Back to Journals » Cancer Management and Research » Volume 18

Prognostic Significance of Sarcopenia in Colorectal Cancer: A Review of Clinical Evidence
Received 2 September 2025
Accepted for publication 18 March 2026
Published 28 March 2026 Volume 2026:18 564390
DOI https://doi.org/10.2147/CMAR.S564390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Shuang Chen,1,2 Peng-ji Gao1,2
1Department of General Surgery, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China; 2Beijing Research Institute of Traumatology and Orthopaedics, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China
Correspondence: Peng-ji Gao, Department of General Surgery, Beijing Jishuitan Hospital, Capital Medical University, No. 31, Xinjiekou East Street, Xicheng District, Beijing, 100035, People’s Republic of China, Tel +8601058398275, Email [email protected]
Background: Colorectal cancer (CRC) is one of the most common and deadly malignancies worldwide. Sarcopenia, defined as a progressive loss of skeletal muscle mass and function, has recently been recognized as an important prognostic factor in CRC, influencing both postoperative complications and long-term survival.
Methods: We conducted a descriptive review of 18 clinical studies investigating the association between sarcopenia and CRC across stages I–IV. Sarcopenia was primarily assessed using computed tomography-derived skeletal muscle index (SMI) or psoas index (PI) at the lumbar vertebrae (L3/L4), with some studies additionally incorporating muscle strength and performance.
Results: The prevalence of sarcopenia among CRC patients ranged from 12% to 60%. Most studies reported higher risks of postoperative complications in sarcopenic patients. For instance, Peng et al demonstrated an increased risk of complications in stage IV CRC patients with sarcopenia (OR: 3.12, 95% CI: 1.14– 8.49). Regarding survival, sarcopenia was consistently associated with worse overall survival (OS), disease-free survival (DFS), and recurrence-free survival (RFS). Brown et al (2018) showed that deterioration in muscle mass and radiodensity significantly predicted poorer OS in 1,924 stage I–III CRC patients (HR: 2.15, 95% CI: 1.59– 2.92). However, several studies reported no significant associations.
Conclusion: Sarcopenia is prevalent in CRC patients and strongly correlates with both short-term surgical outcomes and long-term prognosis. However, current evidence is mainly derived from heterogeneous observational studies, and further prospective studies are needed before sarcopenia assessment can be translated into routine clinical practice.
Keywords: colorectal cancer, sarcopenia, skeletal muscle index, prognosis, postoperative complications, survival
Introduction
Colorectal cancer (CRC) is one of the most common malignancies worldwide, ranking third in global cancer incidence and second in cancer-related mortality.1 In 2020, nearly 2 million new CRC cases and approximately 1 million CRC-related deaths were reported globally, accounting for 10.7% of all newly diagnosed cancers and 9.5% of all cancer deaths.2 The prognosis of CRC patients is primarily determined by tumor stage and the feasibility of curative surgery. However, progressive loss of skeletal muscle mass has also been shown to strongly correlate with increased risk of postoperative complications and mortality.3,4 Sarcopenia, together with cancer-associated cachexia, represents the two major etiologies of muscle loss in patients with malignancies, including CRC.5,6
The concept of sarcopenia was first introduced by Rosenberg in 1989, initially referring to age-related decline in muscle mass.7 The term itself derives from Greek, in which sarx means “flesh” and penia denotes “loss.” Accumulating evidence suggests that sarcopenia may contribute to higher rates of perioperative complications, enhanced susceptibility to chemotherapy- and radiotherapy-related toxicities, and unfavorable survival outcomes among CRC patients.8–10
Despite the growing body of literature on sarcopenia in colorectal cancer, including several systematic reviews and meta-analyses,11,12 substantial heterogeneity remains across published studies. In particular, variability has been reported in diagnostic cut-off values, CT-based assessment approaches, and in the prognostic effects observed across different tumor stages and clinical endpoints.3,4,12–14 As a result, the interpretation and clinical relevance of sarcopenia in CRC remain incompletely clarified.
Therefore, rather than providing another quantitative synthesis, the aim of this review is to offer a descriptive overview of the existing clinical evidence and to discuss potential sources of heterogeneity reported in the literature. We sought to summarize the associations between sarcopenia and postoperative outcomes as well as long-term survival in CRC, while highlighting areas where current evidence appears inconsistent or limited.
Definition and Diagnostic Criteria of Sarcopenia
Since its introduction by Rosenberg, sarcopenia has progressively evolved to be defined as an age-related decline in skeletal muscle mass accompanied by a reduction in muscle strength.15 The first operational consensus was proposed by the European Working Group on Sarcopenia in Older People (EWGSOP) in 2010. This consensus emphasized that sarcopenia should be diagnosed based on the coexistence of low muscle mass and low muscle function (strength or performance), and it provided a diagnostic algorithm centered on gait speed, handgrip strength, and muscle mass assessment.16 In 2018, the group reconvened (EWGSOP2) and revised the definition by placing low muscle strength at the core of sarcopenia diagnosis. According to this updated framework, reduced muscle strength alone is sufficient to indicate “probable sarcopenia.” Confirmation requires evidence of low muscle quantity or quality, while the presence of both these features plus impaired physical performance establishes a diagnosis of severe sarcopenia.17
The etiology of sarcopenia is multifactorial. Based on underlying causes, sarcopenia can be broadly categorized into two types: primary sarcopenia, which is predominantly age-related and occurs in the absence of other apparent causes; and secondary sarcopenia, which results from other conditions such as physical inactivity, malignancy, organ failure, chronic inflammatory diseases, or malnutrition.14,16
These consensus definitions provide important context for understanding sarcopenia; however, in clinical oncology practice, sarcopenia is most commonly assessed using imaging-based measures.
