Back to Journals » International Medical Case Reports Journal » Volume 18
Successful Mechanical Thrombectomy for Bilateral Anterior Cerebral Artery Occlusions in a Rare Anatomical Variant: A Case Report
Authors Ge B ![]() , Zhu J, Zhang F, Han X, Xia Y, Ji Z, Sun P, Li Y, Zhang H, Guo J
, Zhu J, Zhang F, Han X, Xia Y, Ji Z, Sun P, Li Y, Zhang H, Guo J
Received 1 November 2024
Accepted for publication 16 January 2025
Published 20 January 2025 Volume 2025:18 Pages 125—129
DOI https://doi.org/10.2147/IMCRJ.S504211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Beihai Ge,1 Jianjian Zhu,1 Fu Zhang,1 Xianyan Han,1 Yaqian Xia,1 Zeqiang Ji,1 Peili Sun,1 Yuqing Li,1 Huiying Zhang,1 Jianghong Guo2
1Department of Neurology, Rugao Affiliated Hospital of Nantong University, Rugao People’s Hospital, Nantong, Jiangsu, People’s Republic of China; 2Department of Cardiology, Rugao Affiliated Hospital of Nantong University, Rugao People’s Hospital, Nantong, Jiangsu, People’s Republic of China
Correspondence: Jianghong Guo, Department of Cardiology, Rugao Affiliated Hospital of Nantong University, Rugao People’s Hospital, Nantong, Jiangsu, People’s Republic of China, Tel/Fax +86 51387312703, Email [email protected] Beihai Ge, Department of Neurology, Rugao Affiliated Hospital of Nantong University, Rugao People’s Hospital, Nantong, Jiangsu, People’s Republic of China, Tel/Fax +86 51387312703, Email [email protected]
Background: Acute ischemic stroke (AIS) is usually caused by acute occlusion of the cerebral artery. Bilateral anterior cerebral arteries (ACAs) originating from the anterior communicating branch of the same internal carotid artery are a rare anatomical variation in clinical practice. Mechanical thrombectomy (MT) of simultaneous acute occlusion of the bilateral ACAs with this variation has rarely been reported.
Case Presentation: A 49-year-old man was referred for sudden onset of right-side weakness and aphasia for almost 55 min. AIS was considered after no bleeding was observed on emergency head computed tomography. Digital subtraction angiography was performed, and bilateral ACAs were found to originate from the anterior communicating branch of the left internal carotid artery and were occluded in their A2 segment. After immediate emergency MT with a stent retriever, the symptoms obviously improved.
Conclusion: Simultaneous acute occlusion of the bilateral ACAs originating from the anterior communicating branch of the same internal carotid artery is rare in clinical practice. For such patients, MT with a stent retriever is feasible even if there is a risk of thrombectomy escape, and a stent retriever with aspiration or a direct aspiration technique may be more appropriate.
Keywords: acute ischemic stroke, anterior cerebral artery, mechanical thrombectomy, stent retriever, case report
Background
Vascular recanalization methods, including intravenous thrombolysis and mechanical thrombectomy (MT), are effective measures for the treatment of acute ischemic stroke (AIS).1,2 Following six randomized trials,3 MT has become the gold-standard treatment for AIS caused by acute large vessel occlusion in the anterior circulation, such as middle cerebral artery (MCA) M1 segment but not the anterior cerebral artery (ACA) occlusion. Most scholars tend to classify any segment of the ACA as distal arteries during MT.4,5 However, in the present guidelines, there is no consensus on whether to perform MT for patients presenting with AIS caused by distal arteries such as ACA(s).6,7 Furthermore, different first-line MT techniques remain unclear for ACA occlusion.8 We herein present a case of bilateral ACA occlusions with a rare anatomical variant that was successfully reperfused with MT by using a 4×20 stent retriever.
