Back to Journals » International Journal of General Medicine » Volume 18
Predictive Value of the COP-INH Score for Adverse Cardiovascular Events After PCI in ACS Patients
Authors Ou J, Liu Z, Wang Q, Wang Y, Li X
Received 5 July 2025
Accepted for publication 8 October 2025
Published 29 October 2025 Volume 2025:18 Pages 6523—6531
DOI https://doi.org/10.2147/IJGM.S551689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Junping Ou,1,* Zhongwen Liu,1,* Qingyi Wang,2,* Yuping Wang,2 Xiaolin Li1,2
1Department of Cardiology, Ji’an Central People’s Hospital, Ji’an, 343009, People’s Republic of China; 2Medical School, Rehabilitation Medicine Department, Jinggangshan University, Ji’an, 343009, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaolin Li, Medical School, Rehabilitation Medicine Department, Jinggangshan University, Ji’an, 343009, People’s Republic of China, Tel +86 13979609896, Email [email protected]
Background: Patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) require long-term antiplatelet therapy to prevent in-stent restenosis. However, the efficacy of this treatment can be compromised by factors, such as aspirin resistance and variable clopidogrel reactivity, potentially leading to adverse clinical outcomes. This study aims to assess the clinical significance of detecting platelet reactivity to P2Y12 receptor inhibitors and platelet inhibition rates in patients with ACS post-PCI and assessing the relation of the occurrence of major adverse cardiac events (MACE).
Methods: We employed the VerifyNow P2Y12 system to assess platelet reactivity to P2Y12 receptor inhibitors and platelet inhibition rates. The combination of P2Y12 reaction unit and percentage of platelet inhibition [%INH] (COP-INH) score was calculated 30 days post-PCI for patients with ACS. The primary endpoint events included cardiovascular death, non-fatal myocardial infarction, and target vessel revascularization at 1-year follow-up. We analyzed the correlation between the COP-INH score and primary endpoint events.
Results: The incidence of major adverse cardiovascular events was significantly higher in patients with a COP-INH score of 2, compared with those with a score of 1 or 0 (20.31% vs 7.69%, p=0.015). Multivariate analysis revealed that a COP-INH score of 2 is a predictive indicator of major adverse cardiovascular events post-PCI in patients with ACS (p=0.027). In contrast, scores of 1 or 0 showed no significant predictive value.
Conclusion: The COP-INH score may serve as a potential predictor for long-term adverse cardiovascular events following PCI in patients with ACS.
Keywords: platelet reactivity, clopidogrel, acute coronary syndrome, percutaneous coronary intervention, prognosis
Introduction
Dual antiplatelet therapy (DAPT), which includes aspirin and a P2Y12 receptor antagonist, is recommended for at least 1 year post percutaneous coronary intervention (PCI) with drug-eluting stents. This regimen aims to reduce the incidence of stent thrombosis and major adverse cardiac events (MACE).1,2 However, variations in aspirin tolerance and clopidogrel reactivity, along with a strong association between high residual platelet reactivity (HRPR) post-clopidogrel treatment and increased risk of clinical adverse events after PCI,3,4 necessitate regular monitoring of platelet function. The VerifyNow P2Y12 assay, a common method for assessing platelet aggregation function.5,6 However, as a whole blood assay, VerifyNow can be influenced by variables such as platelet or leukocyte counts, as well as haemoglobin or haematocrit.7 To address this question, we took the opportunity of VerifyNow P2Y12 system to measure P2Y12 reactivity and platelet inhibition rate, calculating the combination of P2Y12 reaction unit (PRU) and percentage of platelet inhibition (%INH) score (combination of PRU and %INH COP-INH), and to investigate the correlation between COP-INH scores and adverse cardiovascular events in patients with acute coronary syndrome (ACS) undergoing PCI. To facilitate the early identification of the patients with high aspirin tolerance or high residual platelet reactivity to clopidogrel, and reducing the risk of adverse clinical events post-PCI.
Materials and Methods
The study was conducted in accordance with the Declaration of Helsinki and the Institutional Review Board of Jinggangshan University approved the study protocol. Written informed consent was obtained from each participant before any sample or data collection.
