")
Back to Journals » International Journal of General Medicine » Volume 16
Optimal Treatment Strategies for Resectable Locally Advanced Esophageal Squamous Cell Carcinoma: A Real-World Triple Cohort Analysis Using Propensity Score Matching
Authors Han D , Tian J, Zhao J , Hao S
Received 14 September 2023
Accepted for publication 16 November 2023
Published 22 November 2023 Volume 2023:16 Pages 5467—5479
DOI https://doi.org/10.2147/IJGM.S440270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dan Han,1,2 Jing Tian,3 Junfeng Zhao,2 Shaoyu Hao4,5
1Department of Radiation Oncology, Shandong University Cancer Center, Jinan, Shandong, People’s Republic of China; 2Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University, and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 3Department of Radiation Oncology, Jinan Zhangqiu District People’s Hospital, Jinan, Shandong, People’s Republic of China; 4Department of Thoracic Surgery, Shandong University Cancer Center, Jinan, Shandong, People’s Republic of China; 5Department of Thoracic Surgery, Shandong Cancer Hospital and Institute, Shandong First Medical University, and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China
Correspondence: Shaoyu Hao, Department of Thoracic Surgery, Shandong University Cancer Center, Jinan, Shandong, China; Department of Thoracic Surgery, Shandong Cancer Hospital and Institute, Shandong First Medical University, and Shandong Academy of Medical Sciences, Jinan, Shandong, 250117, People’s Republic of China, Tel +86 13188870730, Email [email protected]
Purpose: This study aims to identify the most effective treatment approach and compares the survival rates, along with complications, in patients with locally resectable esophageal squamous cell carcinoma (ESCC) who were treated with one of the three treatment patterns: neoadjuvant chemotherapy followed by surgery (NCT+S), neoadjuvant chemoradiotherapy followed by surgery (NCRT+S), or surgery followed by chemoradiotherapy (S+CRT).
Methods: We conducted a retrospective analysis of the medical records of ESCC patients who received one of these treatments between March 2015 and March 2022. This analysis aimed to identify differences in long-term survival, pathological responses, and complications across the three treatment groups. To address potential confounding factors, propensity score matching (PSM) and Cox proportional hazards models were utilized.
Results: This study included a cohort of 715 patients: 197 in the NCT+S group, 188 in the NCRT+S group, and 330 in the S+CRT group, all meeting the selection criteria. After PSM, the median disease-free survival (DFS) time was 38.9 months, 25.6 months, and 15.3 months for NCRT+S, NCT+S, and S+CRT groups, respectively. There were statistically significant differences in the 5-year DFS and 5-year OS among the three groups (P=0.04 and P=0.02, post-matching, respectively). Notably, neoadjuvant therapy showed a correlation with increased postoperative anastomotic leakage rates (17.5% in NCRT+S, 10% in NCT+S, and 5% in S+CRT; P=0.03, post-matching), regardless of the PSM adjustment.
Conclusion: The findings indicate that neoadjuvant therapy before surgery offers a significant survival advantage over postoperative adjuvant therapy for patients with locally advanced resectable ESCC. Despite similar safety profiles, neoadjuvant therapy appears to be associated with a higher incidence of anastomotic leakage after surgery.
Keywords: neoadjuvant therapy, esophageal squamous cell carcinoma, postoperative adjuvant therapy, prognosis
Introduction
In 2020, esophageal cancer (EC) was the seventh most commonly diagnosed cancer worldwide, with approximately 604,000 new cases, and it ranked sixth in mortality, resulting in about 544,000 deaths.1 A study utilizing cancer registry data revealed that esophageal squamous cell carcinoma (ESCC) is the main histological subtype in China, accounting for 85.79% of the cases reported.2 Coordinated multidisciplinary treatment approaches are crucial for effectively managing locally advanced EC. Numerous key clinical studies3–6 have supported the use of neoadjuvant therapy, encompassing neoadjuvant chemoradiotherapy (NCRT) or neoadjuvant chemotherapy (NCT) followed by surgical intervention, as the preferred treatment for resectable EC. The CROSS3 and NEOCRTEC50104 trials were instrumental in establishing NCRT as the standard approach for treating locally advanced operable ESCC, demonstrating superior overall survival (OS) compared to surgery alone. Studies such as OEO25 and MAGIC6 indicated that NCT succeeded by surgery could improve 5-year OS by 6% and 13%, respectively, when compared to surgery alone. The National Comprehensive Cancer Network does not recommend postoperative adjuvant therapy for EC,7 whereas Chinese ESCC guidelines advise postoperative chemotherapy, radiotherapy, or chemoradiotherapy for patients with pN+ and pT3-4a ESCC to improve prognosis.8
Two prospective studies have investigated the efficacy of NCRT and NCT in the treatment of locally advanced ESCC. The JCOG1109NExT three-arm Phase III trial demonstrated that the combination of docetaxel, cisplatin, and 5-FU (DCF) significantly enhanced OS when compared to the cisplatin and 5-FU (CF) dual-therapy regimen. Additionally, the study observed no significant difference in 3-year OS rates between the dual-agent chemotherapy and NCRT cohorts.9 A prospective multicenter randomized trial in China (CMISG1701) also indicated equivalent OS and progression-free survival between locally advanced ESCC patients treated with NCRT and NCT.10 Nevertheless, several studies suggest that postoperative adjuvant chemotherapy or radiotherapy can substantially reduce local recurrence and enhance patient survival in comparison to surgery alone.11,12 Only a few studies have examined the effects of varying the sequence of surgical and chemoradiotherapy on the prognosis of patients with resectable ESCC.
In response to this gap, we executed a real-world propensity score-matched (PSM) study, aiming to identify the most efficacious treatment approach and assess the differences in survival, as well as complications among resectable ESCC patients who underwent NCT followed by surgery (NCT+S), NCRT followed by surgery (NCRT+S), or surgery followed by chemoradiotherapy (S+CRT).
