Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Predictors of Acute Exacerbations in COPD: A Systematic Review
Authors Chamaon D ![]() , Lenferink A
, Lenferink A ![]() , Bucsán C, Van Dijk SHB
, Bucsán C, Van Dijk SHB ![]() , Van Beurden WJ
, Van Beurden WJ ![]() , van der Valk PDLPM, van der Palen J
, van der Valk PDLPM, van der Palen J ![]() , Brusse-Keizer MGJ
, Brusse-Keizer MGJ ![]()
Received 16 May 2025
Accepted for publication 10 November 2025
Published 14 February 2026 Volume 2026:21 540753
DOI https://doi.org/10.2147/COPD.S540753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Dumiana Chamaon,1,2 Anke Lenferink,2,3 Charlotte Bucsán,1,2 Sanne H B Van Dijk,2,3 Wendy JC Van Beurden,2 Paul DLPM van der Valk,2 Job van der Palen,1,4 Marjolein GJ Brusse-Keizer3,4
1Section Cognition, Data, and Education, Faculty of Behavioural, Management and Social Sciences, University of Twente, Enschede, the Netherlands; 2Department of Pulmonary Medicine, Medisch Spectrum Twente, Enschede, the Netherlands; 3Health Technology and Services Research, Faculty of Behavioural, Management and Social Sciences, Technical Medical Centre, University of Twente, Enschede, the Netherlands; 4Department of Epidemiology, Medical School Twente, Enschede, the Netherlands
Correspondence: Dumiana Chamaon, Section Cognition, Data, and education, Faculty of Behavioural, Management and Social sciences, University of Twente, Enschede, the Netherlands, Tel +31 6 31751586, Email [email protected]
Background: COPD is characterized by acute exacerbations (AECOPD), which drive its progression and burden. AECOPD can be caused by various factors. Better prediction of AECOPD provides opportunity for initiating preventive treatment.
Methods: This systematic review provides an evidence-based overview of clinical predictors of moderate, severe AECOPD and relapse of moderate and severe AECOPD (≤ 28 days of a previous AECOPD). Cohort studies, case-control studies, or (cluster) randomized controlled trials published in English between January 2011–December 2023 in PubMed, CINAHL, Embase, Web of Science and the Cochrane library were assessed. Eligible studies included patients diagnosed with COPD, aged ≥ 40 years, and who were current or ex-smokers. Predictors of AECOPD were categorized into: patient characteristics, symptoms, biomarkers, lung function test results, and composite scores. Critical appraisal was performed with the QUIPS-tool.
Results: Out of 1261 screened articles, 30 were included. Sixty-one distinct possible predictors of AECOPD were assessed, of which 37 were statistically significant (P < 0.05). Age, AECOPD history, fibrinogen, FEV1, bronchodilator response, health status measured with the COPD specific St. George’s Respiratory Questionnaire (SGRQ-C) score, and COPD GOLD classification (2– 4, B-D) were significant predictors of severe and/or moderate AECOPD in more than one article. Only 11 out of the 30 included studies had a low risk of bias.
Discussion: Based on the highest relative statistical significance, combined with the best overall risk of bias, the most promising predictors of AECOPD are history of ≥ 1 AECOPD, higher SGRQ-C scores, elevated fibrinogen levels, and worse COPD GOLD (2– 4, B-D). Future research should focus on standardization of AECOPD and predictor definitions, including the use of clearly defined cut-off values. Given the complexity and heterogeneity of COPD, combining diverse predictor domains into composite measures may enhance predictive accuracy of AECOPD, and the integration of such composites is promising for advancing COPD management in clinical practice.
Keywords: chronic obstructive pulmonary disease, exacerbation, predictors, disease management, prognostic models
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive lung condition that is characterized by acute symptom deteriorations, which are known as acute exacerbations of COPD (AECOPD). These AECOPD require a change in regular treatment and/or hospitalization depending on their severity. Mild AECOPD only require treatment with short acting bronchodilators (SABDs); moderate AECOPD with SABDs, oral corticosteroids, and/or antibiotics; and severe AECOPD require a visit to the emergency room or a hospitalization.1
AECOPD can be caused by various factors such as respiratory tract infections, environmental factors (eg air pollution), and comorbid conditions (eg heart failure).2 AECOPD have many detrimental effects on the patient. First, the increased airway inflammation and incomplete resolution of symptoms and physiological function after an AECOPD further accelerates the decline in respiratory function.3 Second, AECOPD significantly reduce the patients’ quality of life and increase functional impairment and mortality.4 Third, most COPD-related healthcare costs can be attributed to AECOPD as these often require extensive treatment during a hospitalization.4 Furthermore, since one AECOPD increases the risk of another, AECOPD readmission rates are high.1,5,6 Finally, AECOPD have a negative effect on patients’ mood. Patients often suffer from feelings of anxiety, depression and low energy, which negatively impact their personal and social life, resulting in less participation in social activities when experiencing an AECOPD.3,7,8
Better predicting AECOPD provides the opportunity to initiate preventive treatment (eg pharmacological therapy).9 Several patient characteristics (eg sex, body mass index (BMI), age, smoking status, history of AECOPD) have been linked as predictors for AECOPD.10–12 Moreover, different tools have been assessed on their ability to predict AECOPD, such as the COPD Assessment Test (CAT) or Saint George’s Respiratory Questionnaire (SGRQ).13–15 Although these tools are validated regarding their ability to assess those at risk of AECOPD, they are still not routinely used in clinical practice to predict AECOPD.5,16
Symptoms such as dyspnea or cough have also been identified as predictors of AECOPD.17,18 However, identifying AECOPD based only on patients’ symptoms can be difficult due to the variety in these individual symptoms.16 Furthermore, given the frequent existence of COPD with comorbidities, COPD symptoms lack disease specificity. Therefore, if a patient experiences dyspnea, there may be another underlying cause which should also be assessed such as pneumonia, heart failure, or pulmonary embolism.1
Although recent studies reported promising biomarkers to predict AECOPD, eg eosinophils, C-reactive protein (CRP),19,20 none of these predictors have been implemented yet in standard clinical practice, which so far resulted in the inability to attribute validated biomarkers as a (key) predictor of AECOPD.20–22 In addition, there is a lack of consistent reporting of objective biomarkers.23 Consequently, without an increased symptom like dyspnea, these biomarkers cannot specifically be attributed to AECOPD when measured independently.5,24
AECOPDs are also linked to a decline in lung function.25 Lung function test results (eg forced expiratory volume in the first second (FEV1), forced vital capacity (FVC) ratio) are useful in assessing symptomatic COPD.25 However, there are limitations in their ability of early identifying AECOPD. Although other tests such as walking tests (eg six-minute walk test (6MWT), five-repetition (sit-to-stand test) are seen as powerful predictors in COPD prognosis and show positive results in their ability of predicting AECOPD, they are not routinely used in clinical practice with the purpose of predicting AECOPD.1,26–29
Accurately predicting AECOPD and gaining insights into potential evolving COPD exacerbations remains challenging, as there is no validated tool that is currently implemented in routine clinical management of COPD to predict AECOPD.5,16 Hence, there is a clear need for objectively measurable validated markers to predict AECOPD,23 that can be implemented in standard clinical practice, to enable timely initiation of preventive treatment. The aim of this systematic literature review was therefore to provide an evidence-based overview of clinical predictors of moderate, severe and relapse of AECOPD, consisting of patient characteristics, symptoms, biomarkers, lung function test results, and composites of these.
Methods
Study Selection
Peer-reviewed studies published in English between January 2011 and December 2023 were examined to identify clinical predictors of moderate AECOPD, severe AECOPD (hospitalizations, including pneumonia) and relapse of moderate and severe AECOPD. The predictors of AECOPD were categorized into one or more of the following five groups:
- Patient characteristics: defined as individual attributes, health-related factors, and clinical history, including, but not limited to, age, gender, ethnicity, BMI, COPD disease stage (GOLD30 or ATS/ERS31), smoking status, educational level, number of previous AECOPD, number of previous respiratory-related hospitalizations;
- Symptoms: defined as a physical or mental problem that a person experiences that may indicate a disease or condition32 (eg dyspnea, cough);
- Biomarkers: defined as a biological molecule found in blood, other body fluids, or tissues that can be used to follow body processes and diseases in humans and animals, or that is a sign of a normal or abnormal process, or of a condition or disease33,34 (eg eosinophils, fibrinogen, vitamin D);
- Lung function test results: defined as the results of a respiratory function test (eg FEV1% predicted, FEV1/FVC, FVC% predicted); and
- Composites: defined as a combination of the above mentioned categories (eg BODE index).
