Back to Journals » International Journal of General Medicine » Volume 17
Malignancy in a Solitary Thyroid Nodule: A Retrospective Histopathological Evaluation
Authors Alzahrani HA ![]()
Received 31 October 2023
Accepted for publication 10 January 2024
Published 16 January 2024 Volume 2024:17 Pages 135—140
DOI https://doi.org/10.2147/IJGM.S445734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hassan A Alzahrani
Department of Surgery, College of Medicine, King Khalid University, Abha, Saudi Arabia
Correspondence: Hassan A Alzahrani, Email [email protected]
Objective: This study aimed to assess the presence and type of malignancy in patients who underwent thyroid surgery for solitary thyroid nodules.
Methods: A retrospective review was performed of the case notes of all adult patients with solitary thyroid nodules who underwent thyroid surgery from 1 January 2019 to 31 October 2022. All patients had solitary thyroid nodules identified by ultrasonography. The electronic records of our pathology department were used to determine the pathological diagnosis.
Results: Forty-two patients with solitary thyroid nodules underwent thyroid surgery. The mean age at presentation was 39.1 ± 12.6 years, and 76.2% of patients were female. The malignancy rate was 31%. Further histopathological analysis found that malignant solitary thyroid nodules were mostly papillary carcinoma.
Conclusion: This study indicates that solitary thyroid nodules should be evaluated thoroughly and treated with a high index of suspicion because they have a high chance (31%) of being malignant.
Keywords: thyroid, endocrine, surgery, solitary thyroid nodule, malignancy
Background
Thyroid nodules are distinct lesions in the thyroid gland that are radiologically different from the surrounding thyroid parenchyma and are a common clinical presentation.1 Palpable nodules are found in roughly 5% of the population and are discovered coincidentally on ultrasonography in up to 70% of people, with a higher prevalence in older patients.2,3 The vast majority of nodular lesions are benign follicular nodules, which can be solitary or part of a multinodular goiter. Overall, 7–15% of thyroid nodules are cancerous.1,4–6 The pathological origins of benign thyroid nodules are colloid nodules, Hashimoto’s thyroiditis, simple or hemorrhagic cysts, follicular adenoma, and subacute thyroiditis. Malignant thyroid nodules are papillary cancer, follicular cancer, Hurthle (oncocytic) cell cancer, anaplastic cancer, medullary cancer, thyroid lymphoma, and metastatic deposits.1,2,7 The World Health Organization’s (WHO) histologic categorization of thyroid neoplasms, which was published in its fifth edition in 2022, incorporates a grading system along with newly identified tumor types and subtypes. Benign tumors, low-risk neoplasms, and malignant neoplasms are the three groups (classes) of follicular cell-derived neoplasms. In this revised WHO classification, “Oncocytic cell” has taken the position of “Hürthle cell”.8
A solitary thyroid nodule (STN) is defined as a localized thyroid enlargement accompanied by an apparently normal neighboring gland.9–11 In the assessment of thyroid nodules, ultrasound has become an important diagnostic tool. It is extremely sensitive for detecting nodules, and the sonographic characteristics of the nodules can be used to determine whether further investigation is required.12
To enhance malignancy prediction in thyroid nodules and avoid unnecessary fine needle aspiration cytology (FNAC) from the benign nodules, various ultrasonographic systems have been described. American Thyroid Association (ATA) system categorized thyroid nodules based on echostructure, echogenicity, margins, presence or absence of microcalcifications, and shape. It offers a 5-class scoring system with the following anticipated rates of malignancy for each class: 1% for benign class, 3% for very-low suspicion, 5–10% for low suspicion, 10–20% for intermediate suspicion, and >70–90% for high suspicion.1 The British Thyroid Association (BTA) ultrasonographic classification of thyroid nodules consists of five categories: normal (U1), benign (U2), equivocal/indeterminate (U3), suspicious (U4), and malignant (U5). The following ultrasonographic features are considered predictors of malignancy: eccentric location of the solid portion in partially cystic nodules, non-smooth margins, hypoechogenicity of the solid portion, microcalcification, and taller-than-wide shape.13 However, the most widely accepted ultrasonographic classification system to evaluate thyroid nodules is Thyroid Imaging Reporting and Data System (TI-RADS). TIRADS 1 to TIRADS 5 are the categories. TIRADS 1 corresponds to a normal thyroid gland, TIRADS 2 to benign nodules, TIRADS 3 to possibly benign nodules, TIRADS 4 to nodules with ultrasound features suggestive of malignancy, and TIRADS 5 to nodules with ultrasound features strongly suggestive of malignancy.14–18
The main objective of this study was to assess the presence and type of malignancy in patients who underwent thyroid surgery with clinically detected STNs.
