")
Back to Journals » Patient Preference and Adherence » Volume 17
The Impact of Substantial Improvements in HbA1c and Weight Loss on the Medication Preferences of People with Type 2 Diabetes
Authors Gelhorn HL, Osumili B , Brown K, Ross MM , Schulz A, Fernandez G, Boye KS
Received 14 December 2022
Accepted for publication 10 March 2023
Published 22 March 2023 Volume 2023:17 Pages 793—805
DOI https://doi.org/10.2147/PPA.S401465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Heather L Gelhorn,1 Beatrice Osumili,2 Katelyn Brown,2 Melissa M Ross,1 Andrea Schulz,1 Gabriela Fernandez,1 Kristina S Boye2
1Patient-Centered Research, Evidera, Inc., Bethesda, MD, USA; 2Value, Evidence, and Outcomes, Eli Lilly and Company, Indianapolis, IN, USA
Correspondence: Heather L Gelhorn, Patient-Centered Research, Evidera, Inc., 7101 Wisconsin Avenue, Suite 1400, Bethesda, MD, 20814, USA, Tel +1-970-363-7333, Email [email protected]
Purpose: To quantify the preferences of people with type 2 diabetes (T2D) for treatment attributes of a glucose-dependent insulinotropic polypeptide (GIP)/glucagon-like peptide-1 (GLP-1) receptor agonist (RA) versus an injectable GLP-1 RA medication profile.
Patients and Methods: Injection-naive people taking oral medications for T2D in the US and UK completed a web survey including a discrete choice experiment to quantify patients’ preferences for five treatment attributes: delivery system, frequency of nausea, frequency of hypoglycemia, HbA1c reduction, and weight reduction. Attributes and levels were based on head-to-head clinical trial data of tirzepatide 5mg, 10mg, and 15mg versus semaglutide 1mg. Preference data were analyzed separately by country using multinomial mixed logit (MXL) models. MXL parameters were used to estimate the predicted preference for each tirzepatide dose versus semaglutide 1mg. Direct preferences for each dose of tirzepatide versus semaglutide 1mg were elicited.
Results: Participants (N=620) in the US (N=301) and UK (N=319) were 50.8% and 50.5% female with mean ages of 60.7 years and 58.9 years, respectively. The order and magnitude of relative attribute importance (RAI) scores differed between countries. HbA1c reduction (26.3%) had the greatest impact on US participants’ preferences, and hypoglycemia (32.8%) did among UK participants. Attribute-level marginal utility results indicated preferences for greater HbA1c improvements, the single-use pre-filled pen, lower hypoglycemia, greater weight reductions, and lower frequency of nausea. Assuming the availability of only tirzepatide or semaglutide 1mg, the predicted preference for tirzepatide (5, 10, and 15mg) in the US is 95.6% (vs 4.4% for semaglutide 1mg) and in the UK was 86.3% (vs 13.7% for semaglutide 1mg).
Conclusion: HbA1c reduction, frequency of hypoglycemia, and weight reduction are key drivers of preferences among people with T2D when considering medication options. Overall, people with T2D are likely to prefer the tirzepatide over the semaglutide 1mg medication profiles.
Keywords: patient preferences, discrete choice experiment, patient perspective, incretin
Introduction
The prevalence of diabetes has been increasing worldwide for the past several decades,1 reaching over 37 million people in the US2 and approximately five million people in the UK.3 Over 95% of those with diabetes are classified as having type 2 diabetes (T2D), which is closely associated with higher body mass index (BMI) and low levels of physical activity.1
T2D is diagnosed and monitored by testing glycated hemoglobin A1c (HbA1c), which indicates average blood sugar level over the past few months; normal concentration of glucose in the blood is reflected by HbA1c levels of less than 5.7%, 5.7% to 6.4% reflects prediabetes, and 6.5% or greater reflects T2D.4,5 As diabetes progresses, it can lead to a variety of health complications, including cardiovascular events, neuropathy, kidney failure, and diabetic retinopathy that can result in blindness. To prevent these complications, tight glycemic control and weight management is recommended, while minimizing the risk of hypoglycemia.6,7 First-line therapy depends on comorbidities and patient factors, but generally includes metformin and comprehensive lifestyle modification.8
In addition to lifestyle modifications, there are several pharmacologic approaches to glycemic management of T2D. Incretin-based treatments (for example, glucagon-like peptide-1 [GLP-1] receptor agonists9) offer improved glycemic control, low risk of hypoglycemia, and the potential for clinically relevant weight loss.6 Tirzepatide, a novel glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA, has been approved for the treatment of T2D and is in development for chronic weight management.10,11 Additionally, tirzepatide has been associated with greater reductions in HbA1c and weight loss compared to several other T2D medications, such as basal insulin and GLP-1 RAs.12–14
