Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Peripheral Blood IL-6 and STAT3 Gene Expression as Biomarkers Associated with Neoadjuvant Chemotherapy Response in Triple-Negative Breast Cancer: A Prospective Cross-Sectional Study
Authors Özdemir K, Muhtaroğlu A ![]() , Kamburoğlu MB, Guney Eskiler G
, Kamburoğlu MB, Guney Eskiler G ![]() , Özman Gökçe Z, Kocer B
, Özman Gökçe Z, Kocer B
Received 1 January 2026
Accepted for publication 26 March 2026
Published 8 April 2026 Volume 2026:18 593138
DOI https://doi.org/10.2147/BCTT.S593138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert Clarke
Kayhan Özdemir,1 Ali Muhtaroğlu,2 Muhammet Burak Kamburoğlu,3 Gamze Guney Eskiler,4 Zeynep Özman Gökçe,5 Belma Kocer6
1Department of General Surgery, Sakarya University Faculty of Medicine, Sakarya, Turkey; 2Department of General Surgery, Giresun University Faculty of Medicine, Giresun, Turkey; 3Department of General Surgery, Derince Training and Research Hospital, Kocaeli, Turkey; 4Department of Medical Biology, Sakarya University Faculty of Medicine, Sakarya, Turkey; 5Department of Medical Biochemistry, Bezmialem University Faculty of Medicine, İstanbul, Turkey; 6General Surgery Clinic, Private Beyhekim Hospital, Sakarya, Turkey
Correspondence: Ali Muhtaroğlu, Department of General Surgery, Giresun University Training and Research Hospital, Aksu District, Mehmet Izmen Street, Number: 145, Giresun, PC, 28100, Turkey, Tel +90 506 314 64 41, Fax +90 454 310 20 02, Email [email protected]
Purpose: Triple-negative breast cancer (TNBC) is an aggressive breast cancer subtype with limited targeted treatment options. Blood-based biomarkers that might help predict response to neoadjuvant chemotherapy (NAC) remain lacking. We examined whether pre-treatment peripheral blood expression of interleukin-6 (IL-6) and signal transducer and activator of transcription 3 (STAT3) was associated with clinicopathological features and NAC response in TNBC.
Methods: This prospective cross-sectional study included 20 patients with TNBC and 10 healthy controls. Whole-blood RNA was isolated using Trizol, reverse-transcribed to cDNA, and analysed by RT-qPCR with TaqMan® Gene Expression Assays. Relative expression was calculated with the Livak (2−ΔΔCT) method using GAPDH as the housekeeping gene. Clinicopathological variables and pathological response assessed by the Miller–Payne system were analysed using IBM SPSS Statistics 23.0.
Results: Compared with the control group, IL-6 and STAT3 expression levels were significantly elevated in patients with TNBC by 8.9-fold (p=0.001) and 25.1-fold (p=0.001), respectively. Higher levels of IL-6 and STAT3 expression were associated with adverse pathological features, including lymphovascular invasion, poor tumour differentiation, and reduced rates of complete pathological response. ROC analysis showed modest discriminatory performance for both markers. The AUC for IL‑6 was 0.68 (95% CI: 0.50– 0.86) and for STAT3 was 0.72 (95% CI: 0.53– 0.91).
Conclusion: In this pilot cohort, higher peripheral blood IL-6 and STAT3 expression was associated with unfavourable clinicopathological features in TNBC. These findings suggest that the IL-6/STAT3 axis may have value within broader predictive biomarker panels, although larger prospective studies are needed before any clinical application is considered.
Keywords: triple-negative breast cancer, IL-6, STAT3, gene expression, neoadjuvant chemotherapy, prognostic markers
Introduction
Breast cancer is the most commonly diagnosed malignancy worldwide and remains a leading cause of cancer-related mortality among women. Triple-negative breast cancer (TNBC), characterised by the absence of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) expression, constitutes approximately 10–20% of all breast cancers. The aggressive behaviour exhibited by patients, their relative youth at the time of diagnosis, and the elevated recurrence and metastasis rates that are characteristic of this condition all serve to underscore the poor prognosis that is frequently associated with TNBC.1,2
The biology of TNBC is distinct, displaying substantial molecular heterogeneity, genomic instability, and mutations in key signalling pathways associated with proliferation, invasion, and resistance to chemotherapy.3 Diagnostic approaches involve clinical evaluation, imaging (eg, mammography, ultrasound, MRI), and histopathological confirmation through biopsy and immunohistochemical analysis to establish receptor status.4
The aetiopathogenesis of cancer, including TNBC, is complex, multifactorial, and increasingly recognised as linked to chronic inflammatory processes. The secretion of cytokines and chemokines by chronic inflammation has been demonstrated to facilitate tumourigenesis by promoting a pro-tumoral microenvironment.5 Among these inflammatory mediators, interleukin-6 (IL-6) has emerged as a crucial cytokine involved in tumour progression, immune regulation, and metastasis.6,7
