Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Incidence and Factors Related to Prolonged Postoperative Cognitive Decline (POCD) in Elderly Patients Following Surgery and Anaesthesia: A Systematic Review
Authors Arefayne NR ![]() , Berhe YW
, Berhe YW ![]() , van Zundert AA
, van Zundert AA ![]()
Received 18 July 2023
Accepted for publication 24 October 2023
Published 9 November 2023 Volume 2023:16 Pages 3405—3413
DOI https://doi.org/10.2147/JMDH.S431168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nurhusen Riskey Arefayne,1 Yophtahe Woldegerima Berhe,1 André A van Zundert2
1Department of Anaesthesia, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2The University of Queensland & Royal Brisbane and Women’s Hospital, Department of Anaesthesia and Perioperative Medicine, Brisbane, QLD, Australia
Correspondence: Nurhusen Riskey Arefayne, Tel +251969299996, Fax +2510581141240, Email [email protected]
Aim: The aim of this systematic review is to explore the current literature to provide evidence regarding the incidence and risk factors of prolonged POCD in elderly patients following cardiac and non-cardiac surgical interventions.
Methods: The PubMed and Google Scholar databases were searched using appropriate keywords and search engines for adequate evidence from studies meeting the inclusion criteria so as to reveal the end-point, which was the presence of prolonged POCD in elderly patients following surgery and anaesthesia. The incidence of POCD at different time intervals and the variables predicting the occurrence of POCD were analysed.
Results: The results of 23 articles covering 5077 patients (3694 non cardiac and 1383 cardiac surgeries) were carefully analysed. POCD occurs from the first postoperative day and lasts for potentially long periods. The incidence of POCD in this review ranged from 2.2% to 35.7%. More specifically, it ranged from 2.2% to 31.5% in non-cardiac surgeries and 11.8% to 35.7% in patients who had undergone cardiac surgeries. Some of the independent risk factors (predictors) for the development of POCD were advanced age, high concentration of neuroinflammatory mediators detectable in plasma, low SpO2, longer anaesthetic and surgical duration, and depth of anaesthesia.
Conclusion: This review can only provide limited evidence of prolonged POCD (more than a year) and further research that involves better study designs, larger samples, involving longer follow-up, and at different sites (multicentre) is highly advised. This in turn may help researchers and clinicians to discover the actual causes and risk factors and develop appropriate preventive and treatment protocols to tackle POCD in the ageing surgical population.
Keywords: incidence, postoperative, cognitive dysfunction/decline, elderly patients, surgery, anaesthesia
Introduction
Perioperative cognitive impairment and cognitive decline (dysfunction) are commonly seen side effects among elderly surgical patients who have undergone either cardiac or non-cardiac surgical interventions. Both postoperative delirium (POD) and postoperative cognitive dysfunction (POCD) are common neurocognitive complications affecting the postoperative course and outcome of the care of older patients following surgical and anaesthetic treatments for different pathologies.1–4
Specifically, POCD occurs more often in patients aged ≥75 years who have undergone major cardiac and non-cardiac procedures involving massive tissue trauma and systemic neuroinflammatory surges.5–7The exact mechanisms, causes, risk factors, and incidence of POD and POCD are still not known, with reported incidence ranging from 13% to 50%.8 This makes risk stratification of patients for POCD challenging, and as such, the diagnosis and treatment of POCD remains unresolved in the geriatric population after surgery and anaesthesia.2,8–10
As has been demonstrated in several studies, the risk factors involved in the development of POCD are: a) patient related factors, ie, advanced age, frailty, multimorbidity, presence of preoperative neurocognitive impairment, mobility and malnutrition issues, and polypharmacy; b) surgery-related factors, ie, prolonged and extensive surgeries with substantial tissue trauma and inflammation, such as cardiac surgeries; and c) anaesthesia-related factors, ie, the use of various general anaesthetics, such as inhalational anaesthetics, sedatives, and benzodiazepines, and depth of anaesthesia.11–13 POD and POCD may seem to be similar, though they are different entities. According to the Diagnostic and Statistical Manual of Mental Disorders fifth Edition (DSM-V), delirium is defined as an acutely developing deficit in attention (reduced ability to direct, focus, sustain, and shift attention), coupled with a change in cognition (memory deficit, disorientation, or perceptual disturbance).1