Semaglutide has been approved for the treatment of T2D and chronic weight management.15,16 In a Phase 3, head-to-head study comparing three doses (5mg, 10mg, and 15mg) of tirzepatide to 1mg semaglutide,17 all doses of tirzepatide were found to be superior to semaglutide 1mg with respect to HbA1c reduction; half of the participants who received tirzepatide 15mg achieved an HbA1c of less than 5.7%, which is considered normoglycemia (ie, normal blood glucose levels). Additionally, all three tirzepatide doses were superior to semaglutide 1mg with respect to weight loss, with participants receiving the 15mg dose of tirzepatide achieving nearly double the weight loss of those receiving the 1mg dose of semaglutide.17 Similar to the selective GLP-1 RA class, most of the adverse events (AEs) associated with tirzepatide were gastrointestinal (GI)-related, and the majority were mild to moderate in severity. Treatment discontinuation rates due to AEs were 5.1% (tirzepatide 5mg), 7.7% (tirzepatide 10mg), 7.9% (tirzepatide 15mg), and 3.8% (injectable semaglutide 1mg). Hypoglycemia <54 mg/dL was reported in 0.6% (tirzepatide 5mg), 0.2% (tirzepatide 10mg), and 1.7% (tirzepatide 15mg) of participants in the tirzepatide-treated arms, and in 0.4% of participants in the semaglutide 1mg-treated arm.17
Prior research has demonstrated that achieving near normoglycemia (defined as HbA1c levels near 5.7%) is considered by the majority of people with T2D to be a paradigm shift and viewed as both meaningful and important.18,19 Thus, the new GIP/GLP-1 RA could provide meaningful benefits for people with T2D, given both the potential for significant reductions in HbA1c and weight loss, and also the association between T2D, obesity and negative health outcomes. However, it is unknown how people with T2D value the substantial reductions in HbA1c and weight loss. Furthermore, with the recent introduction of tirzepatide, it is unknown how people with T2D would trade-off between the benefits (including HbA1c reduction and weight loss), the risks (including GI side effects and hypoglycemia), and the administration procedures associated with this new treatment compared with those of currently available T2D treatments. This study aimed to quantify the preferences of people with T2D for the treatment attributes of a GIP/GLP-1 RA (tirzepatide) versus a GLP-1 RA (semaglutide 1mg) using a discrete choice experiment (DCE).
Materials and Methods
Overall Design and Sample
This was a cross-sectional online survey that included a DCE and was conducted among people aged 18 years and older with T2D in the US and UK. The study included a pilot testing phase prior to the main online survey data collection phase, including qualitative and quantitative components.
To be eligible for all study phases, participants had to be a resident of the US or UK, at least 18 years old, report having been diagnosed with T2D by a medical doctor, currently taking at least one oral medication to treat their T2D, and naïve to injectable medications. Individuals were excluded from the study if they had type 1 or gestational diabetes or if they were employed in the pharmaceutical industry or in a position with a direct role in treating people with diabetes. Individuals with established cardiovascular disease (eg, prior stroke, heart attack, or chronic heart failure) were also excluded to align with the SURPASS-2 patient population.17 For the qualitative pilot, individuals were also excluded if they had a cognitive disability, visual impairment, or hearing difficulty.
Participants were recruited by a panel research company specializing in health outcomes research. Invitations to participate were sent via email and social media advertisements, targeting people who had been diagnosed with T2D. Efforts were made to enroll a sample in each country composed of approximately 50% women, and 13% participants aged 18–44 years, 44% participants aged 45–64 years, and 43% participants aged >65 to match the current distribution of T2D.2 All participants provided electronic informed consent prior to participation and were remunerated for their participation.
Survey
The online survey consisted of four sections: 1) Warm-up and Experience with T2D Questions; 2) Treatment Attributes and Levels; 3) DCE and Supplementary Questions; and 4) Sociodemographic and Clinical Form. Within the DCE, participants were asked to choose between two hypothetical treatment options (Figure 1), which were composed of varying levels of a common set of five attributes: 1) HbA1c reduction, 2) weight reduction, 3) type of delivery system, 4) frequency of nausea, and 5) frequency of hypoglycemia/low blood sugar. These attributes were selected because they are key differentiating characteristics and are consistent with relevant attributes included in previous studies of medication preferences among T2D populations.9,20–28 The attribute levels were defined based on the results of the SURPASS-2 trial (Table 1) which was a direct head-to-head study of tirzepatide 5mg, 10mg, and 15mg versus semaglutide 1mg.17 The attribute levels shown within each treatment profile in the DCE were systematically varied based on an experimental design algorithm.
