Back to Journals » Patient Preference and Adherence » Volume 20
Patient Preferences for Treatment in Relapsed/Refractory Acute Leukemia: A Multinational Discrete Choice Experiment
Authors Nier S, Hussain H ![]() , Hitch J, Chowdhury S, Skedgel C
, Hitch J, Chowdhury S, Skedgel C ![]() , Mott DJ
, Mott DJ ![]()
Received 27 January 2026
Accepted for publication 2 June 2026
Published 12 June 2026 Volume 2026:20 599189
DOI https://doi.org/10.2147/PPA.S599189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Samantha Nier,1 Hannah Hussain,2 Jake Hitch,2,3 Sulayman Chowdhury,2 Chris Skedgel,2 David John Mott2
1Acute Leukemia Advocates Network, Bern, Switzerland; 2Office of Health Economics, London, UK; 3Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
Correspondence: David John Mott, Office of Health Economics, Golding’s House 2nd Floor, Hay’s Galleria, 2 Hay’s Lane, London, SE1 2HB, UK, Tel +44 020 7747 7002, Email [email protected]
Purpose: Acute leukemia (AL) is an aggressive cancer of white blood cells that progresses rapidly and requires intensive treatment. While first-line therapies can induce remission, this is not the case for all patients (refractory disease), and many patients experience a relapse. In these situations, treatment decisions become complex due to trade-offs between efficacy, toxicity and quality of life. Despite recognition of the importance of patient preferences in treatment decision-making, limited evidence exists on how individuals with AL value different treatment features.
Patients and Methods: A web-based discrete choice experiment (DCE) was conducted across the UK, USA, France, Germany and Italy to quantify treatment preferences among adults with AL. Attributes were identified through literature review, formative qualitative research and patient input. Each participant completed 12 choice tasks comparing hypothetical treatment profiles varying by chance of response, duration of response, quality of life during treatment and response and mode of administration. Data were analyzed using mixed logit and latent class models to estimate conditional relative attribute importance (RAI) scores, explore preference heterogeneity and assess trade-offs.
Results: A total of 267 respondents completed the study. Across the full sample, the chance of response was the most influential treatment attribute (RAI=62%), followed by quality of life during response (14%), duration of response (9%), quality of life during treatment (8%) and mode of administration (7%). Three latent preference classes were identified: efficacy-focused (47%), convenience- and efficacy-focused (21%) and balanced decision-makers (32%). Respondents in the USA were more likely to belong to the convenience- and efficacy-focused group, suggesting that contextual factors influence preferences.
Conclusion: Patients with AL largely prioritize treatment efficacy but also value quality of life and convenience, indicating that treatment decisions are multifaceted and context dependent. Incorporating patient preferences into clinical development and health technology assessment can promote more person-centered approaches to care.
Keywords: acute leukemia, hematology, oncology, patient preferences, discrete choice experiment
Introduction
Acute leukemia (AL) is an aggressive malignancy of the white blood cells characterized by rapid progression and high mortality if left untreated.1 Two main forms are recognized: acute myeloid leukemia (AML), the most common type in adults, which includes the rare subtype acute promyelocytic leukemia (APL),2 and acute lymphoblastic (or lymphocytic) leukemia (ALL), which is more frequent in children but also occurs in adults.3 AL is relatively rare, with global age-standardized incidence rates of 1.37 per 100,000 population for ALL and 1.73 per 100,000 population for AML in 2021,4 and the overall risk of AL varies among populations of different ages, sexes and geographic locations.
Although clinical presentation and treatment approaches vary by subtype,5 most patients initially experience fatigue, bruising or bleeding, fever, shortness of breath and recurrent infections.6 Due to the disease’s aggressive nature, treatment is initiated rapidly upon diagnosis, and typically involves chemotherapy, targeted therapy, and in some cases stem cell or bone marrow transplantation. Advances in targeted and cellular therapies have improved outcomes in certain subgroups, though their toxicity and accessibility vary widely.7 These intensive regimens aim to achieve remission but often carry a substantial physical and emotional burden for patients and their families,8 which can substantially impact their quality of life (QoL).9
While many patients respond to first-line therapy, some do not achieve remission (refractory disease) or later relapse. Prognosis following relapse remains poor, with limited effective treatment options and low long-term survival rates.10,11 Recent therapeutic innovations have expanded treatment options,12 but have also introduced new uncertainties around long-term benefits, costs and side effects. In this setting, treatment decisions often require trade-offs between potential survival benefits and treatment-related toxicity.
Understanding which treatment characteristics patients value most can inform regulatory, reimbursement and clinical decision-making, particularly in preference-sensitive contexts.13–15 However, few studies have explored treatment preferences in AL. The majority of the existing research has focused primarily on AML, showing that patients prioritize response and survival but that preferences differ by age, gender and treatment experience.16–19
Recently, a broad study explored the treatment preferences of adults with any type of AL in the United Kingdom (UK), finding that preferences differed according to AL (sub)type and the amount of time that had passed since diagnosis.20 This study extended the previous study by collecting data in additional countries, enabling regional comparisons and allowing exploration of whether healthcare system context influences preferences.
Materials and Methods
Study Design
A web-based DCE study was developed and administered to elicit treatment preferences and understand how adult individuals with AL value different aspects of treatment. A benefit of DCEs compared to other methods is that they enable trade-offs to be examined. The study aimed to quantify patients’ preferences, elicit trade-offs, and explore variation across patient subgroups. The study was conducted in accordance with the Declaration of Helsinki and ethical approval for the study was granted by the Economics Research Ethics Committee at City St George’s, University of London (formerly City, University of London), under applications ETH2223-2151 and ETH2425-0034. All participants provided informed electronic consent prior to beginning the survey.
Survey Instrument
The UK survey was fielded first and independently of the subsequent multi-country survey,20 and this study utilized the same underlying DCE design. As per the initial study, potential DCE attributes were identified through background research that included (i) a targeted literature review of previous preference studies in AL and (ii) a review of characteristics of current and forthcoming treatments in the relapsed/refractory setting. This was supplemented by formative qualitative research with people living with AL.21 Two online bulletin boards (OBBs) were used as virtual discussion platforms to engage participants recruited via the patient charity Leukaemia Care (a UK charity and member of the ALAN network): one for AML/APL (n=12) and one for ALL (n=9), to explore potential subtype differences. Insights from the background work and OBBs were reviewed by the study team in consultation with the steering committee of the Acute Leukemia Advocates Network (ALAN) and patient and academic advisory groups. A single DCE design with intentionally broad attributes and levels was developed to reflect the range of treatments available across AL subtypes (Table 1).