On the contrary, defining and diagnosing POCD is challenging in that it mainly refers to a longer-lasting decline in cognitive function mostly following surgery and anaesthesia. Diagnosis of POD is based on the presence of suggestive symptoms. To have a clear definition of POCD, one must evaluate preoperative (baseline) neurocognitive function to know how many of these functional parameters are missing post-surgery and anaesthesia. Due to their close similarity, many clinicians face difficulties in differentiating POD from early POCD. Given the fact that POD is a strong predictive variable for POCD, it is always seen with in the first 3 days post-surgery and anaesthesia, whereas early POCD occurs in the last days of the first week, with the potential to stay longer.14 Although POCD in some patients can stay for weeks to months, it can persist for longer periods (up to over a year), causing permanent dementia in some patients.15–18 There is limited availability of data on the occurrence of POCD for prolonged periods and even persistent cognitive impairment. The purpose of this review is to explore if there is evidence showing prolonged POCD in elderly patients following anaesthesia and surgery, as these patients are potentially prone to developing permanent cognitive decline and dementia.
Methods
We conducted this review from October 2022 to January 2023. The Medical Subject Headings (MeSH) platform was used to generate appropriate keywords for our search to give us an adequate number of studies for our review. Therefore, a literature search was performed on Google Scholar and PubMed using the keywords ‘incidence’ AND ‘postoperative’ AND ‘cognitive dysfunction’ OR ‘cognitive decline’ AND ‘elderly patients’. Filters were used to get free and full-text articles usin different study designs in the last 10 years on elderly patients aged ≥60 years. We obtained a total of 9578 articles (57 from PubMed and 9521 from Google Scholar). After removing duplicates (n=8228), 1350 articles remained. Of these, 955 were excluded after going through their titles and abstracts. Of the 395 articles screened, 295 were removed for such reasons as ineligibility or similarity in objectives. Of the remaining 100 studies, 77 were excluded for such reasons as inaccessibility of free full texts and for reporting POD alone. Finally, 23 studies were included to conduct the final qualitative review, and the references cited in each eligible study were examined to identify their appropriate use. This systematic review was done in line with the recommendations of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Figure 1).
 |
Figure 1 PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) guideline showing the allocation of evidence for final review. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10):e1-34. Creative Commons.19 |
The primary outcome of this review is exploring the incidence of prolonged postoperative cognitive decline in older (≥60 years) patients following both cardiac and non-cardiac surgeries. We have included evidence where authors made a follow-up of patients at different time points up to 1 year. The secondary outcomes focused on risk factors associated with the development of prolonged POCD in this age group. We included data that were published between 2012 and 2022. These included multiple study designs and data-analysis methods reporting the incidence of POCD and the risk factors related to it. Literature reporting any cognitive abnormality other than POCD was excluded, but we used studies that reported POCD that occurred immediately after surgery and POCD that persisted up to 1 year. We appraised the quality of the articles used to determine if they were methodologically sound and met the inclusion criteria. We did this using the mixed-method appraisal tool.20 The relevant data from each selected study were carefully extracted and are summarised in tables (Tables 1 and 2).