Methods
A literature search was performed using PubMed to identify relevant studies published up to December 2024. The search terms included combinations of “colorectal cancer”, “colon cancer”, “rectal cancer”, and “sarcopenia.” Reference lists of relevant reviews and original articles were also screened to identify additional eligible studies.
Studies were considered for inclusion if they met the following criteria: (1) involved adult patients diagnosed with colorectal cancer; (2) evaluated sarcopenia using imaging-based measures, most commonly computed tomography-derived skeletal muscle indices; and (3) reported clinical outcomes, including postoperative complications and/or survival outcomes such as overall survival, disease-free survival, or recurrence-free survival. Reviews, conference abstracts, case reports, and studies lacking relevant outcome data were excluded.
A total of 18 studies met these criteria and were included in the present review.8,9,13,18–32 Given the heterogeneity in study design, sarcopenia definitions, and outcome measures, no formal meta-analysis was performed, and the findings were synthesized descriptively.
Results
To investigate the current progress in sarcopenia research within CRC, we conducted a descriptive review of 18 published studies examining the relationship between sarcopenia and CRC (Table 1). We found that the majority of CRC patients with concurrent sarcopenia were elderly individuals. In most studies, sarcopenia was diagnosed based on the skeletal muscle index (SMI) at the level of the third or fourth lumbar vertebra, whereas a minority of studies employed the psoas muscle index at the same anatomical level for diagnosis.