Study Design and Patients
This study analyzed 337 patients with ACS who underwent PCI at the Ji’an Central People’s Hospital affiliated Jinggangshan University, from November 2017 to December 2023.
After excluding participants with factors such as stable coronary artery disease, current use of anticoagulant or antiplatelet medications, contraindications to aspirin or clopidogrel, severe liver or kidney dysfunction (serum creatinine >2 mg/dL or alanine transaminase levels >3 times the normal limit), thrombocytopenia (less than 100×109/L), recent stroke or transient ischemic attack within the last 3 months, and in-hospital death, 226 participants were included in the study. The participant selection process is depicted in Figure 1.
 |
Figure 1 Patient inclusion flowchart. |
Coronary Angiography and Drug Treatment
Coronary angiography and PCI procedures were performed according to standard protocols.8,9 All patients received a loading dose of 300 mg clopidogrel and 300 mg aspirin prior to the operation. Postoperatively, they were maintained on 75 mg of clopidogrel and 100 mg of aspirin daily for 12 months. The use of statins, angiotensin-converting enzyme inhibitors, or angiotensin receptor blockers followed established guidelines.8
Blood Sample and Platelet Reactivity Assay
To ensure pharmacological efficacy and stability of platelet function, all patients underwent a VerifyNow P2Y12 test 30 days after PCI, a time window considered adequate to the achievement of a steady state of pharmacologic activity and clinical state.10 The VerifyNow P2Y12 assay is a common tool for assessing platelet reactivity used to evaluate the responsiveness of clopidogrel and other thienopyridines.11 This assay measures P2Y12 reactivity, including the P2Y12 reaction unit (PRU) post-drug treatment, baseline values (BASE), and the degree of platelet aggregation and inhibition (%INH). The formula to calculate the platelet inhibition rate is: [(BASE−PRU)/BASE]× 100 [(BASE−PRU)/BASE]×100, representing the change in values before and after treatment.12
Patients were considered to have poor responsiveness to clopidogrel if the PRU was ≥2303 or the inhibition rate (%INH) was <40%.11 The COP-INH score was calculated based on the data obtained 30 days post-PCI: patients who exhibited both increased PRU and decreased %INH received a score of 2, those with either an increase or decrease in one category received a score of 1, and those without changes in both categories received a score of 0.
Definitions and Endpoints of the Study
The occurrence of MACE was recorded from the start of the VerifyNow test. MACE in this study was defined as death from combined cardiovascular causes, non-fatal myocardial infarctions (MIs), and target vessel revascularizations (either PCI or coronary artery bypass grafting [CABG]). All deaths, unless clearly of non-cardiac origin, were classified as cardiac deaths. The analysis of study endpoints was conducted for all patients at 12 months post-operation.
Power Calculation
We postulated that the average difference in MACE rate between the two groups would be 15%.13 Therefore, for 90% power and an alpha riskof 5%, we estimated that 160 patients should be included in each group. We estimated that 5% of patients would be lost to follow-up, so the target number of included patients was 337.
Statistical Analysis
Statistical analyses were performed using SPSS version 20.0. For continuous variables, means were compared using a t-test and presented as arithmetic mean ± standard deviation. Categorical variables were analyzed using chi-square tests or Fisher’s exact test when appropriate. Odds ratios and 95% confidence intervals were calculated using either univariate or multivariate regression models. The cumulative incidence of MACE was compared using Kaplan–Meier survival analysis and the Log rank test. Statistical significance was indicated by a p-value <0.05.
Results
A total of 337 patients completed the 12-month follow-up, with an average follow-up period of 12.6 ± 0.9 months. Statistical analysis revealed that the distribution of VerifyNow results, measured in PRU and percentage of inhibition (%INH), followed a normal distribution. Specifically, 64 patients (18.99%) had a COP-INH score of 2, whereas 273 (81.01%) had either a COP-INH score of 1 or 0.
Clinical Examination Findings
Except for a history of diabetes (48.44% vs 22.34%, p = 0.013) and previous CABG (15.63% vs 5.86%, p = 0.016), no significant differences were observed in other clinical indicators between the two groups (Table 1). Additionally, both groups predominantly used similar medications, including proton pump inhibitors (PPIs) and calcium-channel blockers (CCBs). No significant differences were observed in laboratory indicators between the two groups (Table 2). No significant differences were observed in the characteristics of vascular lesions, culprit vessels, or postoperative thrombosis in myocardial infraction flow velocities (Table 3).
