Back to Journals » International Journal of General Medicine » Volume 18
Predicting Early Dysphagia in Acute Ischemic Stroke Using an Explainable Machine Learning Model
Authors Li Y ![]() , Yu S, Yu X, Tian B
, Yu S, Yu X, Tian B ![]() , Tang J, Qu H, Zhang Y
, Tang J, Qu H, Zhang Y
Received 12 September 2025
Accepted for publication 20 November 2025
Published 5 December 2025 Volume 2025:18 Pages 7341—7356
DOI https://doi.org/10.2147/IJGM.S567157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Ye Li,1,2,* Sihao Yu,3,* Xiaojuan Yu,4 Bei Tian,1,5 Jiayan Tang,1,2 Haihong Qu,4 Yongfang Zhang1,5
1Graduate School, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2School of Nursing and Health Management, Shanghai University of Medicine & Health Sciences, Shanghai, People’s Republic of China; 3Department of Nursing, Longhua Hospital Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 4Department of Nursing, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, Shanghai, People’s Republic of China; 5Department of Nursing, Shanghai University of Medicine & Health Sciences Affiliated Zhoupu Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haihong Qu; Yongfang Zhang, Email [email protected]; [email protected]
Purpose: This study aimed to identify key risk factors and develop an explainable machine learning (ML) model for predicting early dysphagia in patients with acute ischemic stroke (AIS).
Patients and Methods: In this cross-sectional study, 1041 patients with AIS were recruited from two tertiary hospitals. Participants were classified into a non-dysphagia group (n = 736) and a dysphagia group (n = 305). Feature selection was carried out using the Boruta algorithm and logistic regression. The dataset was randomly partitioned into a training set (n = 728) and a test set (n = 313) in a 7:3 ratio. Six ML models were trained with 10-fold cross-validation. Model performance was evaluated based on the area under the receiver operating characteristic curve (AUC-ROC), sensitivity, specificity, accuracy,positive predictive value (PPV), negative predictive value (NPV), F1-score and Youden’s index. Key predictors were interpreted using SHapley Additive exPlanations (SHAP) analysis.
Results: The incidence of early dysphagia with AIS was 29.3%. The Random Forest (RF) model demonstrated the best overall performance, with an AUC-ROC of 0.952 (95% CI: 0.927– 0.976). The significant risk factors identified were Activities of Daily Living (ADL) grade, National Institutes of Health Stroke Scale (NIHSS) score, multifocal lesions, hypoalbuminemia, coronary heart disease, and lesion hemisphere.
Conclusion: ML models may serve as reliable assessment tools for predicting dysphagia in patients with AIS. The RF model demonstrated the best predictive performance. This predictive model could assist clinical healthcare providers in delivering early warnings and developing individualized treatment plans for high-risk patients.
Keywords: ischemic stroke, dysphagia, machine learning, predictive model, risk factors
Introduction
Stroke is the second leading cause of death and the third leading cause of disability worldwide.1 This situation is particularly severe in China, where stroke has become the foremost cause of mortality, against the backdrop of an aging population and continuously rising prevalence of stroke risk factors.2 Ischemic stroke (IS), the most common type of stroke, has been increasing in incidence annually, in contrast to the declining incidence of hemorrhagic stroke (HS).2
Post-stroke dysphagia (PSD) is a common complication of stroke, resulting from neurological damage such as injury to the cortical swallowing center, disruption of corticobulbar tracts, or brainstem lesions, which lead to loss of normal swallowing function.3 A recent meta-analysis incorporating 95 studies reported that the prevalence of dysphagia following IS is approximately 36.8%.4 PSD not only directly contributes to complications such as aspiration pneumonia and malnutrition, but also significantly increases disease burden by prolonging hospitalization, raising healthcare costs, and reducing quality of life.5 It is recognized as the second most important risk factor for mortality after stroke severity itself.5 Moreover, although spontaneous recovery of swallowing function is possible, approximately 30% of patients still cannot achieve safe oral intake 30 days after stroke onset.6
It is widely accepted that initiating early rehabilitation within 24 to 48 hours after stroke onset has a positive effect on neurological recovery.7 According to relevant Chinese guidelines, individualized swallowing assessment and rehabilitation intervention should be initiated within 24 hours of hospital admission to reduce the incidence of dysphagia.8 However, conventional assessment tools have certain limitations.9 For example, the Water Swallowing Test (WST) is simple and easy to perform but carries a risk of inducing aspiration. Although Video Fluoroscopy Swallowing Study (VFSS) and Fiberoptic Endoscopic Evaluation of Swallowing (FEES) are considered gold standards for dysphagia diagnosis, their widespread use is limited due to factors such as radiation exposure, risk of aspiration during the procedure, equipment requirements, and high cost.
Previous studies have indicated that the occurrence of PSD is influenced by multiple interacting factors, including patient characteristics—such as sex, age, race, and chronic comorbidities—as well as stroke-specific features including stroke subtype, lesion location, and National Institutes of Health Stroke Scale (NIHSS) score.4,10,11 Consequently, some researchers have integrated these risk factors into predictive models to identify high-risk individuals. However, most existing prediction studies have focused on swallowing function at specific time points post-stroke, such as 3 days,12,13 7 days,6,14,15 30 days,6,14,16–18 or 6 months.18,19 In comparison, research targeting dysphagia in the hyperacute phase (within 24–48 hours of admission) remains limited, and such studies have predominantly used conventional logistic regression for model development.20,21 In recent years, machine learning (ML) has gained prominence in healthcare due to its strengths in pattern recognition, handling high-dimensional data, and generating accurate predictions, offering new opportunities for predicting post-stroke complications.12,22,23 For instance, one study developed a predictive model for severe dysphagia within 72 hours of admission in patients with IS using six ML algorithms, providing a useful reference for further investigation.12 Nevertheless, ML models are often considered “black boxes” due to their opaque decision-making processes. Explainable artificial intelligence methods, such as feature-based interpretation techniques, have emerged as promising tools to enhance model transparency and clinical trust.24
The primary objective of this study is to develop an interpretable ML model for predicting early dysphagia in patients with IS, based on medical records from the neurology departments of two hospitals. This model aims to quantify key risk factors and analyze clinical characteristics to provide early warnings for healthcare providers, facilitate personalized treatment planning for high-risk individuals, reduce the incidence of adverse outcomes related to dysphagia, and ultimately improve patients’ quality of life.