Case Presentation
A 49-year-old male was referred for sudden onset of right-side weakness and aphasia for 55 minutes, with an initial National Institute of Health Stroke Scale (NIHSS) score of 23 [(3 +2+2)+1+0+0+(0+4)+(0+4)+0+2+3+2+0] and a modified Rankin Scale (mRS) score 3. He had a history of rheumatic heart disease with atrial fibrillation and had been on oral warfarin anticoagulant therapy. AIS was considered after no bleeding was observed on emergency head computed tomography. Considering that the specific value of the patient’s international normalized ratio was unknown and given the risk of intravenous thrombolytic bleeding, we decided to perform MT directly after obtaining the consent of the patient’s family. The patient was then taken to the catheter room and prepared for an endovascular thrombectomy and the door-to-puncture time was 36 minutes. Digital subtraction angiography (DSA) in the posterior–anterior projection showed the bilateral A2 segments ACAs originating from the left A1 segment, and both bilateral A2 segments ACAs were occluded (Figure 1). Consider this rare anatomical variation and the fact that the existing aspiration catheter hardly reaches the occlusive site, MT then was performed by using a 4×20 stent retriever (RECO; Minitech Medical, Wuxi, China) to revascularize the bilateral ACAs (Figure 2). After the respective first thrombectomy trial with the stent retriever, the bilateral ACAs were completely reperfused with modified thrombolysis in cerebral ischemia 3, but secondary thrombi were found in the MCA bifurcation. Most thrombi were removed in the MCA bifurcation after the use of direct aspiration technique. Imaging was performed within the following 24 h using magnetic resonance imaging. A recent infarction in the bilateral ACA territory and part of the left MCA territory was found. The patient achieved an NIHSS of 4 and a mRS of 1 at the 3-month follow-up.
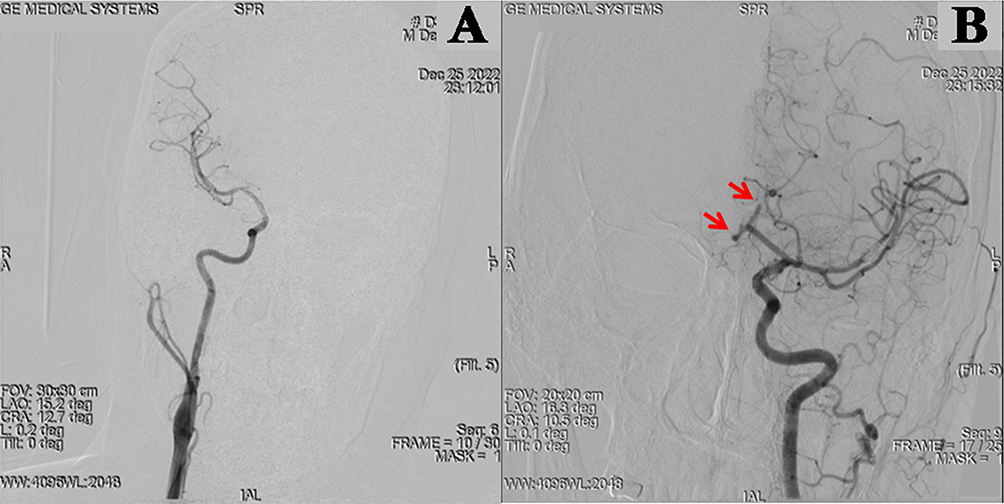 |
Figure 1 Digital subtraction angiography (DSA) of anterior circulation in posterior–anterior projection. (A) DSA in the posterior–anterior projection showed that the right internal carotid artery (ICA) did not send out the anterior cerebral artery (ACA). (B) DSA in the posterior–anterior projection showed bilateral ACAs originating from the left ICA, and both ACAs were occluded in their A2 segment (red arrow). |
 |
Figure 2 Mechanical thrombectomy of bilateral anterior cerebral arteries (ACAs) and left middle cerebral artery (MCA) and diffusion weighted imaging (DWI) images after thrombectomy. (A) A stent retriever (RECO RVV-I-4-20) was employed in the right ACA and good recanalization was achieved in the first pass. (B) Some clots were found in the stent retriever after the first thrombectomy trial with the stent retriever. (C) Bilateral ACAs were completely reperfused with modified thrombolysis in cerebral ischemia (mTICI) 3 after the respective first thrombectomy trial with the stent retriever, but secondary thrombi were found in the MCA bifurcation (green arrow). (D) Most thrombi were removed from the left MCA using a direct aspiration technique. (E) Bilateral ACAs and left MCA were completely reperfused with mTICI 3 after the first thrombectomy trial. (F) Postprocedural magnetic resonance angiography brain DWI showed a recent infarction in the bilateral ACA and part of the left MCA territory (white arrow). |
Discussion/Conclusion
Acute occlusion of the ACA is infrequent and often has poor outcomes, with pleomorphic clinical presentations in clinical practice.9,10 Concerning the differential lumen diameter and the highly heterogeneous angioarchitecture of the ACA, most scholars tend to classify it as distal arteries during MT.4 Therapeutic options for ACA acute occlusion include intravenous thrombolysis or MT.8 The MT in patients with acute occlusions of distal ACA branches appeared safe and technically effective, with high recanalization rates in several studies.11–13 However, one study suggested that despite the high recanalization rate and low complication rate, the clinical outcome of MT of the ACA was unsatisfactory.14 Furthermore, the MT of the ACA has not been strongly recommended by the guidelines in China.7 Therefore, the MT of ACA is controversial.
