Back to Journals » Clinical Ophthalmology » Volume 20
Pretest Probability in Ophthalmology: Preserving Diagnostic Calibration While Moving Beyond Race
Authors Browning DJ ![]()
Received 11 May 2026
Accepted for publication 24 June 2026
Published 7 July 2026 Volume 2026:20 623706
DOI https://doi.org/10.2147/OPTH.S623706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
David J Browning
Department of Ophthalmology, Wake Forest University School of Medicine, Winston-Salem, NC, USA
Correspondence: David J Browning, Wake Forest University School of Medicine, 1 Medical Center Boulevard, Winston-Salem, NC, 27157, USA, Email [email protected]
Purpose: Using a Bayesian framework with emphasis on pretest probability, to evaluate the consequences of removing race-based proxies from clinical reasoning without replacing the information they encode with more precise causal predictors.
Methods: Narrative review and conceptual analysis of Bayesian diagnostic reasoning as applied to current recommendations regarding the use of race and ethnicity in medicine and ophthalmology. Examples are presented in which suppression of population-level proxies alters pretest probability estimation and diagnostic calibration. Representative conditions discussed include sarcoidosis-associated uveitis, giant cell arteritis, and hemoglobinopathy-associated vitreous hemorrhage. A review is presented of the French experience with restrictions on race and ethnicity data collection in healthcare and the ensuing problems encountered and costs incurred.
Results: Bayesian diagnostic theory predicts that test performance depends on pretest probability. Uniform diagnostic thresholds applied across populations with differing disease prevalence may increase low-yield testing in low-prevalence groups while delaying diagnosis in higher-risk populations. Race is a socially constructed category rather than a biological determinant; however, in current clinical practice it may function as a proxy for genetic susceptibility, environmental exposure, geographic ancestry, access to care, referral patterns, and diagnostic delay. Suppressing such proxies without substituting more precise causal variables may degrade diagnostic calibration. Examples from ophthalmology demonstrate how inaccurate estimation of baseline disease probability can lead to both unnecessary testing and avoidable morbidity. Eliminating population descriptors has historically forced clinicians toward less transparent and less precise surrogate markers.
Conclusion: The goal should not be preservation of race-based medicine, but preservation of accurate and equitable diagnostic calibration while transitioning toward mechanism-based predictors. More precise variables, including genetic markers, environmental exposures, and structural determinants of health, should replace imprecise proxies whenever possible. Until such replacements are routinely available, eliminating variables that contribute to estimation of disease probability risks impairing Bayesian clinical reasoning and increasing both over-testing and under-diagnosis.
Keywords: pretest probability, race, proxy, genetics, environmental exposure, ethnicity, access, disparity, Bayesian analysis, diagnostic calibration
Introduction
Pretest probability is the foundation of Bayesian clinical reasoning.1 Accurate diagnostic calibration requires clinicians to estimate the likelihood of disease before ordering a test. When variables that contribute to this estimation are removed without a replacement, the resulting informational void can shift diagnostic thresholds in ways that increase both over-testing and under-testing.
Recent recommendations from the National Academies of Sciences, Engineering, and Medicine (NASEM) call for greater scrutiny of how population descriptors, including race and ethnicity, are used in biomedical research and clinical algorithms.2 These recommendations emphasize three principles: (1) evaluate whether the use of race/ethnicity is appropriate or inappropriate in a given context; (2) increase transparency in how these data are collected and applied; and (3) replace race with more precise causal variables whenever possible.2–4
Proponents of removing race from clinical algorithms offer several reasons for their perspective. They contend that continued use of racial categories, even as provisional proxies, risks treating socially constructed categories as if they directly reflected biological differences, may incorporate historical inequities present in prevalence data into prospective clinical decisions, and could perpetuate patterns of differential care rather than correct them.3 Under this view, precaution favors removal of race as a variable pending development and validation of more precise alternatives, accepting that some uncertainty may accompany the transition until such replacement variables become routinely available. We present a complementary perspective not to dismiss the prevailing one, but to sharpen the central question: not whether to move beyond race, but how and under what conditions such a transition can preserve diagnostic accuracy and equity.
Race is a socially constructed category, not a biological determinant.3 Yet in current clinical practice, race often functions as an imperfect proxy for a heterogeneous set of causal mechanisms: genetic variants, environmental exposures, structural inequities, geographic clustering, referral patterns, and diagnostic delay.2 When the proxy is removed without substituting the underlying causal factors, clinicians may be forced to revert to population-average assumptions that obscure clinically relevant variation in baseline risk.3
The practical goal is to preserve accurate estimation of disease probability while transitioning to more precise, mechanism-based predictors.