Material and Methods
Study Design and Participants
This cross-sectional study employed a convenience sampling method to recruit 1041 patients with AIS from the neurology departments of two tertiary general hospitals in Shanghai, China, between February 2024 and December 2024. The inclusion criteria were as follows: diagnosis of ischemic stroke according to the Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2023,25 confirmed by cranial computed tomography (CT) and/or magnetic resonance imaging (MRI); swallowing function assessment conducted within 24 hours after hospital admission; availability of complete medical records; and age ≥18 years. Exclusion criteria included: pre-existing dysphagia prior to the stroke; delayed hospital admission (≥24 hours from symptom onset to hospital arrival) leading to postponed swallowing assessment and inability to be evaluated within the optimal intervention window for dysphagia; impaired hearing, comprehension, or communication skills; presence of consciousness disorders or severe psychiatric conditions; and comorbid diseases that may cause swallowing dysfunction, such as Parkinson’s disease, myasthenia gravis, or history of head and neck cancer radiotherapy/chemotherapy.
The sample size was calculated using a formula for binary outcome prediction models.26 With an assumed dysphagia prevalence of 36.8% based on previous studies,4 and anticipated model performance indicated by a C-statistic of 0.85 (derived from prior predictive models of early PSD with AUCs of 0.850 and 0.91520,21), and 26 candidate predictor parameters, the required sample size was estimated using the “pmsampsize” package in R software. The calculation showed that at least 571 participants were needed for model training. A total of 1041 patients were ultimately enrolled to ensure sufficient statistical power.
Assessment of Swallowing Function
All patients were assessed within 24 hours of admission by rehabilitation physicians who were blinded to the patients’ clinical outcomes. The evaluation of swallowing dysfunction followed a structured two-step process:8 initial screening, followed by a clinical assessment for those who screened positive, with the final diagnosis of dysphagia based on the results of the Volume-Viscosity Swallow Test (V–VST).During the screening phase, the WST or the Eating Assessment Tool-10 (EAT-10) was used.27 The WST was administered first: patients were asked to sit upright and drink 30 mL of warm water. The swallowing process was observed for duration and signs of coughing. Results were graded on a 5-point scale, ranging from grade 1 (able to drink smoothly in one attempt without coughing) to grade 5 (frequent coughing with inability to swallow). A grade 1 result was considered negative for dysphagia, while grade 2 or higher indicated a need for further evaluation. If a patient could not complete the WST, the EAT-10 questionnaire was used instead. The EAT-10 consists of 10 items scored from 0 to 4, with a total score ranging from 0 to 40. A score ≥ 3 was considered indicative of swallowing difficulties and warranted additional assessment.
Patients who screened positive proceeded to the clinical assessment phase. In this study, a positive V–VST was required for the diagnosis of PSD.21 The V–VST evaluates swallowing safety and efficacy across different food consistencies and volumes. A positive result was defined by the presence of signs such as coughing, voice changes, or oropharyngeal residue. Concurrently, the Functional Oral Intake Scale (FOIS) was used to corroborate swallowing function and feeding status in patients, with scores ranging from Level 1 (nothing by mouth) to Level 7 (full oral diet without restrictions); however, FOIS scores were not used for diagnostic purposes.
Among the 1041 patients included in the study, 305 were diagnosed with dysphagia and assigned to the PSD group, while the remaining 736 without dysphagia comprised the NPSD group.
Collection of Clinical Data
Two investigators independently extracted data from the electronic medical record (EMR) system using a standardized retrieval protocol. The coding and definitions of the features are provided in Supplementary Table 1. To ensure the temporal precedence of predictor variables relative to the outcome, all included variables were measured prior to the occurrence of dysphagia. The collected data comprised:
(1) Demographic characteristics: age, sex, education level, smoking history, drinking history, body mass index (BMI), and medical history including the number of chronic conditions, hypertension, diabetes, hyperlipidemia, coronary heart disease, atrial fibrillation, and history of stroke.
(2) Stroke-related characteristics: Activity of Daily Living (ADL) grade, hypoalbuminemia, NIHSS score, pre-admission Modified Rankin Scale (mRS) grade, lesion hemisphere, multifocal lesions, and treatment methods.
The ADL grade was assessed using the Barthel Index (BI), which classifies patients into four categories: independence (100 points), mild dependence (61–99 points), moderate dependence (41–60 points), and severe dependence (≤40 points). The mRS score was dichotomized into favorable outcome (0–2) and poor outcome (3–5). The lesion hemisphere and multifocal lesions were determined based on imaging findings.
All assessments were performed by neurology healthcare professionals who were blinded to the patients’ swallowing function status.
Feature Selection
Feature selection is a critical step in model development. We employed a combination of the Boruta algorithm and multivariable logistic regression analysis for feature screening, an approach that has been adopted in previous studies.28–30 The Boruta algorithm, built upon the random forest framework, evaluates feature relevance by creating shuffled copies of the original features—known as shadow features—which serve as a benchmark for comparison. It then calculates feature importance scores through multiple random forest iterations. Compared to univariate filtering methods, this approach more reliably prevents the omission of important features and avoids retaining irrelevant ones.29 Features identified as important by Boruta were subsequently included in a multivariable logistic regression analysis to identify factors independently associated with dysphagia. To address potential multicollinearity among variables, Spearman correlation analysis and variance inflation factor (VIF) assessment were conducted. Variables with a correlation coefficient |R| > 0.8 or VIF > 10 were considered to exhibit significant collinearity and were removed from the model.
Model Development and Evaluation
During model development, the dataset was partitioned randomly into a training set (70%), employed for model development, and a hold-out test set (30%), reserved for validation.Using the features selected as described above, prediction models were developed using the following six machine learning algorithms: Support Vector Machine (SVM), Logistic Regression (LR), Least Absolute Shrinkage and Selection Operator (Lasso), Random Forest (RF), K-Nearest Neighbors (KNN), and Artificial Neural Network (ANN). Hyperparameters for each algorithm were optimized through a grid search approach. Model stability and generalizability were further ensured using 10-fold cross-validation.
Model Evaluation
The predictive performance of the models was evaluated by plotting the receiver operating characteristic (ROC) curve and calculating the area under the curve (AUC), sensitivity, sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV), F1-score and Youden’s index. Differences in AUC values between models were compared using the DeLong test. The optimal model was selected based on a comprehensive consideration of both the F1-score and AUC value.