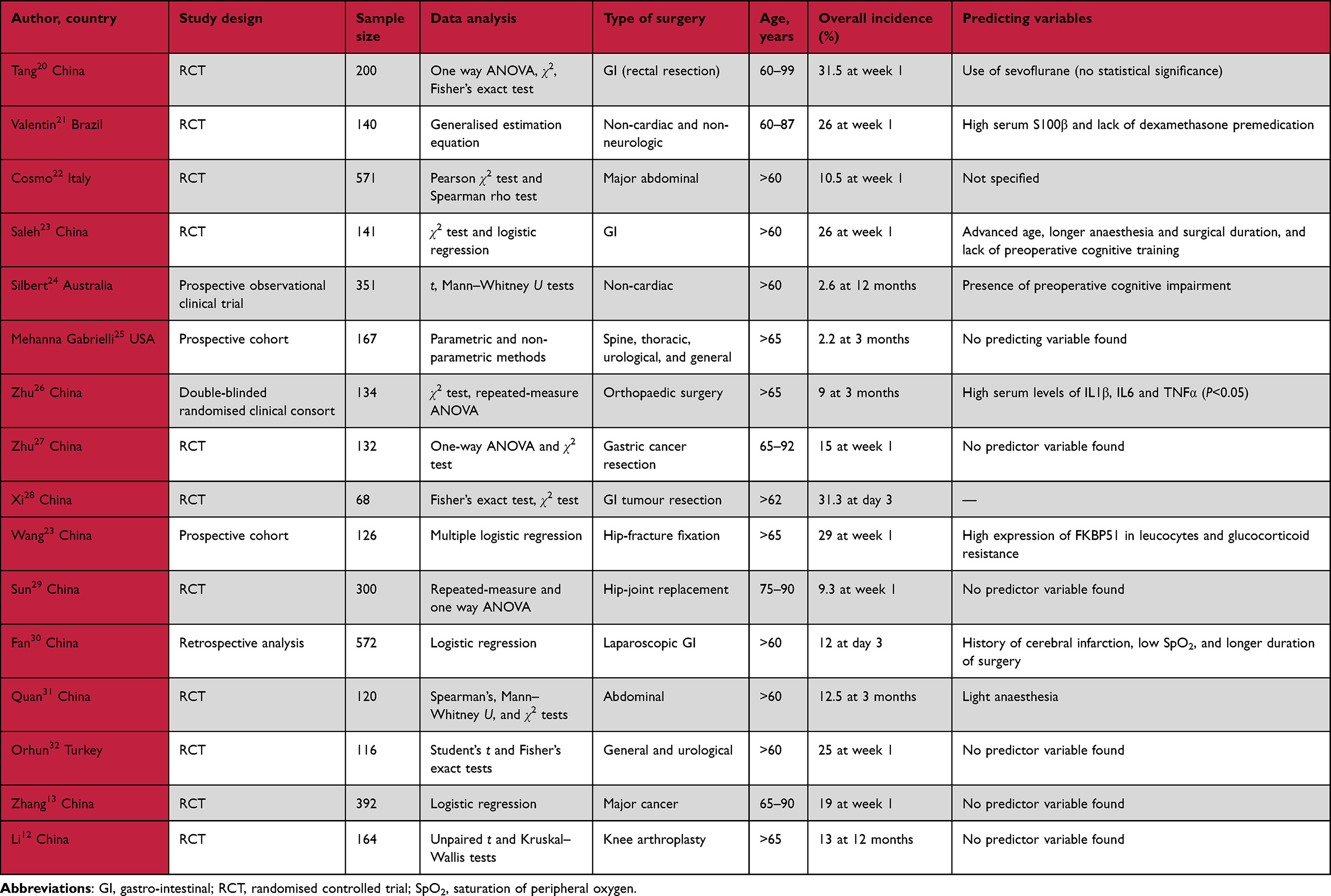 |
Table 1 Incidence of POCD and predicting factors in elderly patients after non-cardiac surgeries (n=16 articles) |
 |
Table 2 Incidence of POCD and predicting factors in elderly patients after cardiac surgery (n=7 articles) |
Results
Basic Description of Reviewed Literature
Our electronic database search (Figure 1) yielded 9578 citations (57 from PubMed and 9521 from Google Scholar). A total of 395 articles were screened, and of these we assessed 100 articles to get 23 studies to conduct our final review. Of these 23 articles, there were two cross-sectional studies, 13 randomised controlled trials, two clinical trials, and six cohorts (observational studies) (Tables 1 and 2).