Simultaneous occlusion of the variant bilateral ACAs is clinically rare. The DSA of this case showed bilateral ACAs originating from the anterior communicating branch of the left ICA, and both ACAs were occluded in their A2 segment; this is related to the patient’s underlying rheumatic mitral stenosis with atrial fibrillation. Leonardo Rangel-Castilla presented a 2-dimensional operative video of MT of azygous ACA acute occlusion.15 There is also a study16 supporting the feasibility of ACA aspiration thrombectomy because it can effectively reduce the chance of fragmented clot escape. Considering the small calibre of the ACA with many acute angles and a tortuous vascular course, the lack of a suitable small-size aspiration catheter in our centre, MT with a stent retriever was adopted in this case. Though both ACAs originated from the same ICA and were occluded at the same time, good results with no complications were achieved in this case.
Successful reperfusion is an independent predictor of a good functional outcome for the MT of the ACA.5 However, in the process of anterior circulation intravenous thrombolysis or MT, the most common thrombus escape event is thrombus escape from the MCA to the ACA rather than the ACA to the MCA. Furthermore, thrombus escape is more common in the process of MT with only the stent retriever, but it is not reported in the process of direct aspiration or stent retriever with aspiration.11,17 In this case, we found that the thrombus escaped to the MCA during the process of MT with a stent retriever in the ACA. After further direct aspiration, we successfully removed the thrombus that escaped to the MCA. The embolism removed from the ACA can easily escape to the MCA, which is related to the obtuse angle formed by the two, the large diameter of the proximal MCA, and its fast blood flow rate during the process of MT with a stent retriever. Therefore, we recommend a stent retriever with aspiration or a direct aspiration technique using suitable devices for the MT of the ACA to avoid thrombus escape and related complications.18,19
To the best of our knowledge, this is the first reported case of simultaneous occlusion and successful MT with a stent retriever of bilateral ACAs originating in the anterior communicating trunk of the ipsilateral ICA. Although thrombus escape occurred during MT with a stent retriever, the patient also achieved a good prognosis, with no complications, which also suggests the importance of using a stent retriever with aspiration or a direct aspiration technique in acute occlusions of ACA. While the case demonstrates technical success, its generalizability is limited by the unique anatomy and single-patient nature. Future low-profile stent retrievers and/or smaller microcatheters designed for distal application appear to be beneficial for patients with acute occlusions of ACA, and similar cases also need to be collected and reported in multicenter studies.
Abbreviations
ACA, anterior cerebral artery; AIS, acute ischemic stroke; DSA, digital subtraction angiography; ICA, internal carotid artery; MCA, middle cerebral artery; mRS, modified Rankin Scale; MT, mechanical thrombectomy; NIHSS, initial national institute of health stroke scale.
Ethics Approval and Consent to Participate
Ethical approval is not required for this study in accordance with local or national guidelines. The patient’s informed consent was obtained during the assessment visits.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to this report, may that be in the conception, design study, execution, acquisition, analysis or interpretation of data; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Joo Won C, Yang Q, Tej IM, et al. The Vecta 46 intermediate catheter for mechanical thrombectomy of distal medium vessel occlusions: a single-center experience. Interv Neuroradiol. 2024. doi:10.1177/15910199241283513
2. Ashutosh PJ, Shashvat MD, Tudor GJ. Indications for mechanical thrombectomy for acute ischemic stroke: current guidelines and beyond. Neurology. 2021;97. doi:10.1212/wnl.0000000000012801
3. Boyle K, Joundi RA, Aviv RI. An historical and contemporary review of endovascular therapy for acute ischemic stroke. Neurovasc Imag. 2017;3(1):1. doi:10.1186/s40809-016-0025-2
4. Saver JL, Chapot R, Agid R, et al. Thrombectomy for distal, medium vessel occlusions: a consensus statement on present knowledge and promising directions. Stroke. 2020;51(9):2872–2884. doi:10.1161/strokeaha.120.028956
5. Anadani M, Alawieh A, Chalhoub R, et al. Mechanical thrombectomy for distal occlusions: efficacy, functional and safety outcomes: insight from the STAR collaboration. World Neurosurg. 2021;151:e871–e879. doi:10.1016/j.wneu.2021.04.136
6. Powers WJ, Derdeyn CP, Biller J, et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(10):3020–3035. doi:10.1161/str.0000000000000074
7. Chinese Society of Neurology, Chinese Stroke Society, Neurology. IGoCSo. Chinese guidelines for the endovascular treatment of acute ischemic stroke 2022. Chin J Neurol. 2022;55(6):565–580.