Methods
This article is a narrative review and conceptual analysis. A search of the PubMed and database was conducted using the following terms: pretest probability, Bayesian reasoning, race, ethnicity, diagnostic calibration, sarcoidosis uveitis, giant cell arteritis, sickle cell vitreous hemorrhage, hemoglobinopathy, and ophthalmology. Studies were selected for inclusion if they provided epidemiological data on disease incidence or prevalence stratified by population group, or if they addressed the clinical or policy implications of race-based versus race-free diagnostic approaches. This is not a systematic review; examples were chosen to illustrate specific, clinically relevant instances of Bayesian miscalibration, and no formal quality assessment of included literature was performed. Conclusions are therefore conceptual and inferential rather than empirical.
In the construction of the Table, incidence and prevalence estimates for each clinical scenario were derived from published epidemiological studies. The proportion of cases attributable to each demographic group was estimated from U.S. Census Bureau population projections and published prevalence ratios from the cited studies. Per-unit procedure costs were sourced from the 2024 Medicare Clinical Laboratory Fee Schedule and the Medicare Physician Fee Schedule (hemoglobin electrophoresis approximately $25; chest CT approximately $250; temporal artery biopsy approximately $1300–$1500). Annual low-yield expenditure under a uniform diagnostic threshold was calculated by multiplying estimated low-prevalence group case counts by per-test cost. No estimate of missed-diagnosis costs under the non-uniform (current practice) approach are presented because estimates of costs related to vision loss, systemic morbidity, inpatient care, and medicolegal liability depend on too many assumptions compared to estimates of direct testing costs. In addition, the status quo is considered tolerable by society, and the argument concerns costs incurred by the NASEM proposal. All values are intended to illustrate order-of-magnitude effects and are not definitive economic analyses.
The Proxy Problem: Information vs Biology
Population-level differences in disease prevalence arise from multiple pathways. Race does not uniquely identify any of these mechanisms, but in the absence of more precise predictors, it may act as an aggregate signal. For example, the increased prevalence of primary open-angle glaucoma (POAG) among individuals of African descent is not caused by race, but reflects contributions from genetic variants (eg, APOL1, SIX1/SIX6), environmental exposures, and disparities in access and diagnosis.5,6 Population-level prevalence differences do not imply biological determinism at the individual level.
A distinction is that self-identified race is not the same as genetic ancestry, and clinicians rarely have access to ancestry data, genotyping, or environmental exposure metrics at the point of care.2 Thus, race functions as a provisional proxy, not a biological category, and should be replaced when more precise variables become available.2
Failure to account for elevated baseline risk may delay diagnosis in higher-risk populations, while overestimation of risk may lead to unnecessary testing in lower-risk groups.7 Both directions of error are relevant.
Pretest Probability and Diagnostic Thresholds
Diagnostic tests do not operate in a vacuum; their predictive value depends on pretest probability.1 When baseline disease probability is assumed to be uniform across populations, diagnostic thresholds may shift toward lower specificity in low-prevalence groups resulting in more low-yield testing; and toward lower sensitivity in high-prevalence groups resulting in delayed diagnosis and avoidable morbidity.7 The goal is to calibrate testing so that high-risk patients are not under-evaluated and low-risk patients are not over-evaluated.
Examples in Ophthalmology
Sarcoidosis and Granulomatous Uveitis
Sarcoidosis prevalence varies widely, from 1–2 per 100,000 in Japan and Korea to 20–35 per 100,000 among African American populations.8–12 These differences reflect a combination of genetic susceptibility, environmental exposures, and structural inequities, not race itself. When clinicians ignore race and instead assume uniform population risk, chest CT imaging may be overused in low-prevalence groups and underused in higher-risk populations.
Giant Cell Arteritis (GCA)
GCA prevalence is highest in individuals of Northern European ancestry (10–20 per 100,000 over age 50) and far lower in Japan, the Middle East, and Sub-Saharan Africa (<1–2 per 100,000).13–15 Ignoring clinically relevant variation in baseline disease probability may increase low-yield temporal artery biopsies in low-prevalence groups while risking delayed diagnosis in higher-risk populations.