Methods
A retrospective cohort study was conducted of all patients who underwent thyroid surgery for STNs identified clinically and confirmed by ultrasonography between 1 January 2019 and 31 October 2022 in Abha Private Hospital, southwestern Saudi Arabia. The electronic records of our pathology department were used to determine the pathological diagnosis.
This research followed the declaration of Helsinki’s ethical principles. The institutional review board of King Khalid University approved the research (ECM #2022-112).
All cases that underwent thyroid surgery for STNs and histopathological evaluation were reviewed. The following parameters were determined for all patients: age, sex, nodule size, type of surgery, and histopathological diagnosis.
The data were entered into a Microsoft Excel spreadsheet. Statistical analysis was performed using Statistical Packages for Social Sciences (SPSS), version 20.0 software (SPSS Inc, Chicago, IL, USA). Proportions were compared between groups using the χ2 test. p <0.05 was considered significant.
Results
During the study period, 42 patients underwent surgery for STNs. Most patients were female (n = 32, 76.2%), 13 cases of STNs (31%) were reported to be malignant, and thyroid lobectomy was the most commonly performed procedure (30, 71.4%) (Table 1).
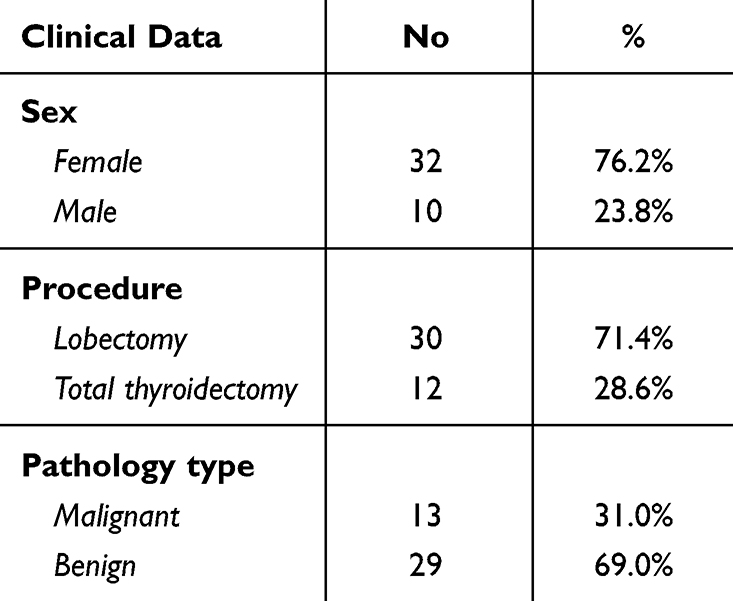 |
Table 1 Bio-Demographic Data |
The mean age was 39.1 ± 12.6 years, and there was a wide range (min–max: 15–67 years). Echogenicity of STNs and their internal contents were variable (Figures 1 and 2). The mean nodule size was 3.8 ± 1.9 cm, and there was a wide range (min–max: 0.6–9.5 cm). Further analysis found that 18 (48.9%) STNs were equal or larger than 4 cm. However, there was no significant correlation between nodule size and the risk of malignancy (p = 0.70). In terms of postoperative histopathology, ten out of the thirteen malignant cases (76.9%) were female, and three (23.1%) were male (male: female ratio of 1:3.3). The remaining 29 STNs were reported to be benign (7 males and 22 females). There was no significant correlation between sex and tumor type (p = 0.999) (Table 2).