8. Cem B, Nicole H, Kristen H, et al. First-line thrombectomy strategy for distal and medium vessel occlusions: a systematic review. J Neurointerv Surg. 2022;15(6). doi:10.1136/jnis-2022-019344
9. Arboix A, García-Eroles L, Sellarés N, Raga A, Oliveres M, Massons J. Infarction in the territory of the anterior cerebral artery: clinical study of 51 patients. BMC Neurol. 2009;9:30. doi:10.1186/1471-2377-9-30
10. Filioglo A, Simaan N, Honig A, et al. Outcomes after reperfusion therapies in patients with ACA stroke: a multicenter cohort study from the EVATRISP collaboration. J Neurol Sci. 2022;432:120081. doi:10.1016/j.jns.2021.120081
11. Miszczuk M, Kleine J, Riegler C, Bauknecht H, Bohner G, Siebert E. Mechanical thrombectomy of acute occlusions of individual distal anterior cerebral artery branches. J clin neurosci. 2022;98:137–141. doi:10.1016/j.jocn.2022.02.003
12. Pfaff J, Herweh C, Pham M, et al. Mechanical thrombectomy of distal occlusions in the anterior cerebral artery: recanalization rates, periprocedural complications, and clinical outcome. AJNR Am J Neuroradiol. 2016;37(4):673–678. doi:10.3174/ajnr.A4594
13. Grossberg J, Rebello L, Haussen D, et al. Beyond large vessel occlusion strokes: distal occlusion thrombectomy. Stroke. 2018;49(7):1662–1668. doi:10.1161/strokeaha.118.020567
14. Uno J, Kameda K, Otsuji R, et al. Mechanical thrombectomy for acute anterior cerebral artery occlusion. World Neurosurg. 2018;120:e957–e961. doi:10.1016/j.wneu.2018.08.196
15. Rangel-Castilla L, Siddiqui A. Azygous anterior cerebral artery acute occlusion managed with endovascular mechanical thrombectomy: 2-dimensional operative video. Operative Neurosurg. 2019;16(4):514–515. doi:10.1093/ons/opy183
16. Chung G, Kwak H, Park J, Lee J. Manual aspiration thrombectomy with a penumbra catheter for acute anterior cerebral artery occlusion. Interv Neuroradiol. 2017;23(4):416–421. doi:10.1177/1591019917702521
17. Kurre W, Vorlaender K, Aguilar-Pérez M, Schmid E, Bäzner H, Henkes H. Frequency and relevance of anterior cerebral artery embolism caused by mechanical thrombectomy of middle cerebral artery occlusion. AJNR Am J Neuroradiol. 2013;34(8):1606–1611. doi:10.3174/ajnr.A3462
18. Ding HJ, Ma C, Ye FP, Zhang JF. Bridging therapy and direct mechanical thrombectomy in the treatment of cardiogenic cerebral infarction with anterior circulation macrovascular occlusion. World J Clin Cases. 2021;9(27):8051–8060. doi:10.12998/wjcc.v9.i27.8051
19. Zhang H, Wang Y, Yaching Z, et al. Effects of taijiquan “yunshou” action motor imagery on hand motor function in hemiplegic patients after stroke (in Chinese). Chin J Mod Nurs. 2014;26(3297–3301):002. doi:10.3760/cma.j.issn.1674-2907
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Eosinophil: A New Circulating Biomarker for Risk of Poor Outcome in Stroke Patients Undergoing Mechanical Thrombectomy
Yu S, Huang ZC, Wang HS, Liu SW, You SJ, Hou J, Guo ZL, Xiao GD
Clinical Interventions in Aging 2023, 18:523-531
Published Date: 28 March 2023
Comparison of the Clinical Outcomes Between Reperfusion and Non-Reperfusion Therapy in Elderly Patients with Acute Ischemic Stroke
Luo X, Chen S, Luo W, Li Q, Zhu Y, Li J
Clinical Interventions in Aging 2024, 19:1247-1258
Published Date: 10 July 2024
Postoperative Blood Glucose Trajectories are Associated with Inflammatory Markers and Functional Outcomes in Acute Ischemic Stroke Treated by Thrombectomy
Liu Y, Zhong H, Huang J, Wang Y
Vascular Health and Risk Management 2026, 22:587043
Published Date: 27 February 2026