")
Back to Journals » Patient Preference and Adherence » Volume 17
Understanding Treatment Preferences Among People Living with HIV in Australia: A Discrete Choice Experiment
Authors Fifer S , Kularatne T, Tan M, Drummond F , Rule J
Received 18 January 2023
Accepted for publication 24 June 2023
Published 26 July 2023 Volume 2023:17 Pages 1825—1843
DOI https://doi.org/10.2147/PPA.S405288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Simon Fifer,1 Thames Kularatne,1 Marcus Tan,2 Fraser Drummond,3 John Rule4,5
1Community and Patient Preference Research Pty Ltd, Sydney, NSW, Australia; 2Reimbursement & Market Access, GlaxoSmithKline Australia Pty Ltd, Melbourne, VIC, Australia; 3Medical Dept, ViiV Healthcare Australia, Melbourne, VIC, Australia; 4National Association of People with HIV Australia, Newtown, NSW, Australia; 5School of Population Health, University of New South Wales, Sydney, Australia
Correspondence: Simon Fifer, Level 20, 25 Bligh St, Sydney, 2000, Australia, Tel +61 403 862 091, Email [email protected]
Purpose: To better understand what is most important to people living with human immunodeficiency virus (PLWH) when choosing their treatment. We assessed how PLWH trade off the potential risks and benefits of oral and long acting injectable (LAI) treatments.
Participants and Methods: Firstly, in-depth interviews were conducted with 11 PLWH to develop a holistic understanding of experiences and determine attributes that contribute to treatment decision-making. Secondly, a discrete choice experiment (DCE) was used to understand the treatment preferences for PLWH with n = 99 PLWH aged 18 years or over with a diagnosis of human immunodeficiency virus (HIV) and who were currently using anti-retroviral therapy (ART). Study participants were presented with 12 scenarios and asked to select their preferred treatment among two hypothetical injectable treatment alternatives, “injection 1” and “injection 2” and their current oral ART treatment. The DCE data were modelled using a latent class model (LCM).
Results: The model revealed significant heterogeneity in preferences for treatment attributes among study participants. Two segments/classes of PLWH were identified. The first segment expressed a strong preference for their current oral treatment; the second segment showed strong preference for the injection treatment and for it to be administered in a GP clinic. Overall, out-of-pocket cost was the most important attribute for participants. One-third of PLWH were willing to switch to an LAI.
Conclusion: Not all PLWH valued the same treatment attributes equally. Overall, out-of-pocket costs for treatments were considered by respondents as the most determining factor in making treatment choices. Results have important implications for healthcare policy and will serve to better inform patients and stakeholders involved in the treatment decision-making process about the treatment preferences of PLWH. Clinicians are encouraged to consider shared decision-making to establish the treatment course that best aligns with PLWH’s treatment goals.
Keywords: patient preferences, discrete choice experiment, conjoint analysis, HIV, treatment goals, shared decision-making
Introduction
Human immunodeficiency virus (HIV) infection is one of the world’s most serious public health challenges. In 2020, globally there were about 38 million people living with HIV (PLWH), of these about 1.5 million were newly infected.1 In Australia in 2020, an estimated 29,090 people were living with HIV, although approximately 9% of these were unaware of their HIV status.2 In Australia, the majority of HIV notifications were attributed to sexual contact between men (59%), or to heterosexual sex (24%).2 Fewer diagnoses were related to injection drug use, or other reasons.2
HIV is a retrovirus that infects immune cells (mainly CD4-positive T-cells and macrophages), destroying or impairing their function. Untreated, it results in progressive depletion of the immune system, leading to immunodeficiency, and eventually death. Antiretroviral therapy (ART) is effective at preventing HIV transmission, progression to acquired immunodeficiency syndrome (AIDS) and death.3,4 In Australia, of the approximately 26,472 people with diagnosed (known) HIV infection, 91% are receiving treatment and 97% of those people diagnosed and receiving treatment have an undetectable viral load.2 Although effective, treatment with ART represents a significant burden, requiring PLWH to take daily oral antiretrovirals.5 Adherence to treatment is critical to achieve and maintain viral suppression.5 However, there are a number of barriers to achieving good adherence. Many PLWH experience physical, emotional and psychosocial challenges with daily oral ART including difficulty swallowing pills, stress from daily dosing routine and concern that having to take pills everyday would increase the chances of the person’s HIV status being revealed.6 For this reason, ARTs with decreased treatment burden are being developed. Long-acting injectable (LAI) formulations which have the potential to improve patient quality of life (QOL), along with physical, emotional and psychosocial health, are now available.
An alternative long acting injectable (LAI) regimen of cabotegravir plus rilpivirine has been assessed in clinical trials which will allow for two-monthly administration of ART and offer potential improvements in long-term adherence. Results from the individual pivotal trials (ATLAS, FLAIR) pooled analyses show that the LAI of cabotegravir plus rilpivirine were noninferior to daily oral regimens for key virologic endpoints at Week 48.7–10 Despite the success of daily oral therapy, considerable interest exists in LAI treatment options. Considering the additional benefits of LAI including long-term adherence and lower frequency of treatment that impacts patient lifestyle, physical, emotional, and psychosocial health, investigating preferences for an injectable treatment option vs current oral therapies was considered timely and important.
