Back to Journals » Cancer Management and Research » Volume 18

Parameters That May Predict NAC Effectiveness in Hormone-Positive Breast Cancer According to CPS Score
Authors Buyukbayram ME ![]() , Hannarici Z, Turhan A, Çağlar AA, Çoban Eşdur P, Bilici M, Tekin SB, Dinar Ayman C
, Hannarici Z, Turhan A, Çağlar AA, Çoban Eşdur P, Bilici M, Tekin SB, Dinar Ayman C
Received 10 October 2025
Accepted for publication 30 December 2025
Published 8 January 2026 Volume 2026:18 569515
DOI https://doi.org/10.2147/CMAR.S569515
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shari Youngblood
Mehmet Emin Buyukbayram,1 Zekeriya Hannarici,2 Aykut Turhan,3 Alperen Akansel Çağlar,1 Pınar Çoban Eşdur,1 Mehmet Bilici,1 Salim Başol Tekin,1 Canan Dinar Ayman1
1Department of Medical Oncology, Atatürk University Faculty of Medicine, Erzurum, Turkey; 2Department of Medical Oncology, Health Sciences University Yuksek Ihtisas Training and Research Hospital, Bursa, Turkey; 3Department of Medical Oncology, Republic of Turkey Ministry of Health Ordu Training and Research Hospital, Ordu, Turkey
Correspondence: Mehmet Emin Buyukbayram, Department of Medical Oncology, Atatürk University Faculty of Medicine, Erzurum, Turkey, 25100, Tel +905392449362, Email [email protected]
Objective: Neoadjuvant chemotherapy (NAC) in hormone-positive operable breast cancer supports breast-conserving surgery, axillary dissection, and survival. However, the pathological complete response (pCR) rates to NAC in hormone-positive breast cancer remain low. Identifying the predictive parameters for pathological response prior to NAC is crucial. In this study, we investigated clinical, pathological, inflammatory, and metabolic parameters that could predict NAC response and survival.
Material and Methods: A retrospective study was conducted on 120 patients with hormone-positive breast cancer. Clinical and pathological stages of patients who underwent surgery following NAC were used to calculate the CPS score (clinical stage score + pathological stage score). The Kruskal Wallis test was employed to compare clinical, pathological, and laboratory parameters with the CPS score. The Bonferroni test was applied for post-hoc analysis. Categorical variables were compared using the Pearson Chi-Square test or Fisher’s exact test.
Results: There was no statistically significant association between the CPS score and age (p=0.106), estrogen receptor positivity (p=0.331), grade (p=0.100), Ki67 (p=0.247), and chemotherapy received (p=0.720). While pCR was statistically significant in univariate analysis (p=0.001), it did not reach statistical significance in the multivariate model (p=0.258). Axillary pathological response (ypN) had a statistically significant correlation with the CPS score (p=0.003). There was no statistically significant association between the CPS score and leukocyte, lymphocyte, neutrophil, or platelet counts, glucose levels, NLR, PNI, or SII values (p > 0.05).
Conclusion: ypN was associated with the CPS score in predicting survival following NAC in hormone-positive breast cancer. No statistically significant association was observed between inflammatory or metabolic parameters and the CPS score. Further validation in larger studies is warranted.
