Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Prevalence and Determinants of Obesity and Overweight Among Children and Adolescents in the Middle East and North African Countries: An Updated Systematic Review
Authors Alruwaili BF, Bayyumi DF, Alruwaili OS ![]() , Alsadun RS, Alanazi AS, Hadi A, Alruwaili NKS, Thirunavukkarasu A, Aldaghmani NF, Alrayes AA
, Alsadun RS, Alanazi AS, Hadi A, Alruwaili NKS, Thirunavukkarasu A, Aldaghmani NF, Alrayes AA
Received 19 February 2024
Accepted for publication 15 May 2024
Published 21 May 2024 Volume 2024:17 Pages 2095—2103
DOI https://doi.org/10.2147/DMSO.S458003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Bashayer Farhan Alruwaili,1 Duaa Fahad Bayyumi,1 Ohud Saud Alruwaili,1 Razan Saud Alsadun,1 Amal Sulaiman Alanazi,2 Amal Hadi,2 Nada Kareem S Alruwaili,3 Ashokkumar Thirunavukkarasu,1 Norah Farhan Aldaghmani,4 Aljawharah Abdulrahman Alrayes4
1Department of Family and Community Medicine, College of Medicine, Jouf University, Sakaka, Saudi Arabia; 2Department of Family Medicine, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 3Department of Primary Healthcare, Ministry of Health, Aljouf Health Cluster, Sakaka, Saudi Arabia; 4College of Medicine, Jouf University, Sakaka, Saudi Arabia
Correspondence: Bashayer Farhan Alruwaili, Department of Family and Community Medicine, College of Medicine, Jouf University, Aljouf, Saudi Arabia, Tel +00966 55 191 3665, Email [email protected]
Abstract: In recent years, the countries of the Middle East and North Africa (MENA) region have experienced alarming increases in the prevalence of childhood overweight and obesity. This updated systematic review sought to measure the prevalence and determinants of obesity and overweight among children and adolescents in MENA countries. A literature search for relevant observational studies published in English was conducted using PubMed, Web of Science, Google Scholar, and Saudi Digital Library. The risk of bias was evaluated using the Newcastle-Ottawa Scale. Twenty-one published articles during the past five years were included in the systematic review. Varied approaches were used to diagnose childhood overweight and obesity, including the International Obesity Taskforce (IOTF), Centre for Disease Control (CDC), World Health Organization (WHO), and Saudi Growth Pattern Curves. We found that the combined prevalence of childhood overweight and obesity in the Middle East is up to 49.4%, depending on the methods applied in their studies. Risk factors identified were age, male gender, lack of sufficient physical activity, consumption of fried food, perceived stress level, number of family members, family size, mother’s occupation, education level, family history of obesity, high energy consumption from carbohydrates, ≥ 2 hours spent on watching television on weekend days with overweight, and always eating breakfast while watching television with obesity. The results of this review indicate that the issue of childhood and adolescent overweight and obesity in the Middle East is substantial and concerning. Most of the risk factors identified are modifiable and, if given appropriate attention, could significantly reduce the burden of associated chronic complications.
Keywords: childhood obesity, screen time, adolescents, Saudi growth pattern, WHO, CDC
Introduction
Globally, public health is being challenged by the increasing prevalence of chronic non-communicable diseases (NCDs).1,2 In high-income nations, NCDs are the principal cause of morbidity and mortality.3,4 In fact, they have already overtaken the healthcare systems of populations in a large number of low- and middle-income nations owing to the adoption of unhealthy lifestyle factors such as a lack of sufficient physical activities, unhealthy dietary habits, and excessive screen time.5 NCDs are responsible for 60% of all mortalities, of which 80% occur in low- and middle-income nations.6
Obesity is regarded as the predominant risk factor for numerous NCDs.7,8 In the last few years, attention has been diverted towards its prevalence among children, and it is called childhood obesity.9,10 Childhood and adolescent obesity and overweight have become significant public health concerns worldwide, with particularly alarming trends observed in the Middle East and North African (MENA) countries.11,12 The increasing rates of obesity and overweight among children and adolescents in this region pose substantial challenges to individual health outcomes, healthcare systems, and societal well-being. Research evidence has confirmed the possible causal association of childhood obesity with metabolic syndrome,13 dyslipidemia,14 type 2 diabetes mellitus,15 hypertension,16 hepatic steatosis,17 asthma,18 early onset adulthood cardiovascular diseases,19 and even premature mortality.20
According to the World Health Organization (WHO) report, over 1 billion individuals globally are obese (39 million children, 340 million adolescents, and 650 million adults), and these figures are exponentially rising. As per WHO statistics, by 2025, about 167 million individuals (children and adults) will lose their health and well-being due to increasing overweight or obesity.21 According to estimates by the World Obesity Federation (WOF), 254 million children are expected to be obese by 2030.22 It is worth noting that there is evidence of geographical differences in the epidemiology of childhood overweight and obesity.23–25