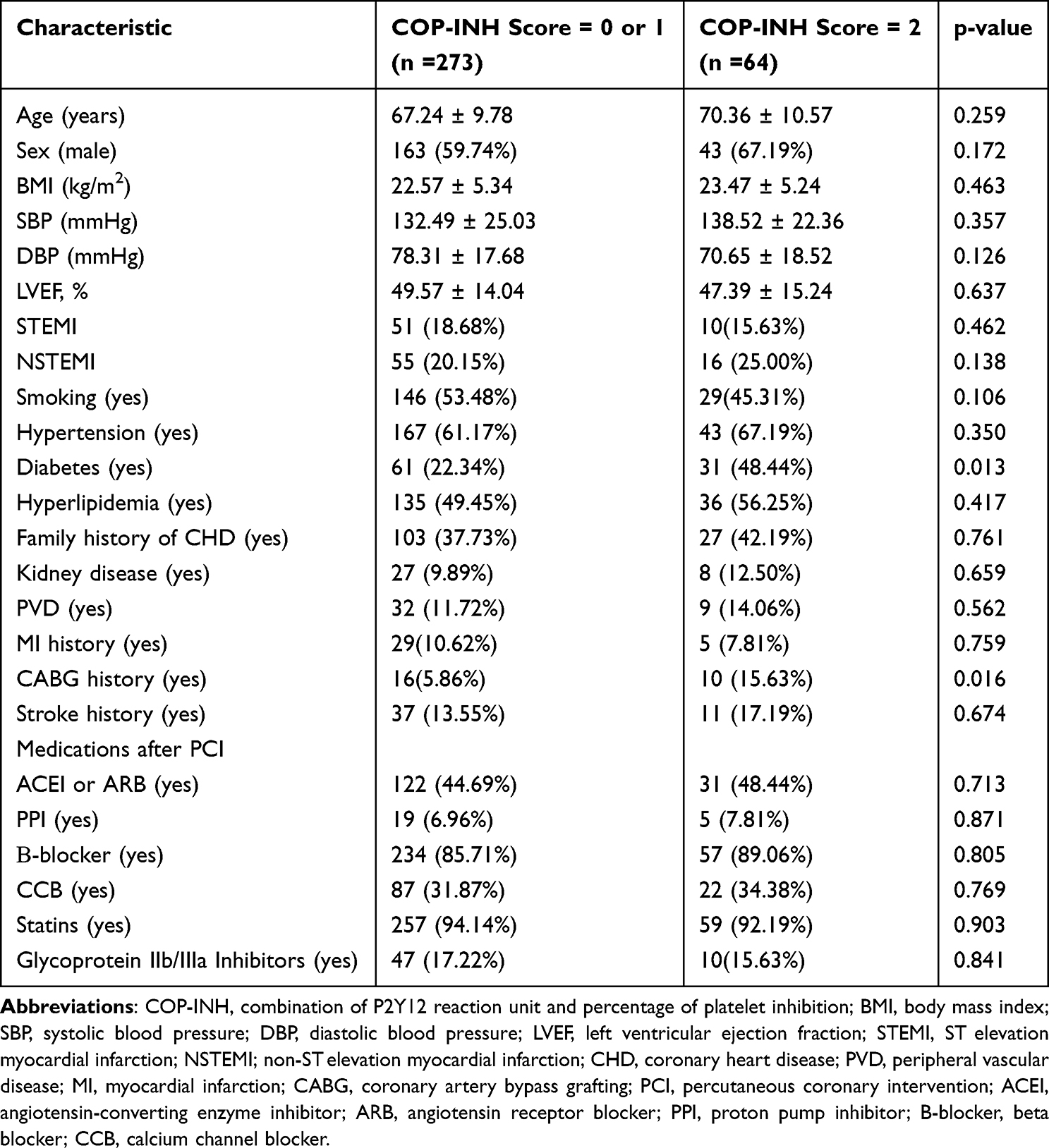 |
Table 1 Patient Characteristics |
 |
Table 2 Laboratory Test Data |
 |
Table 3 Correlation Between COP-INH Score and CHD Characteristics |
Association of COP-INH Score with Clinical Outcomes
Among the 337 patients (94.40%) who completed 1 year of clinical follow-up, the rate of MACE in the COP-INH score = 2 group was significantly higher, compared with the COP-INH score = 1 or 0 group (23.08% vs 5.88%, p = 0.007). No significant differences were observed in individual cardiovascular events between the two groups (Table 4).
