Back to Journals » Journal of Pain Research » Volume 16
Comparative Efficacy of Different Acupuncture-Related Therapies for Primary Tinnitus: A Systematic Review and Network Meta-Analysis Protocol
Authors Yang L, Li X, Fang L, Wu L ![]() , Hu H
, Hu H ![]() , Cheng Y
, Cheng Y
Received 31 March 2023
Accepted for publication 14 June 2023
Published 29 June 2023 Volume 2023:16 Pages 2217—2225
DOI https://doi.org/10.2147/JPR.S414622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Liping Yang,1,* Xingling Li,1,* Lianqiang Fang,1 Lei Wu,1,2 Hantong Hu,1,2 YingYing Cheng1
1Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 2Department of Neurobiology and Acupuncture Research, The Third Clinical Medical College, Zhejiang Chinese Medical University, Key Laboratory of Acupuncture and Neurology of Zhejiang Province, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: YingYing Cheng; Hantong Hu, Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 219 Moganshan Road, Hangzhou City, People’s Republic of China, Email [email protected]; [email protected]
Background: Acupuncture is considered as a potential treatment option for primary tinnitus, as there is a lack of conventional therapies with well-established efficacy. However, there are limited studies that compare the effectiveness of different acupuncture therapies. Thus, this systematic review and network meta-analysis protocol aims to compare the efficacy of various acupuncture-related therapies for primary tinnitus, and determine the optimal treatment.
Methods: A comprehensive search of 10 representative databases will be conducted to identify eligible randomized controlled trials (RCTs) regarding multiple acupuncture-related therapies for primary tinnitus. Two independent researchers will extract data individually, and the methodological quality of each RCT will be assessed using Cochrane’s risk of bias 2.0 tool. Standard pairwise meta-analysis and Bayesian network meta-analysis will be conducted, and WinBUGS V.1.4.3 and R 3.6.2 software will be adopted to synthesize network data and generate relevant graphs. Subgroup analyses, sensitivity analyses, and assessment of publication bias will be conducted as appropriate.
Discussion: This study’s results are anticipated to identify the optimal acupuncture technique for treating primary tinnitus, thereby providing evidence-based clinical decisions for patients and clinicians to select the most effective acupuncture treatment.
Prospero Registration Number: CRD42023399621.
Keywords: acupuncture, moxibustion, tinnitus, meta-analysis, protocol
Introduction
Tinnitus is characterized by the perception of sound without external sound sources. Primary tinnitus is defined as tinnitus without definite causes. This type of tinnitus is often used to describe idiopathic tinnitus for which there is no identifiable cause.1 Primary tinnitus is considered to be a separate entity from secondary tinnitus, which defines tinnitus explicitly associated with a specific medical condition. Primary tinnitus may manifest with or without comorbid hearing loss and mental disorders, and its onset may be acute or persistent. And its causes are often related to stress, hearing loss, and aging.
As a common medical condition, epidemiological research reported that tinnitus affects 10–15% of the general population but is more prevalent in older persons.1 In addition, an up-to-date systematic review2 on the global prevalence and incidence of tinnitus published in 2023 suggests that tinnitus affects more than 740 million adults globally and is perceived as a major problem by more than 120 million people. Characterized by a persistent and frequently upsetting impression of sound, tinnitus can have a negative impact on an individual’s quality of life, causing psychological comorbidities such as sleep disorders, anxiety, and depression.
Regarding the treatment of primary tinnitus, conventional therapeutic therapies recommended by related guidelines mainly include medications, sound therapy, hearing aids, cognitive-behavioral therapy (CBT), and dietary changes and supplements. However, the efficacy of these therapies varies from person to person and frequently only offers modest relief. As a result, acupuncture is gaining popularity as an alternative therapy that an increasing number of tinnitus patients are seeking help. Moreover, despite the fact that more high-level evidence regarding the efficacy of acupuncture for tinnitus is warranted, acupuncture has been regarded as a potential treatment option for tinnitus in some clinical guidelines of tinnitus treatment.1,3
Acupuncture is a traditional Chinese medicine (TCM) therapy to treat various diseases through the insertion of needles along specific meridians or pathways. The precise placement of these needles varies depending on the particular disease being targeted. Acupuncture is often combined with other relevant techniques such as moxibustion, electric stimulation, and acupressure. In recent decades, acupuncture has attracted interest as a feasible treatment option for primary tinnitus. Numerous systematic reviews and meta-analysis studies4–8 have been conducted to evaluate the efficacy of acupuncture for tinnitus. The majority of these studies have shown that acupuncture is effective in alleviating tinnitus symptoms and has a favorable safety profile. Although the exact mechanisms responsible for the therapeutic effects of acupuncture in treating tinnitus have yet to be fully elucidated, previous studies suggested that acupuncture could significantly improve circulation in the inner ear9 and promote neuroplasticity of central auditory pathway.10 Furthermore, acupuncture could regulate neuronal changes in both auditory and extra-auditory brain networks, and it can also influence the somatosensory system.11 These multifaceted effects are likely to contribute to the potential mechanisms underlying acupuncture’s efficacy in alleviating tinnitus. In clinical practice, various modalities of acupuncture are frequently employed in clinical practice for tinnitus treatment, including manual acupuncture (MA), electroacupuncture (EA), warm needling, acupoint injection, and so on. Moreover, these modalities are usually utilized alone or in combination. Despite the wide use of acupuncture for primary tinnitus, there is a great lack of studies that aims to compare the efficacy of various acupuncture therapies.