Patients and Methods
Patients Selection
We conducted a retrospective analysis of ESCC patients who underwent NCRT, NCT plus esophagectomy, or esophagectomy plus adjuvant CRT at our institution between March 2015 and March 2022. The inclusion criteria for this study: histopathological confirmation of ESCC; locally advanced disease stage appropriate for surgical resection (cT1-2N+ and cT3-4aN0/N+), as per the 8th edition of the American Joint Committee on Cancer (AJCC) Tumor Node Metastasis (TNM) Classification; Eastern Cooperative Oncology Group performance status of 0–1; normal hematologic, hepatic, and renal functions, and no history of other malignancies. The research protocol was approved by the Ethics Committee of Cancer Hospital Affiliated to Shandong First Medical University. As this was a retrospective investigation, the necessity for written informed consent was exempted.
Chemotherapy
Both preoperative and postoperative concurrent chemotherapy primarily included platinum-based and fluorouracil drugs (PF regimen), or platinum-based drugs combined with docetaxel, paclitaxel, or albumin paclitaxel (taxane-platinum regimen), all administered intravenously. The PF regimen consisted of platinum-based drugs (nedaplatin at 75 mg/m2, carboplatin with an area under the curve of 5, or cisplatin at 25 mg/m2 on days 1–3) and fluorouracil at 50 mg/m2 on days 1–5 or alternatively S-1 at 60 mg/m2/day orally twice a day on days 1–14. In contrast, the taxane-platinum regimen contained docetaxel (75 mg/m2), paclitaxel (135–175 mg/m2), or albumin-bound paclitaxel (260 mg/m2). Patients in the NCT and NCRT groups typically received 1–3 cycles of preoperative chemotherapy (either PF or taxane-platinum regimens) every three weeks, with an average of two cycles. For the S+CRT group, patients were administered 2–6 cycles of postoperative adjuvant chemotherapy (either PF or taxane-platinum regimens) every three weeks, with a median of four cycles.
Radiotherapy
Patients in the NCRT group were subjected to radiation doses ranging from 40 to 50.4 Gy, while those in the S+CRT group received radiation doses from 45 to 50.4 Gy. Both sets of patients were administered these doses in fractions of 1.8–2.0 Gy, following a schedule of five fractions per week. The radiotherapy techniques employed were intensity-modulated radiation therapy or volumetric intensity-modulated arc therapy, both using 6 MV X-rays.
Surgical Treatment
Several esophagectomy techniques were performed, including thoracostomy esophagectomy or minimally invasive esophagectomy (MIE), each paired with gastric reconstruction and standard lymphadenectomy. The two primary radical surgeries for ESCC mainly include the left thoracic approach esophagectomy (Sweet procedure) and the right thoracic, upper abdominal, and left neck three-incision esophagectomy (McKeown procedure). Esophagectomies were scheduled 4–6 weeks after neoadjuvant therapy in both the NCT and NCRT groups.
Pathology
The pathological TNM stage diagnoses were independently assessed by two pathologists utilizing hematoxylin and eosin staining alongside immunohistochemistry. Their assessments conformed to the protocols outlined in the 8th edition of the AJCC guidelines. The tumor regression grade (TRG) was categorized into four grades, from 0 to 3, based on the criteria by the College of American Pathologists.7 Complete pathologic response (pCR) was defined as an absence of viable tumor cells (grade 0); otherwise, cases were designated as having a non-complete pathologic response (non-pCR) (grade 1 consisted of residual solitary tumor cells or small clusters of tumor cells; grade 2 referred to partial tumor residuals with substantial interstitial fibrosis; and grade 3 indicated negligible or absent tumor cell regression). An R0 resection, indicating a complete tumor resection with a negative microscopic incision margin signifying no residual tumor, was the target outcome.
Follow-Up
The initial follow-up was scheduled one month post-surgery. Thereafter, patients were followed up every three months in the initial two years, bi-annually from the third to the fifth year, and annually until the conclusion of the study. Each follow-up encompassed a medical history review, physical examination, hematological testing, and a comprehensive imaging suite which included cervical, chest, and abdominal computed tomography (CT), along with upper gastrointestinal radiography. If deemed necessary, additional assessments like gastroscopy, magnetic resonance imaging, positron emission tomography-CT, and bone scans were conducted.
Statistical Analysis
Disease-free survival (DFS) was defined as the interval from surgery to the time of disease progression or the last follow-up. OS was determined as the period from the first day of treatment until death or the last follow-up.
For quantitative data, when the distribution is normal, a t-test is used for comparisons between two groups, and analysis of variance is employed for three or more groups. If the distribution is not normal, the Mann–Whitney U-test is used for two groups, and the Kruskal–Wallis test is applied for three or more groups. For categorical data, Fisher’s exact test or chi-square tests are employed. DFS and OS across the three groups were compared employing the Kaplan–Meier method and the Log rank test. A Cox proportional hazards model was used to adjust for confounding factors and to identify independent predictors of OS and DFS, with significance set at P < 0.05.
In order to reduce the effects of confounding factors on outcomes across the groups, we applied a 1:1 PSM technique using the nearest neighbor algorithm (caliper: 0.2). The propensity score was determined using a logistic regression model based on the following confounding variables: sex, age (categorized as ≥60 years or not), smoking history, alcohol use history, comorbidities, family history of malignancy, tumor location, and clinical T and N stages (classified as T1, T2, T3, T4, and N0 or N+). All statistical analyses were performed using SPSS 24.0 for Windows (IBM Corp, Chicago, IL) and R version 4.2.1.