At the cellular level, IL-6 binds to its receptor IL-6R-alpha (GP80), forming a complex with the co-receptor GP130. The activation of this complex results in the phosphorylation and subsequent activation of signal transducer and activator of transcription 3 (STAT3). Following activation, STAT3 translocates to the nucleus, thereby triggering transcription of genes involved in cell survival, proliferation, invasion, and metastasis (Figure 1).8,9 STAT3, in particular, has garnered significant attention due to its constitutive activation in various malignancies, including breast cancer. Aberrant STAT3 signalling has been linked to resistance to chemotherapy, promotion of epithelial–mesenchymal transition (EMT), tumour immune escape, and poor clinical outcomes. In TNBC, persistent activation of the IL-6/STAT3 axis may contribute to the aggressive phenotype and reduced response to conventional treatments.10,11
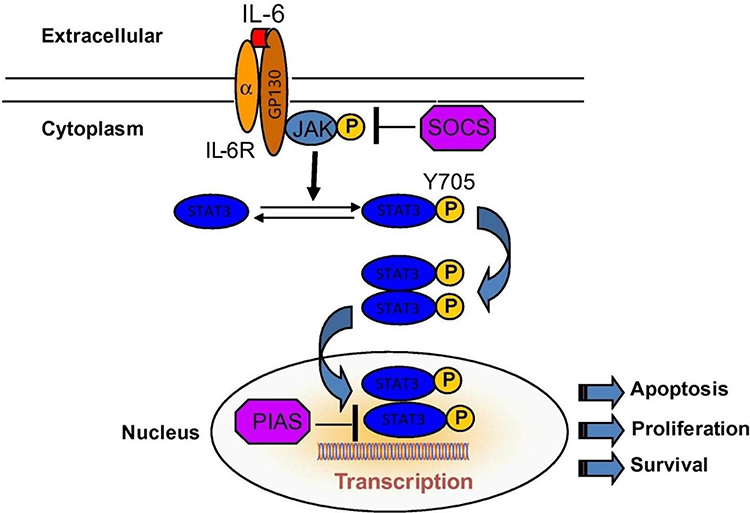 |
Figure 1 Schematic representation of the IL-6/JAK/STAT3 signalling pathway. IL-6 binds to IL-6R and GP130, activates JAK, and promotes phosphorylation of STAT3 at Tyr705. Phosphorylated STAT3 dimerises and translocates to the nucleus, where it regulates transcription of genes involved in apoptosis, proliferation, and survival. SOCS and PIAS act as negative regulators of the pathway.9 |
Although most previous studies have focused on protein expression within tumour tissue, blood-based assays may offer a clinically practical and minimally invasive approach for evaluating systemic inflammatory signalling. However, data on peripheral IL-6 and STAT3 gene expression in TNBC remain limited. We therefore hypothesised that higher pre-treatment peripheral IL-6 and STAT3 expression would be associated with adverse clinicopathological characteristics and poorer pathological response to NAC in TNBC. The aim of this study was to assess IL-6 and STAT3 gene expression levels in peripheral blood samples obtained before NAC and to examine their association with clinicopathological features and Miller–Payne response categories.
Methods
Study Design and Participants
This prospective cross-sectional study was conducted following the approval of the Ethics Committee of Sakarya University Faculty of Medicine (Approval No: 71522473/050.01.04/30). Written informed consent was obtained from all participants. This study was conducted on the relevant ethical principles of the Declaration of Helsinki, revised in 2013.
A total of 20 patients diagnosed with triple-negative breast cancer and a control group of 10 healthy individuals were included in the study. TNBC diagnosis was confirmed by histopathological evaluation and immunohistochemical staining demonstrating negative ER, PR, and HER2 status. To minimise biological variability and potential confounding, participants with any of the following conditions were excluded: active infection; autoimmune or chronic inflammatory disease; recent vaccination (within 4 weeks); or current use of corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), or other immunomodulatory medications.
Sample Collection, RNA Isolation, and RT-qPCR
Peripheral blood samples (5 mL) were collected in EDTA-coated tubes from all participants before treatment initiation. To minimise pre-analytical variation, all samples were obtained after overnight fasting, between 08:00 and 10:00 AM, and processed within 2 hours of collection. Whole blood was used as the sample matrix. Total RNA was isolated using the Trizol reagent method (Invitrogen, USA) according to the manufacturer’s instructions. Following homogenization, 200 µL of chloroform was added to each sample, and the mixture was centrifuged at 12,000 rpm for 15 minutes at 4°C. The aqueous phase containing RNA was collected. RNA quantity was measured using a Qubit 4.0 Fluorometer (Invitrogen, USA), and purity was verified by A260/A280 absorbance ratios of 1.8–2.0. All samples underwent DNase I treatment to eliminate potential contamination with genomic DNA.
Complementary DNA (cDNA) was synthesised from 1 µg of total RNA using the High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems™, Thermo Fisher Scientific, USA), following the manufacturer’s protocol. Synthesised cDNA was stored at –20 °C until analysis. Quantitative real-time PCR (RT-qPCR) was performed using the TaqMan® Gene Expression Assay system (Thermo Fisher Scientific, USA) on a QuantStudio 5 Real-Time PCR System (Applied Biosystems, USA). The following assays were used: IL-6 (Hs00174131_m1), STAT3 (Hs00374280_m1), and GAPDH (Hs02786624_g1). Primer/probe assay IDs, annealing temperature, and amplification efficiency data are provided in Supplementary Table 1.