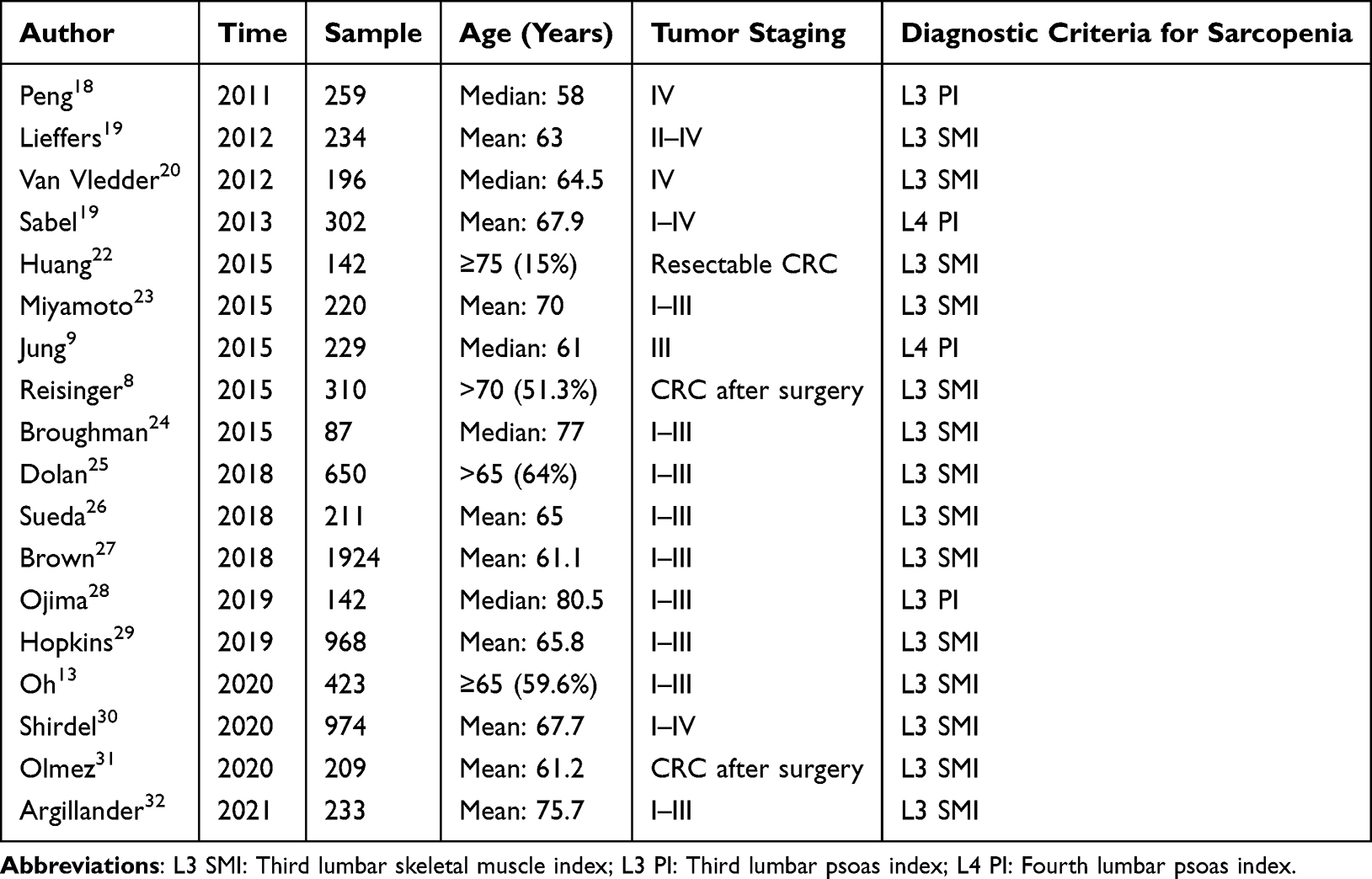 |
Table 1 Basic Information of the Included Studies |
Based on an analysis of 15 previously published studies (Table 2), we observed substantial variability in the reported prevalence of sarcopenia among patients with CRC. For instance, in a 2015 study by Huang et al, 142 resectable CRC patients were evaluated, and the prevalence of sarcopenia was reported to be only 12%. In contrast, Broughman et al (2020) investigated 87 patients with stage I–III CRC and reported a markedly higher prevalence of 57.4%. Taken together, these findings suggest that the prevalence of sarcopenia in CRC patients varies widely across studies, ranging from approximately 12% to 60%.
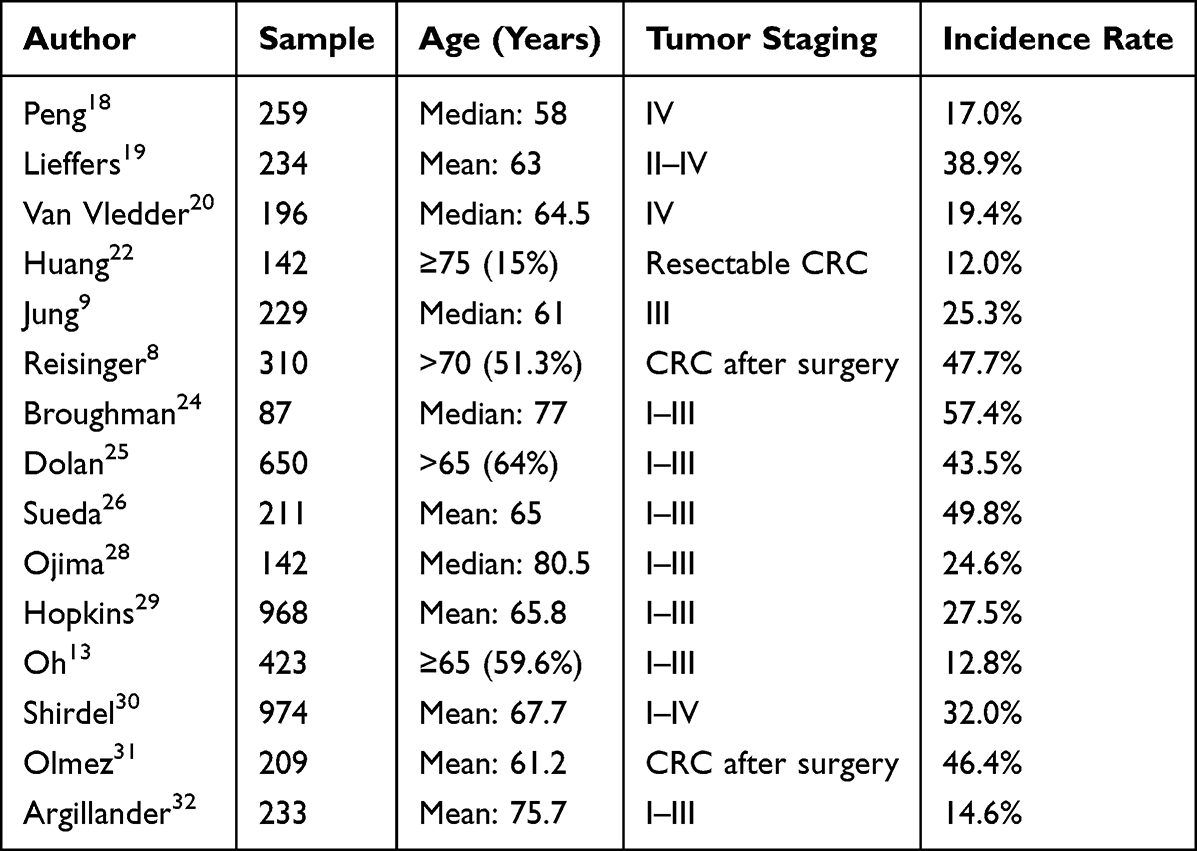 |
Table 2 Prevalence of Sarcopenia in Patients with CRC |
Subsequently, our focus shifted to the impact of sarcopenia on postoperative complications in CRC. A total of eight studies were included in this analysis (Table 3). The majority of these reports consistently demonstrated that CRC patients with sarcopenia had a higher likelihood of developing postoperative complications. For example, Peng et al investigated 259 patients with stage IV CRC and found that those with sarcopenia exhibited significantly higher rates of overall postoperative complications and infections compared with their non-sarcopenic counterparts. Similarly, a meta-analysis conducted by Levolger et al33 identified sarcopenia as an independent risk factor for both postoperative complications and postoperative mortality in CRC patients. Another meta-analysis by Su et al11 confirmed that preoperative sarcopenia was associated with an increased risk of overall postoperative morbidity.
