Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Predictors and Consequences of Delayed Insulin Initiation: A 20-year Retrospective Cohort Study on Diabetes Complications in Southern Thailand
Authors Wang-ae A, Limumpornpetch P, Saelim P, Choomalee K, Sornsenee P ![]()
Received 24 November 2025
Accepted for publication 5 February 2026
Published 21 February 2026 Volume 2026:19 575632
DOI https://doi.org/10.2147/DMSO.S575632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hillary Keenan
Aina Wang-ae,1 Padiporn Limumpornpetch,2 Prapatsorn Saelim,3 Kittisakdi Choomalee,1 Phoomjai Sornsenee1
1Department of Family Medicine and Preventive Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand; 2Division of Endocrinology and Metabolism, Department of Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand; 3Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Correspondence: Phoomjai Sornsenee, Department of Family Medicine and Preventive Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand, Tel +66954204713, Fax +6674451333, Email [email protected]; [email protected]
Purpose: This study aimed to investigate the prevalence, predictors, and clinical consequences of delayed insulin initiation in patients with type-2 diabetes mellitus in a tertiary care setting.
Patients and Methods: A retrospective cohort study was conducted in 973 adults with type-2 diabetes mellitus with initiated insulin therapy between January 1, 2004 and December 31, 2023 at a university hospital in southern Thailand. Delayed insulin initiation was defined as insulin initiation ≥ 6 months after documented treatment failure (glycated hemoglobin ≥ 7% on oral agents), reflecting clinical inertia. Logistic regression was used to identify the predictors of delay. Time-to-event analyses and restricted mean survival time were used to compare diabetes-related complications between groups.
Results: Delayed insulin initiation occurred in 35% of the patients. Independent predictors included higher body mass index, longer duration of diabetes, biguanide use, and diuretic use, whereas dipeptidyl peptidase-4 inhibitor use was associated with timely initiation. Although no significant differences were observed in overall macrovascular or microvascular complication rates, delayed initiation was significantly associated with increased amputation risk (hazard ratio: 2.33; 95% confidence interval: 1.07– 5.07) and earlier onset of microvascular complications within the 10– 15-year window (restricted mean survival time difference: − 0.56 years, p=0.043).
Conclusion: Delayed insulin initiation is common and linked to identifiable clinical characteristics and adverse outcomes, including increased risk of amputation and earlier microvascular complications. Prioritizing timely insulin initiation is essential to reduce long-term complications and preserve limb health, particularly in high-risk individuals.
Keywords: clinical inertia, delayed insulin initiation, diabetes complications, retrospective cohort study, type 2 diabetes mellitus
Introduction
Diabetes mellitus is one of the most prevalent and growing non-communicable diseases globally, posing a critical public health challenge. In 2019, the global prevalence of diabetes among adults aged 20–79 years was estimated to be 9.3% (463 million people) and is projected to increase to 10.2% (578 million) by 2030 and 10.9% (700 million) by 2045 if no substantial interventions are implemented.1 Thailand faces a similarly concerning trend, with the Ministry of Public Health reporting a prevalence of 11.6% in 2021 among individuals aged ≥15 years, which is higher than the global average. An important goal in managing type-2 diabetes mellitus (T2DM) is preventing complications through timely and adequate glycemic control. However, many patients fail to achieve their glycemic targets because of a phenomenon known as clinical inertia.
Clinical inertia is defined as failure to initiate or intensify therapy despite suboptimal glycemic control. This issue is multifactorial, involving both patient-related barriers (such as limited health literacy, psychological resistance, or adherence challenges) and system-level factors such as provider hesitancy, time constraints, and limited healthcare infrastructure.2,3 Globally, clinical inertia affects a significant proportion of patients with T2DM, with prevalence rates of 60.6%, 45.6%, and 68.4% in the United States, United Kingdom, and Thailand, respectively.4
Insulin therapy is a cornerstone of diabetes management for individuals who do not achieve adequate glycemic control with oral hypoglycemic agents or have contraindications to their use. Timely initiation of insulin therapy reduces hyperglycemia and mitigates long-term complications. However, initiation is often delayed in routine clinical practice. For instance, a study in the United States found that only 40.7% of patients with poor glycemic control initiated insulin therapy within 6 months of indication.5 Similar delays have been reported in other regions including the United Kingdom and East Asia. A large population-based study in the United Kingdom found that many patients experienced substantial delays after oral therapy failure, often extending for several years, despite existing complications.6 In Southeast China, delayed insulin initiation was associated with significantly lower odds of achieving glycated hemoglobin (HbA1c) levels <7%, compared with timely initiation,7 whereas a Korean prospective study identified both patient- and physician-related factors contributing to therapeutic inertia.8 Prolonged hyperglycemia is associated with an increased risk of microvascular and macrovascular complications. Studies have linked clinical inertia to adverse outcomes, including an increased risk of complications such as diabetic nephropathy.9 Moreover, early attainment of glycemic targets has been associated with improved long-term durability of control and a reduced risk of complications.10 However, although prior studies have examined the timing of insulin initiation, few have assessed its real-world clinical outcomes using survival analysis, particularly in low- and middle-income countries.
Therefore, in this study, we aimed to examine the time from treatment indication to insulin initiation and its association with the occurrence of diabetes-related complications. In addition, this study investigated the prevalence and duration of delayed insulin initiation among patients with T2DM, explored the clinical factors associated with such delays, and quantified their impact through a retrospective time-to-event analysis in a real-world cohort. These insights may support timely therapeutic interventions and inform strategies for improving long-term diabetes management.
Materials and Methods
Study Design and Setting
This retrospective cohort study was conducted at Songklanagarind Hospital, a tertiary care center in southern Thailand. The study included adult patients with T2DM with initiated insulin therapy between January 1, 2004 and December 31, 2023. Data were retrieved from the electronic medical records of the hospital. The research protocol was approved by the Human Research Ethics Committee of the Faculty of Medicine, Prince of Songkla University (REC 67–229-9-4), a duly constituted ethics committee in accordance with institutional guidelines. The study was conducted in compliance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study.
Study Population
Eligible participants were adults (aged ≥18 years) diagnosed with T2DM who had a recorded HbA1c level ≥7% prior to insulin initiation. Patients were excluded if they had (1) diabetes types other than T2DM, (2) insulin use during pregnancy, (3) insulin use for <6 months, (4) advanced-stage terminal illnesses (such as advanced cancer, chronic obstructive pulmonary disease, or end-stage organ disease), (5) autoimmune diseases, or (6) long-term systemic steroid use (>3 months).
