Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Predicting Individual Response to Acupuncture in Sensorineural Tinnitus Using Integrated Functional Near-Infrared Spectroscopy and Machine Learning: Protocol for a Model Development and Validation Study
Authors Huang X ![]() , Jiang D, Kong D
, Jiang D, Kong D ![]() , Liu H
, Liu H ![]() , Chen L, Li Y, Zhou J, Gao H, Hu H
, Chen L, Li Y, Zhou J, Gao H, Hu H ![]()
Received 28 June 2025
Accepted for publication 26 September 2025
Published 9 October 2025 Volume 2025:18 Pages 6579—6593
DOI https://doi.org/10.2147/JMDH.S550296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Xiaohan Huang,1,* Da Jiang,1,* Debiao Kong,1 Huiting Liu,1 Liao Chen,1 Yang Li,2 Jie Zhou,2,3 Hong Gao,2 Hantong Hu2
1The Third Clinical College, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Department of Neurobiology and Acupuncture Research, Zhejiang Chinese Medical University, Key Laboratory of Acupuncture and Neurology of Zhejiang Province, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Gao, Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China, Email [email protected] Hantong Hu, Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China, Email [email protected]
Background: Research indicates that around 20% of adults experience chronic tinnitus, with about a fifth of these cases being severe. Although various treatments are available for tinnitus, their effectiveness is often limited, and each treatment has clinical constraints. While acupuncture has shown promise in treating tinnitus, individual responses vary significantly. Identifying methods to predict acupuncture’s effectiveness on Sensorineural tinnitus (SNT) patients in advance remains a critical clinical challenge.
Purpose: This study aims to develop and validate a machine learning model based on functional near-infrared spectroscopy (fNIRS) data to predict acupuncture treatment outcomes in SNT patients.
Methods and Analysis: This study will enroll 500 subjects with SNT, with sample size determined via established machine learning feature-to-sample ratio method. Specific brain regions will be scanned using fNIRS pretreatment, collecting data from multiple temporal and frontal lobe channels. Subjects will receive standardized acupuncture over four weeks. Outcomes will be evaluated using validated measures including Tinnitus Severity Grading and Tinnitus Handicap Inventory. Based on treatment responses, subjects will be categorized into “favorable prognosis” or “poor prognosis” groups. The dataset will be randomly split into training (70%) and test (30%) sets. Support Vector Machine (SVM) algorithms will identify features and develop models, with performance evaluated through accuracy, sensitivity, specificity, and AUC.
Anticipated Results: It is anticipated that the fNIRS-based machine learning model will be able to distinguish between patients who will have a favorable response to acupuncture and those who will not, with acceptable accuracy. We expect to identify specific neurofunctional features from the temporal and frontal lobes that are predictive of treatment success. If so, this will provide an objective tool to aid in clinical decision-making and the personalization of tinnitus treatment.
Conclusion: This study represents the first attempt to integrate fNIRS detection with machine learning techniques for predicting acupuncture efficacy in SNT treatment. The methodology addresses several key challenges in acupuncture research through comprehensive data collection and advanced analytical approaches. These findings could potentially enable more personalized treatment approaches for SNT patients and provide a foundation for future studies combining neuroimaging and machine learning in acupuncture research.
Trial Registration: Clinical trials registry (identification code NCT06364670).
Keywords: acupuncture, tinnitus, protocol, functional near-infrared spectroscopy, machine learning
Introduction
Tinnitus is characterized by hearing sounds within the ear without any external sound or electrical stimulus. Research indicates that approximately 20% of adults experience chronic tinnitus, with about a fifth of these cases being severe.1 The impact of tinnitus on individuals varies, affecting both their physical and mental health.2
Sensorineural tinnitus (SNT), the prevalent form of tinnitus, is typically attributed to disorders in the inner ear, auditory nerve, or central auditory system.3 Despite the availability of various treatment approaches, including habituation therapy, cognitive behavioral therapy, sound therapy, pharmacotherapy and hearing aids,4 their effectiveness is often limited, and each has clinical constraints. Consequently, there is no definitive cure for SNT, leading many patients to explore complementary and alternative therapies. Owing to its long history in tinnitus treatment, acupuncture offers advantages such as minimal side effects and cost-effectiveness. An increasing number of clinical studies globally,5–7 as well as systematic reviews and meta-analyses grounded in evidence-based medicine,8,9 generally support the efficacy of acupuncture in treating tinnitus. Despite the overall effectiveness of acupuncture in treating tinnitus, individual responses vary and are influenced by several factors.10 Identifying methods to predict acupuncture’s effectiveness on SNT patients in advance remains a critical clinical challenge. Predicting treatment outcome is a crucial unmet clinical need that would enable more targeted and personalized therapeutic approaches.
The application of ML in acupuncture remains relatively nascent, primarily focused on prescription mining and exploring factors influencing treatment efficacy, acupoint specificity, and acupuncture techniques.11 A particularly promising development in this field has been the use of machine learning (ML) for developing predictive models for acupuncture efficacy on the basis of neural imaging data.12 In 2019, Liu et al13 published a pioneering study using neural imaging data for predicting acupuncture outcomes. Utilizing Support Vector Machine (SVM) for feature identification in white matter fiber connections between the frontal lobe and amygdala in migraine patients at baseline, they successfully forecasted improvements after eight weeks of acupuncture treatment. Similarly, a 2019 study by Harvard University14 utilized SVM ML to establish that functional connectivity in the brain’s default, salience, and executive control networks in chronic low back pain patients could accurately predict acupuncture outcomes after four weeks. Research by Yang et al.15 Employing SVM ML on baseline frontal lobe cortical volume and amygdala fibers in migraine patients identified baseline brain gray matter volume as an objective biomarker for acupuncture response in these patients. These studies underscore the viability and vast potential of utilizing objective, visual neural imaging combined with ML to predict acupuncture efficacy.12
In choosing the integration of neural imaging, our study focuses on functional near-infrared spectroscopy (fNIRS) data. fNIRS, by detecting changes in the intensity of near-infrared light before and after tissue penetration, monitors blood oxygen metabolism and neural activity in specific brain regions. fNIRS offers advantages over functional magnetic resonance imaging (fMRI), particularly its operational silence which is critical for not confounding auditory cortex measurements.16 Recent studies16–19 have revealed significant differences in fNIRS imaging indicators in specific brain regions (eg, the temporal and frontal lobes) in resting tinnitus patients compared with non-tinnitus patients, suggesting that fNIRS is a potential objective neural imaging biomarker for tinnitus diagnosis and prognosis.20
With respect to the selection of the most appropriate ML approach in our study, we adopted an SVM to predict the efficacy of acupuncture treatment in SNT patients. This choice is informed by several compelling advantages that SVM offers within traditional machine learning frameworks. SVM has been established as a leading algorithm in acupuncture efficacy prediction research.21 Its successful application in multiple neural imaging-based ML studies for constructing acupuncture efficacy prediction models13–15 further proves its suitability and validity for our research context. Specifically, in the context of our study where the number of participants (n=500) is moderate relative to the high dimensionality of fNIRS data, SVM is advantageous as it is effective in high-dimensional spaces and less prone to overfitting than more complex models like deep neural networks. Furthermore, the interpretability of the SVM model, through the analysis of feature weights, will allow us to identify the most significant neurophysiological markers from the fNIRS data that predict treatment outcomes.