Results
Patient Characteristics
A total of 715 patients meeting the inclusion criteria were included in the study, distributed as follows: 197 underwent NCRT, 188 had NCT, and 330 received surgery followed by CRT. There were significant differences in age (P=0.033), tumor location (P=0.002), and clinical stage (P<0.001) among the three unbalanced groups. To minimize confounding bias, we implemented a 1:1 PSM study involving the NCRT (n = 80), NCT (n = 80), and S+CRT (n = 80) cohorts. Post-PSM, clinical characteristics were well distributed across the three groups. We did not include chemotherapy regimens as a factor for propensity score matching because, before PSM, 12.7% of patients in the S+CRT group only received adjuvant radiotherapy post-surgery, most of whom were at clinical stage T3N0. This also resulted in variations in chemotherapy regimens among the groups. The baseline clinical characteristics of the three groups, both before and after PSM, are detailed in Table 1.
 |
Table 1 Comparison of Baseline Clinical Characteristics Among Three Groups Before and After Propensity Score Matching |
Surgery‑Related Procedures
Significant differences were found among the three groups, before and after PSM, regarding the surgical approach, surgical type, and lymph node dissection counts (as shown in Table 2). The distribution of open esophagectomy (OE) and MIE significantly varied among the groups, with a higher prevalence of OE in the NCT and S+CRT groups compared to the NCRT group (73.8% vs 75% vs 51.2%, respectively; P=0.011 post-PSM). After PSM, within the NCRT group, three patients (3.8%), two patients (2.5%) in the NCT group, and one patient (1.2%) in the S+CRT group initially intended for MIE were instead converted to OE. A higher percentage of patients in the NCRT group underwent the McKeown esophagectomy compared to the NCT and S+CRT groups (70% vs 37.5% vs 33.8%, respectively; P<0.001 post-PSM). The NCRT group had fewer lymph node dissection counts than the other two groups (P < 0.001).
 |
Table 2 Comparison of Surgical Procedures Among Three Groups Before and After Propensity Score Matching |
Surgery-Related Complications
Surgery-associated complications in the matched groups were comparable to those in the unmatched groups (as detailed in Table 3). A higher incidence of postoperative complications was observed in patients who underwent NCRT compared to those in the NCT and S+CRT groups (27.5%, 18.8% and 11.2%, respectively; P=0.033 after PSM). In the NCRT cohort, 14 patients (17.5%) suffered from anastomotic leakage, a significantly higher number compared to the 8 patients (10.0%) in the NCT group and 4 patients (5.0%) in the S+CRT group (P=0.038 post-PSM). Other postoperative complications, such as anastomotic stenosis or pulmonary complications, showed no significant differences in incidence among the three groups, both before and after matching. Anastomotic stenosis is defined as a narrowing at the site of the anastomosis and adjacent areas, which is not due to tumor recurrence at the anastomosis but is caused by the proliferation of granulation tissue or scarring around the anastomosis. It is characterized by a diameter of less than 1 cm at the narrowed section when assessed endoscopically, or the inability of a standard endoscope (with a diameter of about 1 cm) to pass through, often accompanied by varying degrees of dysphagia.13
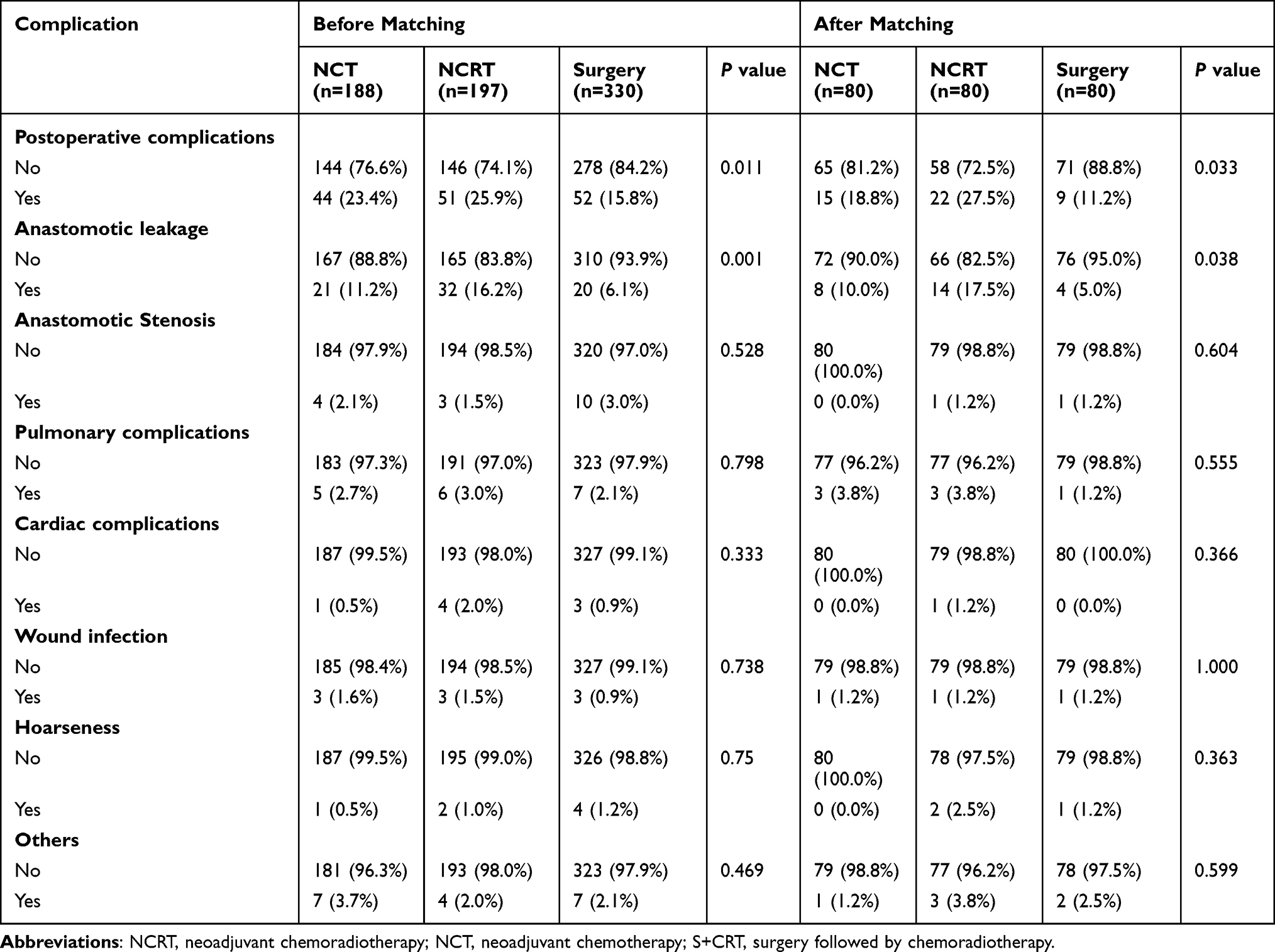 |
Table 3 Comparison of Surgery-Related Complication Among Three Groups Before and After Propensity Score Matching |
Pathology
The rate of successful R0 resections across all three groups demonstrated similarity (NCT 97.5%, NCRT 98.7%, and S+CRT 96.2%, P=0.599 post-PSM), consistent with the cohort prior to matching. Prior to matching, incidences of neural and lymphovascular invasion were significantly lower in the NCRT group (P<0.001). However, post-matching, there were no significant differences in neural invasion across the groups (P=0.101). Further details can be found in Table 4.
