Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Postoperative Complications Following Neoadjuvant Therapy Across Different Oncoplastic Breast Surgery Techniques: A Retrospective Comparative Study in Breast Cancer Patients
Authors Kulturoglu MO ![]() , Dogan L, Gulcelik MA
, Dogan L, Gulcelik MA
Received 5 March 2026
Accepted for publication 20 May 2026
Published 27 May 2026 Volume 2026:18 607172
DOI https://doi.org/10.2147/BCTT.S607172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Mahmut Onur Kulturoglu,1 Lutfi Dogan,1 Mehmet Ali Gulcelik2
1Department of Surgical Oncology, University of Health Sciences, Ankara Etlik City Hospital, Ankara, Turkey; 2Department of Surgical Oncology, University of Health Sciences, Gulhane Faculty of Medicine, Ankara, Turkey
Correspondence: Mahmut Onur Kulturoglu, Email [email protected]
Background: Neoadjuvant therapy (NAT) is increasingly used in breast cancer to downstage tumors and expand eligibility for breast-conserving approaches. NAT may also influence tissue vascularity and wound healing capacity, potentially affecting postoperative morbidity. Oncoplastic breast surgery (OBS) improves cosmetic outcomes while maintaining oncological safety; however, the impact of specific OBS techniques on postoperative complications after NAT remains unclear. In this context, postoperative complications are clinically important as they may lead to delayed initiation of adjuvant therapy, increased hospital stay, higher morbidity, and impaired cosmetic and quality-of-life outcomes. This study aimed to evaluate the associations between different OBS techniques and postoperative complications in patients undergoing surgery after NAT.
Methods: This retrospective study included patients who underwent level II OBS after NAT between 2019 and 2025. Patients were categorized into five groups according to the surgical technique: racquet; vertical; radial fusiform incision; batwing–donut–Grisotti; and J-, L-, or V-shaped mammoplasties. The primary endpoint was comparison of complication rates among techniques. Secondary endpoints included identification of factors associated with complications. Complications were graded using the Clavien–Dindo classification, and overall morbidity was assessed using the Comprehensive Complication Index (CCI).
Results: A total of 556 patients were analyzed. Racquet and vertical mammoplasties were associated with significantly larger resection volumes than the other techniques. These two techniques demonstrated significantly higher rates of overall and major complications, as well as wound dehiscence, surgical site infection, and seroma (p< 0.05). Clavien–Dindo grades and CCI scores were also significantly higher in the racquet and vertical mammoplasty groups. Despite these differences, reoperation rates did not differ significantly between techniques.
Conclusion: Postoperative complication rates were significantly influenced by the OBS technique chosen following NAT. Racquet and vertical mammoplasties were associated with higher morbidity, likely due to larger resection volumes, altered tissue perfusion, and more extensive tissue dissection. Individualized technique selection based on tumor characteristics, breast anatomy, and patient risk factors is essential to minimize complications while preserving oncological safety and aesthetic outcomes.
Keywords: neoadjuvant therapy, breast cancer, oncoplastic surgery, postoperative complications, different oncoplastic techniques
Introduction
Historically, neoadjuvant therapy (NAT) has been used in the treatment of breast cancer to reduce tumor size and downstage axillary lymph node involvement, thereby increasing the likelihood of breast-conserving surgery and potentially avoiding axillary dissection. Over time, its indications have expanded, and it is now increasingly administered to patients with operable early-stage disease. Another advantage of NAT is that it enables in vivo assessment of the tumor response to systemic therapy, providing valuable prognostic and therapeutic information.1 However, concerns remain regarding the potential impact of NAT on postoperative complications. Most agents used for breast cancer treatment exert their cytotoxic effects by inhibiting DNA or RNA synthesis, protein production, or cellular division. Consequently, cytotoxic chemotherapeutic agents may impair wound healing by directly affecting fibroblast proliferation and collagen synthesis, as well as through their effects on the immune system and vascular endothelium. These cytotoxic effects may increase the risk of postoperative complications, although studies investigating the impact of NAT on surgical complications have reported conflicting results.2,3
Surgical management of breast cancer has evolved significantly over time, shifting from radical mastectomy to breast-conserving approaches. The growing emphasis on aesthetic outcomes without compromising oncological safety has increased the demand for oncoplastic breast surgery,4 which combines oncologic resection principles with plastic surgical techniques, allowing for wider tumor excision while preserving the breast contour and symmetry. This approach facilitates larger resections, reduces re-excision rates, improves cosmetic outcomes, and contributes to lower mastectomy rates. Furthermore, oncoplastic surgery has been associated with lower complication rates and reduced overall costs compared with mastectomy followed by immediate reconstruction.5