Keywords: breast neoplasms, neoadjuvant therapy, prognosis
Introduction
Breast cancer (BC) is the most common cancer among women worldwide. According to WHO data for 2020, the annual incidence of BC is 2.28 million cases, with 685,000 deaths reported per year. Surgical intervention, chemotherapy, and radiotherapy are available treatment options for BC. Neoadjuvant chemotherapy (NAC) in BC increases the rate of breast-conserving surgery, provides insight into tumor response to chemotherapy and biology, and improves survival rates. NAC has become the standard of care in patients with locally advanced and inoperable BC.1–5
The goal of NAC is to achieve pathological complete response (pCR). However, response rates to NAC in hormone-positive BC are remain relatively low, with pCR rates ranging from 1–15%.6 While pCR is strongly associated with disease-free survival (DFS) and overall survival (OS) in HER2-positive and triple-negative BC, it is not strongly associated with DFS and OS in hormone-positive BC. Ongoing studies are investigating various parameters including pathological response classifications (residual cancer burden [RCB], Miller-Payne system) and CPS (clinical stage score + pathological stage score) score, estrogen receptor (ER) positivity, grade, Ki67, lymph node ratio, and other parameters to predict DFS and OS.7–10
The CPS score, which combines clinical and pathological staging, has been shown to correlate with both DFS and OS in hormone-positive breast cancer treated with NAC. Subsequently, the CPS+EG score was developed by incorporating ER positivity and tumor grade into the original CPS model. Post-operative Ki67 has also been associated with survival.11–13
Immune status within the tumor microenvironment influences not only the efficacy of immunotherapy, but also the response to other anti-cancer agents and overall survival.14 The information regarding the immune status of the tumor microenvironment in hormone-positive BC is unclear, and it is generally considered to be heterogeneous tumor microenvironment. Conversely, NAC’s relationship with the immune microenvironment has been shown in HER2 and triple-negative BC with tumor-infiltrating lymphocytes.15,16
The importance of inflammatory and hematological parameters has been demonstrated in the treatment of metastatic breast cancer with cyclin-dependent kinase 4/6 inhibitors (CDK4/6i). A low c-reactive protein (CRP)/lymphocyte ratio has been associated with longer progression-free survival (PFS).17 However, the importance of inflammatory and hematological parameters in the treatment of locally advanced breast cancer with NAC, and their relationship with the survival score CPS, remains unclear.
In studies investigating the relationship between FPG and NAC response among metabolic parameters, high fasting plasma glucose (FPG) was associated with lower NAC responses.18 NAC response has also been linked to other components of metabolic syndrome in these studies, which included all subtypes of breast cancer.19
Clinical studies, including genetic research such as PAM50 and immunohistochemical parameters, are ongoing to avoid unnecessary chemotherapy and to predict response to NAC.20
Despite the success of staging and scoring systems in predicting survival, the relationship between simple and easily accessible metabolic and inflammatory parameters and pathological response prior to NAC remains unclear. In this study, we aimed to investigate the relationship of clinical, pathological, and biochemical parameters that may predict the CPS score associated with survival rates in hormone-positive BC.
Materials and Methods
We included 120 patients with locally advanced or inoperable hormone-positive BC, who were given treatment with NAC followed by surgery between April 2011 and December 2022. Inclusion criteria were as follows: (1) histologically confirmed invasive breast cancer, (2) ER positivity (>1%), (3) local and locally advanced disease, (4) neoadjuvant chemotherapy, (5) surgery.
Exclusion criteria were as follows: (1) distant metastasis, (2) HER2-positive, (3) chronic inflammatory diseases, (4) hematological and other malignancies, (5) missing data.
Demographic data including age, sex, and Eastern Cooperative Oncology Group (ECOG) performance scores of 0, 1, 2, 3, and 4, Ki67, grade, ER positivity rate, pCR, post-operative lymph node positivity (ypN), chemotherapy regimens received, and CPS scores were obtained from patient files. The CPS score was calculated by summing the clinical and pathological stage scores as shown in Table 1.
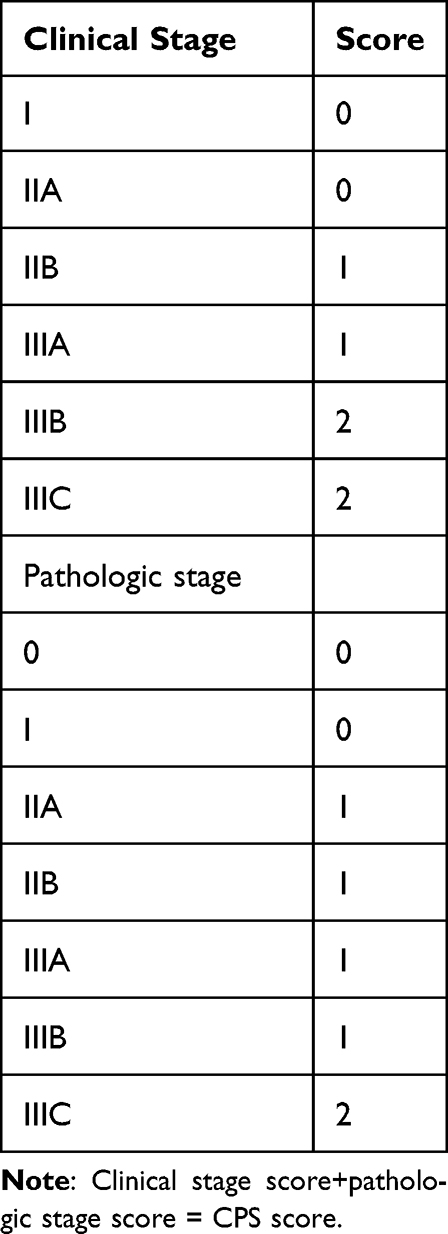 |
Table 1 CPS Score Table |
The patients’ leukocyte, neutrophil, lymphocyte, red blood cell distribution width (RDW), platelet, lactate dehydrogenase (LDH), albumin, CRP, CEA, CA15-3 and FPG values were obtained from the hospitals information system. Blood samples were collected prior to the initiation of NAC.