For countries in the MENA region, only a handful of studies have been conducted to explore the growing issue of childhood overweight and obesity with diverse reference standards, posing a challenge to compare the prevalence of obesity across geographical boundaries. Childhood obesity is largely caused by poor dietary practices, including eating too many foods high in calories and too few fruits and vegetables. Traditionally, the dietary pattern in this region is characterized by dates, whole grains, fruits, vegetables, and lean meat. Nonetheless, the trend is changing toward a high intake of high-caloric junk food among children and adolescents.26–28 Nutrition information, attitudes, and practices are important factors influencing children’s dietary behaviour. Healthy eating habits depend on adequate nutrition information and adopting positive nutrition attitudes and practices.29 The existing works literature indicates the complex relationship between socioeconomic status (SES) and obesity prevalence among children as the association varies by sex, age group, and country. Typically, socioeconomic groups who have more opportunities to consume diets rich in calories (poor SES in developed nations and high SES in developing countries) are more likely to be obese compared to other groups.30–32 Another critical factor to be addressed is physical activities, which are being demonstrated to be an effective intervention for addressing childhood obesity and its associated risk factors and complications.33,34 Regular physical activities are not only critical in helping prevent obesity among children but also it is critical in treating children suffering from obesity with chronic problems.33–36 However, recent studies indicate that children in this region are not physically active to meet the recommended guidelines.33,37 Furthermore, other studies reported that instituting proper early intervention and preventive strategies can help to overcome the major public health problem.38,39 However, it is essential to know the current prevalence and factors associated with childhood and adolescent overweight and obesity. Hence, improving the research evidence by employing a more specific and rigorous systematic approach with the recently published articles in this domain is critical. Hence, the present systematic review was performed to measure the prevalence and identify determinants of childhood and adolescent obesity and overweight in the MENA countries.
Materials and Methods
PRISMA 2020 Statement
We performed this systematic review in compliance with the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 Statement.40
Eligibility Criteria
We included observational cross-sectional studies for the present systematic review. The PICO question was following population (P) included children aged between 1 and 19 years, intervention (I) was not applicable, comparison (C) was also not applicable, and the outcome (O) was the prevalence of childhood overweight and obesity. We applied specific criteria for inclusion and exclusion for all PICO components. This helped us to narrow the search strategies. Observational studies like case reports and case series, editorial articles, letter to editors, and narrative, scoping, and systematic reviews were excluded. Furthermore, we included the only published studies of English of the past five years from the countries of this region.
Databases and Search Strategy
PubMed, Saudi Digital Library, Google Scholar, and Web of Science databases were utilized to find the articles appropriate to the study objectives. We included observational studies that were published between January 01, 2018, and onwards. Only research studies that were published in the English language were included. Keywords used in combination with Boolean operators (“AND” and “OR”) were the following: “childhood obesity”, “overweight”, “children”, “prevalence”, and “Middle East”. The bibliography details of the relevant full-text research studies were also reviewed to find further pertinent studies. During the article selection process for the present systematic review, two independent investigators initially evaluated each research’s eligibility based on the inclusion and exclusion criteria mentioned above. In cases where there was disagreement or contradiction between the two researchers regarding the eligibility of an article, a third researcher was consulted to evaluate the article and reach a consensus decision.
Data Collection and Collation
From relevant full-text articles, the following pieces of information were gathered and organized in a Word file in table format: first author’s name, year of publication, country, study design, sample size, age, overweight and obesity diagnostic criteria, and frequency of overweight and obesity.
Quality Assessment
The quality of eligible studies was evaluated using the Newcastle-Ottawa Scale for cross-sectional research. The Newcastle-Ottawa Scale was originally prepared by the Universities of Newcastle, Australia, and Ottawa, Canada, and numerous studies used the scale for their relevant systematic review and metanalysis.41–43 The scale was adopted and revised for this systematic review. Newcastle-Ottawa Scale is a tool that helps evaluate the methodology of research studies so that informed judgments can be made about their accuracy and consistency. Each section in the Newcastle-Ottawa Scale is usually given a score of either one or two on the basis of methodological quality, ie, the higher the score, the better the methodological quality. For the evaluation of cross-sectional studies, we regarded a score of 1 to 3 as a sign of high, 4 to 5 as moderate, and 6 or above as a low risk of bias.
Results
Study Review and Selection
In this systematic review, 7283 articles were identified in the initial search. After conducting initial filtering of articles for titles and abstracts, 7192 articles were omitted, with 91 studies remained for the full-text review. The reasons for excluding the studies in the initial stages were due to duplicate records, irrelevance, non-availability of full text, and other than English publications. Finally, 21 articles were eligible for inclusion in the systematic review. The main reasons for the exclusion of 70 full-text articles were as follows: review articles, articles not from the Middle East and North Africa, age >19 years, and prevalence of childhood overweight and obesity could not be calculated. Figure 1 demonstrates the flow of study selection and inclusion.