Although neuroimaging and machine learning show promise, most predictive models for acupuncture efficacy have relied on fMRI, which is costly and not universally accessible. Furthermore, few studies have focused specifically on tinnitus, a condition with high inter-individual variability in treatment response. This study addresses this gap by developing an innovative predictive model that integrates accessible fNIRS neuroimaging with SVM-based machine learning. By doing so, we aim to create a practical, objective tool to forecast individual treatment response to acupuncture in patients with SNT. Specifically, this study aims: (1) to develop and validate a machine learning-based prediction model using pretreatment fNIRS data to predict individual treatment response to acupuncture in patients with SNT and (2) to identify key fNIRS features that contribute most significantly to prediction accuracy, thereby potentially revealing neurophysiological markers of treatment responsiveness.
Methods and Design
Study Design and Trial Registration
This study is designed as a prediction model development study using prospectively collected data from 500 SNT patients. The protocol’s reporting follows the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) guidelines22 (see supplementary file 1), as this study focuses on developing and validating a prediction model via machine learning approaches. Additionally, we follow the Guidelines for Developing and Reporting Machine Learning Predictive Models in Biomedical Research (JMIR Guidelines)23 to ensure comprehensive reporting of our machine learning methodology. The overall trial schedule is detailed in Table 1, and the study’s flow diagram is presented in Figure 1. The study protocol has been registered in the Clinical trials registry under the identification code NCT06364670.
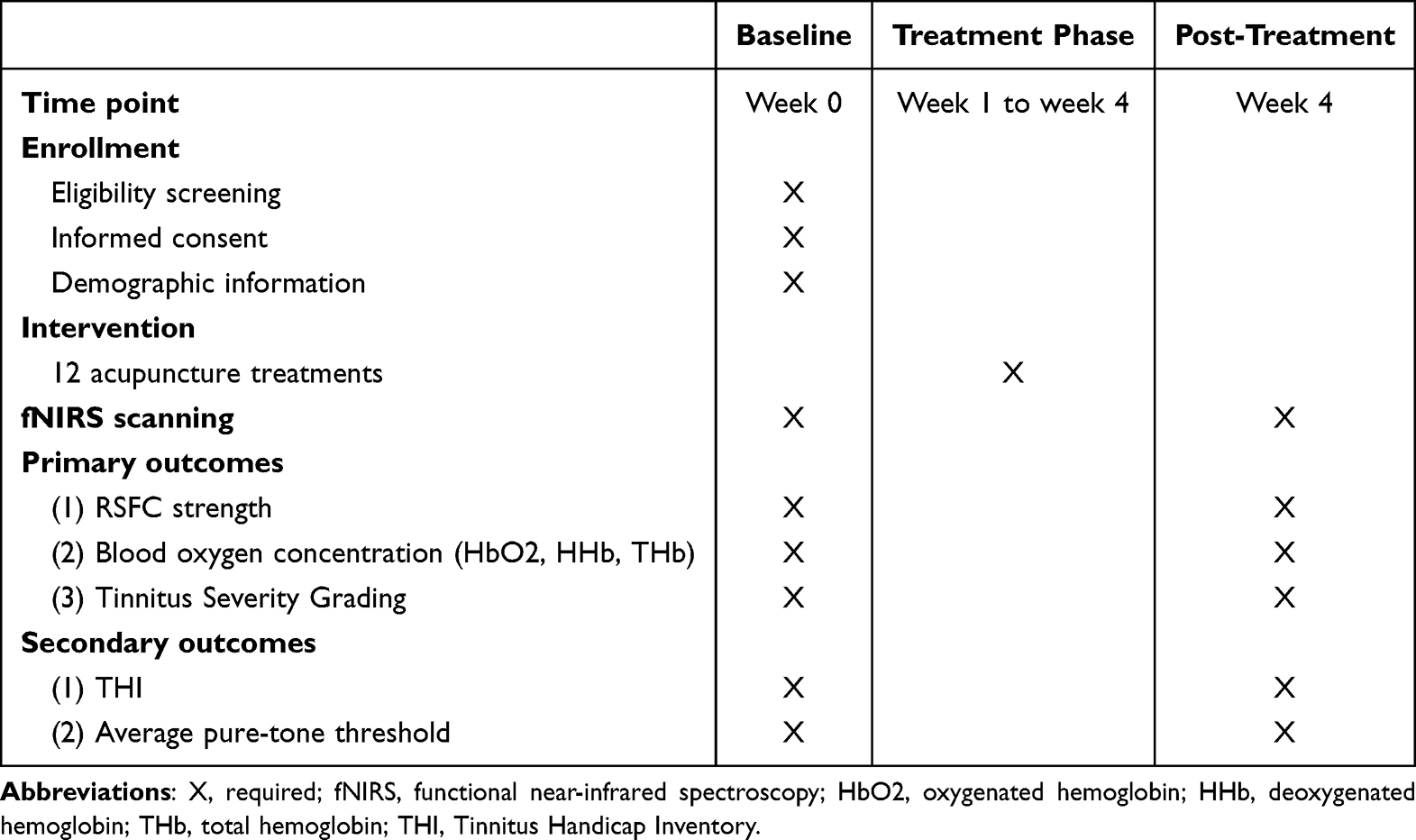 |
Table 1 Schedule of Enrollment, Intervention and Outcome Assessments |
 |
Figure 1 Flow chart of the study process. |
Sample Size Calculation
This project involves the use of SVM-based machine learning to build a predictive model based on selected fNIRS features. The sample size calculation for this machine learning study was primarily based on the feature-to-sample ratio method, which is widely accepted in machine learning research. Our fNIRS system generates multiple hemodynamic parameters (HbO2, HHb, THb) across 52 channels, yielding an initial feature space of approximately 156 features (3 parameters × 52 channels). Through our planned dimensionality reduction pipeline including statistical filtering and principal component analysis (detailed in Feature Selection and Data Reduction), we estimate that approximately 50 potential features will be retained for the final analysis. According to established machine learning principles, which recommend 9–20 samples per feature for stable model performance,24 our initial calculation suggested a minimum requirement of 450 participants (based on 9 samples per feature). Accounting for an anticipated dropout rate of 10% due to various factors, such as incomplete follow-up, poor data quality, or withdrawal from the study, we determined a final target sample size of 500 participants. This sample size ensures sufficient data for both model training (70% of the sample) and testing (30% of the sample) while maintaining robust statistical power for our machine learning analyses.