The studies included in this review were restricted to cohort studies, case-control studies, or (cluster) randomized controlled trials (RCT). The study participants should have a COPD diagnosis according to the GOLD criteria (post-bronchodilator FEV1/FVC < 0.70)30 or ATS-ERS criteria,31 be 40 years of age or older and current or ex-smokers. Additionally, the predictor of AECOPD had to be measured prior to (not during) the AECOPD.
The outcome measures assessed in these studies were moderate and severe AECOPD as well as relapse of AECOPD. Moderate AECOPD was defined as an acute worsening of respiratory symptoms that necessitated additional treatment with antibiotics and/or oral corticosteroids (6). Severe AECOPD was characterized by an acute worsening of symptoms that led to hospitalization.30 Relapse of AECOPD was defined as the occurrence of a moderate or severe AECOPD within 28 days of a prior AECOPD of either severity.35 In studies where moderate and severe AECOPD were combined into a single outcome measure, predictors were categorized as “both moderate and severe AECOPD”.
A predictor was considered statistically significant if the study reported a statistically significant relation (p < 0.05) between the predictor variable and the outcome measure of interest (ie moderate, severe, or relapse of AECOPD). Outcomes presented with only an area under the receiver operating curve (AUROC) were included if the AUROC 95% confidence interval was entirely above 0.5, indicating discriminative performance better than chance.36 The most promising predictors of AECOPD within their respective category were selected based on the highest relative statistical significance of a predictor and the best overall risk of bias of the studies reporting on the predictor.
Screening Process
This systematic review followed the PRISMA guidelines.37 A systematic search was conducted in PubMed, CINAHL, Embase, Web of Science and the Cochrane library (see Supplemental information; Appendix A, Table 1A). Snowballing of identified reviews and included articles was performed (CB or DC) to identify additional eligible articles.
First, the references obtained from the search were uploaded in Covidence,38 a systematic review managing software, and deduplicated. Second, the titles and abstracts of the deduplicated set of articles were screened for eligibility by two independent reviewers (CB or DC and MB or AL or JP or SvD or PV or WB). Third, the full text of the relevant articles was screened for eligibility by two independent reviewers (CB or DC and MB or AL or JP or PV or WB or SvD). Any conflicts during the screening process were resolved by discussion. If no agreement was reached, a third reviewer was consulted to make the final decision.
Data Extraction and Critical Appraisal
Data extraction and critical appraisal (Modified Quality In Prognosis Studies (QUIPS) tool39) were performed (CB or DC). The articles were assessed on low, moderate and high risk of bias, for the domains study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, statistical analysis and reporting, in line with the assessment of Hayden et al (2013).39 If no clear judgement could be made based on the information reported in the article, the risk of bias was assessed as unsure. A random sample of the data extraction and critical appraisal was independently assessed or checked by a second reviewer (MB or AL or SvD or JP). Any conflicts were resolved by discussion.
The following data was extracted from the included articles: 1) general information (title, first author, publication year, country), 2) study information (sample size, study design, eligibility criteria, objective), 3) outcome measure (moderate or severe AECOPD, relapse of moderate or severe AECOPD), 4) predictor information (predictor category (patient characteristics, biomarkers, lung function test results, symptoms, composites), predictor variable (eg age, dyspnea, Fibrinogen), cut-off values and performance of the predictor (ie hazard ratio, odds ratio, risk ratio, incidence ratio ratio)), and 5) covariates in the prediction model (eg age, gender, pack-years, 6-minute walking distance (6MWD)).
Results
The search yielded 1261 articles after deduplication. The title and abstract screening resulted in 231 articles for full text screening. Finally, 30 articles reporting on 25 studies were included for data extraction and critical appraisal (Figure 1). Main reasons for exclusion were no measurement of the outcome of interest (n = 55), other study type (n = 29), and other definitions of moderate, severe AECOPD, or relapse of AECOPD (n = 24).
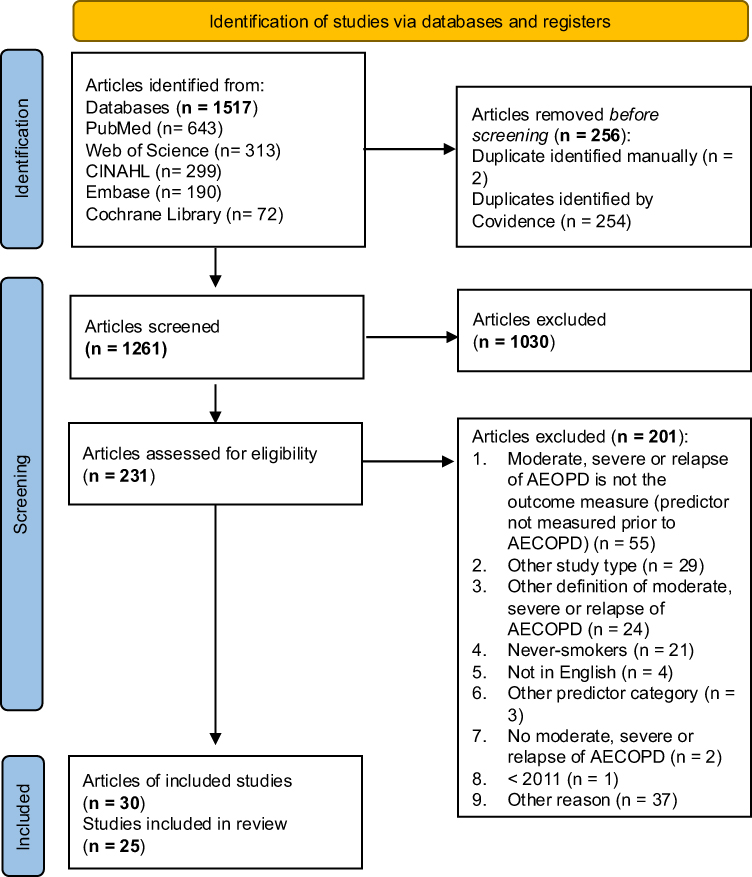 |
Figure 1 PRISMA 2020 flow diagram37 for the identification of studies. Abbreviations: AreaFE%, area under flow-volume curve; BODE index, composite of body-mass index; airflow obstruction, dyspnea, and exercise capacity, CID, clinically important deterioration; (decrease in FEV1 of 100 mL, increase of 4 units in St. George’s Respiratory Questionnaire, and incidence of moderate and/or severe exacerbation), COPD GOLD-classification (1–4); based on lung function, COPD GOLD-classification A-D; based on symptoms and lung function, FEV1% predicted; Forced expiratory volume in 1 second based on population average, FVC% predicted; Forced vital capacity based on population average, mMRC; modified Medical Research Council Dyspnea scale, PaCO2: Partial pressure of carbon dioxide. SGRQ(-C); St. George’s Respiratory Questionnaire (- COPD). Note: Bold font indicates the sum of articles/studies. *No statistical significant relation (p > 0.05) reported. |
Study Characteristics
Table 1 presents an overview of the 30 included articles (reporting 25 distinct studies) and their characteristics, including 21 cohort studies, three RCTs and one case-control study. The sample size ranged between 15 and 10,000 participants with an age range of 59–75 years old, current smokers varied between 10 and 53%, and a FEV1% predicted with a range of 39–76%. Studies were conducted in 19 different countries.