Vitreous Hemorrhage and Hemoglobinopathies
Sickle hemoglobin prevalence ranges from 20–30% in Nigeria to <1% in Japan and Finland.16–18 Discounting population-level prevalence differences and adopting uniform testing thresholds may lead to unnecessary hemoglobin electrophoresis in low-prevalence groups and missed diagnoses in higher-risk populations.
Putting Replacement Variables into Practice
To move beyond race while preserving diagnostic calibration, clinicians need causal, measurable predictors. Examples include genetic markers: SIX6 for POAG and HLA-B27 for acute anterior uveitis; environmental exposures: TB exposure history and histoplasmosis-endemic residence; structural factors: access to care, diagnostic delay, and referral patterns; and geographic ancestry, such as ancestry associated with malaria-endemic areas for hemoglobinopathies. These variables are more precise than race and directly tied to mechanisms that influence disease probability. There are some ophthalmologic diagnoses in which a race-free perspective has a minimal downside, for example conditions with specific imaging signatures such as macular neovascularization diagnosed by optical coherence tomography. These are less dependent on population-level pretest probability than sarcoid uveitis, GCA, or vitreous hemorrhage.
Economic and Clinical Consequences of Threshold Shifts
Based on published incidence and prevalence ranges and U.S. population estimates, the application of uniform, race-agnostic diagnostic thresholds across populations generates systemic miscalibration (Table 1). In low-prevalence groups, this approach results in high-volume, low-yield testing, which incurs significant financial costs and exposes patients to unnecessary procedural risks and anxiety.19,20 Conversely, in high-prevalence populations, assuming a population-average baseline risk results in the systematic underestimation of pretest probability. This informational deficit leads to delayed diagnosis and preventable morbidity, as the clinical “suspicion threshold” for intervention is reached only after further disease progression.7 Both directions of error represent a failure in diagnostic calibration that diverts resources from the populations most in need of early detection and specialized care.1,7
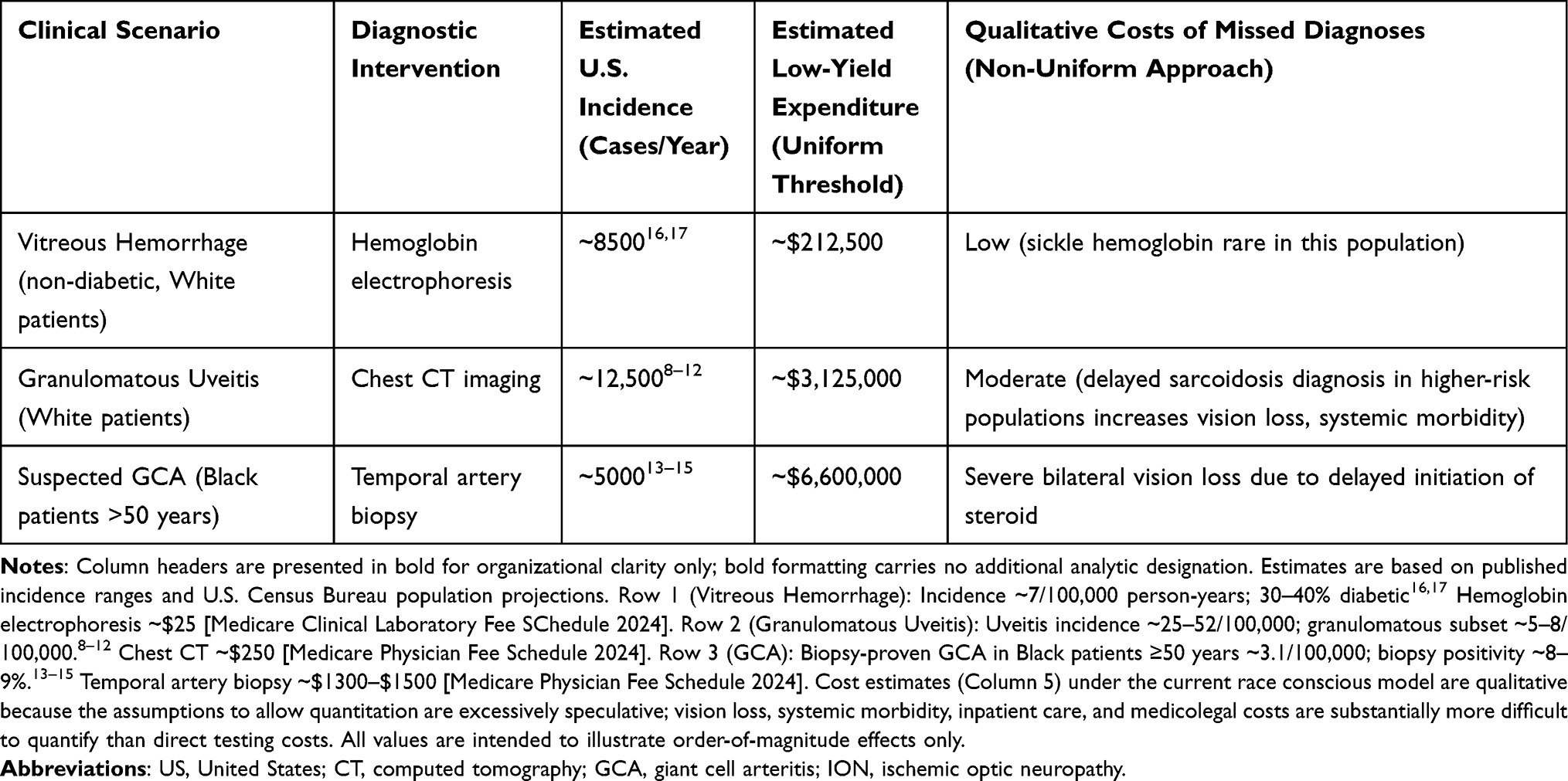 |
Table 1 Estimated Annual U.S. Impact of Uniform vs. Non-Uniform Diagnostic Thresholds in Selected Ophthalmic Scenarios |
The French Experience: Lessons from Proxy Suppression
France’s restrictive policies on the collection of ethnic and racial data in medical and administrative records highlight the clinical cost of what has been termed the “choice of ignorance”.21 In the absence of precise population-level data, clinicians are forced to rely on indirect proxies, such as country of origin or parental birthplace. These proxies are analytically imprecise and ethically fraught, often conflating geographic origin with the actual underlying drivers of disease risk.22