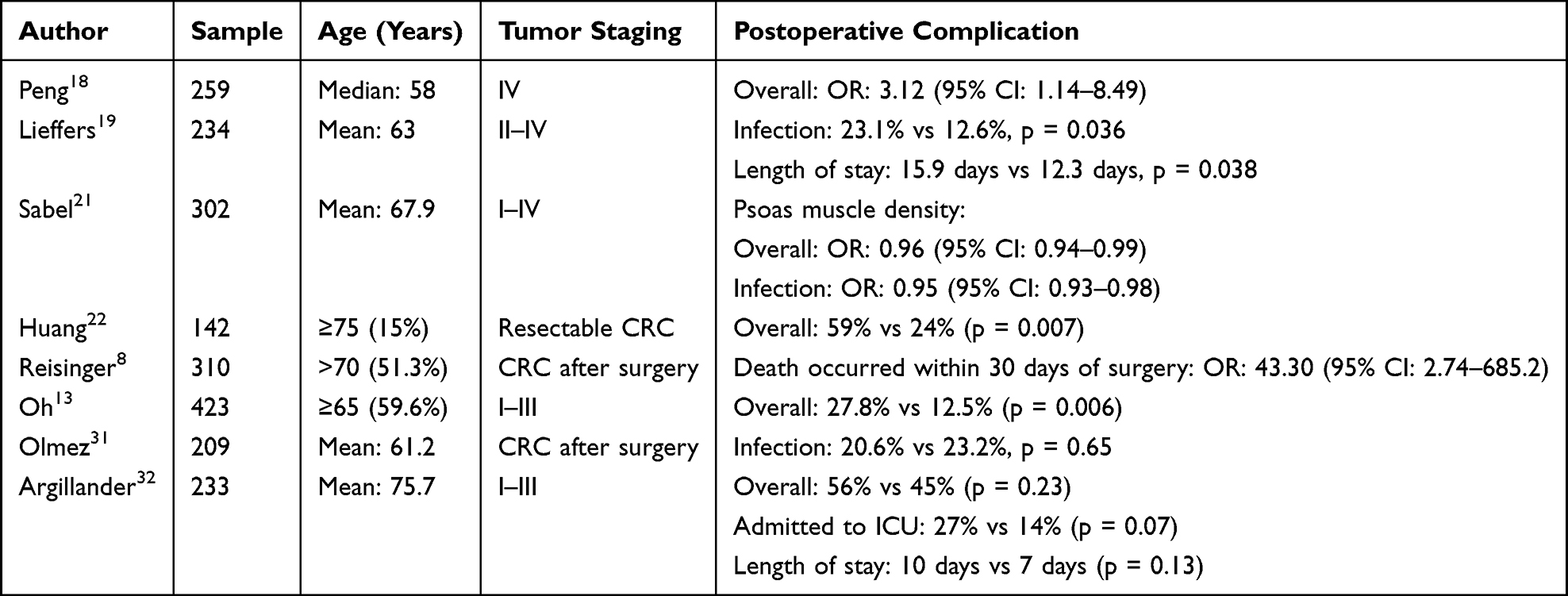 |
Table 3 Impact of Sarcopenia on Postoperative Complications in Patients with CRC |
However, a minority of studies reported conflicting results. For instance, Olmez et al observed no significant difference in postoperative infection rates between CRC patients with and without sarcopenia. Likewise, Argillander et al reported no significant differences in overall postoperative complication rates or length of hospital stay between sarcopenic and non-sarcopenic CRC patients.
To further explore the impact of sarcopenia on the prognosis of CRC, we analyzed 13 studies that reported overall survival (OS) outcomes in CRC patients (Table 4). The majority of these studies demonstrated that CRC patients with sarcopenia had shorter OS compared with those without sarcopenia. For example, a meta-analysis conducted by Levolger et al33 identified sarcopenia as an independent risk factor for reduced OS in CRC patients. Similarly, Su et al11 also reported that preoperative sarcopenia was associated with inferior OS in CRC.
