Back to Journals » Advances in Medical Education and Practice » Volume 14
Physician-Patient Communication Course: When the Inauguration of a New Israeli Medical School Coincided with COVID-19 Pandemic
Authors Kushnir T ![]() , Sandhaus Y
, Sandhaus Y ![]() , Castel H, Golik A, Salai M
, Castel H, Golik A, Salai M ![]() , Tzabari A
, Tzabari A ![]() , Yahav Y, Grossman Z, Mazuz H, Ashkenazi S
, Yahav Y, Grossman Z, Mazuz H, Ashkenazi S
Received 12 April 2023
Accepted for publication 13 August 2023
Published 19 September 2023 Volume 2023:14 Pages 1013—1024
DOI https://doi.org/10.2147/AMEP.S410953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Talma Kushnir,1,2,* Yoram Sandhaus,1,* Hana Castel,1,* Ahuva Golik,1,* Moshe Salai,1,* Avinoam Tzabari,1,* Yakov Yahav,1,* Zachi Grossman,1,* Hana Mazuz,3,* Shai Ashkenazi1,*
1Adelson School of Medicine, Ariel University, Ariel, Israel; 2Department of Psychology, Ariel University, Ariel, Israel; 3Simulation Center, Ariel University, Ariel, Israel
*These authors contributed equally to this work
Correspondence: Talma Kushnir, Adelson School of Medicine, Ariel University, 65 Ramat-HaGolan Street, Ariel, 40700, Israel, Tel +972528651294, Email [email protected]
Purpose: The curriculum of the Adelson School of Medicine at Ariel University, the newly established sixth medical school in Israel, includes a simulation center-based extended course on physician-patient communication, aiming to help students master the core competency of interpersonal and communication skills. For more than a year following the emergence of the COVID-19 pandemic, the school suspended most face-to-face (F2F) encounters, transforming most teaching activities to remote platforms. The paper outlines the ways we adapted teaching of this course to these circumstances, the reactions of students and mentors to the changes and results of 1st year students’ survey.
Methods: During the lockdown in the first year 48 of 70 first-year students participated in a voluntary anonymous online evaluation of the course assessing motivation to become a physician; perceptions, feelings and attitudes towards the communication course, and advantages and disadvantages of online and F2F medical interviews.
Results: 46.1% of the responding students reported that the pandemic strengthened their desire to become physicians. 56.3% claimed that they were able to a relatively large extent to empathize with COVID-19 patients who were exposed to the virus; 79.1% viewed their mentors as positive role models of communication skills. The students were able to receive and offer social support to their peers. They evaluated very highly the short instructional videos produced by the faculty.
Conclusion: During the lockdown, the respondents generally indicated positive attitudes towards the communication course, the mentors and the inclusion of physician-patient communication as a topic in medical education. The students and mentors reported many disadvantages and few advantages of remote learning. Yet inevitably remote learning including online-based simulations is a step towards preparations for future practice within virtual medical care and telemedicine. The limitations of this study include the cross-sectional design, small sample size and self-reporting.
Keywords: Medical education, COVID-19, communication skills, face-to-face, distance teaching, simulations, 1st year students
Introduction
Communication is a basic process in any human interaction and communicating with patients, their families and health professionals is a major component in medical practice.1 The medical dialogue begins when the patient communicates that she or he seeks help from a physician and the physician responds to this this request. Good communication skills that include, for example, active listening, empathy and paying attention to the verbal and nonverbal aspects and cues in the medical encounter were found to improve patient’s compliance with medical recommendations and overall satisfaction.2 As Markos3 suggested, a good communicator listens to the patient and tries to understand his or her special needs and point of view. If the patient realizes that the doctor really cares about how he or she feels and his or her point of view regarding treatment plans, this is a therapeutic process for the patient. The outcomes are improved trust and better adherence to the doctor’s opinions and advice. It follows that competence in interpersonal and communication skills by healthcare professionals is essential for optimal healthcare delivery.4
The Accreditation Council for Graduate Medical Education (ACGME) identified interpersonal and communication skills as one of six areas in which physicians-in-training need to demonstrate competence.5
In the Adelson School of Medicine at Ariel University, the newly established sixth medical school in Israel, we adopted the ACGME approach and included an extended course on physician-patient communication in the curriculum. The course is delivered as a communication skills workshop that promotes experiential learning and creates opportunities for skill practice and coaching by mentors. It is held in the medical simulation center that is located within the university.
Soon after the inauguration of the school in 2019, at the beginning of the second semester, we faced the emergence of the COVID-19 pandemic and consequently the national quarantine with an unexpected shut down of all F2F classes and interactions. In order to preserve studies and promote learning, we immediately switched to the alternative mode, ie, online distance learning.
Courses focusing on non-cognitive aspects of medicine, especially those that specifically target the acquisition of interpersonal skills and professionalism, are often referred to as “Doctoring” courses.6 They are based, among other principles, on the perception of medicine as a “human science”7 and on the importance of direct F2F contact. The pandemic that enforced quarantines/lockdowns and social distancing facilitated the loss of human contact and imposed severe barriers to the delivery and management of such courses. Social distancing practices are diametrically opposed to the students’ ability to maintain direct and close interpersonal contact with mentors and peers.
In a previous paper we described the transition of teaching in the Ariel University School of Medicine from F2F to online distance teaching during the COVID-19 quarantine.8
In the present paper, we focus specifically on the physician-patient communication and professionalism course. We aim to 1. Describe how we adapted the course, not without struggles, to the abrupt and unforeseen circumstances; 2. Report findings from a study among first year medical students regarding the pandemic’s impact on their perceptions of the medical profession, their capacity to empathize with patients and medical staff, and their satisfaction with various teaching modes such as F2F, online simulations and instructional videos. 3. Describe mentors’ reactions to the inevitable changes in the delivery of teaching in the first two years of the medical program.
