Back to Journals » Journal of Asthma and Allergy » Volume 19
Pandemic-Associated Sensitization Patterns and Burden in Chinese Children with Allergic Rhinitis: A Retrospective Phase-Stratified Study
Authors Huang L ![]() , Zhao X
, Zhao X ![]() , Zhou J
, Zhou J ![]() , Ji Z
, Ji Z ![]()
Received 20 March 2026
Accepted for publication 18 June 2026
Published 29 June 2026 Volume 2026:19 610767
DOI https://doi.org/10.2147/JAA.S610767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Longli Huang, Xinfeng Zhao, Jun Zhou, Zexuan Ji
Department of Clinical Laboratory, Hangzhou Children’s Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Zexuan Ji, Department of Clinical Laboratory, Hangzhou Children’s Hospital, 201 Wenhui Road, Hangzhou, Zhejiang, People’s Republic of China, Tel +86 13857156109, Fax +86 571 85463999, Email [email protected]
Background: The coronavirus disease 2019 (COVID-19) pandemic and associated non-pharmaceutical interventions may have altered children’s indoor, outdoor, and dietary exposures. However, phase-specific data on allergen sensitization patterns in pediatric allergic rhinitis (AR) remain limited.
Objective: To assess phase-specific changes in serum allergen-specific immunoglobulin E (sIgE) sensitization patterns, intensity, co-sensitization, and burden in children with AR in Eastern China.
Methods: We analyzed 12,702 children aged 0– 18 years with clinically diagnosed AR who underwent sIgE testing for 19 inhalant and food allergens in Eastern China from 2018 to 2024. Sensitization was compared across pre-pandemic (2018– 2019), lockdown (2020– 2022), and post-lockdown (2023– 2024) phases using Pearson’s χ2-test or Fisher’s exact test and multivariable logistic regression adjusted for age group, sex, and season. Strong sensitization was defined as sIgE ≥ 3.51 IU/mL, and co-sensitization as concurrent sensitization to both allergens in a pair.
Results: Compared with the pre-pandemic phase, the lockdown and post-lockdown phases showed divergent sensitization trajectories, with higher sensitization to several inhalant allergens and lower sensitization to selected food allergens, although selected seafood allergens increased in later phases. Post-lockdown, adjusted analyses showed higher odds for selected indoor, outdoor, and seafood allergens, while other allergens remained stable or showed non-monotonic patterns. Strong-positive responses, selected co-sensitization patterns, and ≥ 4 sensitizations were also more common post-lockdown.
Conclusion: Across the pre-pandemic, lockdown, and post-lockdown periods, children with AR showed divergent trajectories of inhalant and food allergen sensitization, as well as greater post-lockdown sensitization intensity and complexity. These findings reflect phase-specific associations rather than direct causal effects of the pandemic. They may help inform post-pandemic risk stratification in pediatric AR, with greater attention to inhalant allergen control and more cautious interpretation of food sIgE positivity in clinical context.
Keywords: allergic rhinitis, children, allergen sensitization, specific IgE, co-sensitization, COVID-19 pandemic
Introduction
Allergic rhinitis (AR) is a highly prevalent immunoglobulin E (IgE)-driven inflammatory disorder of the nasal mucosa and a major cause of chronic nasal symptoms in children.1,2 AR affects more than 400 million individuals worldwide and poses a major pediatric health burden because persistent nasal symptoms can impair sleep, school performance, and quality of life.1,2
In pediatric AR, sensitization to inhalant allergens, including house dust mites (HDM), animal dander, cockroach, mold, tree pollen, and mixed grass pollen, is central to disease expression.3,4 Accordingly, defining region-specific sensitization profiles facilitates diagnostic panel selection, avoidance counseling, and consideration of allergen immunotherapy.3,4 Co-sensitization is also clinically relevant because polysensitization and cross-reactivity may complicate diagnostic interpretation, influence the selection of relevant allergens for testing, and affect immunotherapy decisions.5,6 Food allergen-specific IgE is also frequently detected among children diagnosed with AR.7,8 However, interpreting serum allergen-specific immunoglobulin E (sIgE) positivity requires careful clinical correlation; a positive skin or blood test indicates sensitization and does not by itself indicate clinically relevant food allergy, clinical allergy severity, symptom burden, or a causal role in nasal symptoms.9,10 Cross-reactivity, particularly pollen-food allergy syndrome, may also contribute to food-specific IgE positivity in patients with rhinitis.11
China’s COVID-19 pandemic control period and subsequent reopening were accompanied by substantial changes in children’s daily environments, including time spent indoors, ventilation and household hygiene practices, outdoor activity, masking practices, and dietary routines.12–15 Such shifts may have modified the balance between indoor, outdoor, and food-related allergen exposures and, in turn, influenced allergen sensitization profiles, including both single-allergen sensitization and co-sensitization patterns.16–19 During the pandemic control period in particular, prolonged indoor living may have increased contact with HDM, pet dander, and household pests,15–17 whereas masking and reduced outdoor activity may have altered pollen exposure,15,20 and changes in home-based diet and food preparation may have reshaped diet-related allergen exposures.21 However, pandemic-related changes may also have affected healthcare access, referral patterns, healthcare-seeking behavior, and testing practices, which could influence observed phase-specific differences in a retrospective clinical cohort.22,23
