Back to Journals » Vascular Health and Risk Management » Volume 22
Postoperative Blood Glucose Trajectories are Associated with Inflammatory Markers and Functional Outcomes in Acute Ischemic Stroke Treated by Thrombectomy
Authors Liu Y, Zhong H, Huang J, Wang Y
Received 6 December 2025
Accepted for publication 24 February 2026
Published 27 February 2026 Volume 2026:22 587043
DOI https://doi.org/10.2147/VHRM.S587043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Yunpeng Liu,* Hanlin Zhong,* Jumei Huang, Yang Wang
Department of Neurosurgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunpeng Liu; Yang Wang, Email [email protected]; [email protected]
Purpose: To describe postoperative blood glucose trajectories in patients with acute ischemic stroke treated by mechanical thrombectomy (MT) and to examine their associations with 90-day functional outcomes and early postoperative inflammatory markers.
Patients and Methods: This retrospective cohort study included 150 patients who underwent MT for large vessel occlusion (LVO) stroke between March 2023 and September 2024. Daily capillary blood glucose levels (fasting and postprandial) were recorded for seven days post-procedure, and linear regression was used to calculate individual postoperative glucose slopes. Patients were classified into a Glucose-Increasing Group or Glucose-Decreasing Group based on the median slope. The primary outcome was the 90-day modified Rankin Scale (mRS). Secondary outcomes included postoperative day-1 levels of C-reactive protein (CRP), interleukin-6 (IL-6), and interleukin-10 (IL-10). Statistical analyses included group comparisons and multivariate logistic regression adjusting for potential confounders.
Results: Patients in the Glucose-Increasing Group had significantly higher median 90-day mRS scores compared with the Glucose-Decreasing Group (4.0 vs 3.0; P = 0.030). They also exhibited higher postoperative inflammatory markers: CRP (5.2 vs 4.1 mg/L; P = 0.022), IL-6 (6.9 vs 5.7 pg/mL; P = 0.015), and IL-10 (134 vs 104 pg/mL; P = 0.0017). However, in multivariate logistic regression, glucose trajectory was not an independent predictor of poor outcome (mRS ≥ 3; OR 0.67, 95% CI 0.34– 1.37; P = 0.272).
Conclusion: An increasing postoperative blood glucose trend is associated with higher early inflammatory marker levels and poorer 90-day functional outcomes in LVO stroke patients undergoing thrombectomy. Although not an independent predictor after adjustment, postoperative glycemic trajectory may reflect underlying metabolic and inflammatory stress. Prospective studies are needed to further clarify these relationships.
Keywords: acute ischemic stroke, mechanical thrombectomy, postoperative hyperglycemia, inflammatory response, functional outcome
Introduction
Acute ischemic stroke (AIS) frequently triggers stress hyperglycemia, even in patients without pre-existing diabetes. Elevated blood glucose in the acute phase of stroke is consistently associated with worse neurological outcomes and higher mortality.1 Hyperglycemia can exacerbate ischemic brain injury by disrupting the blood–brain barrier, amplifying thrombo-inflammatory cascades, and increasing oxidative stress.2 As a result, glycemic control is considered an important aspect of acute stroke care, current guidelines for acute ischemic stroke recommend routine blood glucose monitoring but do not support intensive glucose lowering, as strict glycemic control has not been shown to improve functional outcomes and may increase the risk of hypoglycemia. These recommendations underscore the complexity of glycemic management in the acute stroke setting.3 However, existing guidelines focus mainly on single glucose measurements or target ranges, and investigating postoperative blood glucose trajectories may provide additional insight into systemic stress, inflammation, and functional recovery after mechanical thrombectomy.
Mechanical thrombectomy (MT) has become the standard of care for large vessel occlusion (LVO) strokes, dramatically improving recanalization rates and outcomes.4 However, up to half of patients with successful recanalization still experience poor functional recovery, highlighting the need to identify modifiable predictors of outcome. While admission hyperglycemia has been linked to poor prognosis in several studies, its predictive value in thrombectomy patients remains debated. More recently, researchers have turned their attention to postoperative blood glucose trends, recognizing that a single admission glucose measurement may not adequately capture patient risk.5 Limited evidence suggests that postoperative glucose increases could independently predict worse functional outcomes even in patients with successful recanalization, yet comprehensive studies specifically investigating postoperative glycemic trajectories in LVO stroke patients remain scarce.
Emerging data also indicate that hyperglycemia after stroke may amplify systemic inflammatory responses, further compromising neurological recovery. Elevated blood glucose can promote cytokine release, oxidative stress, and endothelial dysfunction, creating a pro-inflammatory environment that exacerbates secondary brain injury. In turn, inflammation itself can worsen glucose dysregulation, establishing a vicious cycle between metabolic and immune stress.6–8 This underscores the need to explore postoperative glucose trajectories in the context of concurrent inflammatory markers to better understand their collective impact on functional outcomes. Therefore, this study aims to investigate the prognostic significance of postoperative blood glucose trends in patients with LVO stroke treated with MT, and to examine their associations with early postoperative inflammatory responses, thereby providing additional insight into metabolic stress during the acute recovery phase.