Participant Recruitment
Potentially eligible participants with SNT will be recruited from the departments of acupuncture, otorhinolaryngology, and neurology at the Third Affiliated Hospital of Zhejiang Chinese Medical University. Primary recruitment strategies include community outreach activities and social media promotion through the official WeChat platform of the research team.
Diagnostic Criteria
In accordance with the diagnostic standards for SNT outlined in the third edition of the “Clinical Practice Guidelines Development Manual”25 by the American Academy of Otolaryngology-Head and Neck Surgery, the criteria include the following:
- The chief complaint of unilateral or bilateral subjective tinnitus, experiencing ringing in the ears or head, intermittent or continuous, manifesting as sounds such as cicada chirping, whistling, rumbling machinery, and wind, with no objective source of these sounds in the surrounding environment;
- Normal hearing or audiograms indicating sensorineural hearing loss;
- Examination of the external auditory canal, tympanic membrane, eustachian tube, etc., via pure-tone audiometry, tympanometry, the acoustic reflex, otoacoustic emissions, MRI of the internal auditory canal, etc., to confirm sensorineural tinnitus;
- Clinical signs: no inflammation in the external auditory canal, an intact tympanic membrane, and no abnormalities on nasopharyngeal examination;
- Tinnitus impacting the patient’s work, study, sleep, life, and emotions to various degrees.
Inclusion Criteria
- Conforming to the diagnostic criteria for sensorineural tinnitus;
- Chronic tinnitus, lasting for ≥3 months;26
- Ages 18 to 60, regardless of gender;
- Right-handed, with normal cognitive levels, able to cooperate with the study’s experimental process;
- Not involved in other clinical trials and sign an informed consent form.
Exclusion Criteria
- Non-sensorineural tinnitus, such as objective tinnitus due to vascular malformations and conductive tinnitus from external or middle ear disorders.
- Neurological changes, such as acoustic neuroma and cranial trauma;
- Neurological diseases affecting cerebral blood oxygen metabolism, such as cerebrovascular diseases;
- Subjects with psychiatric disorders;
- Subjects with comprehension disorders, complete aphasia, and severe cognitive impairments;
- Those unable to tolerate acupuncture for various reasons;
- Pregnant and lactating women.
Blinding Implementation
Owing to the unique nature of acupuncture procedures, it is impossible to blind acupuncturists. However, blinding principles are applied in other trial aspects by assigning specially designated researchers for acupuncture treatment, fNIRS detection, outcome evaluation, and data analysis. This separation of acupuncturists, evaluators, and statistical analysts aims to reduce bias to the greatest extent possible.
Intervention Procedures
Qualifications of Practitioners
This study will employ licensed doctors with extensive clinical experience in acupuncture as practitioners. One month before the study starts, all practitioners will undergo specialized training to standardize acupuncture practices in this study.
Acupoint Selection
The acupoint selection for this study is based on the traditional principle of combining local and distal acupoints, guided by meridian theory as well as our team’s extensive clinical experience and previous research findings.27 The prescribed acupoints are as follows: acupoint prescription: Conger (affected side), Tinggong (affected side), Tinghui (affected side), Waiguan (both sides), Zhongzhu (both sides), Hegu (both sides), Taixi (both sides), Taichong (both sides), and Zusanli (both sides). Notably, “Conger” means sharp ears in Chinese and it is an experience-based acupoint for treating tinnitus and deafness. The use of this experience-based acupoint was identified through extensive clinical practice by our research team.28,29 The acupoint locations mentioned above are summarized in Table 2. Additionally, a diagram of the acupoint locations can be found in Supplementary File 2.
 |
Table 2 Locations of the Selected Acupoints for Treating SNT |
Acupuncture Procedure
Patients lie flat. After routine disinfection of the skin around the ears, φ0.30 mm×50 mm filiform needles (Huatuo brand, Suzhou Medical Supplies Factory Co., Ltd.) were used for the three ear points. Needles are inserted vertically at Tinggong and Tinghui and slightly tilted forward at “Conger” (toward the ear canal). After insertion, needles are slowly inserted to a depth of approximately 1 inch, using the “Qi-guiding and meridian-unblocking needling technique”, a small-amplitude, low-frequency twisting method, with a 180° amplitude and less than 60 twists/min, until the patient feels a distinct sensation of soreness, numbness, and swelling in the ear area, radiating into the ear canal. Regular acupuncture is performed on limb points via φ0.30×40 mm filiform needles, with the lifting-thrusting and twisting reinforcing-reducing methods. The needles were retained for 30 minutes. During retention, warm needle moxibustion is applied to the three ear points, attaching cut moxa sticks to the needle handles and burning two moxa cones. The participants will receive acupuncture treatment three times a week for 4 weeks.
Concomitant Care and Intervention
Participants must avoid any additional tinnitus treatments that could potentially affect the outcomes of the study. This includes, but is not limited to, pharmacological interventions and behavioral therapy. If a participant does engage in other treatments for tinnitus, the researchers must record relevant details for later analysis. Of note, while our exclusion criteria specifically target conditions that could confound fNIRS measurements or acupuncture responses (such as neurological diseases affecting cerebral blood oxygen metabolism), participants with stable, well-controlled chronic conditions (eg, coronary heart disease, chronic gastroenteritis) may continue their established treatments. This decision is based on the principle that these conditions, when stable and well-managed, are unlikely to significantly impact either tinnitus symptoms or the neurophysiological measurements we are assessing. However, any changes in medication regimens during the study period will be carefully documented.
fNIRS Scanning and Data Processing Procedure
fNIRS Scanning
SNT participants undergo a single resting-state fNIRS scan at baseline, before the 4-week course of acupuncture treatment commences (Week 0). This timing ensures that we capture the pre-treatment neurophysiological state without any influence from acupuncture interventions, which is essential for developing a predictive model based on baseline brain activity patterns. Participants will then undergo post-treatment resting-state fNIRS scans to explore correlations between pre/post-treatment fNIRS data and Tinnitus Severity Grading, THI, and average pure-tone thresholds.
The fNIRS detection equipment employed in this project is a portable near-infrared brain imaging system (NirSmart-6000A, Danyang Huichuang Medical Equipment Co., Ltd., China) with two wavelengths (730 and 850 nm) at a sampling rate of 11 Hz. This device non-invasively detects hemoglobin in tissues via near-infrared light of varying wavelengths. The brain areas examined in this project are selected on the basis of the Brodmann cerebral cortex anatomical regions, the most extensively used system currently. Drawing on similar tinnitus studies,16,18,19 the primary monitoring areas are the bilateral temporal lobes and frontal lobe, as defined in the Brodmann cerebral cortex partition system.