In the field of evidence-based medicine, network meta-analysis (NMA) serves as a validated tool to compare multiple therapies indirectly through a network of trials, providing a more comprehensive evaluation of the relative efficacy of different treatments.12 Notably, NMA overcomes the limitations of conventional meta-analyses, which only allow for the comparison of treatments directly compared in head-to-head trials. In past decades, network meta-analysis has become increasingly popular in the medical field, especially in conditions where head-to-head trials are limited.13 In the context of tinnitus treatment by acupuncture-related therapies, network meta-analysis provides a methodology to determine optimal acupuncture treatment, thereby informing evidence-based decisions for clinicians and tinnitus patients.
Thus, we conduct this systematic review and NMA study to compare the efficacy of different acupuncture-related therapies for primary tinnitus and determine the optimal acupuncture treatment.
Methods
We strictly undertake this NMA study in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines14,15 (uploaded in Supplementary File). Moreover, we have registered this study on the PROSPERO registry with the identification number CRD42023399621, thereby ensuring research transparency.
Databases and Search Strategies
To comprehensively search for qualified acupuncture trials for treating tinnitus, a total of 10 databases, including six English-language databases (PubMed, Cochrane Library, Web of Science, Embase, Scopus, CINAHL) and four Chinese-language databases (China National Knowledge Infrastructure, Wanfang database, Chinese Biomedical Literature Database, and VIP Database for Chinese Technical Periodicals), will be searched from the inception of each database to March 2023. The retrieval strategies will incorporate medical subject headings terms (eg, MeSH for PubMed), keywords, and free terms. These search terms will consist of three major categories, namely the medical conditions (eg, ‘tinnitus’, “ringing ear”, and ‘primary tinnitus’), interventions (eg, “acupuncture”, “manual acupuncture”, “electroacupuncture”, “fire needling”, and “warm needling”), and study designs (eg, “randomized controlled trial”, “RCT”, and “clinical trial”). The specific search strategy employed for PubMed is provided in Table 1, which will be adjusted for the remaining databases.
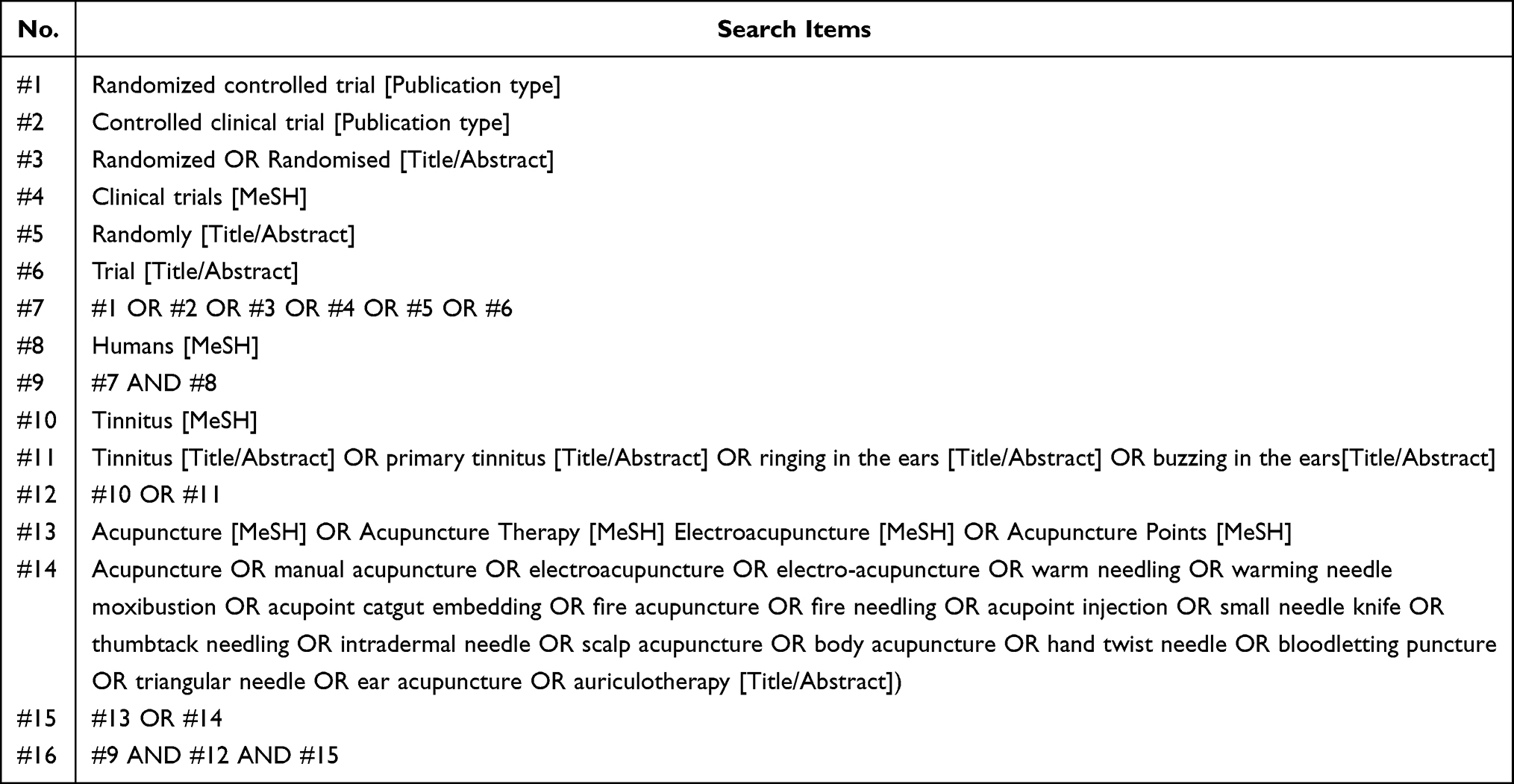 |
Table 1 Search Strategies in PubMed |
In addition, a grey literature search will be conducted to find clinical trials with unpublished data on five major clinical trial registry platforms, which include the National Institute of Health Clinical Registry, the Chinese Clinical Trial Registry, the Australian New Zealand Clinical Trials Registry, the International Clinical Trial Registration Platform (ICTRP), and the ISRCTN registry. Primary investigators of any identified ongoing trials will be contacted by email to request the latest data.