Other studies have assessed factors affecting treatment preferences for PLWH, these include risk of side effects,11,12 efficacy of treatment,12–15 and costs.13,15 Further, drug–drug interactions,12 frequency of administration/regimen convenience,14,16–18 pill count/dosing,18,19 and risk of drug resistance16,17 showed some influence on preferences. Other features of treatment such as food restrictions2,12,18 and adherence2 requirements were found to be less important.
Despite the potential benefits of LAI in the treatment of PLWH, little is understood about patient perceptions of current and proposed future treatments in the Australian setting. Whilst there has been knowledge amongst some PLWH that new methods for delivery of HIV therapies were on the horizon, no detailed studies of PLWH expectations or preferences had been undertaken. Therefore, this study attempts to better understand what is most important to PLWH when choosing treatment options. The objective is to develop a greater understanding of treatment preferences among PLWH when choosing their treatment. We investigate treatment preferences for an LAI vs current oral treatment options.
Materials and Methods
Patient preference research methods were used to assess how PLWH trade off the potential risks and benefits of oral and LAI treatments. Such methods are recommended globally to assess the needs and experiences of patients, and can be used to inform decision-making by regulators and health technology assessors.20
First, we conducted a qualitative research component to develop greater understanding of HIV journeys, challenges, treatment histories and treatment preferences. The findings of this qualitative research were used to then design a Discrete Choice Experiment (DCE). The DCE modelling approach was used to quantitatively determine how the treatments were perceived, and what is most important to PLWH.
Participants were asked to read through the participant information sheet and consent form, then check a box to indicate they had read the information and agreed to participate. This study was approved by the Bellberry Limited Human Research Ethics Committee (Approval number: 2019-12-1132-A-1) in accordance with the National Statement on Ethical Conduct in Human Research.
Qualitative Research (Interviews)
We conducted qualitative research (in-depth interviews) prior to conducting the quantitative research (DCE). The purpose of conducting in-depth interviews was to gather information and improve understanding of the study context and population to be able to better design the DCE.
In-depth interviews were conducted with 11 PLWH to develop a holistic understanding of experiences (including benefits and challenges of treatment) and determine attributes that contribute to treatment decision-making. Participants were recruited via the patient advocacy group National Association of People with HIV Australia (NAPWHA), and were asked questions on their demographics, the impact of HIV on them, their current treatments, experience and satisfaction with treatment, and the attributes they felt were most important in HIV treatment. Each interview lasted between 45 and 60 minutes and was conducted in March and April 2020. The results of these in-depth interviews helped inform the design of the DCE.
Quantitative Survey Design
Patient preference research methods aim to measure the values (needs/views) of patients with a particular condition. The goal is to explore how patients perceive treatments (both current and new treatments) and understand what is most important to these patients when evaluating treatments. Incorporating patient values into health outcomes is known as Patient Value Mapping (PVM).21 We refer to these types of studies as PVM because the process involves mapping treatment characteristics against a patient value framework (deriving a score for each treatment based on what is important to patients). The value framework is established using trade-off techniques (such as DCEs or conjoint analysis) which directly measure the relative value of specific components of a treatment (eg, oral administration vs injection).21,22
This study used DCEs to understand treatment preferences for PLWH. DCEs have a firm theoretical basis in Random Utility Theory initially developed by Thurstone and further developed by Mcfadden23, combined with Lancaster’s theory of value.24 Based on this framework, Louviere and Hensher25 and Louviere and Woodworth26 developed the experimental design approach to operationalise DCE. Acommon underlying assumption of DCEs is that decision-makers trade-off between different treatment attributes to choose a treatment that maximizes utility or value. DCEs are increasingly used to quantify preferences for treatments across a broad range of diseases27–29 and allow for an understanding of the underlying characteristics, or attributes, of treatment that influence treatment choices.
Participants
PLWH were invited to participate in the quantitative online survey if they were 18 years of age or over, had a self-reported diagnosis of HIV and were currently receiving ART. Further, participants had to be an Australian Citizen or a permanent resident. Those participated in the qualitative research were not included in the quantitative online survey to avoid prior knowledge bias of the study.
Treatment-related questions were included in the survey to validate the survey respondents (eg, at your last HIV-viral load measurement, were you virologically suppressed? Which antiretroviral therapy (ART) are you currently taking for HIV?; How many pills do you take for HIV treatment daily?; As an estimate, how much do you pay for your HIV medication (eg, pills) for 2 months?). Also, some selected respondents were recontacted with survey questions to cross check answers. Those who provided non-sensical answers were removed from the survey.
Recruitment was facilitated via invitations from an HIV patient advocacy group (the National Association of People with HIV Australia [NAPWHA]), an online market research panel, social media advertising and “snowballing”. Participants who completed the online survey were reimbursed AU$50 either as an e-gift voucher or equivalent in panel points, or as a donation to NAPWHA.