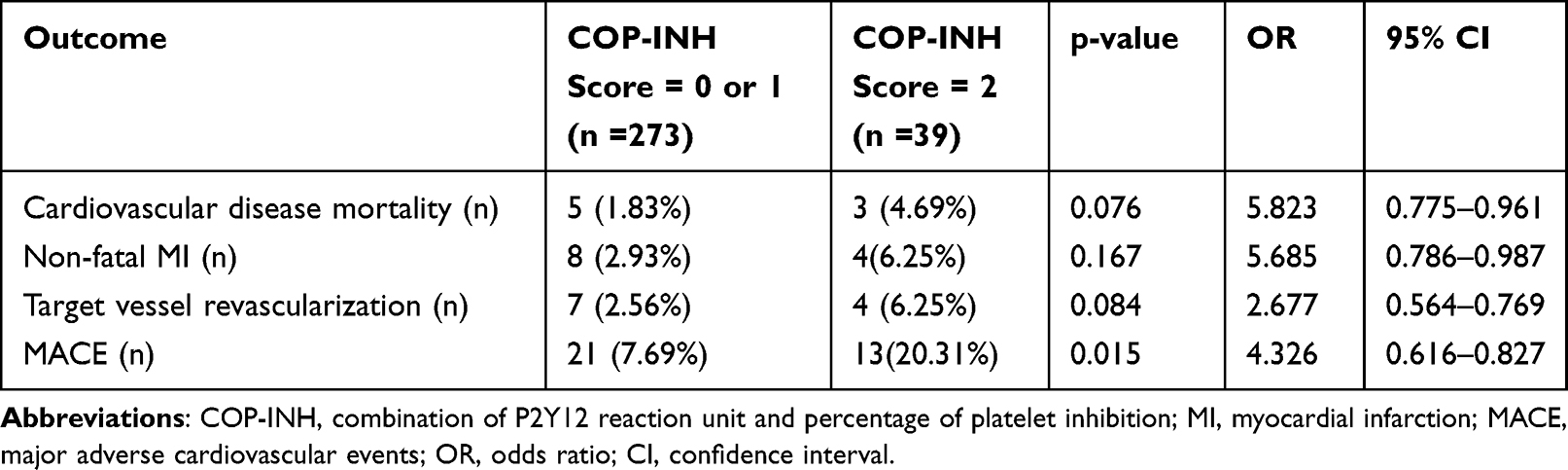 |
Table 4 Follow-Up Results After 1 Year |
Logistic Regression Analysis for Predictors of MACE
During the follow-up period, 32 patients (9.50%) experienced MACE, and 66 patients (19.58%) had a PRU ≥ 230. Among these, 91 patients (27.00%) had a %INH < 40%. A total of 56 patients (16.62%) met both criteria (PRU ≥ 230 and %INH < 40%). Univariate logistic regression analysis revealed that smoking (p = 0.014), diabetes (p = 0.017), history of MI (p = 0.006), history of stroke (p = 0.011), a PRU ≥ 230 (p = 0.016), and a COP-INH score = 2 (p = 0.007) predicted MACE after 1 year (Table 5). However, after adjusting for confounding factors such as age and gender, multivariate statistical analysis indicated that only diabetes, a history of MI and a COP-INH score = 2 were significant predictors of MACE after 1 year of follow-up (p < 0.05) (Table 6), whereas a PRU ≥ 230, a history of stroke, and smoking were not.
 |
Table 5 Univariate Logistic Regression Analysis for Predictors of MACE |
 |
Table 6 Multivariate Logistic Regression Analysis for Predictors of MACE |
Further analysis of patients without MACE using Kaplan–Meier survival analysis revealed significantly higher survival rates for patients with a COP-INH score = 1 or 0 compared with those with COP-INH score = 2 (p < 0.001), as illustrated in Figure 2.