Methods
Study Design and Population
This was a retrospective cohort study conducted at one stroke center in Beijing, China, between March 2023 and September 2024. Consecutive patients who underwent mechanical thrombectomy for acute ischemic stroke were enrolled. Inclusion criteria were: (1) age ≥ 18 years; (2) acute ischemic stroke due to large vessel occlusion confirmed by imaging; (3) successful mechanical thrombectomy within 24 hours of symptom onset; and (4) available blood glucose and inflammatory marker data within the first week post-procedure. Patients with incomplete medical records or early in-hospital mortality were excluded. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University (approval number: 2022-Ke-522). Due to the retrospective nature of the study and the use of anonymized clinical data collected during routine clinical care, the requirement for written informed consent was waived by the Ethics Committee. All patient data were handled confidentially and analyzed anonymously.
Data Collection
Demographic and clinical data, including age, sex, vascular risk factors (hypertension, diabetes mellitus, coronary artery disease, prior stroke), baseline National Institutes of Health Stroke Scale (NIHSS) scores, admission blood glucose levels, and body mass index (BMI), were collected from electronic medical records. Postoperative laboratory tests, including daily blood glucose levels for the first seven days, C-reactive protein (CRP), interleukin-6 (IL-6), and interleukin-10 (IL-10) levels measured on postoperative day 1, were also recorded.
Blood Glucose Trend Analysis
Postoperative blood glucose levels were monitored at least once daily for the first seven days following mechanical thrombectomy, typically measured as fasting capillary blood glucose in the morning and 2-hour postprandial capillary blood glucose levels after each meal. The daily mean blood glucose level was calculated as the arithmetic mean of these measurements.
To facilitate a simple and clinically interpretable characterization of early postoperative glycemic patterns, linear regression analysis was performed for each patient, treating the postoperative day number as the independent variable and the daily mean blood glucose level as the dependent variable. The slope of this regression line represented the rate of change in postoperative blood glucose over the first week. Patients were then stratified into two groups based on the median slope value within the cohort: the Glucose-Increasing Group (slope ≥ median, indicating a stable or rising trend) and the Glucose-Decreasing Group (slope < median, indicating a declining trend). This approach enabled a standardized classification of postoperative glycemic trajectories for assessing their associations with inflammatory markers and functional outcomes, while being intended to capture the overall direction of glucose change rather than to model complex or non-linear glycemic fluctuations during the acute phase.
Outcomes
The primary outcome was the 90-day functional outcome, assessed using the modified Rankin Scale (mRS) via outpatient clinic visits or structured telephone interviews. Poor functional outcome was defined as mRS ≥ 3. Secondary outcomes included postoperative inflammatory marker levels (CRP, IL-6, and IL-10) measured from the first fasting venous blood sample collected on the morning after surgery.
Statistical Analysis
All statistical analyses were performed using GraphPad Prism version 10.0 (GraphPad Software, San Diego, CA, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range [IQR]) as appropriate, and compared using the independent samples t-test or Mann–Whitney U-test. Categorical variables were expressed as counts and percentages, and compared using the chi-square test or Fisher’s exact test. Multivariate logistic regression was performed to identify independent predictors of poor functional outcome (mRS ≥ 3), adjusting for potential confounders (age, baseline NIHSS score, diabetes, hypertension, coronary artery disease, and prior stroke). A two-sided P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Patients
A total of 150 patients who underwent mechanical thrombectomy for acute ischemic stroke were included in this study. Patients were stratified into two groups based on the median slope of their 7-day postoperative blood glucose levels: the Glucose-Increasing Group (n=75) and the Glucose-Decreasing Group (n=75).
The baseline characteristics of the two groups are summarized in Table 1. There were no statistically significant differences in age, gender distribution, baseline NIHSS scores, admission blood glucose levels, body mass index (BMI), or the prevalence of hypertension, diabetes, coronary artery disease (CAS), and prior stroke history between the two groups (all P > 0.05).
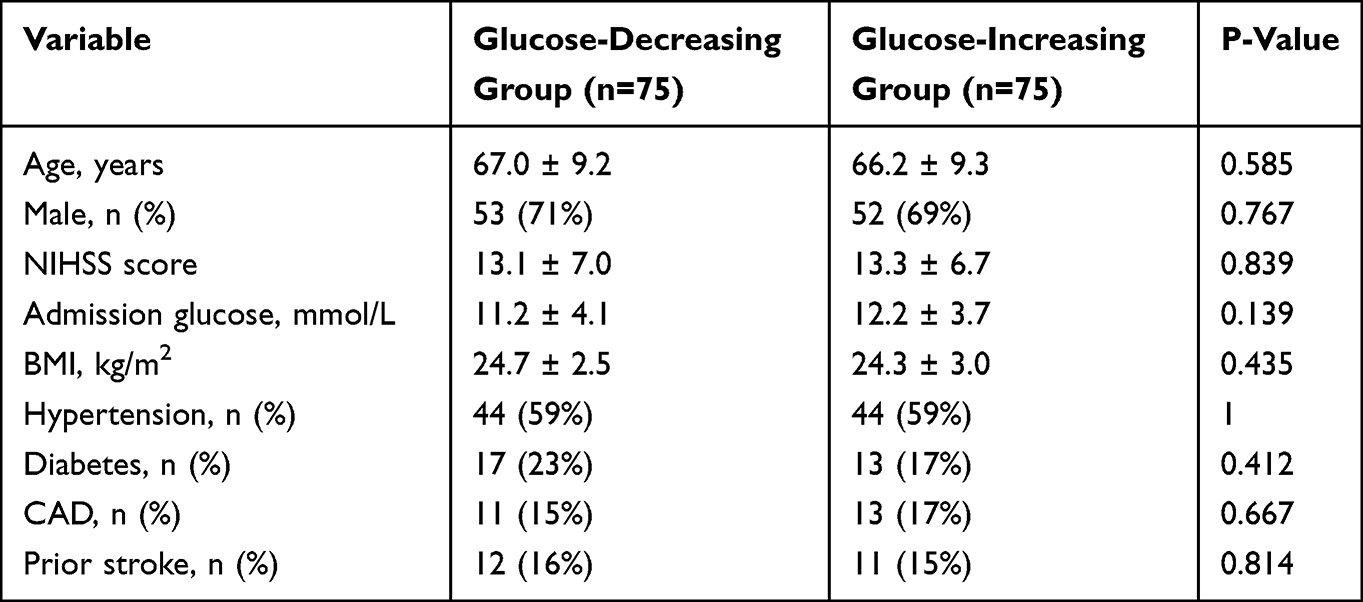 |
Table 1 Baseline Characteristics of the Study Patients According to the Blood Glucose Trend Group (Glucose-Decreasing Group vs Glucose-Increasing Group) |
Comparison of 90-Day Functional Outcomes According to Blood Glucose Trend
The primary outcome of this study was the 90-day functional status, assessed using the mRS. The Glucose-Increasing Group had a higher median 90-day mRS score of 4.0 (IQR, 2.0–5.0) compared to 3.0 (IQR, 2.0–4.0) in the Glucose-Decreasing Group. This difference was statistically significant (P = 0.030), indicating that a increasing postoperative blood glucose trend was associated with poorer functional outcomes at 90 days (Figure 1).