The feasibility of an fNIRS-based detection protocol for tinnitus was established in our team’s previous publication.30 Operationally, participants are fitted with an fNIRS optode cap (depicted in Figure 2). The system integrates 17 sources and 16 detectors positioned 2 cm apart, establishing a 52-channel measurement array (channel configuration shown in Figure 3). These optical components are strategically positioned over frontal and temporal cortical territories following established studies.16 Spatial coordinates for sources, detectors, and anatomical reference markers (Fz, T3, T4 per the 10–20 international EEG placement system) are recorded using an electromagnetic 3D digitizer (Patriot, Polhemus, USA) on an anatomically standardized head phantom. These positional data are subsequently converted to MNI space coordinates and mapped onto the MNI standard brain atlas through NirSpace (Danyang Huichuang Medical Equipment Co., Ltd., China). Subsequently, the signal strength of each fNIRS device channel is examined. Should any channel exhibit weak signal strength, immediate steps, such as probe cleaning, adjusting probe clamp tightness, ensuring proper probe-scalp contact, and moving hair obstructing the signal, are taken. If signal weakness persists after adjustment, the signal strength of the affected channels may increase. A green display of channel signal strength signifies adequacy. Participants will receive a 5-minute resting-state fNIRS scan. During this process, they must remain quiet, awake, undisturbed by external factors, and avoid any bodily or head movement.
 |
Figure 2 The fNIRS optode cap wearing diagram. |
 |
Figure 3 The channel configuration of fNIRS. Notes: S1-S17 represent the sources of the fNIRS device. D1-D16 represent the detectors of the fNIRS device. Green squares with numbers represent fNIRS measurement channels. The black outlined arrows indicate the positions of Fz (frontal midline), T3 (left mid-temporal), and T4 (right mid-temporal) according to the 10–20 international EEG placement system, which are used as anatomical reference markers. |
fNIRS Data Processing
Following the fNIRS scan, raw data including signals of oxygenated hemoglobin (HbO2), deoxygenated hemoglobin (HHb) and total hemoglobin (THb) will be exported. Data processing will be performed using MATLAB (R2022a) with the FC-NIRS toolbox. The preprocessing pipeline will include several key steps to ensure data quality. First, raw light intensity data will be converted to optical density changes. Motion artifacts, identified as sharp spikes in the signal, will be corrected using a wavelet-based method. The signals will then be band-pass filtered within the range of 0.01–0.08 Hz to remove physiological noise such as cardiac pulsations and respiratory effects. Finally, the modified Beer-Lambert law will be applied to convert the optical density data into concentration changes of HbO2, HHb, and THb. Channels with persistent poor signal quality after these steps will be excluded from further analysis.
Outcome Measures
Primary Outcomes
- Interregional RSFC strengthInterregional resting-state functional connectivity (RSFC) strength is determined by calculating the Pearson correlation coefficient of the mean time series between pairs of regions of interest (ROIs). This method quantifies the relationship between different channels or ROIs in the fNIRS time series.31 ROIs are defined based on the Montreal Neurological Institute (MNI) coordinate system and Brodmann areas. In line with previous studies,1 the ROIs selected for this research include the dorsolateral prefrontal cortex (dlPFC), primary auditory cortex and ventral medial prefrontal cortex (vmPFC). These brain regions are mapped to our fNIRS channel locations using the NirSpace software, which provides precise spatial registration between optode positions and brain regions.
- Blood oxygen concentrationBlood oxygen concentration in each measurement channel includes the HbO2 concentration, HHb concentration and THb concentration.
- Tinnitus Severity GradingIn accordance with the “Chinese Association of Traditional Chinese Medicine, Otolaryngology Branch’s” guidelines for assessing and determining treatment effectiveness in tinnitus, severity is scored on the basis of the environmental occurrence of tinnitus, its duration, impact on sleep and work, and the patient’s overall subjective experience. Tinnitus Severity Grading is categorized into five levels from mild to severe (I to V), with level I scoring from 1 to 6 points, level II scoring from 7 to 10 points, level III scoring from 11 to 14 points, level IV scoring from 15 to 18 points, and level V scoring from 19 to 21 points.
Secondary Outcomes
- Tinnitus Handicap Inventory (THI) ScoringThe THI scale, a globally recognized tool for assessing tinnitus severity, consists of 25 questions covering emotional, functional, and severity subscales. The total score ranges from 0 to 100, with lower scores reflecting less disability from tinnitus.
- Pure Tone Audiometry Threshold LevelEach participant undergoes pure tone audiometry in a soundproof room at frequencies of 0.25 kHz, 0.5 kHz, 1 kHz, 2 kHz, 4 kHz, and 8 kHz, with the average hearing threshold being calculated.
Treatment Response Criteria and Group Classification
Treatment response criteria will be evaluated based on the change in Tinnitus Severity Grades before and after one course of acupuncture treatment. The response criteria are defined as follows:
- Complete recovery: Total resolution of tinnitus symptoms
- Significant improvement: Reduction in tinnitus severity by two or more grades
- Partial improvement: Reduction in tinnitus severity by one grade
- Non-response: No change in tinnitus severity.
For machine learning analysis, participants will be stratified into two prognostic groups: those who achieve complete recovery, significant improvement, or partial improvement will be classified into the “favorable prognosis group”, whereas those who do not respond will be categorized into the “poor prognosis group”. Notably, while support vector regression or multi-class classification could potentially provide more granular predictions, we chose binary classification for several reasons: (1) it aligns with clinical decision-making where the primary question is whether a patient will benefit from treatment, (2) it provides more robust statistical power with our sample size, and (3) it reduces the complexity of the predictive model, making it more interpretable for clinical application. Nonetheless, a secondary exploratory analysis using support vector regression or ordinal classification will be performed to predict the degree of improvement (eg, complete recovery, significant improvement, partial improvement, non-response).
Furthermore, to test the robustness of our model against different outcome definitions, a sensitivity analysis will be conducted. For this analysis, we will use an alternative binary classification of treatment response based on the change of THI score. A clinically significant improvement will be defined as a reduction of ≥20 points from baseline, a threshold commonly used in tinnitus research. The SVM model will be re-trained and validated using this THI-based grouping, and its performance will be compared with that of the primary model.
