Back to Journals » International Journal of Women's Health » Volume 17
Oncoplastic or Conventional Breast-Conserving Surgery? Outcomes from a West Java Retrospective Cohort Study
Authors Azhar RY, Dewayani BM ![]() , Erdiansyah Z, Nugraha P
, Erdiansyah Z, Nugraha P ![]() , Muhammad A
, Muhammad A ![]() , Alfarisy AN
, Alfarisy AN ![]()
Received 16 August 2025
Accepted for publication 9 December 2025
Published 17 December 2025 Volume 2025:17 Pages 5533—5540
DOI https://doi.org/10.2147/IJWH.S560836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Raden Yohana Azhar,1,* Birgitta M Dewayani,2,* Zuldi Erdiansyah,1,* Prapanca Nugraha,1,* Arrayyan Muhammad,3,* Ahmad Naufal Alfarisy3,*
1Department of Surgery of Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 2Department Pathology Anatomy of Hasan Sadikin General Hospital, Bandung, West Java, Indonesia; 3Department of Surgery of Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia
*These authors contributed equally to this work
Correspondence: Prapanca Nugraha, Department of Surgery, Hasan Sadikin General Hospital, Jalan Pasteur No. 38, Bandung, West Java, 40161, Indonesia, Email [email protected] Arrayyan Muhammad, Email [email protected]
Purpose: Breast-conserving surgery (BCS) followed by adjuvant radiotherapy is the standard treatment for early breast cancer in Indonesia. Our aim was to compare the outcomes of BCS with oncoplastic surgery (OPS), a less common method of breast cancer treatment in the country.
Patients and Methods: This retrospective cohort study was conducted at Hasan Sadikin General Hospital, Bandung, West Java, Indonesia. Patients with biopsy-proven Stage I to II breast cancer who underwent either OPS or BCS between 1 July 2020 to 30 June 2023, were identified. Data were collected by reviewing patient files and electronic records.
Results: A total of 82 patients were included in the study, with 43 (52.4%) undergoing BCS and 39 (47.6%) undergoing OPS. Age in OPS group 39.25 ± 4.9 was not significant difference compare with BCS group 39.86 ± 5.11. The mean tumor volume was higher in the OPS group (34.72 cm3) compared to the BCS group (22.35 cm3), and postoperative complications were also higher in the OPS group (7.6% vs 0%). Despite the use of frozen section analysis in the operating theatre, the frequency of positive margins was greater in the BCS group (9.3% vs 2.5%). There were no significant differences in the histologic type of tumor and immunohistochemistry between the two groups.
Conclusion: OPS is a valid alternative approach to breast cancer treatment that can be offered to women with early stage breast cancer at complex locations owing to the reduced occurrence of positive margins and thus lowered re-excision rates.
Plain Language Summary: This study compared two types of breast cancer surgery—standard breast-conserving surgery (BCS) and oncoplastic surgery (OPS)—among 82 women in Indonesia treated in the last five years. OPS combines tumor removal with plastic surgery techniques to improve cosmetic outcomes, especially for larger or more difficult-to-reach tumors. Of the 82 patients, 39 underwent OPS and 43 had BCS. Researchers looked at tumor size, whether cancer cells were left at the edges (margin positivity), and complications within 30 days after surgery. The average age of patients in both groups was around 39 years. OPS was more commonly chosen for larger tumors, and it resulted in fewer cases of positive margins— 2.5% in the OPS group compared to 9.3% in the BCS group—suggesting more complete tumor removal. Although OPS had a slightly higher rate of minor complications such as fluid buildup and fat necrosis, these were managed successfully without hospital readmission. Cosmetic outcomes were also better in the OPS group. OPS techniques varied based on tumor location, including flap reconstruction and breast reshaping methods. Despite its benefits, OPS is still new in Indonesia, and its wider use is limited by the need for specialized training and cultural factors that influence surgical choices. Nevertheless, the study concludes that OPS is a safe and effective alternative to standard BCS. It offers better cosmetic results and reduces the need for repeat surgery, making it a promising option for breast cancer treatment as surgical expertise continues to grow in the country.