Eligibility Criteria
Population, Interventions, Comparisons, Outcomes and Study design (PICOS)16 as a framework to formulate eligibility criteria of the included studies in a systematic review and meta-analysis are carefully designed as follows.
Population
The eligible population in this NMA will be patients diagnosed with tinnitus, without any restrictions on gender, age, or disease duration. Moreover, the diagnostic criteria of tinnitus (eg, criteria proposed by relevant clinical guidelines1,3,17) or eligibility criteria of participants must be reported in the original study.
Interventions
The eligible types of intervention in the experimental group can be a single acupuncture method, the combined use of two or more acupuncture-related techniques, or acupuncture combined with other active therapies that are the same as those in the control group. With references to similar meta-analysis studies,18–20 acupuncture-related therapies in our study are defined as invasive acupuncture that involves needle insertion at specific points, including MA, EA, warm needling, fire acupuncture, bloodletting puncture, acupoint catgut embedding, acupoint injection, and so on. Therefore, other acupuncture types without needle insertion (eg, acupressure, cupping, laser acupuncture, and pressed studs) will be excluded.
Comparisons
Eligible types of comparators in the control group can be guideline-recommended active therapies for tinnitus (eg, Western medication, sound therapy, CBT, education and counseling, dietary changes and supplements), acupuncture therapies that differ from those used in the treatment group, and any inactive interventions such as waiting list, blank control, sham acupuncture, and placebo.
Outcomes
At least one of the following outcomes should be reported in potentially eligible studies for selection.
Primary Outcome
The primary outcome of this NMA is tinnitus symptom severity, which can be measured using visual analogue scales (VAS) and/or validated standardized questionnaires, including but not limited to the Tinnitus Functional Index (TFI), Tinnitus Handicap Inventory (THI), Tinnitus Reaction Questionnaire (TRQ), Tinnitus Questionnaire (TQ), and Tinnitus Severity Scale.21
Secondary Outcomes
1. Adverse events.
The number of adverse events associated with acupuncture will be analyzed.
2. Response rate.
The response rate is defined as the percentage of patients with a full or partial response in the total number of patients accrued.
3. Tinnitus-associated psychological status (eg, depression and anxiety).
They can be measured by standardized questionnaires, such as Beck Depression Inventory (BDI), the Hamilton Depression Scale (HAMD), Hamilton Anxiety Scale (HAMA), and Self-Assessment Scale for Anxiety (SAS).
