Back to Journals » International Journal of General Medicine » Volume 16
Patterns of Prescribing Postoperative Analgesic Medication After Thyroid Surgery: A Retrospective Cohort Study
Authors Alzahrani HA ![]()
Received 24 December 2022
Accepted for publication 26 January 2023
Published 2 February 2023 Volume 2023:16 Pages 405—410
DOI https://doi.org/10.2147/IJGM.S401828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Mihajlo Jakovljevic
Hassan A Alzahrani
Department of Surgery, College of Medicine, King Khalid University, Abha, Saudi Arabia
Correspondence: Hassan A Alzahrani, Email [email protected]
Background: Mild-to-moderate postoperative pain is common after surgical procedures of the thyroid. Opioid analgesics have been commonly prescribed in such cases, but their use has been debated owing to concerns regarding the addictive nature of opioids. Recently, experts from the Endocrine Surgery Section of the American Head and Neck Society released a consensus document to limit the use of opioids as the first-line pain control medication after head and neck or endocrine procedures. However, differences in pain management prescriptions have been noted in many settings. This study aims to assess the post-thyroid surgery pain control medication prescription practices of head and neck and endocrine surgeons.
Methods: This study retrospectively reviewed the charts of 105 adult patients who underwent thyroid surgery (total thyroidectomy, thyroid lobectomy, or subtotal thyroidectomy) by head and neck or endocrine surgeons. The type of prescribed pain medication at hospital discharge postoperatively was then retrieved from each patient’s discharge medication list. Descriptive statistics mean, standard deviations, frequencies, and percentages were computed, while the Chi-square test was applied to measure the significant differences among variables at a 5.00% significant level.
Results: An outpatient oral opioid, in the form combining paracetamol and codeine, was prescribed for 62 (59%) patients, whereas 43 (41%) were discharged on paracetamol only.
Conclusion: The use of opioids is the practice pattern for pain management among some head and neck or endocrine surgeons despite emerging evidence that supports the use of non-opioid and other alternative analgesic strategies in outpatient thyroid and parathyroid surgery. Further research and quality improvement interventions should be geared towards leading all health professionals to appropriate prescription practices to improve patient safety and reduce unnecessary opioid prescriptions.
Keywords: thyroid, endocrine, surgery, postoperative, pain medication, opioid, opioid addiction
Background
Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.1 Surgery triggers a wide range of responses in the pain matrix, including pain pathway sensitizations in the peripheral and central nervous systems.2
Postoperative pain management and control are clearly of primary concern to patients, as well as surgeons, to minimize the potential adverse effects associated with the physiological effects of surgery-induced pain. Poor postoperative pain control and increased opioid intake can be predicted by factors such as young age, female gender, smoking, depression, anxiety, use of preoperative analgesia, and type of surgery (major, emergency, or abdominal).3
Several procedures or treatments, such as local anesthetic infiltration, non-opioids, or opioids, were employed for postoperative analgesia. Non-opioids are becoming more widely used in postoperative pain management, either alone or in combination with other analgesics.4
Non-opioid analgesics are classified as acid and non-acid antipyretic drugs. Non-acidic antipyretics (paracetamol and dipyrone) have analgesic and antipyretic properties but are devoid of anti-inflammatory properties while non-steroidal anti-inflammatory drugs (NSAIDs) are acidic antipyretic drugs that extend the bleeding time and were not recommended, historically, for use after thyroid surgery due to the risk of postoperative bleeding.5,6 However, recent evidence has shown no significant increased risk of postoperative hematoma.7
Opioids are classified into illicit opioids, such as heroin, and prescription opioids used as pain relievers, such as oxycodone, codeine, morphine, etc.8 Sedation, dizziness, nausea, vomiting, constipation, physical dependence, tolerance, and respiratory depression are well-known side effects of opioids.9 Patients typically experience mild-to-moderate pain after thyroid surgery.10,11 However, perioperative analgesia strategies after outpatient head and neck surgery (including thyroid surgery) often rely on opioid administration. Additionally, opioid abuse and dependence were significant, wherein 5–7% of patients continue to use opioid medication for up to 6 months after head and neck or endocrine surgery.12,13 Moreover, recent western studies indicate that legally prescribed opioids have resulted in a significantly increased number of deaths over the past two decades.14,15 Shifting to multimodal pain control methods was incorporated to improve the postoperative analgesia quality and minimize opioid use.4,16 Combination of paracetamol, ibuprofen, and tramadol is an example of a multi-modality postoperative pain management regimen.17
In this context, we can say that postoperative pain management practices vary among surgeons worldwide, sometimes with unpleasant consequences. In view of the dearth of similar studies in Saudi Arabia, we have undertaken this study to understand the prescription behavior of head and neck and endocrine surgeons in this regard. The findings of this study will help guide the relevant professional bodies for awareness and capacity building.