Keywords: breast cancer, breast conserving surgery, oncoplastic surgery
Introduction
Breast-conserving surgery (BCS) followed by adjuvant radiotherapy has largely replaced mastectomy as the standard treatment for early breast cancers due to its ability to preserve the breast while maintaining comparable oncological safety.1–3 However, challenges such as larger tumors, extensive resection volumes, and medial tumor locations can limit achieving satisfactory cosmetic outcomes with BCS.4,5
The demand for favorable cosmetic results without compromising cancer treatment efficacy has led to the adoption of oncoplastic surgery (OPS) in breast cancer management. OPS combines oncologic principles with plastic surgical techniques, offering an alternative for treating early and larger breast tumors that might otherwise require mastectomy. OPS includes strategies like minimizing scar visibility, using mastopexy for volume displacement, and employing autologous tissue for volume replacement. Literatures comparing OPS with standard BCS shows similar results in terms of local recurrence rate but with better cosmetic outcomes.6–8 While the Western world is working towards standardizing the approach,9,10 OPS is still a new concept in Indonesia. There are limited numbers of trained oncoplastic breast surgeons in the country, resulting in scarce available data on oncoplastic surgery from Indonesia.
Therefore, this study aimed to compare surgical outcomes between OPS and BCS, focusing on tumor resection volume and margin positivity among early-stage breast cancer patients in Indonesia population. Specifically, the objectives of this study were to compare 30-day postoperative outcomes and complications (such as seroma development, fat necrosis, and wound infection) between the OPS and BCS groups, and to detail the surgical procedures used for OPS depending on the location of the tumor.
Materials and Methods
Study Settings
A multicentre retrospective cohort study was performed at Hasan Sadikin General Hospital (Faculty of Medicine, Universitas Padjadjaran) and Limijati Hospital in Bandung, West Java, covering the period from 1 July 2020 to 30 June 2023. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Review Committees of both institutions in 2023 (Ethical Exemption No. LB.02.01/X.6.5/317/2023). The committees waived informed consent because data were collected retrospectively from existing medical records. Institutional data retention policies were followed and all study data were stored on an encrypted drive accessible only to the research team. Deidentified patient records were used during data entry to ensure confidentiality. A total of 82 patients met the study requirements: 40 from Hasan Sadikin General Hospital and 42 from Limijati Hospital.
Inclusion and Exclusion Criteria
The study included all female patients with biopsy-proven breast cancer staged I–III according to the American Joint Committee on Cancer (AJCC) 8th Edition who underwent oncoplastic surgery (OPS) or breast-conserving therapy (BCT) during the study period. Patients were excluded if their medical records were incomplete or if they did not have follow-up at the participating institutions through 30 days postoperatively.
Data Collection
Demographic, perioperative, operative, and histopathologic data were retrospectively collected by review of patient files and electronic medical records. A multidisciplinary team (breast surgeon, radiologist, and medical oncologist) assessed patients for eligibility for neoadjuvant chemotherapy when tumor downstaging was indicated. The primary surgeon determined the operative approach (OPS or BCT), which was endorsed by the multidisciplinary team. OPS was considered when the breast-to-tumor size ratio or tumor location made satisfactory cosmetic outcomes unlikely with standard BCS. Patients were counselled about procedures, expected outcomes, and potential complications (visual aids such as pictorial drawings were used), and informed consent for surgery was obtained according to institutional practice.
For patients receiving neoadjuvant chemotherapy, the tumor bed was marked with a clip before therapy; post-therapy localization of the clip and any residual tumor used ultrasound or mammographic guidance. All resection specimens were oriented, margins were delineated prior to formalin fixation, and then sent for histopathologic analysis. Trained pathologists recorded specimen dimensions (length × breadth × width) to calculate specimen volume and noted the maximum tumor dimension. Six margins (anterior, posterior, medial, lateral, superior, inferior) were examined for tumor cells; margins were considered negative if no tumor cells were present on the inked surface in accordance with SSO/ASTRO guidelines. Sentinel lymph node–positive patients underwent axillary lymph node dissection and all excised nodes were examined for metastases.