Materials and Methods
A. The Physician-Patient Communication Course at Ariel University
The medical school at Ariel University is based on a four-year program of post-graduate studies and enrolls 70 students each year. In addition to courses in basic medical sciences that are taught in the first year and integrative teaching of the body systems in the second year, the curriculum includes an extended course on physician-patient communication and professionalism. It involves the students throughout the medical program with various levels of investment, the heaviest being in the first year. The class is divided into six small groups, each mentored by an experienced physician who had been previously involved in medical education.
All the meetings are hosted by the medical simulation center at Ariel University. This facility offers a variety of possibilities for holding lectures, practical demonstrations, meetings, recording of activities, production of original videos, and conducting interactive sessions with mentors and professional simulated patients by experienced actors.
B. Basic Features of the Physician-Patient Communication Course
The communication and interpersonal skills course reflects the patient-centeredness approach to healthcare.9 The course was designed based on several pedagogical principles. First, it is delivered as a communication skills workshop, an approach that was found to be superior to alternative delivery approaches, such as lectures, computer-based modules, and video/audio review of communication skills4 and case-based role-play approach.10 Second, it is based on the assumption that verbal communication skills, like manual skills, can be improved with deliberate practice repeated over time.1 Thus, the teaching methods used in this course to promote skill acquisition (rather than just talking about communication) create opportunities for skill practice and coaching.11 This is achieved by using experiential learning through role-playing scenarios, and direct observation of physician-patient encounters by simulated patients. Third, the teaching emphasizes awareness of biopsychosocial aspects related to both physical details emotions, attitudes and cognitions that may affect communication. The fourth important principle is that the course facilitators have extended pedagogical knowledge and experience in communication skills training.
In the first year the students attend extended meetings (six academic hours) every two weeks. Each meeting begins with an assembly of the whole class featuring an introductory presentation, followed by breakout sessions of six small tutorial groups in smaller rooms led by the groups’ mentors.
The majority of the meetings involve participation in simulations of medical encounters with professional actors followed by feed-back rounds with the peer group, the actor and the mentor. The classic contents of the course in the first year include learning basic communication and history-taking skills, adopting a patient-centered communication style, non-verbal communication, identifying the hidden agenda, cultural competence and so on. This format was kept even after the transition to online distance learning using online simulations.
In the second year the emphasis shifts to a broader analysis of professionalism in various medical specialties, preventing errors, developing medical students’ resilience and outreaching to the elderly in the community.
C. How the Communication Course Was Conducted During the Lockdowns and Social Distancing Periods
The communication course started at the beginning of the 2019 academic year, following the festive inauguration of the school. The first semester sailed smoothly. Preparations were made to conduct the second semester in March 2020, starting with medical encounters in the clinics residing within the campus multi-disciplinary treatment center.
In hind sight it appears that this period in time was “the normal” that was soon replaced by the “new normal”.12 Just when the second semester was approaching, rumors were spreading about an unknown mysterious and deadly illness. Worldwide apprehension was rising. Slowly but surely, “The preposterous has happened and has ravaged the world”.13 When life in the shadow of the COVID-19 pandemic became the reality, we realized that we were given a grace period of only one “normal” academic semester by which to ignite the system as planned.
Similar to other medical schools across the globe, since the emergence of the pandemic14 our school had been obliged to adapt all the educational processes by suspending most F2F encounters and transforming teaching into remote online platforms. As students and mentors of the 2019–2020 class were adjusting to the new reality of virtual teaching, learning and assessment, during the next three semesters in the shadow of COVID-19 the academic routines of medical studies were ridden with uncertainty. While we were unrealistically hopeful that the pandemic will be resolved shortly, as time progressed and uncertainty increased, reality of the “new normal” sank in. We made every effort to provide theoretical knowledge as well as to engage students in a variety of simulations and written assignments, requiring them to practicing communication skills so as to ensure that they made progress and complete the first and then the second academic years.
After about a year, F2F teaching was gradually and hesitantly resumed, during the second semester of 2021. The six groups met separately, under strict adherence to the “Green” and “Purple” passes (ie certificates issued by the Israeli Ministry of Health during the pandemic; Green Pass was a valid negative coronavirus test result and Purple Pass represented restrictions on gatherings). To resume F2F meetings on campus we obtained a special permission of the university to hold “a communication workshop” parallel to the classes in anatomy since most studies in the university faculties were still conducted online and the campus was practically deserted. To preserve sufficient social distancing the first meeting was held on a warm day in April 2021 on a tree-lined spacious grass park that felt like a happy reunion and picnic. Later on in the semester, F2F role-playing sessions with simulated patients were resumed within the small groups and lasted till the end of the academic year in June 2021.
Nevertheless, while the original intention was to assess students’ performance at the end of the academic year by OSCE, because of the severe interruptions in three consecutive semesters in 2020–2021, performance evaluation of the students’ progress was switched to online written examinations.
D. Examples of Learning Tasks During the Distance Learning Period
Following the switch to distance online learning, we engaged the first year students in several learning activities throughout the second semester in 2020. The main task was to conduct history taking interviews with volunteers enlisted by each student, using video-chat applications of their choice (eg ZOOM, Skype or WhatsApp) and using the same instructions regarding the contents of information to be gathered. The reports were submitted to the mentors without revealing the identity of the interviewees. This task represents a video-chat replication of the F2F interviews held in the first semester.