Incidence of POCD
The incidence of POCD in aged patients who had undergone cardiac and non-cardiac surgeries at different time points of the postoperative period was 2.2%–35.7%. The maximum incidence of POCD seen in those patients who had undergone non-cardiac surgery (n=3694) was 31.5% and the minimum 2.2%, which were measured at the first postoperative week and at 3 months respectively. Among the study participants had undergone cardiac surgery (n=1383), the maximum incidence of POCD was 35.7% and minimum 11.8%. These two articles measured POCD at the first postoperative week. Regarding the follow-up time, five studies followed patients up to 12 months and four reported POCD at 3 months. There was only one article that reported incidence of POCD at the third postoperative week (27.1%), and in the remaining 13, POCD was reported in the first postoperative week with a maximum incidence of 35.7% (cardiac surgery patients) and minimum incidence of 9.3%, which was present in patients who underwent hip-joint replacement (Figure 2).
 |
Figure 2 Incidence of POCD (postoperative cognitive decline) at three time points in the postoperative period in older patients undergone both cardiac and noncardiac surgeries. |
Predicting Variables of POCD in Elderly Patients
The authors mentioned diversified variables to independently predict POCD in elderly surgical patients. Among these variables, advanced age, elevated serum levels of different categories of inflammatory mediators, longer anaesthetic and surgical duration, and light depth of anaesthesia are the most commonly reported. There is a positive relationship between the presence of POD and POCD. Furthermore, concomitant frailty, low oxygen saturation, presence of preoperative cognitive impairment, and intraoperative haemodynamic instability are also reported as predictors of POCD. There are also authors (n=7) who neither found nor specified any variable to predict POCD (Table 1 and Table 2).
Discussion
In this systematic review, we aimed to show the incidence of prolonged POCD and the possible predictor variables in elderly patients who went through the course of surgery and anaesthesia for both cardiac and non-cardiac surgical pathologies in the postoperative period. Our literature search demonstrated a wide range of incidence of POCD, from as low as 2.2% (in non-cardiac surgery) to as high as 35.7% (in cardiac surgery). The possible explanation for this variation is that the authors used different measuring tools to define POCD, as the specificity, sensitivity, and validity of these tests is highly variable. The shortest time that patients were followed (observed) until they develop POCD was the first days of the first week and the longest time was 12 months (five articles). This again can be one reason for the variation in POCD incidence. One review in 2012 reported that POCD subsides a few days or weeks post-surgery.21
Though limited in number, there are studies reporting the incidence of prolonged POCD of up to 5–7 years post-surgery and anaesthetic exposure. POCD significantly affects the way old people live, compromising their quality of life and independence, which in turn increases health care–related costs, rate of hospitalizations, and overall socioeconomic burden. The risk of 1-year mortality also increases in elderly patients with POCD.22,23
We observed that advanced age and an increase in neuroinflammation are the predicting factors of persistent POCD. This finding is similar to a systematic review done by Susana and et al, in which advanced age and exposure to extensive surgical procedures and prolonged anaesthesia duration were found to be risk factors for the development of prolonged POCD.24 It is known that the risk of having surgical pathologies and neurocognitive dysfunction increases with age. Due to such reasons, it is highly likely that this group of patients are at higher risk of developing POCD.25 A systematic review of 22 articles reported that the incidence of POCD was 9%–54%, where advanced age was the main contributing factor.26
In this systematic review, the maximum incidence of POCD was 35.7%, which was measured in the first week post-cardiac surgery. A systematic review conducted by Patel et al reported a somewhat higher incidence of POCD (40%–60%), which was measured in the first 2 weeks post-cardiac surgical interventions. The authors of this review also reported the incidence of POCD at 3 months was 30%–40% and at 1 year was 10%–20%.27 This supports the notion that the burden of POCD after cardiac surgery on elderly patients is significantly higher than most clinicians think.
