Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Prevalence and Factors Associated with Type 2 Diabetes Self-Management Among Patients Attending Mbale Regional Referral Hospital: A Cross-Sectional Study in Eastern Uganda
Authors Makonje R, Omolo RO ![]() , Mudenda S, Mugenyi N
, Mudenda S, Mugenyi N ![]()
Received 4 February 2026
Accepted for publication 13 May 2026
Published 23 May 2026 Volume 2026:19 598398
DOI https://doi.org/10.2147/DMSO.S598398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Rogers Makonje,1 Ronald Ouma Omolo,2 Steward Mudenda,3 Nathan Mugenyi4
1Department of Nursing, Faculty of Health Sciences, Victoria University, Kampala, Uganda; 2Department of Physiology, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 3Department of Pharmacy, School of Health Sciences, University of Zambia, Lusaka, Zambia; 4Department of Community Health, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda
Correspondence: Ronald Ouma Omolo, Department of Physiology, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda, Email [email protected]
Background: Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder that requires sustained self-management to achieve optimal glycemic control and prevent long-term complications. Effective self-management involves adherence to medication, healthy diet, physical activity, blood glucose monitoring, and regular clinic attendance. However, evidence suggests that self-management practices remain suboptimal in many low- and middle-income countries, including Uganda, and data from regional referral hospitals are limited. This study aimed to determine the prevalence of self-management practices and identify factors associated with effective self-management among patients with T2DM receiving care at Mbale Regional Referral Hospital, Eastern Uganda.
Methods: A hospital-based cross-sectional study was conducted between among 385 adults with T2DM attending the diabetes clinic. Participants were selected using systematic random sampling from the clinic registry. Data were collected using a structured interviewer-administered questionnaire, including the Diabetes Self-Management Questionnaire (DSMQ). DSMQ total scores were transformed to a 0– 100 scale, with a cut-off of ≥ 70% defining good self-management. Descriptive statistics summarized participants’ characteristics, and bivariate and multivariable logistic regression analyses were performed using STATA version 17.0 to identify factors independently associated with good self-management.
Results: Only 34.6% (133/385) of participants demonstrated good self-management. Factors independently associated with good self-management included higher education level (AOR = 2.4, 95% CI: 1.52– 4.81, p=0.001), employment (AOR = 5.3, 95% CI: 3.53– 9.18, p=0.02), higher monthly income (AOR = 3.2, 95% CI: 1.52– 5.98, p=0.001), shorter diabetes duration (1– 5 years vs > 10 years; AOR = 2.7, 95% CI: 1.35– 8.25, p=0.005), awareness of diabetes complications (AOR = 3.1, 95% CI: 1.70– 5.76, p=0.041), and family support (AOR = 2.1, 95% CI: 1.60– 7.74, p=0.006). General diabetes knowledge was not significantly associated with self-management.
Conclusion: The prevalence of good self-management among T2DM patients at Mbale Regional Referral Hospital is low. Socio-economic factors, awareness of diabetes complications, shorter disease duration, and family support significantly influence self-management behaviors. Interventions targeting these factors are essential to improve diabetes outcomes in this setting.
Keywords: type 2 diabetes, self-management, Mbale Regional Referral Hospital, prevalence, associated factors, Uganda
Introduction
Diabetes mellitus, particularly Type 2 diabetes mellitus (T2DM), is a major global public health challenge, contributing substantially to morbidity, mortality, and healthcare expenditure. According to the most recent estimates from the International Diabetes Federation, approximately 589 million adults aged 20–79 years were living with diabetes globally in 2024, and this number is projected to rise to 853 million by 2050, if current trends persist.1,2 The burden is disproportionately increasing in low- and middle-income countries, particularly in Sub-Saharan Africa, where health systems face significant constraints in prevention, diagnosis, and long-term management.2,3
In Sub-Saharan Africa, the rising prevalence of T2DM is driven by rapid urbanization, lifestyle transitions, and limited access to preventive and curative healthcare services.3,4 These challenges are compounded by inadequate health infrastructure, shortages of trained healthcare personnel, and sociocultural factors that influence health-seeking behavior.5 As a result, many patients experience delayed diagnosis, poor glycemic control, and a high risk of complications.
Uganda is experiencing a similar epidemiological transition, with a growing burden of non-communicable diseases alongside persistent infectious diseases. Recent estimates suggest that approximately 716,000 adults were living with diabetes in Uganda in 2021, with prevalence continuing to rise, particularly in urban and peri-urban areas.6,7 Despite this growing burden, access to comprehensive diabetes care, including patient education and long-term follow-up, remains limited in many parts of the country.7
Effective diabetes self-management, encompassing medication adherence, blood glucose monitoring, dietary modification, physical activity, and foot care, is a cornerstone of diabetes care and is essential for achieving optimal glycemic control and preventing complications.8,9 Diabetes self-management is a complex, patient-centered process that requires adequate knowledge, skills, motivation, psychosocial support, and engagement with healthcare providers.10 Poor self-management has been associated with increased rates of complications, hospitalization, reduced quality of life, and higher healthcare costs.11 Although diabetes education and counselling services have been introduced in some Ugandan health facilities, their availability and effectiveness remain limited, particularly in regional and rural settings.12,13
Regional referral hospitals such as Mbale Regional Referral Hospital serve as key access points for diabetes care in Eastern Uganda, managing large patient populations with diverse socioeconomic backgrounds. However, there is limited empirical evidence on the level of diabetes self-management and its determinants within such settings. Understanding these factors is critical for designing targeted, context-specific interventions aimed at improving self-management behaviors, reducing complications, and strengthening diabetes care within the Ugandan healthcare system.
Therefore, this study aimed to determine the prevalence of diabetes self-management practices and identify factors associated with effective self-management among patients with T2DM attending Mbale Regional Referral Hospital.
Materials and Methods
Study Design
A hospital-based cross-sectional study was conducted to determine the prevalence of self-management practices and factors associated with self-management among patients with Type 2 diabetes mellitus (T2DM). The cross-sectional design enabled the assessment of self-management behaviors and associated socio-demographic, clinical, behavioral, and psychosocial factors at a single point in time.
Study Setting
The study was conducted at Mbale Regional Referral Hospital (MRRH), a tertiary public health facility located in Mbale City, Eastern Uganda (01°04′36.0″N, 34°10′35.0″E). MRRH serves as the main referral hospital for several districts in Eastern Uganda and provides specialized outpatient services, including a dedicated diabetes clinic that manages a large number of patients with T2DM. The diabetes clinic operates on scheduled clinic days and offers routine follow-up, medication refills, and diabetes education, making it an appropriate setting for this study.
Study Population
The study population consisted of adult patients diagnosed with T2DM and receiving routine care at the diabetes clinic of MRRH during the study period.
Eligibility Criteria
Inclusion criteria were adults aged 18 years and above with a confirmed diagnosis of T2DM for at least six months, who were regularly attending the diabetes clinic at MRRH and provided written informed consent. The six-month threshold was applied to ensure that participants had sufficient time since diagnosis to initiate and establish routine self-management behaviors, thereby allowing for a more stable and reliable assessment of self-management practices. Exclusion criteria included pregnant women (due to the distinct management of gestational diabetes), patients with severe cognitive impairment or critical illness that limited their ability to respond to the questionnaire, and patients who declined to provide consent.