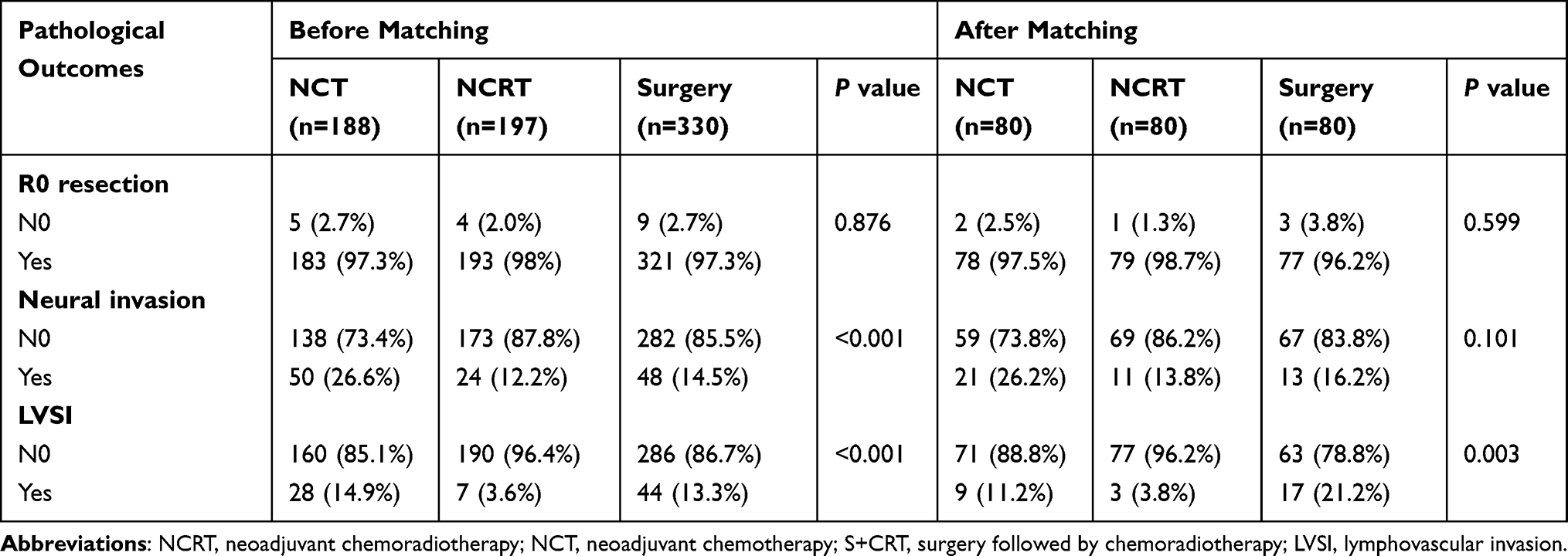 |
Table 4 Comparison of Pathological Outcomes Among Three Groups Before and After Propensity Score Matching |
Pathological differences between NCRT and NCT groups are detailed in Table 5. Compared to the NCT group, the NCRT group showed a higher rate of pCR. Post-matching, pCR rates were 35% for NCRT and 2.5% for NCT (P<0.001). The TRG 0 rate for the primary tumor was 48.8% in the NCRT cohort, significantly higher than the NCT cohort (P<0.001 post-PSM). Correspondingly, patients receiving NCRT demonstrated significantly higher rates of ypT0/Tis (46.2% vs 8.8%; P<0.001, post-PSM) and ypN0 (78.8% vs 45%; P<0.001, post-PSM) compared to those in the NCT cohort. The pathological results were consistent in both matched and unmatched NCRT and NCT cohorts.