Methods
This retrospective cohort study was conducted on all opioid-naive adult patients who underwent thyroid surgery from January 1, 2019, to September 31, 2021. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed.
The study sample included 105 adult patients who underwent total thyroidectomy, thyroid lobectomy, or subtotal thyroidectomy in a private health institute, in southwestern, Saudi Arabia. All adult patients scheduled for elective thyroidectomy under general anesthesia were included in the study. Patients with psychiatric disorders and those taking chronic analgesics were excluded. Age, sex and nationality parameters were determined for all patients.
The field block utilized in all thyroid surgery cases is local wound infiltration of 6–10 mL of 2% lidocaine along the planned incision site.
The type of pain medication prescribed at hospital discharge postoperatively was then retrieved from each patient’s discharge medication list.
Descriptive statistics, frequencies, percentages, arithmetic mean, standard deviation, and 95% confidence intervals (95% CI) for the proportions were computed. The Chi-square test of significance was used to measure the significant differences among variables at a 0.05 significant level. The research followed the declaration of Helsinki’s ethical principles. The research was approved by the research ethics committee of King Khalid University (HAPO-06-B-001; ECM#2021-5913). As the study was retrospective and observational, involved a completely anonymised data and involved no more than minimal risk to subjects, the research ethics committee approved the request to waive the documentation of individual informed consent.
Results
A total of 105 patients underwent outpatient thyroid surgery during the study period. The majority of patients were females (n = 95, 90.5%) and the mean age was 43.3 ± 10.2 years. The majority of patients were Saudi, accounting for 88.57% and the rest were non-Saudi. Of the 12 non-Saudi patients, five were Yemeni, two were Sudanese, and one was from India, Afghanistan, Syria, Egypt and Somalia. Among the participants, 52 (49.5%) patients underwent thyroid lobectomy, 44 (41.9%) underwent total thyroidectomies, and 9 (8.6%) underwent subtotal thyroidectomy. The overall mean operative time was 123.33 ± 49.42 minutes and the overall mean anesthesia time was 142.95 ± 52.02 minutes.
Oral opioid, by combining paracetamol and codeine, was prescribed to 62 (59%) patients upon discharge (95% CI: 49.5–68.1%), whereas 43 (41%) patients were discharged on paracetamol only (95% CI: 31.5–51.0%).
Table 1 shows the distribution of performed surgical procedures by discharge medication. Opioid was prescribed for 63.5% of patients who underwent lobectomy, compared to 54.5% for total thyroidectomy and 55.6% for subtotal thyroidectomy. These differences were not significant (Pearson chi-sq.= 0.833, P = 0.659).
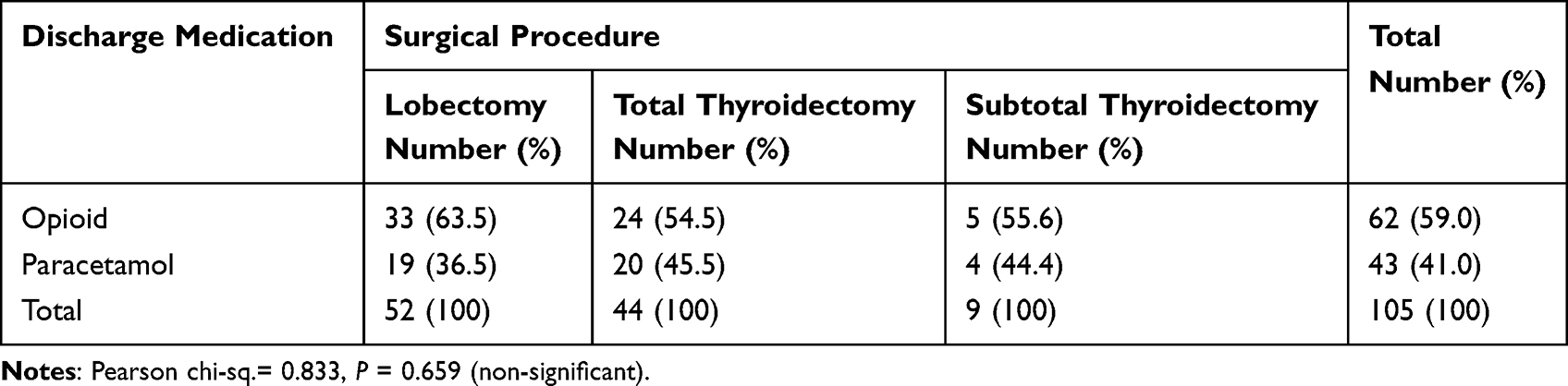 |
Table 1 Distribution of Performed Surgical Procedures by Discharge Medications |
Table 2 shows the distribution of patients’ age groups by discharge medication. Opioid was prescribed for 71.4% of patients aged under 40 years compared to 48.2% among those aged over 40 years. The difference was statistically significant (Pearson chi-sq.= 5.842, P = 0.013).