Sample Size Determination
The sample size was calculated using Cochran’s formula for cross-sectional studies:

Where; n is the required sample size, Z is the standard normal deviate at 95% confidence level (1.96), p is the estimated prevalence of good diabetes self-management (assumed to be 50% due to lack of precise local estimates), and d is the margin of error set at 5%. The calculated minimum sample size was 385 participants.
Sampling Procedure
A systematic random sampling technique was employed. The diabetes clinic registry served as the sampling frame. The sampling interval (k) was determined by dividing the estimated number of patients attending the diabetes clinic during the data collection period (N) by the required sample size (n), such that k = N/n. A random starting point between 1 and k was selected using a simple random method (eg, ballot technique), after which every kth eligible patient was approached for participation. In cases where a selected patient did not meet the eligibility criteria or declined participation, the next eligible patient was recruited to maintain the sampling sequence.
Study Variables
The dependent variable was diabetes self-management practice, categorized as good or poor. The independent variables included: Socio-demographic factors such as age, sex, marital status, education level, employment status, monthly income, and place of residence (urban/rural). Clinical factors were; duration of diabetes, presence of comorbidities (eg, hypertension), type of diabetes treatment, frequency of clinic visits, and access to healthcare services. Knowledge and awareness factors included; knowledge of diabetes management and awareness of diabetes-related complications. Behavioral factors: medication adherence, dietary practices, physical activity, smoking, and alcohol consumption. Psychosocial factors: family and social support, stress levels, attitudes towards self-management, and health-seeking behavior. Then, environmental and cultural factors: access to diabetes care resources, availability of medications and self-monitoring tools, food environment, and cultural beliefs influencing diet and lifestyle. Healthcare access and healthcare accessibility were treated as distinct variables. Healthcare access captured general utilization and availability of services, whereas healthcare accessibility reflected participants’ perceived ease or difficulty in obtaining care.
Data Collection Tool and Procedure
Data were collected using a structured interviewer-administered questionnaire adapted from validated diabetes self-management instruments, including the Diabetes Self-Management Questionnaire (DSMQ). The questionnaire comprised sections on socio-demographic characteristics, clinical history, diabetes-related knowledge, and self-management behaviors. The questionnaire was pretested among approximately 10% of the calculated sample size at a nearby healthcare facility not included in the main study. The pretest assessed clarity, content validity, and reliability of the instrument. Feedback from the pilot study informed minor revisions to improve question wording and flow. The DSMQ was reviewed for contextual relevance, and minor wording modifications were made to enhance clarity for the study population without altering the underlying constructs. The DSMQ has previously demonstrated good internal consistency and validity across diverse populations.14 Face-to-face interviews were conducted by trained research assistants fluent in English and the local language. Interviews were conducted in a private setting within the clinic to ensure confidentiality and encourage accurate responses.
Measurement of Diabetes Self-Management
Diabetes self-management was assessed using the Diabetes Self-Management Questionnaire (DSMQ), developed by Schmitt et al.14 The DSMQ consists of 16 items measuring self-care behaviors related to glycemic control over the preceding eight weeks. Responses were scored on a four-point Likert scale ranging from 0 (“does not apply to me”) to 3 (“applies to me very much”). Negatively worded items were reverse-coded before analysis. The DSMQ items were organized into four subscales: glucose management, dietary control, physical activity, and healthcare use. A total self-management score was computed by summing up all item scores and transforming them to a scale of 0–100. Higher scores indicated better self-management practices. For analytical purposes, self-management was dichotomized into good and poor using a cut-off of ≥70% of the total possible score. This threshold has been applied in previous studies assessing diabetes self-management using composite indices to distinguish between adequate and suboptimal self-care behaviors.14–16 The use of a 70% cut-off is considered a pragmatic approach for categorizing self-management levels in epidemiological analyses where standardized thresholds are not universally established.
Data Management and Analysis
Completed questionnaires were reviewed daily for completeness and consistency. Data were entered into Kobo Toolbox and subsequently exported to STATA version 17.0 (Stata Corp, College Station, TX, USA) for analysis. Double data entry and routine consistency checks were performed to minimize data entry errors. All electronic data were password-protected, and hard-copy questionnaires were stored securely with access restricted to the research team. Descriptive statistics were used to summarize participants’ socio-demographic, clinical, and behavioral characteristics. Categorical variables were described using frequencies and percentages, while continuous variables were summarized using means and standard deviations. The prevalence of diabetes self-management was determined by calculating the proportion of participants who demonstrated good self-management practices based on the Diabetes Self-Management Questionnaire (DSMQ) score. Individual DSMQ total scores were computed by summing up the item responses and transforming the scores to a scale of 0–100. Participants with a total DSMQ score of ≥70% were classified as having good self-management, while those with scores <70% were classified as having poor self-management. The prevalence of good self-management was then calculated as:

Chi-square tests were used for initial bivariate comparisons, while logistic regression analysis was performed to estimate crude and adjusted odds ratios, allowing for control of potential confounders and assessment of independent predictors. Bivariate logistic regression analysis was conducted to assess the association between each independent variable and diabetes self-management status (good vs poor). Variables with a p-value <0.20 at bivariate analysis were considered for inclusion in the multivariable logistic regression model to control for potential confounding. Multivariable logistic regression was performed to identify factors independently associated with good diabetes self-management. Adjusted odds ratios (AORs) with corresponding 95% confidence intervals (CIs) were reported, and statistical significance was set at p <0.05. Prior to multivariable analysis, multicollinearity among independent variables was assessed using variance inflation factors (VIF), with values less than 10 indicating no significant multicollinearity. Model fitness was evaluated using the Hosmer–Lemeshow goodness-of-fit test. Model stability was further assessed by examining the distribution of observations across all categorical variables to identify potential sparse cell counts. All categories included in the regression analysis had sufficient observations to support stable estimation. Additionally, the events-per-variable ratio was considered adequate for the number of predictors included in the multivariable model, reducing the likelihood of model overfitting. All regression outputs were cross-checked to ensure internal consistency between odds ratios and confidence intervals. Data were assessed for completeness prior to analysis. Records with missing key variables were excluded from the final analysis. The proportion of missing data was minimal and did not significantly affect the study findings.
Results
Sociodemographic Characteristics of Diabetic Type II Patients
Table 1 summarizes the sociodemographic characteristics of the 385 participants with type II diabetes stratified by self-management status. Overall, the distribution of age, sex, education level, marital status, employment status, income level, and place of residence appeared broadly comparable between participants with poor and good self-management. The largest proportion of participants were aged 30–39 years (21.3%), followed by those aged ≥60 years (19.0%). Females constituted slightly less than half of the study population (49.9%), with a relatively similar gender distribution across self-management categories. Educational attainment was relatively evenly distributed, with approximately one quarter of participants having no formal education (27.5%) or tertiary education (26.2%). Marital status and employment categories were also proportionally distributed across groups. Most participants reported earning below 1,000,000 UGX per month, and 54.0% resided in rural areas. In this chi-square test, no statistically significant associations were observed between sociodemographic variables and self-management status (all p-values > 0.05). However, these analyses reflect unadjusted comparisons and do not account for potential confounding or category-specific effects, which were further explored using logistic regression.