 |
Table 1 DCE Attributes and Levels |
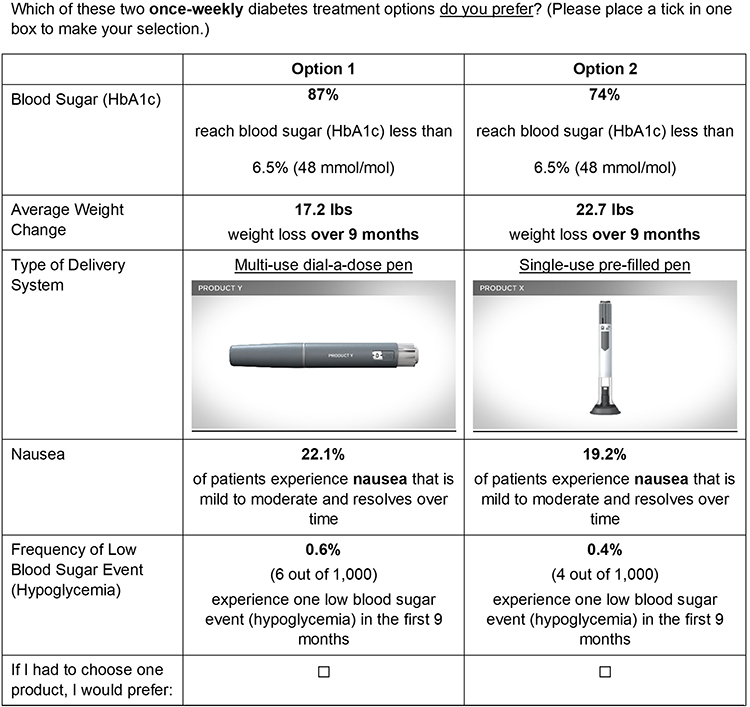 |
Figure 1 Example DCE choice task (UK sample). Abbreviation: HbA1c, glycated hemoglobin A1C. |
The DCE attribute levels were the same for UK and US participants, except for blood sugar (HbA1c) and weight reduction: levels for these two attributes were based on efficacy estimands from SURPASS-2 in the UK and on treatment regimen estimands from SURPASS-2 in the US to reflect country-specific prescribing information. Additionally, HbA1c was reported only as a percent for US participants, but as a percent and mmol/mol for UK participants. Weight loss was presented in units of pounds for US participants, but the option was given to UK participants for representation in pounds, kilograms, or stones.
Prior to completing the DCE questions, participants reviewed written descriptions of the medication attributes. To illustrate the two delivery systems, participants watched two brief (approximately three minutes) videos demonstrating the use of each delivery system. These videos were developed based on the Instructions for Use (IFU) documentation for each product.15,29 Participants were not permitted to fast forward through the videos or to proceed to the next question without first viewing the videos, however they could replay the videos as much as they wanted to for reference during the survey. The order in which these videos were shown to each participant was randomized. The tirzepatide and semaglutide devices were anonymized and only referred to as either Product X or Product Y.
Participants completed nine experimental choice tasks that were used to estimate preferences and five non-experimental, fixed-choice tasks that were embedded within the DCE. The order of the experimental choice tasks, the order of the two hypothetical treatment options within each choice task, and the order of the attributes within each choice task was randomized between participants. Two of the non-experimental questions assessed internal validity: a repeated-choice task to test choice stability and a dominance test to assess participants’ attentiveness. Within the dominance test, each attribute level presented in one option was designed to be equal or superior to each attribute level in the alternative. The other three non-experimental questions appeared after all other choice tasks and were formatted identically to the DCE questions; these were direct comparisons of the anonymized profiles for each dose of tirzepatide (5mg, 10mg, 15mg) versus the profile for semaglutide (1mg).
Pilot Study
Virtual, one-on-one qualitative pilot interviews were conducted with 11 patients with T2D in the US and 10 in the UK to assess the relevance of the attributes and levels included in the DCE, as well as the general clarity, functionality, and understandability of the web survey. Based on the feedback from the qualitative pilot participants, minor revisions were made to improve the clarity of the survey. Subsequent to the qualitative pilot, a quantitative pilot was conducted among 50 patients with T2D in the US and 50 in the UK. These participants completed the web survey, including the DCE, to ensure the functionality of the web survey and the DCE design.
Statistical Analyses
All data were analyzed separately for the US and UK samples using STATA statistical software version 15 (Timberlake Consultants, Richmond, UK). All statistical tests were two-sided, using a significance level of 0.05.