 |
Table 2 Distribution of Patient Age Groups by Discharge Medications |
Discussion
To the author’s knowledge, this is the first study of its kind to be conducted in Saudi Arabia that presents a unique illustration of physicians prescribing patterns of codeine after thyroid surgery. The study results reveal that a majority of patients were discharged with oral opioids, combining paracetamol and codeine, as postoperative pain medication. We believe that inadequate preoperative patient counseling regarding pain management and failure to use multimodality nonopioid pain management may have contributed to this rise in postoperative opioid prescription. This can also be attributed in part to the fact that trainees/residents are largely responsible for writing the prescriptions for discharge. Most of the prescribing trainees/residents are from the general surgery and surgical oncology service, where they may have become accustomed to prescribing opioid for typically major and more painful operations than thyroid procedures. Therefore, educating trainees, nursing staff, and patients prior to surgery is necessary for improved outcomes.
Our finding was similar to the reported studies worldwide, wherein hydrocodone-paracetamol is the most prescribed postoperative opioid medication among American otolaryngologists, followed by oxycodone-paracetamol.18 Codeine-paracetamol is the most prescribed among head and neck surgeons in Canada.19
Codeine is one of the most widely prescribed opioids in Saudi Arabia, and currently, four codeine-containing products are approved by the Saudi Food and Drug Authority.20 Unfortunately, codeine can be purchased over-the-counter (OTC) from licensed pharmacies without a medical prescription.21,22 Codeine is a “mild opioid”, but its long-term use can lead to serious medical problems, such as tolerance and addiction.23,24 This is of paramount importance in areas where patients have unrestricted access to this kind of pain medication, as in our area.
Among specialties, surgery is the second highest specialty in the rate of opioid prescription after the specialty of pain medicine.25 However, the actual need for opioids was questioned, whereas a large prospective initiative investigated the postoperative opioid use by patients who underwent 25 different elective procedures and revealed a large proportion of patients who used little or no opioids postoperatively.26 Additionally, a recent meta-analysis that synthesized data from 44 studies to quantify the opioids leftover levels postoperatively revealed that studies of surgery on non-visceral organs (ie, mastectomy and thyroidectomy) reported significantly more leftover opioids than abdominal or pelvic surgery.27
However, recently published finding indicates an improvement in the acceptance of surgeons for the use of non-opioid and alternative analgesic strategies in outpatient thyroid and parathyroid surgery as a response to emerging reports on adverse outcomes from excessive pain management.14,28
The shift toward non-opioid analgesics was supported by several empirical findings indicating that the intensity of postoperative pain following thyroidectomy is relatively low when compared to other more extensive procedures.29–31 This shift was further supported by the Endocrine Surgery Section of the American Head and Neck Society (AHNS-ES), whereas a consensus statement on perioperative pain management and opioid reduction in head and neck endocrine surgery was recently released from AHNS-ES.17 They indicate that
non-opioid medications and adjunctive strategies can effectively manage pain after head and neck or endocrine procedures and reduce postoperative opioid requirements.
Moreover, they stated that
head and neck endocrine surgeons should judiciously utilize opioid medications and only in cases where first-line non-opioid medications are insufficient or medically contraindicated.
Despite the fact that the current study has shortcomings and limitations due to its design and the relatively small number of subjects, the findings of this study demonstrate that surgeons in our region of the world need to pay more attention to their excessive use of codeine. Moreover, regulations must be established to restrict individual access to OTC codeine and limit codeine to prescription-only, as adopted in many countries worldwide.32
Finally, as our study retrospectively focuses solely on postoperative pain management practices in a single institution, we anticipate that future multicentric research will aim to explore further in terms of surgeons’ and patients’ perspectives on efficient postoperative pain management.
