Back to Journals » Clinical Interventions in Aging » Volume 21
Preoperative PNI-dNLR Score as Predicting Long-Term Survival in Older Adults Undergoing Radical Gastrectomy for Gastric Cancer
Authors Chen XL, Zhang XM, Lin ZX, Huang XL, Chen YZ, Lin WZ, Zheng CY, Lin W
Received 10 March 2026
Accepted for publication 27 May 2026
Published 11 June 2026 Volume 2026:21 607241
DOI https://doi.org/10.2147/CIA.S607241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Xun-Lin Chen,1,2,* Xin-Mei Zhang,1,* Zhi-Xin Lin,1,3 Xiao-Liang Huang,1,2 Yi-Zhou Chen,1,2 Wei-Zhen Lin,1,2 Chang-Yue Zheng,1,2 Wei Lin1,2
1School of Clinical Medicine, Fujian Medical University, Fuzhou, 350122, People’s Republic of China; 2Department of Gastrointestinal Surgery, Affiliated Hospital of Putian University, Putian, 351100, People’s Republic of China; 3Department of Oncology Surgery, Fuzhou Hospital of Traditional Chinese Medicine Affiliated to Fujian University of Traditional Chinese Medicine, Fuzhou, 350003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Lin, Department of Gastrointestinal Surgery, Affiliated Hospital of Putian University, Putian, 351100, People’s Republic of China, Tel +86 0594 2730373, Fax +86 0594 2293910, Email [email protected] Chang-Yue Zheng, Department of Gastrointestinal Surgery, Affiliated Hospital of Putian University, Putian, 351100, People’s Republic of China, Tel +86 0594 2730373, Email [email protected]
Objective: This study aimed to assess the prognostic value of preoperative peripheral blood-based inflammatory and nutritional indices in older adults diagnosed with gastric cancer (GC) undergoing radical gastrectomy and to develop a novel composite prognostic score.
Methods: A retrospective single-center analysis of clinicopathologic data of 609 older adults diagnosed with GC who underwent radical gastrectomy at the Affiliated Hospital of Putian University between 2012 and 2020, was conducted. Multivariate Cox regression analysis was performed to identify independent prognostic factors. A composite score, termed the PNI-dNLR, was constructed using the prognostic nutritional index (PNI) and derived neutrophil-to-lymphocyte ratio (dNLR), and its predictive performance was assessed.
Results: Multivariate Cox regression identified both preoperative PNI (hazard ration [HR], 0.74; 95% confidence interval [CI], 0.57– 0.97; p = 0.027) and dNLR (HR, 1.44; 95% CI, 1.06– 1.94; p = 0.018) as independent prognostic indicators for overall survival (OS) and disease-free survival (DFS). The PNI-dNLR score, derived from these two variables, demonstrated favorable predictive performance as assessed by the Akaike information criterion, Bayesian information criterion, time-dependent concordance index, and time-dependent receiver operating characteristic curve analysis. The PNI-dNLR remained an independent predictor of OS and DFS in multivariate Cox regression models (p < 0.05). Further validation using least absolute shrinkage and selection operator-Cox regression, random survival forest, and survival tree modeling, along with intersecting features from multivariate Cox analysis, supported the prognostic significance of the PNI-dNLR score in this population.
Conclusion: Preoperative dNLR and PNI independently predicted long-term postoperative outcomes in older adults undergoing radical gastrectomy for GC. The combined PNI-dNLR score demonstrated predictive value, which need further prospective multicenter study conducting internal and external validation to confirm before clinic application for risk stratification, personalized prognostic assessment, and treatment planning in this patient population.
Keywords: combined prediction, disease-free survival, elderly patients with gastric cancer, inflammatory indicators, nutritional indicators, overall survival
Introduction
Gastric cancer (GC) ranks fifth globally in both incidence and mortality, with approximately one million newly diagnosed cases and over 650,000 GC-related deaths reported annually.1,2 Although advancements in treatment, particularly radical gastrectomy combined with various adjuvant therapies, have contributed to improved survival rates and quality of life, the prognosis of GC remains poor due to factors such as the low rate of early-stage detection, marked biological heterogeneity, and a high propensity for distant metastasis.3 The global trend toward population aging has led to an increasing proportion of older individuals being diagnosed with malignancies, including GC, introducing significant societal, medical, and economic challenges.4 In addition to tumor-specific factors, older individuals often present with age-associated physiological decline, including multiple organ dysfunction, compromised immune response, and reduced tolerance to surgical stress, all of which contribute to variability in postoperative recovery and long-term survival outcomes. Consequently, the identification of reliable prognostic markers is essential to enhance the accuracy of long-term survival predictions and to inform individualized treatment strategies for older adults with GC.
Emerging evidence suggests that systemic inflammatory responses and malnutrition are closely associated with the prognosis of GC.5–7 Inflammatory mechanisms play a key role in oncogenesis and tumor progression, while nutritional status influences immune competence. Several preoperative inflammatory indicators derived from peripheral blood cell counts, including neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), derived neutrophil-to-lymphocyte ratio (dNLR), systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), and aggregate index of systemic inflammation (AISI), have been consistently associated with disease progression and poor prognosis in individuals with gastric malignancies.8–10 Similarly, composite indices that integrate nutritional and immune parameters, such as the geriatric nutritional risk index (GNRI) and the prognostic nutritional index (PNI), have also been identified as independent prognostic factors in patients with GC.11,12 A previous study found that the combined biomarker of dNLR and PLR was associated with the outcomes of patients with advanced GC receiving anti-PD-1 antibody treatment.13 However, no study has clearly demonstrated the predictive value of PNI or dNLR for the long-term prognosis of older adult patients with GC after surgery, and there are no related studies that have constructed a PNI-dNLR combined scoring model for predicting the prognosis of older adult patients with GC after surgery.
This study aimed to assess the prognostic value of preoperative peripheral blood-based inflammatory and nutritional indices in older adults diagnosed with GC undergoing radical gastrectomy and to develop a novel composite prognostic score.
Materials and Methods
Study Population
Clinicopathologic data from consecutive older adults diagnosed with GC who underwent radical gastrectomy at the Affiliated Hospital of Putian University between 2012 and 2020 were retrospectively reviewed. Inclusion criteria were as follows: (a) age ≥ 65 years; (b) histopathological confirmation of primary gastric adenocarcinoma; (c) absence of peritoneal or distant metastasis as confirmed by intraoperative exploration; and (d) confirmation of R0 resection, as verified by postoperative pathological assessment. Exclusion criteria included: (a) presence of other malignancies; (b) presence of hematological malignancies or autoimmune disorders; (c) severe hepatic or renal dysfunction or other comorbidities contributing to poor nutritional status; (d) severe infections or other inflammatory conditions; (e) receipt of preoperative neoadjuvant therapy; (f) diagnosis of gastric stump cancer; and (g) incomplete clinicopathologic data.
A total of 609 patients met the eligibility criteria and were included in the final study cohort. The median follow-up period were 60 months. Postoperative pathological staging was conducted based on the Eighth Edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual.14 For older adults with advanced-stage GC, adjuvant chemotherapy regimens based on 5-fluorouracil (primarily oxaliplatin + capecitabine or oxaliplatin + S-1) were recommended.15 This study was approved by the Ethics Committee of the Affiliated Hospital of Putian University and conducted in accordance with the principles outlined in the Declaration of Helsinki. Written, informed consent was obtained from all participants.