4. Tinnitus-associated sleeping disturbance.
It can be measured by standardized questionnaires, including but not limited to the Epworth Sleepiness Scale (ESS), the Pittsburgh Sleep Quality Index (PSQI), and the Global Sleep Assessment Questionnaire (GSAQ).
Study Designs
For this NMA, only randomized controlled trials (RCTs) will be eligible. Case studies, reviews, non-RCTs, and other study types will not be accepted. In the case of three-arm studies, data from these studies will be split and processed in the pairwise meta-analysis, which is a widely recognized method.22
Safety Evaluation
To assess the safety of acupuncture in contrast to control treatments, a meta-analysis will be conducted by combining the total number of adverse events. AEs associated with acupuncture-related therapies primarily include fainting, intolerable pain during acupuncture procedures, post-needling discomfort, and hematoma at needling sites.
Selection of Studies
The retrieval records obtained from the 10 databases will be imported into the bibliographic software EndNote (version X9, Clarivate, USA) for study selection by two researchers. When the duplicates have been automatically eliminated in EndNote X9, the studies’ titles and abstracts will be examined to see if they fit the criteria for inclusion. Final eligibility for inclusion will be determined after screening the full-text of the remaining articles. In addition, we will scrutinize the bibliography lists of the included studies to identify any additional RCTs that may meet the eligibility criteria. Any disagreements arising during the study selection process will be resolved by a senior investigator. The study selection procedures are presented using the PRISMA-compliant flowchart, as illustrated in Figure 1. In addition, a list of excluded studies with justifications will be provided.
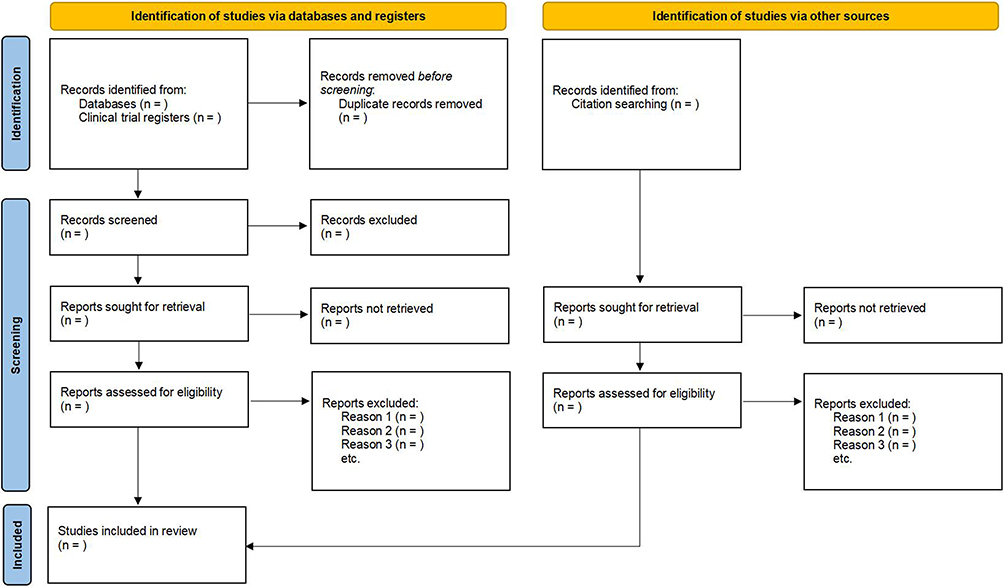 |
Figure 1 PRISMA 2020 flow diagram of study selection for systematic reviews which included searches of databases, registers and other sources. |
Data Extraction and Management
Two investigators will independently adopt Microsoft Excel (Microsoft Corporation, 2019) to extract data from the included RCTs. The extracted information and data will encompass five primary categories, containing participant information, basic study details (first author, publication year, article title), participant information (sample size, gender distribution, average age, tinnitus duration), intervention details (types of acupuncture, number of acupuncture sessions, treatment duration), methods information (study design, time-points of outcome measures), and outcome measurements (primary and secondary outcomes, adverse events). In case of missing crucial data, we will send emails to the primary authors for access. All data entered in Excel will be double-checked and verified by a third researcher to ensure consistency and validity.