The SII was calculated as platelet count (P) × neutrophil count (N)/lymphocyte count (L). NLR was calculated as the ratio of neutrophil count to lymphocyte count, and PNI was calculated using the formula: (10× albumin [g/L] + (0.005 × total lymphocyte count).
Cutoff values for neutrophil count, lymphocyte count, RDW/lymphocyte ratio, glucose/CRP ratio, glucose/LDH ratio, glucose/lymphocyte ratio, CRP/lymphocyte ratio, albumin, CEA, CA15-3, SII, NLR, and PNI were calculated using ROC curve analysis. Approval was obtained from the Ethics Committee of Atatürk University Faculty of Medicine (2024/16). All procedures were conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows Version 25.0 (Statistical Package for the Social Sciences, IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as n and % for categorical variables, and as Median and Interquartile Range (IQR) for continuous variables. Normality was assessed using the Kolmogorov–Smirnov test, which indicated p<0.05. Therefore, the Kruskal–Wallis test was used to compare laboratory values between CPS score groups, with the Bonferroni test employed for post-hoc analysis. Categorical variables were compared using the Pearson Chi-Square test or Fisher’s exact test. Variables associated at p<0.10 in univariate analysis or deemed clinically relevant (pCR, ypN) were entered into a multivariable logistic regression model. This model was used for explanatory purposes, with the aim of identifying independent associations with higher CPS scores rather than to predict individual outcomes. To minimize the risk of overfitting, we ensured that the number of events per variable (EPV) exceeded 10 whenever possible, and limited the final model to the two most relevant variables (pCR and ypN). A p-value of <0.05 was considered statistically significant.
Results
Of the patients included in the study, 28 (23.3%) were under 40 years of age, 65 (54.2%) were between 40–58, and 27 (22.5%) were over 58 years. Two (1.6%) patients were male.
As shown in Table 2, a statistically significant difference was observed between CPS score groups and the variables pCR (p=0.001) and ypN (p<0.001) in univariate analyses. Lower CPS scores were associated with increased survival, and improved nodal response was linked to lower CPS scores and longer survival times. However, no statistically significant differences were found between CPS score groups and age (p=0.106), ECOG (p=0.149), ER positivity (p=0.331), grade (p=0.100), Ki67 (p=0.247), and chemotherapy received (p=0.720).
 |
Table 2 Data on Sociodemographic and Clinical Characteristics (n=120) |
As shown in Table 3, there were no statistically significant differences between the CPS score groups in terms of SII (p=0.981), NLR (p=0.988), and PNI (p=0.839) values. Lymphocyte count (p=0.766), FPG (p=0.187), and CRP (p=0.707) showed no statistically significant differences among CPS score groups.
 |
Table 3 Analysis of Clinical, Haematological and Biochemical Variables in Relation to the CPS Score |
As shown in Table 4, multivariate logistic regression analysis evaluating the effects of various clinical variables on CPS score 2–3, the probability of having CPS score 2–3 appeared to be increased in patients without pCR, although this difference was not statistically significant (OR: 2.20, 95% CI: 0.56–8.69, p=0.258). In terms of lymph node status (ypN), the probability of having CPS 2–3 was significantly increased in patients with stage N1 versus stage N0 (OR: 5.26, 95% CI: 1.80–15.33, p=0.002). Similarly, the probability of having CPS 2–3 was significantly higher in N2 (OR: 8.51, 95% CI: 2.02–35.91, p=0.004) and N3 stages (OR: 7.64, 95% CI: 1.25–46.46, p=0.027). The explanatory power of the model was R2=0.315, and the −2 Log Likelihood value was 123.56. These results show that the strongest predictor of CPS score 2–3 is advanced lymph node involvement (ypN0-N3).