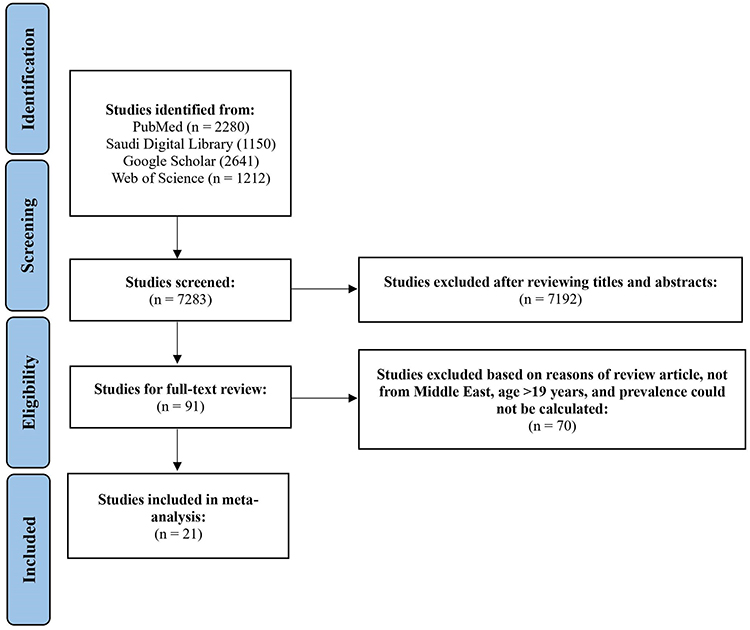 |
Figure 1 PRISMA Flowchart – Study selection process. |
Attributes of Included Studies
Twenty-one articles incorporated in the systematic review were published between the years 2018 and 2023. Four studies originated from Jordan,44–47 four from Saudi Arabia,48–51 two each from Kuwait,52,53 Palestine,54,55 UAE,56,57 Algeria,58,59 and Qatar,60,61 and one each published from Sudan,62 Egypt,63 and Iran.64 Studies enrolled children between 1 and 19 years old. All studies were cross-sectional study design. Varied approaches were used to diagnose childhood overweight and obesity, which included the International Obesity Taskforce (IOTF),50,52,54,58,59 Centre for Disease Control (CDC),46,47,55,56,63 WHO,44,45,49–51,53,57,60,61,64 and Saudi Growth Pattern Curves.48 A study by Al-Hazza et al used three approaches (IOTF, WHO, and Saudi Growth Pattern Curves) to compare and contrast the prevalence of childhood obesity and overweight (Table 1).
 |
Table 1 The Attributes of the Incorporated Articles in the Review (n=21) |
Risk of Bias Assessment
On the risk of bias evaluation of included articles with the Newcastle-Ottawa Scale, all articles had a low risk of bias (score of 7). (Please find more information in the Supplementary Table -Appendix A).
Prevalence of Childhood Overweight and Obesity
This section presents a summary of some of the crucial studies reviewed in this study. According to the present systematic review findings, the prevalence of overweight and obesity was the highest (49.4%) in the Kuwaiti adolescent population, as reported by Al-Haifi et al in 2022.52 Next to Kuwait, overweight (20.9%) and obesity (21.4%) were highly prevalent among Qatari samples. Using CDC criteria, an almost similar proportion of overweight (17.6% and 17.3%) prevalence was reported by Fraiwan et al46 and Zayed et al47 among Jordanian children and adolescents. However, the obesity prevalence was 7.8% and 15.7%, respectively. A study by Al-Hazzaa et al in 2022 among Saudi children used three different criteria (IOTF, WHO, and Saudi Growth Pattern Curves) to compare the identified prevalence of overweight and obesity. In their study, overweight prevalence explored by IOTF, WHO, and Saudi Growth Chart patterns were 18.4%, 19.1%, and 22.4%, respectively.50 The lowest prevalence of overweight and obesity was observed in Sudan,62 followed by Iran.64
Risk Factors of Childhood Overweight and Obesity
The identified determinants for overweight and obesity are summarized in this section. Al-Domi et al 2019 [sedentary activities (RR= 2.0, 95% CI = 1.1–3.6, p=0.02) and eating meal and snacks from school canteen (RR= 1.8),44 Okour et al 2019 [maternal education (p=0.004), maternal occupation (p=0.011), monthly family income (p=0.013), family history of obesity (p=0.001), and eating habits (p=0.001)],45 Al-Lahham et al 2019 [waist circumference with overweight (OR=1.38, 95% CI: 1.27–1.50), waist circumference with obesity (OR=1.79, 95% CI: 1.59–2.02), and living place with obesity (OR=3.58, 95% CI: 1.09–11.81)],55 Al-Haifi et al 2022 [gender (p<0.05)],52 Al-Thani et al 2022 [boys (OR = 1.50, 95% CI = 1.46–1.53, p<0.05) and year of education (OR=1.41, 95% CI= 1.37–1.44, p<0.05),61 Abduelkarem et al 2020 [boys (OR=2.30, 95% CI:1.17–4.50), family history of obesity (OR=2.98, 95% CI:1.09–8.11), and high energy consumption from carbohydrates (OR=1.96, 95% CI: 1.06–3.16)]56 and Ghobadi et al 2018 [≥2 hours of time spent on watching television on weekend days with overweight (OR=2.44, 95% CI: 1.03–5.70) and always eating breakfast while watching television with obesity (OR=2.70, 95% CI:1.02–7.60)].64
Discussion
To the best of our literature search, this is the first study that has assessed the epidemiological dynamics and determinants of childhood overweight and obesity, specifically for the MENA countries, in the past five years. Reportedly, a significant increase in childhood overweight and obesity has been witnessed in the Middle East, particularly in Saudi Arabia,48–50 Kuwait,52,53 and Qatar.55,60 In this systematic review, the prevalence of childhood and adolescent overweight and obesity was the highest (49.4%) in the Kuwaiti population, followed by Qatar.