Each reaction (20 µL total volume) consisted of 10 µL of TaqMan Universal PCR Master Mix, 1 µL of TaqMan Gene Expression Assay, 1 µL of cDNA template, and 8 µL of nuclease-free water. The thermal cycling conditions were as follows: 50°C for 2 minutes, 95°C for 10 minutes, followed by 40 cycles of 95°C for 15 seconds and 60°C for 1 minute. All samples were analysed in triplicate. Technical replicates with a Ct standard deviation > 0.3 were excluded from analysis. Amplification efficiencies for each assay were assessed using standard curves and ranged from 95% to 105%. Relative expression levels of IL-6 and STAT3 were calculated using the 2−ΔΔCt (Livak) method. GAPDH served as the internal control. The calibrator was defined as the mean expression level of the healthy control group. Fold changes were calculated by comparing the ΔCt values of TNBC patients with those of the calibrator group. All ΔCt values were confirmed to be normally distributed before the analysis.
Clinicopathological Evaluation
Clinical variables, including age, tumour size, TNM stage, lymph node status, and lymphovascular invasion, were obtained from medical records. Histological grading was performed according to the Bloom–Richardson system.
Pathological response to NAC was assessed using the Miller–Payne grading system by comparing tumour cellularity in pre-treatment core biopsy specimens and post-treatment surgical specimens. Grade 1 indicated no meaningful change; Grade 2, up to 30% reduction in tumour cells; Grade 3, 30–90% reduction; Grade 4, greater than 90% reduction; and Grade 5, no identifiable malignant cells in the tumour bed (pathologic complete response). For analysis, Grades 4–5 were classified as responders and Grades 1–3 as non-responders.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 23.0. Descriptive statistics were expressed as means, medians, standard deviations, and frequencies, as appropriate. Before all analyses, data normality was tested using the Shapiro–Wilk test. For variables not conforming to a normal distribution, non‑parametric tests (eg, Mann–Whitney U-test) were employed; otherwise, parametric tests were used. To evaluate the potential for false‑positive findings in multiple comparisons, a Bonferroni correction was applied to the significance level when appropriate. A p‑value < 0.05 was considered statistically significant after adjustment. Outlier detection was performed using the 1.5×IQR rule, and identified outliers were excluded from final analyses. There was no missing data in the dataset. A power analysis was conducted using G*Power 3.1. Assuming an effect size of a 2‑fold difference in gene expression (standard deviation = 1.5), α = 0.05, and power n1–β) = 0.80, a minimum of 18 subjects per group was required. The TNBC cohort met this requirement, supporting the feasibility of a pilot analysis; however, the findings are interpreted as preliminary due to the smaller control