Descriptive statistics (eg, mean, median, standard deviation [SD], range for continuous variables, frequency and percentages for categorical variables) were used to characterize the sample based on sociodemographic and clinical characteristics. Additionally, descriptive statistics were used to analyze the internal validity assessments and to summarize responses to the three direct comparison questions that were used to estimate the proportion of participants preferring the profile for each dose of tirzepatide compared with the profile for semaglutide 1mg.
The preference data were analyzed using a mixed logit model (MXL), which is similar to a multinomial logit model, but relaxes the assumption that all participants have the same preferences by introducing random effects into the modelling framework. The MXL was parameterized with HbA1c, weight, and hypoglycemia linearly coded and nausea and device type dummy coded. T-tests were used to determine whether estimated parameters were significantly different from zero. Only data from the nine experimental choice tasks were used in the estimation of preferences. In addition, the relative attribute importance (RAI) was calculated to evaluate the importance of each attribute relative to all other attributes. RAI is calculated as the range of an attribute’s marginal utility divided by the sum of all attributes’ marginal utility ranges.
The predicted preference, or the proportion of participants predicted to prefer each of the medication profiles, and the associated standard errors, were calculated using the model parameter estimates and the performance characteristics of each dose of tirzepatide and semaglutide from the head-to-head trial17 to estimate the predicted probability of preferring each medication profile based on the attributes included in the DCE.
Results
Sample
A total of 620 people with T2D (US=301; UK=319) participated in the main survey between June and August 2022. About half of the participants were female (US: n=153 [50.8%]; UK: n=161 [50.5%]), with a mean age of 60.7 years in the US and 58.9 years in the UK (Table 2). Most participants reported their racial background to be white (US: n=270 [89.7%], UK: n=296 [92.8%]), and almost half reported being retired (US: n=140 [46.5%]; UK: n=145 [45.5%]).
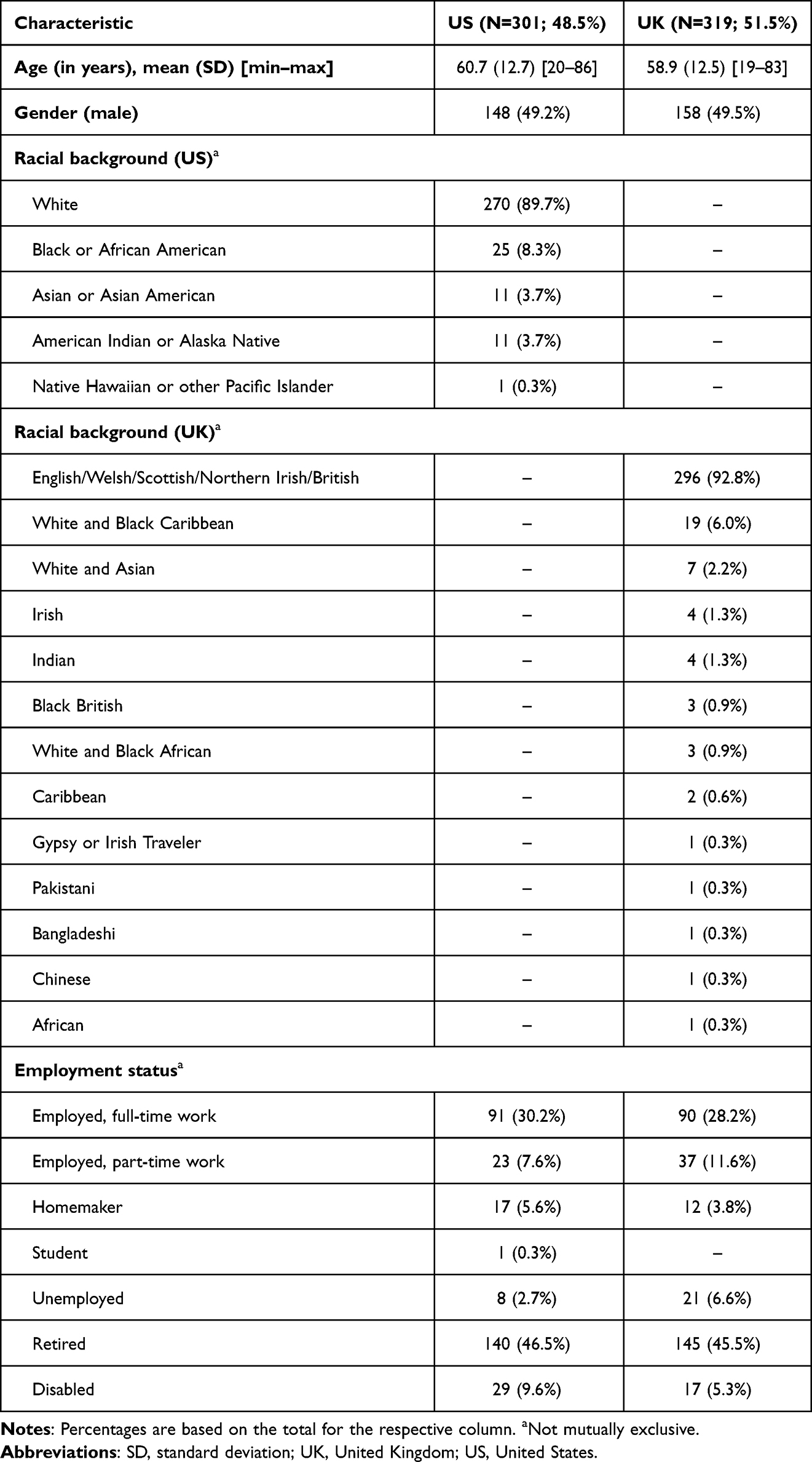 |
Table 2 Sample Sociodemographic Characteristics |
The clinical characteristics of the participants are presented in Table 3. The mean self-reported BMI for participants was 30.9 among US participants and 29.5 among UK participants. There was a range in time since T2D diagnosis, with approximately one-third of the US sample reporting diagnosis within the past 5 years (33.9%), 5 to 10 years ago (32.9%), and ≥11 years ago (33.2%). Slightly more UK participants (42.0%) were diagnosed within the past 5 years, with 25.7% and 32.3% being diagnosed 5 to 10 and ≥11 years ago, respectively. The majority of US participants (n=151, 50.2%) had an HbA1c of 5.00% to 6.99% (31–52 mmol/mol), whereas among UK participants, 37.6% (n=120) had an HbA1c of 7.00–9.99 and 25.4% (n=81) did not know their HbA1c. Participants reported a range of comorbid conditions, most commonly hypertension (45.8%).