Definitions
Older adults with GC were defined as those aged 65 years or older. Age and tumor size were categorized based on their respective median values: 70 years and 50 mm, respectively. dNLR was calculated as the ratio of the absolute neutrophil number to the difference between absolute total leukocyte and absolute neutrophil counts, a proxy for lymphocyte count.16 Body mass index (BMI) was categorized into three groups according to the World Health Organization standards: < 18.5 kg/m2, 18.5–24.9 kg/m2, and > 24.9 kg/m2. Postoperative complications were classified using the Clavien-Dindo (CD) classification system, with a CD grade of ≥ II defined as indicating severe postoperative complications.17
Measurement of Nutritional and Inflammatory Indicators
Hematological and laboratory parameters were obtained within one week prior to surgery and were prospectively recorded in the GC database. These parameters included white blood cell count, neutrophil count, lymphocyte count, monocyte count, platelet count, and serum albumin level.
Formulas used to calculate specific inflammatory and nutritional indices are presented in Supplementary Table 1. Based on 5-year OS outcomes, optimal cut-off values for NLR, LMR, PLR, dNLR, SII, SIRI, AISI, GNRI, and PNI were determined using X-tile software (V3.6.1). The identified cut-off values were 1.4, 4.4, 116.8, 2.2, 401.8, 0.5, 116.7, 96.0, and 46.1, respectively.18
Postoperative Follow-Up
Follow-up assessments were conducted every three months during the first two years after surgery, and every six months from the third to the fifth post-operative year.
The follow-up evaluations included physical examinations; laboratory tests such as complete blood count, biochemical profile, carcinoembryonic antigen (CEA), alpha-fetoprotein, and carbohydrate antigen 19–9; chest radiography; abdominal and pelvic ultrasonography or computed tomography; and annual endoscopic examinations.
As of the final follow-up in December 2025, the overall follow-up rate was 95%.
Statistical Analysis
All statistical analyses were performed using R software, version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria). Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as means with standard deviations or as medians with interquartile ranges, depending on data distribution. Categorical variables were compared using the chi-squared test or Fisher’s exact test, and continuous variables were analyzed using the Mann–Whitney test and the Kruskal–Wallis test. Based on the nature of data, Spearman correlation analysis was applied to assess relationships among indicators. The prognostic performance of individual indicators and the composite PNI-dNLR score was assessed using receiver operating characteristic (ROC) curve analysis, time-dependent ROC analysis, and the concordance index (C-index). Survival outcomes were assessed using the Kaplan–Meier (K–M) method, and comparisons between groups were made using the Log rank test.
Restricted cubic spline (RCS) examined the relationship between independent variables and mortality risk. Univariable and multivariable Cox regression identified independent prognostic factors for OS and DFS, and validated the prognostic value of the PNI-dNLR score. Collinearity [tolerance (Tol), variance inflation factor (VIF)] and interactions were assessed. Model performance was evaluated using Akaike information criteria (AIC) and Bayesian information criterion (BIC) to balance accuracy and complexity.
To further examine the predictive utility of the PNI-dNLR score, the following additional analyses were performed: least absolute shrinkage and selection operator Cox regression (LASSO-Cox) regression, random survival forest (RSF) modeling, and survival tree (ST) modeling. The Schoenfeld residuals method was used to test the proportional hazards assumption of the Cox model. The p values of all variables and the overall model PH test were all greater than 0.05, satisfying the proportional hazards assumption. The VIF variance inflation factor was used to assess collinearity, and the results showed that there was no multicollinearity among the included variables and no interference from extreme outliers. The LASSO-Cox model satisfies the core assumptions of Cox regression through the Schoenfeld residuals, Box-Tidwell test, and VIF test. It then selects the optimal λ coefficient by combining the LASSO penalty function with cross-validation, compressing redundant variables and reducing the risk of model overfitting, thereby completing the optimization and construction of the model. The RSF model, as a non-parametric ensemble model, does not require the proportional hazards assumption. Instead, it ensures the generalization ability and robustness of the model through the OOB error, cross-validation and resampling integration strategies. In the analysis concerning ST modeling, through outlier handling, stratified sampling, pruning optimization, and error analysis, there was no overfitting and the results were stable All tests were two-sided, and statistical significance was defined as p < 0.05.
Results
General Clinicopathologic Features
A total of 609 patients with GC were included in this study, comprising of 459 males (75.4%) and 150 females (24.6%), with a median age of 70 years (interquartile range [IQR]: 67–74). Most patients had no documented preoperative comorbidities (n = 374; 61.4%) and presented with a BMI in the range of 18.5 to 24.9 kg/m2 (n = 453; 74.4%). Most participants were classified as American Society of Anesthesiologists (ASA) physical status grade II (n = 361; 59.3%).
Tumors were predominantly located in the proximal stomach, with the majority measuring less than 5 cm and exhibiting mixed histological differentiation. Total gastrectomy was performed in most cases (n = 488; 80.1%). Open surgical procedures were more frequently employed (n = 354; 58.1%), compared to received laparoscopic approaches (n = 255; 41.9%).
Postoperative pathological evaluation indicated that the most common pathological TNM (pTNM) classification was stage III (n = 308; 50.6%). Vascular and nerve invasion were observed in 26.9% and 23.2% of patients, respectively. Postoperative complications classified as CD grade II or higher occurred in 17.7% of the cohort. Adjuvant chemotherapy was administered to 49.4% of the cohort.
The median follow-up duration was 60 months (IQR: 24–84 months), and the 5-year OS rate was 55.5% (n = 338) (Table 1).
 |
Table 1 Baseline Characteristics |
Screening of Prognostic Predictive Indicators
Spearman correlation analysis was conducted to assess the relationships among preoperative inflammatory and nutritional composite indicators. The PNI demonstrated a moderate correlation with the GNRI, LMR, PLR (all ρ≥0.5, p < 0.05) and a fair correlation with other preoperative inflammatory indicators. A fair negative correlation was observed between PNI and dNLR (r = –0.39, p < 0.05) (Figure 1A).