 |
Figure 1 Comparison of 90-day modified Rankin Scale (mRS) scores between the Glucose-Decreasing Group and the Glucose-Increasing Group. Boxes represent the interquartile range (IQR), the horizontal line inside each box indicates the median value, and whiskers denote the minimum and maximum values. |
Moreover, when analyzing the distribution of mRS categories (0–2 vs 3–6), the proportion of patients with good functional outcomes (mRS ≤ 2) was higher in the Glucose-Decreasing Group (40%) compared to the Glucose-Increasing Group (32%). However, this difference was not statistically significant (P = 0.395).
Multivariate Analysis of Blood Glucose Trend Group and Functional Outcomes
To further assess whether the blood glucose trend group independently predicted poor functional outcomes (defined as mRS ≥ 3 at 90 days), we performed a multivariate logistic regression analysis adjusting for potential confounders, including age, baseline NIHSS score, diabetes, hypertension, coronary artery disease (CAD), and prior stroke.
As shown in Table 2 and illustrated in the forest plot (Figure 2), the blood glucose trend group (Glucose-Increasing vs Glucose-Decreasing) was not an independent predictor of poor outcome (odds ratio [OR], 0.67; 95% CI, 0.34–1.37; P = 0.272). Other baseline factors, including age (OR, 0.99; P = 0.709), baseline NIHSS (OR, 0.98; P = 0.368), diabetes (OR, 1.00; P = 0.998), hypertension (OR, 1.21; P = 0.595), CAD (OR, 1.03; P = 0.951), and prior stroke (OR, 0.75; P = 0.529), were also not significantly associated with poor functional outcomes in this cohort.
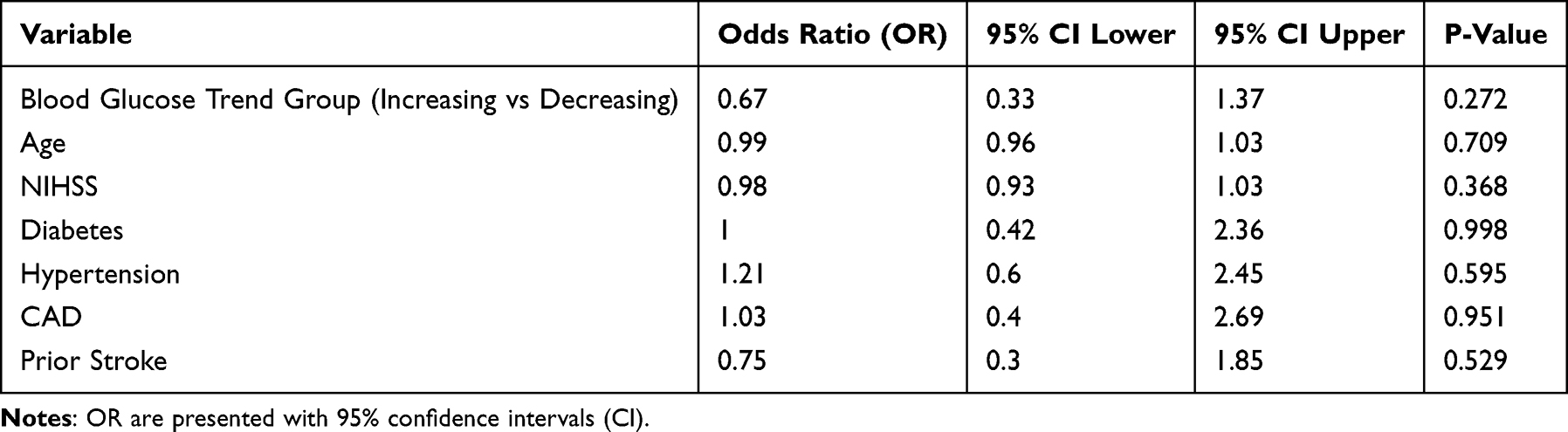 |
Table 2 Results of Multivariate Logistic Regression Analysis for Predicting Poor Functional Outcome (mRS ≥ 3) |
 |
Figure 2 Forest plot of OR and 95% CI predictors of poor outcome (mRS ≥ 3) at 90 days. Squares represent point estimates of ORs, horizontal lines indicate 95% CIs, and the vertical dashed red line represents an OR of 1.0 (no effect). |
Comparison of Postoperative Day 1 C-Reactive Protein (CRP) Levels Between Blood Glucose Trend Groups
To evaluate the inflammatory response in the early postoperative period, CRP levels were measured on postoperative day 1 and compared between the two blood glucose trend groups.