 |
Table 3 Sample Self-Reported Clinical Characteristics |
DCE Internal Validity
Internal validity tests were used to evaluate the DCE data quality. Most participants passed both the dominance test (US: n=248 [82.4%]; UK: n=269 [84.3%]) and the stability test (US: n=257 [85.4%]; UK: n=258 [80.9%]). Almost all participants had response patterns indicating that they were appropriately attending to the choice tasks, as they did not always choose Option 1 or Option 2 (US: n=289 [96.0%]; UK: n=300 [94.0%]). Because these results are in line with other health DCEs in the literature30 and there is evidence that suggests that excluding participants based on the results of internal validity tests can induce selection bias and reduce statistical efficiency,31 all participants who completed the survey were included in the final analyses.
Participant Preferences
The RAI scores derived from participants’ choices in the DCE are presented in Figure 2. RAI indicates how much changes in a particular attribute impacted participants’ decisions relative to changes in the other attributes. Among US participants, HbA1c reduction was the most important driver of preferences (26.3%; 95% confidence interval [CI]: 20.5–32.1%), followed by delivery system (20.9%; 95% CI: 13.5–28.3%). Among UK participants, hypoglycemia was the most important attribute (32.8%; 95% CI: 25.7–40.0%) and HbA1c reduction the second most important (21.6%; 95% CI: 15.3–27.9%), with these two attributes making up over half of the RAI for UK participants.
 |
Figure 2 Relative attribute importance by country. Abbreviation: HbA1c, glycated hemoglobin A1C. |
The marginal utilities for each attribute level are plotted for the US and UK samples in Figure 3. For both samples, when choosing a T2D treatment, participants on average preferred greater HbA1c improvements; the single-use, pre-filled pen over the multi-use, dial-a-dose pen; lower risk of hypoglycemia; greater weight reductions; and lower frequency of nausea.
 |
Figure 3 Marginal utilities by country. *p < 0.05; **p < 0.01; ***p < 0.001. Abbreviations: CI, confidence interval; HbA1c, glycated hemoglobin A1C; MLE, maximum likelihood estimation. |
Predicted Preferences for Tirzepatide vs Semaglutide 1mg Profiles
Predicted choice probability was also estimated for each dose of tirzepatide and semaglutide 1mg using the results of the DCE analyses (Figure 4). Assuming the availability of only tirzepatide or semaglutide 1mg, the predicted preference of tirzepatide in the US was 95.6% for the three doses combined (vs 4.4% for semaglutide 1mg) and in the UK was 86.3% for the three doses combined (vs 13.7% for semaglutide 1mg). Additionally, in each of the three non-experimental choice tasks in which participants were asked to choose between a treatment profile representing each of the tirzepatide doses (5mg, 10mg, and 15mg) vs a treatment profile representing semaglutide 1mg, more participants in the US preferred each dose of tirzepatide over semaglutide and more participants in the UK preferred tirzepatide 5mg and 10mg over semaglutide (all p<0.001) (Supplementary Figure S1).