Postoperative monitoring included surveillance for 30 days to detect readmissions or complications. Seromas were diagnosed clinically and confirmed by ultrasound and were all resolved with a single aspiration. Wound infections were identified and managed guided by culture and sensitivity results.
Data Analysis
Analyses were performed using IBM SPSS Statistics for Windows, Version 22. Quantitative variables are reported as means, and categorical variables as frequencies and percentages. Categorical comparisons used the Chi-square test of independence or Fisher’s exact test when expected cell counts were small. The Mann–Whitney U-test was used to compare quantitative variables that did not meet parametric assumptions. A two-sided significance level of p < 0.05 was applied to all statistical tests.
Results
A total of 82 female patients were included in the analysis, comprising 39 (47,6%) in the OPS group and 43 (52.4%) in the BCS group. The median age for the entire cohort was 50 years, with similar median ages of 49 years in the OPS group and 51 years in the BCS group, a difference that was not statistically significant (p = 0.513). Tumor bed characteristics were detailed for patients who underwent neoadjuvant chemotherapy (see Table 1). The administration of neoadjuvant chemotherapy differed significantly between the OPS and BCS groups, with 76.9% of patients in the OPS group compared to 69.8% in the BCS group (p = 0.222). Invasive ductal carcinoma was the predominant histological type, accounting for 87.3% in the OPS group and 81.4% in the BCS group. The mean tumor volume differed significantly between the two groups, with 34.72 cm3 in the OPS group compared to 22.35 cm3 in the BCS group (p < 0.001). Postoperative margin positivity was notably higher in the BCS group at 9.3% compared to 2.5% in the OPS group, although statistically insignificant (see Table 1).