Data Collection and Variables
Demographic and clinical data were collected from electronic medical records and included age, sex, body mass index (BMI), type of healthcare coverage, religion, and clinical setting (such as endocrine or primary care). Additional clinical variables included baseline HbA1c level, duration of diabetes, and selected comorbidities, such as hypertension, dyslipidemia, and chronic kidney disease (CKD), as well as smoking status. Data on the initial insulin dose and prior use of medications, specifically biguanides, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, sodium-glucose cotransporter-2 (SGLT2) inhibitors, angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs), and diuretics, were also recorded.
For the purposes of this study, “delayed insulin initiation” is operationally defined as “clinical inertia”, referring to the failure to escalate treatment when oral antidiabetic agents are no longer sufficient to maintain glycemic control. This is defined as insulin initiation occurring ≥6 months after a documented HbA1c level ≥7%. Patients were categorized into two groups based on the time interval from treatment failure to insulin initiation: the no-inertia (<180 days) and inertia (≥180 days) groups.
The primary outcome was the first documented occurrence of macrovascular or microvascular complications. Macrovascular outcomes included myocardial infarction, heart failure, stroke, peripheral artery disease, and lower-limb amputation, whereas microvascular outcomes included diabetic retinopathy, nephropathy, and neuropathy. These outcomes were identified through physician-documented diagnoses and confirmed using the International Classification of Diseases, 10th Revision codes. All clinical diagnoses and their timing were manually verified by the research team through a review of both structured codes and physician documentation. Patients were followed up from the date of insulin initiation until the first recorded diabetes-related complication, death, or the end of the follow-up period (on December 31, 2024).
Statistical Analysis
All statistical analyses were performed using R software (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were used to summarize the baseline characteristics. Continuous variables are reported as mean with standard deviation or median with interquartile range and categorical variables as frequency and percentage. Comparisons between groups were conducted using Student’s t-test or Wilcoxon rank-sum test for continuous variables and chi-squared or Fisher’s exact test for categorical variables. Normality was assessed as appropriate using distributional inspection (histograms and Q–Q plots) and the Shapiro–Wilk test. Multivariable logistic regression was performed to identify the factors associated with clinical inertia, with the results presented as adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Time-to-event analyses were conducted using Kaplan–Meier survival curves and compared using Log rank test. Cox proportional hazards regression models were used to assess the association between delayed insulin initiation and the risk of diabetes-related complications, reporting hazard ratios (HRs) with 95% CIs. Statistical significance was defined as a two-sided p-value <0.05. Restricted mean survival time (RMST) analysis was also performed to compare groups within the prespecified 10–15-year window (τ = 5 years). Statistical significance was defined as a two-sided p-value <0.05.
Results
Baseline Characteristics