Conclusions
This study revealed that some head and neck endocrine surgeons continuously prescribe certain opioids despite emerging evidence that supports the use of non-opioid and alternative analgesic strategies in outpatient thyroid surgery. Further research and quality improvement interventions should be geared toward leading all health professionals to appropriate prescribing practices to improve patient safety and reduce unnecessary opioid prescriptions.
Abbreviations
95% CI, 95% confidence intervals; AHNS-ES, Endocrine Surgery Section of the American Head and Neck Society; NSAIDs, non-steroidal anti-inflammatory drugs; OTC, over-the-counter.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The research was performed in accordance with the Helsinki Declaration of 1964 and subsequent amendments and approved by the research ethics committee of King Khalid University (HAPO-06-B-001; ECM#2021-5913). As the study was retrospective and observational, involved a completely anonymised data and involved no more than minimal risk to subjects, the research ethics committee approved the request to waive the documentation of individual informed consent.
Consent for Publication
This manuscript contains no individual person’s data in any form.
Acknowledgments
I would like to thank Prof. Ahmed Mahfouz for editing the manuscript and Mr. Muhammad Abid Khan for his efforts in the data analysis.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding and/or sponsorship was received in relation to this paper.
Disclosure
The author declares that he has no known competing financial interests or personal relationships that could have appeared to influence this work. The author declares that he has no conflicts of interest in this work.
References
1. Merskey H. Pain terms: a list with definitions and notes on usage. Recommended by the IASP Subcommittee on Taxonomy. Pain. 1979;6:249–252.
2. McMahon S, Koltzenburg M, Tracey I, Turk DC. Wall & Melzack’s Textbook of Pain e-Book. Elsevier Health Sciences; 2013.
3. Yang MMH, Hartley RL, Leung AA, et al. Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis. BMJ open. 2019;9(4):e025091. doi:10.1136/bmjopen-2018-025091
4. White PF. The changing role of non-opioid analgesic techniques in the management of postoperative pain. Anesth Analg. 2005;101(5S):S5–S22.
5. Fourcade O, Sanchez P, Kern D, Mazoit JX, Minville V, Samii K. Propacetamol and ketoprofen after thyroidectomy. Eur J Anaesthesiol. 2005;22(5):373–377. doi:10.1017/S0265021505000645
6. Zeilhofer HU, Brune K, McMahon SB, Koltzenburg M. Antipyretic Analgesics: Basic Aspects. Elsevier; 2006.
7. Chin CJ, Franklin JH, Turner B, Sowerby L, Fung K, Yoo JH. Ketorolac in thyroid surgery: quantifying the risk of hematoma. J Otolaryngol. 2011;40(3):196–199.
8. Sandilands EA, Bateman DN. Opioids. Medicine. 2016;44(3):187–189. doi:10.1016/j.mpmed.2015.12.021
9. Ricardo Buenaventura M, Rajive Adlaka M, Nalini Sehgal M. Opioid complications and side effects. Pain Physician. 2008;11:S105–S20.
10. Apfel CC, Kranke P, Eberhart LHJ. Comparison of surgical site and patient’s history with a simplified risk score for the prediction of postoperative nausea and vomiting. Anaesthesia. 2004;59(11):1078–1082. doi:10.1111/j.1365-2044.2004.03875.x
11. Feroci F, Rettori M, Borrelli A, Lenzi E, Ottaviano A, Scatizzi M. Dexamethasone prophylaxis before thyroidectomy to reduce postoperative nausea, pain, and vocal dysfunction: a randomized clinical controlled trial. Head Neck. 2011;33(6):840–846. doi:10.1002/hed.21543
12. Kuo JH, Huang Y, Kluger MD, et al. Use and misuse of opioids after endocrine surgery operations. Ann Surg. 2020;271(6):1156–1164. doi:10.1097/SLA.0000000000003067
13. Long SM, Lumley CJ, Zeymo A, Davidson BJ. Prescription and usage pattern of opioids after thyroid and parathyroid surgery. Otolaryngology. 2019;160(3):388–393. doi:10.1177/0194599818779776
14. Baker DW. History of The Joint Commission’s pain standards: lessons for today’s prescription opioid epidemic. JAMA. 2017;317(11):1117–1118. doi:10.1001/jama.2017.0935
15. Oltman J, Militsakh O, D’Agostino M, et al. Multimodal analgesia in outpatient head and neck surgery: a feasibility and safety study. JAMA Otolaryngol. 2017;143(12):1207–1212.