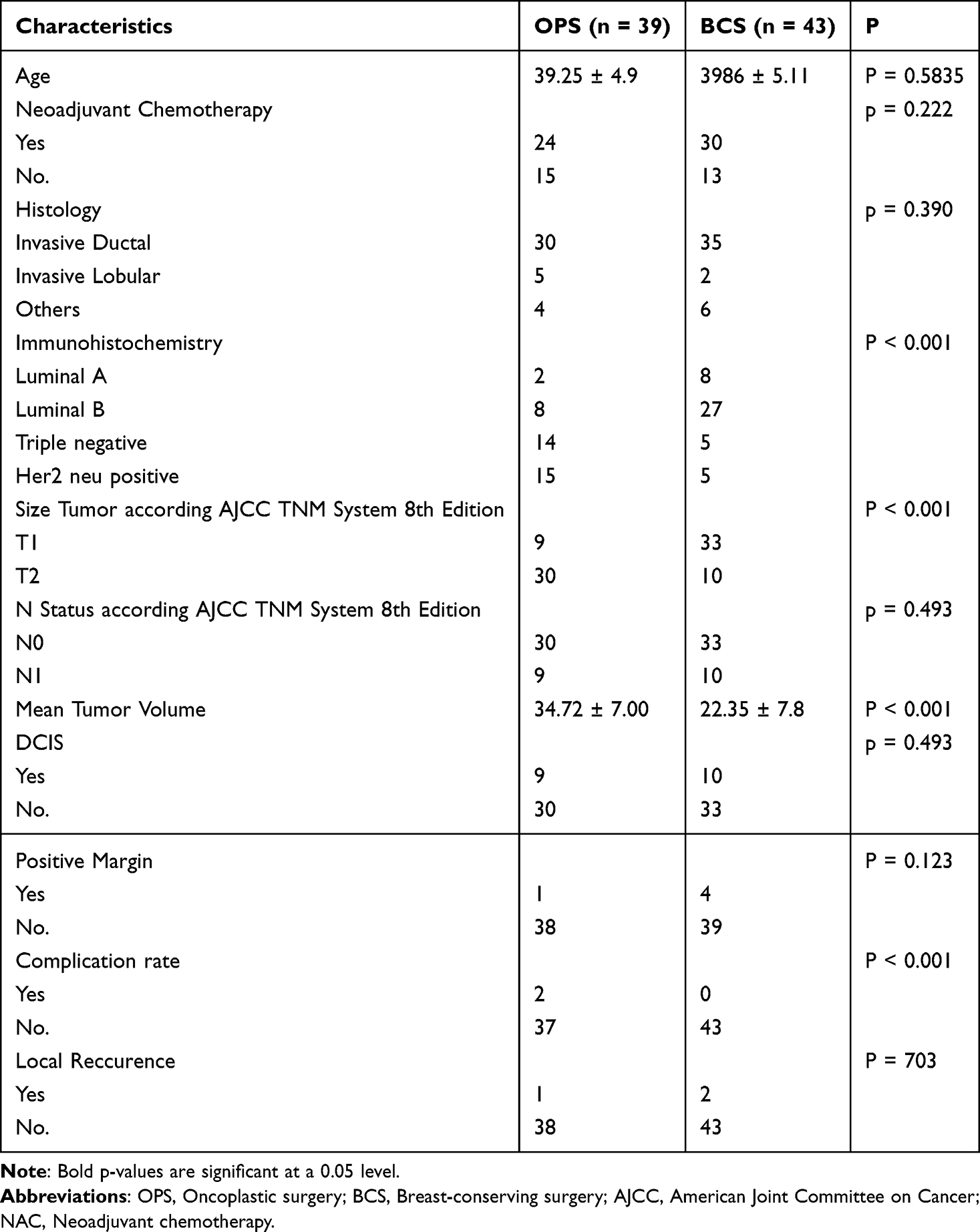 |
Table 1 Tumor Characteristics |
The most frequently performed oncoplastic procedure was inverted T technique with matrix rotation (17.9%), followed by lateral mammoplasty rotation flap (15.4%), and then the inverted T technique and rotation mammoplasty in 15.4% of cases (Table 2). Seventeen patients from the BCS group (8.33%) required margin re-excision, and four of them exhibited residual tumor cells in the resected specimens. All patients achieved negative margins upon re-excision.
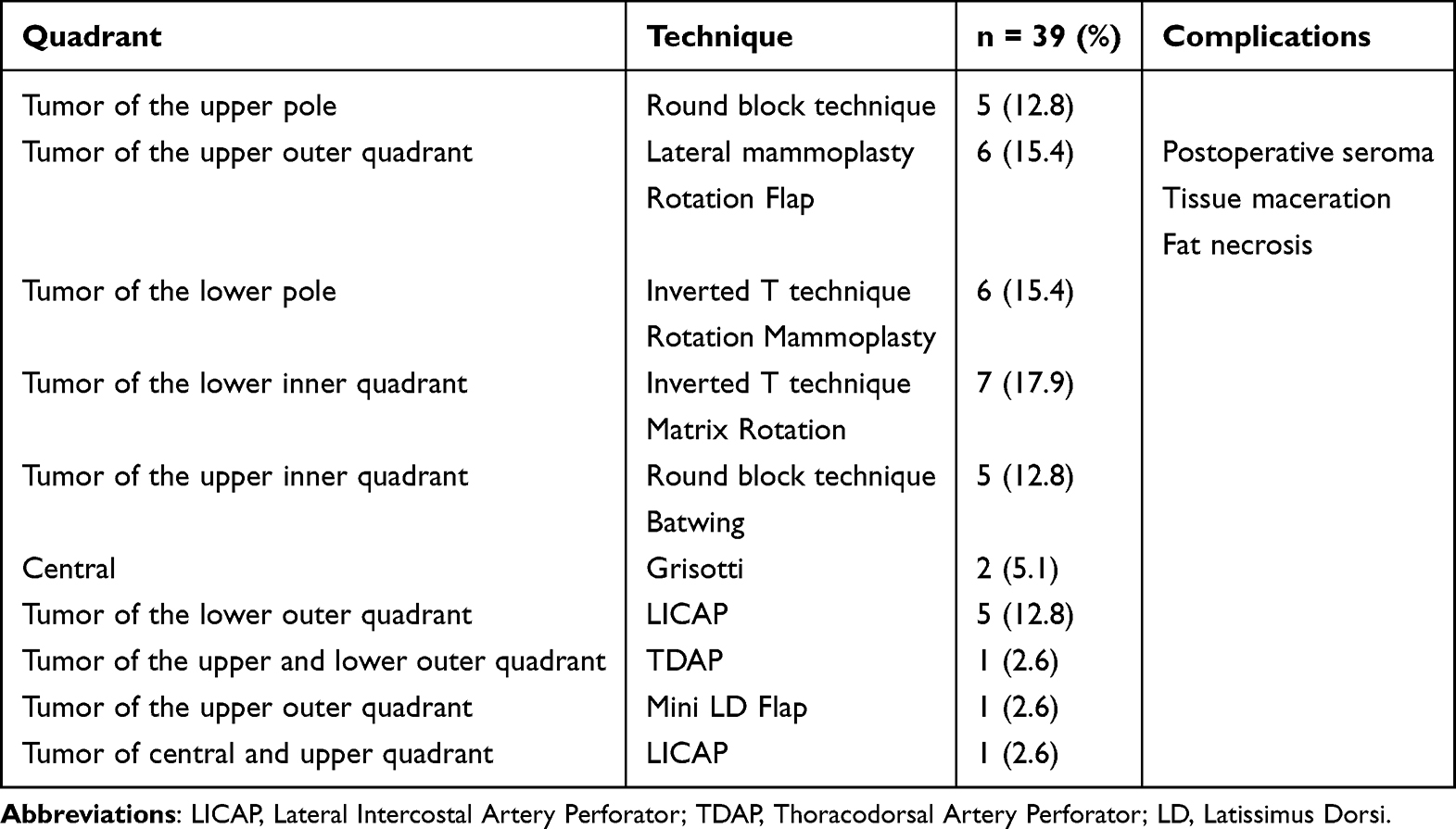 |
Table 2 Location of the Tumor and the Surgical Technique Utilized in Oncoplastic Surgery |
Among the OPS group, five patients had positive margins, with four (66.7%) undergoing reexcision and one (33.3%) not requiring further intervention. During the 30-day follow-up period, two patients experienced postoperative complications, all of whom were from the OPS group. The two complication manage by conservative treatment and none of these patients required readmission due to complications within the 30-day follow-up period.
Discussion
The American Society of Breast Surgeons (ASBrS) defines oncoplastic surgery as a type of breast conservation surgery that involves oncologic partial mastectomy alongside plastic surgery techniques to repair defect of the ipsilateral breast with volume displacement or volume replacement techniques with contralateral symmetry surgery as necessary.1 