 |
Figure 2 Kaplan–Meier analysis of major adverse cardiac events (MACE)-free survival in-patients with COP-INH score of 1 or 0 and those with a COP-INH score of 2. |
Discussion
Despite the widespread adoption of DAPT as a critical component of post-procedural care following PCI, challenges such as in-stent restenosis persist.12 Current insights link these adverse events, particularly HRPR, to clopidogrel treatment.4,10 This study introduces a composite score—the COP-INH score—which integrates P2Y12 reactivity and percentage of platelet inhibition, to assess long-term clinical outcomes in patients with ACS undergoing PCI. Key findings indicate that patients with a COP-INH score of 2 have a significantly higher incidence of MACE, compared with those with scores of 1 or 0.
Furthermore, the percentage of patients with a COP-INH score of 2 was notably higher among patients who experienced MACE than among those without MACE.
Multivariate regression analysis confirmed a COP-INH score of 2 as a significant risk factor for MACE post-PCI in patients with ACS. In contrast, there appears to be no clear correlation between PRU ≥ 230 or INH < 40% and the occurrence of MACE.
This study emphasizes the necessity for individualized therapeutic strategies based on molecular biomarkers, suggesting that patients with a COP-INH score of 2 may benefit from customized antithrombotic approaches. Further research is needed to elucidate the mechanisms linking specific biomarkers to MACE and to develop personalized treatment plans for patients with ACS undergoing PCI.
Additionally, the results reinforce that HRPR post-clopidogrel therapy serves as a predictive marker for adverse cardiovascular events following PCI.3 Previous studies have examined indicators such as PRU, BASE (baseline values of the degree of platelet aggregation), and %INH (inhibition ratio before and after treatment).14 PRU measures platelet reactivity after antiplatelet therapy; higher values indicate stronger reactivity, whereas lower values suggest weaker reactivity. BASE assesses the degree of platelet aggregation under clopidogrel therapy; a higher BASE value denotes greater aggregation. %INH quantifies the change in the inhibitor ratio and post-treatment vs pre-treatment. Notably, administering a maintenance dose of clopidogrel for 4 weeks post-PCI significantly reduces PRU in patients with ACS, establishing ≥230 as a critical threshold for PRU.3
Considering the correlation between PRU and drug response, previous studies have suggested that %INH might be a more sensitive indicator of the efficacy of antiplatelet drugs, where elevated PRU and decreased %INH indicate a poor drug response. Consequently, the incidence of MACE was notably higher in patients with COP-INH score = 2 (high PRU and low %INH) than in those with COP-INH score = 1 or 0, aligning with our findings. No significant differences were observed in the occurrence rates of individual cardiovascular events within MACE, which may be due to their lower frequency. Our univariate analysis revealed that PRU ≥ 230 and COP-INH score = 2, along with factors such as smoking, diabetes, history of myocardial infarction, and stroke, were effective predictors of MACE in patients undergoing PCI surgery, for 1 year following ACS, consistent with prior research.3,15 After adjusting for confounding factors, a COP-INH score of 2 remained a predictive factor for MACE after 1 year in patients with ACS undergoing PCI surgery, whereas PRU ≥ 230 did not.
Our study also found that the critical values of PRU ≥ 230 at 30 days post-PCI and %INH < 40% were not predictive of MACE, consistent with previous studies.16,17 This discrepancy might be due to the fact that most cardiovascular events occur during the acute phase, whereas HRPR is more prevalent perioperatively.18 Kaplan–Meier analysis revealed that the rate of occurrence of MACE in patients with a COP-INH score of 2 was significantly higher than that in patients with COP-INH scores of 1 or 0 (p < 0.001). Moreover, patients with elevated PRU and lower %INH had poor long-term prognosis. Our findings indicate that a higher PRU suggests greater platelet reactivity, whereas a lower %INH implies reduced efficacy of antiplatelet drugs. This suggests that the COP-INH score not only reflects changes in platelet reactivity before and after treatment but also predicts these changes over time. Hence, we believe that achieving substantial reductions in PRU may effectively reduce the risk of MACE postoperatively, which might explain why enhancing antiplatelet therapy based on PRU has not consistently improved patient outcomes in current clinical practice.