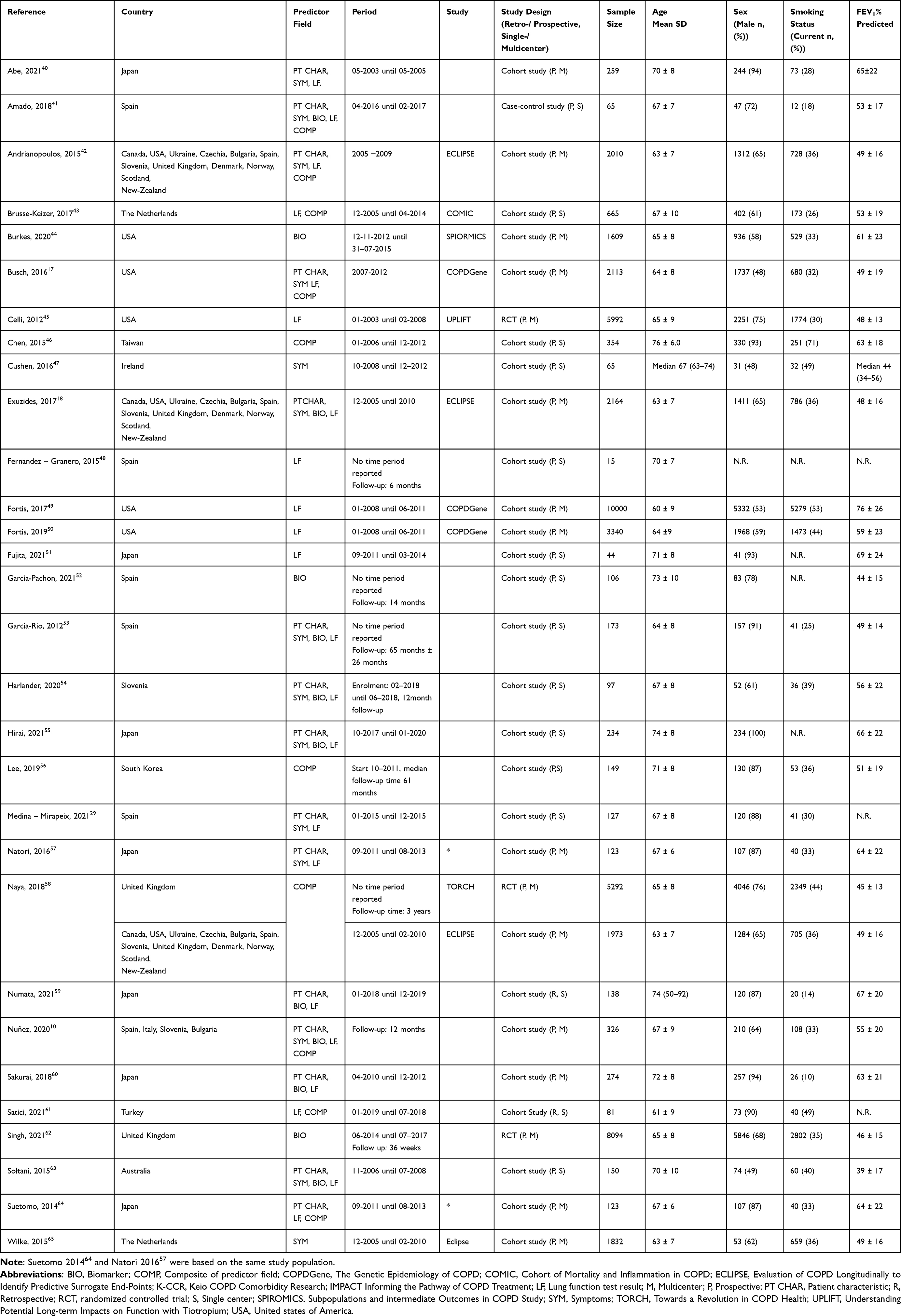 |
Table 1 Overview Characteristics and Demographics of Included Articles (n = 30) |
Risk of Bias
Of the 30 included articles, only 3 articles49–51 had a low risk of bias on all six QUIPS domains. Fourteen articles had an overall high risk of bias, five an overall moderate risk and eleven an overall low risk of bias (Table 2).
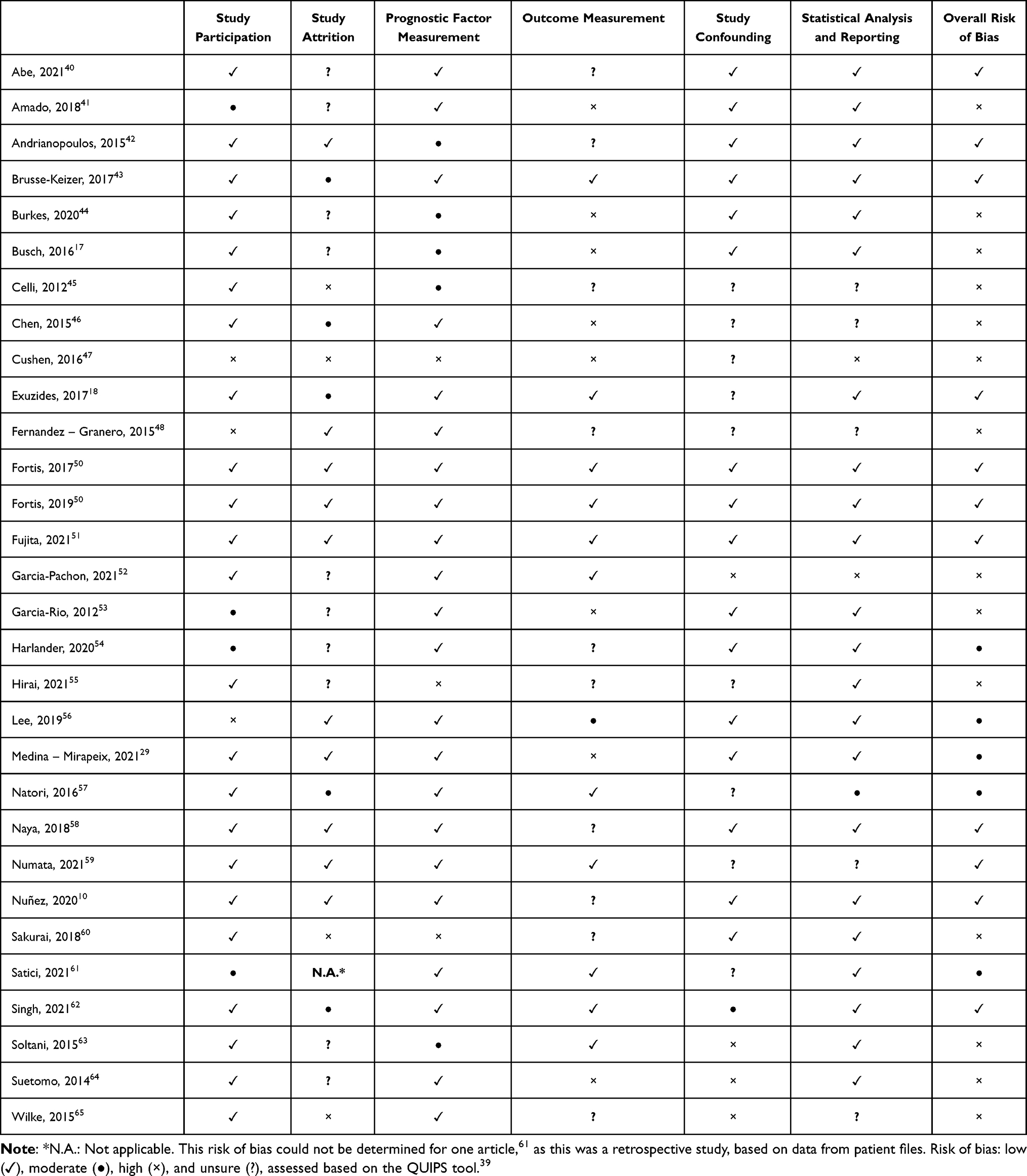 |
Table 2 Risk of bias for each included article (n=30) according to authors’ judgements |
Predictors of AECOPD
Sixty-one possible predictors of AECOPD (patient characteristics n = 12, symptoms n = 8, biomarkers n = 20, lung function test results n = 17, and composites n = 4) were assessed in the 30 included articles. For a full overview of all extracted information per predictor see Supplemental information; Appendix B and table B1.
In total, 37 predictors of AECOPD had a statistically significant correlation (p < 0.05) with the outcome measure of interest (Table 3). Of these, 36 reported an effect measure (eg hazard ratio, risk ratio, likelihood) for moderate (n = 16), severe (n = 24), and both moderate and severe AECOPD (n = 17). Figure 2 provides an overview of the number of times statistical significance and non-statistical significance was reported in a prediction model for these 34 predictors. None of the included articles reported predictors of relapse (within 28 days) of AECOPD.