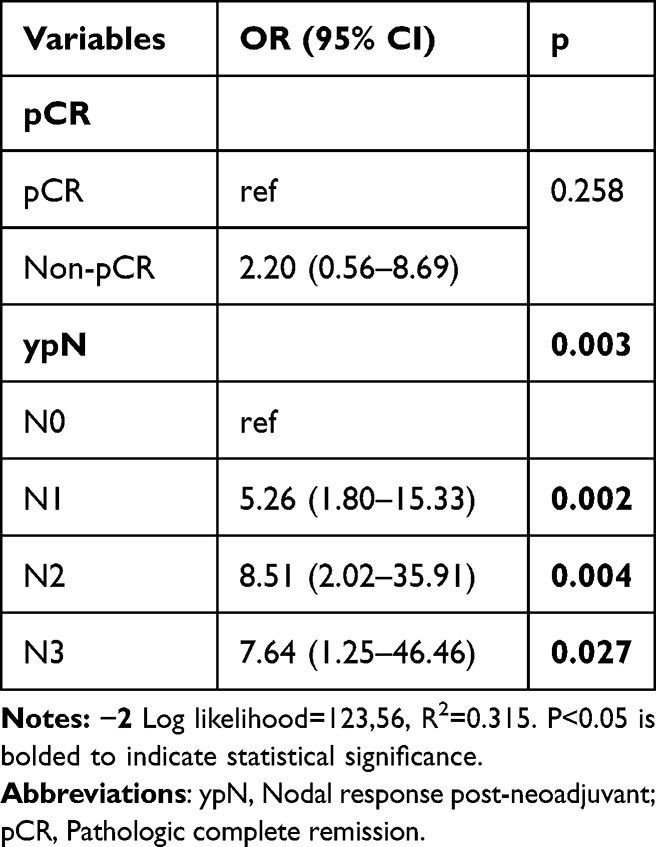 |
Table 4 Multivariate Logistic Regression Results of Various Clinical Variables on CPS Score 2–3 |
Discussion
The CPS score was developed to improve survival prediction by combining clinical and pathological staging, as the response to NAC in hormone-positive BC is limited and the pathological response is not strongly correlated with survival rates.2 Given the modest impact of NAC, research has focused on enhancing the predictive power of CPS to by incorporating additional clinical and pathological indicators to improve the prediction of survival and to avoid unnecessary chemotherapy. The stronger correlation between survival and the CPS score led us to investigate hematologic, clinical, inflammatory, and metabolic parameters that might be associated with the CPS score.
Breast cancer before the age 40 is known as high-risk disease. Despite the use of various age cut-off values in studies evaluating the relationship between age and NAC response in hormone-positive breast cancer, no statistically significant results were found.1,2 Similarly, in our study, age (p=0.106) was not statistically significant.
ER positivity low (%1-10) patient group is known to behave like triple-negative and have better NAC responses.20 In our study, there was no statistically significant relationship between the ER low group (p=0.331) and CPS scoring. This may be attributed to the small number of patients in the ER-low group (n=12) and the fact that the CPS score incorporates clinical stage in addition to pathological response.
In the study by Asano et al, a significant difference in pathological response to NAC was found in terms of grade. Grade 1, 2, and 3 tumors were compared, and better pathological response was obtained in grade 3 tumors.1 In our study, due to the small number of pCR patients (n=19), CPS score was compared with grade, and no statistically significant relationship was found. The majority of our patients being grade 2 may have contributed to the lack of statistical significance.
Joo et al reported that Ki67 was significantly associated with pCR following NAC, without distinguishing BC subtypes.11 Asano et al found a statistically significant relationship between Ki67 cut-off value of 14 and pathological response in hormone-positive subtype, but not with survival. Sheri et al did not find post-NAC Ki67 values prognostic in hormone-positive BC.1,13 In our study, due to the small number of patients achieving pCR (n=19), no statistically significant association was found between Ki67 and CPS score.