In the absence of opportunities for F2F contacts during the lockout in the second semester in 2020, this exercise was devised to practice and maintain the interviewing skills acquired in the first “normal” semester. In addition, this task simulates the pervasive use of remote consultations across all medical specialties nowadays15 and thus it represents a step towards preparing the students to future practice within virtual medical care and telemedicine. As suggested recently,16 as the use of telehealth continues to increase, medical students and residents should become familiar with virtual patient encounters.
Another significant small group activity followed lectures on medical ethics. It involved discussions on ethical dilemmas concerning, for example, treatment of coronavirus patients or prioritizing decisions in emergency services. Individual and collective reports were submitted to the mentors.
A third example of learning tasks concerned outreaching to the community of elderly immigrants. After the end of the third lockdown and a gradual relaxation of COVID-19-related restrictions during the second semester of 2021, students in the second year were required to conduct several consecutive meetings with elderly residents, mostly immigrants who live in seven sheltered hostels managed by Ariel University. These meetings were preceded by lectures on geriatrics and gerontology. The main aim was to acquaint the students with problems and difficulties faced by older people in the community who, despite being independent, usually suffer from a variety of health issues as well as from social isolation that is independent of the effects of the coronavirus. The program was expected to benefit both students and elderly residents, but unfortunately encountered several logistic problems on both sides and was only partially successful. For example, many residents who first consented, later on declined to meet the students. Several residents and students were anxious about contracting the coronavirus in a F2F meeting. Some students with young children had difficulties in finding the time to access specific facilities far from home. Nevertheless, lessons have been learned and the next program, soon to be implemented, is expected to be more successful.
E. Compiling a Collection of Recorded Simulations and Short Instructional Videos
We have compiled a collection of video simulations of medical encounters to be used for tutorials on communication skills and professionalism in medicine. The intention to establish this “bank” preceded the pandemic. The scenarios are prepared by our faculty (the mentors), enacted by them and supported by additional professional actors. The videos are recorded in the simulation center. The growing collection also includes several short instructional videos, each featuring one of the mentors who outline a specific issue and/or medical procedure. Such a video is usually presented to the class prior to participation in a simulation of a medical encounter. The purpose of these videos is to help first- and second-year students who, during the pre-clinical years, have very limited medical knowledge and who usually express concern and even anxiety when required to participate as interviewers or spectators in a simulation.
F. A Survey of Perceptions, Feelings and Attitudes of First Year Medical Students Towards the Communication Course During the COVID-19 Pandemic
During April and May 2020 in the second semester of medical studies, we asked the first-year medical students to participate in a voluntary and anonymous online evaluation of the physician-patient communication course. At that time, social distancing was already enforced and all studies at Ariel University had been shifted completely to virtual learning platforms. The survey included assessment of students’ reactions and attitudes towards the learning demands and environment, the mentors; and indications of their budding professional identity at this phase of the crisis while witnessing the worldwide struggle of medical staff with COVID-19. All participating students provided digital informed consent.
The Survey Questionnaire
The questionnaire included two parts (See Supplementary Figure 1). The first was a single question on professional ambitions:
In what way has your ambition to become a physician changed when you witnessed how healthcare systems and medical teams in Israel and around the world responded to the COVID-19 crisis?
This question had three response options: 1. has affected my ambition negatively; 2. has not changed my ambition; 3. has strengthened my ambition.
Part 2 included 11 questions, each with a 7-point response scale ranging from 1 (to a very small extent) to 7 (to a very large extent). They represented several aspects of students’ responses to medical studies during the COVID-19 era: 2 questions on professional identity (eg “To what extend do you feel already a part of the healthcare/medical system in Israel?“); 3 items on professional skills (eg “As a medical student at this point in time, to what extent do you think you are able to conduct a medical interview, as taught in the physician-patient communication course, on your own?”); 2 items on attitudes towards the course (eg “To what extent do you view the learning of communication skills an essential part of medical education?”; and 4 items on social support from peers in the medical school (eg To what extent are your peers in the communication course helping you with the demands of medical studies?)
Results
A Survey of First-Year Medical Students at the COVID-19 Crisis
Forty-eight students (response rate of 70%) completed the questionnaire, mostly women (86.7%, a close representation of the 81.1% of women in the class). The median age was 28 years and slightly more than half of the respondents were married (53.5%); 14 (34.1%) of the respondents were parents.
Part 1 of the Survey - Professional Ambitions
It appears that engaging in medical studies in the global shadow of the COVID-19 crisis has strengthened the ambition to become physicians of 46% of the respondents. Only 4% claimed that their ambition was impaired and 50% indicated that their professional ambition remained intact. This is a very interesting result when compared to the responses to question 2 (Q2) in part 2 (medicine as a risky profession); 25 (52%) of the respondents felt that they perceived the medical profession as a relatively risky profession (response grades 5–7) and 9 (18.7%) even rated it as a large or very large risk to their health.
Part 2 of the Survey – Identity, Skills, Attitudes and Social Support
Table 1 presents the results of students’ responses to part 2 of the online survey.