Among the 1,886 patients reviewed, 973 met the inclusion criteria. Table 1 summarizes their baseline characteristics; their mean age was 61.8 years, 52.3% were women, and their median BMI was 25.7 kg/m2. The median duration of diabetes was 7.25 years, and the median HbA1c level prior to insulin initiation was 9.6%. Overall, 35% of patients (n=337) had delayed insulin initiation (≥6 months), whereas 65% (n=636) were initiated within 6 months. Patients in the inertia group had significantly higher BMI (26.4 vs 25.4 kg/m2, p=0.002) and longer duration of diabetes (7.62 vs 7.02 years, p=0.009), compared with those in the no-inertia group. Baseline HbA1c level and age were similar between the groups. CKD was more common in the no-inertia group than in the inertia group (36.9% vs 29.4%, p=0.022), particularly at stage ≥IV (11% vs 3%, p<0.001). Other comorbidities, including hypertension, dyslipidemia, neuropathy, and retinopathy showed no significant intergroup differences.
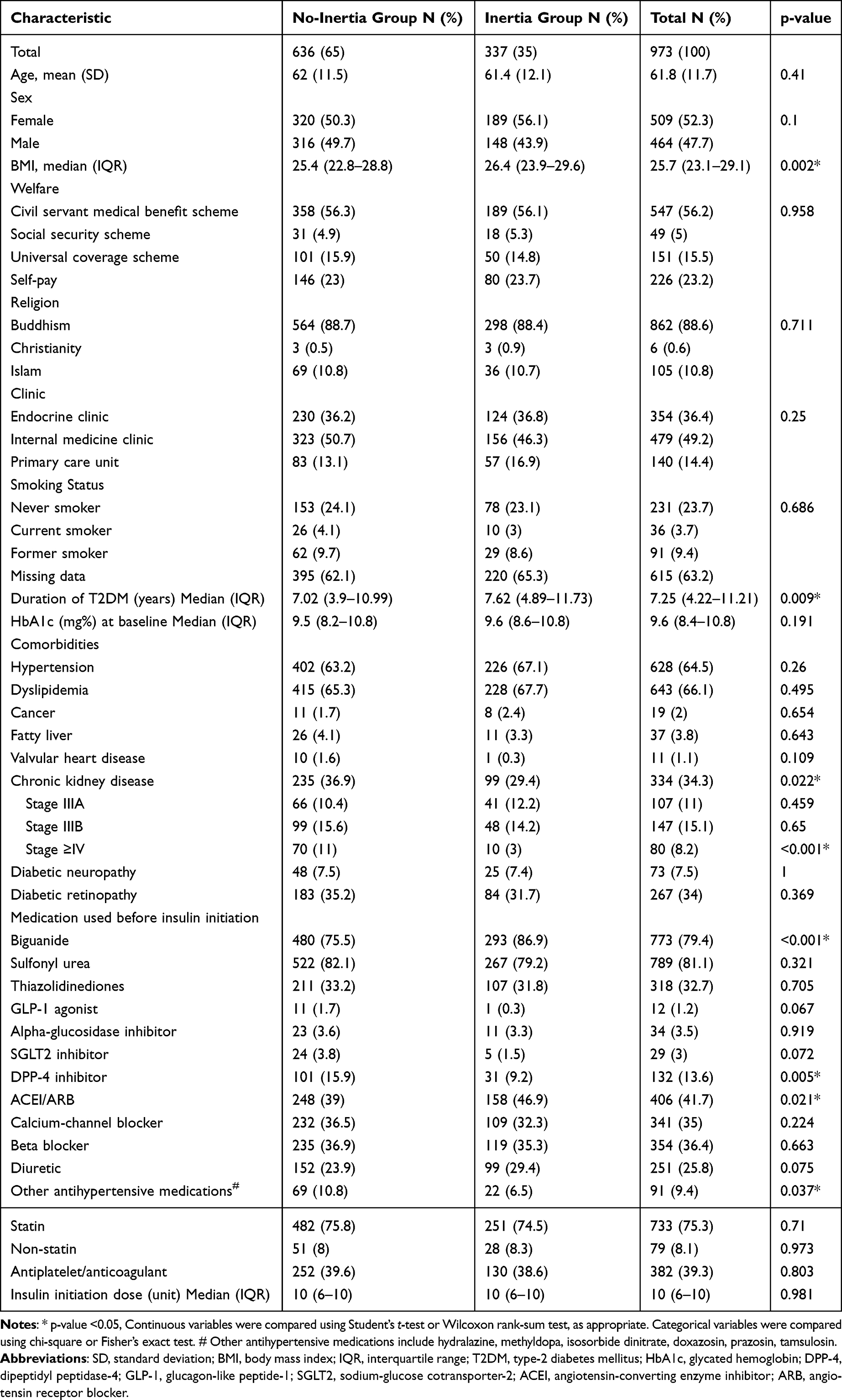 |
Table 1 Baseline Characteristics Comparing Patients in the Inertia and No-Inertia Groups |
Patients in the inertia group were more likely to use biguanides (86.9% vs 75.5%, p<0.001), ACEIs/ARBs (46.9% vs 39.0%, p=0.021), and diuretics (29.4% vs 23.9%, p=0.075), compared with those in the no-inertia group. DPP-4 inhibitor use was higher in the no-inertia group than in the inertia group (15.9% vs 9.2%, p=0.005). The initial insulin doses were similar (median, 10 units; p=0.981) between the groups. Other characteristics such as clinic type, religion, smoking status, and healthcare coverage were comparable between the groups.
Factors Associated with Clinical Inertia
Table 2 presents the results of the multivariable logistic regression analysis examining the factors associated with delayed insulin initiation. The model was developed using a backward stepwise selection approach and adjusted for age, sex, BMI, diabetes duration, baseline HbA1c level, diabetic nephropathy, CKD, and use of relevant medications, including biguanides, GLP-1 receptor agonists, SGLT2 inhibitors, DPP-4 inhibitors, ACEIs/ARBs, and diuretics. Patients with a BMI >25 kg/m2 were significantly more likely to experience clinical inertia (adjusted OR: 1.44; 95% CI: 1.08–1.93; p=0.013), compared with patients with a BMI ≤25 kg/m2. A diabetes duration >5 years was also associated with delayed insulin initiation (adjusted OR: 1.62; 95% CI: 1.17–2.24; p=0.004). Biguanide (adjusted OR: 2.29; 95% CI: 1.54–3.41; p<0.001) and diuretic use (adjusted OR: 1.61; 95% CI: 1.16–2.24; p=0.005) were similarly associated with increased odds of delay. In contrast, DPP-4 inhibitor use was associated with a significantly lower likelihood of clinical inertia (adjusted OR: 0.53; 95% CI: 0.34–0.84; p=0.006). The use of GLP-1 receptor agonist and SGLT2 inhibitor was not significantly associated with delayed insulin initiation in the adjusted model.
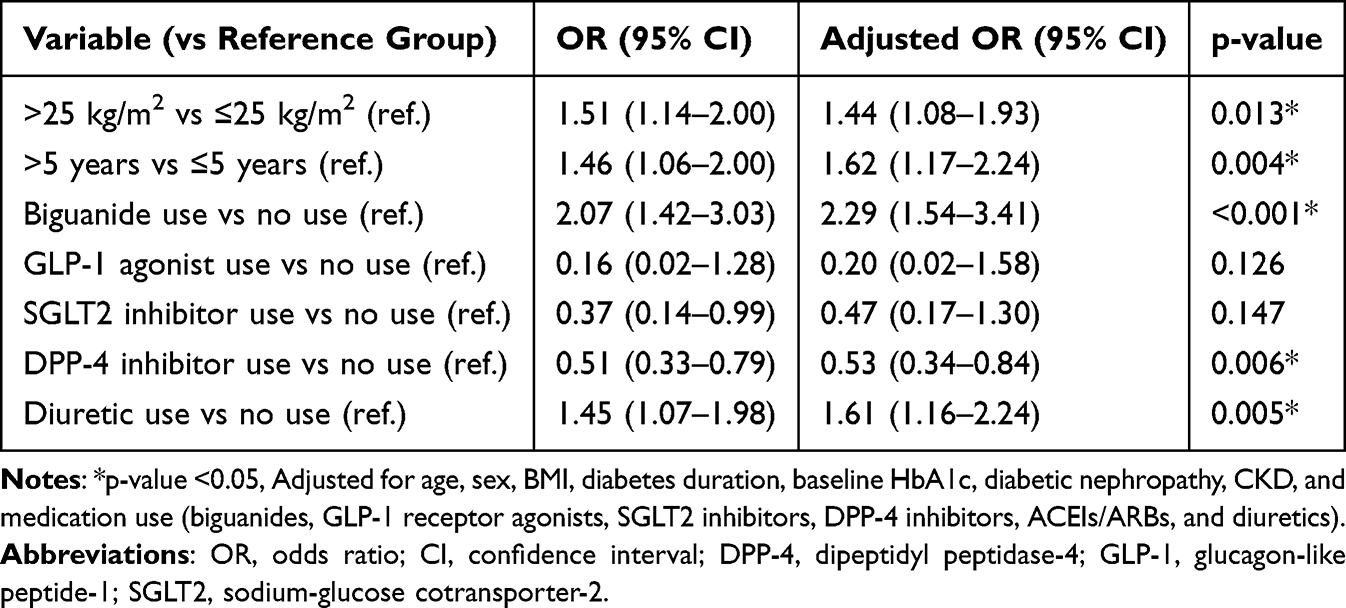 |
Table 2 Multivariable Logistic Regression Analysis for Factors Associated with Clinical Inertia |
Diabetes-Related Complications and Clinical Inertia
The incidence of diabetes-related complications was compared between the inertia and no-inertia groups (Table 3). Macrovascular complications occurred in 36.2% of patients with delayed insulin initiation versus 33.0% of those with timely initiation, although the difference was not significant (p=0.355). Among the individual macrovascular outcomes, ischemic stroke (22.2% vs 16.5%, p=0.046) and lower-limb amputation (4.5% vs 1.7%, p=0.022) were significantly more common in the inertia group versus the no-inertia group. The overall incidence of microvascular complications was comparable between the groups (60.9% and 59.1% in the inertia and no-inertia groups, respectively, p=0.658). No significant differences were found in the individual outcomes of diabetic retinopathy, neuropathy, or nephropathy.