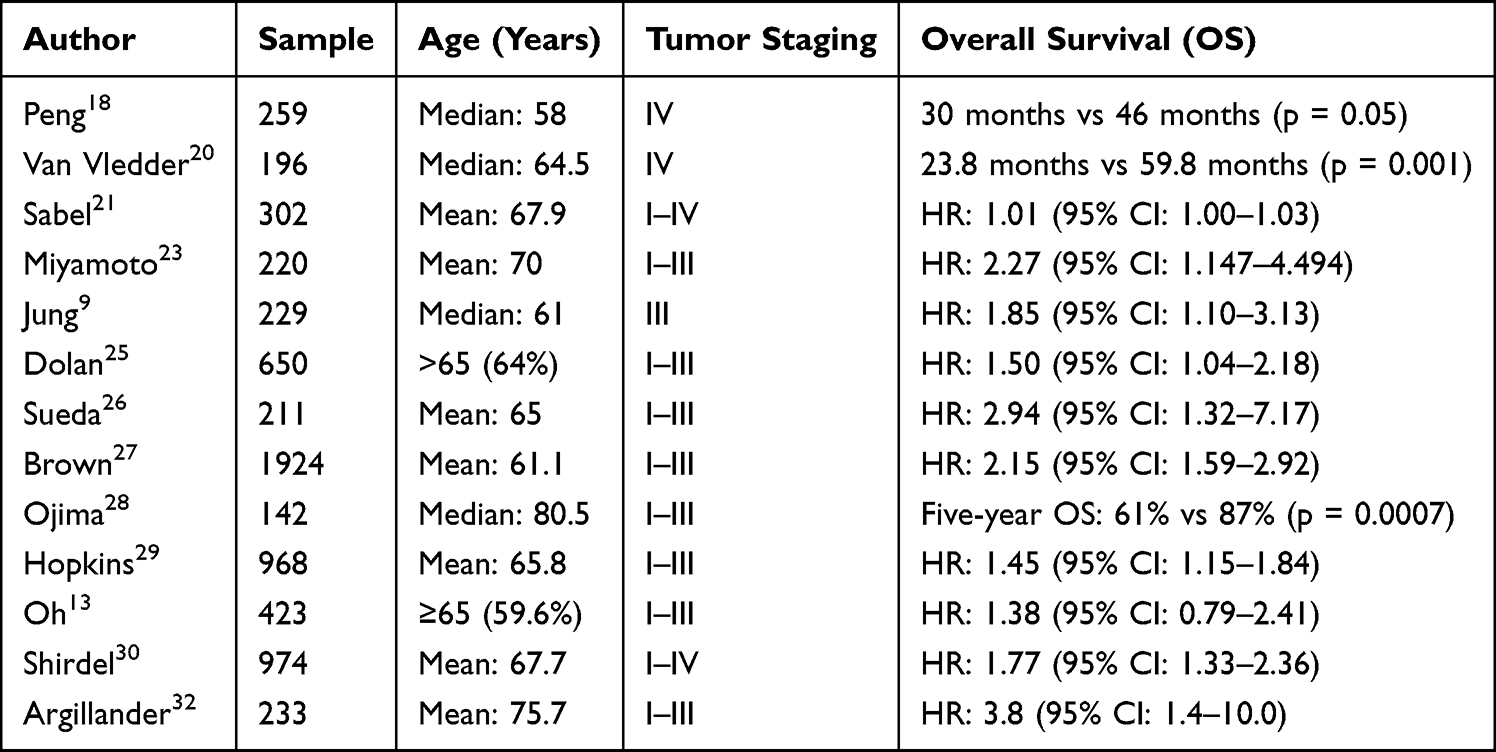 |
Table 4 Impact of Sarcopenia on Overall Survival in Patients with CRC |
Nevertheless, conflicting evidence exists. For instance, a study by Oh et al showed no significant difference in OS between CRC patients with and without sarcopenia.
In addition, we reviewed four studies that reported disease-free survival (DFS) outcomes in patients with CRC (Table 5). Most of these studies indicated that CRC patients with sarcopenia had shorter DFS compared with those without sarcopenia. A meta-analysis by Su et al11 further confirmed that preoperative sarcopenia was a significant risk factor for reduced DFS in CRC patients. However, consistent with the findings for overall survival, Oh et al reported contradictory results, showing no significant difference in DFS between CRC patients with and without sarcopenia.
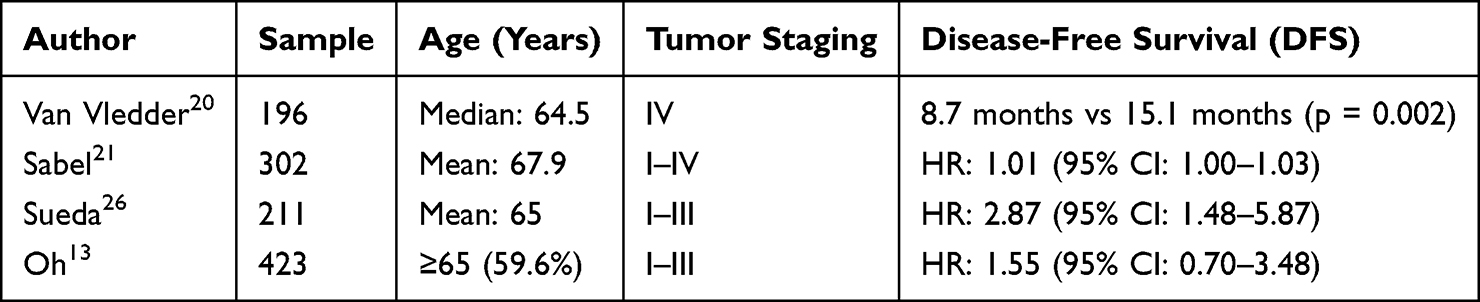 |
Table 5 Impact of Sarcopenia on Disease-Free Survival in Patients with CRC |
We further summarized three studies that reported recurrence-free survival (RFS) outcomes in patients with CRC (Table 6). These studies consistently demonstrated that CRC patients with sarcopenia had shorter RFS compared with those without sarcopenia.