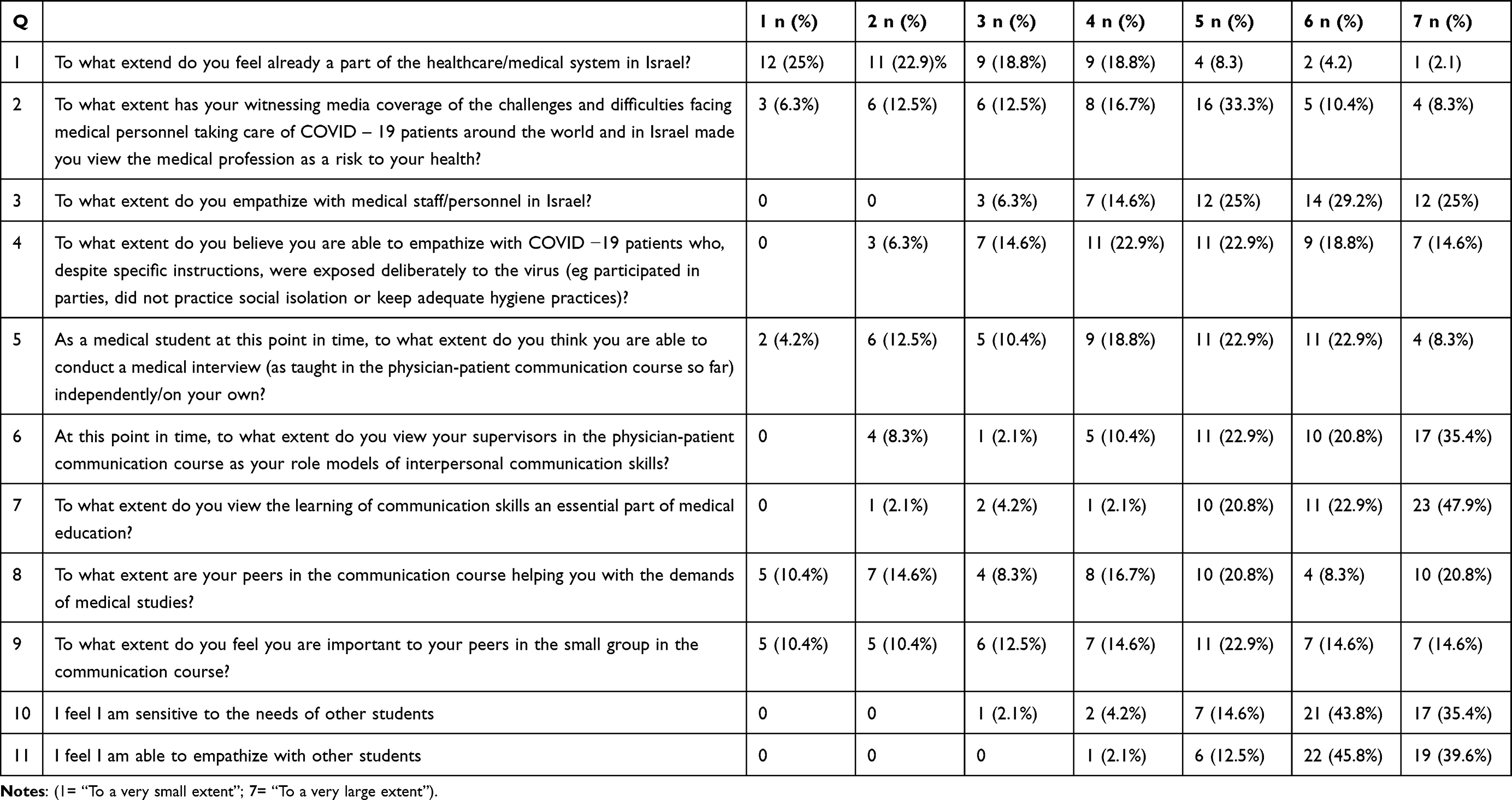 |
Table 1 The Distribution of Students’ Responses to Part 2 of the Online Survey |
a. Professional identity (Q1, Q3). At the second semester of the first year most of the respondents did not yet view themselves as part of the Israeli medical system (Q1); only 7 (14.6%) responded that they felt as part of the system to a relatively large extent (responses 5–7). This reflects the fact that during the first year of medical school at Ariel University, during the COVID-19 crisis, the students were not exposed officially to any parts of the medical system. Nevertheless, most of the respondents (38, 79%) expressed relatively high rates (grades 5–7) of empathy/identification with the medical personnel/teams in Israel (Q3) (Table 2).
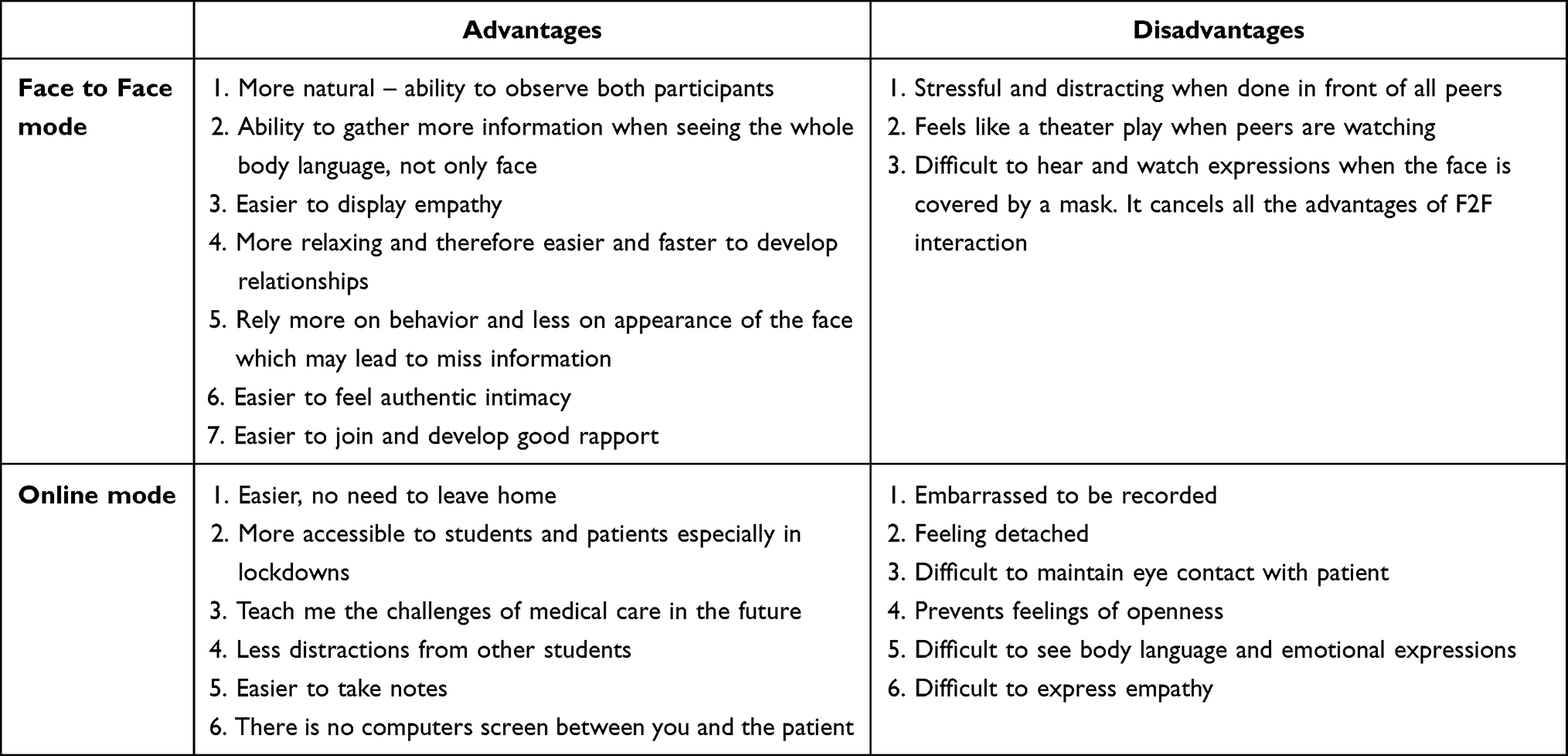 |
Table 2 Students’ Main Reported Advantages and Disadvantages of Face-to-Face Vs Online Simulations of Physician–Patient Interactions |
b. Professional skills (Q4, Q5). Slightly more than half of the respondents (56.3%) claimed that they were able to a relatively large extent (grades 5–7) to empathize with COVID-19 patients who, despite specific instructions - were exposed to the virus (eg participated in parties, did not practice social isolation or kept adequate hygiene practices). However, only a quarter (24%) replied that they were able to empathize to a large or very large extent (grades 6–7).
As to the perceived ability to conduct a medical interview independently (as taught in the physician-patient communication course), about half indicated a rather high degree of interviewing competence; 26 (54.1%) believed to a relatively large extent (grades 5–7) that they were able to be independent, and only 15 students (27.2%) believed to a large or very large extent that they could do it independently.
c. Attitudes towards the course (Q6, Q7). 38 (79.1%) of the respondents viewed their mentors in the physician-patient communication course as their role models of interpersonal communication skills to a relatively large extent (grades 5–7) and 27 (56.2%) – as a high or very high extent. Regarding the endorsement of communication skills as an essential part of medical education, the majority of the respondents, 44 (84.6%), agreed with the statement to a relatively high extent (grades 5–7) and 34 (70.8%) to a large or very large extent.