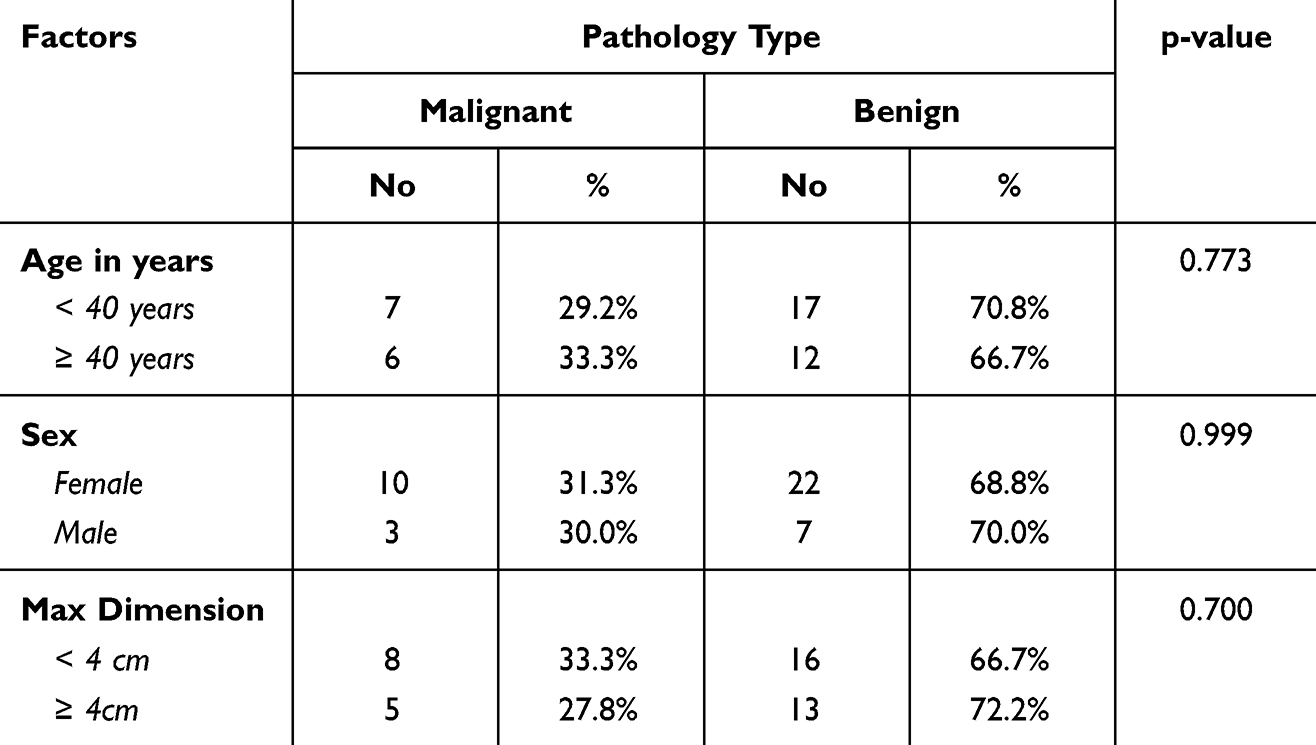 |
Table 2 Distribution of Nodule Pathology Type by Different Bio-Demographic Data |
 |
Figure 1 An isoechoic nodule at the postero-medial aspect of the right lobe showing cystic degeneration. |
 |
Figure 2 An ill-defined irregular hypoechoic non capsulated nodule of the right lobe with multiple foci of pathological heavy calcification. |
Further histopathological analysis found that malignant STNs were papillary carcinoma in nine cases (21.4%), follicular carcinoma in three cases (7.1%), and oncocytic cell carcinoma in one case (2.4%). Benign STNs were mostly colloid nodules (31%), followed by follicular adenoma (19%), Hashimoto’s thyroiditis (11.9%), and oncocytic cell adenoma (2.4%) (Table 3).