The maximum incidence of POCD in patients who underwent non-cardiac surgeries was 31.5%, which was found at the first week following surgery. This result is higher than that of a systematic review done by Kitsis et al, where most of the reviewed articles reported the incidence of POCD to be 10%–15% with a median incidence of 19.3%.28 This difference shows that there is a wide variation among studies regarding the occurrence of postoperative cognitive decline in elderly surgical patients. Even though the causes of the development of POCD seem to be similar, there is a higher incidence of POCD in cardiac surgeries than in non-cardiac surgeries, and the mechanism involved to explain this discrepancy is that there is non-physiological perfusion during cardiopulmonary bypass and presence of cerebral microemboli.23,29
In this systematic review POD, which was measured by various test batteries, was found to be one of the independent risk factors to predict POCD. This finding is similar to the results of a study done by Brown et al, where the incidence of POD was 53.5%, and of these patients, a significant number had developed POCD at 1 month (P=0.02) and 1 year (P=0.033) following cardiac surgeries, respectively. The mechanism for the positive association of POD with POCD, as suggested by the authors of this article, is threefold: 1) insults in surgical neuroinflammation and altered cerebral blood flow predispose aged surgical patients to POD and concomitant (long-lasting) POCD; 2) disturbance of the sleep–wake cycle commonly seen in patients with delirium might lead to changes in cognitive function; and 3) delirium causes changes in white-matter integrity and injury to the subcortical area of the brain, and these changes in turn negatively affect the speed of information-processing capacity in the aged surgical population, hence POCD.29
Factors like frailty and presence of preoperative cognitive impairment are also independent risk factors of POCD in both cardiac and non-cardiac elderly surgical patients.2,29–31 This finding is in line with a systematic review and meta-analysis of 18 studies by Gong et al, 2022, where frailty was associated with an increase in 30-day and 6-month mortality rate. They also reported that the presence of frailty was a predictor of postoperative neurological, renal, vascular, and respiratory system complications in patients who went through both cardiac and non-cardiac surgical procedures.32
Even though the mechanism remains unclear, the surge in neuroinflammatory mediators following both cardiac and non-cardiac surgical interventions has been reported to be a strong predictor of POCD. We have seen that most of the literature in this review article supported this argument (n=8).25,33–39 This is supported by a review done in Germany, where the authors found a strong association of general anaesthesia and neuroinflammation with prolonged POCD. The authors of this systematic review have specifically stated that anaesthetics generally increase neuroinflammation by altering the DNA expression and the function of histone-modifying enzymes of cells and that these changes in turn increase the blood concentration of some pro-inflammatory mediators like TNFα, IL6, and IL1B. Consequently, these factors challenge the normal integrity of the blood–brain barrier of the ageing brain in surgical patients, compromising their cognitive function.40
We have seen that no authors followed patients and measured the incidence of POCD for a prolonged time (more than a year). They did not specifically mention any justification for that, but put it as a limitation of their studies and recommended researchers to undergo further research involving longer follow-up.25,31,34,38,41–43 The authors of all of the reviewed articles of our systematic review reported that surgical stress and neuroinflammation are the main predictors of the development of POCD. A 4-year follow-up study done in 2021 suggested that prophylactic (preoperative) administration of corticosteroids reduces the occurrence of longer POCD in elderly patients. They explained that administering 0.1 mg/kg of preoperative dexamethasone decreases the inflammatory response to surgical trauma following cardiac surgeries. This is evidenced by a decrease in the incidence of POCD in patients who took dexamethasone compared to the placebo group.44
Strengths and Limitations
The strength of this review is that we have used a justifiable number of recent studies with diverse methodologies, which is helpful to avoid possible confounders. As a limitation, we extracted articles only from PubMed and Google Scholar, which might have limited our access to literature with more important information on prolonged POCD.
Conclusion
We have seen very limited evidence showing incidence of prolonged POCD (more than a year), and further research is highly advised that involves better study designs, larger samples, longer follow-up, and different sites (multicentre). This in turn may help researchers and clinicians uncover the actual (root) causes and risk factors of long-lasting postsurgical cognitive decline and associated dementia and to develop appropriate preventive and treatment protocols to tackle POCD in the aged surgical population.