Machine Learning Approach Using fNIRS Imaging Data
Development of Training and Test Sets
At the conclusion of an acupuncture treatment cycle, the recovery status of 500 subjects with SNT is assessed. Based on our predefined response criteria discussed above, the subjects are categorized into either the “favorable prognosis group” or the “poor prognosis group”. Following established machine learning practices, the dataset will be randomly split into a training set (70%) and a test set (30%). This means that 70% of subjects from each group are randomly assigned to the machine learning training set to develop an SVM classifier (predictive model) for forecasting acupuncture efficacy in SNT treatment. The remaining 30% form the test set to evaluate the performance of the classifier generated by the training set.
Feature Selection and Data Reduction
Initial feature selection will begin with independent sample t tests comparing the three hemodynamic parameters (HbO2, HHb, and THb) between response groups across all fNIRS channels. Multiple comparisons will be addressed through False discovery rate (FDR) correction. While this approach identifies statistically significant features, it typically yields numerous features that may be redundant or computationally intensive. To enhance model performance, a two-stage dimensionality reduction strategy will be implemented: first, principal component analysis (PCA) will be used to decrease feature dimensions while preserving 95% data variance; second, Recursive Feature Elimination (RFE) will be implemented as a pre-training step. RFE will utilize cross-validation (RFECV) to identify the optimal feature subset, iteratively eliminating less influential features based on their importance rankings.32 To prevent data leakage, this entire feature selection and dimensionality reduction pipeline will be applied separately within each fold of the cross-validation on the training data only.
SVM Model Development and Machine Training
Following the selection of classification features from fNIRS imaging data, training of the SVM classifier begins. The extracted feature vectors are formatted and fed into the SVM classifier, which is ready for future automatic classification of subjects. The SVM classifier will be developed via the LIBSVM package (version 3.25) in MATLAB 2022a. The implementation follows a systematic procedure.
- Format Conversion: Convert feature vectors into the format required by LIBSVM, where the initial numbers (1 or −1) represent the class labels (1 for “Favorable Prognosis Group” and −1 for “Poor Prognosis Group”), and the subsequent values represent the feature values.
- Data preprocessing: Normalize the data to mitigate the impact of scale differences between the input and output data on the classifier’s performance.
- Kernel selection: Select the Radial Basis Function (RBF) as the kernel function, which maps data non-linearly into a higher-dimensional space and is suitable for handling non-linear feature relationships.
- Hyperparameter optimization: Grid search with 10-fold cross-validation will be used to optimize the RBF kernel parameter (γ) and regularization parameter (C). To obtain a more unbiased estimate of the model’s performance on unseen data, a nested cross-validation approach will also be considered. The 10-fold cross-validation process involves partitioning the training set into ten equal parts, with one used as the validation set and the remaining nine used for training.33 This process repeats ten times, with the average Area Under the ROC Curve (AUC) value from these validations being used to assess the model’s performance. Given that the clinical effectiveness rate of acupuncture may lead to an unequal number of participants in the “favorable” and “poor” prognosis groups, we will assess for data imbalance. If a significant imbalance is detected, we will address it by adjusting the class weights (the C parameter) in the SVM algorithm to apply a higher penalty for misclassifying the minority class, ensuring the model is not biased towards the majority group. Furthermore, to evaluate the model’s discriminative ability for each class independently, we will compute class-specific Receiver Operating Characteristic (ROC) curves and the corresponding AUC for both the favorable and poor prognosis groups.
Model Validation and Performance Assessment
The model’s predictive performance will be evaluated via the held-out test set (30%). To ensure robust performance estimation, bootstrap resampling (1000 iterations) will be performed. The performance metrics include the following:
- AUC with 95% confidence intervals
- Accuracy, sensitivity, and specificityAccuracy = (TP + TN) / (FP + FN +TP + TN)Sensitivity = TP / (FN + TP)Specificity = TN / (TN + FP), where TP means True Positives, FP means False Positives, TN means True Negatives, and FN means False Negatives.
- Positive and negative predictive values
- F1-score and Matthews correlation coefficient
- Balanced accuracy and class-specific ROC-AUC
In addition, to provide a comparative context for the SVM model’s performance, it will be benchmarked against at least one simpler model (eg, logistic regression) and another common machine learning algorithm (eg, random forest).
Statistical Analysis
Statistical analyses will be conducted using SPSS 25.0 (IBM Corp, Armonk, NY, USA) and Python 3.8 with scikit-learn 0.24.2 for machine learning algorithms. Two-tailed tests will be applied, with statistical significance defined as P<0.05. Normally distributed continuous variables (evaluated via Shapiro–Wilk test) will be reported as mean ± standard deviation, non-normal data as median (interquartile range), and categorical variables as frequency (percentage). Missing data, which may include individual fNIRS channel recordings due to technical issues or clinical outcome scores from participant dropout, will be handled using Multiple Imputation by Chained Equations (MICE) for missing data, with sensitivity analyses conducted via complete case analysis and pattern mixture models; cases with >20% missing data will be excluded. For correlation analysis, Pearson’s or Spearman correlation coefficients will be used as appropriate on the basis of the data distribution.
To address potential heterogeneity within the patient cohort, subgroup analyses will be performed to evaluate the robustness of the predictive model. Specifically, the test set will be stratified based on key baseline characteristics including age, sex, tinnitus duration, baseline tinnitus severity (THI score), and the presence of significant comorbidities such as the degree of hearing loss (based on pure-tone audiometry) and emotional distress (based on THI subscale scores). The performance of the final SVM model will be evaluated separately within each subgroup by calculating accuracy, AUC, sensitivity, and specificity. This will allow us to assess whether the model’s predictive power is consistent across these clinically relevant populations. Additionally, correlation analyses in SNT patients will examine potential associations between pre-to-post acupuncture changes in resting-state fNIRS data and corresponding shifts in THI scores and pure-tone thresholds, exploring possible correlations of tinnitus severity and hearing level variations with altered functional connectivity in relevant brain regions.
Ethics and Dissemination
This trial will be conducted in compliance with the Declaration of Helsinki. Ethics approval was obtained from the Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (approval no: ZSLL-KY-2023-011-01). Researchers will comprehensively explain this study to all participants prior to enrollment, including its objectives, anticipated benefits, potential risks and research procedures. The participants will maintain complete autonomy in their decision regarding study participation. Participants who agree to participate in the study will be requested to sign informed consents to ensure the understanding of their involvement. Throughout the study duration, strict confidentiality protocols will be maintained to protect all personal and medical information. The results of this study will be submitted for publication in peer-reviewed publications. To promote transparency and reproducibility, the analysis code used in this study will be made available upon reasonable request or through a public repository such as GitHub upon publication.