 |
Table 3 Overview of the Identified Possible Predictors of AECOPD with Studies That Reported a Statistically Significant Association (P < 0.05) with Moderate, Severe or Both Moderate and Severe AECOPD |
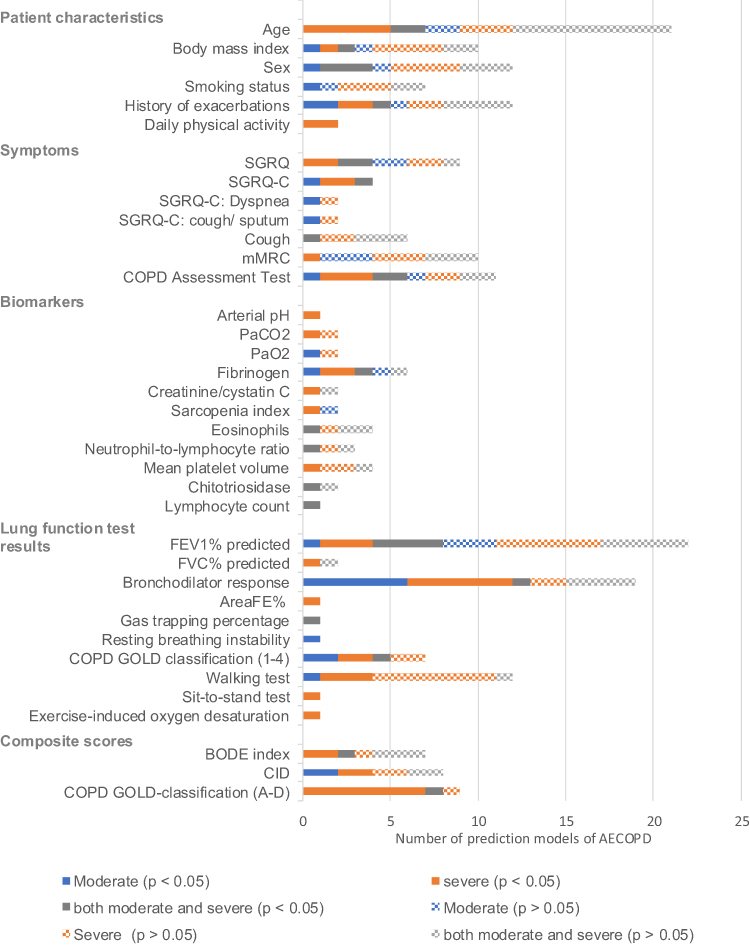 |
Figure 2 Overview of 37 predictors of moderate, severe, and both moderate and severe AECOPD, with the number of times statistical significance (p < 0.05) and non-statistical significance (p > 0.05) was reported in a prediction model of AECOPD. |
Patient Characteristics
Six patient characteristics were identified as statistically significant predictors: age (7 out of 21 prediction models), BMI (3/10 models), sex (4/12 models), smoking status (1/6 models), history of AECOPD (5/7 models), and daily physical activity (2/2 models).
Older age showed an increased risk of severe AECOPD in four models,18,29,42,59 and for both moderate and severe AECOPD in two models.17,59 One article63 found that younger age was associated with a higher risk of severe AECOPD (readmission within 6 months) with a 3% increase for every year younger in age.
Patients with a low versus normal BMI showed a lower likelihood (−14.5%) of moderate AECOPD within the coming year, and an increased risk (+25.5%) of severe AECOPD in patients with a low versus normal BMI.18 Patients with a lower BMI were also at a higher risk of both moderate and severe AECOPD compared to patients with a higher BMI.59
Females were more likely to experience moderate AECOPD,18 and both moderate and severe AECOPD.17 Current smokers had a lower risk of moderate AECOPD compared to former smokers.18 Patients with a history of at least one or more compared to no history of an AECOPD had a higher probability of moderate AECOPD,18,40 severe AECOPD,18,29 or both moderate and severe AECOPD.10 Additionally, a lower level of daily physical activity resulted in a higher risk of severe AECOPD.53
Symptoms
Seven statistically significant predictors were identified in the symptom category: St. George’s Respiratory Questionnaire (SGRQ) (4/9 models), St. George’s Respiratory Questionnaire-COPD (SGRQ-C) (4/4 models), SGRQ-C domain: dyspnea (2/4 models), SGRQ-C domain: cough and/or sputum (1/2 models), cough (1/6 models) COPD Assessment Test (CAT) (6/11 models), (modified) Medical Research Council (mMRC) dyspnea scale (1/10 models).
Health status (symptoms, activity, and impact on daily life) was measured through the SGRQ, with a higher score indicating lower health status.66 Two articles40,42 found a higher SGRQ score to predict severe AECOPD, each using different thresholds. One identified an increased risk at ≥8 points increase over a one year period in the SGRQ total score.40 Another article found an increased risk for those with a SGRQ score ≥45.42 A higher compared to a lower SGRQ total score also increased the risk of both moderate and severe AECOPD.17 Patients with a higher baseline total score in the COPD specific version of the SGRQ (SGRQ-C) were at greater risk of experiencing a moderate AECOPD (+0.6% per SGRQ-C point) within the coming year.18 The SGRQ-C also predicted severe AECOPD in two articles,18,65 although with varying thresholds. One article65 identified a change of 4 points over one year time period to either increase (Δ≥+4 points) or lower (Δ≤−4 points) the risk of severe AECOPD, the other article18 reported +2.2% risk per point increase in SGRQ-C score over a one year time period, compared to patients with a lower score. Additionally, the SGRQ-C also predicted both moderate and severe AECOPD when there is a change of at least four points in the score.65 SGRQ-C Dyspnea or cough and/or sputum, assessed using the SGRQ-C domain score, predicted moderate AECOPD in patients reporting these symptoms compared to those who did not.18 Additionally, frequent coughing was statistically significant for both moderate and severe AECOPD among patients using short acting bronchodilators in one article.17
Patients with a higher CAT score had an increased risk of severe AECOPD,55,61,64 moderate AECOPD,55 and of the combination of moderate and severe AECOPD.10,64 An mMRC dyspnea scale score of ≥2 was statistically significant in predicting higher risk of severe AECOPD in one article.41
Biomarkers
In the biomarker category, eleven statistically significant predictors for AECOPD were found: arterial pH (1/1 model), PaCO2 (1/2 models), PaO2 (1/2 models), fibrinogen (4/6 models), creatinine/cystatin C (1/2 model), sarcopenia index (1/2 model), eosinophils (1/4 models), neutrophil to lymphocyte ratio (NLR) (1/3 models), mean platelet volume (MPV) (1/4 model), chitotriosidase (1/2 models), and lymphocyte count (1/1 model).
A lower arterial pH (per 0.01) increased the risk of a new severe AECOPD within 3- and 6-months of a former severe AECOPD.63 Higher PaCO2 was also identified as a predictor of severe AECOPD in patients with a history of severe AECOPD, with each unit increase raising the risk by approximately 1%.63 A lower PaO2 decreased the risk of a moderate AECOPD.51 Patients with higher baseline fibrinogen levels, in a stable phase, were at a higher risk (+0.1% per mg/dL) of moderate and severe AECOPD.18 Singh et al (2021) observed that patients with fibrinogen levels of ≥3.5 g/L had a higher risk of severe AECOPD and the combination of both moderate and severe AECOPD.62 Patients with low serum creatinine/cystatin C levels (<0.71)55 or a low sarcopenia index (SI) (<73.9)41 were at higher risk of a severe AECOPD.55 Patients with a higher percentage of blood eosinophils,54 or a baseline NLR above the threshold ≥2.760 were at higher risk of both moderate and severe AECOPD. Patients with a lower MPV (≤9fL) had an increased risk of a severe AECOPD.52 Additionally, higher chitotriosidase activity (per 10 Dnmol/h/mL) in combination with ≥1 AECOPD in the previous year, was a predictor of increased risk of both moderate and severe AECOPD.54 Finally, based only on an AUROC value with a confidence interval, lymphocyte count is a predictor of AECOPD,60 with a discriminative ability that is poor (AUROC: 0.60, 95% CI: 0.51–0.68).
Lung Function Test Results
The analysis of lung function test results revealed 10 significant predictors: FEV1% predicted (8/22 models), FVC % predicted (1/2 models), bronchodilator response (BDR) (13/19 models), airway test: area under flow-volume curve (1/1 models), CT-scan: gas trapping percentage (1/1 models), resting breathing instability (1/1 models), COPD GOLD classification (1–4) (5/7 models), 6-minute walking tests (4/12 models), exercise test: five-repetition sit-to-stand test (1/1 models), and exercise-induced oxygen desaturation (1/1 models).