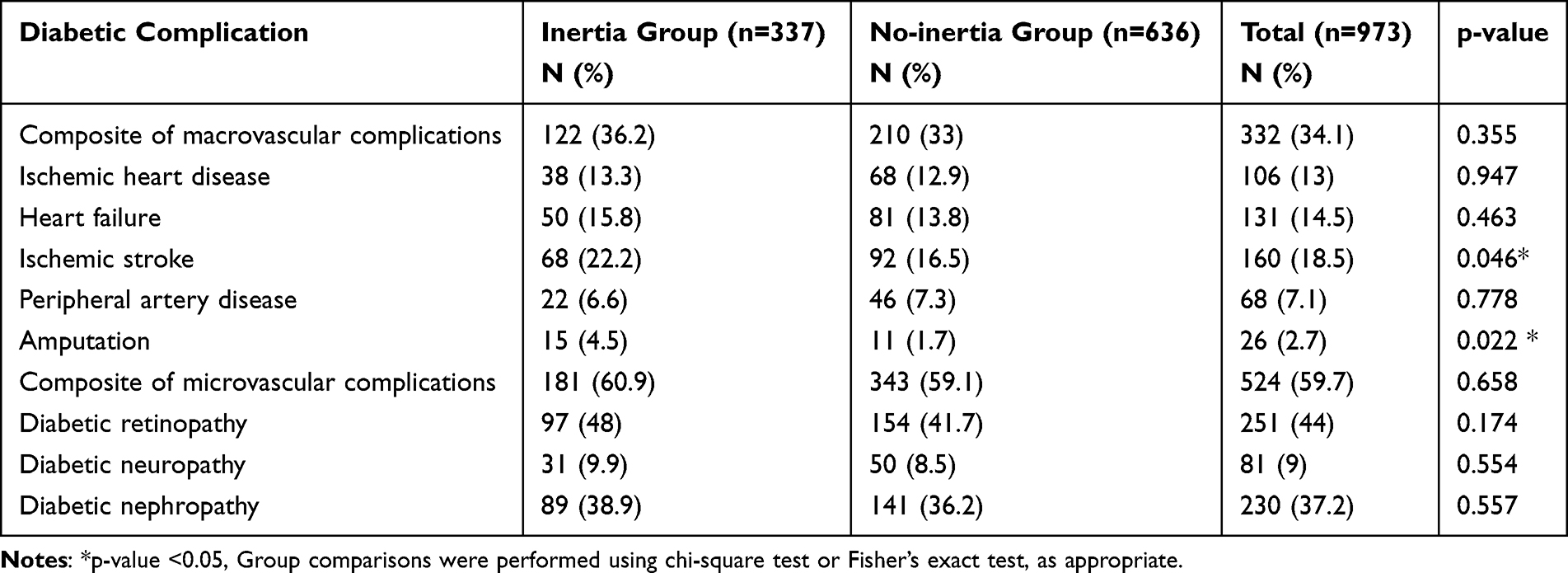 |
Table 3 Incidence of Diabetes-Related Complications in Patients with and without Clinical Inertia |
To further evaluate these associations, a Cox proportional hazards model was used (Table 4). After adjusting for relevant covariates, delayed insulin initiation was not significantly associated with the composite risk of macrovascular (HR: 1.09; 95% CI: 0.84–1.42; p=0.52) or microvascular complications (HR: 1.26; 95% CI: 0.97–1.64; p=0.08). However, a significant association was observed between delayed insulin initiation and increased risk of lower-limb amputation (HR: 2.33; 95% CI: 1.07–5.07; p=0.034), suggesting a potential consequence of prolonged hyperglycemia and therapeutic delay. Kaplan–Meier survival curves (Figures 1–3) illustrate the time-to-event differences between the groups for macrovascular and microvascular outcomes and amputation. Figure 4 shows the restricted mean survival time (RMST) for microvascular complications within the 10–15-year landmark window, which was significantly shorter in the inertia group than in the no-inertia group (4.06 vs 4.62 years; p=0.043), corresponding to a mean difference of 0.56 years (approximately 7 months) in complication-free survival and highlighting the clinically meaningful long-term impact of therapeutic delay.