Results
Since this is a study protocol without completed results, we can only anticipate the results as follows. We anticipate that the SVM model will successfully classify patients into “favorable” and “poor” prognosis groups with a clinically acceptable level of accuracy on the independent test set. The model is expected to identify key predictive features related to baseline functional connectivity within and between the auditory cortex, prefrontal cortex, and other non-auditory regions previously implicated in tinnitus. Subgroup analyses are expected to show consistent model performance across different patient demographics, though some variability may be observed based on tinnitus duration or severity. Furthermore, we hypothesize that changes in the identified predictive fNIRS features from pre- to post-treatment will correlate with clinical improvements as measured by Tinnitus Severity Grading and THI scores.
Discussion
To date, the exact mechanisms underlying tinnitus remain somewhat unclear, but there is growing evidence that increased neural activity and connectivity in the brain’s cortical centers are closely linked to tinnitus onset.34 Studies and clinical trials have revealed that changes in the central nervous system are associated with tinnitus.17,35 These changes occur in different parts of the auditory pathway, including the auditory and non-auditory cortices (eg, the frontal lobe).36 Some experts suggest that tinnitus may be caused by abnormal activities in overlapping brain networks, contributing to tinnitus’s varied symptoms.37 The activation of the auditory cortex during a resting state is believed to be correlated with the loudness of tinnitus. In addition, simultaneous activation of the non-auditory cortex is associated with other related symptoms, such as irritability and distress.38 Therefore, resting-state functional connectivity (RSFC) is selected as the core neuroimaging metric. This methodology derives from synchronized low-frequency blood oxygen level-dependent (BOLD) signal fluctuations observed in functionally linked brain regions.39 Within cognitive neuroscience, RSFC has gained prominence for three key applications: 1) detecting functional connectivity alterations in neuropsychiatric cohorts, 2) mapping brain network architecture, and 3) probing brain-behavior correlation patterns.40 Its validity as a functional connectivity measurement tool has been replicated across independent investigations.39,41
Notably, this project integrates fNIRS detection with cutting-edge machine learning techniques to predict the effectiveness of acupuncture in treating SNT for the first time. While previous neuroimaging studies have utilized fMRI to investigate the central mechanisms of acupuncture, our study leverages the practical advantages of fNIRS. fMRI studies have successfully identified acupuncture-induced changes in brain regions such as the limbic system and default mode network. Our fNIRS-based approach complements this body of work by focusing on cortical hemodynamics with high temporal resolution and patient comfort, providing a different yet valuable perspective on the neurophysiological markers of treatment response. The SVM algorithm will be used to process fNIRS imaging data from SNT patients to create a predictive model of treatment efficacy. Of note, we selected SVM for several specific reasons relevant to our study context. First, this choice balances performance with interpretability for our moderate-sized dataset. Second, SVM is well-suited for high-dimensional data like fNIRS and has a strong track record in neuroimaging-based prediction. Third, SVM offers superior interpretability, allowing clinicians to understand which features drive predictions, which is a crucial consideration in medical applications. However, we acknowledge that more advanced algorithms, such as deep learning models (eg, Convolutional Neural Networks) or other ensemble methods (eg, Random Forest, Gradient Boosting), could potentially capture more complex, non-linear patterns in the data. These models often require larger datasets to train effectively without overfitting. Therefore, while SVM represents a robust and appropriate choice for this study, we recognize the exploration of these alternative algorithms as a valuable direction for future research when larger datasets become available.
This study innovatively employs SVM-based machine learning to develop a model for predicting the effectiveness of acupuncture in treating SNT. If successful, this predictive model is expected to enable doctors to be integrated into clinical workflows as a decision-support system. For instance, a clinician could use the prediction to manage patient expectations, justify a course of acupuncture for likely responders, or recommend alternative therapies for those predicted to have a poor prognosis, thereby optimizing resource allocation and improving patient outcomes. This approach is in line with the “4P” medical model: Predictive, Preventive, Personalized, and Participatory. The 4P model represents the future direction of medicine, predicting individual susceptibility before disease onset, offering targeted preventive measures, and formulating personalized treatment strategies on the basis of each patient’s unique conditions.42 In this context, machine learning (ML) has emerged as a potent tool for implementing the 4P model,43,44 with significant potential in addressing critical clinical challenges. As a key subset of artificial intelligence (AI), ML allows computers to learn from vast amounts of existing data through diverse algorithms and apply these insights to analyze and predict other data.45 Commonly used to identify predictive biomarkers, ML facilitates predictive diagnostics, targeted prevention, and personalized medical services.46 Research published in Science magazine reveals that ML-derived predictive results (model predictions) tend to be more objective and precise than expert opinions (experience predictions).47 This study, therefore, represents a novel contribution to research philosophy.
Despite the innovative approach and rigorous methodology of this study, several limitations should be acknowledged. First, although fMRI offers superior spatial resolution and access to deeper brain structures, we chose fNIRS for its practical advantages in tinnitus research—especially its minimal acoustic interference and greater patient comfort. These features are critical when studying auditory-related conditions. Nonetheless, the limited spatial resolution and penetration depth of fNIRS remain a limitation. Second, the 4-week treatment duration, although consistent with clinical practice, may not capture the full therapeutic potential of acupuncture, which sometimes requires longer treatment periods for optimal effectiveness. Future studies should consider more extended treatment and follow-up periods to assess the sustainability of outcomes. Third, our machine learning approach using SVM, while well established, may not capture all possible non-linear relationships in the data; future studies might benefit from comparing multiple advanced algorithms. Fourth, our patient sample, while reflecting a real-world clinical population, will likely exhibit heterogeneity in comorbidities such as hearing loss and associated emotional distress, which may act as confounding variables. While we plan to conduct subgroup analyses, this heterogeneity could influence the model’s performance. Fifth, by dichotomizing the outcome into “favorable” and “poor” prognosis, we lose some granularity. While this approach enhances the robustness of the binary classification model, future work could employ multi-class classification or support vector regression to predict the specific level of improvement, which may offer more nuanced clinical utility. A further limitation is the inherent risk of overfitting, even with a sample size guided by feature-to-sample ratios; thus, the generalizability of our model will need to be confirmed through external validation on an independent dataset in future studies.
Conclusion
This study protocol outlines the development and validation of a novel predictive model integrating fNIRS neuroimaging and machine learning to forecast individual responses to acupuncture for SNT. By identifying objective, pretreatment neurophysiological markers, this research has the potential to significantly advance the personalization of tinnitus management. If successful, the resulting model will provide clinicians with a valuable tool to optimize treatment strategies, improve patient outcomes, and pave the way for future investigations into the neural mechanisms of acupuncture. The findings will be disseminated through peer-reviewed publication to contribute to the growing field of predictive and personalized medicine.