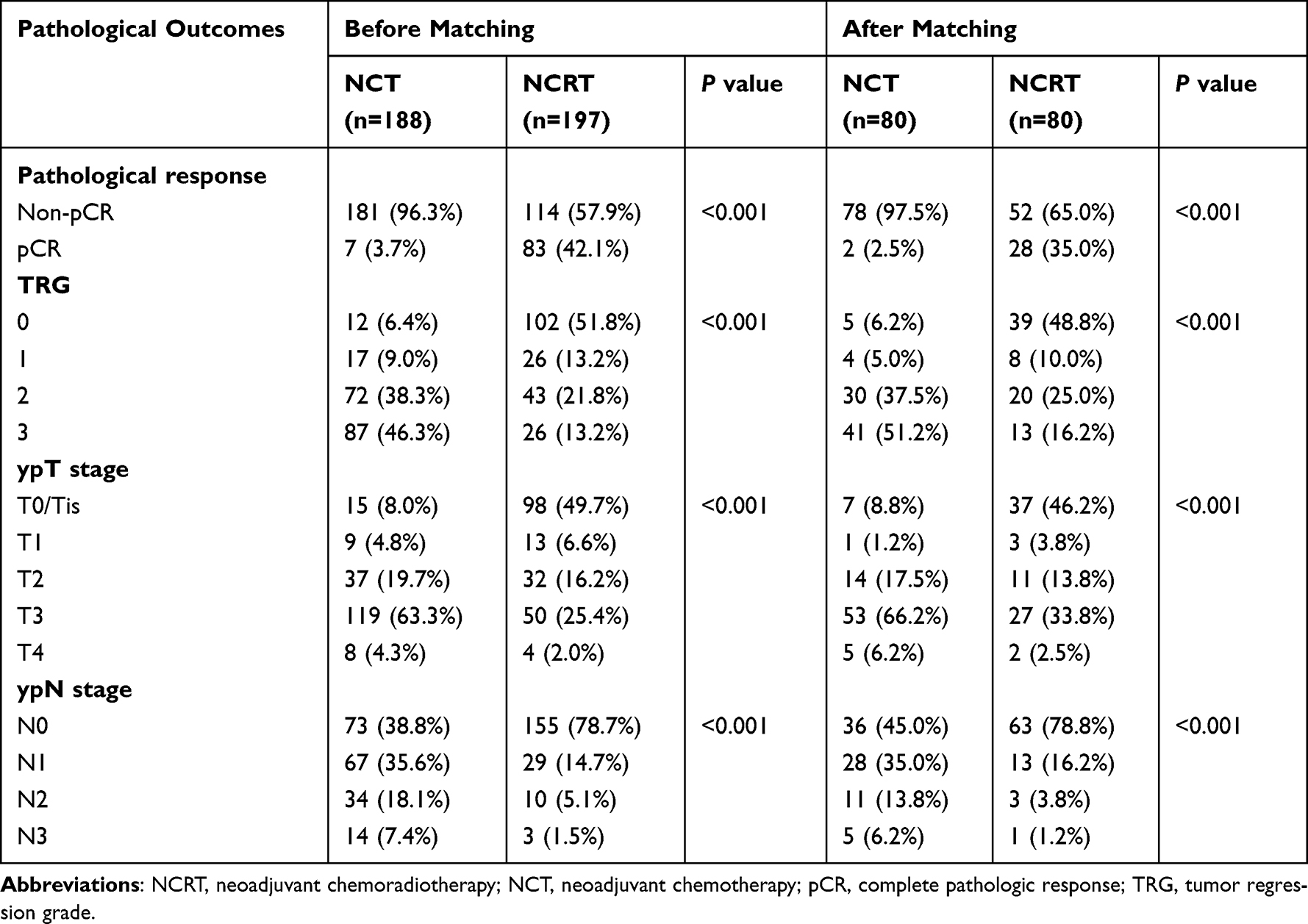 |
Table 5 Comparison of Pathological Outcomes Between the NCT Group and NCT Group Before and After Propensity Score |
OS and DFS
In the cohort under study, the median duration of follow-up was 19.3 months for the NCRT group, with a range from 4 to 66.9 months; 31.45 months for the NCT group, with the duration spanning 2 to 68.4 months; and 20.3 months for the S+CRT group, with a follow-up interval extending from 3 to 90.1 months prior to the initiation of the matching process. The NCT group exhibited a median OS of 47.7 months, with a 95% confidence interval (CI) of 32.8 months to not applicable (NA). This was significantly higher than the 26.3 months median OS observed in the S+CRT group (95% CI: 24.2–28.4 months). As for the median DFS, it was 27.8 months in the NCT group (95% CI: 18.7–43.1 months), compared to 14.6 months in the S+CRT group (95% CI: 12.0–18.7 months). For the NCRT group, the median OS and DFS could not be calculated, with the 95% confidence intervals being 55.9 months to NA and 38.9 months to NA, respectively. There were significant differences in the 5-year OS and DFS (P<0.0001 for OS and P<0.0001 for DFS) across the non-matched groups (Figure 1A and B).
 |
Figure 1 Unmatched Kaplan-Meier survival analysis of DFS (A) and OS (B) among NCT, NCRT and S+CRT groups. Propensity-matched Kaplan-Meier survival analysis of DFS (C) and OS (D) among NCT, NCRT and S+CRT groups. Abbreviations: OS, overall survival; DFS, disease-free survival; NCRT, neoadjuvant chemoradiotherapy; NCT, neoadjuvant chemotherapy; S+CRT, surgery followed by chemoradiotherapy. |
Post-matching, the median follow-up duration was 20.6 months (ranging between 4 and 66.9 months) in the NCRT cohort, 31.8 months (from 7.5 to 68.4 months) in the NCT cohort, and 19.8 months (between 3 and 77.3 months) in the S+CRT cohort. The median OS for the S+CRT group was 30.4 months, with a 95% CI of 21.3 months to NA. In contrast, the median OS remained undefined for both the NCRT group (95% CI: 47.5 months to NA) and the NCT group (95% CI: 39.9 months to NA). Regarding the median DFS, it was recorded as 38.9 months (95% CI: 30.0 months to NA) for the NCRT group, 25.6 months (95% CI: 14.7 months to NA) for the NCT group, and 15.3 months (95% CI: 9.4 to 48.2 months) for the S+CRT group. There were statistically significant differences in the 5-year OS and 5-year DFS across the three groups (P=0.02 and P=0.04, respectively) (Figure 1C and D).
Independent predictors for OS and DFS were identified using the Cox proportional hazards model prior to matching (Table 6). Multivariate analysis revealed that the surgery followed by chemoradiotherapy was a significant independent factor associated with poorer OS compared to NCRT. Furthermore, postoperative pathological T and N stages surfaced as substantial independent predictors for both OS and DFS (P < 0.001).