Oncoplastic breast surgery encompasses a spectrum of techniques that can be broadly categorized into volume displacement and volume replacement procedures. Volume displacement techniques, such as various therapeutic mammoplasty patterns (eg., racquet, vertical, J-, L-, and V-shaped mammoplasties), utilize reshaping of the remaining breast tissue after tumor excision. In contrast, volume replacement techniques involve the use of local or distant flaps to reconstruct the resected defect. These techniques are selected based on tumor location, breast size, and patient-specific anatomical factors, and each carries distinct implications in terms of resection volume, tissue mobilization, and potential postoperative morbidity.6 Although the wider resections and more extensive tissue manipulation in oncoplastic surgery raise concerns regarding an increased risk of postoperative complications, previous studies have demonstrated comparable complication rates between conventional breast-conserving surgery and oncoplastic techniques. However, these studies included a heterogeneous group of oncological and reconstructive procedures. Data specifically evaluating the effect of individual oncoplastic techniques on postoperative complications are limited.7
This study aimed to evaluate the impact of different oncoplastic breast surgery techniques on postoperative complications in patients with breast cancer who underwent surgery after NAT. Specifically, we assessed the incidence and distribution of complications associated with each oncoplastic technique and determined whether the choice of surgical technique influenced postoperative morbidity.
Materials and Methods
This study employed a consecutive sampling method, including all eligible patients who underwent neoadjuvant chemotherapy followed by oncoplastic surgery between 2019 and 2025. All procedures were performed by the same group of breast surgeons, each with more than 10 years of experience in oncoplastic breast surgery, to ensure technical consistency and minimize inter-operator variability across cases. The study was conducted in a single tertiary referral center, and patients were identified from a prospectively maintained institutional database. The study period was intentionally selected starting from 2019, when the surgeons had already exceeded 10 years of oncoplastic surgical experience, thereby ensuring a mature and standardized surgical practice, and extending to the most recent cases to reflect current outcomes. Consecutive patients who met the eligibility criteria during the study period were included in the analysis. Patients were excluded if they had a concurrent malignancy other than breast cancer, had undergone surgery without neoadjuvant therapy, had incomplete clinical or pathological data, or lacked adequate follow-up information.
The primary endpoint of the study was to evaluate the association between the oncoplastic breast surgery technique used and the complication rates observed for each technique. Complication rates were compared across the different surgical technique groups. Independent factors associated with postoperative complications were analyzed as a secondary objective.
Patients were categorized into five groups according to the oncoplastic breast surgery techniques performed, as described by Gulcelik et al8 Level II oncoplastic techniques were classified based on tumor location (primarily breast quadrants), incision planes, and incision lengths. The surgical techniques included in each group were as follows: Group 1, racquet mammoplasty; Group 2, vertical mammoplasty, including Wise-pattern and comma mammoplasty techniques; Group 3, mammoplasty using radial and fusiform incisions; Group 4, donut, Batwing, and Grisotti techniques; and Group 5, dermoglandular rotation flaps, including J-, L-, and V-type mammoplasty techniques.
Data on surgery-related complications were collected, including those occurring after the primary surgery and after any reoperations performed to manage or correct these complications. Potential influencing factors were also recorded, including patient age, body mass index (BMI), comorbidities, smoking history, tumor size, type of breast and axillary surgery performed, excised tissue volume, and whether contralateral symmetrization surgery was performed. Patients were followed up prospectively during their postoperative hospital stay and subsequently evaluated in the outpatient clinic at 1 week, 1 month, and 3 months after surgery. Data on postoperative complications associated with the oncoplastic surgery were collected during these follow-up visits. For patients who underwent contralateral symmetrization surgery, only complications related to the index (cancer-affected) breast were included in the analysis.
Major complications included active bleeding and wound dehiscence. Active bleeding was defined as perioperative bleeding causing hypotension and/or requiring blood transfusion. Wound dehiscence was defined as complete wound separation, wound edges requiring resuturing, or prolonged wound care. Minor complications included partial skin necrosis, surgical site infections, seroma, and hematoma. Partial skin necrosis was defined as superficial skin necrosis or skin loss occurring without complete wound dehiscence. Seroma and hematoma were classified as minor complications if they were clinically stable or successfully managed with percutaneous drainage.