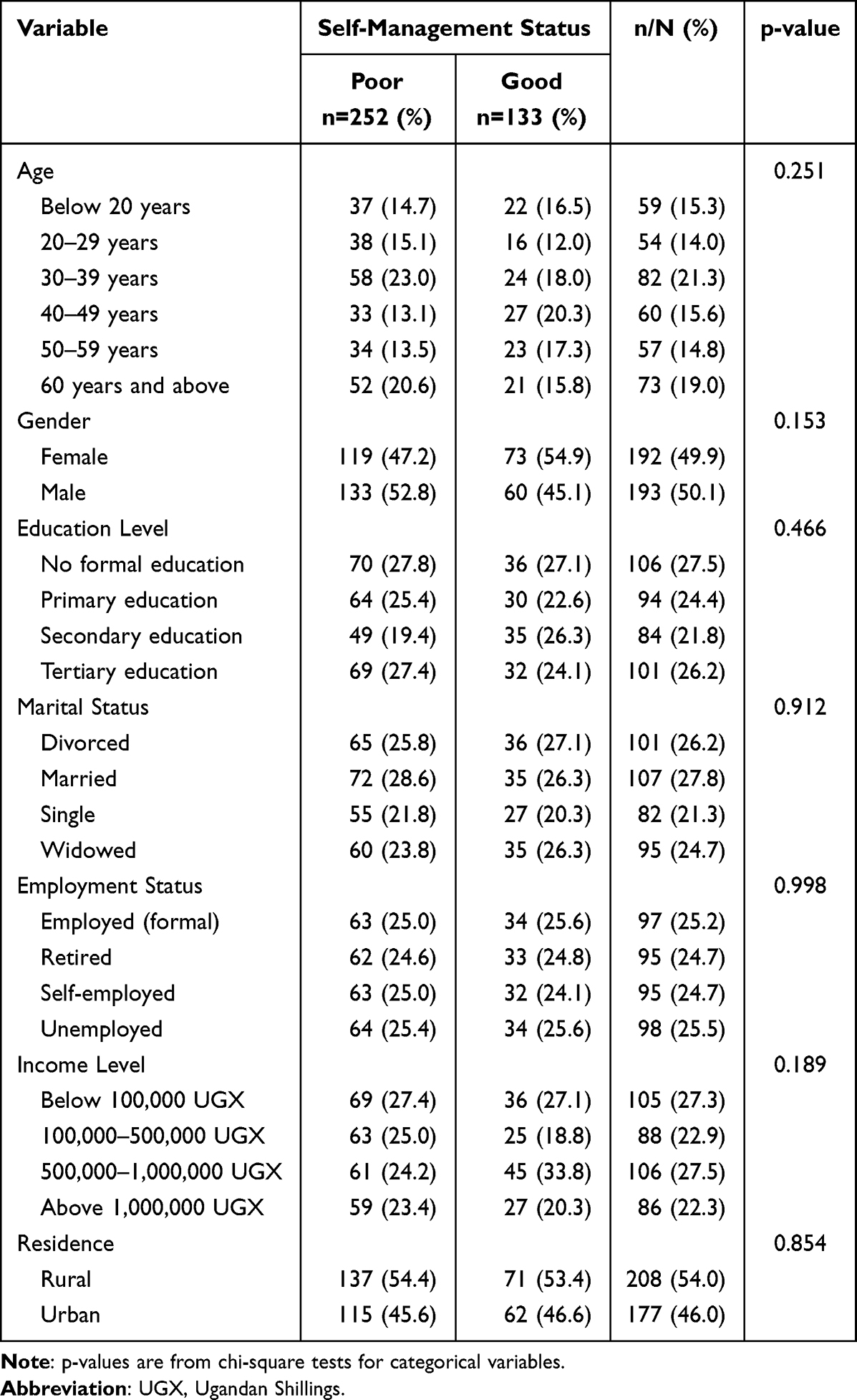 |
Table 1 Showing the Sociodemographic Characteristics of Diabetic Type II Patients |
Prevalence of Self-Management Practices Among Patients with Type II Diabetes
The findings of this study reveal that self-management practices among patients with Type II diabetes were generally suboptimal. Only 34.6% (133/385) of the participants demonstrated good self-management practices, while, 65.4% (252/385), exhibited poor self-management. This suggests that nearly two-thirds of the study population were not adequately engaging in recommended diabetes self-care behaviors.
Description of Clinical and Behavioral Factors Among Diabetic Type II Patients
Table 2 presents the clinical and behavioral characteristics of participants with type II diabetes by self-management status. Several factors showed statistically significant associations with self-management status in chi-square analysis. Although diabetes duration was significantly associated with self-management (p = 0.002), the distribution across categories did not demonstrate a clear linear trend in the descriptive analysis. This suggests that the relationship may be influenced by confounding factors, which were further explored in regression analysis. The presence of comorbidities also showed a significant association with self-management (p=0.009), particularly cardiovascular diseases and hypertension. Treatment modality differed between groups (p = 0.040), with combination therapy and insulin use more common among those with good self-management, while lifestyle modification alone was more frequent among those with poor self-management. Patterns of hospital visits were also significantly associated with self-management status (p=0.030), with participants attending routine scheduled visits more frequently demonstrating better self-management compared to those who sought care only when problems occurred. Perceived access to healthcare (availability and utilization) showed a significant relationship with self-management status (p=0.014), where fair-to-good access was more commonly reported among participants with good self-management. In contrast, knowledge level, awareness of diabetes-related complications, receipt and frequency of diabetes education, medication adherence, diet adherence, and physical activity did not demonstrate statistically significant differences between the two groups (all p>0.05). Behavioral risk factors showed selective associations: Smoking status and alcohol consumption showed minimal differences in distribution between groups in the chi-square analysis, and their apparent statistical significance should be interpreted with caution, as the observed proportions are nearly identical between groups, suggesting that these p-values may not reflect meaningful differences in this sample. Overall, these findings indicate that clinical history, healthcare utilization, and certain lifestyle behaviors are more consistently associated with diabetes self-management than knowledge or educational exposure.