Funding
Departmental-only funding, no external funds.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Majewski P, Zegan-Barańska M, Karolak I, Kaim K, Żukowski M, Kotfis K. Current Evidence Regarding Biomarkers Used to Aid Postoperative Delirium Diagnosis in the Field of Cardiac Surgery. Medicina. 2020;56(10):493. doi:10.3390/medicina56100493
2. Sauër AC, Veldhuijzen DS, Ottens TH, Slooter AJC, Kalkman CJ, van Dijk D. Association between delirium and cognitive change after cardiac surgery. BJA. 2017;119(2):308–315. doi:10.1093/bja/aex053
3. Czok M, Pluta MP, Putowski Z, Krzych ŁJ. Postoperative neurocognitive disorders in cardiac surgery: investigating the role of intraoperative hypotension. A systematic review. Int J Environ Res Public Health. 2021;18(2):786. doi:10.3390/ijerph18020786
4. Huang C, Mårtensson J, Gögenur I, Asghar MS. Exploring postoperative cognitive dysfunction and delirium in noncardiac surgery using MRI: a systematic review. Neural Plast. 2018;2018:1–12. doi:10.1155/2018/1281657
5. Uzoigwe CE. Factors associated with delirium and cognitive decline following Hip fracture surgery. Bone Joint J. 2020;102(12):1675–1681. doi:10.1302/0301-620X.102B12.BJJ-2019-1537.R3
6. Kirfel A, Menzenbach J, Guttenthaler V. Postoperative delirium after cardiac surgery of elderly patients as an independent risk factor for prolonged length of stay in intensive care unit and in hospital. Aging Clin Exp Res. 2021;33(11):3047–3056. doi:10.1007/s40520-021-01842-x
7. Heinrich M, Nottbrock A, Borchers F, et al. Preoperative medication use and development of postoperative delirium and cognitive dysfunction. Clin Transl Sci. 2021;14(5):1830–1840. doi:10.1111/cts.13031
8. Li Y-L, Huang H-F, Le Y. Risk factors and predictive value of perioperative neurocognitive disorders in elderly patients with gastrointestinal tumors. BMC Anesthesiol. 2021;21(1):1–8. doi:10.1186/s12871-021-01405-7
9. Li QH, Yu L, Yu ZW, et al. Relation of postoperative serum S100A12 levels to delirium and cognitive dysfunction occurring after Hip fracture surgery in elderly patients. Brain Behav. 2019;9(1):e01176. doi:10.1002/brb3.1176
10. He X, Long G, Quan C, Zhang B, Chen J, Ouyang W. Insulin resistance predicts postoperative cognitive dysfunction in elderly gastrointestinal patients. Front Aging Neurosci. 2019;11:197. doi:10.3389/fnagi.2019.00197
11. Lertkovit S, Siriussawakul A, Suraarunsumrit P, et al. Polypharmacy in Older Adults Undergoing Major Surgery: prevalence, Association With Postoperative Cognitive Dysfunction and Potential Associated Anesthetic Agents. Front Med. 2022;9. doi:10.3389/fmed.2022.811954
12. Li W-X, Luo R-Y, Chen C, et al. Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients: a randomized controlled preliminary trial. Chin Med J. 2019;132(4):437–445. doi:10.1097/CM9.0000000000000098
13. Zhang Y, Shan G-J, Zhang Y-X, et al. Propofol compared with sevoflurane general anaesthesia is associated with decreased delayed neurocognitive recovery in older adults. Br J Anaesth. 2018;121(3):595–604. doi:10.1016/j.bja.2018.05.059
14. Glumac S, Kardum G, Karanovic N. Postoperative cognitive decline after cardiac surgery: a narrative review of current knowledge in 2019. Med Science Monitor. 2019;25:3262. doi:10.12659/MSM.914435
15. Daiello LA, Racine AM, Yun Gou R, et al. Postoperative Delirium and Postoperative Cognitive Dysfunction: overlap and Divergence. Anesthesiology. 2019;131(3):477–491. doi:10.1097/ALN.0000000000002729
16. Deiner S, Silverstein J. Postoperative delirium and cognitive dysfunction. Br J Anaesth. 2009;103(suppl_1):i41–i6. doi:10.1093/bja/aep291
17. Needham M, Webb C, Bryden D. Postoperative cognitive dysfunction and dementia: what we need to know and do. BJA. 2017;119(suppl_1):i115–i25. doi:10.1093/bja/aex354
18. Shen Y, Li X, Yao J. Develop a Clinical Prediction Model for Postoperative Cognitive Dysfunction after Major Noncardiac Surgery in Elderly Patients: a Protocol for a Prospective Observational Study. Gerontology. 2022;68(5):538–545. doi:10.1159/000517511
19. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–e34. doi: 10.1016/j.jclinepi.2009.06.006
20. Hong QN, Pluye P, Fàbregues S, et al. Mixed methods appraisal tool (MMAT), version 2018. Registration Copyright. 2018;1148552:10.