To assess the consistency between the two reviewers during the data extraction process, inter-rater reliability will be determined via Cohen’s kappa statistics.20 The Cohen’s kappa coefficient values, ranging from 0.0 to 0.2, 0.21 to 0.40, 0.41 to 0.60, 0.61 to 0.75, 0.75 to 0.80, and 0.80 to 1 will be used to categorize the consistency between the raters as poor, slight, moderate, substantive, excellent, and almost perfect, as per the methodology described by Spector et al.23
Risk of Bias Assessment
The methodological quality of each RCT included in the study will be independently assessed by two raters according to the Cochrane Collaboration’s risk of bias (ROB) tool (version 2.0).24 Risk of bias for each included RCT will be assessed depending on five critical factors, namely the randomization process, deviations from the intended treatments, missing outcome data, outcome measurements, and choice of reported outcomes. Each of these domains will be evaluated as low, unclear, or high risk of bias. Additionally, reviewers will assign an overall rating of low (indicating low risk of bias across all domains), unclear (indicating some concerns in at least one domain), or high (indicating high risk of bias in at least one domain or concerns in multiple domains) for each trial. In cases where the two raters disagree, a referee will mediate to resolve the dispute.
Statistical Analysis
Dichotomous data will be analyzed using the Odds Ratio (OR) value with 95% CI and continuous data will be analyzed using the weighted mean difference (WMD) or standardized mean difference (SMD) with 95% CI. To evaluate heterogeneity and identify if the collected studies can be pooled, the Mantel–Haenszel χ2 test and Higgins I2 will be utilized. The fixed-effects model will be applied if I2 is more than 50%; else, the random-effects model will be utilized.25
Network Meta-Analysis and Geometry of the Network
Network plots will be drawn using R (version 3.6, R Foundation for Statistical Computing, Vienna, Austria) and WinBUGS (version 1.4.3, MRC Biostatistics Unit, Cambridge, UK) software to illustrate the comparative relationship between different interventions. Nodes in the network plots signify various interventions, with the node area denoting the number of assessed intervention studies. Direct correlations between two interventions are indicated by lines connecting the nodes, while a lack of connection implies no direct comparison. Larger nodes correspond to a greater number of direct comparisons, and thicker lines represent increased direct comparisons.26 The contribution matrix will be employed to exhibit the percentage information of the direct evidence that contributes to each relative effect estimated for a study. In addition, we will employ uninformative prior distributions for all location parameters of relative treatment effects.
Bayesian network analysis will be established using the Markov chain Monte Carlo method. The initial configuration consists of four chains for simulation analysis, with 50,000 iterations. Annealing will be performed using the initial 20,000 iterations to mitigate the initial value’s influence, and the remaining 30,000 iterations will be utilized for sampling calculations.27 The convergence of the model will be evaluated by the Brooks-Gelman-Rubin diagnosis method. Specifically, when the Potential Scale Reduction Factor (PSRF) approaches 1, it indicates a higher degree of convergence and greater reliability in the results of the consistency model analysis. Conversely, if the PSRF deviates from 1, it suggests lower reliability.27 This implies that the current number of simulations is insufficient for achieving satisfactory convergence, necessitating an increase in the number of simulations.
Finally, to assess the effectiveness of various acupuncture-related therapies for treating tinnitus, ranking probabilities and rankograms will be created to quickly determine the optimal or worst interventions. Meanwhile, we will construct a cumulative ranking plot and calculate the Surface under the Cumulative Ranking (SUCRA) value based on the cumulative data to compare the relative efficacy of various acupuncture methods. A high SUCRA score indicates a better analgesic effect. Specifically, a SUCRA value of 1 indicates that the intervention is considered the best among the compared options, whereas a value of 0 suggests it is the worst.28
Assessment of Inconsistency
The consistency of NMA results will be assessed through the use of the node-splitting method. Finding outcomes that are consistent across direct and indirect comparisons is the primary goal of NMA studies. For achieving this goal, each NMA node will undergo analysis to examine the statistical differences between direct and indirect evidence. A consistency model will be used if the results are consistent (P > 0.05). Conversely, once inconsistency is present, an inconsistency model will be utilized and the contributing factors to the discrepancy will be analyzed. This analysis may include evaluating the contribution degree of direct and indirect comparisons, as well as the degree of heterogeneity in direct comparisons. If substantial inconsistencies persist, the more reliable direct comparison results may be the only ones used for decision-making.
Subgroup Analyses
If deemed available, subgroup analyses will be conducted in accordance with the different characteristics of the included studies as follows.
- Different tinnitus durations
- Different measurement time points of primary outcomes (eg, short-term effect vs long-term effect)
- Different age groups of patients
- Different geographical settings (ie, trials conducted in China vs trials conducted in other countries) of the studies.
Sensitivity Analyses
Sensitivity analyses using the leave-one-out approach will be used to ensure the accuracy and robustness of meta-analysis results. These studies will assess the impact of each individual study on the overall findings, providing a more comprehensive understanding of the robustness of the meta-analysis results.