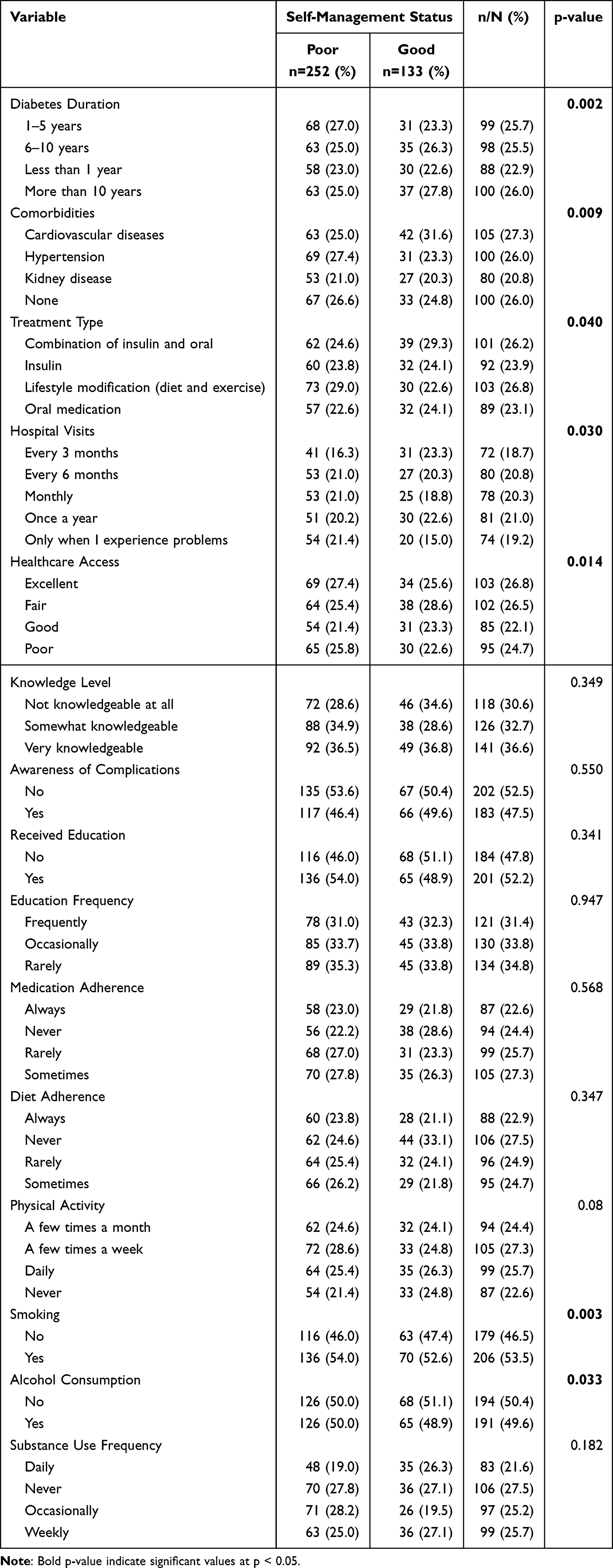 |
Table 2 Showing Description of Clinical and Behavioral Factors Among Diabetic Type II Patients |
Description of Psychological Factors Among Diabetic Type II Patients
Table 3 summarizes psychosocial factors in relation to self-management status. Several psychosocial and access-related variables demonstrated statistically significant associations in chi-square analysis. Social support was significantly associated with self-management (p=0.006), with participants reporting the presence of social support more likely to demonstrate good self-management. Similarly, the level of family support showed a significant relationship with self-management status (p=0.010), where very supportive family environments were more common among those with good self-management. Health-seeking behavior demonstrated a strong association with self-management status (p<0.001). Participants who reported regular or timely health-seeking practices were more frequently observed in the good self-management group, whereas those who never sought care or did so only when symptomatic were more likely to have poor self-management. Perceived importance of self-management was also significantly related to self-management status (p=0.003), indicating that individuals who considered self-management to be very important were more likely to practice better self-management behaviors. Perceived healthcare accessibility (ease or difficulty in obtaining care) showed a significant association with self-management (p<0.001), with easier access reported more often among participants with good self-management. Medication availability was likewise significantly associated with self-management status (p=0.002). Access to healthy food demonstrated a significant relationship with self-management (p=0.012), highlighting the role of environmental and structural factors. In contrast, stress levels and access to self-management tools did not differ significantly between participants with poor and good self-management (p>0.05). Overall, these findings emphasize the importance of psychosocial support, health-seeking behaviors, and access-related factors in influencing diabetes self-management.
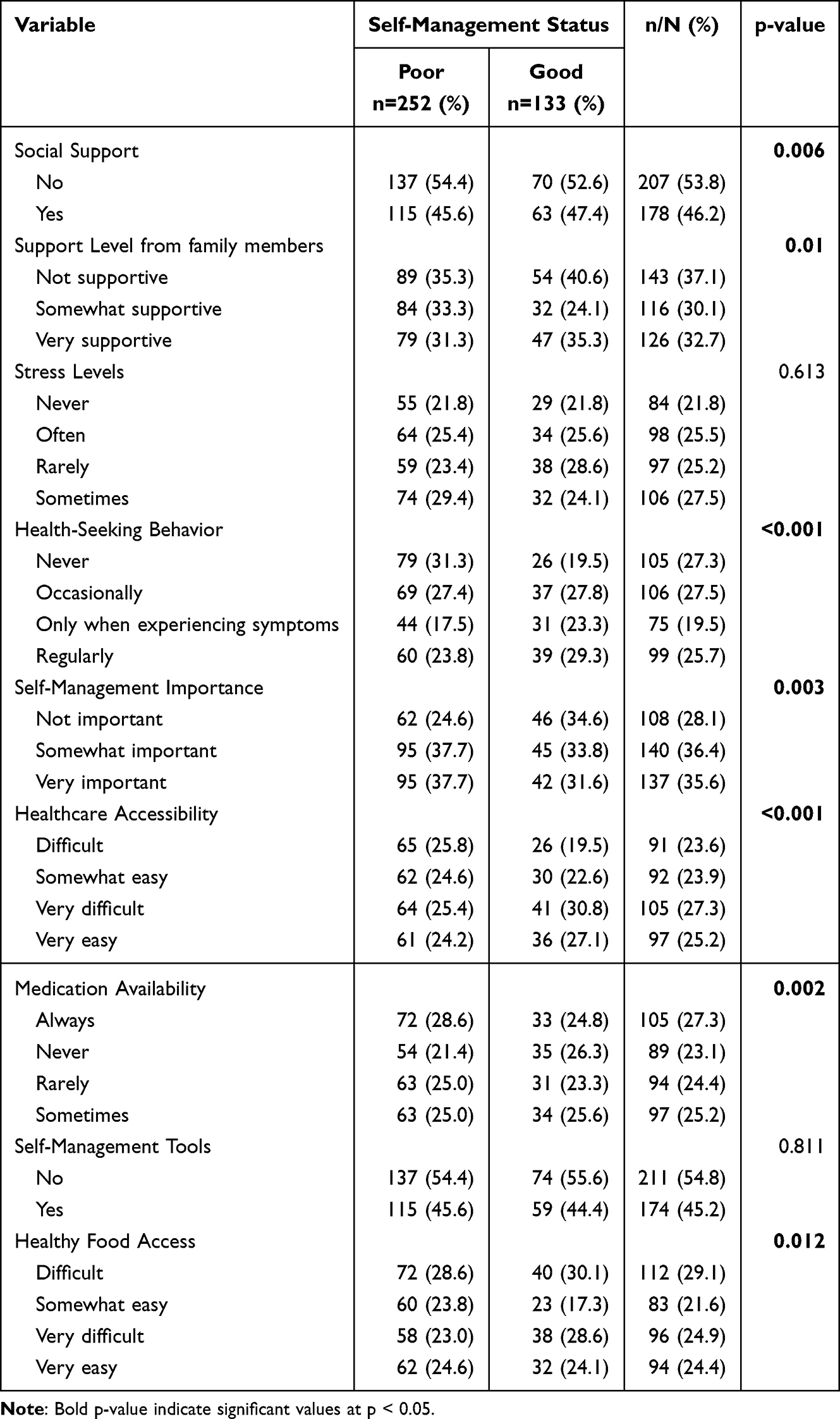 |
Table 3 Showing Description of Psychological Factors Among Diabetic Type II Patients |
Factors Associated with Good Self-Management Practices Among Type II Diabetic Patients
Table 4 presents the bivariate and multivariable logistic regression analyses of factors associated with good self-management practices among patients with type II diabetes.