Volume displacement involves closing of the defect caused by lumpectomy and distributing the resected volume over the conserved breast. There are two levels of volume displacement techniques; level I techniques apply to cases with less than 20% excision of breast volume. These techniques aim for tumor excision with no skin resection, involving straightforward mastopexy techniques and local tissue arrangement. Level II volume displacement techniques are appropriate for resection of 20–50% of breast tissue. The level II techniques include circumvertical mastopexy and reduction mammoplasty. Cases where tissue from other body parts is used to repair defect—including implant placement and flap reconstructions—fall under the category “volume replacement”.
The rise in popularity of OPS is largely due to the unsatisfactory cosmetic results often seen after BCS. OPS can help prevent deformities and poor aesthetic outcomes associated with BCS.4,9 Two key factors that influence aesthetic results are the tumor-to-breast volume ratio and the tumor’s location.
A volume excision of 10% is generally considered an aesthetically acceptable limit for BCS. However, due to the relative lack of tissue, reducing more than 5% of the breast volume medially can lead to poor aesthetic results. Conversely, it is possible to remove up to 15% of the breast volume laterally with positive outcomes. Our research indicated that OPS allows for wide excisions with clear margins and can be used as an alternative to mastectomy for larger cancers. Additionally, OPS did not negatively impact long-term survival in patients. Due to these factors, OPS offers more advantages over BCS.