16. Wu JX, Yeh MW, Livhits MJ. Most patients do not require opioid medication after thyroidectomy. Clin Thyroidol. 2019;31(10):442–444. doi:10.1089/ct.2019;31.442-444
17. Ferrell JK, Shindo ML, Stack JBC, et al. Perioperative pain management and opioid‐reduction in head and neck endocrine surgery: an American Head and Neck Society Endocrine Surgery Section consensus statement. Head Neck. 2021;43(8):2281–2294. doi:10.1002/hed.26774
18. Schwartz MA, Naples JG, Kuo C-L, Falcone TE. Opioid prescribing patterns among otolaryngologists. Otolaryngology. 2018;158(5):854–859. doi:10.1177/0194599818757959
19. Biskup M, Dzioba A, Sowerby LJ, Monteiro E, Strychowsky J. Opioid prescribing practices following elective surgery in Otolaryngology-Head & Neck Surgery. J Otolaryngol. 2019;48(1):1–10.
20. Syed MH, Yasmeen A, Van Hout M-C. Physician perspectives on codeine accessibility, patterns of use, misuse, and dependence in Saudi Arabia. Int J Ment Health Addict. 2021;1–19. doi:10.1007/s11469-021-00670-4
21. Aljadhey H, Assiri GA, Mahmoud MA, Al-Aqeel S, Murray M. Self-medication in Central Saudi Arabia: community pharmacy consumers’ perspectives. Saudi Med J. 2015;36(3):328. doi:10.15537/smj.2015.3.10523
22. Al-Mohamadi A, Badr A, Mahfouz LB, Samargandi D, Al Ahdal A. Dispensing medications without prescription at Saudi community pharmacy: extent and perception. Saudi Pharma J. 2013;21(1):13–18. doi:10.1016/j.jsps.2011.11.003
23. Robinson GM, Robinson S, McCarthy P, Cameron C. Misuse of over-the-counter codeine-containing analgesics: dependence and other adverse effects. NZ Med J. 2010;123(1317):59–64.
24. Kimergård A, Foley M, Davey Z, Dunne J, Drummond C, Deluca P. Codeine use, dependence and help-seeking behaviour in the UK and Ireland: an online cross-sectional survey. QJM. 2017;110(9):559–564. doi:10.1093/qjmed/hcx076
25. Levy B, Paulozzi L, Mack KA, Jones CM. Trends in opioid analgesic–prescribing rates by specialty, US, 2007–2012. Am J Prev Med. 2015;49(3):409–413. doi:10.1016/j.amepre.2015.02.020
26. Thiels CA, Ubl DS, Yost KJ, et al. Results of a prospective, multicenter initiative aimed at developing opioid-prescribing guidelines after surgery. Ann Surg. 2018;268(3):457–468. doi:10.1097/SLA.0000000000002919
27. Schirle L, Stone AL, Morris MC, et al. Leftover opioids following adult surgical procedures: a systematic review and meta-analysis. Syst Rev. 2020;9(1):1–15. doi:10.1186/s13643-020-01393-8
28. Militsakh O, Lydiatt W, Lydiatt D, et al. Development of multimodal analgesia pathways in outpatient thyroid and parathyroid surgery and association with postoperative opioid prescription patterns. JAMA Otolaryngol. 2018;144(11):1023–1029.
29. Motamed C, Merle JC, Yakhou L, et al. Postoperative pain scores and analgesic requirements after thyroid surgery: comparison of three intraoperative opioid regimens. Int J Med Sci. 2006;3(1):11. doi:10.7150/ijms.3.11
30. Eti Z, Irmak P, Gulluoglu BM, Manukyan MN, Gogus FY. Does bilateral superficial cervical plexus block decrease analgesic requirement after thyroid surgery? Anesth Analg. 2006;102(4):1174–1176. doi:10.1213/01.ane.0000202383.51830.c4
31. Kalmovich LM, Cote V, Sands N, Black M, Payne R, Hier M. Thyroidectomy: exactly how painful is it? J Otolaryngol. 2010;39(3):277–283.
32. Kirby T. The end of over-the-counter codeine in Australia. Lancet Psychiatry. 2018;5(5):395. doi:10.1016/S2215-0366(18)30146-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Incidence and Factors Related to Prolonged Postoperative Cognitive Decline (POCD) in Elderly Patients Following Surgery and Anaesthesia: A Systematic Review
Arefayne NR, Berhe YW, van Zundert AA
Journal of Multidisciplinary Healthcare 2023, 16:3405-3413
Published Date: 9 November 2023
Malignancy in a Solitary Thyroid Nodule: A Retrospective Histopathological Evaluation
Alzahrani HA
International Journal of General Medicine 2024, 17:135-140
Published Date: 16 January 2024