Pathological complete response (pCR) rates following NAC are higher in triple-negative and HER2-positive disease, and lower in hormone-positive disease. In our study, the pCR rate was 15.8%, which is consistent with the literature. Numerous studies in the literature have explored different classification systems for assessing pathological responses in NAC, including residual cancer burden (RCB), Miller-Payne, TILs (tumor infiltrating lymphocytes), post-NAC Ki67, post-NAC grade, and their combinations. The correlation between these classification systems and survival remains limited in hormone-positive breast cancer. Given the stronger correlation between CPS score and survival, our study found that pCR was statistically significant in terms of CPS score in univariate analysis (p=0.001), but not in multivariate logistic regression analysis (p=0.258).
Pre- and/or post-NAC lymph node positivity is known to affect the stage and prognosis of the disease. Considering that primary surgical treatment of hormone-positive subtype, which constitutes 65–70% of BC, affects complications and quality of life, axillary pathological complete response is important to avoid unnecessary axillary dissection. Hennessy et al and Rouzier et al found that axillary response had prognostic significance, without differentiating hormone-positive subtype.21,22 Symmans et al identified post-NAC lymph node positivity as a prognostic factor in hormone-positive BC.7 Similarly, in our study, post-NAC axillary pathological response (ypN) was associated with CPS score (p=0.003). These results support the clinical significance and the potential role of ypN guiding adjuvant treatment decisions and may contribute to the individualization of care and de-escalation of axillary surgery.
In the study by Lee et al, pathological complete response rates were found to be similar between patients receiving anthracycline or anthracycline+taxane.23 Estévez et al found better clinical and pathological responses with anthracycline+taxane versus anthracycline alone.24 In our study, there was no statistically significant difference in CPS score between anthracycline+taxane and anthracycline alone.
Inflammation within the tumor microenvironment is known to influence both proliferation and survival. NLR, a well recognized peripheral marker of inflammation, has been reported as a prognostic in many studies.25–27 In the context of NAC response in BC, several studies have identified NLR as predictive of pathological response and survival, while others found no association.28–30 In our study, there was not statistically significant association between CPS score and NLR. This may be due to the heterogeneous nature of the tumor immune microenvironment in hormone-positive breast cancer or to the complex relationship between the tumor microenvironment and inflammation.16
Other systemic inflammation indicators, PNI and SII, have been found prognostic in some tumor types.31,32 In our study, PNI and SII were not statistically significant association with CPS score in hormone-positive BC. This may be attributed to the immunosuppressive nature of the tumor microenvironment in hormone-positive BC, as well as the inclusion of early-stage patients.16
High FPG is known to be significant in the prognosis and recurrence of breast cancer due to insulin resistance and metabolic syndrome. Arıcı et al found high FPG to be associated with low pathological response to NAC.18,19 However, there was no subtype differentiation. In our study, high FPG was not statistically significantly associated to the CPS score in the hormone-positive subtype.
Given the limited number of pCR events and CPS score subgroups, it is possible that some non-significant associations particularly for inflammatory and metabolic parameters may be due to insufficient statistical power rather than true lack of effect.
Our study has several limitations. First, it was a single-center, retrospective analysis. Secondly, instead of directly evaluating OS and DFS, we used the indirectly survival score CPS. The relatively small sample size and the low number of events in key subgroups (such as pCR and CPS=0 groups) reduce the statistical power of our analysis and increase the risk of Type II error (false negative results). Some meaningful associations may have therefore failed to reach statistical significance. The wide confidence intervals observed for some variables (eg, the N3 group) indicate statistical instability, likely due to the limited number of events, and these findings should be interpreted with caution. Our results should be confirmed with multicenter, prospective studies involving larger patient groups.