A 1% lower FEV1% predicted increased the likelihood of patients experiencing moderate AECOPD by 1.06%.18 Lower FEV1% predicted also increased the risk of a severe AECOPD per percentage reduction;42 specifically, by 3%18,63 compared to patients with higher FEV1. A lower FEV1% was a statistically significant risk for both moderate and severe AECOPD in four articles,10,54,55,60 two of them specified cut-off values of <55%10 and <50%,60 and two increased risk per percentage lower in FEV1.54,55 A lower FVC% predicted (per 1%) increased the risk of severe AECOPD by 2%.63 Combined bronchodilator response50 and both pre- and post-bronchodilator49 (defined as an increase in either FEV1 and/or FVC by 12% and ≥0.2L) were statistically significant in predicting more frequent moderate and severe AECOPD in patients.49,50 Furthermore, a lower pre-bronchodilator inspiratory capacity was associated with a higher risk of both moderate and severe AECOPD.45
Lower area under the flow-volume curve (<0.17) was a predictor for a higher risk of severe AECOPD.61 Gas trapping on CT scans increased the risk of both moderate and severe AECOPD in one article.17
Resting breathing instability was a predictor of moderate AECOPD, where patients with an increased coefficient of variation for tidal volume had a higher risk of moderate AECOPD.51
A higher COPD GOLD classification (III or IV versus I–II;64 II–IV versus I57) was associated with a higher risk for moderate57,64 severe,64 and both moderate and severe AECOPD.59 Additionally, a higher COPD GOLD category (II versus I, III versus I–II, IV versus I–III) was found to be a predictor of severe AECOPD in another article.43
Patients with a higher compared to those with a lower baseline 6-minute walking distance, predicted a slightly higher risk of moderate AECOPD (+0.04% per meter) within the coming year.18 In contrast, in two articles29,42 the risk of severe AECOPD increased for patients with a lower 6-minute walking work (6MWW) (≤27,000 m·kg),42 unintended stops,42 and distance <350m29 during the 6-minute walking test (6MWT), compared to patients a higher 6MWW,42 no stops,42 and a 6MWT distance >350 m.29
Patients with lower five-repetition sit-to-stand test (≤2),29 and those with a lower exercise-induced oxygen desaturation (≤88%)42 had a higher risk of severe AECOPD compared to those with higher five-repetition sit-to-stand test (>2), and exercise-induced oxygen desaturation (>88%).
Composite Predictor Categories
Lastly, in the composite category, the following three statistically significant predictors were identified: BODE index defined as BMI, airflow obstruction, dyspnea and exercise capacity67 (3/7 models), COPD GOLD classification (A-D, 8/9 models), and composite clinically important deterioration (CID) defined as a decrease in FEV1 of ≥100 mL, an increase of ≥4 units in the SGRQ and the incidence of a moderate and/or moderate/severe AECOPD68 (4/8 models).
Patients with a BODE index score of ≥3 had a higher risk of severe AECOPD,42,46 and for the combination of moderate and severe AECOPD.46
Patients with a higher COPD GOLD classification (GOLD B-D) compared to GOLD A were at a higher risk of severe AECOPD.43,46,56 Also, patients with a COPD GOLD C-D classification compared to GOLD A were at a higher risk for both moderate and severe AECOPD.46 Patients who met the composite CID criteria were at a higher risk of moderate, and severe AECOPD.58
Discussion
In this review, a total of 37 unique predictors of moderate, severe or both moderate and severe AECOPD were defined in the categories patient characteristics, symptoms, biomarkers, lung function tests, and composites across 30 included articles. None of these articles reported on relapse (within 28 days) of AECOPD. Significant predictors among patient characteristics include age, BMI, sex, smoking status, history of AECOPD and daily physical activity. Higher age and lower BMI are associated with worse COPD outcomes,69 thus it is unsurprising that these factors predict AECOPD. Notably, one study18 reported that current smokers had a lower risk of AECOPD compared to former smokers. This finding aligns poorly with existing literature70,71 and guidelines,69 but may be explained by reverse causality as smokers with more severe COPD are more likely to quit.18 A history of AECOPD has been shown to be the best predictor of frequent AECOPD (defined as ≥2 AECOPDs per year),72 as highlighted in the GOLD 2025 report.69 The current review identified in studies with a low risk of bias that patients with a history of at least one AECOPD already had a significantly increased risk of AECOPD.10,18 These findings validate the GOLD approach of using exacerbation history as a predictor of AECOPD. However, the threshold of ≥2 AECOPDs per year may be overly restrictive, potentially delaying timely preventative interventions. It is not surprising that lower daily physical activity showed to be associated with a higher risk of AECOPD53 in this review, since exercise is recommended for COPD management and lowers the risk of acute exacerbations.69 Contrary to COPD GOLD guidelines, one study in this review found that patients with a younger age had an increased risk of a new severe AECOPD within three and six months.63 According to the authors of this study, this was due to the greater COPD disease severity observed in younger individuals within this study.63
Within the category of symptoms, SGRQ score, SGRQ-C score, SGRQ-C domains score: cough and/or sputum, and dyspnea, mMRC scores, cough, and CAT score were all predictors of AECOPD. SGRQ-C score showed to be the most promising predictor, based on the highest relative statistical significance in its ability to predict AECOPD and the best overall risk of bias. Notably, based on the articles in this review, the potential of the SGRQ-C to predict AECOPD extends beyond its total score to its individual domain scores of dyspnea and cough.17,18 In contrast, the mMRC and CAT score demonstrated weaker predictive performance of AECOPD, with a higher frequency of non-significant models. These findings suggest that they have limited utility as predictive tools. Additionally, the statistical significance reported for the mMRC is derived from studies with a high risk of bias, whereas the studies reporting on the CAT have varying levels of bias. Consequently, the routine use of mMRC and CAT as predictor of AECOPD should be reconsidered. The original SGRQ is not routinely used in clinical practice mostly due to its length and complexity.16 Both SGRQ and SGRQ-C are predictive, though standard assessment through the shorter version (SGRQ-C) could provide a more user friendly and reliable alternative.
Several biomarkers predicted an increased risk of AECOPD, including higher fibrinogen levels, higher blood eosinophils percentage, higher chitotriosidase levels, lower sarcopenia index, lower creatinine/cystatin C levels, and low mean platelet volume. Higher fibrinogen levels seem the most promising biomarker based on the high relative frequency of statistical significant models and the accompanied low risk of bias.18,62 Higher fibrinogen set at a cut-off value of ≥3.5g/L has been proposed to identify patients at elevated risk.62 These findings are in line with previous reviews as they have already shown similar promising predictive ability with a threshold of 3.5g/L.22,73 The assessment of fibrinogen in clinical practice could therefore be a next logical step for predicting patients at risk of AECOPD. Whereas blood eosinophils have been assessed in multiple studies,52,54,60 only one found statistical significance in its predictive ability of AECOPD.54 The GOLD 2025 report suggests a threshold of ≥300 µL for identifying patients at risk of AECOPD and who are more likely to benefit from preventative treatment with inhaled corticosteroids.69 However, there is inconsistency across studies on whether blood eosinophils are able to predict acute exacerbations74,75 and which threshold is appropriate.23 Hence, there is insufficient evidence to recommend eosinophils as individual predictors of AECOPD. Since all biomarkers, except for fibrinogen, were statistically significant in only one study with either moderate or high risk of bias, additional research is needed. Future studies should establish clear thresholds and validate the predictive ability of biomarkers before these can be further implemented in clinical practice.
In the category of lung function test results, higher COPD GOLD classification (1–4), lower FEV1% predicted, lower FVC% predicted, lower bronchodilator response, lower area under the flow-volume curve, gas trapping, resting breathing instability, lower 6-minute walking test results, and lower exercise-induced oxygen desaturation are all statistically significant predictors of AECOPD. All the included articles that reported on the COPD GOLD classification (1–4), although with varying risks of bias, found statistical significance in its ability to predict AECOPD. This is not an unexpected finding, since the former COPD GOLD classification (1–4) is based on the FEV1,69 and the predictor FEV1% predicted also showed to be an independent predictor of AECOPD, albeit in studies with varying risk of bias. A noteworthy finding was that one study with a low risk of bias18 identified a higher six-minute walk distance as a risk predictor for moderate AECOPD, which might be due to possible confounding factors. All other studies, with worse overall risk of bias, showed that a poorer six-minute walk or exercise test performance was associated with increased AECOPD risk. Exercise tests such as the 6-minute walking tests, exercise-induced oxygen desaturation, and the five-repetition sit-to-stand test showed that patients with a better test result had a better outcome (ie lower AECOPD incidence) than those with worse test results. Since impaired physical function has been associated with worse prognosis in COPD,76 it is not surprising that worse results on exercise related tests are predictive for a higher risk of AECOPD.