 |
Table 6 Impact of Sarcopenia on Recurrence-Free Survival in Patients with CRC |
Discussion
This review summarizes the existing clinical evidence regarding the prognostic significance of sarcopenia in patients with colorectal cancer. Across the majority of included studies, sarcopenia was associated with increased postoperative complications and poorer long-term outcomes, including overall survival, disease-free survival, and recurrence-free survival.3,11,14,27 These findings suggest that reduced skeletal muscle mass and quality may reflect a vulnerable physiological state that adversely affects both short-term recovery and long-term oncologic outcomes in CRC.4,25
Several biological and clinical mechanisms may underlie the observed associations between sarcopenia and adverse outcomes. Sarcopenia often reflects impaired nutritional reserve, chronic systemic inflammation, and reduced physical resilience, which may limit tolerance to major surgery and systemic anticancer therapies.34–36 In addition, sarcopenic patients may be more susceptible to postoperative infections, delayed recovery, and treatment-related toxicity, thereby contributing to inferior survival outcomes.9,19
Importantly, the strength and consistency of the reported associations varied across studies. While many investigations demonstrated a clear relationship between sarcopenia and adverse outcomes,8,9,18–23,25–30 several studies reported no significant associations.13,31,32 This heterogeneity may be attributable to differences in study populations, tumor stages, clinical endpoints, and CT-based assessment approaches. Variability in the CT diagnostic cut-off values of sarcopenia may further limit the comparability of results across studies. For instance, Olmez et al31 defined sarcopenia as an L3 SMI of <545 mm2/m2 for men and <385 mm2/m2 for women. In contrast, Oh et al13 defined it as an L3 SMI of <41 cm2/m2 for women and <43 cm2/m2 for men with a body mass index (BMI) of <25 kg/m2, and <53 cm2/m2 for men with a BMI of ≥25 kg/m2.
Differences in tumor stage and treatment context may also contribute to inconsistent findings. In earlier-stage disease, sarcopenia may primarily reflect baseline frailty and physiological reserve, whereas in advanced or metastatic CRC, muscle loss may be more strongly influenced by tumor burden and systemic disease.18,20,30 Furthermore, postoperative outcomes and long-term survival represent distinct clinical endpoints that may be differentially influenced by sarcopenia. With respect to short-term postoperative outcomes, sarcopenia may reflect limited physiological and nutritional reserve, which can impair tolerance to surgical stress and delay recovery. Reduced skeletal muscle mass has been associated with a higher risk of postoperative complications, including infectious events and prolonged hospitalization, suggesting that muscle depletion may compromise perioperative resilience.11 In contrast, the impact of sarcopenia on long-term survival outcomes may be mediated through different mechanisms. Low muscle mass and adverse body composition profiles have been linked to systemic inflammatory responses and metabolic vulnerability, which are known to adversely affect oncologic outcomes and overall survival.25 In addition, sarcopenic patients may experience reduced tolerance to systemic anticancer therapies, leading to increased treatment-related toxicity, dose reductions, or early discontinuation of therapy. Such treatment limitations could, in turn, contribute to inferior disease control and survival outcomes.9 Taken together, these observations suggest that the associations between sarcopenia and adverse outcomes in colorectal cancer may arise through partially distinct pathways depending on the clinical endpoint considered, which could help explain discrepancies among studies evaluating postoperative complications versus long-term survival.
Several limitations of this review should be acknowledged. As a narrative review, no formal systematic search strategy or meta-analysis was performed, and the selection of included studies may be subject to selection bias. In addition, substantial heterogeneity in sarcopenia assessment methods and study design limits direct comparison across studies. Therefore, the findings of this review should be interpreted with caution. Future research should focus on standardized diagnostic criteria and prospective studies to clarify the clinical utility of sarcopenia assessment in colorectal cancer.