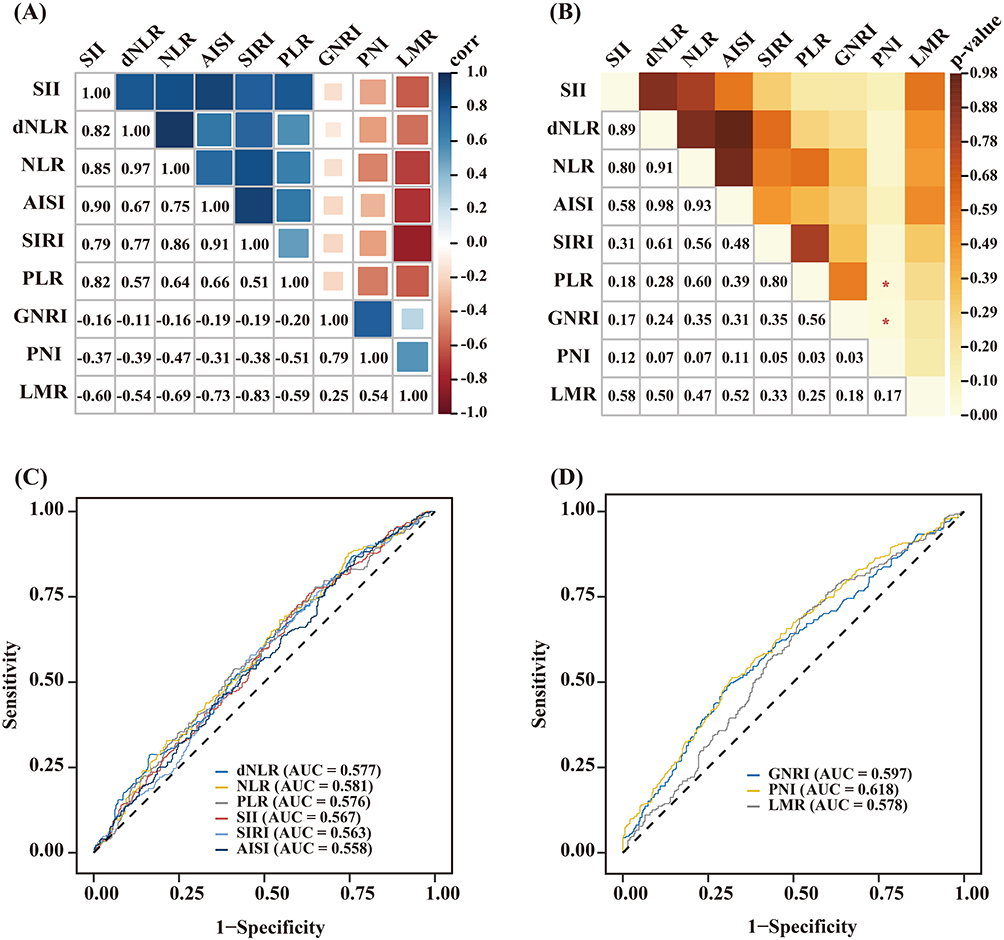 |
Figure 1 Prognostic value of inflammation and nutrition-relative indicators in older adult patients with gastric cancer. (A) Correlation coefficients between inflammation and nutrition-relative indicators in older adult patients with gastric cancer. The number in the box represents the correlation coefficient. (B) Heat map of Delong’s test for ROC curves among inflammation and nutrition-related indicators. (C and D) The receiver operating characteristic (ROC) curves of inflammation and nutrition-relative indicators for diagnosing overall survival in older adult patients with gastric cancer. Abbreviations: NLR, Neutrophil-Lymphocyte Ratio; LMR, Lymphocyte-Monocyte Ratio; PLR, Platelet- Lymphocyte Ratio; dNLR, derived NLR; SII, Systemic Immune-Inflammation Index; SIRI, Systemic Inflammation Response Index; AISI, Aggregate Index of Systemic Inflammation; GNRI, Geriatric Nutritional Risk Index; PNI, Prognostic Nutritional Index. |
ROC curve analysis was used to assess the predictive performance of preoperative inflammatory and nutritional markers for 5-year OS. PNI demonstrated the highest predictive performance (area under the curve [AUC] = 0.618) (Figure 1C and D). The DeLong test results indicated that the AUC of PNI (0.618) was significantly higher than that of PLR (AUC = 0.563, P = 0.035) and GNRI (AUC = 0.558, P = 0.028) (Figure 1B). To assess the independent predictive value of biomarkers while mitigating the effects of multicollinearity, NLR, dNLR, SII, SIRI, AISI, and PNI were jointly included in Cox regression analysis.
Univariable Cox proportional hazards regression analysis indicated that all preoperative inflammatory and nutritional composite indices were significantly associated with 5-year OS (all p < 0.05). After adjusting for clinicopathologic variables, multivariable Cox regression analysis identified only preoperative dNLR (hazard ratio [HR], 1.44; 95% confidence interval [CI], 1.06–1.94; p = 0.018) and PNI (HR, 0.74; 95% CI, 0.57–0.97; p = 0.027) as independent prognostic factors for 5-year OS (Table 2).
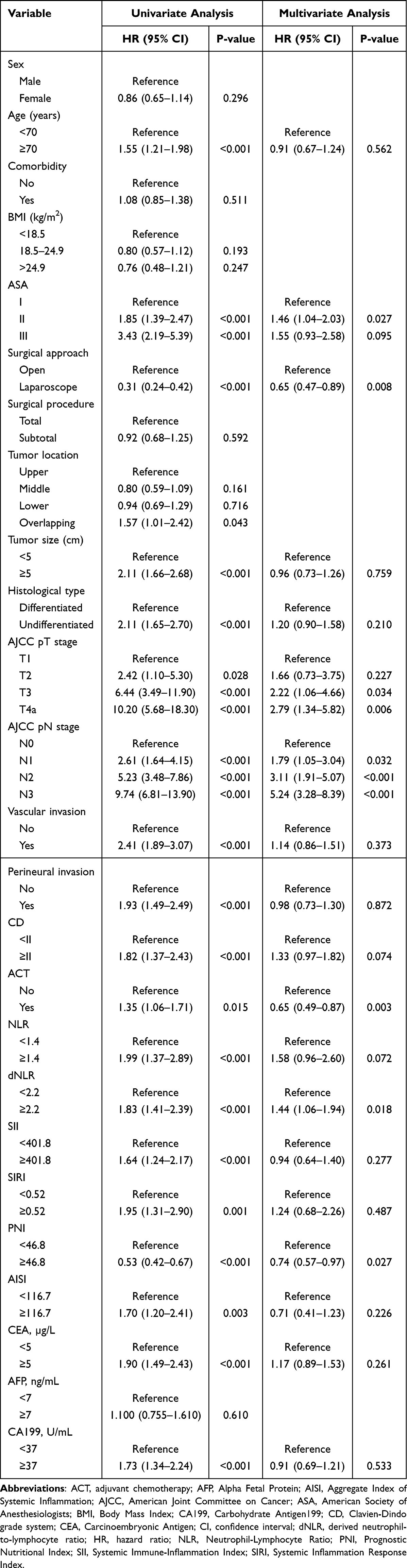 |
Table 2 Univariate and Multivariate Cox Regression Analysis of Preoperative Inflammatory and Nutritional Indicators for 5‑year Overall Survival in Elderly Patients Undergoing Curative Resection for Gastric Cancer |
Association Between PNI and dNLR and Long-Term Postoperative Survival in Older Adults with GC
Baseline characteristics stratified by PNI and dNLR groups are summarized in Supplementary Table 2. Compared with patients in the high PNI group, those in the low PNI group were older, had lower BMI, higher ASA scores, and were more likely to have undergone open surgery. The low PNI groups also demonstrated a higher prevalence of diffuse-type tumors, larger tumor size, more advanced pathological TNM (pTNM) stage, and a higher incidence of severe postoperative complications (all p < 0.05).
Patients in the high dNLR group were more frequently treated with laparoscopic surgery and exhibited larger tumor size, poorer tumor differentiation, more advanced pTNM stage, and higher rates of vascular and perineural invasion, compared to those in the low dNLR group (all p < 0.05).
RCS analysis demonstrated a negative association between PNI and the 5-year risk of death; however, the test for non-linearity was not statistically significant (χ2 = 0.78, p = 0.676; Figure 2A). In contrast, an inverse L-shaped positive association was observed between the dNLR and the 5-year risk of death, with the non-linear correlation test reaching statistical significance (χ2 = 6.56, p = 0.038; Figure 2B).