Our systematic review uncovered a complex spectrum of risk factors leading to the prevalence of obesity and overweight. The detected risks present a diverse array encompassing socio-demographic, lifestyle, and behavioral factors. Among these, age emerged as a significant factor, corroborating existing literature that highlights its pivotal role in susceptibility to weight-related issues.65 Additionally, our findings underscored gender disparities, with male gender surfacing as a notable risk marker in earlier research as well.66 The influence of lifestyle choices, such as regular breakfast consumption and physical activity, was prominent in its impact on weight.67 Intriguingly, the context in which meals were consumed, particularly breakfast while watching television, demonstrated a potential correlation with obesity, signifying the potential implications of mindful eating habits.64 Conversely, a recent meta-analysis by Wang et al 2023 reported that skipping breakfast was associated with overweight and obesity in children and adolescents.68
Education levels within the family unit, encompassing both parents, were established as influential factors, shedding light on the interaction between socioeconomic status and metabolic health outcomes. Furthermore, dietary patterns, including the consumption of fried foods and low-quality diets, were consistently associated with increased risk. The intricate interconnections between family dynamics and obesity were elucidated through aspects like family size, parental obesity, and family history of obesity. Notably, the study revealed the impact of environmental factors, such as living place and income level, on weight status.55,64,67,69–71
The frequency of childhood overweight and obesity across various populations of Middle East countries revealed noteworthy patterns. Among the data analyzed, the prevalence of overweight ranged from 6.2% in Sudan62 to 24% in Kuwait.52 Some countries demonstrated higher rates of overweight but lower rates of obesity, while others displayed lower overweight rates but higher obesity prevalence. Saudi Arabia reported significantly higher rates of both childhood overweight and obesity, and this is an increasing trend in accordance with the earlier studies.69,72–74 Overall, an interesting trend appeared, demonstrating sizable variability in both overweight and obesity rates across the studied countries in the MENA countries. One plausible reason for differences in prevalence among these countries could be the utilization of diverse diagnostic criteria. Nevertheless, this systematic review underscores the diverse and dynamic nature of overweight and obesity prevalence, emphasizing the need for tailored interventions and targeted strategies to address these variations effectively.
Childhood overweight and obesity have not only physical but substantial economic impacts.75 A recently published systematic review and meta-analysis by Ling et al 2023 reported increased length of hospitalization among children with overweight and obesity and expenditures associated with healthcare services outside hospitals, outpatient clinics, medicines, and hospital stay.75 The high prevalence of overweight and obesity among young males and females has also been documented in a systematic review conducted to determine the prevalence and determinants of childhood overweight and obesity in MENA nations.76 Hence, prioritizing the development of strategies to prevent and manage this issue should be a paramount focus on the health agenda of Middle East nations. Further investigations are needed to systematically log epidemiological parameters to understand trends and plan healthcare measures accordingly.
There are a few limitations in this systematic review that need to be considered. Firstly, we only included studies that were observational in nature. Second, we omitted investigations that included children as old as 21 years within the same population. There was significant heterogeneity among the included studies. Furthermore, different criteria were used for the diagnosis of childhood overweight and obesity, such as IOTF, CDC, WHO, and Saudi Growth Pattern Curves, which might be the reason for observed heterogeneity.