All complications were classified according to the Clavien–Dindo classification system. Any deviation from the normal postoperative course that did not require pharmacological or surgical intervention, including wound infections managed with antibiotics alone, was classified as Grade I. Complications requiring pharmacological treatment beyond those permitted for Grade I complications were classified as Grade II. Complications requiring surgical intervention were classified as Grade III.
The Comprehensive Complication Index (CCI) is a widely used tool for grading the overall burden of postoperative complications. The CCI is a continuous scale ranging from 0 (no complications) to 100 (death), allowing quantitative assessment of cumulative morbidity by incorporating all complications and their respective severities.9 This index provides a more comprehensive evaluation of postoperative morbidity than the conventional categorical grading systems. In the present study, the CCI was calculated using a validated online calculator (available at http://www.cci.assessurgery.com).
This study protocol was reviewed and approved by the Health Sciences University, Ankara Etlik City Hospital ethics committee with an approval number AEŞH-BADEK2-2026-212.
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as means and standard deviations (SD) or medians and interquartile ranges [IQRs], as appropriate, while categorical variables are presented as frequencies and percentages (n, %). Categorical variables were compared using the chi-square test and continuous variables were analyzed using one-way ANOVA or Kruskal–Wallis test, as appropriate based on distribution. To identify independent predictors of postoperative complications, multivariate binary logistic regression analyses were performed for both overall and major complications. The following variables were included as covariates based on their clinical relevance: surgical technique group, age, body mass index, tumor size, comorbidity status, and smoking status. Results are reported as odds ratios (OR) with 95% confidence intervals (CI). Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit test. A two-sided p-value ≤ 0.05 was considered statistically significant. Effect sizes were reported for all analyses: Cramér’s V for categorical variables, epsilon squared (ε2) for non-normally distributed continuous variables, and Cohen’s f for normally distributed continuous variables.
A post-hoc power analysis was performed using GPower (version 3.1.9.4). Based on the primary outcome of major complication rates (Cramér’s V=0.154, α=0.05, N=556), the achieved statistical power was 84.3%, confirming adequate sample size for the detection of the observed effect.
Results
This study included 556 patients who underwent oncoplastic breast surgery after NAT. The patients were divided into five groups according to oncoplastic surgical technique: racquet mammoplasty (n=150); vertical mammoplasty (n=138); mammoplasty using radial fusiform incision (n=139); mammoplasty using batwing, donut, and Grisotti techniques (n=81); and mammoplasty using J-, L-, and V-shaped incisions (n=48). The groups were comparable in terms of mean age, BMI, smoking status, and comorbidity profile, with no significant intergroup differences. The median tumor size was 18 mm, with significantly smaller tumors in the vertical (median: 15 mm) and radial fusiform incision (median: 14 mm) mammoplasty groups than in the other groups (p<0.001). When the groups were evaluated in terms of resection volume, the quantity of excised tissue was significantly greater in the racquet (median: 218 cm3) and vertical (median: 188 cm3) mammoplasty groups than in the other groups (p<0.001). No significant differences were observed between the groups with respect to the type of axillary surgery performed; in contrast, contralateral symmetrization procedures were performed more frequently in patients who underwent vertical mammoplasty (Table 1).