group. Because of the limited sample size and sparse subgroup counts, no multivariable regression models or formal sensitivity analyses were performed, and all analyses were interpreted as exploratory. Receiver Operating Characteristic (ROC) analysis was used to assess the discriminatory performance of IL‑6 and STAT3 expression in distinguishing TNBC patients from healthy controls and exploring their association with chemotherapy response. Area under the curve (AUC) values were calculated, along with 95% confidence intervals (CI), using a non-parametric method (DeLong). Sensitivity and specificity values were determined for optimal threshold points based on Youden’s index.
Results
The study included 20 patients with triple-negative breast cancer (TNBC) and 10 healthy control individuals. The mean age of the TNBC group was 44.2 years (range, 31–57 years). Clinical characteristics of the TNBC patients, including tumour size, TNM stage, lymph node status, lymphovascular invasion, histologic grade, and response to neoadjuvant chemotherapy, are summarised in Table 1.
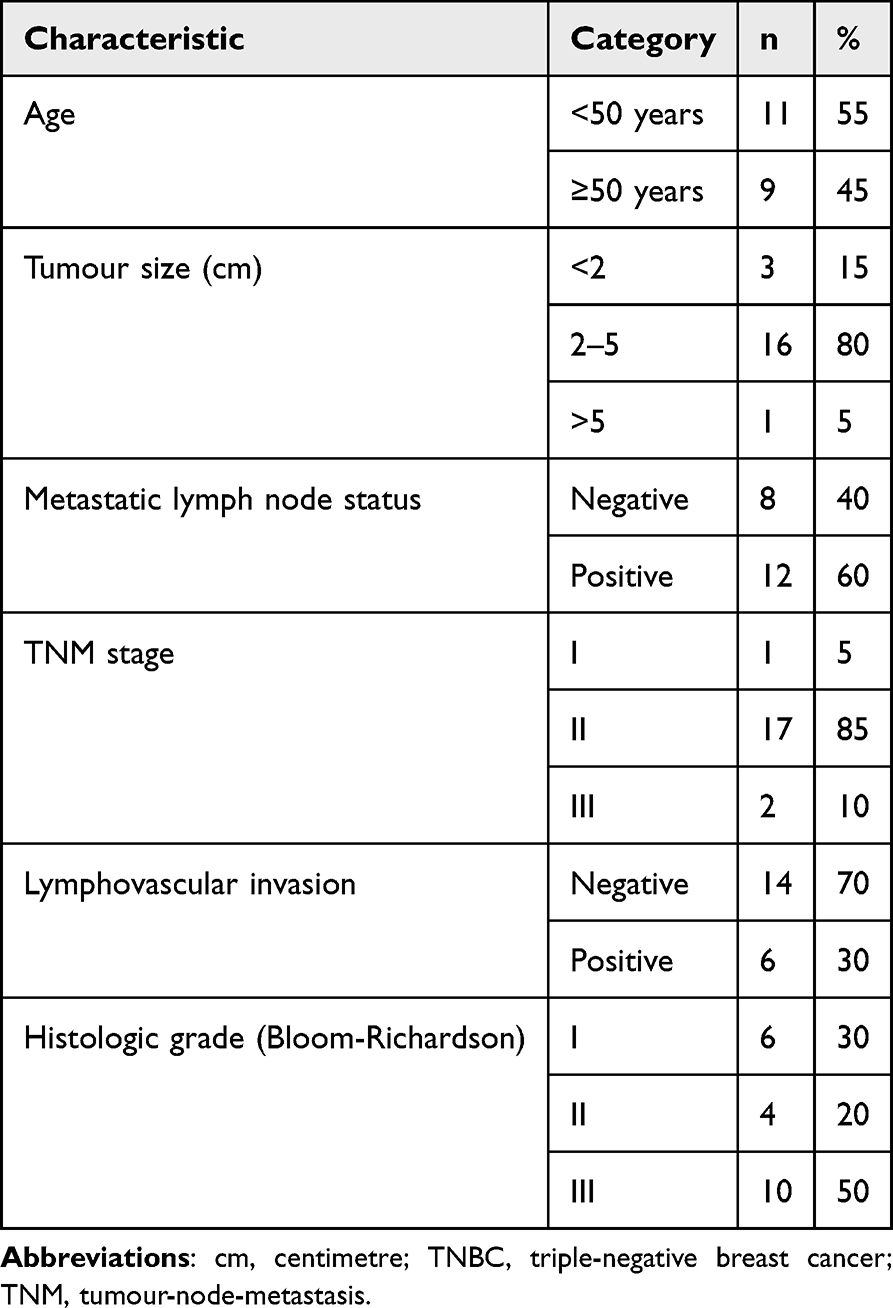 |
Table 1 Baseline Clinicopathological Characteristics of Patients with TNBC (n=20) |
Real-time PCR analysis revealed significantly elevated expression of both IL-6 and STAT3 in the TNBC group compared with healthy controls. The mean fold increase for IL-6 was 8.9-fold (p=0.001), and for STAT3 was 25.1-fold (p=0.001), based on the 2−ΔΔCt method (Figure 2).
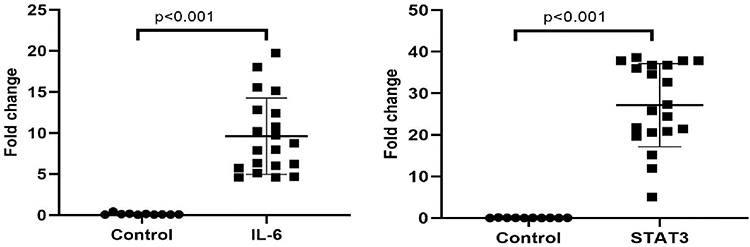 |
Figure 2 Relative peripheral blood IL-6 and STAT3 expression in the TNBC and control groups. Circles indicate healthy controls (n=10), and squares indicate patients with TNBC (n=20). Expression levels are shown as fold-change values calculated by the 2−ΔΔCt method. Horizontal bars represent mean ± SD. p values denote between-group comparisons. |
The distribution of Miller-Payne grades following neoadjuvant chemotherapy is shown in Figure 3: grade 1 in 2 patients, grade 2 in 5 patients, grade 3 in 7 patients, grade 4 in 4 patients, and grade 5 in 2 patients. Patients exhibiting a better pathological response generally demonstrated lower levels of IL-6 and STAT3 expression.
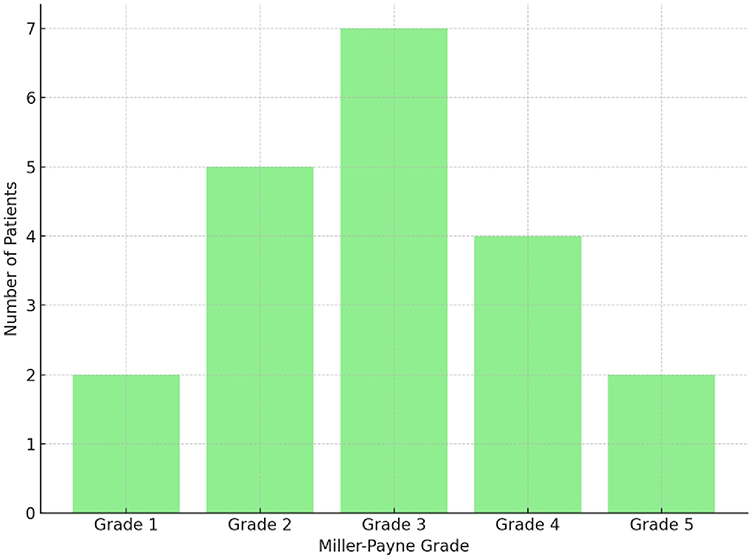 |
Figure 3 Distribution of patients with TNBC according to Miller-Payne grade after neoadjuvant chemotherapy (n=20). Bars represent the number of patients in each Miller-Payne category. |
In exploratory subgroup analyses, elevated expression levels of both markers were significantly correlated with lymphovascular invasion and poorer tumour differentiation. Additionally, higher IL-6 expression was associated with the absence of a complete response, whereas the association between STAT3 expression and response did not achieve statistical significance (Table 2). No significant associations were observed between these markers and factors such as age, tumour size, metastatic lymph node status, or TNM stage.