Survey Development
Attributes and levels for the DCE were derived through a literature review, outcomes of the ATLAS and FLAIR clinical trials,10,30 discussions with the project team, and interviews with the 11 PLWH. Each potential attribute that was identified during this process was discussed with the 11 PLWH to understand the importance they placed on them, and if they understood the terminology used (or whether it should be rephrased). For example, PLWH were confused by the term “patient-years” when assessing long-term risks of medications, stating that the terminology was too complicated and unlikely to be understood in the quantitative survey, therefore risks were described in terms of percentages or “levels of risk”, for example 1 in 50 patients.
Discrete Choice Experiment
Participants completed an online survey which included questions on treatment background, treatment preferences, quality of life and demographics. The survey was conducted between July and August 2020. The key component was the treatment preferences section which was a DCE. It required participants to select their preferred treatment out of two hypothetical injectable treatment alternatives, “injection 1” and “injection 2” and their current treatment, which was a fixed oral ART defined by the participant (current treatment does not change across scenarios). The treatment alternatives were described by various attributes and levels. Based on participant-reported eligibility for concessional healthcare costs (ie, reduced patient co-payments), participants were either shown general or concessional out-of-pocket medication costs (a concession healthcare card is issued by the Australian government to provide access to Pharmaceutical Benefits Scheme prescription items, and certain Medicare services, at a cheaper rate. Eligibility is determined by income and other family circumstances such as pension age, caregiving status, disability, etc.)
The experimental design followed good practice guidelines,31 and the combinations of attribute levels describing the hypothetical injection alternatives presented in the tasks were designed using a D-efficient design structure32 in NGene (ChoiceMetrics Pty Ltd, Sydney, Australia), a software tool used to generate stated choice experimental design. A total of 48 scenarios were developed, which were split into four blocks so that each participant was presented with 12 scenarios.
The DCE scenarios were based on the assumptions that injectable treatments are supported by robust clinical trial evidence, and are recommended by current treatment guidelines; all treatment options have similar efficacy; once the two monthly injection is commenced, oral bridging is available if the PLWH is unable to attend their next scheduled injection; it is possible to discontinue the injection and transition into any fully active oral regimen, and the PLWH would need to continue oral therapy for a period of at least 52 weeks from their last injection (see Figure 1). The reason for assuming that all treatment options/alternatives have similar levels of efficacy was because the current treatments in the market have proven to successfully suppress viral load and reduce the likelihood of HIV transmission to effectively zero. This assumption allowed us to explore other features of treatment comprehensively.
 |
Figure 1 Example DCE scenario. |
The online survey was pilot tested with PLWH prior to launching to test for validity and reliability. Scenarios were revised where needed to improve clarity. Revisions include improvements to the choice question, icons used and presentation of the injectable treatment (how to transition from oral to injectable).
Before commencing the DCE, participants were shown an information page to set the context of the choice task. It included detailed instructions of how to complete the task, along with a table displaying the treatment attributes and respective descriptions (Supplementary Figure 1). It also provided further background information about the hypothetical injectable treatment options
The injection treatment requires an oral lead-in process which involves taking two tablets once daily with a meal for approximately 28 days. The injection is then administered into the gluteus medius (side of buttocks) every second month. The size of the injection needle can vary between 23G (1.5 inch) to 21G (2 inch). This is similar to a standard blood-drawing needle. There are no dietary requirements associated with the injectable treatment.
Participants were presented with 12 scenarios in which they were asked to choose their preferred treatment option. An example scenario is shown in Figure 1. Hypothetical treatment alternatives were further described by various attributes including the frequency of administration, location of administration (the place or setting), the number of pills or injections taken at each time, short- and long-term side effects, adherence, the availability of a patient support program, and out-of-pocket costs (see Table 1 for a list of attributes and their descriptions as used in the survey). Respondents’ answers to the first sections of the survey were used to populate levels for the current oral treatment in the DCE. Surveys took an average duration of 20–25 minutes to complete.