 |
Figure 4 Predicted preference for tirzepatide and semaglutide. Abbreviations: UK, United Kingdom; US, United States. |
Discussion
The treatment landscape for T2D continues to evolve, with newer medications presenting different options to patients and their physicians. The magnitude of decreases in HbA1c and weight loss associated with the novel GIP/GLP-1 RA medication have not been seen with prior diabetes treatments. Therefore, it is important to understand how these larger effects are valued by patients in the context of their medication decisions and relative to other important treatment attributes. Prior qualitative research has demonstrated that many of the trial participants who have taken the new GIP/GLP-1 RA medication have noticed improved glycemic control, weight loss, decreased appetite, and/or increased energy and that these changes were meaningful to them.32 However, we do not know the relative importance of the changes in the various outcomes.
Based on the results of the current study, we conclude that overall, participants from both the US and UK preferred greater reductions in HbA1c, lower rates of hypoglycemia, greater weight loss, the single-use, pre-filled pen, and lower rates of nausea. This study demonstrated that the treatment preferences of individuals with T2D are greatly influenced by the ability of the treatment to reduce HbA1c. Among US participants, reduction in HbA1c was the single most impactful attribute on preferences, and among UK participants, it was the second most impactful after hypoglycemia. This result is not surprising given past research has demonstrated people with T2D in the US and UK place a great deal of importance on reaching near normoglycemia and associate this with a range of positive impacts.18,19 Weight reduction also influenced preferences; however, this attribute was secondary to HbA1c reduction in both countries (US RAI: 18.3%; UK RAI: 17.3%). The RAI for delivery system was higher in the US (RAI: 20.9%) than in the UK (RAI: 9.2%), with patients in both countries preferring the single-use, pre-filled pen over the multi-use, dial-a-dose pen.
There were differences with respect to how changes in attributes influenced preferences of people with T2D in the US compared to the UK. First, improvements in HbA1c had a greater impact on preferences in the US. People with T2D in the UK tend to be less aware of their current HbA1c levels, for example, 8.0% of the US sample compared to 25.4% of the UK sample participating in the current study did not know their current HbA1c, and thus improvements in this attribute may be less salient to people in the UK. Second, hypoglycemia had a greater impact on preferences in the UK. This finding may reflect the fact that people with T2D in the UK are subject to certain restrictions, for example from driving, if they have a history of hypoglycemic events in the past year.33 Further research should investigate the extent to which concerns related to maintaining a license to operate a vehicle might be related to preferences for avoiding medications associated with greater risk of hypoglycemia.
Perhaps not surprisingly, the results of the current study differ from those of prior studies.24,25 In several prior studies, frequency of administration (daily vs weekly) was included as an attribute, as this was a relevant differentiator for the medications of interest. This particular attribute was often of high importance to participants. However, frequency of administration was not a factor in this study given both products are dosed weekly. In addition, the attributes of greatest importance in the current study (eg, HbA1c reduction, hypoglycemia and weight reduction) were of much less importance in the prior studies. This is likely because the magnitude of the improvements in each of these attributes was much larger in this study than in those prior, reflecting the current treatment landscape. Thus, when considering much larger and more salient changes from the patient perspective, this resulted in significantly stronger preferences for improvements in these attributes.
Prior research has demonstrated that improvements in HbA1c, and specifically reaching near normoglycemia, is both meaningful and important to people with T2D in the US and UK.18,19 This study demonstrates that the properties of tirzepatide, a novel, weekly, GIP/GLP-1 RA for T2D are valuable to people with T2D living in the US and UK. The tirzepatide efficacy and safety profiles differ from those of other T2D treatments that are currently available. Most notably, tirzepatide results in substantial reductions in HbA1c and significantly greater weight reduction than other treatments. This study demonstrated the importance of these benefits from the patient perspective, particularly when the magnitude of the improvements is large.
This information may be useful for clinicians when discussing available treatment options with their patients with T2D. This could lead to greater treatment satisfaction, and ultimately better adherence, although further research is needed to determine whether treatments that better match patients’ preferences result in better adherence.