d. Social support from peers in the medical school (Q7–11). The students’ responses revealed a very important pattern regarding the social atmosphere in the virtual class during that time. Despite the lockdowns and social distancing enforced throughout the country that mandated distance learning in the medical school, the students collaborated and supported each other in various ways. Twenty-four (49.9%) reported that their peers helped them to cope with the demands of the course to a relatively high degree (grades 5–7) and 25 (52.1%) claimed that they feel important to their peers in the mentoring group to a relatively high degree (grades 5–7). Furthermore, 38 (79.2%) reported that they were sensitive to the needs of other students to a high or very high degree (grades 6–7); and 41 (85.4%) claimed that they were able to feel sympathetic towards other students to a high or very high degree (grades 6–7).
First Year Students’ Comparisons Between F2F and Online-Based Simulations
In a written exam at the end of the second year, one of the questions required the students to compare the advantages and disadvantages of F2F and online-based simulations they experienced throughout the academic year. The contents of the responses were analyzed qualitatively to trace common positive and negative themes. Although on the whole most of the students found more advantages than disadvantages in the F2F simulations, most students also detected several advantages of online-based simulations. Table 2 summarizes the major points that emerged from the students’ responses.
Student Satisfaction from Short Instructional Videos
When asked at the end of the first year in medical school to rate the helpfulness of the short videos on a scale of 1 to 10, the vast majority of the class (76.2%) rated them as 9–10 and rarely below 7. Such levels of satisfaction support the 2015 Kaltura software company report17 on the impact of video on the learning experience. 93% of their respondents believe that the use of educational videos improves the learning experience and that on the whole videos are good teachers. The length of the instructional videos in our bank varies between 5 and 9 minutes, as recommended in the report for an optimal length.
Mentors’ Experiences of the Switch to Distance on-Line Teaching
Together with the rest of the medical school faculty, the mentors in the communication course adapted quite fast to the demands of online distance learning. Technical or digital naivety was soon aided by information communication support experts of the university. Nevertheless, the mentors longed to resume direct contact with others. In regular Zoom meetings of the mentors held during the entire year, they often expressed their disappointment and even irritation with the termination of F2F student–mentor interactions and its replacement by remote interactions through the ZOOM application. They also voiced dismay over the lack of F2F interactions with fellow mentors and colleagues.
There were two main sources of frustration. The first was the loss of rewarding close and enjoyable human contact that characterizes normal social life in general, and tutoring in particular.