Conclusion
This is the first study to compare inflammatory and metabolic parameters with the CPS survival score in hormone-positive BC treated with NAC. Pathological responses to NAC in hormone-positive BC are not strongly associated with survival. In our study, pCR was not a significant predictor in the multivariate analysis, whereas ypN was associated with survival score (CPS). As metabolic and inflammatory parameters showed were not statistically significant association with CPS score, further validation in larger studies is warranted. Considering the low response rates to NAC in hormone-positive breast cancer, post-NAC ypN status may serve as a stronger prognostic value than pCR in clinical decision-making.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Approval was obtained from the Ethics Committee of Atatürk University Faculty of Medicine (2024/16). All procedures were conducted in accordance with the principles of the Declaration of Helsinki. Given the retrospective design of the study, the requirement for informed consent was waived by the Ethics Committee of Atatürk University Faculty of Medicine. In this retrospective study, data were anonymized and no patient identifiers were used.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Asano Y, Kashiwagi S, Goto W, et al. Prediction of survival after neoadjuvant chemotherapy for breast cancer by evaluation of tumor-infiltrating lymphocytes and residual cancer burden. BMC Cancer. 2017;17(1):888. doi:10.1186/s12885-017-3927-8
2. Jeruss JS, Mittendorf EA, Tucker SL, et al. Combined use of clinical and pathologic staging variables to define outcomes for breast cancer patients treated with neoadjuvant therapy. J Clin Oncol. 2008;26(2):246–9.
3. Marmé F, Lederer B, Blohmer J-U, et al. Utility of the CPS+EG staging system in hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer treated with neoadjuvant chemotherapy. Euro J Cancer. 2016;53:65–74. doi:10.1016/j.ejca.2015.09.022
4. Wang H, Mao X. Evaluation of the efficacy of neoadjuvant chemotherapy for breast cancer. Drug Design Develop Therapy. 2020;14:2423–2433. doi:10.2147/DDDT.S253961
5. Matsunuma R, Watanabe T, Hozumi Y, et al. Preoperative concurrent endocrine therapy with chemotherapy in luminal B-like breast cancer. Breast Cancer. 2020;27(5):819–827. doi:10.1007/s12282-020-01077-0
6. Bonnefoi H, Litiere S, Piccart M, et al. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 Phase III trial. Ann Oncol. 2014;25(6):1128–1136. doi:10.1093/annonc/mdu118
7. Symmans WF, Wei C, Gould R, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049–1060.
8. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi:10.1016/S0140-6736(13)62422-8
9. Ai X, Liao X, Wang M, et al. Prognostic value of lymph node ratio in breast cancer patients with adequate pathologic evidence after neoadjuvant chemotherapy. Med Sci Monitor. 2020;26:e922420.
10. Yau C, Osdoit M, van der Noordaa M, et al. Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: a multicentre pooled analysis of 5161 patients. Lancet Oncol. 2022;23(1):149–160. doi:10.1016/S1470-2045(21)00589-1
11. Joo S, Ko ES, Kwon S, et al. Multimodal deep learning models for the prediction of pathologic response to neoadjuvant chemotherapy in breast cancer. Sci Rep. 2021;11(1):18800. doi:10.1038/s41598-021-98408-8
12. Lee SM, Bae SK, Kim TH, et al. Value of 18F-FDG PET/CT for early prediction of pathologic response (by residual cancer burden criteria) of locally advanced breast cancer to neoadjuvant chemotherapy. Clin Nucl Med. 2014;39(10):882–886. doi:10.1097/RLU.0000000000000531
13. Sheri A, Smith IE, Johnston SR, et al. Residual proliferative cancer burden to predict long-term outcome following neoadjuvant chemotherapy. Ann Med Oncol. 2015;26(1):75–80.