The Glucose-Increasing Group demonstrated a slightly higher median CRP level of 5.2 mg/L (IQR, 3.2–7.0 mg/L), compared to a median of 4.1 mg/L (IQR, 2.8–5.3 mg/L) in the Glucose-Decreasing Group. This difference was statistically significant (P = 0.022), suggesting a modestly greater early postoperative inflammatory response in patients whose blood glucose tended to increase over the first week. Figure 3 illustrates the distribution of CRP levels in the two groups.
 |
Figure 3 Comparison of postoperative day 1 C-reactive protein (CRP) levels between the Glucose-Decreasing Group and the Glucose-Increasing Group. Boxes represent the interquartile range (IQR), the central horizontal line indicates the median value, and whiskers denote the minimum and maximum values. |
Comparison of Postoperative Day 1 IL-6 and IL-10 Levels Between Blood Glucose Trend Groups
To further characterize the postoperative inflammatory and anti-inflammatory responses, we measured interleukin-6 (IL-6) and interleukin-10 (IL-10) levels on postoperative day 1. The Glucose-Increasing Group demonstrated a moderately higher median IL-6 level of 6.9 pg/mL (IQR, 5.3–8.2 pg/mL), compared to 5.7 pg/mL (IQR, 4.6–7.4 pg/mL) in the Glucose-Decreasing Group. This difference was statistically significant (P = 0.015), indicating a modestly enhanced early postoperative inflammatory response in patients whose blood glucose tended to increase over the first week (Figure 4a).
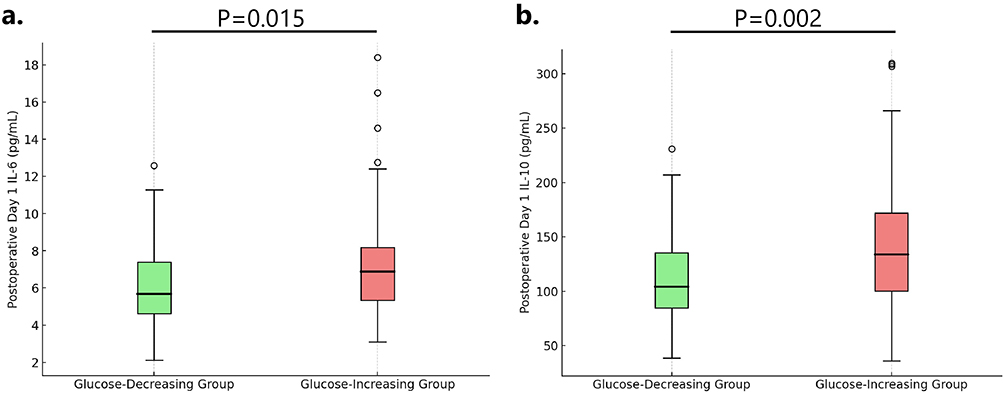 |
Figure 4 (a) Comparison of postoperative day 1 IL-6 levels between the Glucose-Decreasing Group and the Glucose-Increasing Group. (b) Comparison of postoperative day 1 IL-10 levels between the Glucose-Decreasing Group and the Glucose-Increasing Group. Boxes represent the interquartile range (IQR), the horizontal line within each box indicates the median, and whiskers denote the minimum and maximum values. |
Similarly, the Glucose-Increasing Group exhibited a higher median IL-10 concentration of 134 pg/mL (IQR, 96–177 pg/mL), compared to 104 pg/mL (IQR, 84–135 pg/mL) in the Glucose-Decreasing Group. This difference was also statistically significant (P = 0.0017), indicating a moderately enhanced early postoperative anti-inflammatory response in patients with a postoperative increase in blood glucose (Figure 4b).
Discussion
Maintaining optimal glycemic levels in the acute period after ischemic stroke has important clinical implications, particularly in patients with large vessel occlusion (LVO). Hyperglycemia is a common stress response in acute stroke and has long been associated with worse neurological outcomes.9 In the context of mechanical thrombectomy for LVO, our findings reinforce that elevated postoperative blood glucose correlates with poorer functional recovery. This aligns with prior study showing that even when successful recanalization is achieved, patients who exhibit high glucose levels in the hours to days following thrombectomy have higher rates of “futile recanalization” – meaning they fail to attain good functional outcomes despite restored blood flow.10 The clinical relevance is underscored by evidence that post-thrombectomy hyperglycemia is linked to increased 3-month mortality and disability.11 Taken together, these observations highlight that glycemic trends after stroke are more than a benign epiphenomenon; rather, they likely reflect the severity of the injury and may actively contribute to secondary brain damage.