In summary, our study investigated the relationship between P2Y12 reactivity, platelet inhibition rates, and MACE in patients undergoing PCI following ACS. The findings demonstrated that the COP-INH score may help identify patients at risk for adverse cardiovascular events after PCI. In terms of predicting long-term outcomes, the COP-INH score proved to be more effective than PRU or %INH alone. These results offer valuable insights and potential guidance for optimizing antithrombotic therapy post-PCI in patients with ACS, and reducing the risk of adverse clinical events, contributing significantly to clinical practice.
Limitations of the Study
There were several limitations in the present study. First, the small sample size may have been insufficient to uncover any single component of MACE. Second, this study was a single-center design and lack of external validation. The findings of this trial warrant further investigation in a larger, multi-center cohorts.
Conclusion
The COP-INH score may facilitate earlier identification of major adverse cardiovascular event risks during antiplatelet therapy post-PCI and is expected to improve long-term prognosis in patients.
Abbreviations
ACS, acute coronary syndrome: PCI, percutaneous coronary intervention; MACE; major adverse cardiac events; HRPR, high residual platelet reactivity; PRU, P2Y12 reaction unit.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the funds from the Health Commission of Jiangxi Province (Grant Number 202312372, 202312384).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Han YL. De-escalation of anti-platelet therapy in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a narrative review. Chin Med J. 2019;132:197–210. doi:10.1097/CM9.0000000000000047
2. Franey EG, Kritz-Silverstein D, Richard EL. Association of Race and Major Adverse Cardiac Events (MACE): the Atherosclerosis Risk in Communities (ARIC) Cohort. J Agi Circulation Ng Res. 2019;1–7. doi:10.1155/2020/7417242
3. Christine J, Chung Ajay J, Zhang Y, et al. Impact of high on-aspirin platelet reactivity on outcomes following successful percutaneous coronary intervention with drug-eluting stents. Am Heart J. 2018;205:1–30. doi:10.1016/j.ahj.2018.07.020
4. Garabedian T, Alam S. High residualplatelet reactivity on clopidogrel: its significance and therapeuticchallenges overcoming clopidogrel resistance. Cardiovasc DiagnTher. 2013;3(1):23–37. doi:10.3978/j.issn.2223-3652.2013.
5. Matthew J, Price D, Angiolillo J, et al. Platelet reactivity and cardiovascular outcomes after percutaneous coronary intervention: a time-dependent analysis of the Gauging Responsiveness with a VerifyNow P2Y12 assay: impact on Thrombosis and Safety (GRAVITAS) trial. Circulation. 2011;124(10):1132–1137. doi:10.1161/CIRCULATIONAHA.111.029165
6. Johanne S, Benoit L, Etienne. Puymirat, etc. Impact of transfusion in platelet reactivity in patients with anemia and acute MI. Eur Heart J Cardiovascular Pharmacother. 2023;9(7):647–657. doi:10.1093/ehjcvp/pvad055
7. Sophie V, Vanina B, Mohammed A, et al. Are P2Y12 reaction unit (PRU) and % inhibition index equivalent for the expression of P2Y12 inhibition by the VerifyNow assay? Role of haematocrit and haemoglobin levels. Thromb Haemost. 2011;106(2):227–229. doi:10.1160/TH11-01-0046
8. Han Y, Heng Chao, Zeng W. Section of Interventional Cardiology, Chinese Society of Cardiology of Chinese Medical Association.Chinese guideline for percutaneous coronary intervention(pochet guideline). Zhonghua Xin Xue Guan Bing Za Zh. 2016;44:382–400.