Although OPS benefits patients by reducing the re-excision rate, pooled results did not demonstrate an advantage of OPS in reducing the positive-margin rate especially after neoadjuvant chemotherapy setting. Guidelines recommend re-excision of positive margins after initial lumpectomy for breast cancer as a standard of quality care.11 Re-excision is crucial for reducing positive and close margins (< 1 mm or < 2 mm).12 Due to varying indications for re-excision, different surgical teams may perform re-excision for reasons such as an ink-positive margin, uncertain margin status, fragmented specimens, or evidence of residual disease found through postoperative imaging. Consequently, the re-excision rate may be higher than the positive-margin rate. In De la Cruz’s systematic review, the rate of positive margins in oncoplastic surgery showed significant variation (0–39.7%) due to the highly heterogeneous assessment of positive margins. Eleven studies provided specific margin data for 1455 patients. Among these, 143 patients (9.8%) had positive margins, with 113 (7.8%) showing ink on the tumor.13
The issue arises with involved margins in oncoplastic surgery and the oncological safety of margin re-excision. Margin re-excision is feasible even with glandular mobilization. To facilitate this, it is crucial to mark both the tumor bed and surgical field with clips, maintain clear communication between the pathologist and surgeon, and ensure concordance between imaging results and pathological findings. The significance of a margin in focal contact differs from that of multiple involved margins or multifocal/multicentric lesions. Ideally, the same surgeon should perform both surgeries. Realistic consideration of the possibility of margin re-excision is necessary to avoid false reassurance.
In some cases, patients with positive margins after oncoplastic breast-conserving surgery proceed to mastectomy. However, there is considerable variation in mastectomy conversion rates after initial OPBCS for involved margins, ranging from 12.5% to 100%.14–17 Despite this variability, mastectomy is not always required for managing a positive margin after O-BCS. In a retrospective study of 649 patients who underwent oncoplastic Wise pattern reduction, 95% were successfully managed with margin re-excision while preserving breast-conserving therapy, with only one case of in-breast recurrence.17 The use of magnetic resonance imaging (MRI), which enhances lesion detection sensitivity, could potentially increase the mastectomy rate. However, it has not been demonstrated that MRI use increases the risk of involved margins.
Research results showed a decreasing trend in the positive-margin rate and a significantly lower re-excision rate with OPS. However, the reduced re-excision rate in the OPS group did not correlate with lower recurrence rates or longer survival times, indicating that re-excision is not a significant prognostic factor after breast cancer surgery.
The primary challenge with oncoplastic breast surgery in Indonesia is the prevailing belief that radical procedures like mastectomy are the most effective way to prevent cancer recurrence.
Even after the widespread use of systemic therapy to induce a pathological complete response in high-risk patients with operable breast cancer, there is no significant increase in the rates of BCS or OPS. The use of implants for volume replacement after mastectomy is not popular in Indonesia, not only due to financial reasons but also because of religious considerations.
Similar to other Southeast Asian countries, contralateral mammoplasty on the healthy breast to achieve a more symmetrical appearance is not widely accepted in Indonesia. People generally prefer to avoid surgery on the unaffected side of the breast. Oncoplastic surgery techniques are categorized by skill level. While basic methods are within the capabilities of most breast surgeons, more advanced techniques necessitate extensive additional training, experience, and a considerable learning curve.
Our study reported the post-operative outcomes and complications of 82 participants who underwent either OPS or BCS. The 82 participants had mean age of 39.25 ± 4.9 and 39.86 ± 5.11 for OPS and BCS groups respectively. This finding is far younger than other studies by Dogan and Gulcelik (mean age 48 ± 8 and 49 ± 7 for OPS and BCS respectively), Oberhauser et al (60.33 ± 14.94 and 61.67 ± 15.81), and Niinikoski et al (61 ± 8.17 and 62 ± 9.67).2–4 This should raise awareness of earlier age of diagnosis of breast cancer patients in Indonesia.
In both groups, the most common histological type was invasive ductal carcinoma. This finding is in accordance with well-established findings in literatures. The explanation for this finding is that the milk ducts are the most abundant structures in breast tissue. The tumor T staging of the OPS group was more advanced than the BCS group. This is because more advanced tumors need more oncoplastic surgical approach.5
In the present study, we found no significant difference in the rate of postoperative positive margins between patients who underwent Breast Conserving Surgery (BCS) and those who underwent Oncoplastic Breast Surgery (OPS). This finding aligns with the results reported by Hasan et al, who similarly observed comparable margin status between the two surgical approaches.6 In their pooled meta-analysis of 6941 patients, the risk ratio for close/positive margins was RR = 0.58, with a 95% confidence interval of 0.29 to 1.16 and P = 0.12. The consistency of these results suggests that, when performed with appropriate surgical planning and intraoperative assessment, both BCS and OPS can achieve equivalent oncologic safety in terms of margin clearance.