Quality of life (QoL) was defined on a 0–100 scale (100=best imaginable; 0=worst imaginable) and was introduced to participants using the five dimensions of EQ-5D-5L.22 To familiarize respondents with this framework, all participants completed the EQ-5D-5L questionnaire before starting the DCE tasks.
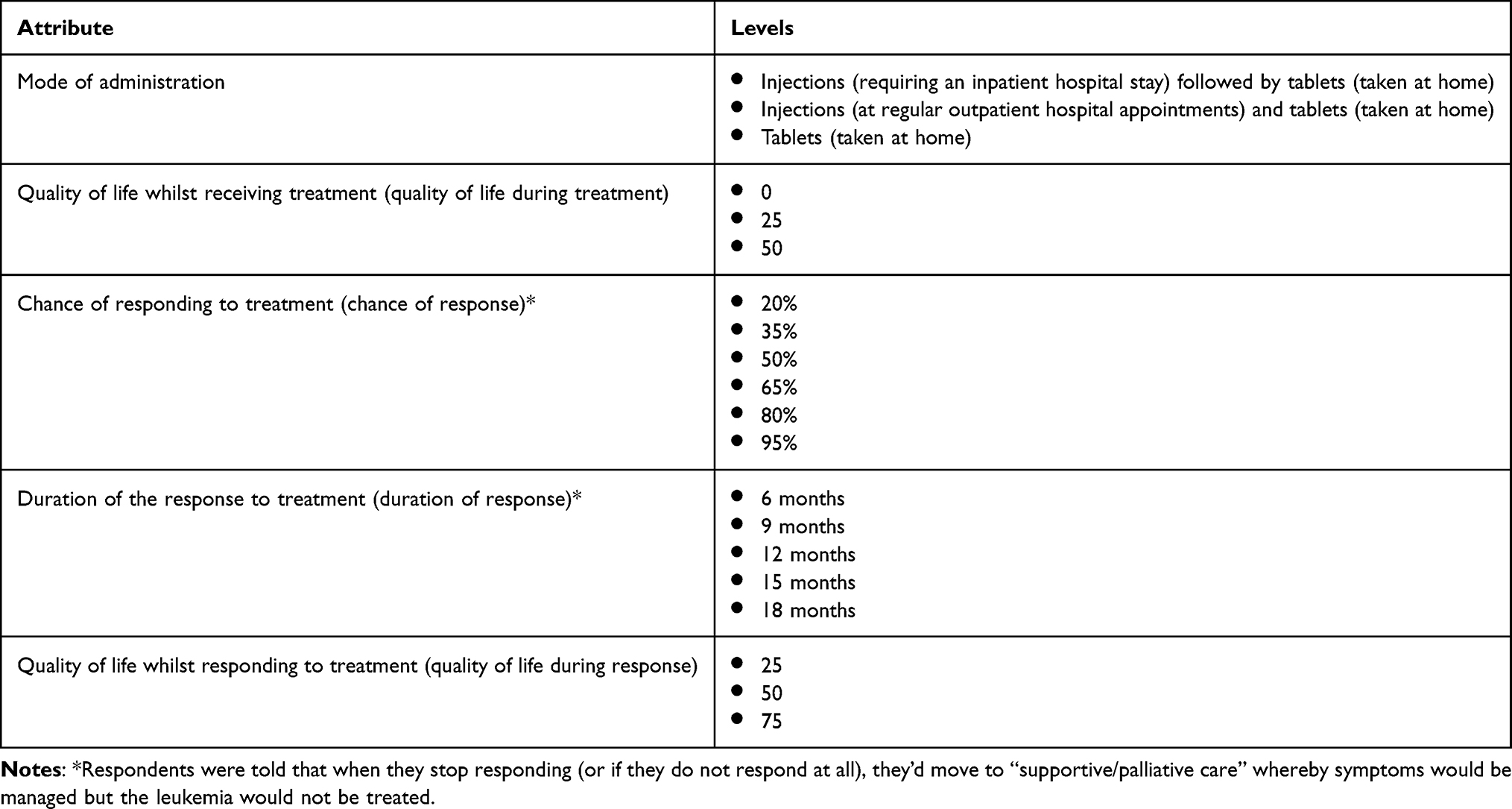 |
Table 1 Attributes and Levels for the DCE |
Each DCE task presented two unlabeled treatment profiles (“Treatment A” and “Treatment B”) and an opt-out option representing no active treatment (i.e., a move to supportive/palliative care). A d-efficient experimental design with 24 choice sets was generated in Ngene and split into two blocks, such that each respondent completed 12 tasks. Constraints were applied to ensure realistic trade-offs: (i) the maximum difference in chance of response within a task was ≤ 30%; (ii) the maximum difference in duration of response was ≤ 6 months; and (iii) QoL during response could not be lower than QoL during treatment. The order of tasks and treatment positions was randomized to minimize bias, with the opt-out option fixed on the right. For the UK survey, the experimental design was only informed by basic directional priors. The resulting UK parameter estimates were then used to update the priors for the subsequent surveys. A simple practice task was included before the main exercise.