14. Dougan M, Dranoff G. Immune therapy for cancer. Annu Rev Immunol. 2009;27(1):83–117. doi:10.1146/annurev.immunol.021908.132544
15. Ingold Heppner B, Untch M, Denkert C, et al. Tumor-infiltrating lymphocytes: a predictive and prognostic biomarker in Neoadjuvant-treated HER2-positive breast cancer. Clin Cancer Res. 2016;22(23):5747–5754. doi:10.1158/1078-0432.CCR-15-2338
16. Cai Y-W, Liu -C-C, Zhang Y-W, et al. MAP3K1 mutations confer tumor immune heterogeneity in hormone receptor–positive HER2-negative breast cancer. J Clin Invest. 2025;135(2):e183656. doi:10.1172/JCI183656
17. Buyukbayram ME, Hannarici Z, Duzkopru Y, et al. The effect of C-reactive protein/lymphocyte ratio (CLR) on PFS in metastatic breast cancer patients treated with CDK4/6 inhibitors: a novel biomarker. Breast. 2024;16:329–339. doi:10.2147/BCTT.S464161
18. Arici S, Geredeli C, Secmeler S, Cekin R, Sakin A, Cihan S. The effects of diabetes and fasting plasma glucose on treatment of breast cancer with neoadjuvant chemotherapy. Curr Probl Cancer. 2020;44(1):100485. doi:10.1016/j.currproblcancer.2019.05.007
19. Zhou Z, Zhang Y, Li Y, et al. Metabolic syndrome is a risk factor for breast cancer patients receiving neoadjuvant chemotherapy: a case-control study. Front Oncol. 2023;12:1080054. doi:10.3389/fonc.2022.1080054
20. Ohara AM, Naoi Y, Shimazu K, et al. PAM50 for prediction of response to neoadjuvant chemotherapy for ER-positive breast cancer. Breast Cancer Res Treat. 2019;173(3):533–543. doi:10.1007/s10549-018-5020-7
21. Hennessy BT, Hortobagyi GN, Rouzier R, et al. Outcome after pathologic complete eradication of cytologically proven breast cancer axillary node metastases following primary chemotherapy. J Clin Oncol. 2005;23(36):9304–9311. doi:10.1200/JCO.2005.02.5023
22. Rouzier R, Pusztai L, Delaloge S, et al. Nomograms to predict pathologic complete response and metastasis-free survival after preoperative chemotherapy for breast cancer. J Clin Oncol. 2005;23(8331):8339. doi:10.1200/JCO.2005.01.2898
23. Lee IH, Lee SJ, Lee J, et al. Utility of 18F-FDG PET/CT for predicting pathologic complete response in hormone receptor-positive, HER2-negative breast cancer patients receiving neoadjuvant chemotherapy. BMC Cancer. 2020;20(1):1106. doi:10.1186/s12885-020-07505-w
24. Estèvez LG, Gradishar WJ. Evidence-based use of neoadjuvant taxane in operable and inoperable breast cancer. Clin Cancer Res. 2004;10(10):3249–3261. doi:10.1158/1078-0432.CCR-03-0133
25. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
26. Tomita M, Shimizu T, Ayabe T, Yonei A, Onitsuka T. Preoperative neutrophil to lymphocyte ratio as a prognostic predictor after curative resection for non-small cell lung cancer. Anticancer Res. 2011;31(9):2995–2998.
27. Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Kubota K. Combination of platelet count and neutrophil to lymphocyte ratio is a useful predictor of postoperative survival in patients with colorectal cancer. Br J Cancer. 2013;109(2):401–407. doi:10.1038/bjc.2013.350
28. Noh H, Eomm M, Han A. Usefulness of pretreatment neutrophil to lymphocyte ratio in predicting disease-specific survival in breast cancer patients. J Breast Cancer. 2013;16(1):559. doi:10.4048/jbc.2013.16.1.55
29. Azab B, Bhatt VR, Phookan J, et al. Usefulness of the neutrophil-to-lymphocyte ratio in predicting short- and long-term mortality in breast cancer patients. Ann Surg Oncol. 2012;19(1):217–224. doi:10.1245/s10434-011-1814-0
30. Suppan C, Bjelic-Radisic V, La Garde M, et al. Neutrophil/lymphocyte ratio has no predictive or prognostic value in breast cancer patients undergoing preoperative systemic therapy. BMC Cancer. 2015;15(1):1027. doi:10.1186/s12885-015-2005-3
31. Mantzorou M, Koutelidakis A, Theocharis S, Giaginis C. Clinical value of nutritional status in cancer: what is its impact and how it affects disease progression and prognosis? Nutr Cancer. 2017;69(8):1151–1176. doi:10.1080/01635581.2017.1367947
32. Yildirim S, Dogan A, Akdag G, et al. The role of laboratory indices on treatment response and survival in breast cancer receiving neoadjuvant chemotherapy. Sci Rep. 2024;14(1):12123. doi:10.1038/s41598-024-63096-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimal Treatment Strategies for Resectable Locally Advanced Esophageal Squamous Cell Carcinoma: A Real-World Triple Cohort Analysis Using Propensity Score Matching
Han D, Tian J, Zhao J, Hao S
International Journal of General Medicine 2023, 16:5467-5479
Published Date: 22 November 2023