However, other studies have reported contrasting outcomes. Mohammedahmed et al and Tian et al demonstrated that OPS was associated with significantly lower rates of positive surgical margins compared to conventional BCS. This discrepancy may be attributed to several factors, including variations in surgical techniques, tumor characteristics, patient selection, and the extent of tissue resection permitted by oncoplastic approaches. OPS allows for wider excision of breast tissue with immediate reshaping, potentially reducing margin positivity while maintaining cosmetic outcomes. In contrast, traditional BCS may be limited by aesthetic considerations that constrain the amount of tissue removed. Differences in pathological assessment methods and definitions of “positive margins” across studies may also contribute to these divergent findings.
Our observation of a higher rate of postoperative complications in the OPS group compared to BCS conflicts with the findings reported by Hasan et al who found no significant difference in surgical complications between OPS and BCS groups.6 Our finding suggests that the more extensive tissue mobilization and reconstruction inherent to oncoplastic techniques may increase the risk of complications such as wound healing issues, infections, and hematomas.
Our finding highlights an important trade-off in breast cancer surgery: while OPS offers oncological and aesthetic benefits—such as reduced re-excision rates and better cosmetic outcomes—it may do so at the cost of higher perioperative morbidity. Our results reinforce the need for careful patient selection when considering oncoplastic techniques, particularly in individuals with comorbidities or other risk factors for poor wound healing.
This multicentre, real-world cohort benefits from multidisciplinary case selection, standardized histopathological review, and detailed perioperative and operative data, which together strengthen the clinical relevance of the observation that OPS achieves lower margin positivity even for more complex tumours. Nonetheless, the retrospective, non-randomized design, modest sample size, heterogeneity of oncoplastic techniques and surgeon experience, short follow-up limited to 30-day outcomes, and absence of standardized cosmetic assessments or validated patient-reported outcome measures constrain causal inference and generalizability. Future research should therefore prioritise prospective, ideally randomized, multicentre studies with standardized OPS protocols and structured surgeon training, extended oncologic and aesthetic follow-up incorporating validated PROMs, and formal cost-effectiveness analyses to clarify which patients benefit most and how perioperative morbidity can be minimised.
Conclusion
The field of oncoplastic breast surgery (OPS) for treating operable breast cancer is still evolving. Despite several challenges in its development, our study provides valuable insights into its current implementation in Indonesia. We observed a higher rate of postoperative complications in the OPS group compared to the conventional breast-conserving surgery (BCS) group, which highlights the need for continued refinement of surgical techniques, perioperative care, and patient selection criteria as the procedure gains wider adoption. Interestingly, our cohort also demonstrated a younger age distribution of Indonesian breast cancer patients compared to reports from other regions, suggesting potential biological, genetic, or sociodemographic differences that may influence surgical decision-making and outcomes. Nevertheless, we remain optimistic that ongoing advancements in surgical science, training, and multidisciplinary collaboration will enable the next generation of breast surgeons to establish OPS as a safe and promising alternative—pending further high-quality evidence—for the treatment of operable breast cancer in Indonesia.
Data Sharing Statement
All data and tables used to support the findings of this study are included within the article and available upon request to the corresponding author.