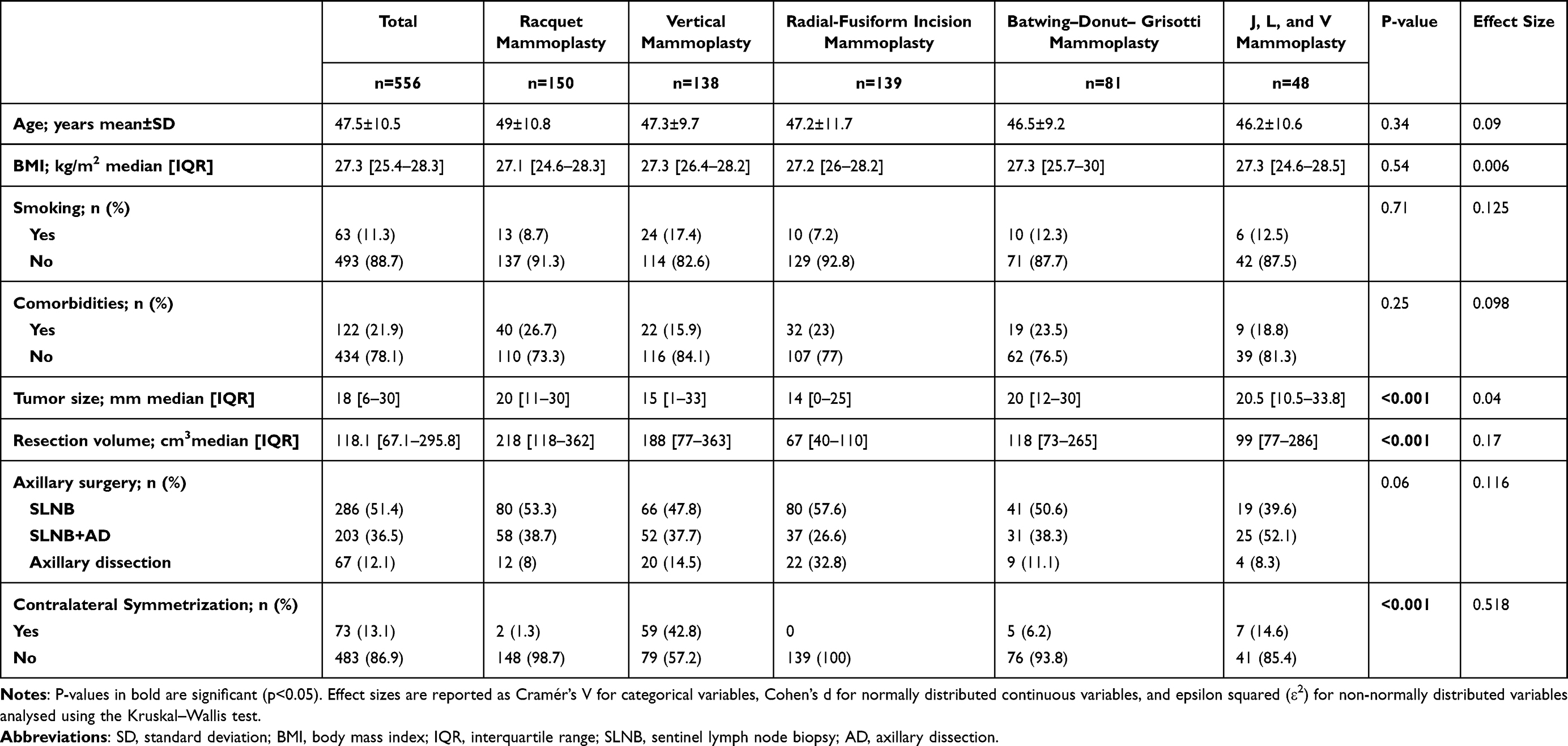 |
Table 1 Comparison of Clinicopathological Characteristics by Oncoplastic Surgical Technique |
When patients were compared in terms of overall postoperative complications, the complication rates were significantly higher in the racquet (37.3%) and vertical (32.6%) mammoplasty groups than in the radial fusiform incision (22.3%), batwing–donut–Grisotti (22.2%), and J-, L-, and V–incision (25%) mammoplasty groups (p=0.03). Overall, complications occurred in 162 (29.1%) patients, with major complications in 71 (12.8%) and minor complications in 109 (19.6%). Major and minor complications were observed concurrently in 18 patients.
Major complications were observed significantly more frequently in the racquet (18.7%), vertical (15.2%), and radial fusiform incision (11.5%) mammoplasty groups than in the batwing–donut–Grisotti (4.9%) and J-, L-, and V–incision (4.2%) mammoplasty groups (p=0.01). Wound dehiscence occurred significantly more frequently in the racquet (14%), vertical (9.4%), and radial fusiform incision (9.4%) mammoplasty groups than in the batwing–donut–Grisotti (1.2%) and J-, L-, and V–incision (2.1%) mammoplasty groups (p=0.01). However, active bleeding rates did not significantly differ between the groups (p=0.55).
The overall rates of minor complications did not significantly differ between the groups (p=0.09). Minor complications included wound infection, partial skin necrosis, seroma, and hematoma. The overall incidence of wound infection was 6.7%. Wound infection rates were significantly higher in the racquet (11.3%), vertical (8%), and J-, L-, and V–incision (6.3%) mammoplasty groups than in the radial fusiform incision (2.9%) and batwing–donut–Grisotti (2.5%) mammoplasty groups (p=0.03). With respect to seroma formation, a significant difference was observed between the groups (p=0.03), with higher rates in the racquet (9.3%) and vertical (12.5%) mammoplasty groups than in the radial fusiform incision (3.6%), batwing–donut–Grisotti (1.2%), and J-, L-, and V–incision (6.5%) mammoplasty groups. The rates of partial skin necrosis (p=0.33) and hematoma formation (p=0.48) did not significantly differ between the groups.