Ten think-aloud cognitive pre-testing interviews with UK participants23 informed survey refinements. Revisions included adding a fixed (non-experimental) six-month treatment-duration attribute to avoid confusion with duration of response, re-ordering attributes for clarity, revising icons and grouping attributes under headings. An example DCE task with the final formatting can be seen in Figure 1. The final survey also collected demographic and clinical information, EQ-5D-5L responses, and included a best-worst scaling exercise (results reported elsewhere).24
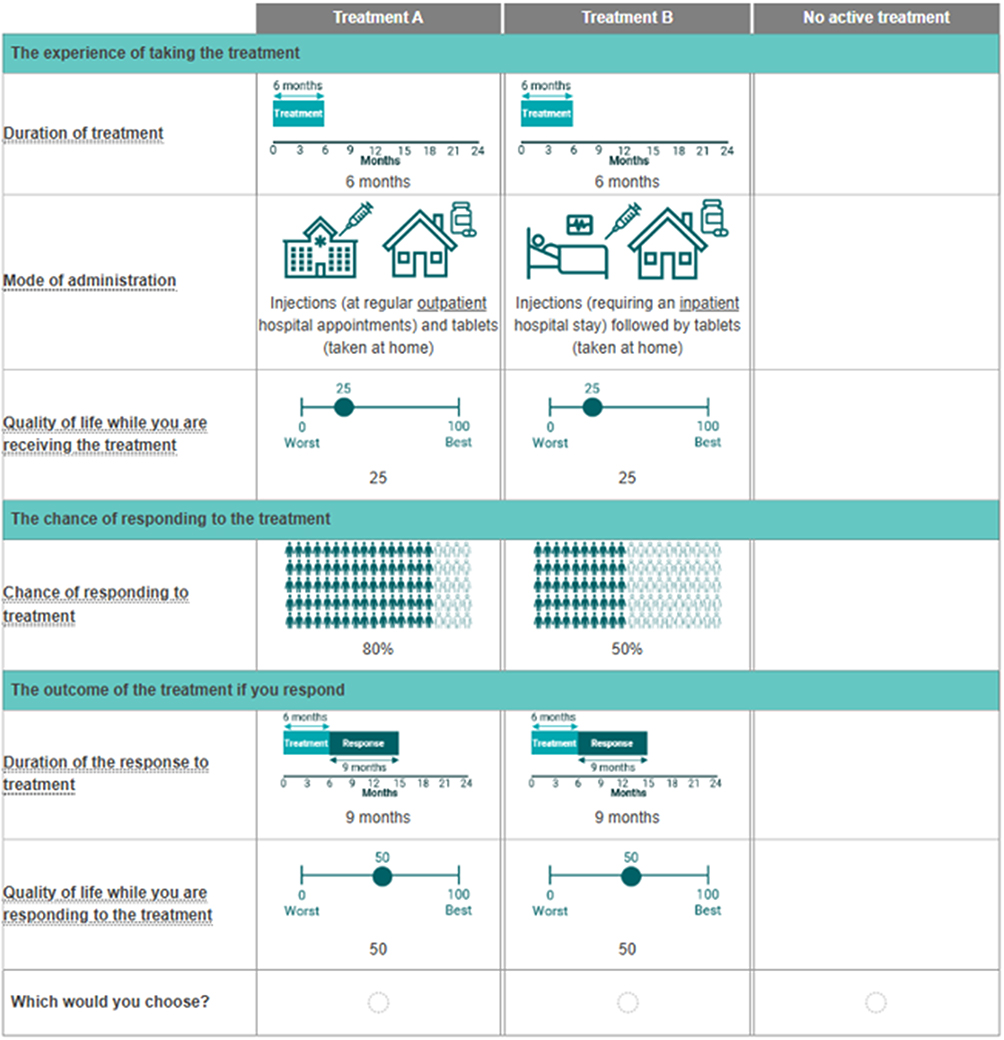 |
Figure 1 DCE Task Example. |
Recruitment
Adults with AL of any (sub)type were eligible to participate in the study. In the UK, all recruitment was conducted via Leukaemia Care, a member organization of ALAN. In all other countries, recruitment was conducted via a specialist patient recruitment agency. We aimed to recruit 100 people with AL in the UK, USA and across the EU4 (France, Germany, Italy and Spain).
Statistical Analysis
The DCE choice data was analyzed within a random utility framework. Several models were estimated for different purposes. As a starting point, a multinomial logit (MNL) model was fitted; however, because this specification does not account for variation in preferences between individuals, a mixed logit model was also used. The mixed logit model estimates the effect of each attribute level as an average across the sample while allowing for differences in preferences between respondents. We initially assumed that preferences for all attribute levels varied randomly (with normal distributions), then simplified the specification by fixing attributes that did not show evidence of heterogeneity. The final model was estimated using simulation with 5,000 Halton draws.
To explore whether preferences differed systematically across participants, latent class models were estimated to identify groups (called “classes”) of respondents with similar preference patterns. Models with different numbers of classes were compared using the Bayesian Information Criterion (BIC), with the three-class model offering the best balance of model fit and parsimony. Characteristics such as age, gender, leukemia subtype, years since diagnosis and relapse history were explored as potential predictors of class membership, and only those that were statistically significant in at least one class were retained in the final model.
Given the relative complexity of these models, exploratory subgroup analyses using simpler MNL models were also conducted to describe broad differences in preferences between key groups. In the mixed logit model, all attribute levels were dummy coded. For the latent class and MNL models, only mode of administration was dummy coded, with all other attributes coded continuously; this reduced the number of estimated parameters, whilst also facilitating the estimation of trade-offs (see below).
Model coefficients were used to generate conditional relative attribute importance (RAI) scores, which express the contribution of each attribute to overall treatment choice on a 0–100% scale. Marginal rates of substitution (MRS) (also known as trade-offs) were derived using the “chance of response” attribute as the numeraire, representing how much chance of response respondents were willing to trade for a favorable change in another attribute (e.g., longer duration of response). Confidence intervals for RAI and MRS estimates were calculated using the Delta method.25 All analyses were conducted using Stata SE, version 15.26
Results
Respondent Characteristics
A total of 267 individuals with acute leukemia completed the DCE survey: 95 from the UK, 88 from the USA, and 84 from France, Germany and Italy combined (hereafter referred to as the EU3 group, as too few participants were recruited in Spain to justify their inclusion). Across the full sample, the mean (SD) age was 55.6 (12.3) years and 60% of respondents were female. Most participants were white (82%), and the majority had completed high school (85%); just over half held a degree or equivalent qualification (51%). The mean age at diagnosis was 51.2 (13.7) years, and mean time since diagnosis was 4.3 (5.9) years. In terms of AL subtype, 62% of respondents had AML, 27% had ALL and 11% had APL. Nearly half of respondents were not receiving active treatment (46%), while 17% were on maintenance therapy and 14% on consolidation therapy. Half (50%) reported never having relapsed, 27% had experienced one relapse, and 54% had received a prior transplant. Regional differences were observed. Respondents from the USA were older on average (59.7 years) compared with those in the UK (53.6 years) and EU3 (53.4 years). Mean time since diagnosis was shortest in the USA (3.0 years) and longest in the UK (6.2 years). The distribution of AL subtype also varied, with ALL more common in the US sample (46%) and AML predominant in the UK (64%) and EU3 (85%). Table 2 presents the demographic and clinical characteristics of the study population.