Acknowledgments
We thank all the patients who agreed to participate in this study and the trainees and surgical residents who helped carry out this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding for the preparation of this study.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Fisher B, Anderson S, Redmond CK, Wolmark N, Wickerham DL, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med. 1995;333(22):1456–1461. doi:10.1056/NEJM199511303332203
2. Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347(16):1227–1232. doi:10.1056/NEJMoa020989
3. Pisansky TM, Halyard MY, Weaver AL, et al. Breast conservation therapy for invasive breast cancer: a review of prior trials and the Mayo Clinic experience. Mayo Clin Proc. 1994;69(6):515–524. doi:10.1016/S0025-6196(12)62241-1
4. Taylor ME, Perez CA, Halverson KJ, et al. Factors influencing cosmetic results after conservation therapy for breast cancer. Int J Radiat Oncol Biol Phys. 1995;31(4):753–764. doi:10.1016/0360-3016(94)00480-3
5. Cochrane RA, Valasiadou P, Wilson ARM, Al-Ghazal SK, Macmillan RD. Cosmesis and satisfaction after breast-conserving surgery correlates with the percentage of breast volume excised. Br J Surg. 2003;90(12):1505–1509. doi:10.1002/bjs.4344
6. Niinikoski L, Leidenius MHK, Vaara P, et al. Resection margins and local recurrences in breast cancer: comparison between conventional and oncoplastic breast conserving surgery. Eur J Surg Oncol. 2019;45(6):976–982. doi:10.1016/j.ejso.2019.02.010
7. Clough KB, Van La Parra RFD, Thygesen HH, et al. Long-term results after oncoplastic surgery for breast cancer: a 10-year follow-up. Ann Surg. 2018;268(1):165–171. doi:10.1097/SLA.0000000000002255
8. Kelemen P, Pukancsik D, Újhelyi M, et al. Comparison of clinicopathologic, cosmetic and quality of life outcomes in 700 oncoplastic and conventional breast-conserving surgery cases: a single-centre retrospective study. Eur J Surg Oncol. 2019;45(2):118–124. doi:10.1016/j.ejso.2018.09.006
9. Weber WP, Soysal SD, El-Tamer M, et al. First international consensus conference on standardization of oncoplastic breast conserving surgery. Breast Cancer Res Treat. 2017;165(1):139–149. doi:10.1007/s10549-017-4314-5
10. Qureshi S, Ghazanfar S, Iqbal S, Bhatti ABH, Quraishy MS. Results of level-II oncoplasty in breast cancer patients: an early experience from a tertiary care hospital in Pakistan. J Pak Med Assoc. 2014;64(3):309–315.
11. Houssami N, Macaskill P, Luke Marinovich M, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21(3):717–730. doi:10.1245/s10434-014-3480-5
12. Rose M, Svensson H, Handler J, Hoyer U, Ringberg A, Manjer J. Oncoplastic breast surgery compared to conventional breast-conserving surgery with regard to oncologic outcome. Clin Breast Cancer. 2019;19(6):423–432.e5. doi:10.1016/j.clbc.2019.05.016
13. De La Cruz L, Blankenship SA, Chatterjee A, et al. Outcomes after oncoplastic breast-conserving surgery in breast cancer patients: a systematic literature review. Ann Surg Oncol. 2016;23:3247–3258.
14. Vohra LM, Jabeen D, Ali D, Abidi SS, Zeeshan S, Sattar AK. Current perspectives of oncoplastic breast surgery in Pakistan. J Pak Med Assoc. 2022;72(Suppl 1):S81–S85. doi:10.47391/JPMA.AKU-16
15. Zeeshan S, Vohra LM, Shamsi US, et al. A single centre experience of local perforator flaps in oncoplastic breast surgery; a cross-sectional study. Ann Med Surg. 2022;84:104916. doi:10.1016/j.amsu.2022.104916
16. Vohra L, Siddiqui T, Farooqi N. Oncoplastic breast conserving surgery in developing country: challenges, promises and outcome. Eur J Surg Oncol. 2019;45(2):e93. doi:10.1016/j.ejso.2018.10.328
17. Ali D, Zeeshan S, Farooqi N, Vohra L. Breast surgery super specialization: impact on advanced surgical training and research. Pak J Med Sci. 2022;38(8):2345–2349. doi:10.12669/PJMS.38.8.6045
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Postoperative Complications Following Neoadjuvant Therapy Across Different Oncoplastic Breast Surgery Techniques: A Retrospective Comparative Study in Breast Cancer Patients
Kulturoglu MO, Dogan L, Gulcelik MA
Breast Cancer: Targets and Therapy 2026, 18:607172
Published Date: 27 May 2026