Current stroke guidelines acknowledge the detrimental association of hyperglycemia with outcome and recommend avoiding extreme hyperglycemia, although the optimal target range remains debated. Notably, while aggressive glucose control might intuitively seem beneficial, randomized trials in acute ischemic stroke have not shown improved outcomes with intensive insulin therapy compared to standard management. The SHINE trial, for example, demonstrated that tightly controlling blood glucose (80–130 mg/dL via IV insulin) conferred no functional benefit over a more moderate insulin regimen targeting <180 mg/dL, while carrying added risk of hypoglycemia.12 These findings suggest that uncontrolled hyperglycemia is harmful, but simply lowering glucose without addressing the underlying ischemic injury or stress response may not reverse the damage. Our study reinforces the importance of avoiding sustained postoperative hyperglycemia in LVO stroke patients, yet it also prompts careful consideration of how and when to intervene. Achieving a euglycemic state through safe methods is still an essential supportive goal, but overly aggressive correction can be counterproductive. Clinicians should aim for prudent glycemic control (eg keeping glucose ~140–180 mg/dL) in the post-thrombectomy period while monitoring closely for hypoglycemia.13 The robust association between post-stroke hyperglycemia and poor outcomes in our cohort emphasizes that these patients are a high-risk population where vigilant metabolic management and supportive care are warranted.
The observation that many patients developed significant hyperglycemia after mechanical thrombectomy is biologically plausible given the profound stress of a large stroke. Acute ischemic stroke triggers a cascade of neuroendocrine stress responses. Critical illness and tissue injury activate the hypothalamic–pituitary–adrenal axis and sympathetic nervous system, leading to surges in counterregulatory hormones (catecholamines, cortisol) that antagonize insulin and drive up blood glucose levels.13 In parallel, severe stroke induces a systemic inflammatory reaction that further disrupts glucose homeostasis. Pro-inflammatory cytokines such as IL-6 and tumor necrosis factor (TNF-α) are released during the acute phase and can impair insulin signaling, exacerbating insulin resistance.9,13 The net result is “stress hyperglycemia,” a state of transient hyperglycemia that occurs despite previously normal glycemic control. This mechanism explains why even non-diabetic patients with a large stroke can experience marked blood glucose elevations.
In our study, the postoperative glucose rise likely reflects this neuroendocrine and inflammatory surge following reperfusion therapy. Reperfusion of ischemic brain tissue, while necessary for salvage, can itself augment metabolic stress through reperfusion injury and oxidative stress, potentially contributing to hyperglycemia. Moreover, mechanical thrombectomy often involves general anesthesia or sedatives and periprocedural dextrose-containing fluids, which might also influence perioperative glucose levels. It should be noted that stress hyperglycemia is usually defined as a transient phenomenon resolving as the acute illness abates.2 By contrast, chronic hyperglycemia due to diabetes is a long-standing condition that can worsen stroke outcomes through pre-existing vascular damage. Distinguishing stress-induced hyperglycemia from uncontrolled diabetes is challenging in retrospective data, but both are relevant. Importantly, the pathophysiological impact of acute hyperglycemia on the injured brain is thought to be detrimental: excess glucose in acute stroke can augment lactic acidosis in ischemic tissue, increase neuronal calcium influx, promote free radical formation, and compromise the blood–brain barrier, thereby enlarging infarct size and increasing risk of hemorrhagic transformation.14 These mechanisms offer a plausible explanation for the worse outcomes observed in patients with higher postoperative glucose levels.
Our findings also revealed a relationship between elevated postoperative blood glucose and heightened inflammation, as evidenced by higher CRP and cytokine levels (IL-6 and IL-10) in these patients. This intersection of hyperglycemia and inflammation is well-recognized in critical illness and stroke. IL-6, a prototypical pro-inflammatory cytokine, rises early after ischemic stroke and correlates with stroke severity and poor prognosis.15,16 CRP, an acute-phase reactant largely driven by IL-6, typically peaks within 2–6 days after stroke and is also a marker of systemic inflammatory burden.17 In our cohort, patients with pronounced hyperglycemia tended to have higher IL-6 and CRP levels, suggesting a more intense systemic inflammatory response accompanying the stress hyperglycemia. This is consistent with the concept that severe strokes (which often produce greater inflammatory responses) are also the ones most likely to precipitate significant stress hyperglycemia. Inflammatory cytokines like IL-6 can create a vicious cycle by worsening insulin resistance and contributing to further glucose elevation.18 Conversely, hyperglycemia itself may amplify inflammation; acute spikes in glucose have been shown to increase circulating cytokine concentrations via oxidative stress mechanisms.19 Thus, hyperglycemia and inflammation can be mutually reinforcing, each exacerbating the other’s deleterious effects on the injured brain.
It is noteworthy that IL-10 was also elevated in patients with high glucose. IL-10 is an anti-inflammatory cytokine, often rising as a compensatory response to counteract excessive inflammation. Elevated IL-10 levels in the hyperglycemic group might reflect the body’s attempt to modulate the heightened inflammatory state. The exact role of IL-10 in stroke is complex; while it generally conveys neuroprotective and anti-inflammatory effects, higher IL-10 has been paradoxically associated with worse outcomes in some analyses, possibly because it signifies a reaction to severe initial injury.20 In our study, the parallel rise of IL-10 with IL-6 and CRP in hyperglycemic patients likely indicates a more substantial immune activation overall in those individuals. These findings support a pathophysiological link between metabolic stress and inflammation after stroke: patients with greater stress (larger infarcts, more tissue injury) develop both higher glucose and a stronger inflammatory response. This milieu – hyperglycemia coupled with inflammation – can potentiate secondary brain damage by promoting endothelial dysfunction, edema, and hemorrhagic complications.21 Some studies have shown that combining blood glucose with leukocyte measures provides stronger prognostic value than using either parameter alone, further suggesting a close association between glycemic status and inflammation.22 Our results therefore underscore the importance of considering inflammatory markers alongside glucose levels when assessing post-stroke patients. Future studies might explore whether anti-inflammatory strategies or insulin therapy modulate these intertwined pathways to improve outcomes.