Eastern China provides a relevant setting for studying pediatric sensitization profiles because allergen patterns are strongly influenced by local climate, urbanization, seasonal pollen exposure, indoor environmental conditions, and regional dietary habits.19,24
To date, phase-stratified comparisons of sIgE-defined allergen sensitization in Chinese children with AR remain scarce, and existing studies have mainly examined sensitization prevalence or a limited number of allergens, rather than simultaneously characterizing sensitization intensity, burden, and co-sensitization complexity.16–18,25 Given these exposure- and healthcare-related changes and the limited phase-specific evidence, we hypothesized that the lockdown and post-lockdown phases were associated with phase-related shifts in allergen sensitization profiles compared with the pre-pandemic baseline. To examine this, we conducted a 7-year retrospective analysis using Laboratory Information System (LIS) records from 12,702 children with AR at a tertiary pediatric hospital in Eastern China, comprehensively evaluating temporal changes in sensitization rates, sIgE intensity, co-sensitization complexity, and sensitization burden across the pre-pandemic (2018–2019), lockdown (2020–2022), and post-lockdown (2023–2024) periods.
Patients and Methods
Study Design and Participants
This retrospective study included children aged 0–18 years who were diagnosed with AR and underwent sIgE testing at the study hospital from January 1, 2018 to December 31, 2024. AR diagnosis was based on compatible nasal symptoms, clinical history, physical examination, allergen sensitization evidence (positive skin prick test or serum sIgE), and clinician assessment, consistent with Chinese pediatric AR diagnostic criteria.26 The diagnostic criteria and clinical workflow for AR diagnosis were applied consistently during 2018–2024. To avoid repeated measurements, only each patient’s index sIgE test at initial diagnosis during the study period was retained. We excluded records with missing key variables (age, sex, date of test, or sIgE values), concomitant acute respiratory tract infections at the index visit, and documented antiallergic medication use prior to the index assessment. The final sample consisted of 12,702 children.
The pandemic phases were defined a priori as pre-pandemic (2018–2019), lockdown (2020–2022), and post-lockdown (2023–2024) phases. The 2020–2022 period was grouped as the lockdown phase because China implemented prolonged nationwide COVID-19 control measures during these years, with substantial relaxation occurring only near the end of 2022. Because only a small number of children underwent index testing in December 2022, this month was retained within the 2020–2022 phase. This grouping was intended to capture broad temporal contrasts rather than fine-grained month-by-month policy changes. The study was conducted in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics Committee of our institution (Approval No. IRB-2025-022 (IIT)). The requirement for informed consent was waived because of the retrospective study design.
Allergen Testing and Data Collection
At the index evaluation, venous blood (2 mL) was collected, and sIgE was measured using an immunoblotting platform (DX-Blot 45 II system, Dexin Biological). All included children underwent the same fixed 19-allergen sIgE panel at the index test. The LIS provided continuous sIgE values (IU/mL) for each allergen during the index test. Sensitization positivity was defined as sIgE ≥0.35 IU/mL. Sensitization intensity was categorized based on sIgE values following manufacturer instructions and established guidelines: Grade 0 (<0.35 IU/mL, negative); Grades 1–2 (0.35–3.50 IU/mL, weakly positive); and Grades 3–6 (≥3.51 IU/mL, strongly positive).24
Statistical Analysis
All analyses were performed using R statistical software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria). Age was summarized as median (IQR) and compared across phases using the Kruskal–Wallis test, whereas categorical variables were compared using Pearson’s χ2-test. Across phases, sensitization positivity (sIgE ≥0.35 IU/mL), the proportion of strong positivity among children sensitized to the corresponding allergen, the prevalence of selected co-sensitization pairs (defined as concurrent positivity to both allergens in a given pair), and the distribution of the number of sensitized allergens were compared using Pearson’s χ2-test or Fisher’s exact test when any expected cell count was <5, as appropriate. For analyses with a significant overall test, pairwise phase comparisons were further performed using Bonferroni adjustment to account for multiple testing.