Of the composite predictors, elevated BODE index scores, COPD GOLD classification (A-D) as a composite measure, and Clinically Important Deterioration were all statistically significant predictors of AECOPD. As expected, the COPD GOLD classification (A-D)—which includes both lung function tests and symptom-based questionnaires (eg CAT, mMRC, clinical COPD questionnaire)—was better at predicting a severe AECOPD, and combined moderate and severe AECOPD, than the COPD GOLD classification based on solely lung function. Since the components of COPD GOLD 1–4 classification (FEV1, mMRC, and CAT) were all independently predictors of AECOPD, it is reasonable to expect that combining these predictors would improve its predictive ability. Due to the complexity and heterogeneity of COPD phenotypes, combining multiple categories of predictors (into composites) may significantly enhance the accuracy of AECOPD risk prediction. COPD is increasingly recognized as a systemic disease, with extrapulmonary manifestations such as cardiovascular comorbidities, metabolic dysfunction, skeletal muscle wasting, and systemic inflammation contributing to its clinical course and prognosis. These systemic features vary across phenotypes and influence both the frequency and severity of acute exacerbations.69 In this context, integrating the most promising predictors of AECOPD from the five categories (history of acute exacerbations, SGRQ-C score, fibrinogen levels, COPD GOLD 2–4, and COPD GOLD B-D classification) may enhance both short- and long-term risk prediction. Accurately predicting AECOPD is crucial for effective disease management. This involves two key types of predictors: long-term predictors that indicate a patient’s general susceptibility to AECOPD, and short-term predictors that signal a likely AECOPD in the near future. Long-term predictors like history of acute exacerbation identify patients at risk of AECOPD and provide valuable insight into those who require close monitoring and optimized clinical management (eg change in pharmacological therapy, a self-management program or pulmonary rehabilitation program). Timely identifying short-term predictors of AECOPD, such as biomarkers (elevated fibrinogen levels) or symptoms (increased cough), is relevant for early deterioration intervention. By recognizing and monitoring both short- and long-term predictors of AECOPD management and prevention of AECOPD improves, hospitalizations reduce, and ultimately healthcare utilization and societal burden reduce.77 Telemonitoring, a rapidly evolving technology, is a promising tool for identifying more short-term predictors. It allows for personalized tracking of symptoms and physiological changes in real-time such as home-based lung function tests and biomarkers.78,79
A key strength of this systematic review is the assessment of a broad range of predictor categories. Evaluating multiple possible predictors or risk factors provides a clearer picture of what might be causing an AECOPD. This review confirmed known predictors and systematically reported the relative frequency of statistical significance of each predictor and the risk of bias in the studies from which these predictors were derived. Additionally, identifying predictors for moderate, severe AECOPD, and relapse of AECOPD ensures that the main types of AECOPD, which result in the highest loss in quality of life and healthcare costs,4 are considered.
However, the review is not without limitations. Although we aimed to provide an overview of the predictors of AECOPD, it does not encompass all potential predictors. Only predictors categorized as biomarkers, symptoms, lung function test results, patient characteristics or composite scores were considered. Beyond these categories, additional predictors such as meteorological factors have been studied, but their impact on COPD is not fully clear.69,80–82 Additionally, articles or analyses that included data from never-smokers were excluded, as smoking-related COPD is the most prevalent form of the disease. Combining predictors from smoking-related and non-smoking-related COPD might not be ideal because the underlying mechanisms and risk factors can differ significantly. There were inconsistencies in the definitions for moderate and severe acute exacerbations, as well as the timeframes for relapse of AECOPD, leading to the exclusion of certain articles or outcomes in this review. These differences in definitions may impact comparability of results across studies, and using the standardized definitions should be considered in future research.
Since only about a third of the included studies in this review had a low risk of bias, future studies should aim to minimize and transparently account for bias. Clearly defining and reporting the study design, will improve methodological quality, hence, prevent concerns about bias.83 Additionally, integrating composites of the analyzed categories, rather than relying on single predictors, may enhance predictive accuracy and improve risk prediction assessment for AECOPD. Notably, among all included articles, only a few predictors demonstrated statistical significance in more than one study. Therefore, further validation research is necessary to confirm these single-study predictors, prior to their integration into clinical practice.
Conclusion
The most promising predictors of AECOPD within the five categories are history of acute exacerbations, SGRQ-C score, fibrinogen levels, COPD GOLD 2–4, and COPD GOLD B-D classification, based on the highest relative statistical significance combined with low overall risk of bias. By combining multiple predictors into composites, the risk prediction of AECOPD may be enhanced. Future research should focus on these composite risk scores and explore the roles of both long- and short-term predictors in guiding COPD management. However, methodological inconsistencies underscore the need for standardized definitions of moderate, severe or relapse of AECOPD and further validation of predictors in studies with a low risk of bias.
Acknowledgments
The authors declare that there are no relevant material or financial interests that relate to the described research and the finding in this work. An abstract was presented at the 2023 ERS International Congress as a poster presentation including preliminary findings of the work presented in this paper. The poster’s abstract was published in ‘Poster Abstracts’ in the European Respiratory Journal 2023: http://publications.ersnet.org/content/erj/62/suppl67/pa3641 and published at the website of the University of Twente https://research.utwente.nl/en/publications/predictors-of-acute-exacerbations-in-copd-a-systematic-review
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the European Union’s Horizon 2020 research and innovation program (grant number 965315).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gold. Global strategy for prevention, diagnosis and management of COPD: 2024 report. global initiative for chronic obstructive lung disease – GOLD2024. p. 0–10;33;6–7;99–115;40–42;86–26.
2. Ko FW, Chan KP, Hui DS, et al. Acute exacerbation of COPD. Respirology. 2016;21(7):1152–1165. doi:10.1111/resp.12780
3. Hillas G, Perlikos F, Tzanakis N. Acute exacerbation of COPD: is it the “stroke of the lungs”? Int J Chron Obstruct Pulmon Dis. 2016;11:1579–1586. doi:10.2147/COPD.S106160
4. COPD GGf. Global Strategy for Prevention, Diagnosis and Management of COPD. Global Initiative for Chronic Obstructive Lung Disease –; 2020.
5. Kim V, Aaron SD. What is a COPD exacerbation? Current definitions, pitfalls, challenges and opportunities for improvement. Eur Respir J. 2018;52(5):1801261. doi:10.1183/13993003.01261-2018
6. Ruan H, Zhang H, Wang J, Zhao H, Han W, Li J. Readmission rate for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Med. 2023;206:107090. doi:10.1016/j.rmed.2022.107090
7. Halpin DM, Decramer M, Celli B, Kesten S, Leimer I, Tashkin DP. Risk of nonlower respiratory serious adverse events following COPD exacerbations in the 4-year UPLIFT(R) trial. Lung. 2011;189(4):261–268. doi:10.1007/s00408-011-9301-8
8. Kessler R, Stahl E, Vogelmeier C, et al. Patient understanding, detection, and experience of COPD exacerbations: an observational, interview-based study. Chest. 2006;130(1):133–142. doi:10.1378/chest.130.1.133
9. Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786–796. doi:10.1016/S0140-6736(07)61382-8
10. Nuñez A, Marras V, Harlander M, et al. Clinical and spirometric variables are better predictors of COPD exacerbations than routine blood biomarkers. Respir Med. 2020;171:106091. doi:10.1016/j.rmed.2020.106091
11. Hunter LC, Lee RJ, Butcher I, et al. Patient characteristics associated with risk of first hospital admission and readmission for acute exacerbation of chronic obstructive pulmonary disease (COPD) following primary care COPD diagnosis: a cohort study using linked electronic patient records. BMJ Open. 2016;6(1):e009121. doi:10.1136/bmjopen-2015-009121
12. Suzuki M, Makita H, Ito YM, Nagai K, Konno S, Nishimura M. Clinical features and determinants of COPD exacerbation in the Hokkaido COPD cohort study. Eur Respir J. 2014;43(5):1289. doi:10.1183/09031936.00110213
13. Asai N, Ohkuni Y, Ohashi W, Kaneko N. Modified MRC assessment and FEV1.0 can predict frequent acute exacerbation of COPD: an observational prospective cohort study at a single-center in Japan. Respir Med. 2023;212:107218. doi:10.1016/j.rmed.2023.107218