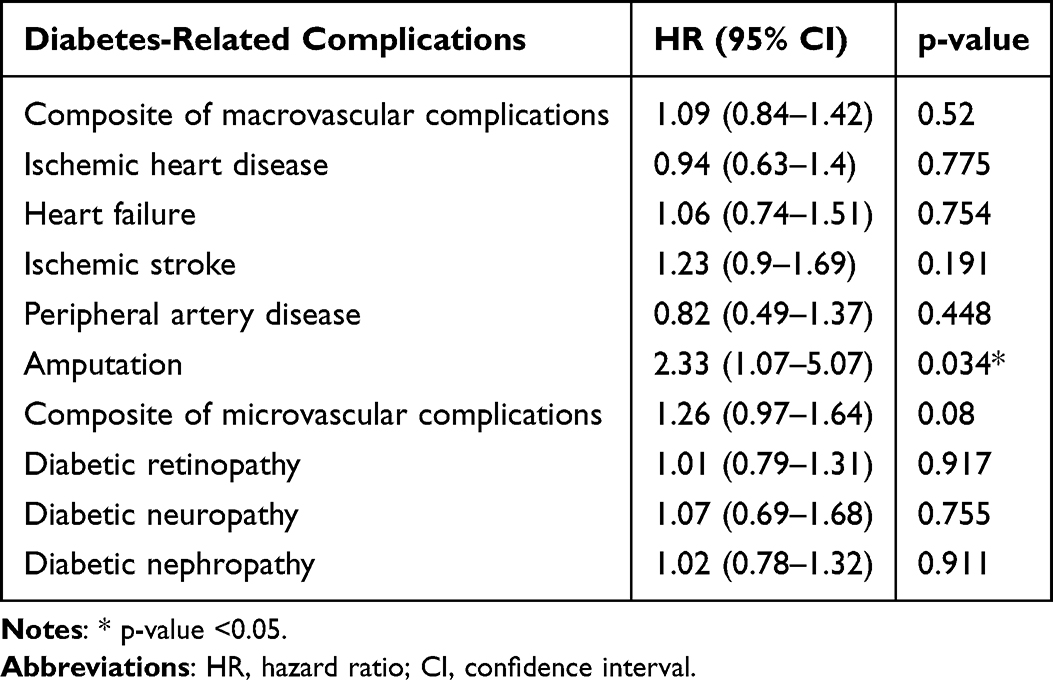 |
Table 4 Cox Proportional Hazards Model for the Effect of Clinical Inertia on Diabetes-Related Complications |
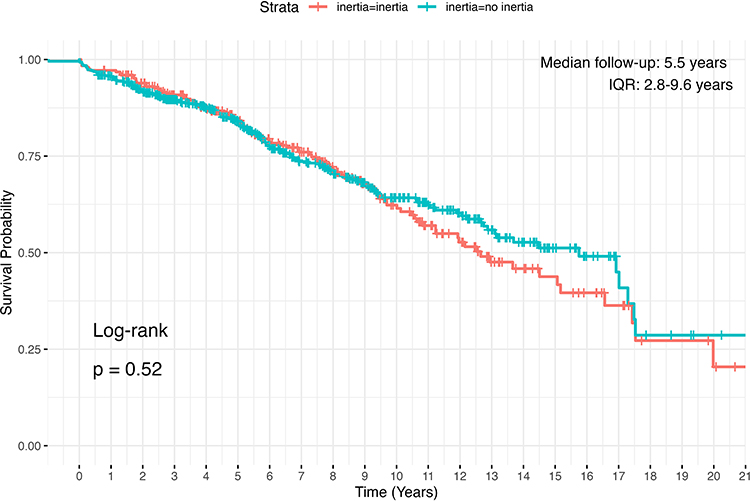 |
Figure 1 Kaplan–Meier survival curve showing composite macrovascular complications stratified by inertia group. Abbreviation: IQR, interquartile range. |
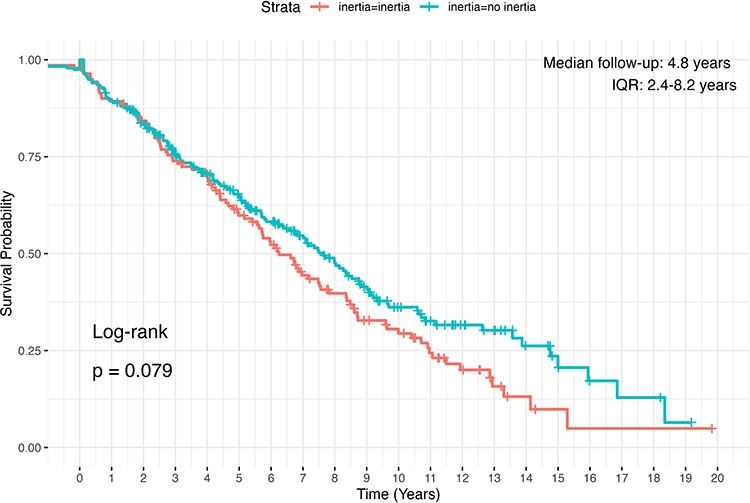 |
Figure 2 Kaplan–Meier survival curve showing composite microvascular complications stratified by inertia group. Abbreviation: IQR, interquartile range. |
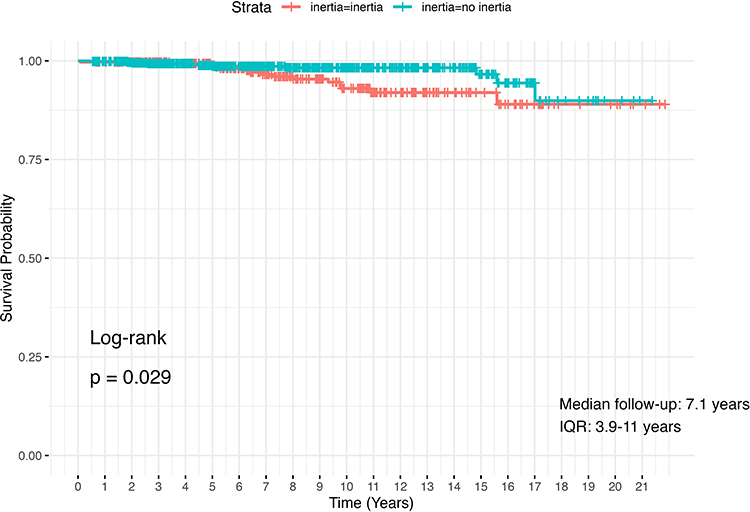 |
Figure 3 Kaplan–Meier survival curve showing the occurrence of amputation stratified by inertia group. |
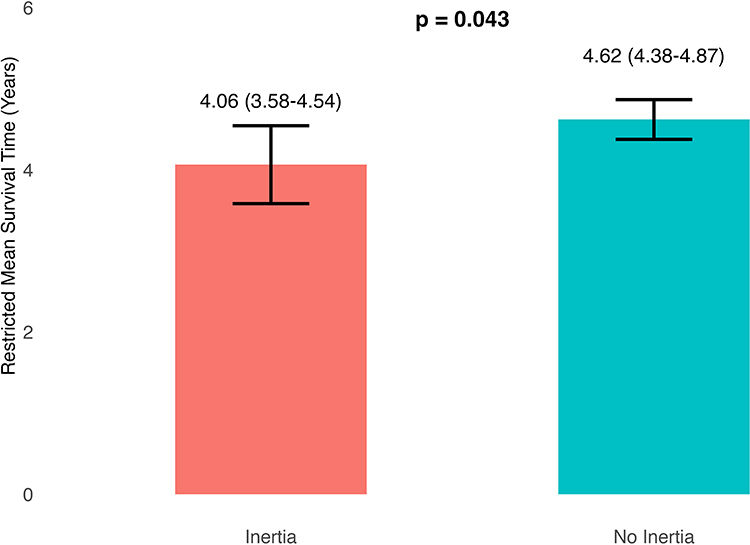 |
Figure 4 Restricted mean survival time from the occurrence of microvascular complication. P-value derived from RMST-based between-group comparison. |
To explore whether longer delays further worsen outcomes, we conducted an exploratory analysis by stratifying the inertia group by delay duration. Kaplan–Meier curves for this analysis (Supplementary Files 1–2) showed no significant differences in event-free survival between the subgroups. However, we observed a non-significant trend suggesting that prolonged delays may be associated with a higher risk of complications. Supplementary Files 3–9 illustrate the survival curves for individual complication outcomes (such as ischemic heart disease, heart failure, and diabetic retinopathy), which show consistent directions of risk across complications but without statistical significance in most cases.