Certainty of Evidence
The certainty of evidence will be evaluated by two reviewers in adherence to the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system, which has been proven as a consensus on rating the quality of evidence and strength of recommendations.29 The GRADE consists of five major items that will be rated, namely the methodological quality of the included studies (risk of bias), the degree of agreement between different study results (inconsistency), the accuracy of the combined study results (imprecision), the extent of studies included to meet the criteria (publication bias), and the extrapolation of the study population, interventions, and outcome measures (indirectness). The assessment for certainty of evidence will strictly follow the GRADE guidelines and will involve four steps: (1) presentation of the direct and indirect treatment estimates for each comparison in the evidence network, (2) rating the quality of each direct and indirect effect estimate, (3) presentation of the NMA estimate for each comparison in the evidence network, and (4) rating the quality of each NMA effect estimate. Finally, the certainty of research evidence will be graded as high, moderate, low, or very low.
Assessment of Publication Biases
If primary outcomes are reported in 10 or more included studies, we will evaluate the potential publication bias using funnel plots. Additionally, we will assess the impact of significant publication bias on meta-analysis outcomes by conducting Egger tests, where a p-value less than 0.05 is considered to indicate significant bias.30
Ethical Consideration
Given that all the original data in this NMA are obtained from public data in published clinical studies. Moreover, our study does not include any personal data of patients, so ethical approvals are not required for this study.
Discussion
Given the treatment of primary tinnitus is complex and challenging, diverse kinds of acupuncture-related methods are available in clinical practice. Moreover, a specific acupuncture method can be used alone, or used in combination with other acupuncture methods or guideline-recommended active therapies (eg, Western medication, sound therapy, CBT, education, and counseling).1 Therefore, it is of clinical importance to rank the relative efficacy of different acupuncture-related methods through evidence-based methods.
Although several SRs and meta-analysis studies have been published in recent years with promising results favoring the effect of acupuncture for tinnitus, the bulk of them use the traditional meta-analysis method to compare the efficacy of just one form of acupuncture-related therapy with other active treatments. Thus far, the relative effectiveness of these acupuncture approaches and their integrated use has been little understood, thereby making it difficult for clinicians to choose the best one to employ in clinical practice. For addressing these gaps, it is important to perform a comparative study to determine the optimal acupuncture method or combination. NMA is a suitable method for this purpose, as it can achieve the integration of both direct and indirect comparisons across various kinds of treatments in a single analysis. This method has been increasingly used in recent years to rank the efficacy of multiple acupuncture therapies for various diseases, including knee osteoarthritis,31 postherpetic neuralgia,32 chronic aspecific low back pain,33 and major depressive disorder.34
Nonetheless, to the best of our knowledge based on a prior literature search, to date, there has only been a previously published NMA study35 in this field. However, this NMA study is limited by several drawbacks. First, it only included studies published before November 2017. A few RCTs36–38 have been published since the publication of the previous NMA study to further investigate the efficacy and safety of acupuncture for alleviating primary tinnitus. In order to determine the most recent evidence, it is crucial to include the results of recent clinical trials in an updated systematic review. Second, the criteria of PICOS components in this SR and NMA study35 lack rigorous design. For example, participants would be eligible if they were diagnosed with tinnitus, rather than primary tinnitus. Interventions were restricted to manual acupuncture, electroacupuncture, and warm needling. Outcome measurements only included the response rate, rather than more validated outcomes such as THI. Third, eligible types of studies are undemanding, making both controlled clinical trials (CCTs) and RCTs would be eligible in this SR and NMA study.35 As a result, our study will undertake the most comprehensive and up-to-date literature search, including more eligible RCTs published between 2018 and 2023.36–38 In addition, our study will improve the establishment of PICOS by incorporating more rigorous but feasible inclusion and exclusion criteria.
To note, our study is limited by certain flaws. First, due to translation services for other languages (eg, German, Spanish, Korean, and Japanese) are not affordable, the publication language is restricted to Chinese and English, which may result in selection bias of eligible studies. Second, it is likely that the vast majority of the RCTs included in the study will be hosted in China. However, prior research has suggested that the majority of acupuncture studies published by Chinese produced positive results,39 thus indicating a possible publication bias that may weaken the study’s robustness.
Conclusions
In summary, this protocol elaborates on the methodological procedures of a study that aims to rank the relative efficacy of different acupuncture-related therapies. The complete systematic review and NMA conducted under this protocol is anticipated to determine the optimal acupuncture method for primary tinnitus, thereby providing evidence-based clinical decisions for patients and clinicians to select the most effective acupuncture treatment.
Acknowledgment
Liping Yang and Xingling Li contributed equally to this work as co-first authors.