21. Caza N, Taha R, Qi Y, Blaise G. The effects of surgery and anesthesia on memory and cognition. Prog Brain Res. 2008;169:409–422.
22. Goettel N, Burkhart CS, Rossi A, et al. Associations between impaired cerebral blood flow autoregulation, cerebral oxygenation, and biomarkers of brain injury and postoperative cognitive dysfunction in elderly patients after major noncardiac surgery. Anesth Analg. 2017;124(3):934–942. doi:10.1213/ANE.0000000000001803
23. Tarasova IV, Trubnikova OA, Syrova ID, Barbarash OL. Long-Term Neurophysiological Outcomes in Patients Undergoing Coronary Artery Bypass Grafting. Br J Cardiovascular Surgery. 2021;36(5):629–638. doi:10.21470/1678-9741-2020-0390
24. Vacas S, Degos V, Feng X, Maze M. The neuroinflammatory response of postoperative cognitive decline. Br Med Bull. 2013;106(1):161–178. doi:10.1093/bmb/ldt006
25. Saleh AJ, Tang G-X, Hadi SM, et al. Preoperative cognitive intervention reduces cognitive dysfunction in elderly patients after gastrointestinal surgery: a randomized controlled trial. Med Sci Monitor. 2015;21:798. doi:10.12659/MSM.893359
26. Bhushan S, Li Y, Huang X, Cheng H, Gao K, Xiao Z. Progress of research in postoperative cognitive dysfunction in cardiac surgery patients: a review article. Int J Surgery. 2021;95:106163. doi:10.1016/j.ijsu.2021.106163
27. Patel N, Minhas JS, Chung EM. Risk factors associated with cognitive decline after cardiac surgery: a systematic review. Cardiovasc Psychiatry Neurol. 2015;2015:1–12. doi:10.1155/2015/370612
28. Kitsis P, Zisimou T, Gkiatas I, et al. Postoperative Delirium and Postoperative Cognitive Dysfunction in Patients with Elective Hip or Knee Arthroplasty: a Narrative Review of the Literature. Life. 2022;12(2):314. doi:10.3390/life12020314
29. Brown IVCH, Probert J, Healy R, et al. Cognitive decline after delirium in patients undergoing cardiac surgery. Anesthesiology. 2018;129(3):406–416. doi:10.1097/ALN.0000000000002253
30. Nomura Y, Nakano M, Bush B, et al. Observational study examining the association of baseline frailty and postcardiac surgery delirium and cognitive change. Anesth Analg. 2019;129(2):507. doi:10.1213/ANE.0000000000003967
31. Silbert B, Evered L, Scott DA, et al. Preexisting cognitive impairment is associated with postoperative cognitive dysfunction after Hip joint replacement surgery. Anesthesiology. 2015;122(6):1224–1234. doi:10.1097/ALN.0000000000000671
32. Gong S, Qian D, Riazi S, et al. Association Between the FRAIL Scale and Postoperative Complications in Older Surgical Patients: a Systematic Review and Meta-Analysis. Anesth Analg. 2015
33. Wan J, Luo P, Du X, Yan H. Preoperative red cell distribution width predicts postoperative cognitive dysfunction after coronary artery bypass grafting. Biosci Rep. 2020;40(4):4. doi:10.1042/BSR20194448
34. Tang N, Ou C, Liu Y, Zuo Y, Bai Y. Effect of inhalational anaesthetic on postoperative cognitive dysfunction following radical rectal resection in elderly patients with mild cognitive impairment. J Int Med Reserch. 2014;42(6):1252–1261. doi:10.1177/0300060514549781