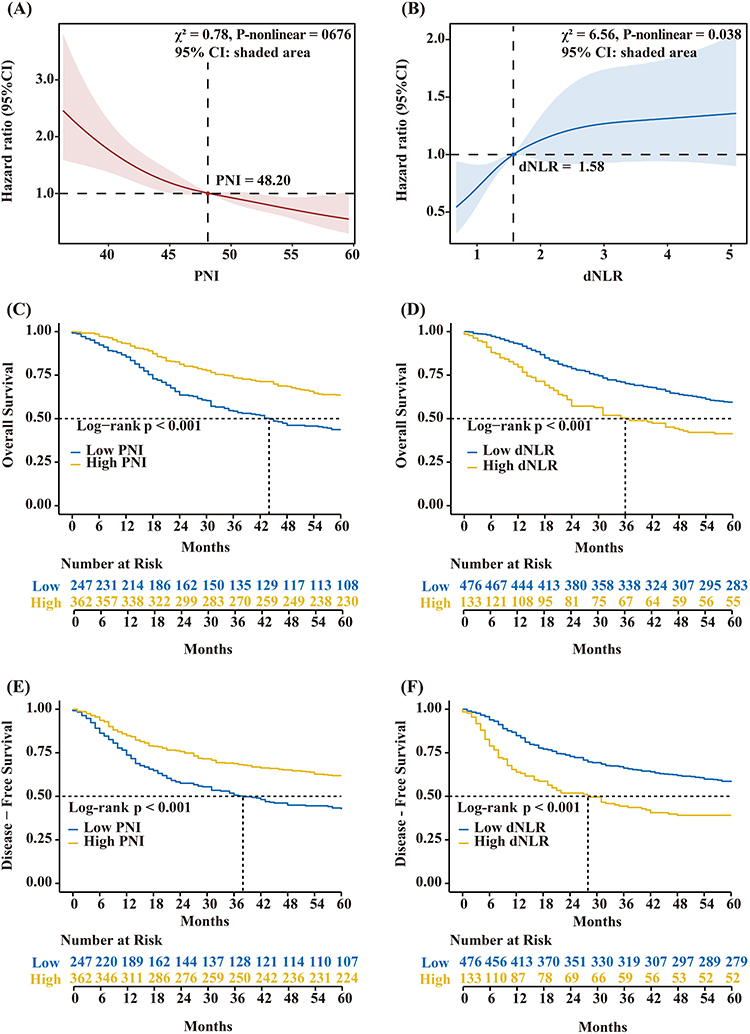 |
Figure 2 Survival analysis stratified by preoperative PNI and dNLR in older adult gastric cancer patients. Restricted cubic spline analysis of (A) PNI and (B) dNLR for overall survival. Kaplan-Meier analysis of overall survival stratified by (C) PNI and (D) dNLR. Kaplan-Meier analysis of disease-free survival stratified by (E) PNI and (F) dNLR. Abbreviations: PNI, Prognostic Nutritional Index; dNLR, derived NLR. |
K–M survival analysis indicated that the 5-year OS rate was significantly higher in the high PNI group compared to the low PNI group (63.5% vs 43.7%, p < 0.001; Figure 2C), whereas the 5-year OS rate was significantly lower in the high dNLR group compared to the low dNLR group (41.4% vs 59.5%, p < 0.001; Figure 2D).
Similarly, the 5-year DFS rate was significantly higher in the high PNI group than in the low PNI group (61.9% vs 42.5%, p < 0.001; Figure 2E), and significantly lower in the high dNLR group compared to the low dNLR group (39.1% vs 58.2%, p < 0.001; Figure 2F).
Multivariable Cox proportional hazards regression analysis indicated no significant interaction between PNI and dNLR (p for interaction = 0.645). Collinearity diagnostics indicated no evidence of multicollinearity between PNI and dNLR (tolerance = 0.870, VIF = 1.150).
Development of the PNI-dNLR Score Model
Based on the two identified prognostic factors, PNI and dNLR, patients were stratified into four subgroups: high PNI–low dNLR, high PNI–high dNLR, low PNI–low dNLR, and low PNI–high dNLR.
K–M survival analysis demonstrated that the highest 5-year OS rate was observed in the high PNI–low dNLR subgroup (65.3%), followed by the high PNI–high dNLR (48.7%) and low PNI–low dNLR (47.1%) subgroups. The lowest OS was recorded in the low PNI–high dNLR subgroup (38.3%) (p < 0.001). No statistically significant difference in OS was observed between the high PNI–high dNLR and low PNI–low dNLR subgroups (48.7% vs 47.1%, p = 0.830) (Figure 3A).
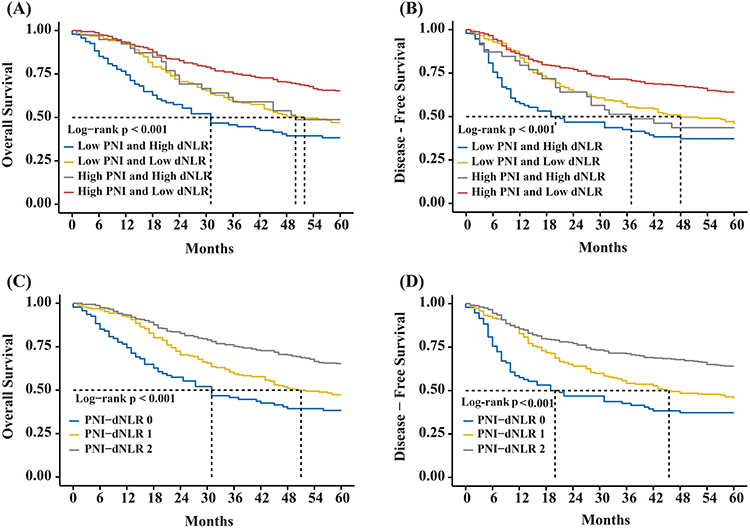 |
Figure 3 The Kaplan-Meier curves for overall survival (OS) and disease-free survival (DFS) of elder patients with gastric cancer according to the combined assessment of preoperative PNI and dNLR. (A) Kaplan‐Meier analysis for OS according to combination of preoperative PNI and dNLR. (B) Kaplan‐Meier analysis for DFS according to combination of preoperative PNI and dNLR. (C) Kaplan‐Meier analysis for OS according to PNI-dNLR score. (D) Kaplan‐Meier analysis for DFS according to PNI-dNLR score. Abbreviations: PNI, Prognostic Nutritional Index; dNLR, derived NLR. |
A similar trend was observed for 5-year DFS. The high PNI–low dNLR subgroup showed the highest DFS rate (64.1%), followed by the low PNI–low dNLR (45.8%) and high PNI–high dNLR (43.6%) subgroups, while the lowest DFS was seen in the low PNI–high dNLR subgroup (37.2%) (p < 0.001). No statistically significant difference in DFS was observed between the low PNI–low dNLR and high PNI–high dNLR subgroups (45.8% vs 43.6%, p = 0.163) (Figure 3B).
Based on these findings, the PNI-dNLR score model was constructed by grouping patients into three categories: high score group (high PNI–low dNLR), moderate score group (high PNI–high dNLR or low PNI–low dNLR), and low score group (low PNI–high dNLR).
A decrease in the PNI-dNLR score was found to be associated with older age, lower BMI, higher ASA classification, open surgical approach, diffuse tumor type, larger tumor size, more advanced pTNM stage, presence of vascular invasion, higher CD grade, and elevated CEA levels (all p < 0.05; Supplementary Table 3).
Prognostic Value of the Preoperative PNI-dNLR Score Model for Long-Term Survival
K–M survival analysis indicated significant differences in 5-year OS across the three PNI-dNLR score groups. The high score group demonstrated the highest 5-year OS rate (65.3%), followed by the moderate score group (47.4%) and the low score group (38.3%) (p < 0.001; Figure 3C).
Similarly, significant differences were observed in 5-year DFS across the three groups. The highest DFS was noted in the high score group (64.1%), followed by the moderate score group (45.3%) and the low score group (37.2%) (p < 0.001; Figure 3D).
Univariate Cox regression analysis identified multiple variables as significantly associated with 5-year OS, including age, ASA classification, surgical method, tumor size, tumor differentiation, pathological T (pT) stage, pathological N (pN) stage, vascular and perineural invasion, CD grade, administration of postoperative chemotherapy, and the PNI-dNLR score (p < 0.05 for all). In the multivariate Cox regression analysis adjusting for sex, age, comorbidity, BMI and ASA classification, PNI-dNLR score was identified as independent prognostic factors for 5-year OS, along with ASA classification (all p < 0.05; Table 3).