A second significant source of frustration was students’ tendency to leave their ZOOM windows blank, leading to inability to monitor their presence during the online sessions, especially those that involved the whole class. The difficulty in assessing the level of student involvement in the course may cause mentors to feel they are “talking to the wall”, reactions that signify negative impact on teacher motivation. Fortunately, attendance in the small groups meetings was maximal. One advantage of blank ZOOM windows was a reduction of visual distraction when only the interviewer and simulated patient appeared on the screen, leading to improved performance.
Discussion
A. Students’ Responses
The responses of the first year medical students to the evaluation survey were generally encouraging in the sense that they indicated positive attitudes towards the course, towards the mentors as well as to the inclusion of physician-patient communication as a topic in medical education. These responses emerged despite the fact that the sudden transition to distance learning was totally unplanned and therefore reactive (rather than proactive), thus without extended curriculum planning and faculty preparation.18
It is also interesting that at this early stage of medical studies almost 80% of the survey respondents identified and empathized with Israeli healthcare teams to a great extent, although most of them did not yet consider themselves as part of the medical system. This finding is not surprising since, because of social distancing, these first year students had not yet been involved as professionals with the medical system. Social distancing and online learning have changed how students interacted with their mentors, the medical school and class mates and at least temporarily, the students lacked direct contact with role models and patients. It is therefore probable that the pandemic caused a major disruption that may have interfered with their professional socialization process.19 Socialization in medicine involves interactions with role models and mentors, exposure to clinical and non-clinical experiences, and a community of practice.20 Since socialization is considered a core process in professional identity formation (PIF),20 the disruption of these crucial experiences and interactions during remote learning and social distancing may have negatively affected PIF among these and other first year medical students.
Encouraging students to volunteer at this early stage might have prevented this situation to some extent. The first two years in medical school are the preclinical stage in which students mostly study on campus. Due to the lack of clinical and professional experience, volunteer work (nothings beyond their level of competence) such as participating in hotline or call-centers, monitoring asymptomatic patients during self-isolation through telephone or text-messages and public health education are some possible activities preclinical students can contribute to healthcare efforts during social distancing.19 Such participation in pandemic efforts may influence the development of professional values and identity of medical students,21 by reinforcing values, such as altruism, serving the community and society in times of crisis, and solidarity with the profession.22
Almost half of the respondents reported a strengthening of their desire to become physicians while almost none felt weakened, despite the perception of the profession as risky. It is perhaps the constant portrayal in the mass media of heroic acts of caring and self-sacrifice in the care of acutely ill COVID-19 patients that supports the perception of the medical profession as both risky and heroic.
Another encouraging finding was that despite lockdowns and distance learning, the students were able to receive and also offer practical and emotional support to their peers. This is an important finding with positive implications on the resilience of the students facing the crisis.
Following compulsory military service and then pre-med education, many of our medical students are relatively mature, in their mid-30’s, married with young children or co-habiting with a partner. With such background it may be assumed that practical and emotional support during lockdowns was available from family sources and contributed to their resilience. However, the students also reported that they gave and received social support from their class mates. Since the communication class includes six organic groups, each headed by a mentor, the students studied together in small groups (usually from the same geographical location), in which it is easier to form close relationships and consult with the mentor in each issue, not necessarily related to the specific communication course. Moreover, the students were supported by the medical student union so that practical assistance was easily available.
It was recently found among young students that the higher the degree of perceived social support, the lower is the degree of students’ general anxiety, and the lower is the degree of impact by the COVID-19 pandemic.23 The availability of social support also reflects previous findings that the shared identity and experience of being in a disaster leads people to cooperate in response to a crisis.24
The medical students at Ariel University experienced both F2F and distance online-based learning. They were therefore in a good position to compare their recent experiences of both teaching methods. It is interesting to note that the students were able to find some advantages of practicing interviewing skills through remote online simulations of physician-patient encounters (and not only disadvantages). Similarly, they pointed out several disadvantages of F2F simulations. This finding implies that both methods have merits for skill learning, perhaps depending on the particular student and therefore in the future the course could benefit from combining features of both modes of learning. As the use of telehealth keeps increasing, boosted by social distancing regulations, we could not agree more with the recent conclusion that medical students should become familiar with virtual patient encounters,13 and that developing telemedicine competencies should become an integral part of medical education.25
Limitations of the Student Study
The conclusions from the student part of this study should be viewed with great caution given the limitations of the study. Although the response rate is 69% of the entire class, the sample is very small and it may not represent the medical student population from the other five Israeli medical schools or students in more advanced years. In addition, the study was cross-sectional and unfortunately lacks a systematic follow up of the students involved. It is therefore impossible to compare the results to data collected from the same students at later stages of their medical education, particularly after the pandemic ended. Finally, the results are dependent on subjective self-reporting”.
B. Mentors’ Reactions
Mentors’ frustration with remote teaching is consistent with their regrets over the loss of F2F contact with students and other faculty members. It could be that physicians with vast professional experience and for whom becoming a mentor was a personal choice, are personally motivated by strong universal social needs for psychological communion, ie for fitting in and getting along with others.26 Zoom meetings with colleagues and students in which human contact is conducted by “talking heads” and regulated by the limits of an application greatly curtails and even thwarts the fulfillment of such needs thus reducing motivation for further similar contacts beyond those that are necessary.
A recent interesting description of physician motivation was presented by Dawnay27 who suggested that many physicians enjoy practicing medicine because they like affiliating with other people, the chance to meet new people and the ability to positively affect their lives. Indeed, some years ago a study found that tutoring medical students is one of the preferred activities of board-certified primary physicians and a means of preventing burnout.28 Moreover, the same survey found that burnout, which is mainly caused by repeated stresses and frustrations, is associated with discrepancies between the intensity of activities that the physician performs in the office and the level of satisfaction the physician receives from these activities.28 The sudden and complete social distancing leading to the loss of F2F contact and of the pleasure of student-mentor affiliation severely frustrated mentors’ social needs.