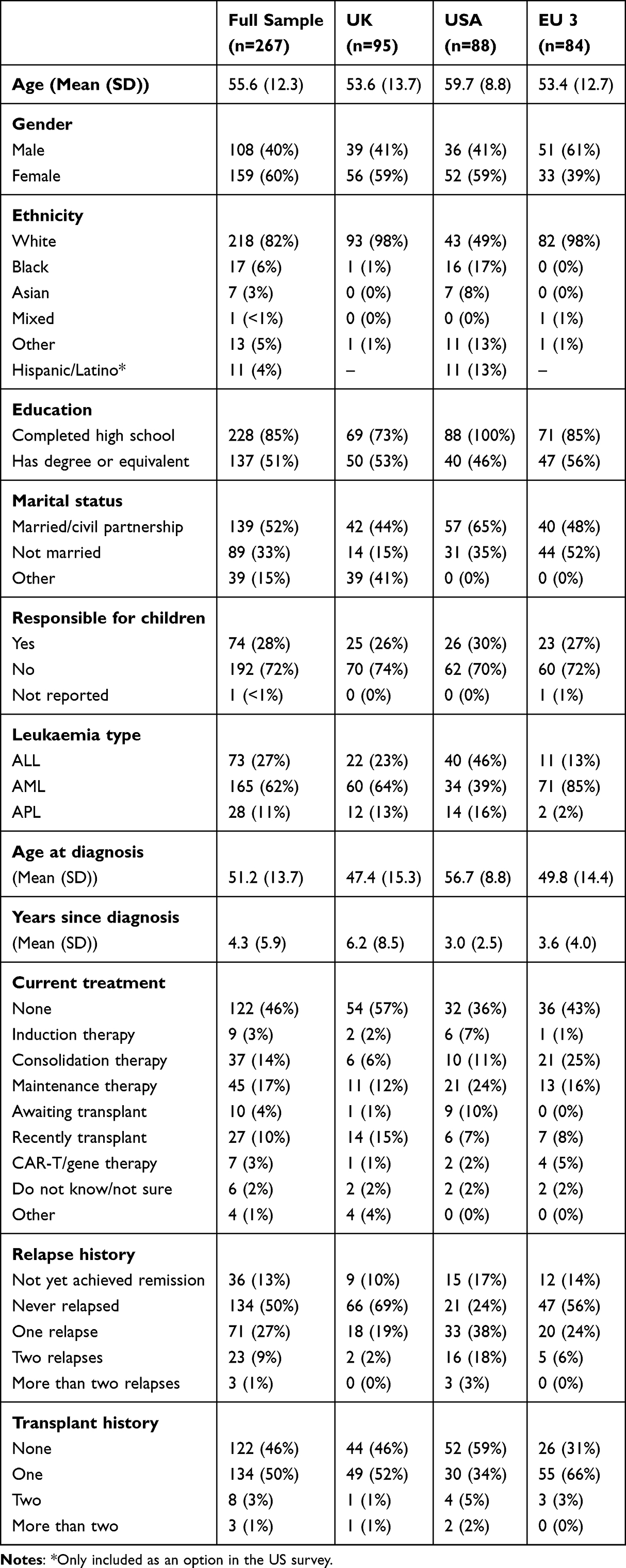 |
Table 2 Demographic and Clinical Information |
Conditional Relative Attribute Importance (RAI) Scores
Figures 2 and 3 present the estimated preference weights and corresponding conditional RAI scores from the preferred mixed logit model. On average, respondents’ preferences were ordered as expected, with more favorable treatment characteristics associated with higher preference weights (Figure 2). The chance of response was by far the most influential factor in treatment choice. Each increase in response probability was associated with a marked rise in utility, and the difference between the lowest and highest levels translated into a conditional RAI score of 62.2% (Figure 3). This indicates that respondents placed substantially greater weight on the likelihood of achieving a response than on any other aspect of treatment.
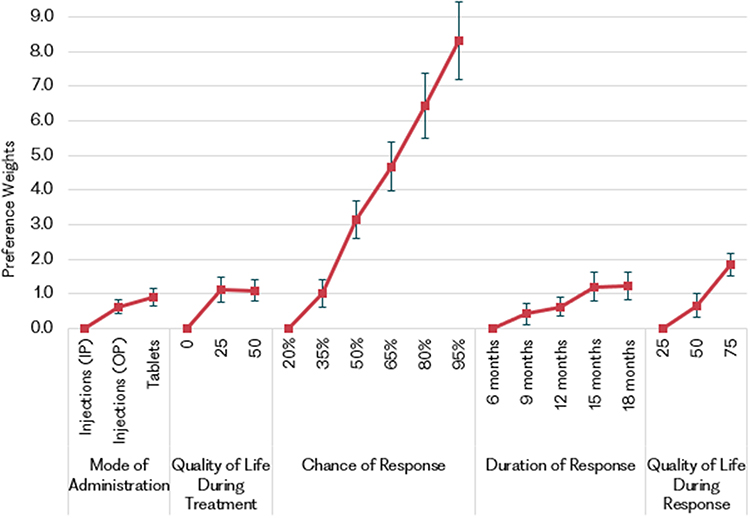 |
Figure 2 Preference Weights (Mixed Logit Model). |
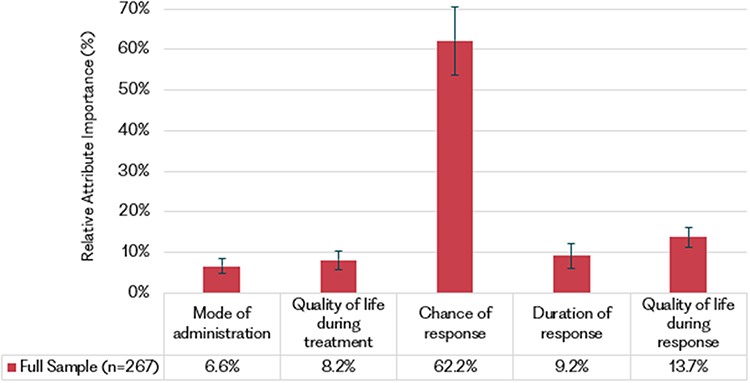 |
Figure 3 Conditional RAI Scores (Mixed Logit Model). |
The next most important attribute was quality of life during response (RAI=13.7%). Respondents clearly differentiated between the levels, strongly preferring a score of 75 over 25 or 50, indicating that perceived wellbeing once treatment is effective is highly valued. Quality of life during treatment contributed less (RAI=8.2%), with little difference in preference between scores of 25 and 50. This pattern suggests that respondents, on average, prioritized their long-term recovery and functioning once the disease responded to therapy, rather than short-term comfort while undergoing treatment.