Discussion
This 20-year retrospective cohort study highlighted the predictors and clinical consequences of delayed insulin initiation therapy in patients with T2DM in a real-world tertiary care setting. Patients in the inertia group were more likely to have a higher BMI, longer duration of diabetes, and concurrent use of biguanides or diuretics. The observed prevalence in our study is comparable to that reported in previous research, which found rates ranging from 27.8% to 30% in tertiary hospital settings when using similar 6-month delay definitions.7 Other studies have documented even longer delays before insulin initiation, often using different criteria such as HbA1c level ≥8% and failure on two or more oral agent use.6,8 These differences in the reported prevalence may be attributed to the varying definitions of clinical inertia and differences in treatment-intensification protocols across healthcare systems.
Several factors were significantly associated with delayed insulin initiation. Higher BMI was linked to clinical inertia, which is consistent with the findings of previous studies that highlighted concerns regarding insulin-associated weight gain as a barrier to starting therapy.8,11,12 This may reflect a clinical tendency to postpone insulin initiation in patients with obesity in the hope that further lifestyle modifications might improve glycemic control. Similarly, a longer duration of diabetes was independently associated with inertia, which is consistent with previous findings.6,8,13,14 Most studies reported this association descriptively, whereas one study offered possible explanations, suggesting that longer disease duration may be accompanied by an increased fear of lifelong insulin dependence, stigma surrounding public injections, and concerns regarding treatment costs.15
In this study, the continued use of metformin at the time of insulin initiation was significantly associated with clinical inertia. Metformin is typically maintained unless contraindicated, as recommended in clinical guidelines.16 Its persistence may reflect a treatment approach in which glycemic control is perceived as adequate with oral agents. Prior research has shown that inertia is common among metformin-treated patients without contraindications, particularly when HbA1c level elevation is modest.17 This pattern may be explained by status-quo bias and decision uncertainty among providers, which are recognized as contributors to therapeutic inertia.18 A higher prevalence of CKD was observed in the no-inertia group, possibly reflecting earlier metformin discontinuation and limited oral-agent intensification, which may have led to timely insulin initiation. However, CKD was not retained in the final multivariable model, suggesting that it may not have been an independent driver of the association. Diuretic use has also been associated with delayed initiation of insulin. This likely reflects the presence of comorbidities, such as hypertension, heart failure, or CKD, which often require polypharmacy and complex management. In these cases, providers may hesitate to initiate insulin therapy instead of choosing to optimize current treatments. The link between increased clinical complexity, polypharmacy, and therapeutic inertia has been well-documented in diabetes care.4 Conversely, DPP-4 inhibitor use was associated with a reduced likelihood of clinical inertia. These agents are typically added after the failure of standard oral therapies. A Thai cost-effectiveness analysis found that they were less favorable for monotherapy in older adults, potentially limiting their accessibility.19 Their use may indicate more complex cases, in which multiple agents have already been used, thereby increasing the likelihood of timely treatment escalation. Although we identified several clinical predictors of inertia, the underlying reasons are likely multifactorial and extend beyond measurable clinical characteristics. Patient-level barriers such as fear of injections, stigma, and concerns regarding long-term dependence may be reinforced by misinformation or misconceptions about insulin, leading to reluctance toward timely initiation.20,21 These informational and behavioral determinants were not directly measured in our dataset and should be evaluated in future prospective or mixed-methods studies.
Among the individual complications, lower-limb amputation emerged as a key adverse outcome, occurring significantly more often in the inertia group and remaining associated with delayed insulin initiation after multivariable adjustment. This aligns with prior evidence showing that poor glycemic control, as indicated by elevated HbA1c level, is strongly associated with an increased risk of lower-limb amputation in patients with diabetes.21–24 This association is supported by pathophysiological mechanisms involving peripheral neuropathy, microvascular dysfunction, arterial insufficiency, and impaired wound healing, which together contribute to ulcer development and delayed tissue repair.25 Our findings extend this understanding by showing that delayed insulin initiation is significantly associated with amputation risk, suggesting that failure to escalate therapy in a timely manner may lead to persistent hyperglycemia and an increased risk of limb-threatening outcomes. To reduce preventable amputations, efforts should focus on the early identification of high-risk patients through foot examinations and vascular assessments, along with timely treatment escalation. Patient education is essential to address the fear of injections and misinformation, particularly among those with peripheral artery disease, prior ulcers, or neuropathy.
Despite a comprehensive analysis, no significant differences were found between the delayed and timely insulin-initiation groups regarding the incidence of macrovascular and microvascular complications based on both Cox regression and Kaplan–Meier analyses. The median follow-up period in our study may not have been sufficient to fully capture the long-term progression of chronic vascular complications. Nonetheless, the trends observed in both the main analysis and supplementary files suggest worse outcomes with longer delays, particularly in the inertia group. The null findings for composite endpoints should be interpreted cautiously. Composite outcomes may dilute effects when individual complications differ in latency, baseline risk, and causal pathways. In addition, competing events (eg, death) and residual confounding inherent to retrospective real-world data may attenuate observable associations. Notably, the consistent direction of effect across several outcomes and the significant associations for amputation and RMST-derived earlier microvascular events support a clinically meaningful impact of prolonged hyperglycemia and delayed escalation. Previous cohort studies with longer follow-ups, such as a 13-year analysis of newly diagnosed diabetes in Lithuania, documented a significant cumulative incidence of microvascular complications and peripheral artery disease, most notably 9 years after diagnosis.26 Another community-based study reported that clinical inertia was associated with a 50% increased risk of diabetic nephropathy over a similar timeframe.9 However, unlike these studies, our research uniquely focused on the timing of escalation from oral therapy to insulin, highlighting therapeutic inertia in initiation rather than in intensification. Although the outcomes may appear similar, our work underscores the actionable insight that delaying insulin initiation may pose significant long-term risks.