In addition to metabolic and inflammatory factors, cardiac biomarkers such as N-terminal pro–B-type natriuretic peptide (NT-proBNP) and cardiac troponins have been consistently reported as important predictors of poor functional outcome and mortality after acute ischemic stroke.23,24 Elevated levels of these biomarkers are thought to reflect underlying cardiac dysfunction, neurocardiac injury, or a systemic stress response, all of which may contribute to unfavorable neurological recovery.25 Many patients with ischemic stroke have underlying cardiac pathologies, such as atrial fibrillation or heart failure, which predispose them to cerebral ischemia, and higher levels of cardiac injury biomarkers may further indicate a state of neurohormonal activation that promotes inflammatory cascades, endothelial dysfunction, and adverse outcomes.26 In the acute stroke setting, cardiac injury and stress hyperglycemia may coexist and interact, as both can be driven by sympathetic nervous system activation, dysregulation of the hypothalamic–pituitary–adrenal axis, and systemic inflammatory responses; therefore, cardiac biomarkers may represent additional confounding or mediating factors in the relationship between postoperative glycemic patterns and functional outcomes.27 In the present retrospective cohort, NT-proBNP and troponin levels were not routinely measured in all patients and therefore could not be included in the analysis, which represents an important limitation of this study. Future prospective studies integrating comprehensive cardiac biomarker profiling with dynamic glucose monitoring and inflammatory marker assessment may provide a more complete understanding of how metabolic–cardiac–inflammatory interactions influence recovery after mechanical thrombectomy.
Our results are in line with a growing body of literature highlighting post-stroke hyperglycemia as a predictor of poor outcome, especially in LVO stroke treated with thrombectomy. Numerous prior studies have documented that an elevated admission glucose impairs recovery after endovascular therapy. For instance, Kim et al reported that patients presenting with blood glucose >140 mg/dL had significantly lower chances of functional independence at 3 months.28 More recent analyses have shifted focus from a single glucose value to the trajectory and dynamics of glucose post-stroke. Merlino et al introduced the concept of “persistent hyperglycemia,” finding that patients who remained hyperglycemic from admission through 24 hours had higher mortality and hemorrhagic transformation rates despite successful thrombectomy.5 Similarly, a systematic review and meta-analysis by Perez-Vega et al confirmed that higher peri-procedural glucose levels are associated with worse functional outcomes after mechanical thrombectomy across multiple studies.29 Our study’s finding of a strong association between postoperative glucose rise and poor 90-day outcomes echoes these reports, and further supports that stress hyperglycemia indices—such as the glucose-to-A1c ratio (GAR) or stress hyperglycemia ratio (SHR)—which adjust for chronic glycemic status, have been shown to be robust predictors of stroke outcomes.30,31 For example, SHR levels have been independently associated with an increased risk of recurrent stroke, composite vascular events, poor functional outcomes, and early neurological deterioration.32 These results reinforce and expand upon existing observations in a retrospective clinical cohort, underscoring the significant prognostic value of postoperative glycemic trends.
This study has several limitations that warrant consideration and also highlight opportunities for future research. First, as a single-center, retrospective analysis, causal inference is limited and residual confounding cannot be excluded. Postoperative blood glucose trajectories were summarized using a slope-based classification derived from intermittent capillary measurements over a limited time window, which may not fully capture non-linear glucose dynamics or short-term variability. Although admission and baseline glucose levels are established prognostic factors in acute ischemic stroke, the present study focused on postoperative glucose trajectories, and the joint consideration of multiple glucose-related measures warrants further investigation. In addition, Inflammatory markers were assessed at a standardized early postoperative timepoint to reflect acute inflammatory stress rather than longitudinal immune dynamics, and potential confounders such as infection, infarct volume, or procedural complications were not comprehensively evaluated. Accordingly, the observed associations should be interpreted as exploratory and non-causal. Finally, functional outcomes were analyzed using dichotomized mRS scores; while this approach is commonly adopted in retrospective studies with modest sample sizes, ordinal shift analysis would be preferable in larger cohorts and should be considered in future investigations. Future prospective, multicenter studies with larger sample sizes, more frequent glucose monitoring, and serial inflammatory assessments are needed to validate these findings and to further elucidate the interplay between stress hyperglycemia, inflammation, and functional recovery after thrombectomy.
Conclusion
In conclusion, our findings suggest that an increasing trend in postoperative blood glucose during the first week after mechanical thrombectomy for large vessel occlusion stroke is associated with higher inflammatory marker levels and poorer 90-day functional outcomes. These results underscore the clinical importance of monitoring postoperative glucose trajectories and highlight the complex interplay between stress hyperglycemia, inflammation, and stroke recovery. While causality cannot be definitively established in this retrospective analysis, our study reinforces the need for vigilant glycemic management and suggests that future prospective investigations incorporating continuous glucose monitoring and targeted metabolic interventions may help improve outcomes in this high-risk population.