 |
Table 6 Multivariate Analyses of Prognostic Factors Related to OS and DFS Before Propensity Score |
Discussion
A comprehensive, surgery-focused treatment is standard for locally advanced resectable ESCC, including either preoperative neoadjuvant treatments like NCRT and NCT or surgery followed by adjuvant therapies (chemotherapy/radiotherapy). On the one hand, CROSS3 trial from the Netherlands in 2012 and the NEOCRTEC50104 study from China in 2018 have offered significant evidence for the application of NCRT in resectable ESCC. Prospective phase III clinical trials JCOG1109NExT9 and CMISG170110 concluded that surgical resection after NCT and NCRT for resectable EC were equivalent in efficacy. The 2022 CSCO Esophageal Cancer Treatment Guidelines of China recommend adding NCT for resectable EC, specifically for stages cT1b-cT2N+ or cT3-cT4a any N.14 However, it remains uncertain whether NCT can supplant the treatment mode of NCRT in China. Both NCRT and NCT are recommended as first-line treatments for locally advanced resectable ESCC, yet the optimal strategy remains a subject of debate. On the other hand, although preoperative chemoradiotherapy followed by surgery is recognized as an effective strategy for EC treatment, there are few studies specifically addressing the impact of the order of EC surgery and chemoradiation on prognosis, with conflicting results. Hong et al15 through analysis of the Surveillance, Epidemiology, and End Results database proved that preoperative chemoradiotherapy is superior to postoperative chemoradiotherapy for locally advanced EC. However, prospective trials by Lv et al16 and propensity-matched studies by Hsu et al11 have indicated that preoperative and postoperative chemoradiation offer similar survival benefits for patients with locally advanced ESCC. Whether neoadjuvant chemoradiation and adjuvant postoperative chemoradiotherapy are equivalent for ESCC remains a question worthy of further investigation. Multimodal therapy for locally advanced ESCC is currently the best treatment strategy. The optimal approach for patients with EC continues to be a topic of discussion, as only a handful of studies have compared the results of resectable ESCC patients treated with NCRT followed by surgery, NCT followed by surgery, or surgery complemented with adjuvant chemoradiotherapy. We carried out a PSM study to examine the clinicopathological features and survival outcomes of patients treated with NCRT, NCT, and surgery followed by adjuvant chemoradiotherapy. Our findings highlighted the 5-year DFS and OS advantage of neoadjuvant therapy followed by surgery over surgery combined with adjuvant chemoradiotherapy but also found that neoadjuvant therapy was linked with an elevated rate of postoperative anastomotic leakage, both before and after PSM.
Our study is retrospective in nature, and all our patients are diagnosed with locally advanced resectable ESCC. We utilized PSM to ensure balanced baseline characteristics among the three groups. Notably, prior to matching, we observed a higher proportion of patients aged under 60, and more with tumors located in the lower esophagus, within the NCRT group. This may reflect surgical concerns about complications, including anastomotic fistulas. Such complications might be exacerbated by radiation-induced fibrosis in the mid-to-upper esophagus. The decision regarding the clinical treatment regimen was primarily based on a multidisciplinary team (MDT) approach. Each case was discussed within a multidisciplinary oncology team, which consisted of surgical oncologists, gastrointestinal medical oncologists, radiation oncologists, and radiologists. This team-based approach guaranteed the selection of the most suitable individualized treatment plans leveraging collective expertise. For instance, patients with esophageal ulcers might choose between neoadjuvant therapy or direct surgery. Furthermore, patient preference played a role in the treatment options. After reviewing the potential benefits, risks, and side effects of each treatment option, some patients may express a preference that was considered.
NCRT continues to be a standard treatment for resectable, locally advanced ESCC. Yet, a significant proportion of ESCC patients in China opt for surgery, and the Chinese guidelines recommend postoperative adjuvant chemoradiotherapy for patients at the pT3-4aN0 or pN+ stage.8 Based on these guidelines, a PSM study17 revealed that postoperative radiotherapy was significant association with improved OS and DFS in pT3N0M0 ESCC patients. Therefore, in our research, patients with pT3N0M0 received only postoperative radiotherapy, while those with pT4 or N+ were treated with postoperative adjuvant chemoradiotherapy. The 5-year DFS and OS were significantly higher in patients undergoing preoperative chemoradiotherapy compared to those receiving postoperative chemoradiotherapy. Yu et al18 supported this, showing that preoperative radiotherapy improved 5-year OS relative to postoperative radiotherapy in TNM stage II/III ESCC patients. The efficacy of adjuvant therapy for ESCC is still under debate due to the absence of high-quality randomized trials. Several retrospective studies19–24 have evaluated the role of adjuvant therapy in locally advanced operable ESCC, yielding mixed results concerning DFS and OS. Li et al19 found that adding postoperative chemoradiotherapy in pN+ ESCC patients correlated with increased in 3-year DFS and OS. A meta-analysis20 involving 8198 patients suggested that postoperative radiotherapy may improve DFS and reduce the risk of locoregional recurrence in ESCC patients. Similarly, Zeng et al21 reported that postoperative radiotherapy lowered the locoregional recurrence rate in TNM stage III ESCC patients. Song et al22 observed that postoperative chemoradiotherapy significantly reduced distant metastasis compared to postoperative radiotherapy in pN+ stage ESCC patients. Conversely, research by Zou et al23 and Li et al24 found no significant differences in locoregional recurrence or distant metastasis between patients receiving postoperative chemoradiotherapy or postoperative radiotherapy. Future high-quality prospective studies are necessary to establish the most effective postoperative adjuvant strategy for ESCC patients.
The combination of surgery and adjuvant chemoradiotherapy has shown limited effectiveness in prolonging OS and DFS for patients with locally advanced ESCC. Notably, neoadjuvant therapy offers improved outcomes, although these benefits carry associated risks. A randomized clinical trial25 revealed a 9.6% incidence of postoperative anastomotic leakage in the NCRT group and an 11.1% incidence in the NCT group among patients with locally advanced ESCC. Our retrospective PSM study corroborated these findings, showing a higher incidence of postoperative anastomotic leakage in the neoadjuvant therapy group (NCRT, 17.5%; NCT, 10%) compared to the surgery plus chemoradiotherapy (S+CRT) group (5%). Interestingly, the incidence of leakage in the neoadjuvant treatment group was slightly lower than that of the surgery-alone group in two large phase III clinical studies3,4 of CROSS and NEOCRTEC5010 (22.3% vs 29.8% and 8.6% vs 12.3%, respectively). Furthermore, a report26 by the Society of Thoracic Surgeons, incorporating data from 7595 esophagectomies, concluded that 10.4% of patients in the surgery group and 11.2% in the neoadjuvant radiation group experienced anastomotic leak. There was no statistically significant difference between the groups, although the database lacked detailed information on the specific chemotherapy type and radiation dose. These results are inconsistent, and our experience suggests that the risk of leakage increases when the anastomosis is located at the irradiation site, with a higher dose potentially correlating with increased risk.27,28 Commonly, surgeons opine that neoadjuvant therapy might compromise the postoperative overall health of ESCC patients, potentially leading a higher incidence of anastomotic fistulas.