Model Interpretability
Given that ML is often considered a “black-box” approach, interpretable machine learning methods enhance the transparency, trustworthiness, and robustness of predictive models by quantifying and visualizing the decision-making process.24 In this study, SHapley Additive exPlanations (SHAP) was applied to interpret the best-performing prediction model. SHAP values were computed to evaluate the importance of each feature. We also visualized the distribution of feature contributions using summary plots and analyzed individual feature effects through dependency plots. Furthermore, two representative prediction explanations for IS patients were illustrated using SHAP force plots to demonstrate model interpretation at the individual level.
Statistical Analysis
Statistical analyses were conducted with SPSS Statistics, version 27.0 (IBM Corp., Armonk, NY), and R software, version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria). All continuous variables exhibited non-normal distributions and are summarized as median and interquartile range (IQR).Group comparisons were performed using the Mann–Whitney U-test. Categorical variables are presented as numbers and percentages, and were analyzed using the chi-square test. A two-tailed P value < 0.05 was considered statistically significant.
Results
Participant Characteristics
A total of 1041 patients with AIS were included in this study. The subject recruitment flowchart is presented in Supplementary Figure 1. The overall cohort had a median age of 70 years (IQR 62–78), 61.6% were male, and the median NIHSS score was 2 (IQR 0–6). PSD was present in 305 patients, accounting for 29.3% of the sample. The detailed FOIS scores of patients with dysphagia are provided in Supplementary Table 2. Comparisons of clinical characteristics showed that the PSD group was significantly older, had lower education levels, lower BMI, a higher number of chronic conditions, and higher prevalence of diabetes, coronary heart disease, atrial fibrillation, and previous stroke history compared to the NPSD group (all P < 0.05).Regarding stroke-related characteristics, the PSD group demonstrated more severe dependence in ADL, higher rates of hypoalbuminemia, higher NIHSS scores, higher mRS scores, higher proportion of right/bilateral hemisphere lesions, more multifocal lesions, and higher rates of thrombolysis/thrombectomy treatment (all P < 0.05). The clinical characteristics of the participants are summarized in Table 1.
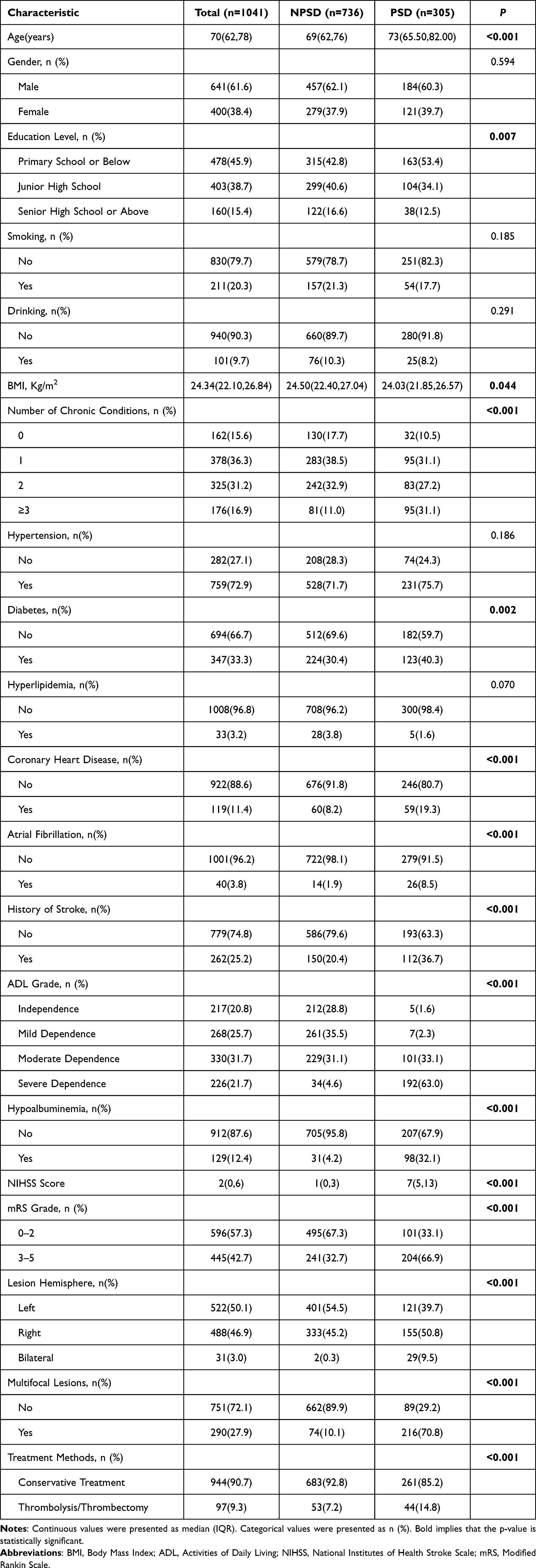 |
Table 1 Clinical Characteristics of AIS Patients |
Supplementary Table 3 describes the characteristics of the training and test sets. The dataset of 1041 patients was split into a training set (n = 728) and a test set (n = 313). The proportion of patients with dysphagia was similar between the two sets (70.9% vs 70.3%, P = 0.848). A statistically significant difference was observed in the presence of multifocal lesions (P = 0.026), while all other features were well-balanced. Although this difference was statistically significant, the absolute difference in the prevalence of multifocal lesions between the training and test sets was relatively small (25.8% vs 32.6%). We believe this modest imbalance is unlikely to substantially impact the model’s generalization performance. Overall, the training and test sets were well-matched, providing a reliable basis for further analysis.
Feature Selection for Model Construction
To enhance the practicality and feasibility of the predictive model, we applied the Boruta algorithm to analyze 20 candidate features and identify the most relevant predictors. As shown in Figure 1, the following variables were identified as important: NIHSS score, ADL grade, presence of multifocal lesions, hypoalbuminemia, affected hemisphere, coronary heart disease, age, number of chronic conditions, mRS grade, hyperlipidemia, history of stroke, and BMI.
 |
Figure 1 Feature importance ranking derived from the Boruta algorithm, with features highlighted in green confirmed as important. |
These variables were subsequently entered into a forward stepwise multivariable logistic regression analysis. The results indicated that NIHSS score, ADL grade, multifocal lesions, hypoalbuminemia, affected hemisphere, and coronary heart disease remained significant predictors in the multivariable model (P < 0.05), while the other variables were excluded due to lack of statistical significance. These findings are presented in Table 2.
 |
Table 2 Multivariable Logistic Regression Analysis of Dysphagia in Patients with IS |
Furthermore, Spearman correlation analysis and VIF evaluation were conducted to assess multicollinearity among the selected features. All correlation coefficients between variables were below 0.8, and all VIF values were ≤ 10, indicating no significant multicollinearity. Detailed results are provided in Supplementary Tables 4 and 5.