14. Jo YS, Yoon HI, Kim DK, Yoo C-G, Lee C-H. Comparison of COPD assessment test and clinical COPD Questionnaire to predict the risk of exacerbation. Int J Chron Obstruct Pulmon Dis. 2017;13:101–107. doi:10.2147/COPD.S149805
15. Kim V, Zhao H, Regan E, et al. The st. george’s respiratory questionnaire definition of chronic bronchitis may be a better predictor of COPD exacerbations compared with the classic definition. Chest. 2019;156(4):685–695. doi:10.1016/j.chest.2019.03.041
16. Zhang J, Chen F, Wang Y, Chen Y. Early detection and prediction of acute exacerbation of chronic obstructive pulmonary disease. Chin Med J Pulm Crit Care Med. 2023;1(2):102–107. doi:10.1016/j.pccm.2023.04.004
17. Busch R, Han MK, Bowler RP, et al. Risk factors for COPD exacerbations in inhaled medication users: the COPDGene study biannual longitudinal follow-up prospective cohort. BMC Pulm Med. 2016;16(1):28. doi:10.1186/s12890-016-0191-7
18. Exuzides A, Colby C, Briggs AH, et al. Statistical modeling of disease progression for chronic obstructive pulmonary disease using data from the ECLIPSE study. Med Decis Making. 2017;37(4):453–468. doi:10.1177/0272989X15610781
19. Bafadhel M, Pavord ID, Russell REK. Eosinophils in COPD: just another biomarker? Lancet Respir Med. 2017;5(9):747–759. doi:10.1016/S2213-2600(17)30217-5
20. Pantazopoulos I, Magounaki K, Kotsiou O, et al. Incorporating biomarkers in COPD management: the research keeps going. J Pers Med. 2022;12(3):379. doi:10.3390/jpm12030379
21. Sin DD, Hollander Z, DeMarco ML, McManus BM, Ng RT. Biomarker development for chronic obstructive pulmonary disease. from discovery to clinical implementation. Am J Respir Crit Care Med. 2015;192(10):1162–1170. doi:10.1164/rccm.201505-0871PP
22. Waeijen-Smit K, DiGiandomenico A, Bonnell J, et al. Early diagnostic BioMARKers in exacerbations of chronic obstructive pulmonary disease: protocol of the exploratory, prospective, longitudinal, single-centre, observational MARKED study. BMJ Open. 2023;13(3):e068787. doi:10.1136/bmjopen-2022-068787
23. Mathioudakis AG, Janssens W, Sivapalan P, et al. Acute exacerbations of chronic obstructive pulmonary disease: in search of diagnostic biomarkers and treatable traits. Thorax. 2020;75(6):520–527. doi:10.1136/thoraxjnl-2019-214484
24. Hurst JR, Donaldson GC, Perera WR, et al. Use of plasma biomarkers at exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006;174(8):867–874. doi:10.1164/rccm.200604-506OC
25. Bhatt SP. Predicting chronic obstructive pulmonary disease exacerbations: when the past does not inform the future. Ann Am Thorac Soc. 2024;21(3):382–383. doi:10.1513/AnnalsATS.202311-934ED
26. Santos-de-Araújo AD, da Luz Goulart C, Marinho RS, et al. The six-minute step test can predict COPD exacerbations: a 36-month follow-up study. Sci Rep. 2024;14(1):3649. doi:10.1038/s41598-024-54338-9
27. Morakami FK, Morita AA, Bisca GW, et al. Can the six-minute walk distance predict the occurrence of acute exacerbations of COPD in patients in Brazil? J Bras Pneumol. 2017;43(4):280–284. doi:10.1590/S1806-37562016000000197
28. Spruit MA, Polkey MI, Celli B, et al. Predicting outcomes from 6-minute walk distance in chronic obstructive pulmonary disease. J Am Med Dir Assoc. 2012;13(3):291–297. doi:10.1016/j.jamda.2011.06.009
29. Medina-Mirapeix F, Bernabeu-Mora R, Valera-Novella E, Gacto-Sanchez M, Bernabeu-Mora M, Sanchez-Martinez MP. The five-repetition sit-to-stand test is a predictive factor of severe exacerbations in COPD. Ther Adv Chronic Dis. 2021;12:2040622320986718. doi:10.1177/2040622320986718
30. COMMITTEE G. global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2021).
31. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
32. Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. doi:10.1186/s13047-020-00383-2
33. Agency EM: biomarker. Available from: https://www.ema.europa.eu/en/glossary/biomarker.
34. Institute NC: NCI Dictionary of Cancer Terms. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms.
35. Burge S, Wedzicha JA. COPD exacerbations: definitions and classifications. Eur Respir J. 2003;21(41 suppl):46s. doi:10.1183/09031936.03.00078002
36. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. 2010;5(9):1315–1316. doi:10.1097/JTO.0b013e3181ec173d
37. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
38. Covidence: better systematic review management https://www.covidence.org.
39. Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158(4):280–286. doi:10.7326/0003-4819-158-4-201302190-00009
40. Abe Y, Suzuki M, Makita H, et al. One-year clinically important deterioration and long-term clinical course in Japanese patients with COPD: a multicenter observational cohort study. BMC Pulm Med. 2021;21(1):159. doi:10.1186/s12890-021-01510-w
41. Amado CA, Garcia-Unzueta MT, Lavin BA, et al. the ratio serum creatinine/serum cystatin c (a surrogate marker of muscle mass) as a predictor of hospitalization in chronic obstructive pulmonary disease outpatients. Respiration. 2019;97(4):302–309. doi:10.1159/000494296
42. Andrianopoulos V, Wouters EF, Pinto-Plata VM, et al. Prognostic value of variables derived from the six-minute walk test in patients with COPD: results from the ECLIPSE study. Respir Med. 2015;109(9):1138–1146. doi:10.1016/j.rmed.2015.06.013
43. Brusse-Keizer M, Klatte M, Zuur-Telgen M, Koehorst-Ter Huurne K, van der Palen J, VanderValk P. Comparing the 2007 and 2011 GOLD classifications as predictors of all-cause mortality and morbidity in COPD. COPD. 2017;14(1):7–14. doi:10.1080/15412555.2016.1206875
44. Burkes RM, Ceppe AS, Doerschuk CM, et al. Associations among 25-hydroxyvitamin d levels, lung function, and exacerbation outcomes in COPD: an analysis of the spiromics cohort. Chest. 2020;157(4):856–865. doi:10.1016/j.chest.2019.11.047
45. Celli BR, Decramer M, Lystig T, Kesten S, Tashkin DP. Longitudinal inspiratory capacity changes in chronic obstructive pulmonary disease. Respir Res. 2012;13(1):66. doi:10.1186/1465-9921-13-66
46. Chen CZ, Ou CY, Yu CH, Yang SC, Chang HY, Hsiue TR. Comparison of global initiative for chronic obstructive pulmonary disease 2013 classification and body mass index, airflow obstruction, dyspnea, and exacerbations index in predicting mortality and exacerbations in elderly adults with chronic obstructive pulmonary disease. J Am Geriatr Soc. 2015;63(2):244–250. doi:10.1111/jgs.13258
47. Cushen B, McCormack N, Hennigan K, Sulaiman I, Costello RW, Deering B. A pilot study to monitor changes in spirometry and lung volume, following an exacerbation of Chronic Obstructive Pulmonary Disease (COPD), as part of a supported discharge program. Respir Med. 2016;119:55–62. doi:10.1016/j.rmed.2016.08.019
48. Fernandez-Granero MA, Sanchez-Morillo D, Leon-Jimenez A. computerised analysis of telemonitored respiratory sounds for predicting acute exacerbations of COPD. Sensors. 2015;15(10):26978–26996. doi:10.3390/s151026978
49. Fortis S, Eberlein M, Georgopoulos D, Comellas AP. Predictive value of prebronchodilator and postbronchodilator spirometry for COPD features and outcomes. BMJ Open Respir Res. 2017;4(1):e000213. doi:10.1136/bmjresp-2017-000213
50. Fortis S, Comellas A, Make BJ, et al. Combined forced expiratory volume in 1 second and forced vital capacity bronchodilator response, exacerbations, and mortality in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2019;16(7):826–835. doi:10.1513/AnnalsATS.201809-601OC
51. Fujita Y, Yamauchi M, Yoshikawa M, et al. Resting breathing instability during wakefulness as a predictor of clinical outcome in COPD. Respir Care. 2021;66(9):1477–1484. doi:10.4187/respcare.08877
52. Garcia-Pachon E, Baeza-Martinez C, Ruiz-Alcaraz S, Grau-Delgado J. Prediction of three-month readmission based on haematological parameters in patients with severe COPD exacerbation. Adv Respir Med. 2021;89(5):501–504. doi:10.5603/ARM.a2021.0076
53. Garcia-Rio F, Rojo B, Casitas R, et al. Prognostic value of the objective measurement of daily physical activity in patients with COPD. Chest. 2012;142(2):338–346. doi:10.1378/chest.11-2014
54. Harlander M, Lestan D, Turel M. Chitotriosidase activity in plasma and COPD exacerbations. Lung. 2020;198(2):299–306. doi:10.1007/s00408-020-00331-8
55. Hirai K, Tanaka A, Homma T, et al. Serum creatinine/cystatin C ratio as a surrogate marker for sarcopenia in patients with chronic obstructive pulmonary disease. Clin Nutr. 2021;40(3):1274–1280. doi:10.1016/j.clnu.2020.08.010
56. Lee SJ, Yun SS, Ju S, et al. Validity of the GOLD 2017 classification in the prediction of mortality and respiratory hospitalization in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:911–919. doi:10.2147/COPD.S191362
57. Natori H, Kawayama T, Suetomo M, et al. Evaluation of the modified medical research council dyspnea scale for predicting hospitalization and exacerbation in japanese patients with chronic obstructive pulmonary disease. Intern Med. 2016;55(1):15–24. doi:10.2169/internalmedicine.55.4490
58. Naya IP, Tombs L, Muellerova H, Compton C, Jones PW. Long-term outcomes following first short-term clinically important deterioration in COPD. Respir Res. 2018;19(1):222. doi:10.1186/s12931-018-0928-3
59. Numata TA, Matsui J, Okuda Y, et al. Risk factor of moderate-to-severe exacerbation in patients with chronic obstructive pulmonary disease. Jikeikai Medical Journal. 2021;68(4):99–109.
