:10.1161/01.STR.24.7.987
3. Davis SM, Broderick J, Hennerici M, et al. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology. 2006;66(8):1175–1181. doi:10.1212/01.wnl.0000208408.98482.99
4. Zhang Q, Jia M, Wang Y, Wang Q, Wu J. Cell death mechanisms in cerebral Ischemia–Reperfusion Injury. Neurochem Res. 2022;47(12):3525–3542. doi:10.1007/s11064-022-03697-8
5. Seo W-K, Seok H-Y, Kim JH, et al. C-reactive protein is a predictor of early neurologic deterioration in acute ischemic stroke. J Stroke Cerebrovasc Dis. 2012;21(3):181–186. doi:10.1016/j.jstrokecerebrovasdis.2010.06.002
6. Bucci T, Pastori D, Pignatelli P, et al. Albumin levels and risk of early cardiovascular complications after ischemic stroke. Stroke. 2024;55(3):604–612. doi:10.1161/STROKEAHA.123.044248
7. Taverna M, Marie A-L, Mira J-P, Guidet B. Specific antioxidant properties of human serum albumin. Ann Intensive Care. 2013;3(1):4. doi:10.1186/2110-5820-3-4
8. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
9. Pikija S, Sztriha LK, Killer-Oberpfalzer M, et al. Neutrophil to lymphocyte ratio predicts intracranial hemorrhage after endovascular thrombectomy. J Neuroinflamma. 2018;15(1):319. doi:10.1186/s12974-018-1359-2
10. Müller L, Hahn F, Mähringer-Kunz A, et al. Immunonutritive scoring for patients with hepatocellular carcinoma undergoing transarterial chemoembolization: evaluation of the CALLY index. Cancers. 2021;13(19):5018. doi:10.3390/cancers13195018
11. Pan Y, Liu Z, Tu R, et al. The value of the CRP-albumin-lymphocyte index (CALLY index) as a prognostic biomarker in acute ischemic stroke. Sci Rep. 2025;15(1):13672. doi:10.1038/s41598-025-97538-7
12. Zhu L, Jie S, Wu S, et al. Ineffective recanalization and complications in patients with acute ischemic stroke receiving endovascular treatment: predictive value of the C-reactive protein-albumin-lymphocyte (CALLY) index. J Inflamm Res. 2025;18:14649–14661. doi:10.2147/JIR.S535881
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Albumin Level is Associated with Short-Term and Long-Term Outcomes in Sepsis Patients Admitted in the ICU: A Large Public Database Retrospective Research
Cao Y, Su Y, Guo C, He L, Ding N
Clinical Epidemiology 2023, 15:263-273
Published Date: 3 March 2023
Neutrophil Percentage-to-Albumin Ratio and Risk of Mortality in Patients on Peritoneal Dialysis
Yu Y, Zhong Z, Yang W, Yu J, Li J, Guo X, Chen J, Mao H, Li Z
Journal of Inflammation Research 2023, 16:6271-6281
Published Date: 21 December 2023
Association Between the C-Reactive Protein–Albumin–Lymphocyte Index and Endometriosis: Insights from the 1999–2006 National Health and Nutrition Examination Survey
Xu X, Cheng H, Ye X, Chang X
International Journal of Women's Health 2025, 17:4267-4280
Published Date: 7 November 2025
A Correlational Study on CALLY Index as a Potential Predictive Indicator for Postoperative in-Hospital Mortality in Acute Aortic Dissection Patients
Zhang H, Jiang F, Lin J, Yu X, Peng Y, Chen L, Lin Y
Journal of Inflammation Research 2025, 18:15833-15846
Published Date: 11 November 2025
Association Between Systemic Immune-Inflammation Index and in-Hospital and Long-Term All-Cause Mortality in Patients with Type 2 Diabetes Mellitus Complicated by Spontaneous Intracerebral Hemorrhage
Shen Y, Gao A, Shen Y, Gao S, Rong Y, Fan Z, Li Q, Lin T, Yang S, Liang H
Journal of Inflammation Research 2026, 19:549520
Published Date: 10 January 2026