It appears then that the online learning mode may be less able to cultivate the relationship motivational facet of learning that plays a major role in F2F meetings. Based on the strong preference of both students and mentors for F2F skill learning and mentoring every effort should made to preserve this mode as far as possible.
As many students participate in remote learning by connecting to the ZOOM application with their cellular phone, a metaphor of telemedicine ironically suggested by Dawnay27 seems to apply to distance teaching and mentoring – The mentor arrives now “in the pocket or bag” of the students.
Conclusions
The findings demonstrate some of the impact of the pandemic on students’ perceptions of the medical profession, their capacity to empathize with patients and medical staff (communication skills), and their satisfaction with various teaching modes involved in this specific course, such as face-to-face and online simulations. The study highlighted the mentors’ perspective of teaching during social distancing. The findings help understand how switching to online learning during the pandemic influenced medical education on the whole and particularly student–mentor interactions in our communication course.
As educators in the physician-patient communication course at Ariel University Medical School, we summarized some of events and consequences of the tumultuous challenges we faced during the first two academic years. In a nut-shell, after initial drastic setbacks we soon rose to the challenge and were determined as ever to continue running our program, despite severe and unprecedented barriers.
We believe that through constantly adapting to unexpected challenges and setbacks dealt by the pandemic, we have managed even during lockdowns to teach successfully the physician-patient communication program that keeps evolving based on constant evaluation and student feed-back.
Although tele-teaching of communication skills has many drawbacks, it is here to stay in various forms. At some time during the pandemic it was obviously the only available alternative for teaching pre-clinical courses. Moreover, students identified some advantages of tele-teaching for skill learning. As Papapanou29 concluded, the adoption of online learning is a key strategy for ensuring continuity in medical education during COVID-19 pandemic.
Moving forward to a complete and long-term return to F2F medical education, we should be able to make the process more flexible and even reduce “classroom seat time”30 by incorporating into the design of future teaching the advantages of both F2F learning at the campus and offering online contents. However, we should be prepared to face in the future further waves and lockdowns due to unforeseen pandemics. Luckily, we now have a basic confidence and organizational memory of how we are able to quite rapidly adapt to sudden changes.
Based on the analysis of ten Cate14 on possible effects of the pandemic on medical competence, during the pandemic we learnt that flexibility and creativity are essential ingredients in coping with unexpected challenges to medical education at two levels at least: the micro level of the individual (teacher and student) and the meso level of the local program and institution. It is time now to figure out which of these innovations and adaptations should be retained, refined and integrated into the educational system.
The students’ favorable views regarding the inclusion of the physician-patient communication course in the new medical school curriculum indicate that they identify with ACGME’s recognition of interpersonal and communication skills as one of six areas in which physicians-in-training need to demonstrate competence.5
Students’ and mentors’ absolute preference for F2F mode of learning of communication skills suggests that the teaching of skills that involve interpersonal interactions and mentoring should be held as far as possible by F2F mode of learning unless circumstances mandate remote learning. Online learning should be used mainly for acquiring academic knowledge through texts, videos and lectures (live or recorded).
Finally, as Levine concluded31 since the learning that matters most in the development of health care professionals occurs in the context of relationships, every effort should be made to provide opportunities to develop close and meaningful relationships between mentors and students, an aspect of education that is hindered by distance/online learning.
Acknowledgments
We thank Oz Hamzani, a doctoral student in the Department of Psychology at Ariel University, who assisted at compiling the final questionnaire and analyzing the data.
Ethics Approval and Consent to Participate
The students’ survey was approved by the Institutional Ethics Committee of Ariel University (Reference number: AU-MED-TK-20200422). All participating students provided informed consent.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Henry SG, Holmboe ES, Frankel RM. Evidence-based competencies for improving communication skills in graduate medical education: a review with suggestions for implementation. Med Teach. 2013;35(5):395–403. PMID: 23444891. doi:10.3109/0142159X.2013.769677
2. Jahan F, Siddiqui H. Good communication between doctor-patient improves health outcome. Euro. J Med Health Sci. 2019;1(4). doi:10.24018/ejmed.2019.1.4.84
3. Markides M. The importance of good communication between patient and health professionals. J Pediatr Hematol Oncol. 2011;33(Suppl 2):S123–5. PMID: 21952568. doi:10.1097/MPH.0b013e318230e1e5
4. Stephens E, William L, Lim LL, et al. Complex conversations in a healthcare setting: experiences from an interprofessional workshop on clinician-patient communication skills. BMC Med Educ. 2021;21(1):343. doi:10.1186/s12909-021-02785-7
5. Exploring the ACGME core competencies: interpersonal and communication skills (Part 6 of 7). Available from: https://knowledgeplus.nejm.org/blog/exploring-acgme-core-competencies/.
6. Hafferty FW, Gaufberg EH, O’Donnell JF. The role of the hidden curriculum in “on doctoring” courses. AMA J Ethics. 2015;17(2):129–137. doi:10.1001/virtualmentor
7. Kumagai AK. From competencies to human interests. Acad Med. 2014;89(7):978–983. doi:10.1097/ACM.0000000000000234
8. Sandhaus Y, Kushnir T, Ashkenazi S.Electronic distance learning of pre-clinical studies during the COVID-19 pandemic: a preliminary study of medical student responses and potential future impact. Isr Med Assoc J. 2020;22(8):489–493. PMID: 33236581.
9. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington DC: National Academy Press; 2001.