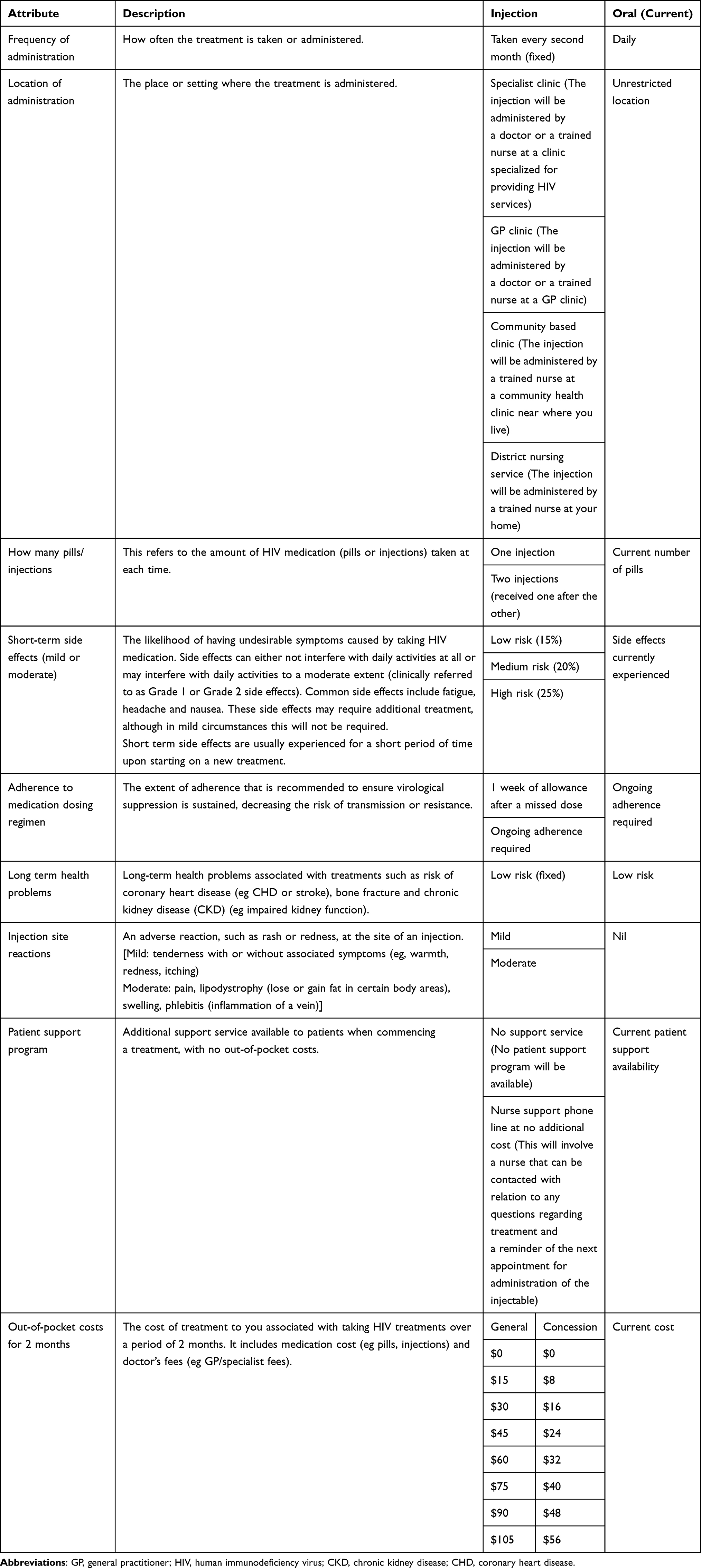 |
Table 1 Attributes and Levels Presented in the DCE |
Quality of Life
Quality of life (QoL) was assessed using the PozQoL scale.33 Total scores, and scores on the sub domains health concerns, psychological, social and functional were calculated. Higher scores indicated better quality of life.
Statistical Considerations
Data from participants who completed the survey too quickly, gave non-sensical answers or were suspected duplicates were removed (n = 5 for DCE task). Survey data outside of the DCE component were summarized descriptively. Descriptive analysis of demographic and quality of life data was performed using R software. For the DCE analysis, the categorical attributes were re-coded using simple dummy coding, using one of the levels as a reference category (for an attribute with Ɩ levels, Ɩ−1 dummy variables were created) and the numerical attributes (cost and number of pills) were treated as continuous variables.
A latent class model was chosen to model the overall utility for alternative respondent choice situations. This was chosen as it can account for preference heterogeneity (variation) within the sample. This is handled using discrete distributions which classify participants into “latent classes” or segments based on their choices. Model fit was assessed using adjusted McFadden Pseudo R2. DCE data were modelled using NLOGIT version 6 (Econometric Software Inc, Plainview, NY, USA). Positive coefficients for an attribute level indicate that it is preferred over its corresponding reference category.
The parameter estimates were used to calculate the relative importance of each attribute by computing the overall percentage influence on change in utility between the lowest and highest levels of each attribute.34 Parameter estimates were considered statistically significant at the 5% level.
The relative importance of each attribute was calculated by finding the maximum difference in utility between the attribute’s level and expressing it as a percentage of the sum of all maximum differences.
Results
Qualitative Research Findings
We interviewed 11 PLWH, 9 men and 2 women. The majority participated via telephone interview (n=10/11). Participants were aged 31 to 62 years of age and had been living with HIV for a median 22 years (range 15 to 38 years). Participants reported contracting HIV through unprotected sexual activity, intravenous drug use or via a blood product. They reported that diagnosis with HIV was difficult to accept and commonly led to a downward spiral in physical and emotional health. Around the time of diagnosis, many reported heightened anxiety, and some experienced intense discrimination or hatred from others, and the death of friends. Those with longer diagnoses reported there was limited information or treatment options at the time of their diagnosis. Many reported profound impacts on their lives including symptoms, treatment side effects, hospitalization, depression, guilt, anxiety, stigma and discrimination. They suffered financial burden. However, despite these challenges, PLWH were resilient and had a positive attitude. For some, it had led to a healthier lifestyle, and for others it had led to feelings of empowerment or provided a platform to help others.