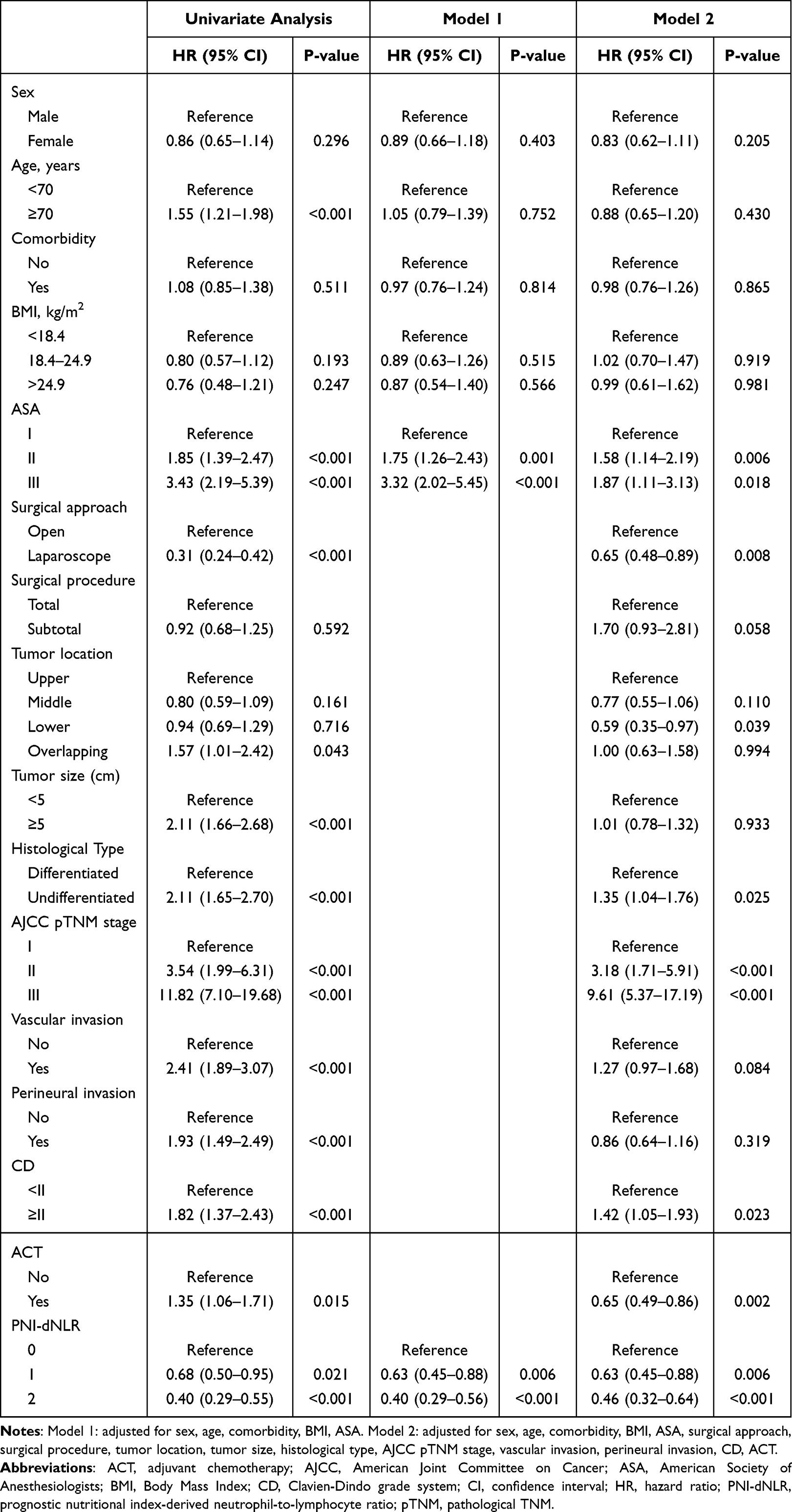 |
Table 3 Univariate and Multivariate Cox Regression Analysis of the Preoperative PNI‑dNLR Score for Overall Survival in Elderly Patients Undergoing Curative Resection for Gastric Cancer |
When the other clinicopathologic variables was included in the multivariable model, the score itself emerged as an independent predictor of 5-year OS. Other independent prognostic variables identified in model 2 included ASA classification, surgical approach, tumor’s histological type, pTNM stage, CD grade, and postoperative chemotherapy (all p < 0.05; Table 3).
For 5-year DFS, univariate Cox regression analysis identified PNI-dNLR score as significant predictors (p < 0.05). In the multivariate model that included clinicopathologic variables, the score itself remained an independent prognostic factor (all p < 0.05; Supplementary Table 4).
Evaluation of PNI-dNLR Score Model
Goodness-of-fit analysis demonstrated that the preoperative PNI-dNLR score model demonstrated superior model performance compared with the individual use of preoperative PNI and dNLR. Specifically, the PNI-dNLR score model yielded the lowest AIC value (853.89 vs 858.85 vs 868.69) and BIC value (867.09 vs 872.04 vs 881.88) (Supplementary Table 5). Time-dependent C-index analysis demonstrated that the preoperative PNI-dNLR score model exhibited superior predictive performance for 1-, 3-, and 5-year OS and 5-year DFS in older adults with GC. Further analysis using time-dependent ROC (Time-ROC) curve analysis demonstrated that the AUC values for the PNI-dNLR score at various time points for both OS and DFS were higher than those observed for PNI and dNLR alone (Figure 4A and B). When compared with preoperative PNI and dNLR used individually, the PNI-dNLR score consistently achieved higher C-index values: PNI-dNLR vs PNI vs dNLR: 1-year OS: 0.634 vs0.595 vs 0.619; 3-year OS: 0.614 vs 0.592 vs 0.573; 5-year OS: 0.601 vs 0.582 vs 0.560; 1-year DFS: 0.617 vs 0.578 vs 0.608; 3-year DFS: 0.604 vs 0.576 vs 0.573; 5-year DFS: 0.598 vs 0.574 vs 0.565) (Figure 4C).
 |
Figure 4 The time-dependent receiver operating characteristic curve curves of inflammation and nutrition-relative indicators for diagnosing (A) overall survival and (B) disease-free survival in older adult patients with gastric cancer. (C) Construction of 5-year survival prediction models and C-index analysis in elderly gastric cancer patients after surgery. Abbreviations: PNI, Prognostic Nutritional Index; dNLR, derived NLR. |
To further validate the prognostic value of the PNI-dNLR score, three feature selection methods were applied to identify relevant prognostic variables for 5-year OS: LASSO-Cox regression, RSF, and ST modeling. These methods identified 4, 8, and 5 significant or high-importance variables, respectively (Supplementary Figures 1–3 and Supplementary Table 6).
By intersecting the variables identified through these three methods with the independent prognostic factors obtained from multivariate Cox regression analysis, the PNI-dNLR score model consistently remained, alongside pTNM stage and surgical method, an important prognostic factor influencing outcomes in older adults with GC (Figure 5A). We compared the C-index of four models (COX, ST, LASSO-COX, and RSF, Figure 5B). The results showed that the RSF model achieved the highest C-index (0.805) on the test set, significantly outperforming the other models (eg, P < 0.05), indicating its superior discriminatory ability in differentiating the prognosis risk of patients. Figure 5C presents the time-dependent ROC curves of each model at different follow-up time points. The RSF model demonstrated the highest AUC) at all time points, further confirming its stable predictive accuracy. For the RSF model, we conducted a SHAP explainability analysis. Figure 5D shows the SHAP beeswarm plot, where each point represents the SHAP value of a sample, and the color indicates the feature value size. This plot visually reveals the contribution direction and degree of each feature to the model’s prediction, with TNM stage, surgical approach, and PNI-dNLR score having the most significant impact on prognosis risk. A bar chart of variable importance (Figure 5E), quantitatively displays the average absolute SHAP values of each feature, confirming that TNM stage, surgical approach, and PNI-dNLR score are the top three important predictors in the RSF model, consistent with clinical understanding. A waterfall plot of the prediction decomposition of a representative high-risk sample (Figure 5F), clearly illustrates how each feature collaboratively leads to the prediction of high risk for this sample, enhancing the transparency and clinical interpretability of the model’s prediction.