Model Development and Evaluation
In this study, we developed six ML models—RF, SVM, LR, KNN, Lasso, and ANN—to predict early dysphagia in patients with AIS. The performance of each model was evaluated on both training and test sets.
On the training set (Figure 2A), RF achieved the highest AUC (0.959, 95% CI: 0.945–0.973), followed by KNN (0.953, 95% CI: 0.936–0.969), Lasso (0.951, 95% CI: 0.935–0.967), LR (0.949, 95% CI: 0.932–0.966), ANN (0.944, 95% CI: 0.927–0.963), and SVM (0.942, 95% CI: 0.920–0.963). DeLong’s test indicated no significant differences in AUC among the models on the training set (P > 0.05, Supplementary Table 6).
 |
Figure 2 Performance comparison of different ML models. (A) ROC curves of the six predictive models on the training set. (B) ROC curves of the six predictive models on the test set. |
On the test set (Figure 2B), ANN achieved the highest AUC (0.962, 95% CI: 0.944–0.980), followed by KNN (0.958, 95% CI: 0.935–0.980), RF (0.952, 95% CI: 0.927–0.976), Lasso (0.950, 95% CI: 0.928–0.972), LR (0.950, 95% CI: 0.928–0.972), and SVM (0.946, 95% CI: 0.922–0.971). DeLong’s test was used to compare the AUC values of the models on the test set. ANN showed significantly better performance than SVM, LR, and Lasso (P < 0.05), but no significant differences were observed when compared to RF and KNN, suggesting comparable predictive ability among these three models (Supplementary Table 6). However, based on a comprehensive evaluation of performance metrics, RF was selected as the optimal model. This decision was driven by its superior and more balanced F1-score (0.837) compared to other models, as presented in Table 3, alongside its high AUC. The hyperparameter configurations for all models are provided in Supplementary Table 7.
 |
Table 3 Performance of Models on the Dataset |
Interpretation of the RF Model Using SHAP
To provide a comprehensive interpretation of the RF model, we applied SHAP. As shown in Figure 3A, the mean absolute SHAP values were used to visualize the contribution intensity of each feature. ADL grade (0.132) had the highest impact, followed by NIHSS score (0.124), multifocal lesions (0.093), hypoalbuminemia (0.030), coronary heart disease (0.020), and lesion hemisphere (0.010).Figure 3B displays a beeswarm plot illustrating the distribution of SHAP values for each feature, demonstrating how different feature values influence the predictions. The x-axis represents the SHAP value, indicating the magnitude and direction of each feature’s contribution. The color gradient from purple (low feature values) to yellow (high feature values) helps visualize value-dependent effects. ADL grade showed a substantial influence on the output, with higher values (yellow) associated with increased risk and lower values (purple) corresponding to reduced effects. NIHSS score, multifocal lesions, hypoalbuminemia, coronary heart disease, and lesion hemisphere also exhibited significant effects on predictions.
 |
Figure 3 Interpretation of the optimal model (RF) using SHAP. (A) Feature importance ranking based on mean |SHAP values|. (B) Beeswarm plot of SHAP values. (C) SHAP dependence plots for individual features. |
Figure 3C presents SHAP dependence plots for individual features, illustrating the impact of each variable on the model predictions under the influence of their strongest interacting features. All features showed a positive correlation with the predicted outcome, confirming their roles as risk factors. As shown in the figure, the most frequent and pronounced interaction was observed between ADL grade and multifocal lesions. A positive trend was evident between ADL grade and the predicted outcome: as the level of ADL dependency increased, the corresponding SHAP values also rose. Furthermore, the color gradient representing multifocal lesions indicates that patients with both multifocal lesions and moderate-to-severe ADL dependency had higher SHAP values than those without multifocal lesions. In contrast, patients with no or only mild ADL dependency exhibited the opposite pattern. Additionally, for the continuous variable NIHSS score, a non-linear relationship with dysphagia risk was observed. The risk associated with NIHSS scores between 10–15 was weaker than that for scores around 5–7, while a sharp increase in SHAP values was seen for scores exceeding 15. The presence of multifocal lesions further enhanced the risk contribution of higher NIHSS scores.
Figure 4A and B show SHAP waterfall plots, which visualize the cumulative contribution of each feature to the prediction output for individual patients. Each bar represents a feature, with purple indicating a risk-reducing (negative) contribution and yellow indicating a risk-increasing (positive) contribution. Figure 4C and D are force plots that illustrate how each feature shifts the model’s prediction from the base value to the final output f(x). Purple arrows represent features that decrease the prediction, while yellow arrows represent those that increase it.
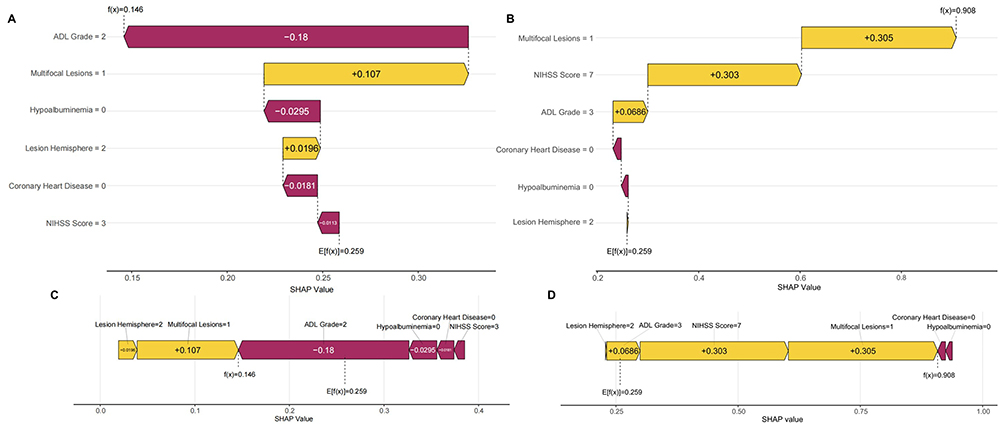 |
Figure 4 Local interpretability of the model using SHAP explanations. (A) SHAP waterfall plot for a representative NPSD patient. (B) SHAP waterfall plot for a representative PSD patient. (C) SHAP force plot for the same NPSD patient in panel A. (D) SHAP force plot for the same PSD patient in panel B. |
Figure 4A and C correspond to a NPSD patient. Mild ADL dependency, absence of hypoalbuminemia and coronary heart disease, and a low NIHSS score were the main factors reducing the predicted risk. Although the presence of multifocal lesions and right hemisphere involvement slightly increased the risk, their contributions were relatively small. The final prediction value was 0.146, indicating a low risk of dysphagia.