Most participants reported feeling sufficiently supported and voiced immense gratitude for the range of effective treatments available. Most were highly adherent with their current treatment, although a few had elected to have extended treatment breaks in the past. Most welcomed a long-lasting injection as a further treatment option to reduce the pill burden, and also as it meant few restrictions; however, some expressed reluctance to switch from their current oral therapy as they were already satisfied with their oral regimen and had concerns around sustained efficacy particularly with a once every 2 months injection. The key attributes important for HIV treatment for PLWH were efficacy (undetectable viral load), side effect profile, and the frequency of administration.
Quantitative Research Findings
Participants
A total of 120 PLWH responded to the quantitative survey, of whom 104 (87%) were included in the analysis (16 responses were removed in the initial data cleaning based on incompletions, failing the attention checks, completing the survey too fast and nonsensical open text responses). Of these, 99 were included in the DCE (5 were excluded due to admitting a poor understanding of the task).
Demographics of included participants are presented in Table 2. Participants represented all states and territories in Australia and were an ethnically diverse sample. The majority of participants were male; homosexual; and living in a metropolitan or city area. The majority (56%) of participants reported no side effects from their treatment, but 13% reported difficulty with pill swallowing and 60% reported missing one or more doses of medication in the previous 6 months (Table 2).
 |
Table 2 Participant Demographics and Clinical Characteristics |
The mean quality of life scores for PozQoL were total 3.52, health concerns 3.27, psychological 3.36, social 3.51 and functional 4.01. Based on thresholds for Average PozQoL, scores for the overall assessment of QoL and for the domains a moderate QoL was observed, with the exception of the social domain where a high QoL was seen (see thresholds for average PozQol scores at https://www.pozqol.org/using-pozqol/interpreting-pozqol-scores). Open ended responses revealed factors that contributed to the quality of life of participants such as: “I do my best to not let HIV define who I am as an individual it plays a big part in just getting on with your life” while others felt that “Taking a pill every day is a constant, daily reminder that I’ m HIV+ and I find that depressing.”
Results of Discrete Choice Experiment
The best fitting model was an LCM with two classes or segments of participants based on their preference for HIV treatments (Table 3). The utility equations are provided in the Supplementary Information. The attributes patient support program and injection site reactions were not significant in the model and were removed from the final model. The aggregate class probabilities for segment 1 and segment 2 were 0.64 and 0.36, respectively. One way of thinking of this is that approximately 64% of participants were likely to belong to Segment 1 and 36% to Segment 2 (although the model assumes everyone is a mixture of both segments up to a certain probability). The first segment (“segment 1”) were participants who expressed a strong preference for their current oral treatment. Participants in the second segment (“segment 2”) showed strong preference for the injection treatment, and for it to be administered in a GP clinic. The positive constants for current treatment (status quo) for general patients (1.273) and for concession patients (1.887) for segment 1 indicated that participants were more likely to stick with the current oral treatment over the injection treatment, holding all else equal. As for segment 2, the negative constants for current treatment for general patients (−2.126) and for concession patients (−1.940) indicated that participants preferred the injection alternatives over their current treatment (holding all else equal). Across both segments, low risk side effects were preferred to high-risk side effects.
 |
Table 3 LCM Model Output |
For segment 1, a specialist clinic was preferred as a place of administration to a community-based clinic or a district nursing service. Participants in segment 1 also showed sensitivity to the number of injections, preferring one injection over two injections. In comparison, participants in segment 2 were generally more likely to have a higher preference for a GP clinic over a specialist clinic. In terms of out-of-pocket cost, increase in out-of-pocket cost resulted in a significant decrease in preference for both groups.
Adherence to medication dosing regimen had no significant effect on treatment preferences in either class. It is important to note that this does not equate to these attributes being unimportant to participants. Rather, due to the nature of the trade-off tasks, it may simply be that other attributes (such as side effects and cost) were more important in comparison.
Attributes significantly associated with the probability of belonging to segment 2 included participants who currently paid for their HIV medication and were currently employed (full/part time or casual). Those who currently experience a lower QoL were likely to support the new injection treatment.
Attribute Importance
In standard choice models, the utility parameters cannot typically be directly compared as the attributes represented by each parameter are presented on different scales. However, the model parameters can be used to evaluate the relative importance of attributes by comparing the difference in utility between the lowest and highest levels.34
Overall, out-of-pocket cost was the most important attribute for participants. It was dominant in both segments and accounted for more than 65% of preferences for general patients and more than 50% for concession patients. For general patients, location of administration was the second most important factor for consideration (9% for segment 1 and 23% for segment 2). The remaining was shared between number of injections (2%), side effects (5%) and adherence (1%) for Segment 1, and side effects (14%), adherence (8%) and the number of injections (2%) in the order of importance for Segment 2 (Figure 2). For concession patients, similar preferences were reported: location of administration was the second most important factor for consideration (19% for segment 1 and 19% for segment 2). The remaining was shared between side effects (22%), number of injections (11%), and adherence (1%) for Segment 1 and number of injections (12%), adherence (7%) and side effects (2%) for Segment 2 (Figure 2).
 |
Figure 2 Relative attribute importance. (A) General patient. (B) Concession patients. |
Discussion
This study examined the treatment preferences for PLWH for a new long-acting injectable treatment. In-depth interviews along with literature review were used to inform the quantitative experiment. This was particularly important, as it provided details on the profound impact that HIV has on PLWH, but also identified potentially confusing terminology which was then amended prior to the quantitative part of the study.