9. Davide C, Dominick J. Timing, selection, modulation, and duration of P2Y(12) inhibitors for patients with acute coronary syndromes undergoing PCI. JACC Cardiovasc Interv. 2023;16(1):1–18. doi:10.1016/j.jcin.2022.10.023
10. Saia F, Marino M, Campo G, et al. Incidence and outcome of high on-treatment platelet reactivity in patients with nonST elevation acute coronary syndromes undergoing percutaneous coronary intervention (from the VIP [VerifyNow and Inhibition of Platelet Reactivity] Study). Am J Cardiol. 2013;112(6):792–798. doi:10.1016/j.amjcard.2013.05.010
11. Seung-Yul L, Young-Hoon J, Kyeong H. P2Y(12) inhibitor monotherapy combined with colchicine following PCI in ACS patients: the MACT pilot study. JACC Cardiovasc Interv. 2023;16(15):1845–1855. doi:10.1016/j.jcin.2023.05.035
12. Ferreiro JL, Vivas D, Hera DL, et al. High and low on-treatment platelet reactivity to P2Y12 inhibitors in a contemporary cohort of acute coronary syndrome patients undergoing percutaneous coronary intervention. Thrombosis Res. 2019;175:95–101. doi:10.1016/j.thromres.2019.01.021
13. Kristian T, Joseph S, Alpert AS, et al. Fourth universal definition of myocardial infarction. Circulation. 2018;138(20):e618–e651. doi:10.1161/CIR
14. Nakamura M, Isshiki T, Kimura T, et al. Optimal cut off value of P2Y12 reaction units to prevent major adverse cardiovascular events in the acute periprocedural period: post-hoc analysis of the randomized PRASFIT-ACS study. Int J Cardiol. 2015;182:541–548. doi:10.1016/j.ijcard.2015.01.026
15. Siller-Matula JM, Trenk D, Schrör K, et al. Response variability to P2Y12 receptor inhibitors: expectations and reality. JACC:Cardiovasc Interv. 2013;6(11):1111–1128. doi:10.1016/j.jcin.2013.06.011
16. Wang L, Hong-Liang C, Jing-Xia Z. Triglyceride-glucose index predicts adverse cardiovascular events in patients with diabetes and acute coronary syndrome.Cardiovasc Diabetol. 2020;19.1;
17. Ang L, Thani KB, Ilapakurti M, et al. Elevated plasma fibrinogen rather than residual platelet reactivity after clopidogrel pre-treatment is associated with an increased ischemic risk during elective percutaneous coronary intervention. J Am Coll Cardiol. 2013;61(1):23–34. doi:10.1016/j.jacc.2012.09.037
18. T AR, Brand kanters NC, Roozendaal NMJ, et al. Perioperative platelet reactivity over time in patients undergoing vascular surgery: an observational pilot study. PLoS One. 2024;19(6):e0304800. doi:10.1371/journal.pone.0304800
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combination of TyG Index and GRACE Risk Score as Long-Term Prognostic Marker in Patients with ACS Complicated with T2DM Undergoing PCI
Qin Z, Xu S, Yuan R, Wang Z, Lu Y, Xu Y, Lv Y, Yu F, Bai J, Zhang H, Zhang L, Zhang J, Tang J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3015-3025
Published Date: 28 September 2022
Advanced Lung Cancer Inflammation Index for Predicting Prognostic Risk for Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention
Wang X, Wei C, Fan W, Sun L, Zhang Y, Sun Q, Liu Y, Liu J
Journal of Inflammation Research 2023, 16:3631-3641
Published Date: 23 August 2023
The Impact of Patient Adherence to Dual Antiplatelet Medication Following Percutaneous Coronary Intervention on the Occurrence of Adverse Cardiovascular Events
Mansurova JA, Orekhov A, Zhunuspekova AS, Kassymova AA, Karazhanova LK
Patient Preference and Adherence 2024, 18:425-434
Published Date: 17 February 2024
PEAR1, PON1, CYP2C19, CYP1A2 and F2R Polymorphisms are Associated with MACE in Clopidogrel-Treated Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention
Du P, Li X, Li D, Ma Y, Ni M, Li Y, Li W, Wang A, Xu X
Pharmacogenomics and Personalized Medicine 2024, 17:611-621
Published Date: 21 December 2024
Prognostic Value of Systemic Inflammation Scores in Patients with Acute Coronary Syndrome Who Underwent Percutaneous Coronary Intervention: A Prospective Cohort Study
Wang X, Wang L, Qi Y, Liu Y, Zhang Y, Song G, Sun Q, Wei C, Liu J, Shi F, Sun L
Journal of Inflammation Research 2025, 18:15627-15643
Published Date: 8 November 2025