Conclusion
The prevalence of childhood overweight and obesity in the MENA countries is alarming and thus necessitates a multifaceted approach. Most of the recognized risk factors are modifiable, and if proper attention is given, the burden of long-term clinical complications associated with this problem will be significantly reduced. Regular targeted health-awareness campaigns aimed at the improvement of physical activities, nutrition intake quality, and reduction of screen time among children and adolescents in this region must be conducted. In addition, cooperation among the countries of the MENA region in the aspect of evidence, best practice sharing, and coordinated efforts should further contribute to the fight against childhood obesity. Lastly, continued evaluation with exploratory prospective studies is needed in the region to understand its epidemiology in totality, as there is limited data about its prevalence and risk factors in this region.
Acknowledgments
Authors wish to thank Ayed Al-Qahtani and Sultan Al-Aqidi for their support in conceptualization.
Funding
“This work was funded by the Deanship of Graduate Studies and Scientific Research at Jouf University under grant No. (DGSSR-2023-01-02145)”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Asadi-Lari M, Ahmadi Teymourlouy A, Maleki M, Afshari M. Opportunities and challenges of global health diplomacy for prevention and control of noncommunicable diseases: a systematic review. BMC Health Serv Res. 2021;21(1):1193. doi:10.1186/s12913-021-07240-3
2. Canfell OJ, Davidson K, Woods L, et al. Precision public health for non-communicable diseases: an emerging strategic roadmap and multinational use cases. Front Public Health. 2022;10:854525. doi:10.3389/fpubh.2022.854525
3. Piovani D, Nikolopoulos GK, Bonovas S. Non-communicable diseases: the invisible epidemic. J Clin Med. 2022;11(19):5939. doi:10.3390/jcm11195939
4. Ramesh S, Kosalram K. The burden of non-communicable diseases: a scoping review focus on the context of India. J Educ Health Promot. 2023;12:41. doi:10.4103/jehp.jehp_1113_22
5. Manderson L, Risk JS. lifestyle and non-communicable diseases of poverty. Globalization Health. 2023;19(1):13. doi:10.1186/s12992-023-00914-z
6. Ndubuisi NE. Noncommunicable diseases prevention in low- and middle-income countries: an overview of Health in All Policies (HiAP). Inquiry. 2021;58:46958020927885. doi:10.1177/0046958020927885
7. Zatońska K, Psikus P, Basiak-Rasała A, et al. Obesity and chosen non-communicable diseases in PURE Poland cohort study. Int J Environ Res Public Health. 2021;18(5):2701. doi:10.3390/ijerph18052701
8. Alemi S, Nakamura K, Arab AS, et al. Prevalence, determinants, and association of overweight/obesity with non-communicable disease-related biomedical indicators: a cross-sectional study in schoolteachers in Kabul, Afghanistan. PLOS Global Public Health. 2023;3(3):e0001676. doi:10.1371/journal.pgph.0001676
9. Jebeile H, Kelly AS, O’Malley G, Baur LA. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022;10(5):351–365. doi:10.1016/s2213-8587(22)00047-x
10. Smith JD, Fu E, Kobayashi MA. Prevention and management of childhood obesity and its psychological and health comorbidities. Annu Rev Clin Psychol. 2020;16(1):351–378. doi:10.1146/annurev-clinpsy-100219-060201
11. Alhamed A, Al-Zeer A, Alsaawi F, et al. The shifting patterns of childhood obesity: insights from national school screening data. Saudi Pharm J. 2023;31(12):101862. doi:10.1016/j.jsps.2023.101862
12. Al Yazeedi B, Berry DC. Childhood overweight and obesity is increasing in gulf cooperation council countries: a review of the literature. J Transcult Nurs. 2019;30(6):603–615. doi:10.1177/1043659619829528
13. Jankowska A, Brzeziński M, Romanowicz-Sołtyszewska A, Szlagatys Sidorkiewicz A. Metabolic syndrome in obese children-clinical prevalence and risk factors. Int J Environ Res Public Health. 2021;18(3):1060. doi:10.3390/ijerph18031060
14. Brzeziński M, Metelska P, Myśliwiec M, Szlagatys-Sidorkiewicz A. Lipid disorders in children living with overweight and obesity- large cohort study from Poland. Lipids Health Dis. 2020;19(1):47. doi:10.1186/s12944-020-01218-6
15. Q-X H, Zhao L, Tong J-S, et al. The impact of obesity epidemic on type 2 diabetes in children and adolescents: a systematic review and meta-analysis. Primary Care Diabetes. 2022;16(6):736–744. doi:10.1016/j.pcd.2022.09.006
16. James BC, Venkateswaran A, A A, Premkumar B, S B. The prevalence of elevated blood pressure and its association with obesity in children aged 6–13 years in rural India: a cross-sectional study. Cureus. 2023;15(4):e37916. doi:10.7759/cureus.37916
17. Marcinkiewicz K, Horodnicka-Józwa A, Jackowski T, et al. Nonalcoholic fatty liver disease in children with obesity- observations from one clinical centre in the Western Pomerania region. Front Endo. 2022;13:992264. doi:10.3389/fendo.2022.992264
18. Stratakis N, Garcia E, Chandran A, et al. The role of childhood asthma in obesity development: a nationwide US multicohort study. Epidemiology. 2022;33(1):131–140. doi:10.1097/ede.0000000000001421
19. Chung ST, Krenek A, Magge SN. Childhood obesity and cardiovascular disease risk. Curr Atheroscler Rep. 2023;25(7):405–415. doi:10.1007/s11883-023-01111-4
20. Lindberg L, Danielsson P, Persson M, Marcus C, Hagman E. Association of childhood obesity with risk of early all-cause and cause-specific mortality: a Swedish prospective cohort study. PLoS Med. 2020;17(3):e1003078. doi:10.1371/journal.pmed.1003078
21. WHO. World Obesity Day 2022 – accelerating action to stop obesity. 2023, https://www.who.int/news/item/04-03-2022-world-obesity-day-2022-accelerating-action-to-stop-obesity#:~:text=More%20than%201%20billion%20people,they%20are%20overweight%20or%20obese.