Acknowledgments
We would like to thank Zeping Jin, Yixin Lin, and other colleagues from the Department of Neurosurgery, Beijing Chao-Yang Hospital, for their support and contributions to this study. This paper has been uploaded to Research Square as a preprint: https://doi.org/10.21203/rs.3.rs-6875883/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Multidisciplinary Clinical Research Innovation Team Program of Beijing Chao-Yang Hospital (Project Number: CYDXK202204), Capital Medical University.
Disclosure
No potential conflicts of interest were reported by the authors.
References
1. Ferrari F, Moretti A, Villa RF. Hyperglycemia in acute ischemic stroke: physiopathological and therapeutic complexity. Neural Regenerat Res. 2022;17(2):292–11. doi:10.4103/1673-5374.317959
2. Yao M, Hao Y, Wang T, et al. A review of stress-induced hyperglycaemia in the context of acute ischaemic stroke: definition, underlying mechanisms, and the status of insulin therapy. Front Neurol. 2023;14:1149671. doi:10.3389/fneur.2023.1149671
3. Prabhakaran S, Gonzalez NR, Zachrison KS, et al. Guideline for the Early Management of Patients With Acute Ischemic Stroke: a Guideline From the American Heart Association/American Stroke Association. Stroke. 2026;57:e01.
4. Jadhav AP, Desai SM, Jovin TG. Indications for Mechanical Thrombectomy for Acute Ischemic Stroke: current Guidelines and Beyond. Neurology. 2021;97(20 Suppl 2):S126–S136. doi:10.1212/WNL.0000000000012801
5. Merlino G, Smeralda C, Sponza M, et al. Dynamic hyperglycemic patterns predict adverse outcomes in patients with acute ischemic stroke undergoing mechanical thrombectomy. J Clin Med. 2020;9(6):1932. doi:10.3390/jcm9061932
6. Rom S, Zuluaga-Ramirez V, Gajghate S, et al. Hyperglycemia-driven neuroinflammation compromises BBB leading to memory loss in both diabetes mellitus (DM) type 1 and type 2 mouse models. Mol Neurobiol. 2019;56(3):1883–1896. doi:10.1007/s12035-018-1195-5
7. Desilles J-P, Syvannarath V, Ollivier V, et al. Exacerbation of thromboinflammation by hyperglycemia precipitates cerebral infarct growth and hemorrhagic transformation. Stroke. 2017;48(7):1932–1940. doi:10.1161/STROKEAHA.117.017080
8. Won SJ, Tang XN, Suh SW, Yenari MA, Swanson RA. Hyperglycemia promotes tissue plasminogen activator‐induced hemorrhage by increasing superoxide production. Ann Neurol. 2011;70(4):583–590. doi:10.1002/ana.22538
9. Merlino G, Pez S, Gigli GL, et al. Stress hyperglycemia in patients with acute ischemic stroke due to large vessel occlusion undergoing mechanical thrombectomy. Front Neurol. 2021;12:725002. doi:10.3389/fneur.2021.725002
10. Tang T, Li D, Fan T-P, et al. Postoperative blood glucose increase is associated with futile recanalization in patients with successful thrombectomy: a retrospective study. BMC Neurol. 2023;23(1):447. doi:10.1186/s12883-023-03512-z
11. Zhang W, Liu Y, Zhou H, et al. Postoperative blood glucose increase can predict all-cause mortality within 3 months after successful interventional recanalization in patients with acute large vessel occlusion cerebral infarction. Diabetol Metab Syndr. 2025;17(1):42. doi:10.1186/s13098-025-01597-9
12. Johnston KC, Bruno A, Pauls Q, et al. Intensive vs standard treatment of hyperglycemia and functional outcome in patients with acute ischemic stroke: the SHINE randomized clinical trial. JAMA. 2019;322(4):326–335. doi:10.1001/jama.2019.9346
13. Zhang Y, Yin X, Liu T, Ji W, Wang G. Association between the stress hyperglycemia ratio and mortality in patients with acute ischemic stroke. Sci Rep. 2024;14(1):20962. doi:10.1038/s41598-024-71778-5
14. Alquisiras-Burgos I, Aguilera P. Involvement of glucose transporter overexpression in the protection or damage after ischemic stroke. Neural Regenerat Res. 2022;17(4):783–784. doi:10.4103/1673-5374.322456
15. Worthmann H, Tryc AB, Dirks M, et al. Lipopolysaccharide binding protein, interleukin-10, interleukin-6 and C-reactive protein blood levels in acute ischemic stroke patients with post-stroke infection. J Neuroinflammation. 2015;12(1):1–9. doi:10.1186/s12974-014-0231-2
16. Pawluk H, Woźniak A, Grześk G, et al. The role of selected pro-inflammatory cytokines in pathogenesis of ischemic stroke. Clin Interventions Aging. 2020;Volume 15:469–484. doi:10.2147/CIA.S233909
17. Winbeck K, Poppert H, Etgen T, Conrad B, Sander D. Prognostic relevance of early serial C-reactive protein measurements after first ischemic stroke. Stroke. 2002;33(10):2459–2464. doi:10.1161/01.STR.0000029828.51413.82