10. Agago TA, Wonde SG, Bramo SS, Asaminew T. Simulated patient-based communication skills training for undergraduate medical students at a university in Ethiopia. Adv Med Educ Pract. 2021;12:713–721. PMID: 34211311; PMCID: PMC8240861. doi:10.2147/AMEP.S308102
11. Back AL, Fromme EK, Meier DE. Training clinicians with communication skills needed to match medical treatments to patient values. J Am Geriatr Soc. 2019;67(S2):S435–S441. doi:10.1111/jgs.15709
12. Kachra R, Brown A. The new normal: medical education during and beyond the COVID-19 pandemic. Can Med Educ J. 2020;11(6):e167–e169. doi:10.36834/cmej.70317
13. Carraccio C. Carraccio C. Harnessing the potential futures of CBME here and now. Acad Med. 2021;96(7S):S6–S8. doi:10.1097/ACM.0000000000004102
14. Ten Cate O, Schultz K, Frank JR, et al. Questioning medical competence: should the COVID-19 crisis affect the goals of medical education? Med Teach. 2021;43(7):817–823. doi:10.1080/0142159X.2021.1928619
15. Anderson J, Walsh J, Anderson M, Burnley R. Patient satisfaction with remote consultations in a primary care setting. Cureus. 2021;13(9):e17814. doi:10.7759/cureus.17814
16. Amin S, Chin J, Terrell MA, Lomiguen CM. Addressing challenges in humanistic communication during COVID-19 through medical education. Front Commun. 2021;6. doi:10.3389/fcomm.2021.619348
17. The state of video in education 2015 – a Kaltura report. Available from: https://site.kaltura.com/rs/984-SDM-859/images/The_State_of_Video_in_Education_2015_a_Kaltura_Report.pdf.
18. Ghazi-Saidi L, Criffield A, Kracl CL, McKelvey M, Obasi SN, Vu P. Moving from face-to-face to remote instruction in a higher education institution during a pandemic: multiple case studies. Int J Technol Educ Sci. 2020;4(4):370–383. doi:10.46328/ijtes.v4i4.169
19. Findyartini A, Anggraeni D, Husin JM, Greviana N. Exploring medical students’ professional identity formation through written reflections during the COVID-19 pandemic. J Public Health Res. 2020;9(Suppl 1):1918. PMID: 33409249; PMCID: PMC7771024. doi:10.4081/jphr.2020.1918
20. Cruess RL, Cruess SR, Boudreau JD, Snell L, Steinert Y. A schematic representation of the professional identity formation and socialization of medical students and residents: a guide for medical educators. Acad Med. 2015;90(6):718–725. doi:10.1097/ACM.0000000000000700
21. Tempski P, Arantes-Costa FM, Kobayasi R, et al. Medical students’ perceptions and motivations during the COVID-19 pandemic. PLoS One. 2021;16(3):e0248627. doi:10.1371/journal.pone.0248627
22. Miller DG, Pierson L, Doernberg S. The role of medical students during the COVID-19 pandemic. Ann Intern Med. 2020;173(2):145–146. doi:10.7326/M20-1281
23. Mai Y, Wu YJ, Huang Y. What type of social support is important for student resilience during COVID-19? A latent profile analysis. Front Psychol. 2021;12:646145. doi:10.3389/fpsyg.2021.646145
24. Drury J, Cocking C, Reicher S. The nature of collective resilience: survivor reactions to the 2005 London bombings. Int J Mass Emerg Disaster. 2009;27(1):66–95. doi:10.1177/028072700902700104
25. Armon S, Benyamini Y, Grisaru-Granovsky S, Avitan T. Online obstetrics and gynecology medical students clerkship during the COVID-19 pandemic: a pilot study [published online ahead of print, 2021 Jan 9]. Med Sci Educ. 2021;31(2):1–5. doi:10.1007/s40670-020-01181-y
26. Abele AE, Wojciszke B. Introduction: the big two of agency and communion as an overarching framework in psychology. In: Abele AE, Wojciszke B, editors. Agency and Communion in Social Psychology. Abingdon, UK: Routledge.p.5. Routledge; 2018. doi:10.4324/9780203703663
27. Dawnay G. Is this really doctoring? Brit J Gen Pract. 2020;70(698):455. doi:10.3399/bjgp20X712445
28. Kitai E, Kushnir T, Herz M, Melamed S, Vigiser D, Granek M. Correlation of work structure and job satisfaction among Israeli family physicians. Israel Med Assoc J. 1999;1:236–240.
29. Papapanou M, Routsi E, Tsamakis K, et al. Medical education challenges and innovations during COVID-19 pandemic. Postgrad Med J. 2021;29. doi:10.1136/postgradmedj-2021-140032
30. Zheng M, Bender D, Lyon C. Online learning during COVID-19 produced equivalent or better student course performance as compared with pre-pandemic: empirical evidence from a school-wide comparative study. BMC Med Educ. 2021;21(1):495. doi:10.1186/s12909-021-02909-z
31. Levine MP. Role models’ influence on medical students’ professional development. AMA J Ethics. 2015;17(2):142–146. doi:10.1001/virtualmentor.2015.17.2.jdsc1-1502
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medical Students’ Perceptions Towards Online Teaching During the Covid-19 Pandemic: A Cross-Sectional Study from Saudi Arabia
Dergham P, Saudagar FNI, Jones-Nazar CC, Hashim SA, Saleh K, Mohammedhussain AA, Wafai SA, Madadin M
Advances in Medical Education and Practice 2023, 14:407-419
Published Date: 23 April 2023
Assessment of Factors That Students Perceive to Affect Their Virtual Learning of Clinical Skills for OSCE
Peramuna Gamage M, Baskaran R, Mukhopadhyay S, Dalavaye N, Leveridge B, Ganesananthan S, Spencer R, Manivannan S, Zaben M
Advances in Medical Education and Practice 2023, 14:707-712
Published Date: 7 July 2023