The evolution of newborn sickle cell screening in France illustrates this diagnostic challenge. Historically, screening was targeted based on a clinician’s perception of geographic origin, a proxy prone to significant measurement error that risked both the under-diagnosis of at-risk infants and the over-testing of others.23–25 Recognizing that these opaque signals were failing to preserve diagnostic calibration in an increasingly admixed population, France recently moved toward universal screening.23 This shift acknowledges that suppressing population-level variables without providing high-resolution replacements (such as biogeographic ancestry or genetic markers) risks systemic inequity. Policies that suppress population-level variables do not eliminate the influence of population risk; they replace transparent variables with less accurate, less accountable surrogates.26,27
The French move to universal neonatal screening, while correcting the failures of ethnicity-based targeting, has been associated with tradeoffs: an increased false-positive rate requiring follow-up testing, greater resource requirements that have been unevenly distributed across regional health systems, and heterogeneous implementation quality across metropolitan and overseas territories.23,24 Furthermore, some have observed that equity improvements in French healthcare began to emerge before formal data-restriction policies took effect, complicating causal attribution to the policy itself.22 The French case is understood not as a straightforward demonstration of the harms of race-data suppression, but as an example in which the costs of proxy suppression and the costs of proxy retention must be weighed within a clinical context.
The Argument That Race-Based Proxies Perpetuate Inequity
A counterargument to the position advanced in this article is that retaining race-based proxies risks perpetuating, rather than correcting, diagnostic inequities. This concern has precedents. Race corrections in spirometry reference equations systematically underestimated obstruction severity in Black patients, delaying their access to pulmonary care.3 Pulse oximetry overcorrected for skin pigmentation in ways that masked clinically significant hypoxemia.3 The race adjustment in estimated glomerular filtration rate (eGFR) equations delayed referral to nephrology for Black patients with chronic kidney disease.4 The proxies did not neutrally encode biological risk, but instead a history of inequitable data collection, clinical underrepresentation, and structural disadvantage, which was then propagated into prospective care decisions.
However, this history strengthens, rather than weakens, the argument for transition to validated mechanistic variables. The eGFR correction was eliminated not by removing the notion that biology influences filtration, but by replacing the race-adjusted equation with one based on cystatin C, a more precise, race-independent biomarker.4 Ophthalmology should pursue the same goal: identify which aspects of population-level risk are being captured by race, and replace them with measurable, mechanism-specific variables. The argument that race proxies perpetuate inequity is thus not an argument for accepting blurred pretest probability estimation, but for making that estimation more rigorous and less dependent on socially constructed categories.