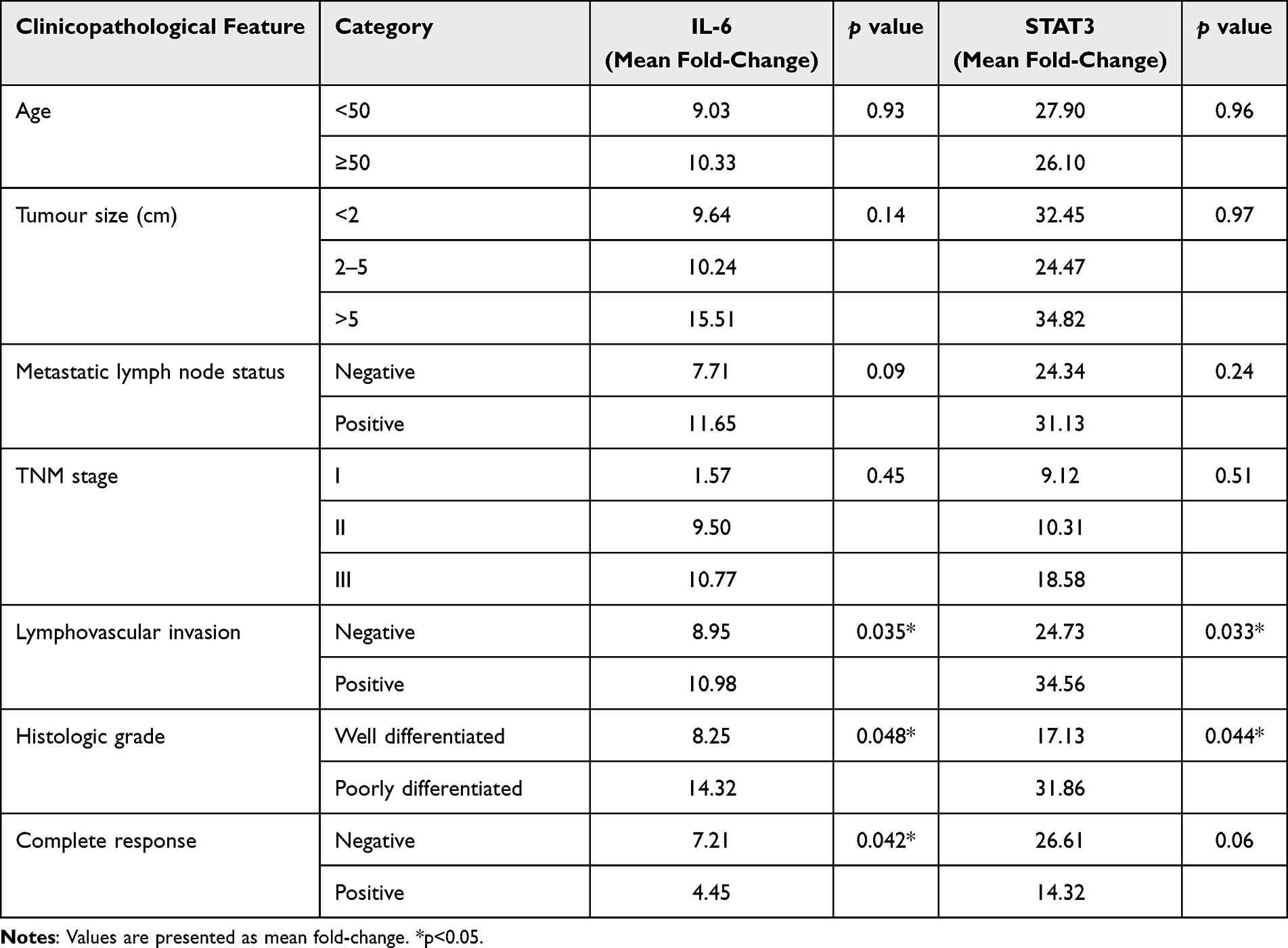 |
Table 2 Association Between IL-6 and STAT3 Expression and Clinicopathological Features in TNBC (n=20) |
Receiver operating characteristic analysis suggested modest discriminatory performance for both genes. For IL-6, the AUC was 0.721 (95% CI 0.524–0.918; p=0.084), with an optimal cut-off value of 6.32, 68% sensitivity, and 52% specificity. For STAT3, the AUC was 0.683 (95% CI 0.476–0.889; p=0.16), with an optimal cut-off value of 9.23, 62% sensitivity, and 56% specificity (Figure 4).
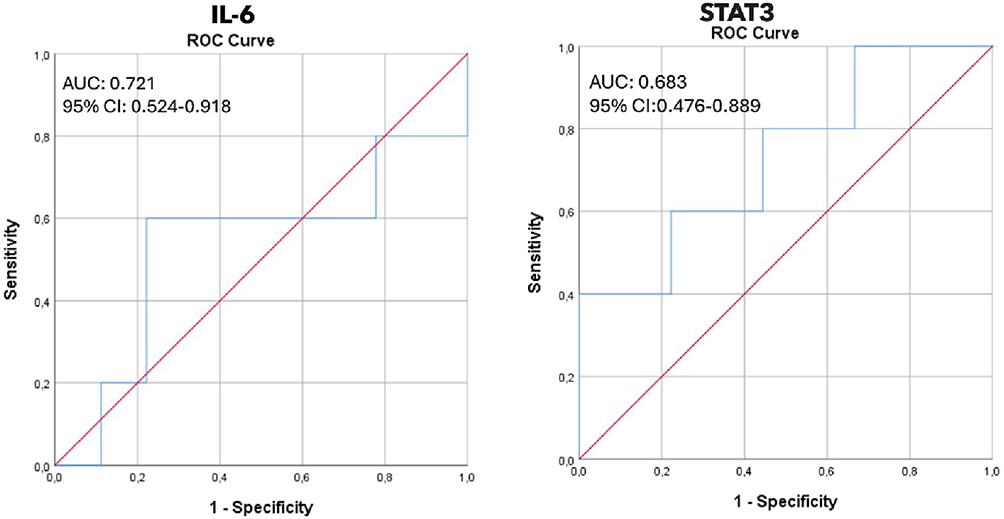 |
Figure 4 Receiver operating characteristic curves for IL-6 and STAT3 expression in distinguishing TNBC cases from healthy controls. The blue line represents the observed ROC curve, and the red diagonal line represents the line of no discrimination (AUC=0.50). AUC values and 95% confidence intervals are shown within each panel. |
When clinicopathological variables were evaluated according to these threshold values, IL-6 expression above 6.32 was associated with higher TNM stage and absence of complete response. No statistically significant threshold-based association was observed for STAT3 in this exploratory analysis (Table 3).