Conclusions
Sarcopenia is a common condition among patients with colorectal cancer and has been frequently associated with adverse postoperative outcomes and poorer long-term prognosis, including overall survival, disease-free survival, and recurrence-free survival. The available evidence suggests that reduced skeletal muscle mass and quality may reflect diminished physiological reserve and increased vulnerability in CRC patients. However, the existing literature is predominantly based on heterogeneous observational studies, with substantial variability in sarcopenia assessment methods, diagnostic cut-off values, patient populations, tumor stages, and clinical endpoints. As a result, the prognostic impact of sarcopenia in CRC cannot be interpreted uniformly across all clinical contexts. Therefore, while sarcopenia assessment may offer useful prognostic information and contribute to risk stratification in colorectal cancer, its routine application in clinical practice requires caution. Future studies employing standardized diagnostic criteria and well-designed prospective designs are needed to clarify the clinical utility of sarcopenia assessment and to determine whether targeted interventions can improve outcomes in patients with CRC.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Beijing Municipal Public Welfare Development and Reform Pilot Project for Medical Research Institutes (JYY2023-11, JYY2023-8).
Disclosure
The authors declared no competing interests in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca Cancer J Clin. 2021;71(3):209–8. doi:10.3322/caac.21660
2. Morgan E, Arnold M, Gini A, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023;72(2):338–344. doi:10.1136/gutjnl-2022-327736
3. Sun G, Li Y, Peng Y, et al. Can sarcopenia be a predictor of prognosis for patients with non-metastatic colorectal cancer? A systematic review and meta-analysis. Int J Colorectal Dis. 2018;33(10):1419–1427. doi:10.1007/s00384-018-3128-1
4. Cespedes Feliciano EM, Avrutin E, Caan BJ, et al. Screening for low muscularity in colorectal cancer patients: a valid, clinic-friendly approach that predicts mortality. J Cachexia Sarcopenia Muscle. 2018;9(5):898–908. doi:10.1002/jcsm.12317
5. Peterson SJ, Mozer M. Differentiating sarcopenia and cachexia among patients with cancer. Nutrit Clin Pract. 2017;32(1):30–39. doi:10.1177/0884533616680354
6. Zeng X, Chen S, Lin Y, et al. Acylated and unacylated ghrelin inhibit apoptosis in myoblasts cocultured with colon carcinoma cells. Oncol Rep. 2018;39(3):1387–1395. doi:10.3892/or.2018.6213
7. Rosenberg IH. Summary comments. Ame J Clin Nutrit. 1989;50(5):1231–1233. doi:10.1093/ajcn/50.5.1231
8. Reisinger KW, van Vugt JLA, Tegels JJW, et al. Functional compromise reflected by sarcopenia, frailty, and nutritional depletion predicts adverse postoperative outcome after colorectal cancer surgery. Ann Surg. 2015;261(2):345–352. doi:10.1097/SLA.0000000000000628
9. Jung H-W, Kim JW, Kim J-Y, et al. Effect of muscle mass on toxicity and survival in patients with colon cancer undergoing adjuvant chemotherapy. Supportive Care Cancer. 2015;23(3):687–694. doi:10.1007/s00520-014-2418-6
10. Choi MH, Oh SN, Lee IK, et al. Sarcopenia is negatively associated with long-term outcomes in locally advanced rectal cancer. J Cachexia Sarcopenia Muscle. 2018;9(1):53–59. doi:10.1002/jcsm.12234
11. Su H, Ruan J, Chen T, et al. CT-assessed sarcopenia is a predictive factor for both long-term and short-term outcomes in gastrointestinal oncology patients: a systematic review and meta-analysis. Cancer Imaging. 2019;19(1):82. doi:10.1186/s40644-019-0270-0
12. Benedek Z, Coroș MF. The impact of sarcopenia on the postoperative outcome in colorectal cancer surgery. Med Pharm Rep. 2023;96(1):20–27. doi:10.15386/mpr-2483
13. Oh RK, Ko HM, Lee JE, et al. Clinical impact of sarcopenia in patients with colon cancer undergoing laparoscopic surgery. Ann Surg Treatment Res. 2020;99(3):153–160. doi:10.4174/astr.2020.99.3.153
14. Takiguchi K, Furuya S, Sudo M, et al. Prognostic effect of sarcopenia in colorectal cancer recurrence. Nutrition. 2021;91-92:111362. doi:10.1016/j.nut.2021.111362
15. Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127(5):990s–1s. doi:10.1093/jn/127.5.990S
16. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
17. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
18. Peng PD, Van Vledder MG, Tsai S, et al. Sarcopenia negatively impacts short-term outcomes in patients undergoing hepatic resection for colorectal liver metastasis. HPB. 2011;13(7):439–446. doi:10.1111/j.1477-2574.2011.00301.x
19. Lieffers JR, Bathe OF, Fassbender K, et al. Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br J Cancer. 2012;107(6):931–936. doi:10.1038/bjc.2012.350
20. Van Vledder MG, Levolger S, Ayez N, et al. Body composition and outcome in patients undergoing resection of colorectal liver metastases. Br J Surg. 2012;99(4):550–557. doi:10.1002/bjs.7823