Funding
The work was supported by the Zhejiang Province Public Welfare Technology Application Research (grant number: LTGY23H270003), Zhejiang Provincial Famous Traditional Chinese Medicine Experts Inheritance Studio Construction Project (grant number: GZS2021027) and Project of Zhejiang Provincial Administration of Traditional Chinese Medicine (grant number: 2018ZA058, 2021ZB097). The funders did not and will not have a role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no conflicts of interest.
References
1. Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. 2014;151:S1–s40. doi:10.1177/0194599814545325
2. Jarach CM, Lugo A, Scala M, et al. Global prevalence and incidence of tinnitus: a systematic review and meta-analysis. JAMA Neurol. 2022;79:888–900. doi:10.1001/jamaneurol.2022.2189
3. Cima RFF, Mazurek B, Haider H, et al. A multidisciplinary European guideline for tinnitus: diagnostics, assessment, and treatment. Hno. 2019;67:10–42. doi:10.1007/s00106-019-0633-7
4. Huang K, Liang S, Chen L, Grellet A. Acupuncture for tinnitus: a systematic review and meta-analysis of randomized controlled trials. Acupunct Med. 2021;39:264–271. doi:10.1177/0964528420938380
5. Liu F, Han X, Li Y, Yu S. Acupuncture in the treatment of tinnitus: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2016;273:285–294. doi:10.1007/s00405-014-3341-7
6. Wu Q, Wang J, Han D, Hu H, Gao H. Efficacy and safety of acupuncture and moxibustion for primary tinnitus: a systematic review and meta-analysis. Am J Otolaryngol. 2023;44:103821. doi:10.1016/j.amjoto.2023.103821
7. Kim JI, Choi JY, Lee DH, Choi TY, Lee MS, Ernst E. Acupuncture for the treatment of tinnitus: a systematic review of randomized clinical trials. BMC Complement Altern Med. 2012;12:97. doi:10.1186/1472-6882-12-97
8. He M, Li X, Liu Y, et al. Electroacupuncture for tinnitus: a systematic review. PLoS One. 2016;11(3):e0150600. doi:10.1371/journal.pone.0150600
9. Cai W, Chen AW, Ding L, Shen WD. Thermal effects of acupuncture by the infrared thermography test in patients with tinnitus. J Acupunct Meridian Stud. 2019;12:131–135. doi:10.1016/j.jams.2019.05.002
10. Chang CH, Lin CD, Hsieh CL. Electroacupuncture promotes neuroplasticity of central auditory pathway: an auditory evoked potentials study. Evid Based Complement Alternat Med. 2022;2022:6855775. doi:10.1155/2022/6855775
11. Hu H, Gao H. Potential value of electroacupuncture in alleviating tinnitus. Neuromodulation. 2022;25:786–787. doi:10.1016/j.neurom.2021.11.008
12. Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ. 2005;331:897–900. doi:10.1136/bmj.331.7521.897
13. Rouse B, Chaimani A, Li T. Network meta-analysis: an introduction for clinicians. Intern Emerg Med. 2017;12:103–111. doi:10.1007/s11739-016-1583-7
14. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. doi:10.1186/2046-4053-4-1
15. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162:777–784. doi:10.7326/m14-2385
16. Amir-Behghadami M, Janati A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg Med J. 2020;37:387. doi:10.1136/emermed-2020-209567
17. Lewis S, Chowdhury E, Stockdale D, Kennedy V. Assessment and management of tinnitus: summary of NICE guidance. BMJ. 2020;2020:368.
18. Choi TY, Jun JH, Choi JY, Kim JI, Lee MS, Ernst E. Acupuncture for the treatment of chronic obstructive pulmonary disease: a protocol of a systematic review. BMJ Open. 2014;4:e004590. doi:10.1136/bmjopen-2013-004590
19. Hu H, Li Z, Cheng Y, Gao H. The efficacy and safety of acupuncture for depression-related insomnia: protocol for a systematic review and meta-analysis. J Pain Res. 2022;15:1939–1947. doi:10.2147/jpr.s370476
20. Fan L, Gao Y, Zhou J, Hu H, Gao H. The efficacy and safety of acupuncture for tinnitus-associated insomnia: a protocol for a systematic review and meta-analysis. J Pain Res. 2022;15:2957–2965. doi:10.2147/jpr.s383968
21. Fackrell K, Hall DA, Barry JG. Tools for Tinnitus Measurement: Development and Validity of Questionnaires to Assess Handicap and Treatment Effects. New York: Nova Science Publishers Inc; 2014.