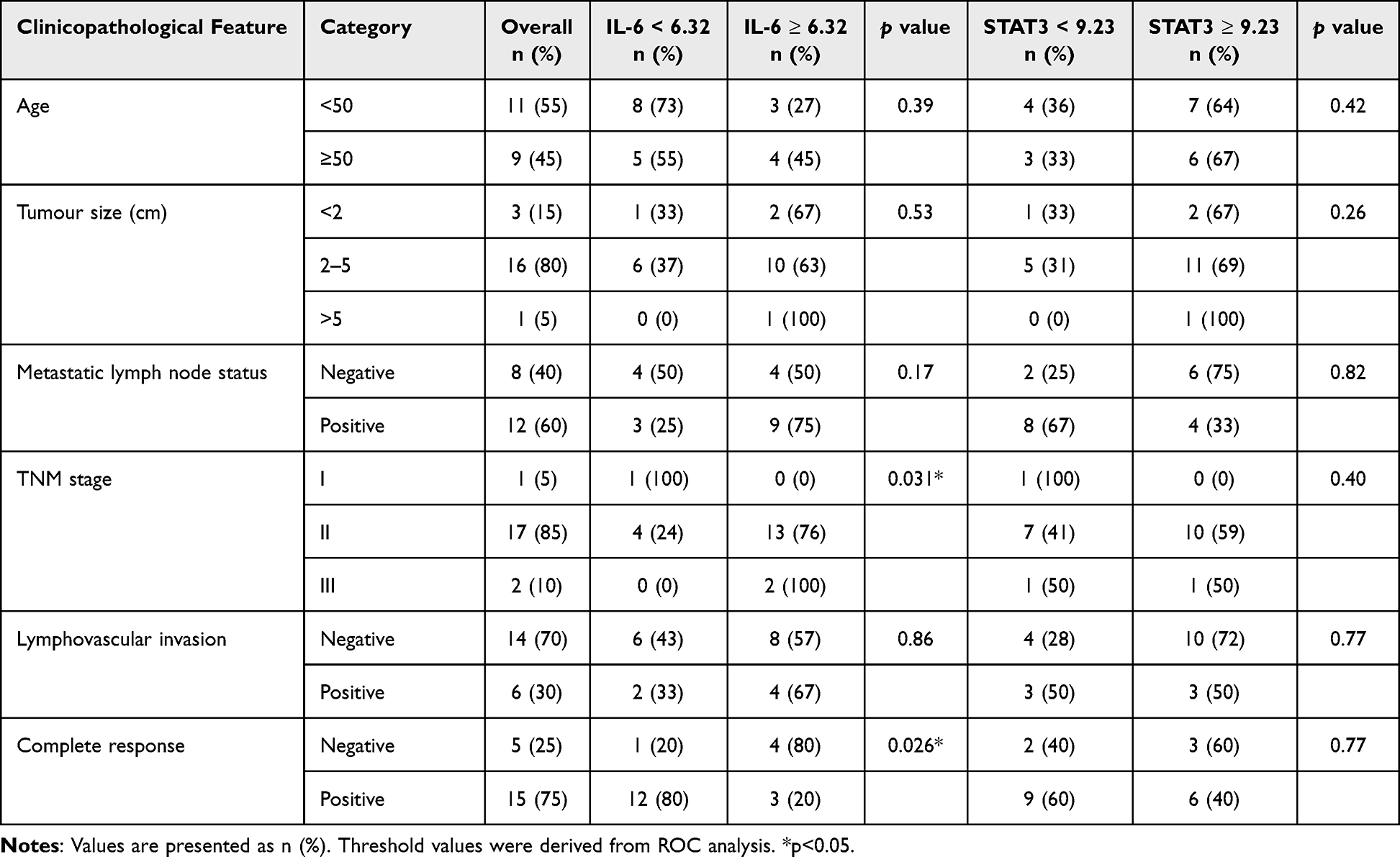 |
Table 3 Distribution of Clinicopathological Features According to IL-6 and STAT3 Threshold Values |
Discussion
Several conclusions can be drawn from this study. Firstly, the expression levels of IL-6 and STAT3 in peripheral blood were significantly elevated in patients with TNBC compared to healthy controls. Secondly, higher expression levels were associated with pathological features indicative of more aggressive disease, notably lymphovascular invasion and poorly differentiated tumours. Thirdly, the correlation with treatment response was more pronounced for IL-6 than for STAT3 within this cohort, although ROC analysis demonstrated only modest discriminatory capacity overall.