Overall, the treatment mode (ie, injection vs oral) was very important to participants when choosing a treatment alternative and was found to be the main differentiator between the segments. Out-of-pocket cost was the most important treatment attribute for participants when making decisions about their own treatment. It accounted for more than 50% of their preferences for treatment (67% for general patients and 51% for concession patients), such that there was a significant decrease in preferences for the treatment alternatives as cost increased. There were, however, two segments of decision-makers identified, largely based on their willingness to consider the new injection alternatives presented.
Given the importance of efficacy in this setting, and the evidence of non-inferiority of injectables compared to oral ART, we did not include efficacy as an attribute within our DCE. Others have previously reported the strong preference for PLWH for efficacious treatments.19,35,36
Existing literature on treatment preferences for ART has highlighted the importance of quality of life,36 long-term side effects;19,35 with pharmacologic considerations such as dosing and pill burden being less important in some studies, but not others.19,35,36 In other jurisdictions, cost remained a barrier for some PLWH.36
To the best of our knowledge, this study is the first to elicit treatment preferences of PLWH in Australia and the first to comprehensively assess treatment preferences for LAI vs oral treatments currently available. Mühlbacher et al used DCEs to understand preferences of PLWH in Germany,11 focusing on the impact of treatment on life expectancy, probability of long-term side effects, flexibility of dosing, and indicators of quality of life. Ostermann et al35 used DCEs to quantify preferences of PLWH in the US for key characteristics of modern ART including dosing, administration characteristics, side effects and long-term effects. Our study incorporates some of the attributes of both of the above studies but relevant and important to both oral and LAI as indicated by the PLWH in our study context.
Our study did not directly consider the potential impact of fear or stigma associated with needles and the impact this may have on treatment preference. For example, there have been some reports that there is a fear of LAI in those with a history of injection drug use, as there is a concern that LAI may trigger recurrence.37 Some who receive episodic injections for other conditions may be reticent to add LAIs to their treatment regimen, including people with diabetes.37 However, others suggested that for those experienced with episodic injections, addition of LAI for HIV would not be an issue.37 Although directly not incorporated as a variable in the models, respondents’ dislike or fear of needles is represented in their behaviour by choosing the “current treatment” in the DCE and therefore in the model constants. Other possible barriers to switching to a two monthly LAI are giving up the habit of taking medicine daily/changing established routine/habit, sense of control, inability to travel for a long period of time and inconvenience caused by frequent medical visits as revealed by the open text responses in the survey:
I have no problem taking a tablet every day which has come part of my daily routine.
I am not interested in injectables at all because my HIV meds are just one of a number of tablets I take every day which I will continue to take regardless.
If I wanted to travel at some point in time, it would be easier to take a few bottles of tablets with me and I could then stay away for more than 2 months.
If 6 monthly injectables were an option I would have chosen some of them.
Injections, no matter how infrequent, are far more invasive than popping a pill daily.
Pills can be swallowed anywhere, are convenient, robust, no refrigeration needed, cheap, space efficient.
While our study has shown that approximately two-thirds of PLWH preferred current oral but, there does appear to be a place for injectable treatment. Such preferences should be taken into account when selecting potential ART. Injectable treatment may provide a convenient option and may be practical for people who travel frequently, or for those who have swallowing difficulties, those taking other medications (drug–drug interactions) or drug malabsorption.38 Further, our study found that PLWH felt an injectable treatment reduced anxiety around pill burden (specifically the reduced need to hide medication, or less requirement to physically store medication), missed doses, swallowing pills, or the impact of hot weather on pill storage.
I would prefer the injectable treatment. Taking a pill every day is a constant, daily reminder that I’m HIV+ and I find that depressing.
I’ve been worried about my adherence so the injectables were the most appealing.
Injections are more convenient than pills. Venue for administration of injectable medicine also very important as I work full time and it is very difficult to attend a clinic during business hours.
Conclusion
In summary, the results from this study could be used to better understand treatment preferences among PLWH for a new LAI treatment. Outcomes can be used to guide informed decisions around the value of new and existing medications. The majority of people in this sample are conservative in their treatment decisions for HIV and are not open to a new injectable treatment. However, the remaining segments are actively looking for something new, and display a strong preference for the new injection. Out-of-pocket cost was the most important factor for this sample when considering treatments, and all would prefer low risk side effects. Clinicians are encouraged to consider shared decision-making to establish the treatment course that best aligns with PLWH’s treatment goals.
Limitations and Future Research
We acknowledge there are some limitations to our study. In the qualitative component, participants were all treatment-experienced and study could have benefitted from PLWH who were diagnosed more recently and treatment-naïve. Recruitment of the quantitative survey through consumer support groups and online panels may mean that those included were not representative of the overall population of PLWH. In terms of demographics, more women and those with indigenous backgrounds would have improved the representativeness and generalisability of the findings. It was a challenging task as the study relied on self-reported data, and participation was restricted to PLWH who had internet access. Finally, although the treatment attributes evaluated in the DCE were derived from literature research and our knowledge of the area, it is possible that the study did not include some attributes that PLWH would consider important.