There are some limitations which should be considered when interpreting the results of this study. First, all data were self-reported, including participants’ clinical data. Second, participants in this study were people with T2D taking oral medications and who were naïve to injectable medications. While the sample was fairly diverse, it was not necessarily fully representative of the US or UK T2D populations. The preferences of the participants in this study may not be generalizable to all people with T2D. Third, the SURPASS-2 trial did not assess long-term complications associated with T2D, and therefore these attributes, such as outcomes related to cardiovascular or kidney disease, were not included in this study.
Conclusion
While several studies have previously examined the treatment preferences of people with T2D, this study added to the existing literature by highlighting how the greater magnitude of HbA1c decrease and weight loss associated with the new class of GIP/GLP-1 RA medication impacts the preferences of people with T2D. This study demonstrated that HbA1c reduction, weight reduction and frequency of hypoglycemia are key drivers of the preferences of people with T2D. Overall, people with T2D are likely to prefer medication profiles associated with tirzepatide, a novel GIP/GLP-1 RA over semaglutide 1mg, a GLP-1 RA.
Abbreviations
AE, adverse event; BMI, body mass index; CI, confidence interval; DCE, discrete choice experiment; GI, gastrointestinal; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide 1; HbA1c, glycated hemoglobin A1c; IFU, Instructions for Use; MXL, mixed logit model; RA, receptor agonist; RAI, relative attribute importance; SD, standard deviation; SGLT2, sodium–glucose cotransporter 2; T2D, type 2 diabetes.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study received approval from Ethical & Independent Review Services [Study Number: 21181-01] on October 29, 2021. E&I is a central independent review board (IRB) that was used because there are not internal IRBs at the authors’ institutions. The study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments.
Acknowledgments
Editorial assistance for manuscript preparation was provided by Caroline Cole.
Funding
This study was funded by Eli Lilly and Company, Indianapolis, USA.
Disclosure
Heather L Gelhorn is an employee of Evidera, a consultancy that provides scientific consulting services to pharmaceutical companies. Melissa M Ross is an employee of Evidera, a consultancy that provides scientific consulting services to pharmaceutical companies. Andrea Schulz is an employee of Evidera, a consultancy that provides scientific consulting services to pharmaceutical companies. Gabriela Fernandez is an employee of Evidera, a consultancy that provides scientific consulting services to pharmaceutical companies. Beatrice Osumili is an employee and shareholder of Eli Lilly and Company. Katelyn Brown is an employee and shareholder of Eli Lilly and Company. Kristina S Boye is an employee and shareholder of Eli Lilly and Company. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Diabetes; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes.
2. Centers for Disease Control and Prevention. National diabetes statistics report; 2022. Available from: https://www.cdc.gov/diabetes/data/statistics-report/index.html.
3. Diabetes UK. Diabetes statistics; 2022. Available from: https://www.diabetes.org.uk/professionals/position-statements-reports/statistics.
4. Centers for Disease Control and Prevention. Type 2 diabetes; 2022. Available from: https://www.cdc.gov/diabetes/basics/type2.html.
5. American Diabetes Association. Understanding A1C: diagnosis; 2022. Available from: https://www.diabetes.org/diabetes/a1c.
6. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–2786. doi:10.2337/dci22-0034
7. ElSayed NA, Aleppo G, Aroda VR, et al. 9. pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S140–S157. doi:10.2337/dc23-S009
8. American Diabetes Association. Introduction: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S1–S2. doi:10.2337/dc19-Sint01
9. Igarashi A, Bekker Hansen B, Langer J, et al. Preference for oral and injectable GLP-1 RA therapy profiles in Japanese patients with type 2 diabetes: a discrete choice experiment. Adv Ther. 2021;38(1):721–738. doi:10.1007/s12325-020-01561-1
10. European Medicines Agency, Eli Lilly and Company. Mounjaro solution for injection in pre-filled pen [Summary of product characteristics]. Available from: https://ec.europa.eu/health/documents/community-register/2022/20220915156773/anx_156773_en.pdf.
11. US Food and Drug Administration, Eli Lilly and Company. MOUNJAROTM (tirzepatide) injection, for subcutaneous use [Package insert]; 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215866s000lbl.pdf.
12. Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4): a randomised, open-label, parallel-group, multicentre, phase 3 trial. Lancet. 2021;398(10313):1811–1824. doi:10.1016/S0140-6736(21)02188-7
13. Frias JP, Nauck MA, Van J, et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: a randomised, placebo-controlled and active comparator-controlled Phase 2 trial. Lancet. 2018;392(10160):2180–2193. doi:10.1016/S0140-6736(18)32260-8
14. Ludvik B, Giorgino F, Jodar E, et al. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial. Lancet. 2021;398(10300):583–598. doi:10.1016/S0140-6736(21)01443-4
15. Novo Nordisk. Ozempic (semaglutide) injection, for subcutaneous use. In: Highlights of Prescribing Information. Novo Nordisk; 2017.