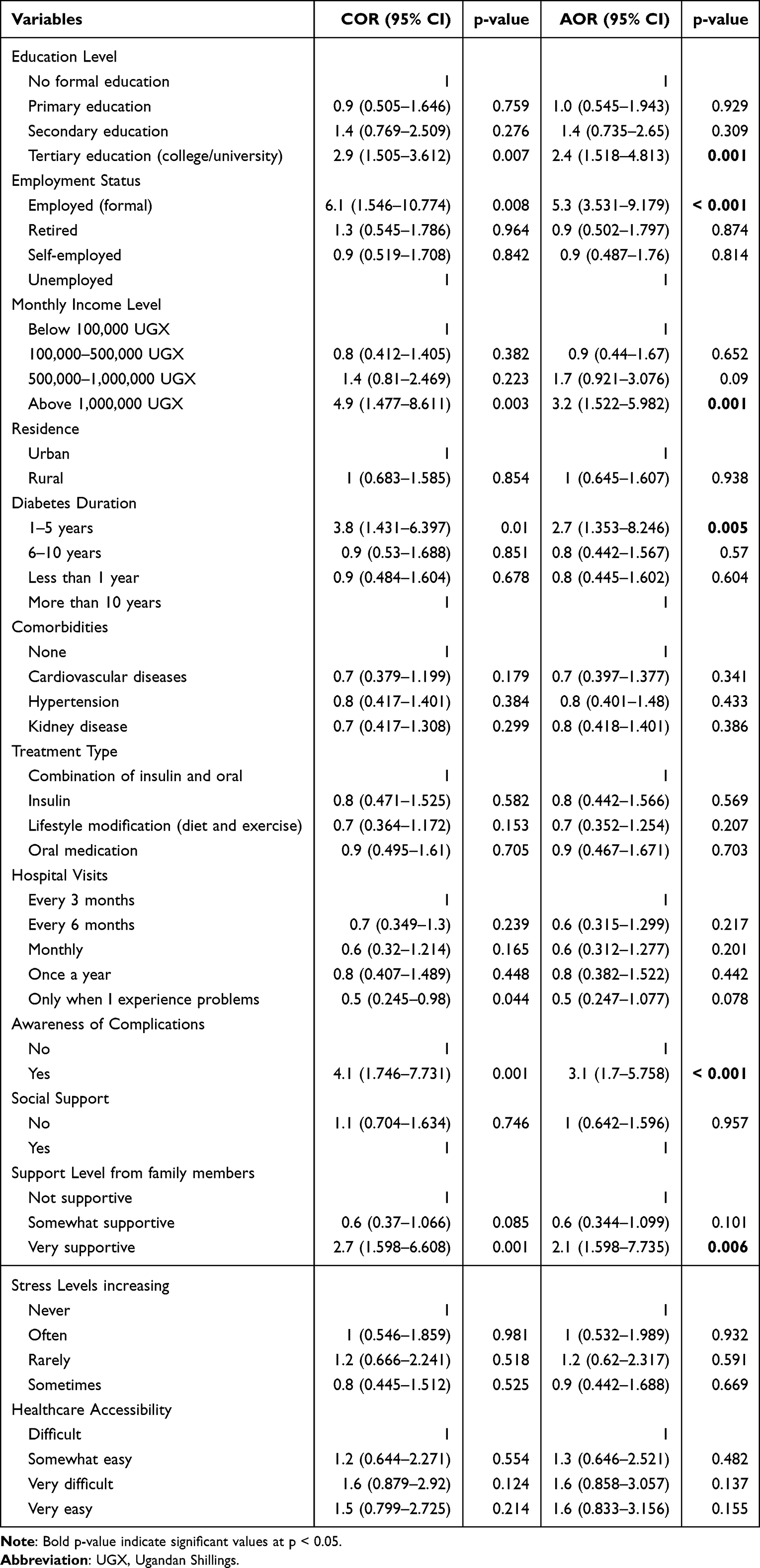 |
Table 4 Showing Factors Associated with Good Self-Management Practices Among Type II Diabetic Patients |
While chi-square analyses (Tables 1–3) provide unadjusted comparisons across groups, logistic regression allows for estimation of crude and adjusted odds ratios while accounting for potential confounding and evaluating category-specific effects relative to reference groups. Therefore, variables not statistically significant in chi-square analysis may still emerge as significant predictors in regression models.
After adjustment for potential confounders, higher educational attainment was a significant predictor of good self-management. Patients with tertiary education were more than twice as likely to demonstrate good self-management compared to those with no formal education (AOR = 2.4, 95% CI: 1.518–4.813; p=0.001). Formal employment was also significantly associated with good self-management (AOR = 5.3, 95% CI: 3.531–9.179; p=0.020), as was higher monthly income, particularly earnings above 1,000,000 UGX (AOR = 3.2, 95% CI: 1.522–5.982; p=0.001). Clinical factors showed mixed associations. Although the descriptive analysis (Table 2) did not demonstrate a clear directional trend across diabetes duration categories, multivariable regression revealed that participants with a duration of 1–5 years had significantly higher odds of good self-management compared to those with longer disease duration. This difference may reflect the effect of confounding variables not accounted for in unadjusted analyses. Awareness of diabetes-related complications remained an independent predictor of good self-management (AOR = 3.1, 95% CI: 1.7–5.758; p=0.041). Additionally, strong family support was significantly associated with better self-management practices; patients reporting very supportive family members were more likely to have good self-management compared to those with no support (AOR = 2.1, 95% CI: 1.598–7.735; p=0.006). In contrast, residence, presence of comorbidities, treatment type, hospital visit frequency, social support overall, stress levels, and healthcare accessibility were not significantly associated with good self-management after adjustment (p>0.05). These findings suggest an important role of socioeconomic factors, disease experience, knowledge, and family support in influencing diabetes self-management behaviors. The emergence of significant associations for education, employment, and income in the regression analysis, despite non-significant chi-square results, may reflect the effect of confounding, as well as the ability of regression models to estimate category-specific effects relative to a reference groups. Overall, the identified predictors are consistent with established models of chronic disease self-management, where socioeconomic capacity, disease-related knowledge, and family support interact to influence patient behavior.