18. Al-Mansoori L, Al-Jaber H, Prince MS, Elrayess MA. Role of inflammatory cytokines, growth factors and adipokines in adipogenesis and insulin resistance. Inflammation. 2022;45(1):31–44. doi:10.1007/s10753-021-01559-z
19. Esposito K, Nappo F, Marfella R, et al. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation. 2002;106(16):2067–2072. doi:10.1161/01.CIR.0000034509.14906.AE
20. Sun W, Wang S, Nan S. The prognostic determinant of Interleukin‐10 in patients with acute ischemic stroke: an analysis from the perspective of disease management. Dis. Markers. 2021;2021(1):6423244. doi:10.1155/2021/6423244
21. Venkat P, Chopp M, Chen J. Blood–brain barrier disruption, vascular impairment, and ischemia/reperfusion damage in diabetic stroke. J Am Heart Assoc. 2017;6(6):e005819. doi:10.1161/JAHA.117.005819
22. Xia C, Wang X, Lindley RI, et al. Combined utility of blood glucose and white blood cell in predicting outcome after acute ischemic stroke: the ENCHANTED trial. Clin Neurol Neurosurg. 2020;198:106254. doi:10.1016/j.clineuro.2020.106254
23. Ran J, Liu Y, Ma H, Zhang Y. Accuracy of NT-proBNP for predicting mortality amongst patients with ischemic stroke: a systematic review and meta-analysis. BMC Med. 2025;23(1):476. doi:10.1186/s12916-025-04299-1
24. Zhang Y, Ouyang M, Qiu J, Cao X, Xu B, Sui Y. Prognostic Value of Serum Cardiac Troponin in Acute Ischemic Stroke: an Updated Systematic Review and Meta-Analysis. J Stroke Cerebrovasc Dis. 2022;31(6):106444. doi:10.1016/j.jstrokecerebrovasdis.2022.106444
25. Xu C, Zheng A, He T, Cao Z. Brain-Heart Axis and Biomarkers of Cardiac Damage and Dysfunction after Stroke: a Systematic Review and Meta-Analysis. Int J Mol Sci. 2020;21(7):1.
26. Chen Z, Venkat P, Seyfried D, Chopp M, Yan T, Chen J. Brain-Heart Interaction: cardiac Complications After Stroke. Circ Res. 2017;121(4):451–468. doi:10.1161/CIRCRESAHA.117.311170
27. Volpe M, Carnovali M, Mastromarino V. The natriuretic peptides system in the pathophysiology of heart failure: from molecular basis to treatment. Clin Sci. 2016;130(2):57–77. doi:10.1042/CS20150469
28. Kim J-T, Jahan R, Saver JL, Investigators S. Impact of glucose on outcomes in patients treated with mechanical thrombectomy: a post hoc analysis of the solitaire flow restoration with the intention for thrombectomy study. Stroke. 2016;47(1):120–127. doi:10.1161/STROKEAHA.115.010753
29. Perez-Vega C, Domingo RA, Tripathi S, et al. Influence of glucose levels on clinical outcome after mechanical thrombectomy for large-vessel occlusion: a systematic review and meta-analysis. J Neurointervent Surg. 2022;14(1):
30. Chen X, Liu Z, Miao J, et al. High stress hyperglycemia ratio predicts poor outcome after mechanical thrombectomy for ischemic stroke. J Stroke Cerebrovascular Dis. 2019;28(6):1668–1673. doi:10.1016/j.jstrokecerebrovasdis.2019.02.022
31. Zhu B, Pan Y, Jing J, et al. Stress hyperglycemia and outcome of non-diabetic patients after acute ischemic stroke. Front Neurol. 2019;10:1003. doi:10.3389/fneur.2019.01003
32. Li W, Yan H, Gao Y, et al. Stress Hyperglycemia Ratio and Adverse Outcomes in Acute Mild Ischemic Stroke or High-Risk Transient Ischemic Attack: a Secondary Analysis of the INSPIRES Trial. Stroke. 2025;57(2):349–361. doi:10.1161/STROKEAHA.125.052987
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictors of Early Neurological Deterioration and Functional Outcome in Acute Ischemic Stroke: The Importance of Large Artery Disease, Hyperglycemia and Inflammatory Blood Biomarkers
Sabir Rashid A, Huang-Link Y, Johnsson M, Wetterhäll S, Gauffin H
Neuropsychiatric Disease and Treatment 2022, 18:1993-2002
Published Date: 6 September 2022
Eosinophil: A New Circulating Biomarker for Risk of Poor Outcome in Stroke Patients Undergoing Mechanical Thrombectomy
Yu S, Huang ZC, Wang HS, Liu SW, You SJ, Hou J, Guo ZL, Xiao GD
Clinical Interventions in Aging 2023, 18:523-531
Published Date: 28 March 2023
Comparison of the Clinical Outcomes Between Reperfusion and Non-Reperfusion Therapy in Elderly Patients with Acute Ischemic Stroke
Luo X, Chen S, Luo W, Li Q, Zhu Y, Li J
Clinical Interventions in Aging 2024, 19:1247-1258
Published Date: 10 July 2024
The Prognosis of Neutrophil-to-Lymphocyte Ratio and Lymphocyte-to-Monocyte Ratio in Elderly with Acute Ischemic Stroke
Wang J, Zhao Y, Lv C, Li F
Clinical Interventions in Aging 2024, 19:1715-1720
Published Date: 19 October 2024
Successful Mechanical Thrombectomy for Bilateral Anterior Cerebral Artery Occlusions in a Rare Anatomical Variant: A Case Report
Ge B, Zhu J, Zhang F, Han X, Xia Y, Ji Z, Sun P, Li Y, Zhang H, Guo J
International Medical Case Reports Journal 2025, 18:125-129
Published Date: 20 January 2025