These findings are biologically plausible and align closely with existing knowledge regarding the IL-6/STAT3 axis. IL-6 plays a role in fostering a pro-inflammatory tumour microenvironment and has been linked to processes such as epithelial-mesenchymal transition, immune evasion, angiogenesis, and metastatic progression.12–15 STAT3, as a downstream transcription factor, regulates genes involved in proliferation, survival, and invasion and has repeatedly been linked to treatment resistance and poor outcome in breast cancer.10,11,16,17 Our data do not establish causation, but they do suggest that peripheral blood expression of these genes may reflect the same aggressive biology described in tissue-based and experimental studies.
The present study does not assert a significant conceptual breakthrough. Instead, it provides preliminary clinical evidence derived from a minimally invasive sampling methodology. While much of the existing research has concentrated on tumour tissue or protein expression, this study investigates pre-treatment peripheral blood gene expression to assess whether a more practical biomarker source can still yield clinically relevant information. The modest area under the curve values suggest that IL-6 and STAT3 are unlikely to serve effectively as standalone diagnostic markers. If their utility is confirmed, it is more probable that they would contribute value within multi-marker models or in combination with established clinicopathological variables.
From a translational perspective, the IL-6/STAT3 axis remains an appealing target because it sits at the intersection of inflammatory signalling and treatment resistance. Experimental and early clinical studies have suggested that agents targeting IL-6, the IL-6 receptor, or STAT3 may help reduce stemness, chemoresistance, and metastatic behaviour in TNBC.18–20 Our findings are consistent with that direction of research, but they should not be interpreted as evidence that either marker is ready for clinical decision-making.
Future investigations should assess these markers within larger prospective cohorts, preferably incorporating paired tumour tissue and blood samples, along with longitudinal sampling during treatment and monitoring of survival outcomes. Validation at the protein level, such as through ELISA-based measurement of circulating IL-6, would further elucidate the relationship between transcriptional alterations and biologically relevant protein activity. If validated, such research could contribute to the refinement of biomarker panels designed to identify patients at increased risk of an insufficient response to neoadjuvant chemotherapy.
Study Limitations
This study has several limitations that must be acknowledged to provide context for interpreting the findings. First and foremost, the relatively small sample size limits the statistical power of the analyses and the generalisability of the results. This limitation is particularly pronounced in subgroup analyses, where certain clinical categories—such as patients with tumour size >5 cm—contained only a single case, thereby restricting the ability to detect meaningful differences. Accordingly, the findings should be regarded as preliminary and underscore the need for validation in larger, independent cohorts with more balanced clinical subgroup distributions.
Secondly, the cross-sectional study design and the lack of longitudinal follow-up data preclude drawing definitive conclusions about the causal relationship between elevated IL-6/STAT3 expression and long-term clinical outcomes, such as overall or disease-free survival. Future prospective studies with serial sampling and survival endpoints are essential to further elucidate the prognostic significance of these molecular markers in the context of triple-negative breast cancer.
A further limitation lies in the exclusive use of peripheral blood samples for gene expression analysis. While peripheral blood sampling is minimally invasive and clinically feasible, it may not fully capture the complex molecular landscape and cellular heterogeneity of the tumour microenvironment. Blood-based expression primarily reflects systemic immune activity and inflammatory status rather than tumour-intrinsic gene expression patterns. This methodological choice may, in part, account for the moderate diagnostic performance observed in the ROC analyses. Incorporating paired tumour tissue samples into future research would provide a more comprehensive understanding of the pathophysiological roles of IL-6 and STAT3 in TNBC and enhance the interpretability of biomarkers.
Despite applying exclusion criteria and standardised sample handling protocols—including fasting blood collection within a fixed time window and processing within two hours—to mitigate pre-analytical and biological confounding, the potential for residual confounding remains. Subclinical inflammation, undiagnosed comorbidities, psychosocial stress, or the use of unreported medications (such as NSAIDs or corticosteroids) could still influence cytokine expression levels. This inherent limitation is common in observational biomarker studies and should be considered when interpreting the observed associations between IL-6/STAT3 expression and neoadjuvant chemotherapy response.
Conclusion
In this prospective cross-sectional pilot study, higher pre-treatment peripheral blood IL-6 and STAT3 expression were associated with unfavourable clinicopathological features in TNBC, and IL-6 in particular showed an association with poorer pathological response to neoadjuvant chemotherapy. These findings support further study of the IL-6/STAT3 axis as part of broader biomarker strategies associated with treatment response. Larger, well-powered prospective studies are needed before these markers can be considered for routine clinical use.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available due to participant confidentiality reasons. Still, they are available as an anonymised aggregate format from the corresponding author on reasonable request.
Ethical Considerations
This prospective cross-sectional study was conducted following the approval of the Ethics Committee of Sakarya University Faculty of Medicine (Approval No: 71522473/050.01.04/30). Written informed consent was obtained from all participants. This study was conducted on the relevant ethical principles of the Declaration of Helsinki, revised in 2013.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no conflicts of interest to declare that are relevant to the content of this article.