On multivariate binary logistic regression analysis, surgical technique was an independent predictor of both overall (p=0.040) and major complications (p=0.026). Specifically, racquet mammoplasty was associated with a five-fold increased risk of major complications compared to J-L-V mammoplasty (OR=5.037, 95% CI: 1.148–22.094, p=0.032), after adjusting for age, BMI, tumor size, comorbidities, and smoking status. No other variables were identified as independent predictors of postoperative complications.
The Clavien–Dindo complication classifications significantly differed between the groups (p=0.04). Clavien–Dindo grade II complications were significantly more frequent in the racquet (16.7%), vertical (11.6%), and batwing–donut–Grisotti (8.6%) mammoplasty groups than in the radial fusiform incision (2.5%) and J-, L-, and V–incision (4.2%) mammoplasty groups (p=0.01). However, the rates of Clavien–Dindo grade I (p=0.36) and grade III (p=0.76) complications did not significantly differ between the groups.
When complications were evaluated using the CCI, the scores were significantly higher in patients who underwent racquet, vertical, and J-, L-, and V–incision mammoplasties than in those who underwent radial fusiform incision and batwing–donut–Grisotti mammoplasties (p=0.02). The rates of reoperation due to complications did not differ between the groups (p=0.76) (Table 2).
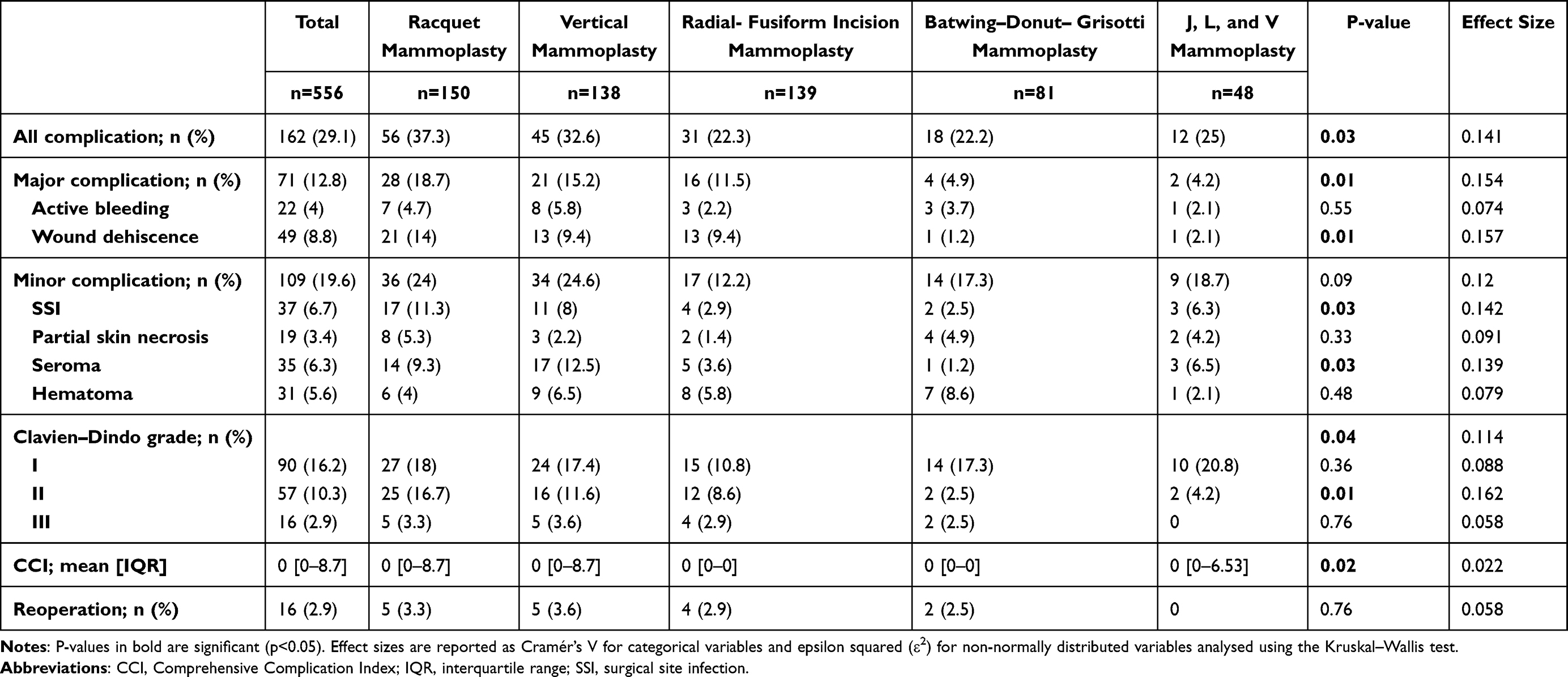 |
Table 2 Comparison of Postoperative Complications by Oncoplastic Surgical Technique |
Discussion
In this study, we evaluated the association between oncoplastic surgical technique selection and postoperative complications following NAT, and the choice of oncoplastic technique was found to significantly influence complication rates. The racquet and vertical mammoplasty techniques were associated with higher overall and major complication rates, as well as higher Clavien–Dindo grades and CCI scores. This difference may be related to larger resection volumes and the need for more extensive tissue dissection inherent to these techniques. Nevertheless, comparable reoperation rates across techniques suggest that most complications were successfully managed with conservative treatment rather than surgical reintervention.