Figure 4B and D correspond to a PSD patient. Moderate ADL dependency, an NIHSS score of 7, and the presence of multifocal lesions strongly increased the predicted risk, resulting in a final prediction value of 0.908, suggesting a very high risk of dysphagia.
Discussion
PSD is a common complication of AIS that predisposes patients to multiple somatic complications and severe psychosocial dysfunction, and represents the second leading risk factor for post-stroke mortality.5,31 Our findings indicate that the incidence of PSD in AIS was 29.3%, which is higher than the 22.0% reported in a recent study,32 but lower than the 36.8% reported in a meta-analysis.4 These discrepancies may be attributed to differences in assessment tools, timing of evaluation, and patient populations. Nonetheless, all studies consistently highlight that post-stroke dysphagia is a frequent complication requiring clinical attention. Therefore, early identification of high-risk patients and implementation of individualized swallowing assessments and rehabilitation interventions within 24 hours of admission are essential to promote neurological recovery and reduce mortality.8,33
ML offers significant advantages in handling complex medical data, enabling more accurate predictions.12 In this study, six different ML models were developed to predict early dysphagia. The results demonstrated that RF, KNN, and ANN exhibited strong predictive performance. Overall, RF achieved the best performance, with an AUC of 0.952 (95% CI: 0.927–0.976) and an F1-score of 0.837 in the test set. Previous comparative studies have also found that RF achieves the highest accuracy in disease risk prediction.34 As an ensemble learning algorithm, RF constructs multiple decision trees using randomly selected features and samples, and combines their outputs to improve classification accuracy and generalization.34,35 More notably, RF can be integrated with explainable AI frameworks such as SHAP,36,37 maintaining high predictive performance while significantly enhancing the transparency and interpretability of the decision-making process. This provides a reliable theoretical and practical basis for model outputs, holding substantial value in clinical decision-making.24
According to relevant Chinese guidelines, individualized swallowing assessment and rehabilitation intervention should be initiated within 24 hours of hospital admission to reduce the incidence of dysphagia.8 However, conventional assessment tools have certain limitations.9 For example, the Water Swallowing Test (WST) is simple and easy to perform but carries a risk of inducing aspiration. Although Video Fluoroscopy Swallowing Study (VFSS) and Fiberoptic Endoscopic Evaluation of Swallowing (FEES) are considered gold standards for dysphagia diagnosis, their widespread use is limited due to factors such as radiation exposure, risk of aspiration during the procedure, equipment requirements, and high cost.
The development of PSD involves multiple interacting factors. Our study considered readily available admission factors as candidate predictors. Using the Boruta algorithm and logistic regression, six features were selected as final predictors. To enhance model interpretability, SHAP was applied to quantify the contribution of each feature to the predictions.38 The features, in descending order of contribution, were ADL grade, NIHSS score, multifocal lesions, hypoalbuminemia, coronary heart disease, and lesion hemisphere.
Both the Boruta algorithm and SHAP interpretation identified ADL and NIHSS as core predictors of dysphagia, consistent with previous studies by Lu et al and Ye et al12,21 BI assesses ADL in stroke patients, reflects physical performance.21 A low BI is often associated with stroke severity, and patients with ADL impairment are at higher risk of dysphagia. IS Patients with a BI score ≤ 60 are at higher risk of developing dysphagia.39 In our study, patients with moderate-to-severe ADL dependency exhibited a more than sevenfold increase in risk. Individual force plots (Figure 4) showed that severe ADL dependency increased the SHAP value by 0.0686, whereas mild dependency had no predictive value for the outcome.Furthermore, PSD and ADL impairment interact bidirectionally: dysphagia exacerbates ADL impairment through nutritional deficits and complications, while reduced ADL delays swallowing recovery.40 The NIHSS score is a core indicator of stroke severity, with higher scores indicating greater neurological impairment.21 A meta-analysis showed that the prevalence of dysphagia was higher in patients with NIHSS scores of 11–20 than in those with scores of 5–10 or <5.4 Although the optimal cutoff value of the NIHSS score for predicting dysphagia remains controversial (with proposed values including 7,41 9,42 and 1243), the median score in our dysphagia group was 7.SHAP dependence plots (Figure 3C) further revealed a nonlinear relationship between NIHSS score and dysphagia risk. Specifically, patients with scores between 5–10 had elevated risk, while those with scores of 11–20 faced even higher risk. This pattern may reflect anatomical differences; for instance, Labeit et al44 found that patients with infratentorial strokes had lower NIHSS cutoffs due to direct brainstem involvement, which significantly increases dysphagia risk. Thus, clinical assessments should incorporate anatomical localization.
Multifocal lesions, defined as strokes occurring in two or more locations, often indicate extensive brain damage.45 When these lesions affect key swallowing-related regions—such as the brainstem swallowing center, the cortical-basal ganglia-cerebellar circuit regulating swallowing, and the cerebellum coordinating muscle contraction—the risk of dysphagia increases significantly.46,47 Moreover, Figure 4 shows that the presence of multifocal lesions amplified the risk contributions of high NIHSS scores and moderate-to-severe ADL grade. This suggests that multifocal lesions not only pose an independent risk but also exacerbate the effects of other factors. Clinically, this underscores the need for vigilant screening and early intervention in patients with multifocal lesions, even if other risk factors appear moderate.