References
1. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938–10. doi:10.1056/NEJMra1001389
2. Denkert C, Liedtke C, Tutt A, von Minckwitz G. Molecular alterations in triple-negative breast cancer-the road to new treatment strategies. Lancet. 2017;389(10087):2430–2442. doi:10.1016/S0140-6736(16)32454-0
3. Bianchini G, Balko JM, Mayer IA, Sanders ME, Gianni L. Triple-negative breast cancer: challenges and opportunities of a heterogeneous disease. Nat Rev Clin Oncol. 2016;13(11):674–690. doi:10.1038/nrclinonc.2016.66
4. Rakha EA, Reis-Filho JS, Ellis IO. Basal-like breast cancer: a critical review. J Clin Oncol. 2008;26(15):2568–2581. doi:10.1200/JCO.2007.13.1748
5. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
6. Kumari N, Dwarakanath BS, Das A, Bhatt AN. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumour Biol. 2016;37(9):11553–11572. doi:10.1007/s13277-016-5098-7
7. Guo Z, Zhang H, Fu Y, et al. Cancer-associated fibroblasts induce growth and radioresistance of breast cancer cells through paracrine IL-6. Cell Death Discov. 2023;9(1):6. doi:10.1038/s41420-023-01306-3
8. Johnson DE, O’Keefe RA, Grandis JR. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat Rev Clin Oncol. 2018;15(4):234–248. doi:10.1038/nrclinonc.2018.8
9. Guo Y, Xu F, Lu T, Duan Z, Zhang Z. Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat Rev. 2012;38(7):904–910. doi:10.1016/j.ctrv.2012.04.007
10. Yu H, Lee H, Herrmann A, Buettner R, Jove R. Revisiting STAT3 signalling in cancer: new and unexpected biological functions. Nat Rev Cancer. 2014;14(11):736–746. doi:10.1038/nrc3818
11. Morrow E, Pennel K, Hatthakarnkul P, et al. High expression of STAT3 within the tumour-associated stroma predicts poor outcome in breast cancer patients. Cancer Med. 2023;12(12):13225–13240. doi:10.1002/cam4.6014
12. Siersbæk R, Scabia V, Nagarajan S, et al. IL6/STAT3 signaling hijacks estrogen receptor α enhancers to drive breast cancer metastasis. Cancer Cell. 2020;38(3):412–423.e9. doi:10.1016/j.ccell.2020.06.007
13. Chen J, Wei Y, Yang W, et al. IL-6: the link between inflammation, immunity and breast cancer. Front Oncol. 2022;12:903800. doi:10.3389/fonc.2022.903800
14. Castro-Espin C, Cairat M, Navionis AS, et al. Prognostic role of pre-diagnostic circulating inflammatory biomarkers in breast cancer survival: evidence from the EPIC cohort study. Br J Cancer. 2024;131(9):1496–1505. doi:10.1038/s41416-024-02858-6
15. Manore SG, Doheny DL, Wong GL, Lo HW. IL-6/JAK/STAT3 signaling in breast cancer metastasis: biology and treatment. Front Oncol. 2022;12:866014. doi:10.3389/fonc.2022.866014
16. Wen Y, Zhu Y, Zhang C, et al. Chronic inflammation, cancer development and immunotherapy. Front Pharmacol. 2022;13:1040163. doi:10.3389/fphar.2022.1040163
17. Liu J, Lin PC, Zhou BP. Inflammation fuels tumor progress and metastasis. Curr Pharm Des. 2015;21(21):3032–3040. doi:10.2174/1381612821666150514105741
18. Lee CH, Park SY, Lee JS, et al. MSN/STAT3 drives cancer stemness and chemoresistance via IL-6/LPAR1 ligand receptor complex in triple-negative breast cancer. Breast Cancer Res. 2025;27(1):136. doi:10.1186/s13058-025-02072-z
19. Berger K, Persson E, Gregersson P, et al. Interleukin-6 induces stem cell propagation through liaison with the sortilin-progranulin axis in breast cancer. Cancers. 2023;15(24):5757. doi:10.3390/cancers15245757
20. Chang Q, Bournazou E, Sansone P, et al. The IL-6/JAK/Stat3 feed-forward loop drives tumorigenesis and metastasis. Neoplasia. 2013;15(7):848–862. doi:10.1593/neo.13706
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Based on the Dual Pathway of Interaction-Mediated NF-κB in Cell Apoptosis and Immune Inflammation to Study the Effect of Danzhi Xiaoyao Powder on the Learning and Cognitive Ability of AD Model Rats
Wang HP, Li MC, Yang J, Zhou J, Meng ZP, Hu YY, Lyu YJ, Chen YQ, Han YM, Pei WL
Degenerative Neurological and Neuromuscular Disease 2025, 15:41-64
Published Date: 14 April 2025
A Randomized Controlled Pilot Study Evaluating the Safety and Efficacy of Nifuroxazide in Patients with Ulcerative Colitis
AlRasheed HA, Abdallah MS, El-Khateeb E, Kamal M, Alrubia S, Alsegiani AS, Ahmed TI, Bahaa MM
Drug Design, Development and Therapy 2025, 19:5539-5552
Published Date: 30 June 2025
Development and Validation of a New Immune-Inflammatory-Nutritional Score to Predict Pathological Complete Response in Triple-Negative Breast Cancer Undergoing Neoadjuvant Chemotherapy: A Two-Center Study
Wang S, Song Y, Ding J, Li M, Wang Y, Bai Y, Zi H, Sun J, Fan C, Chen H, Luo T, Wang T
Journal of Inflammation Research 2025, 18:9365-9378
Published Date: 16 July 2025
Exploring Carbon Dot Nanoparticles for Imaging and Cellular Interaction in Triple-Negative Breast Cancer
Bahadorani M, Wu K, Wei J, Zadegan R
International Journal of Nanomedicine 2025, 20:14823-14835
Published Date: 9 December 2025