Discussion
Prevalence of Self-Management Practices Among Patients with Type II Diabetes
This study found that self-management practices among patients with Type II diabetes attending Mbale Regional Referral Hospital were generally low. Only about one-third of participants (34.6%) demonstrated good self-management practices, while nearly two-thirds (65.4%) exhibited poor self-management. This finding indicates a substantial gap in adherence to recommended diabetes self-care behaviors, including medication adherence, dietary control, physical activity, and regular health monitoring. Comparable studies in sub-Saharan Africa similarly report suboptimal diabetes self-management. For instance, a study in the central zone of Tigray, Ethiopia found that only 37.3% of patients had good diabetes self-care practice, aligning closely with our findings.17 A systematic review of self-care among diabetic patients in Ethiopia noted that overall good self-care practice varied widely but remained low in many settings, with a pooled estimate of about 49% across multiple studies.18 Moreover, a study in Northwest Ethiopia reported that only 28.4% of patients demonstrated desirable self-care behaviors.19 Research from Ghana also highlights sub-optimal self-care, particularly in areas such as self-monitoring of blood glucose and foot care.20 The similarity between our results and those from other African settings may be driven by shared challenges in low-resource settings. However, these comparisons should be interpreted with caution, as different studies have used varying measurement tools for self-management, such as the Summary of Diabetes Self-Care Activities (SDSCA) and other composite indices, whereas the present study utilized the Diabetes Self-Management Questionnaire (DSMQ). Differences in instrument structure, scoring systems, and domains assessed may limit direct comparability of prevalence estimates across studies. Despite these methodological differences, the overall pattern across studies suggests that suboptimal diabetes self-management remains a persistent challenge in low- and middle-income settings. Many patients in SSA face barriers such as limited access to diabetes education and monitoring tools, financial constraints, low health literacy, and competing socioeconomic priorities, all of which impede consistent engagement in self-management behaviors.21 Although some studies report higher rates of good self-care in specific domains or settings, such as dietary practices in certain regions, the overall picture remains that many patients do not meet recommended self-management standards.22 In contrast, research from high-income countries generally shows higher levels of self-management adherence, likely reflecting better patient education, more robust healthcare infrastructure, and greater access to self-monitoring tools. In Uganda and similar low-resource settings, barriers such as limited access to diabetes educators, high out-of-pocket healthcare costs, inconsistent follow-up, and competing socioeconomic priorities may negatively affect patients’ ability to engage in sustained self-management. The low prevalence observed in this study underscores the urgent need for context-specific interventions aimed at strengthening diabetes education, follow-up care, and patient empowerment at regional referral hospitals.
Factors Associated with Good Self-Management Practices Among Type II Diabetic Patients
Educational Attainment
This study demonstrated that higher educational attainment was independently associated with good self-management practices. Patients with tertiary education were more than twice as likely to practice good self-management compared to those with no formal education. This finding suggests that education enhances health literacy, enabling patients to better understand diabetes management instructions, recognize the importance of lifestyle modification, and adhere to treatment regimens. Similar associations have been reported in Ethiopia,23,24 where higher education was linked to improved self-care behaviors and glycemic control. In addition, systematic reviews also support the importance of education interventions in enhancing self-management and glycemic outcomes, demonstrating that structured diabetes education significantly improves patients’ ability to engage in self-care and control blood glucose.25 However, the strength of this association may differ across contexts: in settings with limited access to formal diabetes education or follow-up support, even those with higher general education may not achieve better self-management. The observed association suggests that educational attainment is a key facilitator of effective self-care, and interventions that improve health literacy and provide tailored education could help bridge gaps among patients with lower formal education.
Employment Status
Formally employed participants were significantly more likely to demonstrate good self-management compared to unemployed individuals. Formal employment may confer financial stability, access to health insurance, and the ability to afford medications, nutritious foods, and transportation to healthcare facilities.
Recent evidence supports the influence of socioeconomic factors like employment and income on diabetes self-care behaviors. For example, studies examining socioeconomic determinants of diabetes care have indicated that employment and income status are linked to patterns of health behavior and care engagement in people with diabetes, including exercise habits and healthcare utilization.26 Research from Japan demonstrates that individuals in full-time work were more likely to report good self-rated health and engage in better health behaviors compared to those without work time, suggesting a positive association between employment and aspects of diabetes care behaviors.26 Additionally, work environment factors such as supportive workplace culture have been shown to influence diabetes self-management behaviors, including glucose monitoring and lifestyle adherence, underscoring the role of the work setting in shaping self-care.27 Conversely, some research suggests that the relationship between employment and diabetes self-care may be complex and mediated by factors such as job stress, work schedules, and glycemic control.28 Taken together, these findings indicate that formal employment may facilitate better self-management through multiple pathways, including economic resources and structured routines. However, job quality, workplace support, and work-life balance also appear to interact with self-care practices. This highlights the need for workplace health promotion and policies that support diabetes self-management, particularly for unemployed or informally employed individuals who may face greater barriers to effective diabetes care.
Monthly Income
Higher income was a strong predictor of good self-management, with patients earning above 1,000,000 UGX being significantly more likely to adhere to self-care practices. Adequate income enables patients to purchase medications, maintain recommended diets, engage in physical activity, and attend regular clinic visits. Studies from low- and middle-income settings similarly report that economic constraints hinder self-management; for example, qualitative research across sub-Saharan Africa highlights that low-income limits access to medications, nutritious diets, and monitoring, impeding self-care behaviors.29 However, not all studies find a direct income–self-management link; research in South Africa found that household income was not a primary determinant of adherence, possibly because extreme socioeconomic disadvantage was pervasive, making income differences less pronounced.30 The observed association in our study underscores the importance of financial capacity in enabling patients to engage in sustained diabetes self-care, suggesting that social protection and subsidized care could reduce income-related disparities in outcomes.
Duration of Diabetes
In this study, participants with a shorter duration of diabetes (1–5 years) were more likely to demonstrate good self-management compared to those with longer disease duration (>10 years). This suggests that individuals earlier in the disease trajectory may be more motivated, more recently exposed to diabetes education, and more engaged with care recommendations.
This finding is consistent with studies reporting that shorter disease duration is associated with better adherence to self-care behaviors, possibly due to higher motivation and closer clinical follow-up after diagnosis.31 However, contrasting evidence exists, with some studies suggesting that longer duration may improve certain self-care domains due to accumulated experience.32 The observed pattern in this study may reflect declining adherence over time, possibly due to treatment fatigue, reduced follow-up intensity, or competing life demands among long-term patients. This underscores the need for continuous reinforcement of self-management education and support throughout the disease course, particularly for patients with long-standing diabetes.
Non-Significant Behavioral and Knowledge Factors
In this study, several variables commonly associated with diabetes self-management, including general diabetes knowledge, medication adherence, dietary practices, and physical activity, were not independently associated with self-management after adjustment. This finding may appear unexpected given existing literature; however, several explanations are plausible. First, self-reported measures of behaviors such as medication adherence and diet may be subject to recall and social desirability bias, potentially reducing variability and attenuating associations. Second, these behaviors are often interrelated and may be mediated by broader socioeconomic and psychosocial factors such as income, education, and family support, which remained significant in the adjusted model. Third, general knowledge alone may not be sufficient to drive behavior change unless it is accompanied by perceived risk, motivation, and enabling resources. These findings highlight the complex and multifactorial nature of diabetes self-management and suggest that structural and psychosocial determinants may play a more dominant role than individual-level knowledge or reported behaviors in this setting.
Awareness of Diabetes Complications
Awareness of diabetes-related complications was independently associated with better self-management, whereas general diabetes knowledge (as assessed in descriptive analysis) was not significantly associated with self-management status. These findings suggest that awareness of potential complications may be a more behaviorally actionable construct than general knowledge alone. Patients who were aware of potential complications such as retinopathy, nephropathy, and neuropathy may be more motivated to engage in preventive behaviors due to perceived risk and severity. This aligns with evidence from Kenya33 and other sub-Saharan African settings, where awareness of complications has been shown to influence adherence to self-care practices.34 In contrast, general knowledge of diabetes, while important, may not necessarily translate into behavior change unless it is linked to perceived personal risk. These findings highlight the importance of targeted educational interventions that emphasize complication awareness, rather than relying solely on general diabetes education, as a strategy to improve self-management behaviors.