Beyond the top three predictors, the model also identified hypoalbuminemia, coronary heart disease, and lesion hemisphere as significant risk factors. Hypoalbuminemia was significantly associated with dysphagia, consistent with previous reports.21,48 As a key biomarker of malnutrition, hypoalbuminemia reflects depleted protein reserves and impaired synthesis, increasing complication rates and worsening functional outcomes in acute stroke.49 Protein is essential for maintaining muscle mass and function, and low levels contribute to sarcopenia,50 which directly impairs the coordinated action of swallowing-related muscles (masticatory and tongue muscles), increasing the risk of pharyngeal residue and aspiration.51 Coronary heart disease also played a significant role in predicting dysphagia. Żdanowicz et al found that coronary heart disease was associated with dysphagia severity on day 7 post-stroke, though this link has been rarely reported previously.52 Coronary heart disease and IS often coexist, and both are associated with dysphagia. A study involving elderly hospitalized patients in China found that approximately 39.6% of patients with coronary heart disease experienced dysphagia.53 Moreover, stroke patients with CHD tend to have more severe conditions.54 Further prospective studies are needed to elucidate the mechanisms by which influences PSD. In contrast to some previous studies, we found that right/bilateral hemisphere lesions were risk factors for dysphagia, aligning with Krekeler et al.11 PSD primarily occurs in the pharyngeal phase, with left hemisphere lesions often affecting oral-stage function and right hemisphere lesions impairing pharyngeal function.55 Bilateral involvement not only increases dysphagia risk but also is associated with a recovery rate only 32% of that seen in unilateral cases.56 However, findings remain controversial; a meta-analysis showed no significant effect of lesion hemisphere on dysphagia occurrence.4 Future studies with larger samples are needed to validate the impact of different lesion hemispheres on dysphagia onset and recovery.
Currently, VFSS and FEES are recognized as the gold standards for diagnosing dysphagia.9 However, their widespread implementation within 24 hours of admission for patients with AIS faces practical challenges, including high economic costs and technical operational difficulties. Therefore, this study aimed to develop a simple, rapid, cost-effective, and accurate non-invasive predictive model to address these limitations. Building on its excellent predictive performance, our RF model presents distinct practical advantages for early screening in terms of accessibility, cost-effectiveness, and immediate availability upon admission. We envision a clear pathway for its clinical integration. The model could be implemented as a decision-support tool within the Hospital Information System. In practice, upon patient admission, inputting the six core predictors would trigger an automatic calculation of dysphagia risk and an early warning for high-risk individuals. This alert would directly prompt physicians to initiate standardized clinical swallowing assessments. This envisioned workflow ensures that limited healthcare resources, including eventual VFSS/FEES referrals, are prioritized for the patients at greatest need, thereby optimizing the entire clinical pathway from prediction to intervention for PSD management.
This study has several limitations. First, although two tertiary hospitals were included, both were located in Pudong New Area, Shanghai, which may introduce sampling bias and limit generalizability. Second, although multiple sensitive and specific assessment tools were used, instrumental evaluations were not routinely performed due to clinical constraints (eg, unstable patient condition, high cost, and operational complexity), potentially leading to underdiagnosis. Third, the sample size limited external validation, which may affect the model’s applicability to other populations. Fourth, the exclusion of conscious but uncooperative patients or those with significant communication/language disorders potentially omits individuals with more severe strokes and limits the generalizability of our findings to the broader stroke population. Finally, despite efforts to include comprehensive factors, some potential predictors (eg, marital status, insular lesions) were not analyzed due to insufficient data. Future multicenter prospective studies with larger samples and more diverse data are warranted to validate the model’s performance, improve its predictive power, and enhance clinical applicability.
Conclusion
This study developed a ML model to predict the risk of dysphagia within 24 hours of admission in patients with acute ischemic stroke, using readily available clinical data. Among the six ML algorithms evaluated, the RF model demonstrated the best overall performance. Furthermore, by incorporating SHAP-based interpretability analysis, the model’s clinical applicability has been enhanced in terms of both transparency and reliability. Future studies should expand the sample size and validate the generalizability of the model across multiple centers and diverse populations.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Yongfang Zhang, upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Shanghai University of Medicine and Health Sciences Affiliated Zhoupu Hospital (2024-C-010-E01), and written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by The Scientific Research Program of Shanghai Pudong New Area Health Commission (the General Program, PW2023A-71), the Shanghai Municipal Health Commission Key Discipline Construction Program (Cardiology, 2024ZDXK0019), the Hospital Management Research Fund of Shanghai Hospital Association (X2025112), and the Shanghai Pudong New Area Health Commission Integrated Chinese and Western Medicine Flagship Hospital (General Hospital, YC-2023-0401).
Disclosure
The authors declare no conflicts of interest.
References
1. Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization: global Stroke Fact Sheet 2025. Int J Stroke. 2025;20(2):132–144. doi:10.1177/17474930241308142
2. Tu WJ, Wang LD. China stroke surveillance report 2021. Mil Med Res. 2023;10(1):33. doi:10.1186/s40779-023-00463-x
3. Li X, Wu M, Zhang J, et al. Post-stroke dysphagia: neurological regulation and recovery strategies. Biosci Trends. 2025;19(1):31–52. doi:10.5582/bst.2025.01029
4. Wen X, Fan B, Zhan J, et al. Integrated analysis of the prevalence and influencing factors of poststroke dysphagia. Eur J Med Res. 2025;30(1):27. doi:10.1186/s40001-024-02263-y
5. Labeit B, Michou E, Hamdy S, et al. The assessment of dysphagia after stroke: state of the art and future directions. Lancet Neurol. 2023;22(9):858–870. doi:10.1016/s1474-4422(23)00153-9
6. Galovic M, Stauber AJ, Leisi N, et al. Development and Validation of a Prognostic Model of Swallowing Recovery and Enteral Tube Feeding After Ischemic Stroke. JAMA Neurol. 2019;76(5):561–570. doi:10.1001/jamaneurol.2018.4858
7. Wang H, Ai Y, Zhu L, Shi H, Hou R. Efficacy of early rehabilitation nursing on the prognosis of China stroke patients: a systematic review and meta-analysis of randomized controlled trials. Geriatric Nurs. 2025;64:103332. doi:10.1016/j.gerinurse.2025.04.005
8. Chinese Stroke Association Dysphagia and Nutrition Management Consensus Expert Committee. Chinese dysphagia and nutrition management manual for acute stroke patients. Chin J Stroke. 2019;14(11):1153–1169. doi:10.3969/j.issn.1673-5765.2019.11.014.