Oncoplastic breast surgery techniques are classified based on the volume of excised breast tissue (level I: <20%; level II: 20–50%; level III: >50%). The quantity of resected tissue and the extent of tissue mobilization for reconstruction may influence postoperative outcomes. However, studies directly comparing different oncoplastic surgical techniques remain limited. In a study evaluating patient-reported outcomes following level I and II oncoplastic breast surgery techniques, similar outcomes were reported across techniques in terms of breast satisfaction, psychosocial well-being, and sexual well-being.10 Another study evaluating long-term outcomes of level II oncoplastic techniques demonstrated favorable local control and low complication rates, although without direct comparison between individual techniques.11
In a previous study evaluating patients who did not receive NAT, differences in complication rates among oncoplastic techniques were reported, with racquet and vertical mammoplasties being associated with higher morbidity. This was attributed to larger tissue resections and increased wound tension, particularly in vertical mammoplasty, where extensive skin undermining and pillar approximation may predispose to wound dehiscence.8 Importantly, in such cases, inadequate tension-free closure may necessitate modification of the surgical approach. In the present study, which specifically included patients treated with NAT, postoperative complications were compared across different oncoplastic techniques. Racquet and vertical mammoplasties were associated with significantly larger excision volumes and higher overall complication rates, particularly wound dehiscence. Seroma formation and surgical site infections were also more frequent in these groups. Although minor complication rates overall were similar between groups, the distribution of specific complications varied according to surgical technique. These findings suggest that the observed differences may be influenced not only by surgical technique but also by tumor burden, resection extent, and patient-related factors.
It is important to acknowledge that these associations may be affected by residual confounding factors, including tumor size, breast volume, comorbidities, and extent of resection, which may not be fully controlled in this retrospective design. In addition, selection bias inherent to non-randomized studies may have influenced the distribution of surgical techniques among patients. Therefore, the observed relationships should be interpreted as associations rather than causal effects.
The increasing use of NAT has led to a higher rate of breast-conserving and oncoplastic procedures. Chemotherapy may adversely affect wound healing through its effects on immune function, leukocyte count, and fibroblast-mediated collagen synthesis, potentially leading to impaired tissue repair. However, existing literature has reported conflicting findings regarding the impact of NAT on postoperative complications. Some studies have demonstrated no significant difference in complication rates between patients receiving NAT and those undergoing upfront surgery,12 while a meta-analysis similarly found no overall association. Notably, the authors emphasized substantial heterogeneity across studies, partly due to differences in surgical techniques, which may independently influence complication risk.2 In this context, the present study adds value by specifically evaluating technique-related variability in patients undergoing NAT, demonstrating significant differences in complication profiles across oncoplastic approaches.
Oncoplastic breast surgery has been increasingly adopted because it enables oncologically safe resection while improving aesthetic outcomes and expanding indications for breast-conserving surgery. However, concerns remain regarding potential increases in postoperative morbidity due to larger resections and reconstructive manipulation of glandular tissue.13 Despite these concerns, most studies report comparable complication rates between oncoplastic and conventional breast-conserving surgery.14–16 Wound dehiscence appears to be more frequent after oncoplastic procedures when managed conservatively, although rates of major complications such as infection, hematoma, seroma, necrosis, and reoperation are generally similar between approaches.16,17 Overall, these findings support the safety profile of oncoplastic breast surgery, while highlighting the importance of patient selection and surgical planning.