16. European Medicines Agency (EMA). Ozempic solution for injection in pre-filled pen [Summary of product characteristics]. Available from: https://www.ema.europa.eu/en/documents/product-information/ozempic-epar-product-information_en.pdf.
17. Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503–515. doi:10.1056/NEJMoa2107519
18. Gelhorn H, Balantac Z, Shinde S, Thieu VT, Boye KS. The burden of type 2 diabetes and the value of achieving near normoglycemia from the patient perspective. Diabetes Ther. 2021;12(7):1821–1837. doi:10.1007/s13300-021-01054-6
19. Gelhorn HL, Ross MM, Shinde S, Thieu VT, Boye KS. The benefits of safely achieving near normoglycemia from the perspective of people with type 2 diabetes: a quantitative survey study. Patient Prefer Adherence. 2022;16:1897. doi:10.2147/PPA.S366966
20. Flood EM, Bell KF, de la Cruz MC, Ginchereau-Sowell FM. Patient preferences for diabetes treatment attributes and drug classes. Curr Med Res Opin. 2017;33(2):261–268. doi:10.1080/03007995.2016.1253553
21. Mansfield C, Sikirica MV, Pugh A, et al. Patient preferences for attributes of type 2 diabetes mellitus medications in Germany and Spain: an online discrete-choice experiment survey. Diabetes Ther. 2017;8(6):1365–1378. doi:10.1007/s13300-017-0326-8
22. Thieu VT, Robinson S, Kennedy-Martin T, Boye KS, Garcia-Perez LE. Patient preferences for glucagon-like peptide 1 receptor-agonist treatment attributes. Patient Prefer Adherence. 2019;13:561–576. doi:10.2147/PPA.S187907
23. Polster M, Zanutto E, McDonald S, Conner C, Hammer M. A comparison of preferences for two GLP-1 products--liraglutide and exenatide--for the treatment of type 2 diabetes. J Med Econ. 2010;13(4):655–661. doi:10.3111/13696998.2010.529377
24. Gelhorn HL, Bacci ED, Poon JL, Boye KS, Suzuki S, Babineaux SM. Evaluating preferences for profiles of glucagon-like peptide-1 receptor agonists among injection-naive type 2 diabetes patients in Japan. Patient Prefer Adherence. 2016;10:1337–1348. doi:10.2147/PPA.S109289
25. Gelhorn HL, Poon JL, Davies EW, Paczkowski R, Curtis SE, Boye KS. Evaluating preferences for profiles of GLP-1 receptor agonists among injection-naive type 2 diabetes patients in the UK. Patient Prefer Adherence. 2015;9:1611–1622. doi:10.2147/PPA.S90842
26. Gelhorn HL, Stringer SM, Brooks A, et al. Preferences for medication attributes among patients with type 2 diabetes mellitus in the UK. Diabetes Obes Metab. 2013;15(9):802–809. doi:10.1111/dom.12091
27. Brooks A, Langer J, Tervonen T, Hemmingsen MP, Eguchi K, Bacci ED. Patient preferences for GLP-1 receptor agonist treatment of type 2 diabetes mellitus in Japan: a discrete choice experiment. Diabetes Ther. 2019;10(2):735–749. doi:10.1007/s13300-019-0591-9
28. Hauber AB, Nguyen H, Posner J, Ervin C, LaRue S, Kalsekar I. Patient preferences for frequency of Glucagon-Like Peptide-1 Receptor Agonist (GLP-1RA) injections in the treatment of type 2 diabetes.
29. Eli Lilly and Company. Data on file, draft TZP IFU; 2021.
30. Johnson FR, Yang JC, Reed SD. The internal validity of discrete choice experiment data: a testing tool for quantitative assessments. Value Health. 2019;22(2):157–160. doi:10.1016/j.jval.2018.07.876
31. Lancsar E, Louviere J. Deleting ‘irrational’responses from discrete choice experiments: a case of investigating or imposing preferences? Health Econ. 2006;15(8):797–811. doi:10.1002/hec.1104
32. Matza LS, Stewart KD, Landó LF, Patel H, Boye KS. Exit interviews examining the patient experience in clinical trials of tirzepatide for treatment of type 2 diabetes. Patient. 2022;15(3):367–377. doi:10.1007/s40271-022-00578-8
33. Diabetes.co.uk. Driving and hypoglycemia. Available from: https://www.diabetes.co.uk/driving-and-hypoglycaemia.html.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.