21. Sabel MS, Terjimanian M, Conlon ASC, et al. Analytic morphometric assessment of patients undergoing colectomy for colon cancer. J Surg Oncol. 2013;108(3):169–175. doi:10.1002/jso.23366
22. Huang DD, Wang SL, Zhuang CL, et al. Sarcopenia, as defined by low muscle mass, strength and physical performance, predicts complications after surgery for colorectal cancer. Colorectal Dis. 2015;17(11):O256–64. doi:10.1111/codi.13067
23. Miyamoto Y, Baba Y, Sakamoto Y, et al. Sarcopenia is a negative prognostic factor after curative resection of colorectal cancer. Ann Surg Oncol. 2015;22(8):2663–2668. doi:10.1245/s10434-014-4281-6
24. Broughman JR, Williams GR, Deal AM, et al. Prevalence of sarcopenia in older patients with colorectal cancer. J Geriatric Oncol. 2015;6(6):442–445. doi:10.1016/j.jgo.2015.08.005
25. Dolan RD, Almasaudi AS, Dieu LB, et al. The relationship between computed tomography-derived body composition, systemic inflammatory response, and survival in patients undergoing surgery for colorectal cancer. J Cachexia Sarcopenia Muscle. 2019;10(1):111–122. doi:10.1002/jcsm.12357
26. Sueda T, Takahasi H, Nishimura J, et al. Impact of low muscularity and myosteatosis on long-term outcome after curative colorectal cancer surgery: a propensity score–matched analysis. Dis Colon Rectum. 2018;61(3):364–374. doi:10.1097/DCR.0000000000000958
27. Brown JC, Caan BJ, Meyerhardt JA, et al. The deterioration of muscle mass and radiodensity is prognostic of poor survival in stage I–III colorectal cancer: a population-based cohort study (C-SCANS). J Cachexia Sarcopenia Muscle. 2018;9(4):664–672. doi:10.1002/jcsm.12305
28. Ojima Y, Harano M, Sumitani D, et al. Impact of preoperative skeletal muscle mass and quality on the survival of elderly patients after curative resection of colorectal cancer. J Anus Rectum Colon. 2019;3(4):143–151. doi:10.23922/jarc.2018-034
29. Hopkins JJ, Reif RL, Bigam DL, et al. The impact of muscle and adipose tissue on long-term survival in patients with stage I to III colorectal cancer. Dis Colon Rectum. 2019;62(5):549–560. doi:10.1097/DCR.0000000000001352
30. Shirdel M, Andersson F, Myte R, et al. Body composition measured by computed tomography is associated with colorectal cancer survival, also in early-stage disease. Acta oncologica. 2020;59(7):799–808. doi:10.1080/0284186X.2020.1744716
31. Olmez T, Karakose E, Keklikkiran ZZ, et al. Relationship between sarcopenia and surgical site infection in patients undergoing colorectal cancer surgical procedures. Surg Infect. 2020;21(5):451–456. doi:10.1089/sur.2019.285
32. Argillander TE, Spek D, Van Der Zaag-Loonen HJ, et al. Association between postoperative muscle wasting and survival in older patients undergoing surgery for non-metastatic colorectal cancer. J Geriatric Oncol. 2021;12(7):1052–1058. doi:10.1016/j.jgo.2021.04.004
33. Levolger S, Van Vugt JL, de Bruin RW, et al. Systematic review of sarcopenia in patients operated on for gastrointestinal and hepatopancreatobiliary malignancies. Br J Surg. 2015;102(12):1448–1458. doi:10.1002/bjs.9893
34. Roubenoff R. Catabolism of aging: is it an inflammatory process? Curr Opin Clin Nutr Metab Care. 2003;6(3):295–299. doi:10.1097/01.mco.0000068965.34812.62
35. Lyu W, Tanaka T, Son BK, et al. Associations of nutrition-related, physical, and social factors and their combinations with sarcopenia in community-dwelling older adults: Kashiwa cohort study. Nutrients. 2022;14(17):3544. doi:10.3390/nu14173544
36. Ghiotto L, Muollo V, Tatangelo T, et al. Exercise and physical performance in older adults with sarcopenic obesity: a systematic review. Front Endocrinol. 2022;13:913953. doi:10.3389/fendo.2022.913953
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
IGFBP5 is Upregulated and Associated with Poor Prognosis in Colorectal Cancer
Deng Y, Yang X, Hua H, Zhang C
International Journal of General Medicine 2022, 15:6485-6497
Published Date: 6 August 2022
Low Pre-ChemoradiotherapyPan-Immune-Inflammation Value (PIV) Measures Predict Better Survival Outcomes in Locally Advanced Pancreatic Adenocarcinomas
Topkan E, Selek U, Kucuk A, Pehlivan B
Journal of Inflammation Research 2022, 15:5413-5423
Published Date: 18 September 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023
Impact of Preoperative Neutrophil Percentage-to-Albumin Ratio (NPAR) on Short-Term Complications and Long-Term Prognosis in Patients Undergoing Robot-Assisted Laparoscopic Radical Surgery for Colorectal Cancer
Wang J, Hu T, Yu N
Journal of Inflammation Research 2026, 19:556408
Published Date: 13 February 2026
SLC2A3 Expression is Differentially Associated with Postoperative Recurrence, Complications, and Liver Metastasis in Colorectal Cancer
Peng S, Zuo J, Wang Z, Zheng K, Lu F
Cancer Management and Research 2026, 18:594748
Published Date: 8 May 2026