Duration of response also influenced choice (RAI=9.2%). Longer durations were generally preferred, though the pattern was non-linear - improvements up to about 15 months were viewed as more meaningful than further gains beyond that point. This diminishing marginal value may reflect patients’ perception that extended remission periods are beneficial up to a threshold, after which other factors become more salient. Mode of administration had the smallest overall effect (RAI=6.6%). Participants favored oral tablets over injections, and both over inpatient hospital administration, suggesting a clear preference for less intrusive and more home-based treatment. These convenience gains were relatively minor compared with improvements in efficacy and quality of life.
Overall, respondents preferred treatments with a greater chance of response, longer duration of response, and better quality of life during and following treatment, and they favored oral tablets over outpatient injections or inpatient hospital administration.
Additional analyses examined variation in conditional RAI scores by AL subtype and geographic region (Supplementary Figures S1 and S2). Across disease subtypes (ALL, AML, APL), the overall pattern of preferences was consistent, with chance of response remaining the dominant driver of treatment choice. Minor differences were observed for mode of administration, which was not considered important by respondents with APL (Supplementary Figure S1), though the sample size was low for this subgroup. Regional analyses showed broadly similar results between the UK and EU3, with overlapping confidence intervals for all attributes, indicating no statistically significant differences. In contrast, respondents in the USA displayed a distinct pattern, placing relatively less emphasis on chance of response and quality of life during treatment, and greater weight on duration of response, quality of life during response, and mode of administration (Supplementary Figure S2).
Preference Heterogeneity
Figure 4 illustrates conditional RAI scores across the three classes identified in the latent class analysis, indicating meaningful variation in how respondents valued treatment characteristics. Although the overall sample placed greatest importance on the chance of response, the relative weight assigned to efficacy and QoL attributes differed substantially across classes.
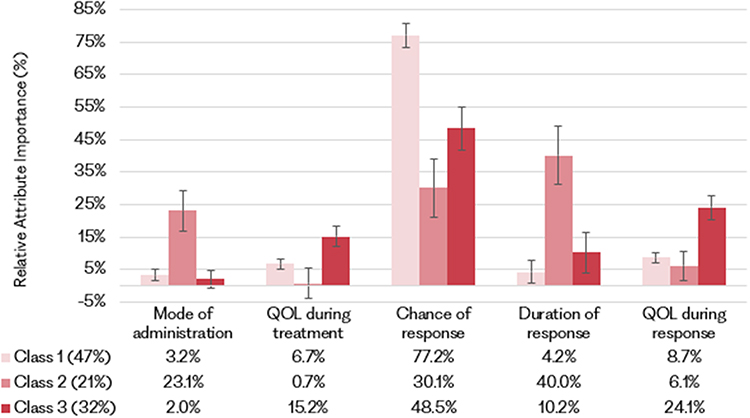 |
Figure 4 RAI scores (Latent class model). |
Class 1 (47% membership) predominantly made choices based on the chance of response attribute (RAI=77%). All other attributes were statistically significant but much smaller in magnitude, suggesting that treatment efficacy was their primary concern; as a result, this class was labelled as “efficacy-focused”. Class 2 (21% membership) exhibited more balanced preferences. Duration of response (RAI=40%) and chance of response (RAI=30%) were highly influential in combination, and mode of administration was also important (RAI=23%). In contrast, quality of life during treatment was not important (RAI not statistically different from zero), and quality of life during response was of relatively low importance (RAI=6%). Therefore, Class 2 was labelled “convenience- and efficacy-focused”.
Class 3 (32% membership) considered nearly all attributes important except for mode of administration. The most influential attribute was chance of response (RAI=49%), followed by quality of life during response (RAI=24%), quality of life during treatment (RAI=15%), and duration of response (RAI=10%). Therefore, Class 3 was labelled as “balanced decision-makers”.
Class-membership analysis showed that respondents more recently diagnosed and those who had relapsed in the past were more likely to belong to Class 1 (efficacy-focused), while those in the USA were less likely, compared with Class 3 (balanced decision-makers). Participants in the USA and those with ALL were more likely to belong to Class 2 (convenience- and efficacy-focused) relative to Class 3.
Trade-Offs
Figure 5 presents the estimated trade-offs between treatment attributes, expressed as marginal rates of substitution (MRS), derived from the latent class model. These values quantify the extent to which respondents in each preference class were willing to forgo improvements in treatment efficacy (chance of response) in exchange for gains in other treatment characteristics.
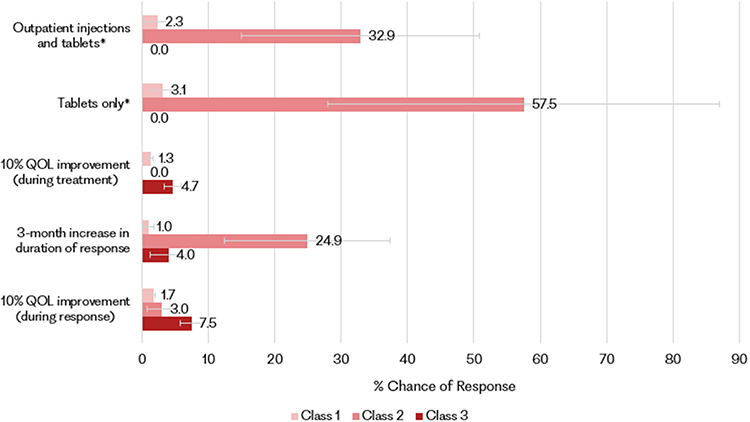 |
Figure 5 Trade-offs (Latent class model). *Relative to “Injections (requiring an inpatient hospital stay) followed by tablets (taken at home)”. |
Given the high importance of treatment efficacy for Class 1 (efficacy-focused), respondents in this group were largely unwilling to trade off meaningful improvements in chance of response for other benefits. For example, to achieve a 10% improvement in quality of life during response, respondents would only forgo around 1.7% of response probability.