22. WOF. Atlas of childhood obesity. Available from: https://www.worldobesity.org/nlsegmentation/global-atlas-on-childhood-obesity.
23. Dong Y, Ma Y, Dong B, et al. Geographical variation and urban-rural disparity of overweight and obesity in Chinese school-aged children between 2010 and 2014: two successive national cross-sectional surveys. BMJ Open. 2019;9(4):e025559. doi:10.1136/bmjopen-2018-025559
24. Vasiljevic I, Petkovic J. The prevalence of overweight and obesity: a measurement-based analysis of 6–9-year-old school children from Montenegro. Orig Res Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1194600.
25. Nittari G, Scuri S, Sagaro GG, Petrelli F, Grappasonni I. Epidemiology of obesity in children and adolescents. Teamwork in Healthcare. 2020;1:20.
26. El-Shaheed AA, Mahfouz NN, Moustafa RSI, Elabd MA. Alarming Eating Behaviours among Adolescents in Egypt. Open Access Maced J Med Sci. 2019;7(13):2189–2193. doi:10.3889/oamjms.2019.583
27. Nasreddine L, Shatila H, Itani L, Hwalla N, Jomaa L, Naja F. A traditional dietary pattern is associated with lower odds of overweight and obesity among preschool children in Lebanon: a cross-sectional study. Eur J Nutr. 2019;58(1):91–102. doi:10.1007/s00394-017-1574-0
28. Hwalla N, Chehade L, O’Neill LM, et al. Total usual nutrient intakes and nutritional status of united Arab emirates children (4 Years–12.9 Years): findings from the kids nutrition and health survey (KNHS) 2021. Nutrients. 2023;15(1):234. doi:10.3390/nu15010234
29. Bellew W, Bauman A, Kite J, et al. Obesity prevention in children and young people: what policy actions are needed? Public Health Res Prac. 2019;29(1). doi:10.17061/phrp2911902.
30. Zhou H, Gao L, Wu Y, et al. Association and potential mediators between socioeconomic status and childhood obesity in China: findings from a national cohort study. Global Health J. 2023;7(3):157–166. doi:10.1016/j.glohj.2023.07.001
31. Wang Y, Lim H. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int Rev Psychiatry. 2012;24(3):176–188. doi:10.3109/09540261.2012.688195
32. Williams AS, Ge B, Petroski G, Kruse RL, McElroy JA, Koopman RJ. Socioeconomic status and other factors associated with childhood obesity. J Am Board Fam Med. 2018;31(4):514–521. doi:10.3122/jabfm.2018.04.170261
33. Al-Hazzaa HM. Physical inactivity in Saudi Arabia revisited: a systematic review of inactivity prevalence and perceived barriers to active living. Int J Health Sci. 2018;12(6):50–64.