Finally, variability in complication reporting systems and surgical technique classification across studies limits direct comparisons in the literature. This underscores the need for standardized reporting of postoperative outcomes in oncoplastic breast surgery to improve comparability and strengthen evidence-based surgical decision-making.
This study has some limitations that should be acknowledged. Data on patient-reported outcomes were not included; therefore, patient satisfaction and quality-of-life outcomes following different oncoplastic surgical techniques could not be evaluated. In addition, the retrospective design introduces inherent limitations and unmeasured confounding. The conclusions primarily reflect short-term postoperative outcomes, and long-term functional and patient-reported outcomes were not assessed.
Conclusion
The selection of an oncoplastic surgical technique after NAT was found to be associated with postoperative complication rates. When planning oncoplastic breast surgery after NAT, oncological safety, tumor size, resection volume, and the extent of the surgical technique should be carefully considered to minimize the risk of complications. Appropriate technique selection may contribute to reducing surgical morbidity while supporting optimal oncological and aesthetic outcomes. These findings should be interpreted in the context of a retrospective single-center study reporting short-term postoperative outcomes.
Abbreviations
AD, axillary dissection; BMI, body mass index; CCI, comprehensive complication index; CI, confidence interval; IQR, interquartile range; NAT, neoadjuvant therapy; OBS, oncoplastic breast surgery; OR, odds ratio; SD, standard deviation; SLNB, sentinel lymph node biopsy; SSI, surgical site infection.
Data Sharing Statement
The datasets were requested from the corresponding author (Mahmut Onur Kulturoglu).
Ethics Approval and Informed Consent
Ethical approval for this study was obtained from the Ethics Committee of the Ankara Etlik City Hospital (approval number: AEŞH-BADEK2-2026-212). This study was conducted in accordance with the Declaration of Helsinki, and informed consent was obtained from eligible participants.
Consent for Publication
This manuscript does not contain any individual person’s data in any form (including individual details, images, or videos).
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The Authors declare that they have no conflict of interests. The Authors declare that the article has been submitted only to this journal and has not been published, published in the press, or sent elsewhere (including preprint servers). The Authors verify that the research complies with ethical rules, including compliance with the legal requirements of the country of study.
References
1. Asaoka M, Gandhi S, Ishikawa T, Takabe K. Neoadjuvant chemotherapy for breast cancer: past, present, and future. Breast Cancer. 2020;14.
2. Lorentzen T, Heidemann LN, Möller S, Bille C. Impact of neoadjuvant chemotherapy on surgical complications in breast cancer: a systematic review and meta-analysis. Euro J Surg Oncol. 2022;48(1):44–9. doi:10.1016/j.ejso.2021.09.007
3. Sutton TL, Johnson N, Schlitt A, Gardiner SK, Garreau JR. Surgical timing following neoadjuvant chemotherapy for breast cancer affects postoperative complication rates. Ame J Surg. 2020;219(5):741–745. doi:10.1016/j.amjsurg.2020.02.061
4. Shojaee L, Sayyadi S, Dehghanian E, Shakeriastani K, Shokoohy F, Shakeriastani K. Comparative analysis of postoperative complications and outcomes between oncoplastic and conventional breast-conserving surgery in iranian females. Indian J Surg. 2026;88(1):86–92. doi:10.1007/s12262-025-04348-2
5. Jonczyk MM, Jean J, Graham R, Chatterjee A. Surgical trends in breast cancer: a rise in novel operative treatment options over a 12 year analysis. Breast Cancer Res Treat. 2019;173(2):267–274. doi:10.1007/s10549-018-5018-1
6. Vindigni V, Marena F, Zanettin C, Bassetto F. Breast reconstruction: the oncoplastic approach. J Clin Med. 2024;13(16):4718. doi:10.3390/jcm13164718