Our RMST analysis further emphasized the clinical burden of delayed insulin initiation, revealing shorter complication-free survival in the inertia group. Although traditional HRs did not show significant differences for some outcomes, RMST offered a more interpretable and clinically relevant metric that captured the cumulative impact of therapeutic delay. These findings support the value of RMST in evaluating long-term outcomes and guiding timely decision-making in diabetes management. Intensive glycemic control having limited benefits in advanced-stage diabetes is a misconception. However, landmark trials such as the UK Prospective Diabetes Study, Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation, and the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications have shown that glycemic control provides long-term vascular protection.27–30 This benefit persists even after glycemic targets are relaxed, through a “legacy effect.” Therefore, insulin initiation should be reframed not as a last resort, but as a proactive strategy for organ preservation, particularly in patients at high risk for vascular complications.
This study offers real-world evidence on the predictors and consequences of delayed insulin initiation in a large cohort of patients with T2DM over a 20-year period. It is the first to apply survival analysis specifically to insulin-related clinical inertia, evaluating both macrovascular and microvascular outcomes. Its key strengths include the use of long-term electronic health records and outcome validation through a manual review of clinical documentation. This study also employed multiple analytical methods such as Cox regression and RMST to assess the timing and burden of complications. Distinguishing delays in insulin initiation from broader treatment intensification provides a focused and clinically actionable perspective.
However, this study has some limitations. As this was a single-center retrospective study conducted in a tertiary hospital, generalizability may be limited. Residual confounding from unmeasured factors such as socioeconomic status or patient preferences is possible. The data relied on medical records, which may have been incomplete or delayed. Psychosocial variables were not included, and the follow-up period may not have fully captured the long-term complications. Time-varying covariates were not modelled and key variables were fixed at baseline, potentially limiting causal interpretation. Additionally, this study did not quantify the strength of the association between clinical inertia and diabetic complications.
Future studies should incorporate clinical-, behavioral-, and system-level variables to enhance the prediction of therapeutic inertia. Prospective research designs are warranted to assess the effectiveness of structured interventions including early escalation protocols, multidisciplinary care models, and targeted patient education. An integrated approach combining timely insulin initiation with comprehensive chronic disease management may reduce preventable complications and improve long-term health outcomes.
Conclusion
This study showed that delayed insulin initiation, an indicator of clinical inertia, is common and associated with higher BMI, longer diabetes duration, and continued use of biguanides and diuretics. Although no significant differences were observed in the overall rates of macrovascular or microvascular complications, delayed initiation was linked to a higher risk of lower-limb amputation and an earlier onset of microvascular complications. These findings underscore the need for timely escalation of treatment to prevent avoidable outcomes. Insulin treatment should be viewed as a proactive intervention, especially for high-risk patients. Strategies that support earlier risk identification, provider action, and patient engagement are essential for reducing inertia and improving long-term diabetes outcomes.
Abbreviations
T2DM, type-2 diabetes mellitus; HbA1c, glycated hemoglobin; BMI, body mass index; CKD, chronic kidney disease; DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; SGLT2, sodium-glucose cotransporter-2; ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; ORs, odds ratios; CIs, confidence intervals; HRs, hazard ratios; RMST, restricted mean survival time.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author, Phoomjai Sornsenee, upon reasonable request.
Ethics Approval and Informed Consent
The protocol for this research project has been approved by a suitable constituted Ethics Committee of the institution and it conforms to the provisions of the Declaration of Helsinki (Human Research Ethics Committee, Faculty of Medicine, Prince of Songkla University, Approval No. REC 67-229-9-4). The requirement for patient consent was waived because of the retrospective nature of the study and the use of fully anonymized data, which involved no identifiable patient information.
Acknowledgments
We extend our gratitude to the Department of Family Medicine and Preventive Medicine at the Prince of Songkla University for facilitating this study as part of the Family Medicine residency training course. We are also grateful to Mr. Napon Meenmanee, Division of Digital Innovation and Data Analytics, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand, for his assistance in retrieving and compiling the data from the hospital database.
Author Contributions
Conceptualization: A.W., P.S., and P.L.; Methodology: A.W. and P.L.; Software: P.Sa. and K.C.; Validation: A.W. and P.S.; Formal analysis: A.W., P.S., P.Sa., and K.C.; Investigation: A.W.; Resources: A.W., P.S., and P.L.; Data curation: A.W.; Writing—original draft preparation: A.W., P.Sa., and K.C.; Writing—review and editing: P.S. and P.L.; Visualization: A.W. and P.S.; Supervision: P.S. and P.L.; Project administration: A.W. and P.S. All authors have read and agreed to the published version of the manuscript. All authors have agreed on the journal to which the article will be submitted and agree to take responsibility and be accountable for the contents of the article.