34. Headid Iii RJ, Park SY. The impacts of exercise on pediatric obesity. Clin Exp Pediatr. 2021;64(5):196–207. doi:10.3345/cep.2020.00997
35. Alalawi A, Blank L, Goyder E. School-based physical activity interventions among children and adolescents in the middle East and Arabic speaking countries: a systematic review. PLoS One. 2023;18(7):e0288135. doi:10.1371/journal.pone.0288135
36. Bülbül S. Exercise in the treatment of childhood obesity. Turk Pediatri Ars. 2020;55(1):2–10. doi:10.14744/TurkPediatriArs.2019.60430
37. Chaabane S, Chaabna K, Abraham A, Mamtani R, Cheema S. Physical activity and sedentary behaviour in the Middle East and North Africa: an overview of systematic reviews and meta-analysis. Sci Rep. 2020;10(1):9363. doi:10.1038/s41598-020-66163-x
38. Kar SS, Dube R, Kar SS. Childhood obesity-an insight into preventive strategies. Avicenna J Med. 2014;4(4):88–93. doi:10.4103/2231-0770.140653
39. Brown T, Moore TH, Hooper L, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2019;7(7):Cd001871. doi:10.1002/14651858.CD001871.pub4
40. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
41. Herzog R, Álvarez-Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Á G. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? a systematic review. BMC Public Health. 2013;13(1):154. doi:10.1186/1471-2458-13-154
42. Ribeiro CM, Beserra BTS, Silva NG, et al. Exposure to endocrine-disrupting chemicals and anthropometric measures of obesity: a systematic review and meta-analysis. BMJ Open. 2020;10(6):e033509. doi:10.1136/bmjopen-2019-033509
43. Newcastle-Ottawa Scale OHRI. Ottawa Hospital Research Institute. 2023. https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp#:~:text=The%20Newcastle%2DOttawa%20Scale%20(NOS)%20is%20an%20ongoing%20collaboration,%2C%20Australia%20and%20Ottawa%2C%20Canada.
44. Al-Domi HA, Faqih A, Jaradat Z, Al-Dalaeen A, Jaradat S, Amarneh B. Physical activity, sedentary behaviors and dietary patterns as risk factors of obesity among Jordanian schoolchildren. Diabetes Metab Syndr. 2019;13(1):189–194. doi:10.1016/j.dsx.2018.08.033
45. Okour AM, Saadeh RA, Hijazi MH, Khalaileh HEA, Alfaqih MA. Socioeconomic status, perceptions and obesity among adolescents in Jordan. Pan Afr Med J. 2019;34:148. doi:10.11604/pamj.2019.34.148.19641
46. Fraiwan M, Almomani F, Hammouri H. Body mass index and potential correlates among elementary school children in Jordan. Eat Weight Dis. 2021;26(2):629–638. doi:10.1007/s40519-020-00899-3
47. Zayed AA, Beano AM, Haddadin FI, et al. Prevalence of short stature, underweight, overweight, and obesity among school children in Jordan. BMC Public Health. 2018;16(1):1040. doi:10.1186/s12889-016-3687-4
48. AlEnazi S, AlAjlan R, AlKhalaf H, et al. Prevalence of obesity among children and adolescents in Saudi Arabia: a multicenter population-based study. Saudi j med med sci. 2023;11(1):1.
49. Albaker W, Saklawi R, Bah S, Motawei K, Futa B, Al-Hariri M. What is the current status of childhood obesity in Saudi Arabia?: evidence from 20,000 cases in the Eastern Province: a cross-sectional study. Medicine. 2022;101(27):e29800. doi:10.1097/md.0000000000029800
50. Al-Hazzaa HM, Alrasheedi AA, Alsulaimani RA, et al. Prevalence of overweight and obesity among Saudi children: a comparison of two widely used international standards and the national growth references. Front Endo. 2022;13:954755. doi:10.3389/fendo.2022.954755
51. Almaqhawi A, Alkhateeb A, AlHussain AK, Alqahtani KS, Aldrweesh AK, Aljarri SA. Prevalence and associated risk factors of childhood obesity in the eastern province of Saudi Arabia. Cureus. 2022;14(10):e30015. doi:10.7759/cureus.30015
52. Al-Haifi AR, Al-Awadhi BA, Al-Dashti YA, et al. Prevalence of overweight and obesity among Kuwaiti adolescents and the perception of body weight by parents or friends. PLoS One. 2022;17(1):e0262101. doi:10.1371/journal.pone.0262101
53. AlRodhan Y, AlAbdeen Y, Saleh E, et al. Obesity and maternal perception: a cross-sectional study of children aged 6 to 8 years in Kuwait. East Mediterr Health J. 2019;25(7):465–472. doi:10.26719/emhj.18.060
54. Salah RO, Ghandour R, Husseini A. Prevalence of overweight, obesity, and associated factors among adolescents in the occupied Palestinian territory: a cross-sectional study. Lancet. 2021;2021:
55. Al-Lahham S, Jaradat N, Altamimi M, et al. Prevalence of underweight, overweight and obesity among Palestinian school-age children and the associated risk factors: a cross sectional study. BMC Pediatr. 2019;19(1):483. doi:10.1186/s12887-019-1842-7
56. Abduelkarem AR, Sharif SI, Bankessli FG, Kamal SA, Kulhasan NM, Hamrouni AM. Obesity and its associated risk factors among school-aged children in Sharjah, UAE. PLoS One. 2020;15(6):e0234244. doi:10.1371/journal.pone.0234244
57. Almulla AA, Zoubeidi T. Association of overweight, obesity and insufficient sleep duration and related lifestyle factors among school children and adolescents. Interna J Adole Med Heal. 2022;34(2):31–40. doi:10.1515/ijamh-2021-0041
58. Benmohammed K, Valensi P, Nguyen MT, Benmohammed F, Lezzar A. Prevalence and complications of obesity and overweight among Algerian adolescents. Mediterr j Nutr Metab. 2018;11(1):11–19. doi:10.3233/MNM-17173
59. Aissaoui N. Prevalence and factors favoring overweight and obesity in Algerian child and adolescent; case of the population of Constantine/Algeria. J Bio Res Health Eco. 2020;1(3):9–19.