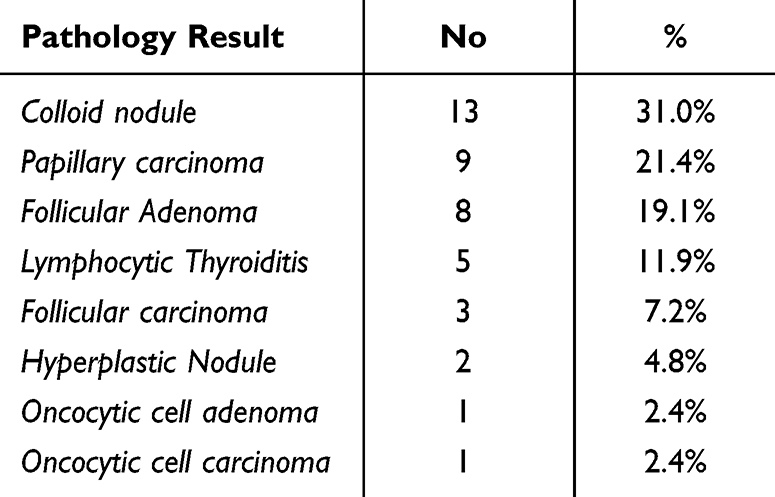 |
Table 3 Pathology Results |
Discussion
Our study revealed that the malignancy rate of STNs was 31%. This indicated that nearly one-third of patients who undergo surgery for STNs have thyroid cancer, which is a significant number. This finding is consistent with most published international data, which indicate that STNs have a higher chance of being malignant than multiple nodules.9–11,19,20 Our study was similar to that reported by Tai et al, who reported that the malignancy rate of STNs was 33.6%.9 Additionally, Iqbal et al reported high cancer frequency for STNs (42.27%).11 Moreover, more recent studies by Keh et al and Nasr et al reported that the prevalence of malignancy in STNs was 34.4% and 26%, respectively.19,20
On the contrary, these findings contradict published data from other parts of the world, which indicate that STNs have a low and the same risk of malignancy as multiple nodules.21–23 Papini et al found that only 9.2% of STNs were malignant.22 Frates et al found that the prevalence of cancer was similar between patients with STNs and patients with multiple nodules, whereas it was estimated to be 14.8 and 14.9, respectively.23 However, a recent meta-analysis by Brito et al refuted these published data by demonstrating that patients with multiple nodules are less likely to have thyroid cancer than patients with a solitary nodule.24 Consequently, surgeons frequently view STNs with a high level of suspicion and tend to favor surgical excision.
Our study revealed that the most common malignancy type was papillary (69.2%), followed by follicular (23.1%). This result is consistent with data published about the pattern of thyroid cancers in Saudi Arabia.25,26 Our results are also consistent with international data indicating that papillary and follicular thyroid cancers are the most common types and account for 90% of all thyroid cancers.1,27,28 Additionally, our results demonstrated that the nodule size in ultrasonography is not predictive of malignancy, consistent with most international published data.22,29–32
Although the current study has limitations related to its design and the low number of studied subjects, it shows that STNs should be managed with a high index of suspicion because the chance of malignancy is high.
This study retrospectively focused solely on the postoperative histopathological malignancy rate of STNs in a single institute. We anticipate that future multicenter studies will further explore STNs in sonographic findings and FNAC analysis and compare them with multinodular goiters.
Conclusions
The study offers insightful information on the characteristics of patients undergoing thyroid surgery for STNs. It indicates that 31% of STNs were malignant, with papillary carcinoma being the most frequent kind of malignancy. Nodule size and malignancy risk did not significantly correlate, according to the study. This study demonstrates that STNs have a high probability of becoming malignant (31%); therefore, they should be extensively investigated and treated with a high index of suspicion.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The research was performed in accordance with the Helsinki Declaration of 1964 and subsequent amendments and approved by the research ethics committee of King Khalid University (ECM #2022-112). As the study was retrospective and observational, involved a completely anonymised data and involved no more than minimal risk to subjects; the research ethics committee approved the request to waive the documentation of individual informed consent.