35. Valentin LSS, Pereira VFA, Pietrobon RS, et al. Effects of single low dose of dexamethasone before noncardiac and nonneurologic surgery and general anesthesia on postoperative cognitive dysfunction—a Phase III double blind, randomized clinical trial. PLoS One. 2016;11(5):e0152308. doi:10.1371/journal.pone.0152308
36. Zhu Y-Z, Yao R, Zhang Z, Xu H, Wang L-W. Parecoxib prevents early postoperative cognitive dysfunction in elderly patients undergoing total knee arthroplasty: a double-blind, randomized clinical consort study. Medicine. 2016;95:28.
37. Fan Y, Liu X, Wu S, Liu Y. The risk factors for cognitive dysfunction in elderly patients after laparoscopic surgery: a retrospective analysis. Medicine. 2021;100(2):2. doi:10.1097/MD.0000000000023977
38. Wang L-W, Zhu M-J, Li Y, et al. FKBP51 is associated with early postoperative cognitive dysfunction in elderly patients undergoing Hip fracture surgery. Medicine. 2019;98:5.
39. Quan C, Chen J, Luo Y, et al. BIS‐guided deep anesthesia decreases short‐term postoperative cognitive dysfunction and peripheral inflammation in elderly patients undergoing abdominal surgery. Brain Behav. 2019;9(4):e01238. doi:10.1002/brb3.1238
40. Rump K, Adamzik M. Epigenetic Mechanisms of Postoperative Cognitive Impairment Induced by Anesthesia and Neuroinflammation. Cells. 2022;11(19):2954. doi:10.3390/cells11192954
41. De Cosmo G, Sessa F, Fiorini F, Congedo E. Effect of remifentanil and fentanyl on postoperative cognitive function and cytokines level in elderly patients undergoing major abdominal surgery. J Clin Anesth. 2016;35:40–46. doi:10.1016/j.jclinane.2016.07.016
42. Xi L, Fang F, Yuan H, Wang D. Transcutaneous electrical acupoint stimulation for postoperative cognitive dysfunction in geriatric patients with gastrointestinal tumor: a randomized controlled trial. Trials. 2021;22(1):1–10. doi:10.1186/s13063-021-05534-9
43. Sun S-H, Yang L, Sun D-F, et al. Effects of vasodilator and esmolol-induced hemodynamic stability on early post-operative cognitive dysfunction in elderly patients: a randomized trial. Afr Health Sci. 2016;16(4):1056–1066. doi:10.4314/ahs.v16i4.23
44. Glumac S, Kardum G, Sodic L, et al. Longitudinal assessment of preoperative dexamethasone administration on cognitive function after cardiac surgery: a 4-year follow‐up of a randomized controlled trial. BMC Anesthesiol. 2021;21(1):129. doi:10.1186/s12871-021-01348-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patterns of Prescribing Postoperative Analgesic Medication After Thyroid Surgery: A Retrospective Cohort Study
Alzahrani HA
International Journal of General Medicine 2023, 16:405-410
Published Date: 2 February 2023
Beyond The Age Limit: A Comparative Study (<70 Vs ≥70 Years) in Breast Cancer Characteristics and Surgical Management in Women
Buyukasik S, Kankaya B, Altundal YE, Ozgul M, Kapan S
Breast Cancer: Targets and Therapy 2025, 17:1231-1246
Published Date: 12 December 2025