60. Cheema S, Abraham A, El-Nahas KG, et al. Assessment of overweight, obesity, central obesity, and type 2 diabetes among adolescents in Qatar: a cross-sectional study. Int J Environ Res Public Health. 2022;19(21):14601. doi:10.3390/ijerph192114601
61. Al-Thani MH, Khalifa SAH, Akram H, Vinodson B, Ijaz MA. The characteristics of excess body weight in the school-going students of Qatar. Apollo Med. 2022;19(2). doi:10.1371/journal.pmed.1003887
62. Hussein MD, Alonazi NA, Mohamed S. Prevalence of obesity, overweight, underweight, and stunting among school children in Argo city, Northern Sudan. Sudan J Paediatr. 2018;18(2):15–19. doi:10.24911/sjp.106-1544799078
63. El-Aty NS A, Osman SR, Ahmed ES, GadAllah MA. Overweight and obesity prevalence among upper egypt primary schools’ children using Egyptian and CDC growth charts. Appl Nurs Res. 2020;56:151346. doi:10.1016/j.apnr.2020.151346
64. Ghobadi S, Totosy de Zepetnek JO, Hemmatdar Z, et al. Association between overweight/obesity and eating habits while watching television among primary-school children in the city of Shiraz, Iran. Public Health Nutr. 2018;21(3):571–579. doi:10.1017/s1368980017003251
65. Choi MJ, Kang H, Choi J. Risk factors for obesity in five-year-old children: based on Korean National Health Insurance Service (NHIS) Data. Children. 2022;9(3):1.
66. Bekhwani AR, Khan M. Various risk factors of overweight and obesity among children aged 5–16 years. J Coll Physicians Surg Pak. 2022;32(6):763–767. doi:10.29271/jcpsp.2022.06.763
67. Hamaideh SH, Al-Khateeb RY, Al-Rawashdeh AB. Overweight and obesity and their correlates among Jordanian adolescents. J Nurs Scholarsh. 2010;42(4):387–394. doi:10.1111/j.1547-5069.2010.01367.x
68. Wang K, Niu Y, Lu Z, Duo B, Effah CY, Guan L. The effect of breakfast on childhood obesity: a systematic review and meta-analysis. Front Nutr. 2023;10:1222536. doi:10.3389/fnut.2023.1222536
69. Alwan I A, Al Fattani A, Longford N. The effect of parental socioeconomic class on children’s body mass indices. J Clini Res Pedia Endo. 2013;5(2):110. doi:10.4274/Jcrpe.898
70. Manal Ibrahim AK, Mousa Ali AH, Erika Sivarajan F. Predictors of obesity in school aged Jordanian adolescents. Interna J Nurs Prac. 2010;16(4):397–405. doi:10.1111/j.1440-172X.2010.01857.x
71. Nasreddine L, Mehio‐Sibai A, Mrayati M, Adra N, Hwalla N. Adolescent obesity in Syria: prevalence and associated factors. Child Care Health Dev. 2010;36(3):404–413. doi:10.1111/j.1365-2214.2009.01042.x
72. Alenazi SA, Koura HM, Zaki SM, Mohamed AH. Prevalence of obesity among male adolescents in Arar Saudi Arabia: future risk of cardiovascular disease. Indian J Community Med. 2015;40(3):182. doi:10.4103/0970-0218.158864
73. Al-Hazzaa HM, Al-Nakeeb Y, Duncan MJ, et al. A cross-cultural comparison of health behaviors between Saudi and British adolescents living in urban areas: gender by country analyses. Int J Environ Res Public Health. 2013;10(12):6701–6720. doi:10.3390/ijerph10126701
74. El Mouzan MI, Foster PJ, Al Herbish AS, et al. Prevalence of overweight and obesity in Saudi children and adolescents. Ann Saudi Med. 2010;30(3):203–208. doi:10.4103/0256-4947.62833
75. Ling J, Chen S, Zahry NR, Kao TA. Economic burden of childhood overweight and obesity: a systematic review and meta-analysis. Obes Rev. 2023;24(2):e13535. doi:10.1111/obr.13535
76. Farrag NS, Cheskin LJ, Farag MK. A systematic review of childhood obesity in the Middle East and North Africa (MENA) region: prevalence and risk factors meta-analysis. Adv Pediatr Res. 2017;4. doi:10.12715/apr.2017.4.8.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.