Future research should explore heterogeneity in preferences between various demographic subgroups (eg, treatment-naïve vs treatment experienced, ethnic minorities vs others, various age groups) to enhance understanding of treatment preferences among PLWH in Australia.
Acknowledgments
The authors thank Belinda Butcher BSc(Hons) MBiostat PhD CMPP for providing medical writing support in accordance with Good Publication Practice 3 (GPP3) guidelines (http://ismpp.org/gpp3). Medical writing support was funded by ViiV Healthcare.
We thank NAPWHA for their assistance with recruitment. The authors would also like to thank Ariana Cabrera and Declan Monro for technical help and Lili Toh for helping with the revisions.
Funding
The study was funded by ViiV Healthcare. Company who provided funding was not part of the overall study design. Members of companies were involved in final discussion of results and dissemination. The funding bodies had no specific role in study design, data collection, data analysis and interpretation or writing the manuscript.
Disclosure
SF and TK are employed by CaPPRe. CaPPRe has consulted to AbbVie, Amgen, AstraZeneca, Celgene, CSL Behring, Edwards, GSK, Ipsen, Janssen, Novo Nordisk, Roche, Sanofi, Shire and UCB, outside of the submitted work. MT is an employee of GSK. FD is an employee of ViiV Healthcare. The authors report no other conflicts of interest in this work.
References
1. UNAids. Fact Sheet - World Aids Day. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf.
2. Zwar N, Streeton CL. Pretravel advice and hepatitis A immunization among Australian travelers. J Travel Med. 2007;14(1):31–36. doi:10.1111/j.1708-8305.2006.00088.x
3. Cohen MS, Chen YQ, McCauley M, et al. Antiretroviral therapy for the prevention of HIV-1 transmission. N Eng J Med. 2016;375(9):830–839. doi:10.1056/NEJMoa1600693
4. Rodger AJ, Lodwick R, Schechter M, et al. Mortality in well controlled HIV in the continuous antiretroviral therapy arms of the SMART and ESPRIT trials compared with the general population. Aids. 2013;27(6):973–979. doi:10.1097/QAD.0b013e32835cae9c
5. European AIDS Clinical Society. EACS Guidelines Version 11.0 October 2021; 2021. Available from https://www.eacsociety.org/media/final2021eacsguidelinesv11.0_oct2021.pdf.
6. de Los Rios P, Okoli C, Castellanos E, et al. Physical, emotional, and psychosocial challenges associated with daily dosing of HIV medications and their impact on indicators of quality of life: findings from the positive perspectives study. AIDS Behav. 2021;25(3):961–972. doi:10.1007/s10461-020-03055-1
7. Swindells S, Andrade-Villanueva JF, Richmond GJ, et al. Long-acting Cabotegravir + Rilpivirine for maintenance therapy: ALTAS week 48 results.
8. Overton ET, Orkin C, Swindells S, et al. Monthly Long-Acting Cabotegravir and Rilpivirine is Noninferior to Oral ART as Maintenance Therapy for HIV-1 Infection: week 48 Pooled Analysis From the Phase 3 ATLAS and FLAIR Studies.
9. Overton ET, Richmond G, Rizzardini G, et al. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: a randomised, multicentre, open-label, phase 3b, non-inferiority study. Lancet. 2020;396(10267):1994–2005. doi:10.1016/S0140-6736(20)32666-0
10. Swindells S, Andrade-Villanueva J-F, Richmond GJ, et al. Long-Acting Cabotegravir and Rilpivirine for Maintenance of HIV-1 Suppression. N Engl J Med. 2020;382(12):1112–1123. doi:10.1056/NEJMoa1904398
11. Mühlbacher AC, Stoll M, Mahlich J, Nübling M. Evaluating the concordance of physician judgments and patient preferences on AIDS/HIV therapy - A Discrete Choice Experiment. Health Econ Rev. 2013;3(1):30. doi:10.1186/2191-1991-3-30
12. Bregigeon-Ronot S, Cheret A, Cabie A, et al. Evaluating patient preference and satisfaction for human immunodeficiency virus therapy in France. Patient Prefer Adherence. 2017;11:1159–1169. doi:10.2147/PPA.S130276
13. Hendriks A, Wijnen B, van Engelen R, et al. A best-worst scaling in Colombian patients to rank the characteristics of HIV/AIDS treatment. J Med Econ. 2018;21(5):468–473. doi:10.1080/13696998.2018.1440401
14. Simoni JM, Beima-Sofie K, Mohamed ZH, et al. Long-Acting Injectable Antiretroviral Treatment Acceptability and Preferences: a Qualitative Study Among US Providers, Adults Living with HIV, and Parents of Youth Living with HIV. AIDS Patient Care STDS. 2019;33(3):104–111. doi:10.1089/apc.2018.0198
15. Hauber AB, Mohamed AF, Watson ME, Johnson FR, Hernandez JE. Benefits, risk, and uncertainty: preferences of antiretroviral-naive African Americans for HIV treatments. AIDS Patient Care STDS. 2009;23(1):29–34. doi:10.1089/apc.2008.0064
16. Beusterien KM, Dziekan K, Flood E, Harding G, Jordan JC. Understanding patient preferences for HIV medications using adaptive conjoint analysis: feasibility assessment. Value Health. 2005;8(4):453–461. doi:10.1111/j.1524-4733.2005.00036.x
17. Beusterien KM, Dziekan K, Schrader S, et al. Patient preferences among third agent HIV medications: a US and German perspective. AIDS Care. 2007;19(8):982–988. doi:10.1080/09540120701294278
18. Stone VE, Jordan J, Tolson J, Miller R, Pilon T. Perspectives on adherence and simplicity for HIV-infected patients on antiretroviral therapy: self-report of the relative importance of multiple attributes of highly active antiretroviral therapy (HAART) regimens in predicting adherence. J Acquir Immune Defic Syndr. 2004;36(3):808–816. doi:10.1097/00126334-200407010-00007
19. Muhlbacher AC, Stoll M, Mahlich J, Nubling M. Patient preferences for HIV/AIDS therapy - A discrete choice experiment. Health Econ Rev. 2013;3(1):14. doi:10.1186/2191-1991-3-14
20. The PREFER Consortium. PREFER Recommendations - Why, when and how to assess and use patient preferences in medical product decision-making; 2022. Available from: https://zenodo.org/record/6491042#.YpQTXhNBz0p.