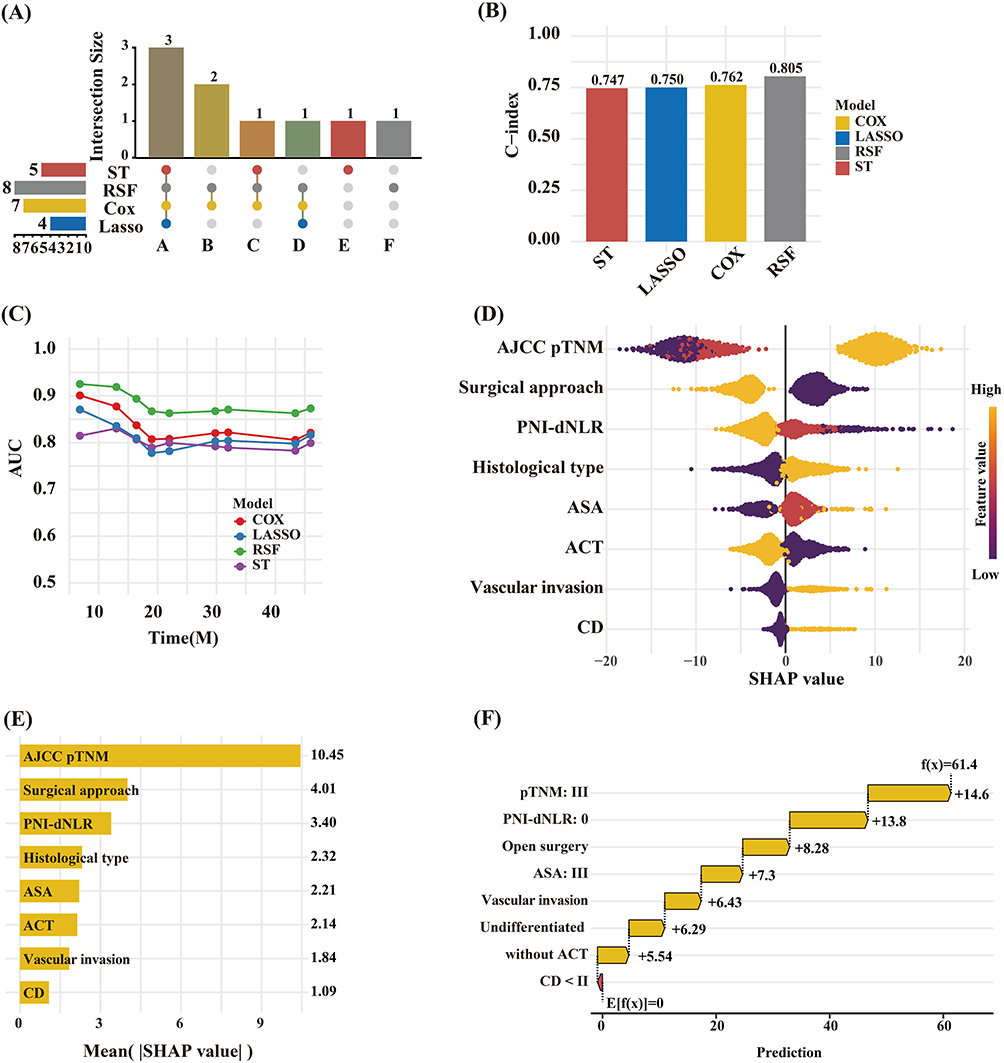 |
Figure 5 (A) Upset plot of interactions between the predictors. A PNI-dNLR, Surgical approach, AJCC pTNM. B Histological type, CD, C ACT, D ASA, E BMI, F Vascular invasion. (B) C-index of the four models. (C) Time-dependent ROC curves. (D)SHAP beeswarm plot of feature importance. (E) Mean absolute SHAP values (VIMP) of each predictor. (F) Waterfall plot of feature contributions to individual prediction. Abbreviations: BMI, Body Mass Index; ASA, American Society of Anesthesiologists; AJCC, American Joint Committee on Cancer; CD, Clavien-Dino grade system; ACT, adjuvant chemotherapy. |
Discussion
Although numerous studies have reported a strong association between preoperative blood-based inflammatory and nutritional indicators and outcomes in various malignancies, including GC, their prognostic significance in older adults with GC remains insufficiently defined. In the present study, the dNLR and PNI were consistently identified as independent prognostic factors for long-term postoperative survival in this population. Elevated dNLR and reduced PNI were significantly associated with poorer prognostic outcomes.
Furthermore, a composite preoperative score, termed the PNI-dNLR score, was developed by integrating dNLR and PNI. This model demonstrated superior predictive performance compared to the individual indicators alone, and more effectively stratified risk within the study population. These findings support the utility of the PNI-dNLR score as a clinically applicable tool for individualized prognostic assessment and treatment planning in older adults undergoing radical gastrectomy for GC.
Inflammation plays a key role in the initiation and progression of malignant tumors.5,19 Previous studies, including that by Proctor et al reported that elevated dNLR is strongly associated with poor prognosis across various malignancies and serves as an independent prognostic marker.20 Li et al reported that dNLR outperformed several widely used inflammation-based and nutritional biomarkers in predicting outcomes in patients with GC.21 Although prior studies have supported the prognostic use of dNLR in the general GC population, its specific relevance to older adults with GC has remained unclear. In the present study, an elevated preoperative dNLR was positively associated with increased mortality risk and was identified as an independent predictor of long-term postoperative survival in this older adult cohort.
Proctor et al also reported that NLR offers prognostic value comparable to dNLR, with minor but sustained advantages.20 Additional studies have indicated that both dNLR and NLR independently predict OS and PFS in patients with GC.10 Furthermore, dNLR has shown prognostic accuracy comparable to, or slightly exceeding, that of NLR in various other malignancies, including melanoma, bladder cancer, renal cancer, and breast cancer.22 Consistent with these findings, the current analysis demonstrated that dNLR outperformed NLR in predicting long-term survival outcomes. As dNLR is calculated using total white blood cell and neutrophil counts, its elevation primarily reflects an increase in neutrophil-mediated inflammatory responses. Neutrophils, as a major component of peripheral white blood cells, contribute to tumor progression through the secretion of various pro-tumorigenic mediators, including vascular endothelial growth factor (VEGF), ROS, nitric oxide, interleukin-18, and matrix metalloproteinases. Additionally, neutrophils may impair anti-tumor immunity by inhibiting T cell-mediated responses.23 This study not only confirmed the independent prognostic significance of dNLR in older adults with GC but also provided further evidence supporting its potential to serve as a substitute for NLR in predicting long-term cancer outcomes.
Nutritional status is a well-established determinant of cancer prognosis. Prior studies have demonstrated a correlation between malnutrition and adverse oncologic outcomes, as well as an increased risk of mortality among older adults.24,25 Early identification of nutritional deficits in individuals with cancer is essential to facilitate timely nutritional support, which may contribute to improved clinical outcomes.
Screening tools, such as the Mini Nutritional Assessment–Short Form and the Nutrition Risk Screening 2002, are frequently used to assess nutritional risk.26,27 However, the applicability of these tools may be limited by the complexity of their scoring systems and the subjective nature of questionnaire-based assessments. In contrast, the PNI, derived from serum albumin concentration and peripheral blood lymphocyte count, offers an objective and readily accessible measure of nutritional status.28
Prior studies have indicated that a low PNI is significantly associated with reduced overall OS and DFS following gastrectomy.29 Jing et al reported that, among patients with early-stage GC, older adults with lower PNI levels had a poorer prognosis.30 Consistent with these findings, the present study conformed the prognostic relevance of PNI in older adults undergoing curative gastrectomy, and was identifying it as an independent protective factor for long-term survival. These results further support the prognostic relevance of nutritional status in older adults with GC.