In our retrospective study’s subgroup analysis, we noted significant differences in TRG rates of the primary lesion (P < 0.001) and pCR rates (P < 0.001) between the NCRT and NCT groups. The 5-year OS rate in the NCRT group indicated a potential survival advantage over the NCT group, although this was not statistically significant post-matching. These results are consistent with the findings of the multicenter phase III POET29 and NeoRes30 trials. However, the applicability of these trials’ results was somewhat restricted, as they mainly included patients with adenocarcinomas. A randomized clinical trial, CMISG1701, which compared these two preoperative therapies utilizing MIE for locally advanced resectable ESCC, concluded that the nCRT group exhibited a higher pCR rate (35.7% vs 3.8%; P < 0.001) than the nCT group.10 However, due to the brief follow-up period, it remains unclear whether a superior pCR could yield an OS benefit for ESCC patients. Our study provides further insights on this matter. Distinctively, while the CMISG1701 study only evaluated ESCC patients at the cT3-4aN0-1M0 stage, we extended our criteria to include patients at stage N2-3 ESCC, accommodating clinical demands.
Our study has certain limitations. The primary limitation was its retrospective nature; despite our efforts to enhance comparability between groups via PSM, inherent limitations of this study design remain. Secondly, the surgical methods and types were not evenly distributed across the groups. The NCRT group had a higher proportion of patients undergoing MIE and McKeown procedure, largely due to the increased patient intake post-MIE. Nonetheless, current studies31–34 affirms that MIE yields comparable long-term survival outcomes to OE for treating localized ESCC. Additionally, our Cox proportional hazards model identified that the surgical approach and type did not independently affect OS and DFS pre-matching. Moreover, there was inconsistency in the chemotherapy regimens across the three groups, and differences in adjuvant therapy were noted between the NCRT and NCT groups. To validate our findings, a multicenter, prospective randomized controlled trial is necessary. Given the rapid advancements in immunotherapy, the management strategies for locally resectable advanced ESCC now demand personalized selection and multidisciplinary collaboration.
Conclusion
In conclusion, preoperative neoadjuvant therapy tends to improve the prognosis of resectable ESCC more effectively than postoperative adjuvant therapy, but it requires careful monitoring for potential complications. Personalizing neoadjuvant treatment strategies to each patient’s individual needs, considering their personal preferences and the expertise of a multidisciplinary team, is a more appropriate approach.
Data Sharing Statement
The supporting data for this study can be procured from the corresponding author, provided a reasonable request is made.
Ethical Approval and Consent to Participate
This study has been approved by the Ethics Committee of Cancer Hospital Affiliated to Shandong First Medical University (number: SDTHEC2023004019). As the research was retrospective, there was no requirement for patient consent. We declare that patients’ information will be kept confidential and that we adhere to the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Chen R, Zheng R, Zhang S, et al. Patterns and trends in esophageal cancer incidence and mortality in China: an analysis based on cancer registry data. J Natl Cancer Center. 2023;3(1):21–27. doi:10.1016/j.jncc.2023.01.002
3. van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074–2084. doi:10.1056/NEJMoa1112088
4. Yang H, Liu H, Chen Y, et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): a phase III multicenter, randomized, open-Label clinical trial. J Clin Oncol. 2018;36(27):2796–2803. doi:10.1200/JCO.2018.79.1483
5. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11–20. doi:10.1056/NEJMoa055531
6. Allum WH, Stenning SP, Bancewicz J, et al. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol. 2009;27(30):5062–5067. doi:10.1200/JCO.2009.22.2083
7. Ajani JA, D’Amico TA, Bentrem DJ, et al. Esophageal and esophagogastric junction cancers, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(7):855–883. doi:10.6004/jnccn.2019.0033
8. Chinese Medical Doctor Association Radiation oncologist Branch, Radiation Oncology Therapeutics Society of Chinese Medical Association, Tumor Radiation Therapy Committee of Chinese Anti-Cancer Association. Chinese guidelines for radiotherapy of esophageal cancer. J Int Oncol. 2022;49(11):641–657. doi:10.3760/cma.j.cn371439-20211021-00002
9. Nakamura K, Kato K, Igaki H, et al. Three-arm phase III trial comparing cisplatin plus 5-FU (CF) versus docetaxel, cisplatin plus 5-FU (DCF) versus radiotherapy with CF (CF-RT) as preoperative therapy for locally advanced esophageal cancer (JCOG1109, NExT study). Jpn J Clin Oncol. 2013;43(7):752–755. doi:10.1093/jjco/hyt061
10. Tang H, Wang H, Fang Y, et al. Neoadjuvant chemoradiotherapy versus neoadjuvant chemotherapy followed by minimally invasive esophagectomy for locally advanced esophageal squamous cell carcinoma: a prospective multicenter randomized clinical trial. Ann Oncol. 2023;34(2):163–172. doi:10.1016/j.annonc.2022.10.508
11. Hsu PK, Chen HS, Liu CC, et al. Pre-versus postoperative chemoradiotherapy for locally advanced esophageal squamous cell carcinoma. J Thorac Cardiovasc Surg. 2017;154(2):732–740.e2. doi:10.1016/j.jtcvs.2017.03.038
12. Ando N, Kato H, Igaki H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann Surg Oncol. 2012;19(1):68–74. doi:10.1245/s10434-011-2049-9
13. Chinese Society of Digestive Endoscopy, Endoscopic Submucosal Dissection Collaborative Group, Chinese Medical Doctor Association of Endoscopists, Beijing Medical Association of Digestive Endoscopy. Expert consensus on endoscopic prevention and treatment of benign and malignant strictures of the esophagus (2020, Beijing). Chin J Digest Endoscopy. 2021;38(3):173–185.