Consent for Publication
This article contains no individual person’s data in any form.
Acknowledgments
I would like to thank Mr Muhammad Abid Khan for his efforts in the data analysis.
Author Contributions
The author made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding and/or sponsorship was received in relation to this paper.
Disclosure
The author declares that he has no known competing financial interests or personal relationships that could have appeared to influence this work. The author declares that he has no conflict of interest.
References
1. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
2. Burman KD, Wartofsky L. Clinical practice. Thyroid nodules. New Engl J Med. 2015;373(24):2347–2356. doi:10.1056/NEJMcp1415786
3. Walsh JP. Managing thyroid disease in general practice. Med J Aust. 2016;205(4):179–184. doi:10.5694/mja16.00545
4. Werk EE, Vernon BM, Gonzalez JJ, Ungaro PC, McCoy RC. Cancer in thyroid nodules: a community hospital survey. Arch Int Med. 1984;144(3):474–476. doi:10.1001/archinte.1984.00350150058018
5. Belfiore A, Giuffrida D, La Rosa GL, et al. High frequency of cancer in cold thyroid nodules occurring at young age. Eur J Endocrinol. 1989;121(2):197–202. doi:10.1530/acta.0.1210197
6. Lin J-D, Chao T-C, Huang B-Y, Chen S-T, Chang H-Y, Hsueh C. Thyroid cancer in the thyroid nodules evaluated by ultrasonography and fine-needle aspiration cytology. Thyroid. 2005;15(7):708–717. doi:10.1089/thy.2005.15.708
7. Gharib H, Papini E. Thyroid nodules: clinical importance, assessment, and treatment. Endocrinol Metab Clinics North Am. 2007;36(3):707–735. doi:10.1016/j.ecl.2007.04.009
8. Jung CK, Bychkov A, Kakudo K. Update from the 2022 World Health Organization classification of thyroid tumors: a standardized diagnostic approach. Endocrinol Metab. 2022;37(5):703–718. doi:10.3803/EnM.2022.1553
9. Tai JD, Yang JL, Wu SC, Wang BW, Chang CJ. Risk factors for malignancy in patients with solitary thyroid nodules and their impact on the management. J Cancer Res Ther. 2012;8(3):379. doi:10.4103/0973-1482.103516
10. Gupta M, Gupta S, Gupta VB. Correlation of fine needle aspiration cytology with histopathology in the diagnosis of solitary thyroid nodule. J Thyroid Res. 2010;2010:1–5. doi:10.4061/2010/379051
11. Iqbal M, Mehmood Z, Rasul S, Ss HS, Bokhari I. Carcinoma thyroid in multi and uninodular goiter. J Colle Phys Surgeons. 2010;20(5):310–312.