7. Moen M, Holton T, Phung A, et al. Complications after oncoplastic breast reduction and impact on time to adjuvant therapy. Plast Reconstr Surg Glob Open. 2024;12(7):e6010. doi:10.1097/GOX.0000000000006010
8. Gulcelik MA, Dogan L, Karanlik H, Akinci M, Ugurlu MU, Gulluoglu BM. Profile of surgical complications and complication-led reoperation rates in breast cancer patients who underwent oncoplastic breast surgery with volume displacements. Euro J Surg Oncol. 2025;51(8):110252. doi:10.1016/j.ejso.2025.110252
9. Slankamenac K, Graf R, Barkun J, Puhan MA, Clavien P-A. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg. 2013;258(1):1–7. doi:10.1097/SLA.0b013e318296c732
10. Ritter M, Oberhauser I, Montagna G, et al. Comparison of patient-reported outcomes among different types of oncoplastic breast surgery procedures. J Plastic, Reconstruct Aesthetic Surg. 2022;75(9):3068–3077. doi:10.1016/j.bjps.2022.04.051
11. Gulcelik MA, Dogan L, Karaman N, Bahcecitapar M, Ozaslan C. Oncoplastic level II surgical techniques for breast cancer treatment: long-term outcomes. Breast Care. 2022;17(1):24–30. doi:10.1159/000514468
12. Nussbaumer RL, Maggi N, Castrezana L, et al. The impact of neoadjuvant systemic treatment on postoperative complications in breast cancer surgery. Breast Cancer Res Treat. 2023;197(2):333–341. doi:10.1007/s10549-022-06811-0
13. Benedict KC, Brown MI, Berry HA, Berry SM, O’Brien RC, Davis JM. Oncoplastic breast reduction: a systematic review of postoperative complications. Plastic Reconstruct Surg Global Open. 2023;11(10):e5355. doi:10.1097/GOX.0000000000005355
14. Crown A, Scovel LG, Rocha FG, Scott EJ, Wechter DG, Grumley JW. Oncoplastic breast conserving surgery is associated with a lower rate of surgical site complications compared to standard breast conserving surgery. Am J Surg. 2019;217(1):138–141. doi:10.1016/j.amjsurg.2018.06.014
15. Heil J, Riedel F, Golatta M, Hennigs A. Measurement and optimizing cosmetic outcomes for breast excisions/factors influencing aesthetic outcomes of breast conservation surgery. In: Oncoplastic Breast Surgery Techniques for the General Surgeon. Cham: Springer; 2020:93–106.
16. Rasmussen LF, Kiilerich CH, Trøstrup H, Hansen LB. Surgical outcomes and complications: a study comparing oncoplastic surgery and lumpectomy. Ann Breast Surg. 2024;8:24. doi:10.21037/abs-23-69
17. Almeida NR, Brenelli FP, Dos Santos CC, et al. Comparative study of surgical and oncological outcomes in oncoplastic versus non oncoplastic breast-conserving surgery for breast cancer treatment. JPRAS Open. 2021;29:184–194. doi:10.1016/j.jpra.2021.05.010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pretreatment System Inflammation Response Index (SIRI) is a Valuable Marker for Evaluating the Efficacy of Neoadjuvant Therapy in Breast Cancer Patients
Zhang Y, Wu J, Chen W, Liang X
International Journal of General Medicine 2024, 17:4359-4368
Published Date: 25 September 2024
Peripheral TNF-α and CD8+/CD28+ T Lymphocytes as Alternatives for PD-L1 Prediction in Breast Cancer Tumor Microenvironment: Stratified by Neoadjuvant Therapy
Wu J, Ou X, Yuan K, Shi F, Zhou Q, Lyu S, Li Y, Zhao Y, Cao Y, Sun J, Song Q
Breast Cancer: Targets and Therapy 2025, 17:627-637
Published Date: 19 July 2025
Oncoplastic or Conventional Breast-Conserving Surgery? Outcomes from a West Java Retrospective Cohort Study
Azhar RY, Dewayani BM, Erdiansyah Z, Nugraha P, Muhammad A, Alfarisy AN
International Journal of Women's Health 2025, 17:5533-5540
Published Date: 17 December 2025
Deep Learning Radiomics of Multiparametric MRI for Individualized Prediction of Axillary Lymph Node Response After Neoadjuvant Chemotherapy in Breast Cancer
Li S, Li R, Xu M, Liao J, Cao Z, Gong B, Yan F, Wang M, Tan H
Breast Cancer: Targets and Therapy 2026, 18:568337
Published Date: 21 January 2026
Efficacy and Safety of Neoadjuvant Stereotactic Body Radiotherapy (SBRT) Combined with Chemoimmunotherapy in Locally Advanced Breast Cancer: A Single-Center, Retrospective Pilot Study
Zhai M, Bi J, Ke Z, Hu M, Pi G, Li Y, He H, Li Y, Zheng H, Wu X, Verma V, Shao J, Han G
Breast Cancer: Targets and Therapy 2026, 18:577469
Published Date: 7 March 2026