In contrast, Class 2 (convenience- and efficacy-focused) placed less weight on efficacy and were willing to accept substantial reductions in chance of response in exchange for greater convenience or improved quality of life. For instance, participants in this group would forgo up to a 58% chance of response to receive treatment as tablets taken at home rather than as an inpatient hospital therapy. However, it should be noted that confidence intervals around the larger MRS estimates are wide, and these values should be interpreted with appropriate caution.
Respondents in Class 3 (balanced decision-makers) were generally cautious about trading efficacy but would accept moderate reductions to improve quality of life during response, such as 7.5% in chance of response for a 10% improvement in quality of life during response.
Discussion
This study extends the earlier UK analysis20 to include respondents from the USA, France, Germany and Italy. The expanded dataset confirms two central findings: first, that the chance of response is the dominant driver of treatment preferences in this setting among people living with AL internationally; and second, that there is substantial heterogeneity in patient preferences. As in the UK-only analysis, respondents placed the greatest importance on the chance of response, followed by quality of life during response. This finding is consistent with evidence that patients with hematological malignancies often prioritize quality of life and functioning once remission is achieved, over temporary treatment burden.27–29 Duration of response was also valued, although with diminishing marginal importance for longer durations beyond approximately 15 months. This pattern may reflect that the range of durations presented in the DCE (6–18 months) was relatively short and that respondents perceived improvements beyond a certain point as less meaningful.
The latent-class analysis identified three distinct preference profiles. Latent class models are widely used to identify subgroups with distinct preference structures in health preference studies, allowing for richer understanding of preference heterogeneity.30 Two mirrored those previously reported in the UK sample: an efficacy-focused group (Class 1) who prioritized chance of response almost exclusively, and a balanced decision-making group (Class 3) who valued multiple attributes but still ranked efficacy highest. Together these groups accounted for 79% of the full sample. Individuals diagnosed more recently and those with experience of relapse were more likely to belong to the efficacy-focused group, suggesting that recent confrontation with disease progression heightens concern with achieving a treatment response. Similar patterns have been reported in other oncology preferences studies, where respondents in relapse or refractory settings tend to prioritize efficacy outcomes such as progression-free or overall survival, over toxicity or convenience considerations.31 The third group, Class 2 (convenience- and efficacy-focused), was unique to the multi-country analysis. Respondents in this class were disproportionately from the USA and attached high importance to both chance and duration of response. They expressed strong preferences for oral or outpatient treatment over inpatient hospital administration and were willing to forgo substantial improvements in response probability in exchange for greater convenience.
These cross-country differences are noteworthy. Cross-national variation in oncology preferences has been documented in the wider literature, suggesting that health-system design and cultural expectations influence trade-off behavior.31 Notably, oncology treatments are typically approved earlier in the US compared to Europe,32 which could influence patients’ expectations and preferences around treatment. Furthermore, inpatient care within the US healthcare system is associated with significant direct costs to patients33 and may explain the greater aversion to hospital-based treatment. Respondents in the UK and EU3, who face fewer personal costs, were less likely to belong to Class 2 - the group that placed high importance on treatment convenience. This pattern suggests that financial context and healthcare system structure may shape how patients prioritize convenience relative to efficacy.
Exploratory subgroup analyses revealed little variation by AL subtype, except that respondents with APL placed no measurable importance on mode of administration. While this could reflect the relatively standardized treatment paradigm in APL,34 which means that people with APL face fewer trade-offs between competing treatment attributes, this result should be interpreted cautiously given the small sample size (n=28). While some AML preference studies found limited variation in preferences across patient sub-groups (eg., age), there remains little evidence comparing valuations by subtype.17 Regional comparisons confirmed that respondents in the USA placed less emphasis on chance of response and quality of life during treatment, while placing greater weight on duration of response, mode of administration and post-treatment quality of life. Preferences in the UK and EU3 were broadly aligned.
Overall, these findings show that, while people with AL largely prioritize treatments with a higher chance of response, many consider a range of factors, including quality of life and mode of administration. Therefore, although the development and access of clinically effective treatments in the relapsed/refractory settings are a priority, it is important that the broader impact on people with AL is not overlooked. The preference heterogeneity identified within the patient population highlights the importance of individual treatment discussions between patients and clinicians to ensure that patients’ priorities are understood and considered within decision-making. Furthermore, it is important to note that preferences may differ across regions, and treatments that are well suited to people in one country may not be as well suited to people in another. While the evidence in this study is not indication-specific, HTA agencies are increasingly incorporating patient preference data into deliberative processes to contextualize clinical evidence and ensure evaluations reflect outcomes that matter to patients.
Strengths and Limitations
This study followed established best-practice guidance for stated-preference research,35 incorporating formative qualitative work, “think-aloud” cognitive pre-testing,23 and iterative feedback from patient and academic advisory groups. Collaboration with ALAN and Leukemia Care ensured that the survey was relevant, comprehensible and patient-centered.
Nonetheless, several limitations warrant consideration. Recruitment targeted participants across the UK, EU4 and USA, but sample targets for Spain were not achieved, restricting the European analysis to the EU3 (France, Germany and Italy). Recruiting individuals with a rare and severe disease such as AL for online research proved challenging. To facilitate enrolment, no demographic or disease-type quotas were applied, resulting in heterogeneity across regions, for example, 85% of the EU3 patient sample had AML compared to 39% in the USA. These differences limit comparability between regions. In addition, the average participant age (56 years) was lower than the typical age at AML diagnosis (median=69 years),36 likely reflecting greater digital engagement among younger patients and limiting generalizability to the broader population. As with all DCEs, hypothetical choices may not capture the full complexity of real-world treatment decisions, particularly in life-threatening conditions. Furthermore, the treatment status question in the survey did not distinguish between the reasons for not receiving treatment (eg., remission or palliative care), limiting our ability to examine preference heterogeneity within this group.