12. Hambly NM, Gonen M, Gerst SR, et al. Implementation of evidence-based guidelines for thyroid nodule biopsy: a model for establishment of practice standards. Am J Roentgenol. 2011;196(3):655–660. doi:10.2214/AJR.10.4577
13. Perros P, Boelaert K, Colley S, et al. Guidelines for the management of thyroid cancer. Clin. Endocrinol. 2014;81:1–122. doi:10.1111/cen.12515
14. Kwak JY, Han KH, Yoon JH, et al. Thyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer risk. Radiology. 2011;260(3):892–899. doi:10.1148/radiol.11110206
15. Horvath E, Majlis S, Rossi R, et al. An ultrasonogram reporting system for thyroid nodules stratifying cancer risk for clinical management. J Clin Endocrinol Metab. 2009;94(5):1748–1751. doi:10.1210/jc.2008-1724
16. Tessler FN, Middleton WD, Grant EG, et al. ACR thyroid imaging, reporting and data system (TI-RADS): white paper of the ACR TI-RADS committee. J Am College Radiol. 2017;14(5):587–595. doi:10.1016/j.jacr.2017.01.046
17. Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L. European Thyroid Association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS. Eur Thyroid j. 2017;6(5):225–237. doi:10.1159/000478927
18. Shin JH, Baek JH, Chung J, et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised Korean Society of Thyroid Radiology consensus statement and recommendations. Korean j radiol. 2016;17(3):370–395. doi:10.3348/kjr.2016.17.3.370
19. Keh SM, El-Shunnar SK, Palmer T, Ahsan SF. Incidence of malignancy in solitary thyroid nodules. J Laryngology Otol. 2015;129(7):677–681. doi:10.1017/S0022215115000882
20. Nasr B, Qubati M, Qubati S, et al. Solitary Thyroid Nodule: clinical, Sonography and Pathological Evaluation Risk of Malignancy. Int J Otolaryngol Head Neck Surgery. 2021;10(5):441–476. doi:10.4236/ijohns.2021.105041
21. Marqusee E, Benson CB, Frates MC, et al. Usefulness of ultrasonography in the management of nodular thyroid disease. Ann Internal Med. 2000;133(9):696–700. doi:10.7326/0003-4819-133-9-200011070-00011
22. Papini E, Guglielmi R, Bianchini A, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002;87(5):1941–1946. doi:10.1210/jcem.87.5.8504
23. Frates MC, Benson CB, Doubilet PM, et al. Prevalence and distribution of carcinoma in patients with solitary and multiple thyroid nodules on sonography. J Clin Endocrinol Metab. 2006;91(9):3411–3417. doi:10.1210/jc.2006-0690
24. Brito JP, Yarur AJ, Prokop LJ, McIver B, Murad MH, Montori VM. Prevalence of thyroid cancer in multinodular goiter versus single nodule: a systematic review and meta-analysis. Thyroid. 2013;23(4):449–455. doi:10.1089/thy.2012.0156
25. Saeed MI, Hassan AA, Butt ME, et al. Pattern of thyroid lesions in western region of Saudi Arabia: a retrospective analysis and literature review. J Clin Med Res. 2018;10(2):106. doi:10.14740/jocmr3202w
26. Albalawi IA, Mirghani HO. Pattern and temporal profile of thyroid carcinoma in the Kingdom of Saudi Arabia: a review and meta-analysis. Australas Med J. 2019;12(12). doi:10.35841/1836-1935.12.12.356-363
27. Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–1214. doi:10.1089/thy.2009.0110
28. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
29. Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;237(3):794–800. doi:10.1148/radiol.2373050220
30. Leenhardt L, Hejblum G, Franc B, et al. Indications and limits of ultrasound-guided cytology in the management of nonpalpable thyroid nodules. J Clin Endocrinol Metab. 1999;84(1):24–28. doi:10.1210/jcem.84.1.5418
31. McHenry CR, Huh ES, Machekano RN. Is nodule size an independent predictor of thyroid malignancy? Surgery. 2008;144(6):1062–1069. doi:10.1016/j.surg.2008.07.021
32. Brito JP, Gionfriddo MR, Al Nofal A, et al. The accuracy of thyroid nodule ultrasound to predict thyroid cancer: systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99(4):1253–1263. doi:10.1210/jc.2013-2928
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patterns of Prescribing Postoperative Analgesic Medication After Thyroid Surgery: A Retrospective Cohort Study
Alzahrani HA
International Journal of General Medicine 2023, 16:405-410
Published Date: 2 February 2023
Assessment of Lower Limb Deep Vein Thrombosis: Characterization and Associated Risk Factors Using Triplex Doppler Imaging
Abdelmalik BHA, Leslom MMA, Gameraddin M, Alshammari QT, Hussien R, Alyami MH, Salih M, Yousef M, Yousif E
Vascular Health and Risk Management 2023, 19:279-287
Published Date: 4 May 2023