Univariable logistic regression was used to estimate odds ratios (ORs) for phase contrasts; these estimates are presented in Supplementary eTable 4, and the same univariable models were repeated within subgroups defined by sex, age group, and season (sex-stratified estimates in Supplementary eTable 1, age-stratified estimates in Supplementary eTables 2a–2c, and season-stratified estimates in Supplementary eTables 3a–3d). For each allergen, separate pairwise multivariable logistic regression models were used to estimate adjusted odds ratios (AORs) for the predefined phase contrasts, controlling for age group, sex, and season of the index test date (spring: March–May; summer: June–August; autumn: September–November; winter: December–February). Because mango and pineapple had sparse phase-specific sensitization counts, Firth-penalized logistic regression was used for these two allergens in both univariable and multivariable phase-contrast analyses to reduce sparse-data bias and improve estimate stability. Conventional logistic regression was used for all other allergens. P values from these logistic regression models were unadjusted two-sided model-based P values. Within each phase, pairwise associations between selected allergen pairs were assessed descriptively using unadjusted 2×2 contingency tables. Odds ratios with 95% confidence intervals (CIs) were estimated using Fisher’s exact test; when any cell count was zero, a continuity correction of 0.5 was applied to all four cells before estimation. These within-phase co-sensitization ORs were interpreted as descriptive measures of association rather than causal or mechanistic effect estimates. No formal a priori sample size calculation was performed because of the retrospective design; all eligible records meeting the prespecified inclusion and exclusion criteria during the study period were included. All tests were two-sided, and P <0.05 was considered statistically significant.
Results
Patient Characteristics