21. Fifer S, Galinsky J, Richard S. Myeloma patient value mapping: a discrete choice experiment on myeloma treatment preferences in the UK. Patient Prefer Adherence. 2020;14:1283. doi:10.2147/PPA.S259612
22. Fifer S, Keen B, Newton R, Puig A, McGeachie M. Understanding the Treatment preferences of people living with Schizophrenia in Australia; a patient value mapping study. Patient Prefer Adherence. 2022;16:1687. doi:10.2147/PPA.S366522
23. McFadden DL. Conditional Logit Analysis of Qualitative Choice Analysis. New York Academic Press; 1974.
24. Lancaster KJ. A new approach to consumer theory. J Political Eco. 1966;74(2):132–157. doi:10.1086/259131
25. Louviere JJ, Hensher DA. On the design and analysis of simulated choice or allocation experiments in travel choice modelling. Transp Res Rec. 1982;890(1982):11–17.
26. Louviere JJ, Woodworth G. Design and analysis of simulated consumer choice or allocation experiments: an approach based on aggregate data. J Marketing Res. 1983;20(4):350–367. doi:10.1177/002224378302000403
27. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making. PharmacoEconomics. 2008;26(8):661–677. doi:10.2165/00019053-200826080-00004
28. Marshall D, Bridges JFP, Hauber B, et al. Conjoint analysis applications in health — how are studies being designed and reported? Patient Centered Outcomes Res. 2010;3(4):249–256. doi:10.2165/11539650-000000000-00000
29. Soekhai V, de Bekker-Grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. PharmacoEconomics. 2019;37(2):201–226. doi:10.1007/s40273-018-0734-2
30. Rizzardini G, Overton ET, Orkin C, et al. Long-acting injectable cabotegravir+ rilpivirine for HIV maintenance therapy: week 48 pooled analysis of phase 3 ATLAS and FLAIR trials. J Acquired Immune Deficiency Syn. 2020;85(4):498. doi:10.1097/QAI.0000000000002466
31. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health--a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
32. Rose JM, Bliemer MCJ. Constructing efficient stated choice experimental designs. Transport Rev. 2009;29(5):587–617. doi:10.1080/01441640902827623
33. Brown G, Mikolajczak G, Lyons A, et al. Development and validation of PozQoL: a scale to assess quality of life of PLHIV. BMC Public Health. 2018;18(1):527. doi:10.1186/s12889-018-5433-6
34. Gonzalez JM. A guide to measuring and interpreting attribute importance. Patient Patient Centered Outcomes Res. 2019;12(3):287–295. doi:10.1007/s40271-019-00360-3
35. Ostermann J, Muhlbacher A, Brown DS, et al. heterogeneous patient preferences for modern antiretroviral therapy: results of a discrete choice experiment. Value Health. 2020;23(7):851–861. doi:10.1016/j.jval.2020.03.007
36. Eaton EF, McDavid C, Banasiewicz MK, Mugavero MJ, Knight SJ. Patient preferences for antiretroviral therapy: effectiveness, quality of life, access and novel delivery methods. Patient Prefer Adherence. 2017;11:1585–1590. doi:10.2147/PPA.S142643
37. Philbin MM, Parish C, Bergen S, et al. A qualitative exploration of women’s interest in long-acting injectable antiretroviral therapy across six cities in the women’s interagency HIV study: intersections with current and past injectable medication and substance use. AIDS Patient Care STDS. 2021;35(1):23–30. doi:10.1089/apc.2020.0164
38. Jolayemi O, Bogart LM, Storholm ED, et al. Perspectives on preparing for long-acting injectable treatment for HIV among consumer, clinical and nonclinical stakeholders: a qualitative study exploring the anticipated challenges and opportunities for implementation in Los Angeles County. PLoS One. 2022;17(2):e0262926. doi:10.1371/journal.pone.0262926
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.