Future research should seek to replicate these findings in a broader range of countries, including those outside of Europe and North America, to improve the generalizability of preference estimates across different cultural and healthcare contexts.
Conclusion
This study provides new multi-country evidence on how people living with AL evaluate treatment options in the relapsed/refractory setting. Across all regions and subtypes, the chance of achieving a response was the most influential driver of treatment choice, but many respondents also valued treatment convenience and post-treatment quality of life. The findings highlight substantial heterogeneity in patient priorities, underscoring the importance of individual treatment discussions and the need for clinical, regulatory and HTA decisions to reflect outcomes beyond efficacy alone.
Acknowledgments
The authors are grateful to Zack Pemberton-Whiteley for his contributions to the project, to Richard Norman for his review of an earlier draft report, and to the members of the project’s Academic Steering Group (Jayne Galinsky, Phil Kinghorn, Paula Lorgelly, and Mandy Ryan) and Patient Advisory Group (Gillian Adams, Rian Harvey, and Gill Murphy), as well as ALAN’s Steering Committee, for their input at various stages of the project. The authors are also grateful to the many individuals who participated in the research activities.
Aspects of this work have been previously presented and published. Formative qualitative research underpinning this study was presented at the American Society of Hematology (ASH) Annual Meeting 2023, with the abstract published in Blood [doi:10.1182/blood-2023-172871]. The UK results were presented at the European Hematology Association (EHA) Annual Congress 2024, with the abstract published in HemaSphere [doi:10.1002/hem3.104]. The UK results were published in full in this journal in 2024 [doi:10.2147/PPA.S442530]. The US results were accepted for publication as an abstract in Blood at ASH 2025 [doi:10.1182/blood-2025-7949]. The full multinational findings were published in an earlier working paper by ALAN and OHE in October 2025 [https://www.ohe.org/publications/patient-preferences-for-treatment-in-relapsed-refractory-acute-leukemia/].
Funding
This project was funded by the Acute Leukemia Advocates Network (ALAN).
Disclosure
Hannah Hussain, David Mott and Chris Skedgel are employees of the Office of Health Economics (OHE), a registered charity, and an Independent Research Organisation, which receives funding from a variety of private and public sector sources. Jake Hitch and Sulayman Chowdhury were employees of OHE when the manuscript was originally prepared. Hannah Hussain, Jake Hitch, Sulayman Chowdhury, David Mott, and Chris Skedgel report grants from ALAN to OHE during the conduct of this study. Samantha Nier reports consultancy fees from ALAN during the conduct of this study. ALAN receives unrestricted grant funding from a range of pharmaceutical companies. The authors report no other conflicts of interest in this work.
References
1. Okikiolu J, Dillon R, Raj K. Acute leukaemia. Medicine. 2021;49(5):274–13. doi:10.1016/j.mpmed.2021.02.004
2. Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136–1152. doi:10.1056/NEJMra1406184
3. Terwilliger T, Abdul-Hay M. Acute lymphoblastic leukemia: a comprehensive review and 2017 update. Blood Cancer J. 2017;7(6):e577–e577. doi:10.1038/bcj.2017.53
4. Han X, Yun Z, Liu Z, et al. Global, regional, and national burden of acute leukemia and its risk factors from 1990 to 2021 and predictions to 2040: findings from the global burden of disease study 2021. Biomed Eng Online. 2025;24(1):72. doi:10.1186/s12938-025-01403-7
5. Chennamadhavuni A, Iyengar V, Mukkamalla SKR, Shimanovsky A. Leukemia. In: StatPearls [Internet]. StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK560490/.
6. Shephard EA, Neal RD, Rose PW, Walter FM, Hamilton W. Symptoms of adult chronic and acute leukaemia before diagnosis: large primary care case-control studies using electronic records. Br J Gen Pract. 2016;66(644):e182–e188. doi:10.3399/bjgp16X6839897.
7. Lee JB, Vasic D, Kang H, Fang KKL, Zhang L. State-of-Art of cellular therapy for acute leukemia. Int J Mol Sci. 2021;22(9):4590. doi:10.3390/ijms22094590
8. Oliva EN, Ionova T, Nier S, et al. Disease and treatment burden in patients with leukaemia: family members/partner perspective. Front Hematol. 2025;4:1570055. doi:10.3389/frhem.2025.1570055
9. Pemberton-Whiteley Z, Nier S, Geissler J, et al. Understanding quality of life in patients with acute leukemia, a global survey. J Patient-Centered Res Rev. 2023;10(1):21–30. doi:10.17294/2330-0698.1951
10. Shahswar R, Gabdoulline R, Krueger K, et al. A novel prognostic risk model for patients with refractory/relapsed acute myeloid leukemia receiving venetoclax plus hypomethylating agents. Leukemia. 2025;39(3):614–622. doi:10.1038/s41375-024-02501-6
11. Bataller A, Kantarjian H, Bazinet A, et al. Outcomes and genetic dynamics of acute myeloid leukemia at first relapse. Haematologica. 2024;109(11):3543–3556. doi:10.3324/haematol.2024.285057
12. Jabbour E, Pui CH, Kantarjian H. Progress and innovations in the management of adult acute lymphoblastic leukemia. JAMA Oncol. 2018;4(10):1413–1420. doi:10.1001/jamaoncol.2018.1915
13. Mott DJ. Incorporating quantitative patient preference data into healthcare decision making processes: is HTA falling behind? Patient. 2018;11(3):249–252. doi:10/gdtkc6
14. Bouvy JC, Cowie L, Lovett R, Morrison D, Livingstone H, Crabb N. Use of patient preference studies in HTA decision making: a NICE perspective. Patient. 2020;13(2):145–149. doi:10.1007/s40271-019-00408-4
15. van Overbeeke E, Forrester V, Simoens S, Huys I. Use of patient preferences in health technology assessment: perspectives of Canadian, Belgian and German HTA representatives. Patient. 2021;14(1):119–128. doi:10.1007/s40271-020-00449-0