9. Jiang Y, Chi Y, Pan R, et al. Advancing stroke patient care: a network meta-analysis of dysphagia screening efficacy and personalization. Front Neurol. 2024;15:1380287. doi:10.3389/fneur.2024.1380287
10. Maciejewska O, Kępczyńska K, Polit M, Domitrz I. Dysphagia in Ischaemic Stroke Patients: one Centre Retrospective Study. Nutrients. 2024;16(8):1196. doi:10.3390/nu16081196
11. Krekeler BN, Schieve HJP, Khoury J, et al. Health Factors Associated With Development and Severity of Poststroke Dysphagia: an Epidemiological Investigation. J Am Heart Assoc. 2024;13(7):e033922. doi:10.1161/jaha.123.033922
12. Ye F, Cheng LL, Li WM, Guo Y, Fan XF. A Machine-Learning Model Based on Clinical Features for the Prediction of Severe Dysphagia After Ischemic Stroke. Int J Gen Med. 2024;17:5623–5631. doi:10.2147/ijgm.S484237
13. Saab R, Balachandar A, Mahdi H, et al. Machine-learning assisted swallowing assessment: a deep learning-based quality improvement tool to screen for post-stroke dysphagia. Front Neurosci. 2023;17:1302132. doi:10.3389/fnins.2023.1302132
14. Hu X, Wang M, Wang Z, et al. Predictors and lesion patterns of dysphagia and swallowing outcomes after acute intracerebral hemorrhage. Ther Adv Neurol Disord. 2025;18:17562864241311130. doi:10.1177/17562864241311130
15. Zhang P, Zhang W, Shi W, et al. Swallowing function after acute ischemic stroke: development and validation of a novel clinical prognostic model. Front Nutr. 2022;9:970253. doi:10.3389/fnut.2022.970253
16. Gandolfo C, Sukkar S, Ceravolo MG, et al. The predictive dysphagia score (PreDyScore) in the short- and medium-term post-stroke: a putative tool in PEG indication. Neurol Sci. 2019;40(8):1619–1626. doi:10.1007/s10072-019-03896-2
17. Yoon KJ, Park CH, Rho MH, Kim M. Disconnection-Based Prediction of Poststroke Dysphagia. AJNR Am J Neuroradiol. 2023;45(1):57–65. doi:10.3174/ajnr.A8074
18. Seo M, Lee C, Nam K, Kwon BS, Kim BH, Park JW. Predicting Long-Term Prognosis of Poststroke Dysphagia with Machine Learning. J Clin Med. 2025;14(14):5025. doi:10.3390/jcm14145025
19. Lee WH, Lim Mh, HG S, My S, Oh BM, Kim S. Development of a Novel Prognostic Model to Predict 6-Month Swallowing Recovery After Ischemic Stroke. Stroke. 2020;51(2):440–448. doi:10.1161/strokeaha.119.027439
20. Zhang L, Tang X, Wang C, et al. Predictive Model of Dysphagia and Brain Lesion-Symptom Mapping in Acute Ischemic Stroke. Front Aging Neurosci. 2021;13:753364. doi:10.3389/fnagi.2021.753364
21. Lu C, Zhou Y, Shen Y, Wang Y, Qian S. Establishment and validation of early prediction model for post-stroke dysphagia. Aging Clin Exp Res. 2025;37(1):145. doi:10.1007/s40520-025-03060-1
22. Xie M, Liu Z, Dai F, Cao Z, Wang X. Predicting Stroke-Associated Pneumonia in Acute Ischemic Stroke: a Machine Learning Model Development and Validation Study with CBC-Derived Inflammatory Indices. Int J Gen Med. 2025;18:3117–3128. doi:10.2147/ijgm.S524450
23. Bonkhoff AK, Grefkes C. Precision medicine in stroke: towards personalized outcome predictions using artificial intelligence. Brain. 2022;145(2):457–475. doi:10.1093/brain/awab439
24. Alkhanbouli R, Matar Abdulla Almadhaani H, Alhosani F, Simsekler MCE. The role of explainable artificial intelligence in disease prediction: a systematic literature review and future research directions. BMC Med Inform Decis Mak. 2025;25(1):110. doi:10.1186/s12911-025-02944-6
25. Chinese Society of Neurology, Cerebrovascular Disease Group. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2023. Chin J Neurol. 2024;57(6):523–559.
26. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
27. Ye C, Zhao L, He X, et al. Association between oral dryness and dysphagia in community-dwelling older population. J Nutr Health Aging. 2025;29(6):100533. doi:10.1016/j.jnha.2025.100533
28. Chen Y, Lv W, Liu X, et al. Development of a prediction model for hemorrhagic transformation after intravenous thrombolysis in patients with acute ischemic stroke: a retrospective analysis. BMC Med Inform Decis Mak. 2025;25(1):227. doi:10.1186/s12911-025-03068-7
29. Shan X, Zhang M, Liang Y, et al. Application of Machine Learning to Predict Postoperative Nausea and Vomiting in Laparoscopic Sleeve Gastrectomy. Obes Surg. 2025;35(7):2663–2672. doi:10.1007/s11695-025-07951-0
30. Li A, Liu Y, Luo Y, et al. Machine learning based predictive model of the risk of Tourette syndrome with SHAP value interpretation: a retrospective observational study. Sci Rep. 2025;15(1):18336. doi:10.1038/s41598-025-01874-7
31. Karisik A, Moelgg K, Buergi L, et al. Impact of dysphagia on early psychosocial consequences after acute ischemic stroke. J Neurol Sci. 2025;476:123624. doi:10.1016/j.jns.2025.123624
32. Karisik A, Moelgg K, Buergi L, et al. Dysphagia increases the risk of post-stroke fatigue. Eur J Neurol. 2025;32(1):e16570. doi:10.1111/ene.16570
33. Hotz JF, Kaindl L, Schneider L, et al. Dysphagia Management is Associated with Reduced Mortality in Patients with Moderate to Severe Acute Ischemic Stroke. Neurol Ther. 2025;14(4):1539–1552. doi:10.1007/s40120-025-00783-1
34. Uddin S, Khan A, Hossain ME, Moni MA. Comparing different supervised machine learning algorithms for disease prediction. BMC Med Inf Decis Making. 2019;19(1):281. doi:10.1186/s12911-019-1004-8
35. Henriksson A, Zhao J, Dalianis H, Boström H. Ensembles of randomized trees using diverse distributed representations of clinical events. BMC Med Inform Decis Mak. 2016;16(Suppl 2):69. doi:10.1186/s12911-016-0309-0
36. Lin Z, He H, Yan M, Chen X, Chen H, Ke J. Machine learning and the nomogram as the accurate tools for predicting postoperative malnutrition risk in esophageal cancer patients. Front Nutr. 2025;12:1606470. doi:10.3389/fnut.2025.1606470