Family Support
Strong family support emerged as a significant predictor of good self-management. Patients who reported very supportive family environments were more likely to adhere to diabetes self-care practices. Family members can influence dietary choices, medication adherence, emotional wellbeing, and health-seeking behavior. This result is in line with research from Uganda showing that perceived social support from family is significantly associated with optimal diabetes self-management behavior among adult patients.35 Similarly, qualitative work in South Africa found that family involvement plays a key role in facilitating self-management by bolstering motivation and reinforcing healthy behaviors.36 These findings suggest that in many sub-Saharan African contexts, where formal healthcare education and resources may be limited, family support becomes particularly influential in daily self-care routines. In contrast, in some high-resource settings where structured diabetes education and professional support are more accessible, the relative impact of family support may be weaker because patients have additional avenues for guidance. The observed association underscores the potential benefit of integrating family-centered approaches into diabetes care interventions in Uganda to strengthen long-term self-management outcomes.
Overall, the findings of this study suggest that diabetes self-management is influenced by an interplay of socioeconomic capacity, disease-related awareness, and family support systems, rather than isolated behavioral factors alone. These results reinforce the importance of adopting a comprehensive, patient-centered approach that addresses both individual and structural determinants of self-management in resource-limited settings.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design limits the ability to establish causal relationships between identified factors and diabetes self-management practices. Second, self-management behaviors were assessed using self-reported measures, which may be subject to recall bias and social desirability bias, potentially leading to overestimation of adherence. Third, the study was conducted in a single regional referral hospital and included only patients attending routine clinic care, which may limit the generalizability of findings to individuals not engaged in regular healthcare services. Additionally, important clinical indicators such as glycemic control (eg, HbA1c levels), as well as detailed assessments of mental health and health literacy, were not included and may have influenced self-management behaviors. Despite these limitations, the study provides valuable context-specific evidence on the determinants of diabetes self-management in a resource-limited setting.
Conclusion
This study demonstrates a high prevalence of poor self-management practices among patients with Type II diabetes attending Mbale Regional Referral Hospital, highlighting substantial challenges in adhering to recommended self-care behaviors essential for optimal glycemic control. Good self-management was significantly associated with higher educational attainment, formal employment, higher monthly income, shorter duration of diabetes (1–5 years), awareness of diabetes-related complications, and strong family support. These findings indicate that socioeconomic factors, psychosocial support, and complication-specific awareness are closely linked with self-management behaviors in this low-resource setting. Strengthening structured diabetes education that emphasizes awareness of potential complications, promoting family-centered care, and improving access to affordable diabetes services may help enhance self-management, reduce the risk of complications, and improve quality of life among patients with Type II diabetes. It is important to note that, because the study was cross-sectional design and relied on self-reported measures, the findings demonstrate associations rather than causal relationships, and prevalence estimates may be affected by reporting bias.
Data Sharing Statement
The dataset generated and analyzed during the study are available from the first author, Mr Rogers Makonje, [email protected] on reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Uganda Heart Institute Research and Ethics Committee (Approval Number: UHI-REC 478). Written informed consent was obtained from all participants prior to enrolment. Participation was voluntary, and participants were informed of their right to withdraw at any stage without affecting their care. No personal identifiers were collected, and confidentiality of all participant information was strictly maintained. In addition, procedures as per the Helsinki Declaration were observed.
Acknowledgments
We thank all participants who participated in the study and research assistants who helped in data collection.
Author Contributions
RM: Conceptualization, Investigation, Writing–review and editing, ROO: Writing– original draft, Methodology, Writing–review and editing, SM: Writing–review and editing, Formal analysis, Data curation, NM: Formal analysis, Writing–review and editing, Supervision. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work did not receive any external funding for this study.
Disclosure
The authors declare no conflict or competing interests.
References
1. Genitsaridi I, Salpea P, Salim A, et al. of the IDF Diabetes Atlas: global, regional, and national diabetes prevalence estimates for 2024 and projections for 2050. Lancet Diabetes Endocrinol. 2026;14:149–16. doi:10.1016/S2213-8587(25)00299-2
2. Magliano DJ, Boyko EJ, Atlas D. 3. The global picture of diabetes. In: Diabetes Atlas.
3. Motala AA, Mbanya JC, Ramaiya K, Pirie FJ, Ekoru K. Type 2 diabetes mellitus in sub-Saharan Africa: challenges and opportunities. Nat Rev Endocrinol. 2022;18:219–229. doi:10.1038/s41574-021-00613-y
4. Irakoze Mukamana S. The impact of urbanization on diabetes prevalence and management in sub-Saharan Africa. Res Output J Biol Appl Sci. 2024;3:50–53.
5. Pastakia SD, Pekny CR, Manyara SM, Fischer L. Diabetes in Sub-Saharan Africa–from policy to practice to progress: targeting the existing gaps for future care for diabetes. Diabetes Metab Syndr Obes. 2017;10:247–263. doi:10.2147/DMSO.S126314
6. World Health Organization, Regional Office for Africa. Uganda Casts the Spotlight on Diabetes; Adopts Global Diabetes Targets. 2023. Available from: https://www.afro.who.int/countries/uganda/news/uganda-casts-spotlight-diabetes-adopts-global-diabetes-targets.
7. Bahendeka S, Wesonga R, Mutungi G, Muwonge J, Neema S, Guwatudde D. Prevalence and correlates of diabetes mellitus in Uganda: a population‐based national survey. Trop Med Int Health. 2016;21:405–416. doi:10.1111/tmi.12663
8. Powers MA, Bardsley JK, Cypress M, et al. Diabetes self-management education and support in adults with type 2 diabetes: a consensus report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. J Am Pharm Assoc. 2020;60:e1–e18.
9. Tusubira AK, Ssinabulya I, Kalyesubula R, et al. Self-care and healthcare seeking practices among patients with hypertension and diabetes in rural Uganda. PLOS Global Public Health. 2023;3:e0001777. doi:10.1371/journal.pgph.0001777
10. Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12:1–5. doi:10.1186/2251-6581-12-14
11. Chatterjee S, Khunti K, Davies MJ. Type 2 diabetes. Lancet. 2017;389:2239–2251. doi:10.1016/S0140-6736(17)30058-2
12. Chang H, Hawley NL, Kalyesubula R, et al. Challenges to hypertension and diabetes management in rural Uganda: a qualitative study with patients, village health team members, and health care professionals. Int J Equity Health. 2019;18:38. doi:10.1186/s12939-019-0934-1
13. Rutebemberwa E, Bagonza J, Tweheyo R. Pathways to diabetic care at hospitals in rural Eastern Uganda: a cross sectional study. BMC Health Serv Res. 2019;19:33. doi:10.1186/s12913-019-3873-z
14. Schmitt A, Gahr A, Hermanns N, Kulzer B, Huber J, Haak T. The Diabetes Self-Management Questionnaire (DSMQ): development and evaluation of an instrument to assess diabetes self-care activities associated with glycaemic control. Health Qual Life Outcomes. 2013;11:138. doi:10.1186/1477-7525-11-138
15. Kim MJ. Relationship Between Cognitive Impairment and Self-Management of Older Adults with Type 2 Diabetes. University of Illinois Chicago; 2021.