16. Saini L, Griffin JD, Pandya BJ, et al. Patient and physician preferences for acute myeloid leukemia maintenance treatments following hematopoietic stem cell transplantation. Patient Prefer Adherence. 2023;17:2805–2819. doi:10.2147/PPA.S421871
17. Richardson DR, Crossnohere NL, Seo J, et al. Age at diagnosis and patient preferences for treatment outcomes in AML: a discrete choice experiment to explore meaningful benefits. Cancer Epidemiol Biomarkers Prev. 2020;29(5):942–948. doi:10.1158/1055-9965.EPI-19-1277
18. LoCastro M, Wang Y, Sanapala C, et al. Patient preferences, regret, and health-related quality of life among older adults with acute myeloid leukemia: a pilot longitudinal study. J Geriatr Oncol. 2023;14(5):101529. doi:10.1016/j.jgo.2023.101529
19. Seo J, Smith BD, Estey E, Voyard E, O’ Donoghue B, Bridges JFP. Developing an instrument to assess patient preferences for benefits and risks of treating acute myeloid leukemia to promote patient-focused drug development. Curr Med Res Opin. 2018;34(12):2031–2039. doi:10.1080/03007995.2018.1456414
20. Mott D, Hitch J, Nier S, Pemberton-Whiteley Z, Skedgel C. Patient preferences for treatment in relapsed/refractory acute leukemia in the United Kingdom: a discrete choice experiment. Patient Prefer Adherence. 2024;18:1243–1255. doi:10.2147/ppa.s442530
21. Hollin IL, Craig BM, Coast J, et al. Reporting formative qualitative research to support the development of quantitative preference study protocols and corresponding survey instruments: guidelines for authors and reviewers. Patient. 2020;13(1):121–136. doi:10.1007/s40271-019-00401-x
22. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
23. Campoamor NB, Guerrini CJ, Brooks WB, Bridges JFP, Crossnohere NL. Pretesting discrete-choice experiments: a guide for researchers. Patient - Patient-Centered Outcomes Res. 2024;17(2):109–120. doi:10.1007/s40271-024-00672-z
24. Mott D, Hussain H, Chowdhury S, Nier S, Skedgel C. Understanding the preferences of people with acute leukemia for different health outcomes. Office of Health Economics; 2025. Available from: https://www.ohe.org/publications/understanding-the-preferences-of-people-with-acute-leukemia-for-different-health-outcomes/.
25. Mott DJ, Chami N, Tervonen T. Reporting quality of marginal rates of substitution in discrete choice experiments that elicit patient preferences. Value Health. 2020;23(8):979–984. doi:10.1016/j.jval.2020.04.1831
26. Announcing Stata Release 15. Available from: https://www.stata.com/stata15/.
27. Schölvinck AFM, de Graaff BMB, van den Beld MJ, Broerse JEW. Research in haematological cancers: what do patients in the Netherlands prioritise? Eur J Cancer Care. 2019;28(2):e12989. doi:10.1111/ecc.12989
28. Fifer S, Godsell J, Opat S, et al. Understanding the experience, treatment preferences and goals of people living with chronic lymphocytic leukemia (CLL) in Australia. BMC Cancer. 2024;24(1):831. doi:10.1186/s12885-024-12589-9
29. Le H, Ryan K, Wahlstrom SK, et al. Oncologist and patient preferences for novel agents in first-line treatment for chronic lymphocytic leukemia: commonalities and disconnects. Patient Prefer Adherence. 2021;15:99–110. doi:10.2147/PPA.S289139
30. Zhou M, Thayer WM, Bridges JFP. Using latent class analysis to model preference heterogeneity in health: a systematic review. PharmacoEconomics. 2018;36(2):175–187. doi:10.1007/s40273-017-0575-4
31. Gribben JG, Bachy E, Ray M, et al. Patient and physician treatment preferences in relapsed/refractory follicular lymphoma: a discrete choice experiment in the United States, United Kingdom, France, Germany, Brazil, and Japan. Front Oncol. 2025;15:1589722. doi:10.3389/fonc.2025.1589722
32. Lythgoe MP, Desai A, Gyawali B, et al. Cancer therapy approval timings, review speed, and Publication of Pivotal Registration Trials in the US and Europe, 2010-2019. JAMA Network Open. 2022;5(6):e2216183. doi:10.1001/jamanetworkopen.2022.16183
33. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA. 2018;319(10):1024. doi:10.1001/jama.2018.1150
34. Iyer SG, Elias L, Stanchina M, Watts J. The treatment of acute promyelocytic leukemia in 2023: paradigm, advances, and future directions. Front Oncol. 2023;12:1062524. doi:10.3389/fonc.2022.1062524
35. Bridges JFP, de Bekker-Grob EW, Hauber B, et al. A roadmap for increasing the usefulness and impact of patient-preference studies in decision making in health: a good practices report of an ISPOR Task Force. Value Health. 2023;26(2):153–162. doi:10.1016/j.jval.2022.12.004
36. Krayem B, Frisch A, Horowitz N. Novel therapies for acute myeloid leukemia. Does age still matter? Blood Rev. 2025;74:101317. doi:10.1016/j.blre.2025.101317
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient Preference for Self-Injection Devices in Rheumatoid Arthritis: A Discrete Choice Experiment in China
Wei Y, Zhao J, Ming J, Zhang X, Chen Y
Patient Preference and Adherence 2022, 16:2387-2398
Published Date: 31 August 2022
The Impact of Substantial Improvements in HbA1c and Weight Loss on the Medication Preferences of People with Type 2 Diabetes
Gelhorn HL, Osumili B, Brown K, Ross MM, Schulz A, Fernandez G, Boye KS
Patient Preference and Adherence 2023, 17:793-805
Published Date: 22 March 2023
Understanding Treatment Preferences Among People Living with HIV in Australia: A Discrete Choice Experiment
Fifer S, Kularatne T, Tan M, Drummond F, Rule J
Patient Preference and Adherence 2023, 17:1825-1843
Published Date: 26 July 2023
Eliciting Depression Patients’ Preferences for Medication Management: A Protocol for Discrete Choice Experiment
Xie P, Li HQ, Peng WL, Yang H
Patient Preference and Adherence 2024, 18:289-300
Published Date: 2 February 2024
Patient Preferences for Treatment in Relapsed/Refractory Acute Leukemia in the United Kingdom: A Discrete Choice Experiment
Mott DJ, Hitch J, Nier S, Pemberton-Whiteley Z, Skedgel C
Patient Preference and Adherence 2024, 18:1243-1255
Published Date: 17 June 2024