37. Qi B, Kong K, Wu Q, et al. Machine learning-driven prediction of risk factors for postoperative re-fractures in elderly OVCF patients with underlying diseases: model development and validation. Front Med Lausanne. 2025;12:1616923. doi:10.3389/fmed.2025.1616923
38. Balagurunathan Y, Mitchell R, El Naqa I. Requirements and reliability of AI in the medical context. Phys Med. 2021;83:72–78. doi:10.1016/j.ejmp.2021.02.024
39. Reyes-Torres CA, Castillo-Martínez L, Ramos-Vázquez AG, Chávez-Moreno DV, Serralde-Zúñiga AE. A low phase angle determined by bioelectrical impedance analysis is associated with oropharyngeal dysphagia among institutionalized older adults. Rev Assoc Med Bras. 2021;67(8):1161–1166. doi:10.1590/1806-9282.20210578
40. Mao L, Wang J, Li Y, et al. Risk factors for dysphagia in patients with acute and chronic ischemic stroke: a retrospective cohort study. Heliyon. 2024;10(2):e24582. doi:10.1016/j.heliyon.2024.e24582
41. Rao Y, Wei J, Liu S, Liao B. Preliminary exploration of clinical prediction model of severe swallowing disorder after acute ischemic stroke based on nomogram model. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023;35(4):371–375. doi:10.3760/cma.j.cn121430-20220525-00512
42. Jeyaseelan RD, Vargo MM, Chae J. National Institutes of Health Stroke Scale (NIHSS) as An Early Predictor of Poststroke Dysphagia. Pm r. 2015;7(6):593–598. doi:10.1016/j.pmrj.2014.12.007
43. Wang Z, Shi Y, Zhang L, Wu L, Fang Q, Huiling L. Nomogram for predicting swallowing recovery in patients after dysphagic stroke. JPEN J Parenter Enteral Nutr. 2022;46(2):433–442. doi:10.1002/jpen.2115
44. Labeit B, Mueller H, Muhle P, et al. Predicting Dysphagia with National Institute of Health Stroke Scale: distinction between Infra- and Supratentorial Region is Essential. Cerebrovasc Dis. 2018;46(3–4):152–160. doi:10.1159/000493371
45. Wang Z, Shi R, Moreira P. Post-stroke dysphagia: identifying the evidence missing. Review. Front Med. 2025;12:2025. doi:10.3389/fmed.2025.1494645
46. Wilmskoetter J, Bonilha L, Martin-Harris B, Elm JJ, Horn J, Bonilha HS. Factors Influencing Oral Intake Improvement and Feeding Tube Dependency in Patients with Poststroke Dysphagia. J Stroke Cerebrovasc Dis. 2019;28(6):1421–1430. doi:10.1016/j.jstrokecerebrovasdis.2019.03.031
47. Sasegbon A, Cheng I, Hamdy S. The neurorehabilitation of post-stroke dysphagia: physiology and pathophysiology. J Physiol. 2025;603(3):617–634. doi:10.1113/jp285564
48. Safia A, Najjar R, Abdelhadi U, et al. The association between cervical diffuse idiopathic skeletal hyperostosis and dysphagia. Sci Rep. 2025;15(1):24613. doi:10.1038/s41598-025-08937-9
49. Zhao J, Chen M, Mo J, et al. Prognostic value of albumin-based malnutritional indices on short-term outcome in acute ischemic stroke patients undergoing reperfusion therapy. Front Nutr. 2025;12:1659446. doi:10.3389/fnut.2025.1659446
50. Seğmen F, Aydemir S, Kayan T, et al. Clinical Significance of Sarcopenia Defined by the Cross-Sectional Area of the Masseter Muscle in Cerebrovascular Events: a Retrospective Cohort Study. Medicina. 2025;61(2):268. doi:10.3390/medicina61020268
51. Pinho J, Meyer T, Schumann-Werner B, et al. Swallowing muscle mass contributes to post-stroke dysphagia in ischemic stroke patients undergoing mechanical thrombectomy. J Cachexia, Sarcopenia Muscle. 2024;15(4):1539–1548. doi:10.1002/jcsm.13512
52. Żdanowicz A, Sobkowiak H, Gawrysiak M, Wiszniewska M. Swallowing Disorders in Ischemic Stroke: a Retrospective Analysis of Dysphagia Severity Differences Based on Hemisphere Damage and Patient Age. J Clin Med. 2025;14(3):900. doi:10.3390/jcm14030900
53. Yu L, Li Y, Zhang D, et al. A risk prediction model for dysphagia in older patients: a single-center prospective study. Geriatr Nurs. 2022;44:24–29. doi:10.1016/j.gerinurse.2021.12.013
54. Chinese Expert Consensus Writing Group for the Diagnosis and Treatment of Atherosclerotic Ischemic Stroke/Transient Ischemic Attack with Coronary Heart Disease. Chinese expert consensus on the diagnosis and treatment of atherosclerotic ischemic stroke/transient ischemic attack complicated with coronary heart disease. Natl Med J China. 2022;102(45):3569–3580.
55. Qin Y, Tang Y, Liu X, Qiu S. Neural basis of dysphagia in stroke: a systematic review and meta-analysis. Front Hum Neurosci. 2023;17:1077234. doi:10.3389/fnhum.2023.1077234
56. Jin X, Shang S, Tong H, Liu M, Li D, Xiao Y. Predictors of recovery from dysphagia after stroke: a systematic review and meta-analysis. Int J Nurs Sci. 2025;12(2):184–191. doi:10.1016/j.ijnss.2025.02.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Lung Ultrasound-Based Nomogram for the Prediction of Refractory Mycoplasma pneumoniae Pneumonia in Hospitalized Children
Liu G, Wang G, Yang Z, Liu G, Ma H, Lv Y, Ma F, Zhu W
Infection and Drug Resistance 2022, 15:6343-6355
Published Date: 31 October 2022
Using Machine Learning Algorithms to Predict High-Risk Factors for Postoperative Delirium in Elderly Patients
Liu Y, Shen W, Tian Z
Clinical Interventions in Aging 2023, 18:157-168
Published Date: 8 February 2023
Ten-Year Multicenter Retrospective Study Utilizing Machine Learning Algorithms to Identify Patients at High Risk of Venous Thromboembolism After Radical Gastrectomy
Liu Y, Song C, Tian Z, Shen W
International Journal of General Medicine 2023, 16:1909-1925
Published Date: 18 May 2023
A Prospective Study of Stroke Characteristics, Risk Factors, and Mortality in a Tertiary Hospital of Northern Ethiopia
Gidey K, Hailu A
International Journal of General Medicine 2023, 16:5051-5061
Published Date: 3 November 2023
A Machine-Learning Model Based on Clinical Features for the Prediction of Severe Dysphagia After Ischemic Stroke
Ye F, Cheng LL, Li WM, Guo Y, Fan XF
International Journal of General Medicine 2024, 17:5623-5631
Published Date: 28 November 2024