16. Mikhael EM, Hassali MA, Hussain SA. Effectiveness of diabetes self-management educational programs for type 2 diabetes mellitus patients in middle east countries: a systematic review. Diabetes Metab Syndr Obes. 2020;13:117–138. doi:10.2147/DMSO.S232958
17. Mariye T, Tasew H, Teklay G, Gerensea H, Daba W. Magnitude of diabetes self-care practice and associated factors among type two adult diabetic patients following at public Hospitals in central zone, Tigray Region, Ethiopia, 2017. BMC Res Notes. 2018;11:380. doi:10.1186/s13104-018-3489-0
18. Ketema DB, Leshargie CT, Kibret GD, et al. Level of self-care practice among diabetic patients in Ethiopia: a systematic review and meta-analysis. BMC Public Health. 2020;20:309. doi:10.1186/s12889-020-8425-2
19. Abate TW, Tareke M, Tirfie M. Self-care practices and associated factors among diabetes patients attending the outpatient department in Bahir Dar, Northwest Ethiopia. BMC Res Notes. 2018;11:800. doi:10.1186/s13104-018-3874-8
20. Mogre V, Abanga ZO, Tzelepis F, Johnson NA, Paul C. Adherence to and factors associated with self-care behaviours in type 2 diabetes patients in Ghana. BMC Endocr Disord. 2017;17:20. doi:10.1186/s12902-017-0169-3
21. Ageru TA, Le CN, Wattanapisit A, et al. Diabetes self-care intervention strategies and their effectiveness in Sub-Saharan Africa: a systematic review. PLoS One. 2024;19:e0305860. doi:10.1371/journal.pone.0305860
22. Muhammad EA, Shewarega ES, Baffa LD, et al. Dietary practice and associated factors among patients with type 2 diabetes mellitus in the horn of Africa: a systematic review and meta-analysis. BMC Nutr. 2025;11:81. doi:10.1186/s40795-025-01064-8
23. Berhe KK, Demissie A, Kahsay AB, Gebru HB. Diabetes self care practices and associated factors among type 2 diabetic patients in Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia-a cross sectional study. Int J Pharm Sci Res. 2012;3:4219.
24. Gurmu Y, Gela D, Aga F. Factors associated with self-care practice among adult diabetes patients in West Shoa Zone, Oromia Regional State, Ethiopia. BMC Health Serv Res. 2018;18:732. doi:10.1186/s12913-018-3448-4
25. Shiferaw WS, Akalu TY, Desta M, Kassie AM, Petrucka PM, Aynalem YA. Effect of educational interventions on knowledge of the disease and glycaemic control in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2021;11:e049806. doi:10.1136/bmjopen-2021-049806
26. Yamaoka T, Sugiyama T, Ihana‐Sugiyama N, et al. Associations between income/employment status and diabetes care processes, health behaviors, and health outcomes in Japan: a cross‐sectional study using claims data linked to a questionnaire survey. J Diabetes Invest. 2024;15:1684–1695. doi:10.1111/jdi.14301
27. Li J, Luo D, Zhang N, Guo H, Shi Y, Duan Z. Workplace culture of health and self-management behaviours among employees with type 2 diabetes: a cross-sectional moderated mediation study in urban China. BMJ open. 2025;15:e100263. doi:10.1136/bmjopen-2025-100263
28. Lin MH, Ou HY, Wang RH, Lin CH, Liao HY, Chen HM. Glycaemic control mediates the relationships of employment status and self‐stigma with self‐care behaviours in young adults with type 2 diabetes. J Clin Nurs. 2022;31:582–591. doi:10.1111/jocn.15915
29. Desse TA, Namara KM, Manias E. Patient-perceived challenges to type 2 diabetes self-management in sub-Saharan Africa: a qualitative exploratory study. Sci Diabetes Self Manag Care. 2024;50:456–468. doi:10.1177/26350106241279809
30. Hellebo A, Kengne AP, Obse A, et al. Social determinants of health and diabetes self-care management in South Africa. BMC Public Health. 2024;24:2806. doi:10.1186/s12889-024-20200-w
31. Oluma A, Mosisa G, Abadiga M, Tsegaye R, Habte A, Abdissa E. Predictors of adherence to self-care behavior among patients with diabetes at public hospitals in West Ethiopia. Diabetes Metab Syndr Obes. 2020;13:3277–3288. doi:10.2147/DMSO.S266589
32. Degefa G, Wubshet K, Tesfaye S, Hirigo AT. Predictors of adherence toward specific domains of diabetic self-care among type-2 diabetes patients. Clin Med Insights. 2020;13:1179551420981909. doi:10.1177/1179551420981909
33. Mutai C. Risk Factors and Complications Associated with Diabetes Mellitus in Patients with Heart Failure: A Case-Control Study. University of Nairobi; 2022.
34. Johnson BB, Jarvis MA, Chipps JA. Self-management knowledge, attitudes and practices among persons with type 2 diabetes in Ghana. Afr J Prim Health Care Fam Med. 2025;17:4696. doi:10.4102/phcfm.v17i1.4696
35. Onyango JT, Namatovu JF, Besigye IK, Kaddumukasa M, Mbalinda SN. The relationship between perceived social support from family and diabetes self-management among patients in Uganda. Pan Afr Med J. 2022;41. doi:10.11604/pamj.2022.41.279.33723
36. Mphasha M, Mothiba T, Skaal L. Family support in the management of diabetes patients’ perspectives from Limpopo province in South Africa. BMC Public Health. 2022;22:2421. doi:10.1186/s12889-022-14903-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Drug Resistance Patterns and Trends in Patients with Suspected Drug-Resistant Tuberculosis in Dalian, China: A Retrospective Study
Pan Y, Yu Y, Lu J, Yi Y, Dou X, Zhou L
Infection and Drug Resistance 2022, 15:4137-4147
Published Date: 30 July 2022
Prevalence and Factors Associated with Hepatitis B Infection Among Outpatient Adults in South-Western Uganda
Rugaatwa Ndibarema E, Olum R, Ayebare D, Kabakyenga J
Hepatic Medicine: Evidence and Research 2022, 14:163-172
Published Date: 19 October 2022
Prevalence and Factors Associated with Alcohol Consumption Among Secondary School Students in Nekemte, Ethiopia: A Cross-Sectional Study
Shibiru T, Arulandhu A, Belete A, Etana J, Amanu W
Substance Abuse and Rehabilitation 2023, 14:35-47
Published Date: 12 May 2023
Prevalence and Associated Factors of Chronic Obstructive Pulmonary Disease Among Adults in Neno District, Malawi: A Cross-Sectional Analytical Study
Zaniku HR, Connolly E, Aron MB, Matanje BL, Ndambo MK, Talama GC, Munyaneza F, Ruderman T, Rylance J, Dullie LW, Lalitha R, Banda NPK, Muula AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:389-401
Published Date: 5 February 2024
Prevalence and Determinants of Self‑Medication Among Adult Outpatients in a Rural Health Facility in Northern Uganda: A Cross‑Sectional Study
Watuwa PP, Opito R, Okello S, Asapo RM, Baguma I, Okello J, Onap O, Ayikobua ET, Odung T, Lubogo P
Patient Preference and Adherence 2026, 20:575475
Published Date: 29 January 2026