60. Sakurai K, Chubachi S, Irie H, et al. Clinical utility of blood neutrophil-lymphocyte ratio in Japanese COPD patients. BMC Pulm Med. 2018;18(1):65. doi:10.1186/s12890-018-0639-z
61. Satici C, Demirkol MA, Arpinar Yigitbas B, Erinc A, Kosar AF. Area under flow-volume loop may predict severe exacerbation in COPD patients with high grade of dyspnea. Respir Physiol Neurobiol. 2021;294:103771. doi:10.1016/j.resp.2021.103771
62. Singh D, Criner GJ, Dransfield MT, et al. InforMing the PAthway of COPD Treatment (IMPACT) trial: fibrinogen levels predict risk of moderate or severe exacerbations. Respir Res. 2021;22(1):130. doi:10.1186/s12931-021-01706-y
63. Soltani A, Reid D, Wills K, Walters EH. Prospective outcomes in patients with acute exacerbations of chronic obstructive pulmonary disease presenting to hospital: a generalisable clinical audit. Intern Med J. 2015;45(9):925–933. doi:10.1111/imj.12816
64. Suetomo M, Kawayama T, Kinoshita T, et al. COPD assessment tests scores are associated with exacerbated chronic obstructive pulmonary disease in Japanese patients. Respir Investig. 2014;52(5):288–295. doi:10.1016/j.resinv.2014.04.004
65. Wilke S, Jones PW, Mullerova H, et al. One-year change in health status and subsequent outcomes in COPD. Thorax. 2015;70(5):420–425. doi:10.1136/thoraxjnl-2014-205697
66. American Thoracic Society A: st. George’s Respiratory Questionnaire (SGRQ). Available from: https://www.thoracic.org/members/assemblies/assemblies/srn/questionaires/sgrq.php#:~:text=Part%201%20%3A%20Symptoms%20component%20(frequency,refer%20to%20current%20state%20as.
67. Corlateanu A, Plahotniuc A, Corlateanu O, et al. Multidimensional indices in the assessment of chronic obstructive pulmonary disease. Respir Med. 2021;185:106519. doi:10.1016/j.rmed.2021.106519
68. Singh D, Maleki-Yazdi MR, Tombs L, Iqbal A, Fahy WA, Naya I. Prevention of clinically important deteriorations in COPD with umeclidinium/vilanterol. Int J Chron Obstruct Pulmon Dis. 2016;11:1413–1424. doi:10.2147/COPD.S101612
69. GOLD. Global strategy for prevention, diagnosis and management of COPD: 2025 Report. 2025 GOLD report: global initiative for chronic obstructive lung disease GOLD; 2025. p. 36–7;44;50–1;64–6;86–7;109–23.
70. Li X, Wu Z, Xue M, Du W. Smoking status affects clinical characteristics and disease course of acute exacerbation of chronic obstructive pulmonary disease: a prospectively observational study. Chron Respir Dis. 2020;17:1479973120916184. doi:10.1177/1479973120916184
71. Wang G, Ma A, Zhang L, et al. Acute exacerbations of chronic obstructive pulmonary disease in a cohort of Chinese never smokers goes along with decreased risks of recurrent acute exacerbation, emphysema and comorbidity of lung cancer as well as decreased levels of circulating eosinophils and basophils. Front Med Lausanne. 2022;9:907893. doi:10.3389/fmed.2022.907893
72. Whittaker H, Rubino A, Mullerova H, et al. Frequency and severity of exacerbations of COPD associated with future risk of exacerbations and mortality: a uk routine health care data study. Int J Chron Obstruct Pulmon Dis. 2022;17:427–437. doi:10.2147/COPD.S346591
73. Duvoix A, Dickens J, Haq I, et al. Blood fibrinogen as a biomarker of chronic obstructive pulmonary disease. Thorax. 2013;68(7):670–676. doi:10.1136/thoraxjnl-2012-201871
74. Singh D, Wedzicha JA, Siddiqui S, et al. Blood eosinophils as a biomarker of future COPD exacerbation risk: pooled data from 11 clinical trials. Respir Res. 2020;21(1):240. doi:10.1186/s12931-020-01482-1
75. Chen F, Yang M, Wang H, Liu L, Shen Y, Chen L. High blood eosinophils predict the risk of COPD exacerbation: a systematic review and meta-analysis. PLoS One. 2024;19(10):e0302318. doi:10.1371/journal.pone.0302318
76. Vaes AW, Burtin C, Casaburi R, et al. Prevalence and prognostic importance of exercise limitation and physical inactivity in COPD. Breathe. 2024;20(2):230179. doi:10.1183/20734735.0179-2023
77. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
78. Lenferink A, Brusse-Keizer MGJ, van der Palen J, Effing TW. Personalizing self-management interventions in COPD - looking beyond one-size-fits-all. Int J Chron Obstruct Pulmon Dis. 2025;20:65–68. doi:10.2147/COPD.S511278
79. Lu JW, Wang Y, Sun Y, et al. Effectiveness of telemonitoring for reducing exacerbation occurrence in COPD patients with past exacerbation history: a systematic review and meta-analysis. Front Med Lausanne. 2021;8:720019. doi:10.3389/fmed.2021.720019
80. Huh JY, Hong J, Han DW, Park YJ, Jung J, Lee SW. The Impact of air pollutants and meteorological factors on chronic obstructive pulmonary disease exacerbations: a nationwide study. Ann Am Thorac Soc. 2022;19(2):214–226. doi:10.1513/AnnalsATS.202103-298OC
81. Marovics G, Pozsgai E, Nemeth B, Czigany S, Nemeth-Simon S, Giran J. How vulnerable are patients with COPD to weather extremities?-a pilot study from Hungary. Healthcare. 2022;10(11). doi:10.3390/healthcare10112309
82. Jenkins CR, Celli B, Anderson JA, et al. Seasonality and determinants of moderate and severe COPD exacerbations in the TORCH study. Eur Respir J. 2011;39(1):38–45. doi:10.1183/09031936.00194610
83. Pannucci CJ, Wilkins EG. Identifying and avoiding bias in research. Plast Reconstr Surg. 2010;126(2):619–625. doi:10.1097/PRS.0b013e3181de24bc
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Patterns, Socioeconomic Status and Clinical Burden in Mild COPD: A Swedish Real-World, Retrospective Cohort Study, the ARCTIC Study
Larsson K, Lisspers K, Ställberg B, Johansson G, Gutzwiller FS, Mezzi K, Bjerregaard BK, Jorgensen L, Koo H, Janson C
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1409-1421
Published Date: 21 June 2022
A Social Return on Investment Analysis of Improving the Management of Chronic Obstructive Pulmonary Disease Within the Spanish National Healthcare System
Merino M, Martín Lorenzo T, Maravilla-Herrera P, Ancochea J, Gómez Sáenz JT, Hass N, Molina J, Peces-Barba G, Trapero-Bertran M, Trigueros Carrero JA, Hidalgo-Vega Á
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1431-1442
Published Date: 21 June 2022
A Prediction Scoring Model for the Effect of Withdrawal or Addition of Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease
Lee JH, Kim S, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:113-127
Published Date: 15 February 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Real-World Disease Burden and Healthcare Resource Utilization Among Patients with COPD and Asthma Using Triple Therapy (FF/UMEC/VI) in the United States
Igboekwe E, Verma S, Paczkowski R
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:281-296
Published Date: 25 January 2024