Proponents of a race-free approach may accept some loss of efficiency but argue that the trade-off is worth it to avoid repeating past discrimination. That is a values-based position, not one that can be settled by efficiency arguments, even with guardrails. If we choose that path, we should be clear about what we are choosing to set aside.
Feasibility in Resource-Limited Settings
The practical feasibility of substituting mechanism-based predictors for race depends on context. Genetic panels, optical coherence tomography angiography-based biomarkers, environmental exposure histories, and ancestry information may be unavailable or impractically expensive to obtain in practices that serve the highest-risk populations.
Implementation should therefore be staged. Mandating race removal on a uniform timeline, without ensuring access to the replacement variables risks concentrating diagnostic inaccuracy in the settings least equipped to absorb it, an outcome that would worsen, rather than correct, inequities that motivated the reform. A transition plan should therefore stratify by clinical setting, fund access to replacement diagnostics in underserved settings, and monitor equity of outcomes.
Knowledge Gaps and Future Research Priorities
Whether the current evidence base is sufficient to support a race-free diagnostic framework in ophthalmology is unknown. The argument presented identifies a plausible and historically exemplified risk, diagnostic miscalibration from proxy suppression, but does not provide evidence of measurable harm at a population level, which would require further research.
Five types of studies would help clarify the situation. First, continued large-scale mapping of specific genetic modifiers (such as SIX1/SIX6) across diverse clinical populations would sharpen the genetic replacement part encoded by race. Second, prospective comparative studies are needed that test whether replacement of race with mechanistic alternatives preserves or improves diagnostic sensitivity and specificity in high-prevalence ophthalmic populations compared with current race-stratified approaches. Third, validation studies of candidate replacement variables (genetic markers, environmental exposure indices, structural determinants of health) are needed from diverse, real-world populations rather than academic referral centers. Fourth, low-cost screening tools appropriate for resource-limited settings need to be developed and validated before race-based proxies are retired in those contexts. Fifth, pians for prospective monitoring of diagnostic equity metrics need proofing before large scale implementation.
Conclusion
Pretest probability is central to clinical diagnosis. Removing variables that contribute to estimating disease probability without replacing the information they encode risks degrading diagnostic calibration. Race is an imprecise and socially constructed proxy, not a biological determinant, and should be replaced with more precise causal predictors as they become available.
The goal is not to preserve race-based medicine, but to preserve accurate, equitable, mechanism-informed clinical reasoning. Diagnostic thresholds should reflect true variation in disease probability, not assumptions of uniformity.
The path forward would be smoothed by prioritizing the development of validated replacement variables before retiring race. Attention to feasibility is needed in resource-limited settings, where the populations at highest risk have the least access to expensive testing. Monitoring for equity throughout the transition should be emphasized so that reform does not inadvertently widen the gaps it aims to close.
Funding
There is no funding to report.
Disclosure
Dr David Browning reports Meeting/travel support from the University of Kentucky; Stock or stock options from Zeiss Meditec, outside the submitted work.
References
1. McKay KM, Lim LL, Van Gelder RN. Rational laboratory testing in uveitis: a Bayesian analysis. Surv Ophthalmol. 2021;66:802–6. doi:10.1016/j.survophthal.2021.02.002
2. National Academies of Sciences, Engineering, and Medicine. Using Population Descriptors in Genetics and Genomics Research. Washington, DC: The National Academies Press; 2023.
3. Vyas DA, Eisenstein LG, Jones DS. Misrepresenting race - the misuse of race correction in clinical algorithms. N Engl J Med. 2020;383:874–882. doi:10.1056/NEJMms2004740
4. Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385:1737–1749. doi:10.1056/NEJMoa2102953
5. Khor CC, Do T, Jia H, et al. Genome-wide association study identifies SIX1/SIX6 as a susceptibility locus for primary open-angle glaucoma. Nat Genet. 2014;46:1121–1125.
6. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma: the Baltimore Eye Survey. JAMA. 1991;266(3):369–374. doi:10.1001/jama.1991.03470030069026
7. Pauker SG, Kassirer JP. The threshold approach to clinical decision making. New Engl J Med. 1980;302(20):1109–1117. doi:10.1056/NEJM198005153022003
8. Rybicki BA, Major M, Popovich JJ, Maliarik MJ, Iannuzzi MC. Racial differences in sarcoidosis incidence. Am J Epidemiol. 1997;145:234–241. doi:10.1093/oxfordjournals.aje.a009096
9. Baughman RP, Teirstein AS, Judson MA, et al. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001;164:1885–1889. doi:10.1164/ajrccm.164.10.2104046
10. Morimoto T, Azuma A, Abe S, et al. Epidemiology of sarcoidosis in Japan. Eur Respir J. 2008;31:372–379. doi:10.1183/09031936.00075307
11. Kim DS. Sarcoidosis in Korea: report of the second nationwide survey. Sarcoidosis Vasc Diffuse Lung Dis. 2001;18:176–180.
12. Cozier YC, Berman JS, Palmer JR, et al. Sarcoidosis in Black women in the United States: data from the Black Women’s Health Study. Chest. 2011;139:144–150. doi:10.1378/chest.10-0413
13. Petri H, Nevitt A, Sarsour K, Napalkov P, Collinson N. Incidence of giant cell arteritis and characteristics of patients. Rheumatology. 2015;54:2081–2088.
14. Kobayashi S, Yano T, Matsumoto Y, et al. Clinical and epidemiological features of giant cell arteritis in Japan. Mod Rheumatol. 2003;13:63–67.
15. Al-Rowaih A, Sailler L, Astudillo L, et al. Giant cell arteritis in the Middle East: a rare disease. Clin Rheumatol. 2010;29:1199–1203. doi:10.1007/s10067-010-1459-6
16. Piel FB, Hay SI, Gupta S, Weatherall DJ, Williams TN. Global burden of sickle cell anaemia in children under five, 2010-2050. PLoS Med. 2013;10:e1001484. doi:10.1371/journal.pmed.1001484
17. Akinyanju OO. A profile of sickle cell disease in Nigeria. Ann N Y Acad Sci. 1989;565:126–136. doi:10.1111/j.1749-6632.1989.tb24159.x
18. Colah R, Mukherjee MB, Martin S, Ghosh K. Sickle cell disease in tribal populations in India. Ind J Med Res. 2015;141:509–515. doi:10.4103/0971-5916.159492
19. Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307:1513–1516. doi:10.1001/jama.2012.362
20. Kale MS, Bishop TF, Federman AD, Keyhani S. Overuse of health care services in the United States: an understudied problem. JAMA Intern Med. 2013;173:142–148. doi:10.1001/2013.jamainternmed.1022
21. Simon P. The choice of ignorance: the debate on ethnic and racial statistics in France. French Polit Culture Soc. 2008;26:7–31. doi:10.3167/fpcs.2008.260102
22. Cheillan D, Vercherat M, Chevalier-Porst F, et al. False-positive results in neonatal screening for cystic fibrosis based on a three-stage protocol (IRT/DNA/IRT): Should we adjust the IRT cut-off to ethnic origin?. J Inherit Metab Dis. 2005;28:813–818.
23. Haute Autorite de Sante. Depistage neonatal de la drepanocytose en France. Communique de presse; 2022.
24. Daniel Y, Elion J, Allaf B, et al. Newborn screening for sickle cell disease in Europe. Int J Neonatal Screening. 2019;5(1):15.
25. Bardakdjian-Michau J, Bahuau M, Hurtrel D, et al. Neonatal screening for sickle cell disease in France. J Clin Pathol. 2009;62:31–33.
26. Gragert L, Eapen M, Williams E, et al. HLA match likelihoods for hematopoietic stem-cell grafts in the U.S. registry. NEJM. 2014;371:339–348.
27. Beaman J, Petts A. Towards a global theory of colorblindness: Comparing colorblind racial ideology in France and the United States. Sociol Compass. 2020;14:e12774.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Race, Ethnicity, and Sustained Opioid Use After Major Abdominal Surgery for Cancer
Owusu-Agyemang P, Feng L, Cata JP
Journal of Pain Research 2023, 16:3759-3774
Published Date: 7 November 2023
An Umbrella Review of Relational Enablers of Psychological Safety and Identity-Related Gaps in the Evidence: Implications for Healthcare and Organizational Settings

Gonzalez M, Chowdhury F, Kee M, MacLeod B, Skidmore B, Woodgate RL
Journal of Healthcare Leadership 2026, 18:569934
Published Date: 30 January 2026
Reporting of Race and Ethnicity in SLE Studies in High-Impact Rheumatology Journals
Eroglu I, Suter LG, Baker H
Open Access Rheumatology: Research and Reviews 2026, 18:526618
Published Date: 25 April 2026