Malnutrition is often accompanied by immunodeficiency. Lymphocytes, which are central to immune function, contribute to tumor immune surveillance through mechanisms such as interferon-γ production, cytotoxic activity, and the induction of tumor cell apoptosis. These mechanisms are critical for inhibiting tumor progression and limiting immune escape.31
Given the association between poor nutritional status and delayed postoperative recovery, increased incidence of complications, and reduced adherence to adjuvant therapies, optimization of preoperative nutritional status in older adults with GC is of critical importance.32
In this study, optimal cut-off values for inflammatory and nutritional biomarkers were determined using X-tile software. X-tile, a bioinformatics tool developed by Robert et al, is designed to assess the association between biomarkers and survival outcomes.18 It identifies the optimal threshold for classifying continuous variables by calculating the minimum p value based on the log-rank χ2 statistic. This approach has been widely used for determining cut-off values in survival analysis.33 The prognostic influence of sex and age in older adults with GC remains a subject of debate.34,35 In the current analysis, multivariate Cox regression indicated that neither sex nor age served as independent prognostic factors, consistent with the findings reported by Li et al34 However, Lu et al reported that while sex was not a significant factor, age ≥ 75 years was associated with poorer prognosis.35 Since the release of the initial report by Kitano et al on the feasibility of laparoscopic gastrectomy for gastric malignancies, numerous studies have demonstrated comparable long-term survival outcomes between laparoscopic and other open surgical approaches.35–38 In contrast, this study identified laparoscopic surgery as an independent protective factor for long-term prognosis in older adults, based on multivariate Cox regression analysis. Additionally, the presence of severe postoperative complications was significantly associated with poorer long-term outcomes.
Several factors may explain these findings. Older adults often present with compromised physiological status and multiple preoperative comorbidities, which can result in reduced surgical tolerance and a higher incidence of postoperative complications. Compared with open surgery, laparoscopic procedures are associated with reduced surgical trauma and lower complication rates, providing greater benefits in short-term postoperative recovery.35,38 Although the current findings indicate potential long-term prognostic advantages of laparoscopic surgery in older adults with GC, further multicenter studies are required to elucidate the underlying mechanisms.
In this study, a novel prognostic score model, the PNI-dNLR score, was developed by integrating the PNI and dNLR. The prognostic utility of this composite score, along with individual markers, was assessed in older adults undergoing radical gastrectomy for GC. Both PNI and dNLR are reliable, cost-effective, and clinically accessible biomarkers for predicting long-term outcomes in this population. Importantly, the PNI-dNLR score demonstrated superior predictive performance compared with the use of either marker alone, potentially enhancing survival risk stratification while reducing the likelihood of false-positive or false-negative results.
However, several limitations of this study should be acknowledged. The retrospective single-center nature of the study introduces the potential for selection bias, and the analysis may be limited by incomplete or missing data. Unmeasured confounding factors like socioeconomic status, educational level, dietary habits, alcohol consumption, frailty, elaborate comorbid conditions, and nutritional interventions may influence PNI and dNLR values and were not fully accounted for in the current model. During the study period, neoadjuvant chemotherapy had not been widely implemented as a standard component of GC treatment protocols; therefore, individuals who received neoadjuvant therapy were not included, and the predictive value of the PNI-dNLR score in this subgroup remains to be determined. The same dataset was used to determine the cut-off values, which could cause bias. As the model was developed based on data from an Eastern population without internal and external validation and certain statistical procedures could cause overfitting due to application of more than one model to identical data, the generalizability of the conclusion may be limited. The predictive performance of the combined PNI-dNLR score was modest, which need further prospective multi-center study enrolling a large sample of patients to confirm. Finally, Incorporating brief comparison with previously established prognostic scores or models will confirm the clinical application value of combined PNI-dNLR score. Despite these limitations, the findings of this study demonstrated that PNI, dNLR, and the combined PNI-dNLR score are significantly associated with OS and DFS in older adults with GC. These findings provide additional evidence to support the use of inflammation- and nutrition-based biomarkers in population-level prognostic assessment.
Conclusion
The preoperative PNI-dNLR score, a composite index integrating PNI and dNLR, demonstrated superior predictive performance compared to the individual use of either biomarker. This model effectively stratified older adults with GC into distinct risk groups and was independently associated with OS and DSF. The PNI-dNLR score, which need further prospective multicenter study conducting internal and external validation to confirm, may serve as a valuable and objective tool for preoperative prognostic assessment and individualized treatment planning in this population.
Abbreviations
AIC, Akaike information criterion; AISI, aggregate index of systemic inflammation; AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiologists; AUC, area under the curve; BIC, Bayesian information criterion; BMI, body mass index; CD, Clavien-Dindo; CEA, carcinoembryonic antigen; CI, confidence interval; C-index, concordance index; DFS, disease-free survival; dNLR, derived neutrophil-to-lymphocyte ratio; GC, gastric cancer; GNRI, geriatric nutritional risk index; HR, hazard ratio; IQR, interquartile range; K–M, Kaplan–Meier; LASSO-Cox, least absolute shrinkage and selection operator Cox regression; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PFS, progression-free survival; PLR, platelet-to-lymphocyte ratio; PNI, prognostic nutritional index; PNI-dNLR, prognostic nutritional index-derived neutrophil-to-lymphocyte ratio (score); pN, pathological N (stage); pT, pathological T (stage); pTNM, pathological TNM; RCS, restricted cubic spline; ROC, receiver operating characteristic; RSF, random survival forest; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; ST, survival tree; Time-ROC, time-dependent receiver operating characteristic; Tol, tolerance; VEGF, vascular endothelial growth factor; VIF, variance inflation factor.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author (Wei Lin).
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Affiliated Hospital of Putian University (Approval Number: 2025445). Written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
National Science and Technology Project Recordation (Grant No. 2024L3006): “Research on Functional Components of Bee Products against Gastric Cancer and Promoting Wound Healing and Key Technologies for Industrialization” (Fujian Bee Product Development Engineering Technology Research Center).
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–19. doi:10.3322/caac.21834
2. Sundar R, Nakayama I, Markar SR, et al. Gastric cancer. Lancet. 2025;405(10494):2087–2102. doi:10.1016/S0140-6736(25)00052-2
3. Li C, Chen D, Yang H. Trends in incidence, survival and mortality of gastric cancer in the United States: a population-based study, 2001–2015. Asian Pac J Cancer Prev. 2023;24(6):2011–2020. doi:10.31557/APJCP.2023.24.6.2011
4. Marubashi S, Takahashi A, Kakeji Y, et al. Surgical outcomes in gastroenterological surgery in Japan: report of the National Clinical Database 2011–2019. Ann Gastroenterol Surg. 2021;5(5):639–658. doi:10.1002/ags3.12462
5. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
6. Salas S, Cottet V, Dossus L, et al. Nutritional factors during and after cancer: impacts on survival and quality of life. Nutrients. 2022;14(14):2958. doi:10.3390/nu14142958
7. Shachar SS, Williams GR, Muss HB, Nishijima TF. Prognostic value of sarcopenia in adults with solid tumours: a meta-analysis and systematic review. Eur J Cancer. 2016;57:58–67. doi:10.1016/j.ejca.2015.12.030
8. Tan S, Zheng Q, Zhang W, Zhou M, Xia C, Feng W. Prognostic value of inflammatory markers NLR, PLR, and LMR in gastric cancer patients treated with immune checkpoint inhibitors: a meta-analysis and systematic review. Front Immunol. 2024;15:1408700.