Generative AI Statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Abbreviations
SNT, sensorineural tinnitus; ML, machine learning; SVM, Support Vector Machine; fNIRS, functional near-infrared spectroscopy; fMRI, functional magnetic resonance imaging; HbO2, oxygenated hemoglobin; HHb, deoxygenated hemoglobin; THb, total hemoglobin; THI, Tinnitus Handicap Inventory; RFE, Recursive Feature Elimination; RBF, Radial Basis Function.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (approval no: ZSLL-KY-2023-011-01). All participants will be fully informed of the study before enrollment and sign an informed consent form. Participants have the right to request withdrawal from the study at any time.
Consent for Publication
All of the material, including figures and tables, is owned by the authors and is authorized for publication. Figure 2 masks facial feature information.
Acknowledgments
The authors thank all those involved in the study, including practitioners, assessors and participants.
Funding
This work was supported by the Zhejiang Province Public Welfare Technology Application Research (Zhejiang Provincial Natural Science Foundation of China under Grant No. LTGY23H270003). The funder had no role in the design, execution, or reporting of the study.
Disclosure
The authors declare no potential conflicts of interest related to commercial or financial affiliations in this research.
References
1. Elgoyhen AB, Langguth B, De Ridder D, Vanneste S. Tinnitus: perspectives from human neuroimaging. Nat Rev Neurosci. 2015;16(10):632–642. doi:10.1038/nrn4003
2. McCormack A, Edmondson-Jones M, Somerset S, Hall D. A systematic review of the reporting of tinnitus prevalence and severity. Hear Res. 2016;337:70–79. doi:10.1016/j.heares.2016.05.009
3. Møller AR. Sensorineural tinnitus: its pathology and probable therapies. Int J Otolaryngol. 2016;2016:1–13. doi:10.1155/2016/2830157
4. Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: tinnitus executive summary. Otolaryngol–Head Neck Surg. 2014;151(4):533–541. doi:10.1177/0194599814547475
5. Li C, Mao W, Zhang L, et al. Tongdu tiaoshen acupuncture for subjective tinnitus:a randomized controlled trial. Zhongguo Zhen Jiu. 2024;44(6):648–652. doi:10.13703/j.0255-2930.20230808-k0001
6. Doi MY, Borges R, Tano SS, Marchiori LLM, Schultz AR. Effectiveness of acupuncture therapy as treatment for tinnitus: a randomized controlled trial. Braz J Otorhinolaryngol. 2016;82(4):458–465. doi:10.1016/j.bjorl.2016.04.002
7. Naderinabi B, Soltanipour S, Nemati S, Saberi A, Parastesh S. Acupuncture for chronic nonpulsatile tinnitus: a randomized clinical trial. Caspian J Intern Med. 2018;9(1):38–45. doi:10.22088/cjim.91.38
8. Wu Q, Wang J, Han D, Hu H, Gao H. Efficacy and safety of acupuncture and moxibustion for primary tinnitus: a systematic review and metaanalysis. Am J Otolaryngol. 2023;44(3):103821. doi:10.1016/.amjoto.2023.103821
9. Huang K, Liang S, Chen L, Grellet A. Acupuncture for tinnitus: a systematic review and meta-analysis of randomized controlled trials. Acupunct Med. 2021;39(4):264–271. doi:10.1177/0964528420938380
10. Lin TY, Yang SW, Lee YS, et al. Analysis of factors influencing the efficiency of acupuncture in tinnitus patients. Evid-Based Compl Altern Med ECAM. 2019;2019:1318639. doi:10.1155/2019/1318639
11. Liang J, Han MY, Wang CB, Lü XL, Sun ZR, Yin HN. Research progress in the integration of machine learning and acupunctology. Zhen Ci Yan Jiu. 2021;46(6):460–463. doi:10.13702/j.1000-0607.20210160
12. Yin T, Ma P, Tian Z, et al. Machine learning in neuroimaging: a new approach to understand acupuncture for neuroplasticity. Neural Plast. 2020;2020:1–14. doi:10.1155/2020/8871712
13. Liu J, Mu J, Chen T, Zhang M, Tian J. White matter tract microstructure of the mPFC‐amygdala predicts interindividual differences in placebo response related to treatment in migraine patients. Hum Brain Mapp. 2019;40(1):284–292. doi:10.1002/hbm.24372
14. Tu Y, Ortiz A, Gollub RL, et al. Multivariate resting-state functional connectivity predicts responses to real and sham acupuncture treatment in chronic low back pain. Neuroimage Clin. 2019;23:101885. doi:10.1016/j.nicl.2019.101885
15. Yang XJ, Liu L, Xu ZL, et al. Baseline brain gray matter volume as a predictor of acupuncture outcome in treating migraine. Front Neurol. 2020;11:111. doi:10.3389/fneur.2020.00111
16. Shoushtarian M, Alizadehsani R, Khosravi A, et al. Objective measurement of tinnitus using functional near-infrared spectroscopy and machine learning. PLoS One. 2020;15(11):e0241695. doi:10.1371/journal.pone.0241695
17. San Juan J, Hu XS, Issa M, et al. Tinnitus alters resting state functional connectivity (RSFC) in human auditory and non-auditory brain regions as measured by functional near-infrared spectroscopy (fNIRS). PLoS One. 2017;12(6):e0179150. doi:10.1371/journal.pone.0179150
18. Issa M, Bisconti S, Kovelman I, Kileny P, Basura GJ. Human auditory and adjacent nonauditory cerebral cortices are hypermetabolic in tinnitus as measured by functional near-infrared spectroscopy (fNIRS). Neural Plast. 2016;2016:1–13. doi:10.1155/2016/7453149
19. Schecklmann M, Giani A, Tupak S, et al. Functional near-infrared spectroscopy to probe state- and trait-like conditions in chronic tinnitus: a proof-of-principle study. Neural Plast. 2014;2014:1–8. doi:10.1155/2014/894203
20. Basura GJ, Hu X, Juan JS, Tessier A, Kovelman I. Human central auditory plasticity: a review of functional near‐infrared spectroscopy (fNIRS) to measure cochlear implant performance and tinnitus perception. Laryngoscope Investig Otolaryngol. 2018;3(6):463–472. doi:10.1002/lio2.185
21. Yin T, He ZX, Sun RR, et al. Progress and prospect of machine learning in research of acupuncture and moxibustion. Zhongguo Zhen Jiu. 2020;40(12):1383–1386. doi:10.13703/j.0255-2930.20191026-0002
22. Collins GS, Reitsma JB, Altman DG, Moons KGM. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350(jan07 4):g7594. doi:10.1136/bmj.g7594
23. Luo W, Phung D, Tran T, et al. Guidelines for developing and reporting machine learning predictive models in biomedical research: a multidisciplinary view. J Med Internet Res. 2016;18(12):e323. doi:10.2196/jmir.5870
24. Riley RD, Snell KI, Ensor J, et al. Minimum sample size for developing a multivariable prediction model: PART II - binary and time-to-event outcomes. Stat Med. 2019;38(7):1276–1296. doi:10.1002/sim.7992
25. Rosenfeld RM, Shiffman RN, Robertson P. Clinical practice guideline development manual, third edition: a quality‐driven approach for translating evidence into action. Otolaryngol–Head Neck Surg. 2013;148(S1). doi:10.1177/0194599812467004
26. Zenner HP, Delb W, Kröner-Herwig B, et al. on the interdisciplinary S3 guidelines for the treatment of chronic idiopathic tinnitus. Hno. 2015;63(6):419–427. doi:10.1007/s00106-015-0011-z
27. Song Y, Zhao X, Wang L. Study on acupoint selection patterns and theoretical basis of acupuncture treatment for primary tinnitus based on data mining technology. J Tianjin Univ Tradit Chin Med. 2022;41(6):723–727.