Funding
This study received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes Atlas, 9th edition. Diabet Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
2. Gabbay RA, Kendall D, Beebe C, et al. Addressing therapeutic inertia in 2020 and beyond: a 3-year initiative of the American diabetes association. Clin Diabetes. 2020;38(4):371–12. doi:10.2337/cd20-0053
3. Khunti K, Millar-Jones D. Clinical inertia to insulin initiation and intensification in the UK: a focused literature review. Primary Care Diabetes. 2017;11(1):3–12. doi:10.1016/j.pcd.2016.09.003
4. Almigbal TH, Alzarah SA, Aljanoubi FA, et al. Clinical inertia in the management of type 2 diabetes mellitus: a systematic review. Medicina. 2023;59(1):182. doi:10.3390/medicina59010182
5. Raccah D, Guerci B, Ajmera M, et al. Clinical implications of prolonged hyperglycaemia before basal insulin initiation in type 2 diabetes patients: an electronic medical record database analysis. Endocrinol Diabetes Metab. 2019;2(3):e00061. doi:10.1002/edm2.61
6. Rubino A, McQuay LJ, Gough SC, Kvasz M, Tennis P. Delayed initiation of subcutaneous insulin therapy after failure of oral glucose-lowering agents in patients with type 2 diabetes: a population-based analysis in the UK. Diabet Med. 2007;24(12):1412–1418. doi:10.1111/j.1464-5491.2007.02279.x
7. Chen P, Ma X, Chen H, Wang K, Zhou L. Delays in insulin initiation among patients with type 2 diabetes mellitus in Southeast China: a retrospective, real-world study. Diabetes Metab Syndr Obes. 2020;13:3059–3068. doi:10.2147/DMSO.S256381
8. Kim SG, Kim NH, Ku BJ, et al. Delay of insulin initiation in patients with type 2 diabetes mellitus inadequately controlled with oral hypoglycemic agents (analysis of patient- and physician-related factors): a prospective observational DIPP-FACTOR study in Korea. J Diabetes Investig. 2017;8(3):346–353. doi:10.1111/jdi.12581
9. Kaewbut P, Kosachunhanun N, Phrommintikul A, Chinwong D, Hall JJ, Chinwong S. Effect of clinical inertia on diabetes complications among individuals with type 2 diabetes: a retrospective cohort study. Medicina. 2021;58(1):63. doi:10.3390/medicina58010063
10. Kim KJ, Choi J, Bae JH, et al. Time to reach target glycosylated hemoglobin is associated with long-term durable glycemic control and risk of diabetic complications in patients with newly diagnosed type 2 diabetes mellitus: a 6-year observational study. Diabetes Metab J. 2021;45(3):368–378. doi:10.4093/dmj.2020.0046
11. Galdón Sanz-Pastor A, Justel Enríquez A, Sánchez Bao A, Ampudia-Blasco FJ. Current barriers to initiating insulin therapy in individuals with type 2 diabetes. Front Endocrinol. 2024;15:1366368. doi:10.3389/fendo.2024.1366368
12. Khunti K, Nikolajsen A, Thorsted BL, Andersen M, Davies MJ, Paul SK. Clinical inertia with regard to intensifying therapy in people with type 2 diabetes treated with basal insulin. Diabetes Obes Metab. 2016;18(4):401–409. doi:10.1111/dom.12626
13. Zografou I, Strachan M, McKnight J. Delay in starting insulin after failure of other treatments in patients with type 2 diabetes mellitus. Hippokratia. 2014;18(4):306–309.
14. Shabnam S, Gillies CL, Davies MJ, et al. Factors associated with therapeutic inertia in individuals with type 2 diabetes mellitus started on basal insulin. Diabet Res Clin Pract. 2023;203:110888. doi:10.1016/j.diabres.2023.110888
15. Arshad I, Mohsin S, Iftikhar S, Kazmi T, Nagi LF. Barriers to the early initiation of Insulin therapy among diabetic patients coming to diabetic clinics of tertiary care hospitals. Pak J Med Sci. 2019;35(1):39–44. doi:10.12669/pjms.35.1.237
16. ElSayed NA, McCoy RG, Aleppo G, American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2025. Diabetes Care. 2025;48(1 Suppl 1):S181–S206. doi:10.2337/dc25-S009
17. Mahabaleshwarkar R, Gohs F, Mulder H, et al. Patient and provider factors affecting clinical inertia in patients with type 2 diabetes on metformin monotherapy. Clin Ther. 2017;39(8):1658–1670.e6. doi:10.1016/j.clinthera.2017.06.011
18. Reach G. Clinical inertia, uncertainty and individualized guidelines. Diabetes Metab. 2014;40(4):241–245. doi:10.1016/j.diabet.2013.12.009
19. Permsuwan U, Dilokthornsakul P, Thavorn K, Saokaew S, Chaiyakunapruk N. Cost-effectiveness of dipeptidyl peptidase-4 inhibitor monotherapy versus sulfonylurea monotherapy for people with type 2 diabetes and chronic kidney disease in Thailand. J Med Econ. 2017;20(2):171–181. doi:10.1080/13696998.2016.1238386
20. Imran S, Ali R, Mahboob G. Frequency of lower extremity amputation in diabetics with reference to glycemic control and Wagner’s grades. J Coll Physicians Surg Pak. 2006;16(2):124–127.
21. Dulyapach K, Ngamchaliew P, Vichitkunakorn P, Sornsenee P, Choomalee K. Prevalence and associated factors of delayed diagnosis of type 2 diabetes mellitus in a tertiary hospital: a retrospective cohort study. Int J Public Health. 2022;67:1605039. doi:10.3389/ijph.2022.1605039
22. Pratueangpong T, Buathong N, Sornsenee P. Prevalence of common diabetes mellitus misinformation exposure, cognitive attitude, and intention to share information among patients in a primary care unit. Healthcare. 2025;13(14):1762. doi:10.3390/healthcare13141762
23. Yusof NM, Rahman JA, Zulkifly AH, et al. Predictors of major lower limb amputation in children presenting to a single tertiary centre with perceived or true food allergies. Singapore Med J. 2015;56(11):626–631. doi:10.11622/smedj.2015172
24. Kostov G, Doykov M, Hristov B, et al. Risk factors related to amputation in diabetic foot patients: single center outcomes. Folia Med. 2024;66(5):629–636. doi:10.3897/folmed.66.e131632
25. Zhao W, Katzmarzyk PT, Horswell R, et al. HbA1c and lower-extremity amputation risk in low-income patients with diabetes. Diabetes Care. 2013;36(11):3591–3598. doi:10.2337/dc13-0437
26. Caruso P, Scappaticcio L, Maiorino MI, Esposito K, Giugliano D. Up and down waves of glycemic control and lower-extremity amputation in diabetes. Cardiovasc Diabetol. 2021;20(1):135. doi:10.1186/s12933-021-01325-3
27. Piliponienė L, Veličkienė D, Kregždytė R. Microvascular complications, peripheral artery disease and mortality in patients with type 2 diabetes mellitus, in two counties of Southern Lithuania over 13 years: analysis using a cohort database of the national health insurance. Medicina. 2021;57(12):1380. doi:10.3390/medicina57121380
28. King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48(5):643–648. doi:10.1046/j.1365-2125.1999.00092.x
29. ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–2572.
30. Nathan DM, DCCT/EDIC Research Group. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37(1):9–16. doi:10.2337/dc13-2112
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efferocytosis: An Emerging Therapeutic Strategy for Type 2 Diabetes Mellitus and Diabetes Complications
Liu X, Liu H, Deng Y
Journal of Inflammation Research 2023, 16:2801-2815
Published Date: 7 July 2023