9. Feier CVI, Muntean C, Faur AM, et al. An exploratory assessment of pre-treatment inflammatory profiles in gastric cancer patients. Diseases. 2024;12(4):78. doi:10.3390/diseases12040078
10. Yu C, Jiang H, Wang L, Jiang Z, Jin C. Baseline (derived) neutrophil-lymphocyte ratio associated with survival in gastroesophageal junction or gastric cancer treated with ICIs. Front Oncol. 2025;15:1404695. doi:10.3389/fonc.2025.1404695
11. Matsunaga T, Saito H, Osaki T, et al. Impact of geriatric nutritional risk index on outcomes after gastrectomy in elderly patients with gastric cancer: a retrospective multicenter study in Japan. BMC Cancer. 2022;22:540. doi:10.1186/s12885-022-09638-6
12. Yang Y, Gao P, Song Y, et al. The prognostic nutritional index is a predictive indicator of prognosis and postoperative complications in gastric cancer: a meta-analysis. Eur J Surg Oncol. 2016;42(8):1176–1182. doi:10.1016/j.ejso.2016.05.029
13. Pan Y, Si H, Deng G, et al. A composite biomarker of derived neutrophil-lymphocyte ratio and platelet-lymphocyte ratio correlates with outcomes in advanced gastric cancer patients treated with Anti-PD-1 antibodies. Front Oncol. 2022;11:798415. doi:10.3389/fonc.2021.798415
14. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
15. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017;20(1):1–19. doi:10.1007/s10120-016-0622-4
16. Deng Q, He B, Liu X, et al. Prognostic value of pre-operative inflammatory response biomarkers in gastric cancer patients and the construction of a predictive model. J Transl Med. 2015;13:66. doi:10.1186/s12967-015-0409-0
17. Clavien PA, Barkun J, De Oliveira ML, et al. The clavien-dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
18. Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10(21):7252–7259. doi:10.1158/1078-0432.CCR-04-0713
19. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
20. Proctor MJ, McMillan DC, Morrison DS, Fletcher CD, Horgan PG, Clarke SJ. A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer. Br J Cancer. 2012;107(4):695–699. doi:10.1038/bjc.2012.292
21. Song S, Li C, Li S, Gao H, Lan X, Xue Y. Derived neutrophil to lymphocyte ratio and monocyte to lymphocyte ratio may be better biomarkers for predicting overall survival of patients with advanced gastric cancer. Onco Targets Ther. 2017;10:3145–3154. doi:10.2147/OTT.S138039
22. Duan J, Pan L, Yang M. Preoperative elevated neutrophil-to-lymphocyte ratio (NLR) and derived NLR are associated with poor prognosis in patients with breast cancer: a meta-analysis. Medicine. 2018;97(49):e13340. doi:10.1097/MD.0000000000013340
23. Ardi VC, Kupriyanova TA, Deryugina EI, Quigley JP. Human neutrophils uniquely release TIMP-free MMP-9 to provide a potent catalytic stimulator of angiogenesis. Proc Natl Acad Sci U S A. 2007;104(51):20262–20267. doi:10.1073/pnas.0706438104
24. Fielding RA, Landi F, Smoyer KE, Tarasenko L, Groarke J. Association of anorexia/appetite loss with malnutrition and mortality in older populations: a systematic literature review. J Cachexia Sarcopenia Muscle. 2023;14(2):706–729. doi:10.1002/jcsm.13186
25. Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489–495. doi:10.1016/S1470-2045(10)70218-7
26. Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56(6):M366–372. doi:10.1093/gerona/56.6.M366
27. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z; Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003;22(3):321–336. doi:10.1016/S0261-5614(02)00214-5
28. Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi. 1984;85(9):1001–1005.
29. Deng H, He Y, Huang G, Huang Y, Wu J, Qin X. Predictive value of prognostic nutritional index in patients undergoing gastrectomy for gastric cancer: a systematic review and meta-analysis. Medicine. 2024;103(41):e39917. doi:10.1097/MD.0000000000039917
30. Jing Y, Ren M, Li X, et al. The effect of Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in early gastric cancer. J Inflamm Res. 2024;17:10273–10287. doi:10.2147/JIR.S499094
31. Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity. 2004;21(2):137–148. doi:10.1016/j.immuni.2004.07.017
32. Yun JH, Song GJ, Son MW, Lee MS. Global leadership initiative on malnutrition criteria and immunonutritional status predict chemoadherence and survival in Stage II/III Gastric Cancer Treated with XELOX Chemotherapy. Nutrients. 2024;16(20):3468. doi:10.3390/nu16203468
33. Chen C, Yang H, Cai D, Xiang L, Fang W, Wang R. Preoperative peripheral blood neutrophil-to-lymphocyte ratios (NLR) and platelet-to-lymphocyte ratio (PLR) related nomograms predict the survival of patients with limited-stage small-cell lung cancer. Transl Lung Cancer Res. 2021;10(2):866–877. doi:10.21037/tlcr-20-997
34. Du Y, Li Y, Tan Z, et al. Prognostic value of combining preoperative immune-inflammatory-nutritional index and tumor biomarkers in gastric cancer patients undergoing radical resection. Front Nutr. 2025;12. doi:10.3389/fnut.2025.1562202
35. Lin GS, Huang XY, Lu J, et al. A good preoperative immune prognostic index is predictive of better long-term outcomes after laparoscopic gastrectomy compared with open gastrectomy for stage II gastric cancer in elderly patients. Surg Endosc. 2022;36(3):1814–1826. doi:10.1007/s00464-021-08461-7
36. Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc. 1994;4(2):146–148.
37. Wang JB, Zhong Q, Chen QY, et al. Well-designed retrospective study versus small-sample prospective study in research based on laparoscopic and open radical distal gastrectomy for advanced gastric cancer. Surg Endosc. 2020;34(10):4504–4515. doi:10.1007/s00464-019-07237-4
38. Inokuchi M, Nakagawa M, Tanioka T, Okuno K, Gokita K, Kojima K. Long- and short-term outcomes of laparoscopic gastrectomy versus open gastrectomy in patients with clinically and pathological locally advanced gastric cancer: a propensity-score matching analysis. Surg Endosc. 2018;32(2):735–742. doi:10.1007/s00464-017-5730-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Emerging Roles and Mechanisms of PAQR3 in Human Cancer: Pathophysiology and Therapeutic Implications
Guo Q, Liu XL, Zhai K, Chen C, Ke XX, Zhang J, Xu G
International Journal of General Medicine 2023, 16:4321-4328
Published Date: 22 September 2023
Machine Learning for Prediction of Non-Small Cell Lung Cancer Based on Inflammatory and Nutritional Indicators in Adults: A Cross-Sectional Study
Wang Q, Liang T, Li Y, Liu X
Cancer Management and Research 2024, 16:527-535
Published Date: 30 May 2024
Identification and Clinical Validation of High HSP60 Expression Predicts Poor Prognosis in Patients with Ovarian Cancer
Zheng M, Li S, Deng J, Huang C, Zhang H
International Journal of General Medicine 2025, 18:103-111
Published Date: 8 January 2025
Low Serum Cholinesterase Levels Predict Poor Prognosis in Patients with Ovarian Cancer
Su H, Liao D, Huang C, Liu Q, Yu L
International Journal of General Medicine 2025, 18:1023-1033
Published Date: 25 February 2025
The Naples Prognostic Score Exerts a Significant Impact on the Prognosis of Patients Diagnosed with External Auditory Canal Carcinoma After Surgery
Xu XL, Cheng H, Wu XM, Xu JH
Cancer Management and Research 2025, 17:985-996
Published Date: 25 May 2025