14. Wang LH, Huang J, Han YT. The Chinese Society of Clinical Oncology (CSCO): Clinical Guidelines for the Diagnosis and Treatment of Esophageal Cancer. China: People’s Health Press; 2022.
15. Hong JC, Murphy JD, Wang SJ, et al. Chemoradiotherapy before and after surgery for locally advanced esophageal cancer: a SEER-Medicare analysis. Ann Surg Oncol. 2013;20(12):3999–4007. doi:10.1245/s10434-013-3072-9
16. Lv J, Cao XF, Zhu B, et al. Long-term efficacy of perioperative chemoradiotherapy on esophageal squamous cell carcinoma. World J Gastroenterol. 2010;16(13):1649–1654. doi:10.3748/wjg.v16.i13.1649
17. Yang J, Zhang W, Xiao Z, et al. The impact of postoperative conformal radiotherapy after radical surgery on survival and recurrence in pathologic T3N0M0 esophageal carcinoma: a propensity score-matched analysis. J Thorac Oncol. 2017;12(7):1143–1151. doi:10.1016/j.jtho.2017.03.024
18. Yu J, Ouyang W, Li Y, et al. Value of radiotherapy in addition to esophagectomy for stage II and III thoracic esophageal squamous cell carcinoma: analysis of surveillance, epidemiology, and end results database. Cancer Med. 2019;8(1):21–27. doi:10.1002/cam4.1731
19. Li L, Zhao L, Lin B, et al. Adjuvant therapeutic modalities following three-field lymph node dissection for stage II/III esophageal squamous cell carcinoma. J Cancer. 2017;8(11):2051–2059. doi:10.7150/jca.18981
20. Liu T, Liu W, Zhang H, et al. The role of postoperative radiotherapy for radically resected esophageal squamous cell carcinoma: a systemic review and meta-analysis. J Thorac Dis. 2018;10(7):4403–4412. doi:10.21037/jtd.2018.06.65
21. Zeng Y, Yu W, Liu Q, et al. Difference in failure patterns of pT3-4N0-3M0 esophageal cancer treated by surgery vs surgery plus radiotherapy. World J Gastrointest Oncol. 2019;11(12):1172–1181. doi:10.4251/wjgo.v11.i12.1172
22. Song T, Chen P, Fang M, et al. The role of adjuvant chemoradiotherapy over radiotherapy after R0 resection for stage II–III esophageal squamous cell carcinoma. Cancer Manag Res. 2020;12:1631–1639. doi:10.2147/CMAR.S232930
23. Zou B, Tu Y, Liao D, et al. Radical esophagectomy for stage II and III thoracic esophageal squamous cell carcinoma followed by adjuvant radiotherapy with or without chemotherapy: which is more beneficial? Thorac Cancer. 2020;11(3):631–639. doi:10.1111/1759-7714.13307
24. Li J, Qiu R, Hu Y, et al. Postoperative adjuvant therapy for patients with pN+ esophageal squamous cell Carcinoma. Biomed Res Int. 2021;2021:8571438. doi:10.1155/2021/8571438
25. Wang H, Tang H, Fang Y, et al. Morbidity and mortality of patients who underwent minimally invasive esophagectomy after neoadjuvant chemoradiotherapy vs neoadjuvant chemotherapy for locally advanced esophageal squamous cell carcinoma: a randomized clinical trial. JAMA Surg. 2021;156(5):444–451. doi:10.1001/jamasurg.2021.0133
26. Kassis ES, Kosinski AS, Ross P, et al. Predictors of anastomotic leak after esophagectomy: an analysis of the society of thoracic surgeons general thoracic database. Ann Thorac Surg. 2013;96(6):1919–1926. doi:10.1016/j.athoracsur.2013.07.119
27. Juloori A, Tucker SL, Komaki R, et al. Influence of preoperative radiation field on postoperative leak rates in esophageal cancer patients after trimodality therapy. J Thorac Oncol. 2014;9(4):534–540. doi:10.1097/JTO.0000000000000100
28. Vande Walle C, Ceelen WP, Boterberg T, et al. Anastomotic complications after Ivor Lewis esophagectomy in patients treated with neoadjuvant chemoradiation are related to radiation dose to the gastric fundus. Int J Radiat Oncol Biol Phys. 2012;82(3):e513–e519. doi:10.1016/j.ijrobp.2011.05.071
29. Stahl M, Walz MK, Riera-Knorrenschild J, et al. Preoperative chemotherapy versus chemoradiotherapy in locally advanced adenocarcinomas of the oesophagogastric junction (POET): long-term results of a controlled randomised trial. Eur J Cancer. 2017;81:183–190. doi:10.1016/j.ejca.2017.04.027
30. von Döbeln GA, Klevebro F, Jacobsen AB, et al. Neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy for cancer of the esophagus or gastroesophageal junction: long-term results of a randomized clinical trial. Dis Esophagus. 2019;32(2). doi:10.1093/dote/doy07
31. Gottlieb-Vedi E, Kauppila JH, Malietzis G, et al. Long-term survival in esophageal cancer after minimally invasive compared to open esophagectomy: a systematic review and meta-analysis. Ann Surg. 2019;270(6):1005–1017. doi:10.1097/SLA.0000000000003252
32. Gottlieb-Vedi E, Kauppila JH, Mattsson F, et al. Long-term survival in esophageal cancer after minimally invasive esophagectomy compared to open esophagectomy. Ann Surg. 2022;276(6):e744–e748. doi:10.1097/SLA.0000000000004645
33. Nuytens F, Dabakuyo-Yonli TS, Meunier B, et al. Five-year survival outcomes of hybrid minimally invasive esophagectomy in esophageal cancer: results of the MIRO randomized clinical trial. JAMA Surg. 2021;156(4):323–332. doi:10.1001/jamasurg.2020.7081
34. Liu F, Yang W, Yang W, et al. Minimally invasive or open esophagectomy for treatment of resectable esophageal squamous cell carcinoma? Answer from a real-world multicenter study. Ann Surg. 2023;277(4):e777–e784. doi:10.1097/SLA.0000000000005296
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.