28. Wu Q, Han D, Lin L, Gao H. Experience introduction of GAO hong in treating tinnitus with method of guiding qi and unblocking collaterals. New Chinese Med. 2022;54(10):219–222. doi:10.13457/j.cnki.jncm.2022.10.052
29. Shao L, Hu H, Lv H, Wang Z, Gao H. Experience analysis of GAO hong in treating sensorineural deafness with method of guiding qi and unblocking collaterals. Zhejiang Journal Integr Tradit Chin Westem Med. 2021;31(3):281–283.
30. Hu H, Lin X, Fang L, Li Y, Gao H. Evaluating the efficacy and underlying mechanisms of acupuncture for chronic subjective tinnitus using functional near-infrared spectroscopy: study protocol for a randomized controlled trial. JPR. 2023;16:3367–3378. doi:10.2147/JPR.S433048
31. Song H, Chen L, Gao R, et al. Automatic schizophrenic discrimination on fNIRS by using complex brain network analysis and SVM. BMC Med Inf Decis Making. 2017;17(Suppl 3):166. doi:10.1186/s12911-017-0559-5
32. Escanilla NS, Hellerstein L, Kleiman R, Kuang Z, Shull JD, Page D. Recursive feature elimination by sensitivity testing. Proc Int Conf Mach Learn Appl. 2018;2018:40–47. doi:10.1109/ICMLA.2018.00014
33. Jung Y, Hu J. A K -fold averaging cross-validation procedure. J Nonparam Stat. 2015;27(2):167–179. doi:10.1080/10485252.2015.1010532
34. Engineer ND, Møller AR, Kilgard MP. Directing neural plasticity to understand and treat tinnitus. Hear Res. 2013;295:58–66. doi:10.1016/j.heares.2012.10.001
35. Husain FT, Schmidt SA. Using resting state functional connectivity to unravel networks of tinnitus. Hear Res. 2014;307:153–162. doi:10.1016/j.heares.2013.07.010
36. Lanting C, WoźAniak A, Van Dijk P, Langers DRM. Tinnitus- and task-related differences in resting-state networks. In: Van Dijk P, Başkent D, Gaudrain E, De Kleine E, Wagner A, Lanting C editors. Physiology, Psychoacoustics and Cognition in Normal and Impaired Hearing. Vol 894. Advances in Experimental Medicine and Biology. Springer International Publishing; 2016:175–187. doi:10.1007/978-3-319-25474-6_19
37. De Ridder D, Vanneste S, Weisz N, et al. An integrative model of auditory phantom perception: tinnitus as a unified percept of interacting separable subnetworks. Neurosci Biobehav Rev. 2014;44:16–32. doi:10.1016/j.neubiorev.2013.03.021
38. Deco G, Jirsa VK, McIntosh AR. Emerging concepts for the dynamical organization of resting-state activity in the brain. Nat Rev Neurosci. 2011;12(1):43–56. doi:10.1038/nrn2961
39. Fox MD, Raichle ME. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev Neurosci. 2007;8(9):700–711. doi:10.1038/nrn2201
40. Greicius M. Resting-state functional connectivity in neuropsychiatric disorders. Curr Opin Neurol. 2008;21(4):424–430. doi:10.1097/WCO.0b013e328306f2c5
41. Damoiseaux JS, Greicius MD. Greater than the sum of its parts: a review of studies combining structural connectivity and resting-state functional connectivity. Brain Struct Funct. 2009;213(6):525–533. doi:10.1007/s00429-009-0208-6
42. Golubnitschaja O, Kinkorova J, Costigliola V. Predictive, preventive and personalised medicine as the hardcore of ‘horizon 2020’: EPMA position paper. EPMA J. 2014;5(1):6. doi:10.1186/1878-5085-5-6
43. Barrett M, Boyne J, Brandts J, et al. Artificial intelligence supported patient self-care in chronic heart failure: a paradigm shift from reactive to predictive, preventive and personalised care. EPMA J. 2019;10(4):445–464. doi:10.1007/s13167-019-00188-9
44. Garnica O, Gómez D, Ramos V, Hidalgo JI, Ruiz-Giardín JM. Diagnosing hospital bacteraemia in the framework of predictive, preventive and personalised medicine using electronic health records and machine learning classifiers. EPMA J. 2021;12(3):365–381. doi:10.1007/s13167-021-00252-3
45. Deo RC. Machine learning in medicine. Circulation. 2015;132(20):1920–1930. doi:10.1161/CIRCULATIONAHA.115.001593
46. Kinkorová J, Topolčan O. Biobanks in the era of big data: objectives, challenges, perspectives, and innovations for predictive, preventive, and personalised medicine. EPMA J. 2020;11(3):333–341. doi:10.1007/s13167-020-00213-2
47. Athey S. Beyond prediction: using big data for policy problems. Science. 2017;355(6324):483–485. doi:10.1126/science.aal4321
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Pain and Function in Patients with Nonspecific Low Back Pain: Study Protocol for an Up-to-Date Systematic Review and Meta-Analysis
Li Y, Liu Y, Zhang L, Zhai M, Li L, Yuan S, Li Y
Journal of Pain Research 2022, 15:1379-1387
Published Date: 10 May 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Effectiveness of Pharmacopuncture in Patients with Lumbar Spinal Stenosis: A Protocol for a Multi-Centered, Pragmatic, Randomized, Controlled, Parallel Group Study
Lee JY, Park KS, Kim S, Seo JY, Cho HW, Nam D, Park Y, Kim EJ, Lee YJ, Ha IH
Journal of Pain Research 2022, 15:2989-2996
Published Date: 23 September 2022
Comparative Efficacy of Different Acupuncture-Related Therapies for Primary Tinnitus: A Systematic Review and Network Meta-Analysis Protocol
Yang L, Li X, Fang L, Wu L, Hu H, Cheng Y
Journal of Pain Research 2023, 16:2217-2225
Published Date: 29 June 2023