22. Rücker G, Cates CJ, Schwarzer G. Methods for including information from multi-arm trials in pairwise meta-analysis. Res Synth Methods. 2017;8:392–403. doi:10.1002/jrsm.1259
23. Spector A, Orrell M, Schepers A, Shanahan N. A systematic review of ‘knowledge of dementia’ outcome measures. Ageing Res Rev. 2012;11:67–77. doi:10.1016/j.arr.2011.09.002
24. Flemyng E, Dwan K, Moore TH, Page MJ, Higgins JP. Risk of bias 2 in Cochrane reviews: a phased approach for the introduction of new methodology. Cochrane Database Syst Rev. 2020;10:Ed000148. doi:10.1002/14651858.ed000148
25. Higgins J, Thomas J, Chandler J, Cumpston M, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons; 2019.
26. Chaimani A, Salanti G. Visualizing assumptions and results in network meta-analysis: the network graphs package. Stata J. 2015;15:905–950. doi:10.1177/1536867X1501500402
27. Zhou Z, Xu G, Huang L, et al. Effectiveness and safety of acupuncture-related therapies for chronic musculoskeletal pain: a protocol for systematic review and network meta-analysis. J Pain Res. 2022;15:3959–3969. doi:10.2147/jpr.s387756
28. Fu HJ, Zhou H, Tang Y, et al. Tai Chi and other mind-body interventions for cancer-related fatigue: an updated systematic review and network meta-analyses protocol. BMJ Open. 2022;12:e052137. doi:10.1136/bmjopen-2021-052137
29. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. doi:10.1136/bmj.39489.470347.AD
30. Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics. 2018;74:785–794. doi:10.1111/biom.12817
31. Lee B, Kim TH, Birch S, et al. Comparative effectiveness of acupuncture in sham-controlled trials for knee osteoarthritis: a systematic review and network meta-analysis. Front Med. 2022;9:1061878. doi:10.3389/fmed.2022.1061878
32. Cui Y, Zhou X, Li Q, et al. Efficacy of different acupuncture therapies on postherpetic neuralgia: a Bayesian network meta-analysis. Front Neurosci. 2022;16:1056102. doi:10.3389/fnins.2022.1056102
33. Baroncini A, Maffulli N, Eschweiler J, Molsberger F, Klimuch A, Migliorini F. Acupuncture in chronic aspecific low back pain: a Bayesian network meta-analysis. J Orthop Surg Res. 2022;17:319. doi:10.1186/s13018-022-03212-3
34. Zhichao H, Ching LW, Huijuan L, et al. A network meta-analysis on the effectiveness and safety of acupuncture in treating patients with major depressive disorder. Sci Rep. 2021;11:10384. doi:10.1038/s41598-021-88263-y
35. Pang P, Shi Y, Xu H, Deng L, Wu S, Chen X. Acupuncture methods put to the test for a tinnitus study: a Bayesian analysis. Complement Ther Med. 2019;42:205–213. doi:10.1016/j.ctim.2018.11.017
36. Manz EJ, Sertel S, Szecsenyi J, Plinkert PK, Joos S. Acupuncture as complementary treatment for acute tinnitus: a randomized controlled pilot study. Complement Med Res. 2021;28:96–103. doi:10.1159/000508630
37. Kim BH, Moon YK, Kim MH, Nam HJ. Comparing the effects of manual acupuncture, electroacupuncture, and transcutaneous electrical nerve stimulation on chronic tinnitus: a randomized controlled trial. Integr Med Res. 2020;9:100409. doi:10.1016/j.imr.2020.100409
38. Su Q, Shi X, Zhang J, Li M. Intervention of the syndrome-position point selection method on idiopathic tinnitus of phlegm-fire stagnation pattern: a randomized controlled study. J Healthc Eng. 2022;2022:9664078. doi:10.1155/2022/9664078
39. Gang WJ, Gong CZ, Jing XH. Acupuncture randomized controlled trials: comparing China-based vs. Western-based studies. Zhongguo Zhen Jiu. 2022;42:3–7. doi:10.13703/j.0255-2930.20201224-k0001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Pain and Function in Patients with Nonspecific Low Back Pain: Study Protocol for an Up-to-Date Systematic Review and Meta-Analysis
Li Y, Liu Y, Zhang L, Zhai M, Li L, Yuan S, Li Y
Journal of Pain Research 2022, 15:1379-1387
Published Date: 10 May 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Opioid-Sparing Effect of Acupuncture After Abdominal Surgery: A Systematic Review and Meta-Analysis Protocol
Joo C, Kim KH, Jang BH, Huang CW, Kang JW, Lee JD, Lee S, Lee S
Journal of Pain Research 2023, 16:1095-1101
Published Date: 29 March 2023
Effectiveness of Combination of Thunder Fire Moxibustion with Other Forms of Traditional Chinese Medicine for Osteoarthritis Knee: A Meta-Analysis
Wei W, Qin Y, Lin J
Journal of Pain Research 2025, 18:3087-3099
Published Date: 21 June 2025