In total, 12,702 children with AR were included in the study (pre-pandemic: n = 2233; lockdown: n = 5770; post-lockdown: n = 4699) (Table 1). The male proportion was similar across phases (62.0–63.5%; P = 0.099). The median age increased from 5 years (IQR, 3–7) pre-pandemic to 6 years (IQR, 4–9) post-lockdown (P <0.001), with a corresponding shift toward older age groups (7–18 years: 27.5% to 44.4%; 0–3 years: 25.8% to 17.5%; P <0.001). Seasonal distribution also differed across phases (P <0.001), with relatively more presentations in spring and fewer in autumn.
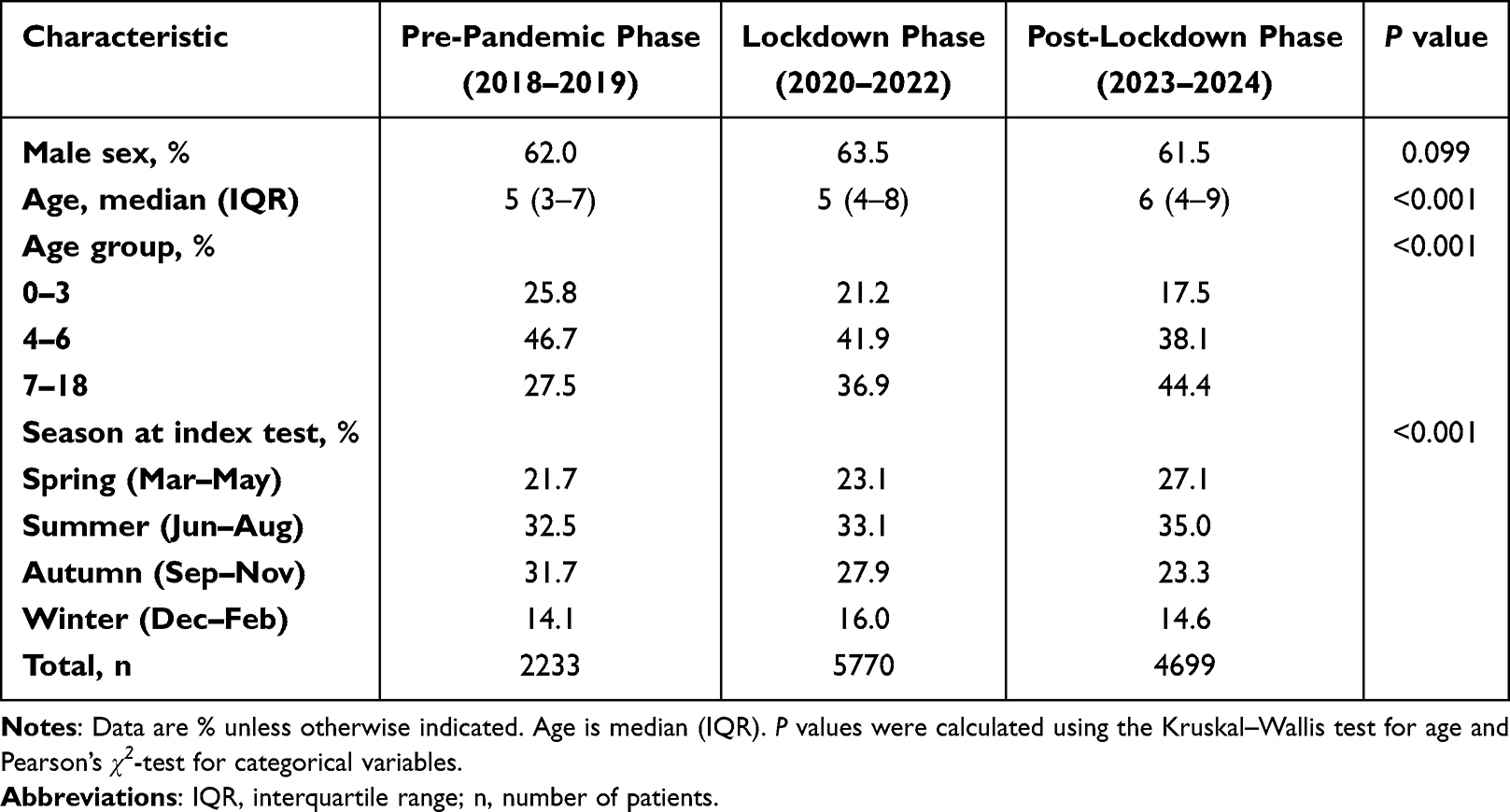 |
Table 1 Baseline Characteristics Across Pandemic Phases |
Phase-Stratified Sensitization Rates
HDM was the most common inhalant sensitizer across the phases (P = 0.071). Sensitization to pet dander increased markedly from the pre-pandemic to post-lockdown phase (cat hair: 3.6% to 9.9%; dog hair: 0.8% to 11.0%; both P <0.001), and pollen sensitization also increased (mixed grass: 3.5% to 7.0%; tree pollen: 0.6% to 3.2%; both P <0.001). In contrast, egg and milk sensitization decreased relative to the pre-pandemic levels (egg: 17.4% to 4.7%; milk: 36.0% to 22.5%; both P <0.001). Several allergens showed non-monotonic patterns in crude sensitization rates, including house dust, mold, and beef (all P <0.001), whereas pineapple showed no phase-related difference (P =0.948) (Table 2).
 |
Table 2 Allergen Sensitization Rates Across Pandemic Phases |
Regression Analyses Across Pandemic Phases
After adjustment for age group, sex, and season, the adjusted odds of sensitization to both cat hair and dog hair were higher in 2020–2022 and 2023–2024 than in 2018–2019, and were also higher in 2023–2024 than in 2020–2022 (all P <0.001; Table 3). Cockroach sensitization was significantly higher in 2023–2024 than in both earlier phases, whereas the 2020–2022 versus 2018–2019 contrast was borderline but not statistically significant (AOR 2.01, 95% CI 0.98–4.12; P = 0.057). HDM sensitization was relatively stable compared with the pre-pandemic phase, although it was modestly lower in 2023–2024 than in 2020–2022 (AOR 0.89, 95% CI 0.82–0.97; P = 0.006). Although crude house dust sensitization rates showed a non-monotonic pattern (Table 2), the adjusted pairwise comparisons were not statistically significant (AORs 0.28, 0.45, and 1.50; all P >0.05).
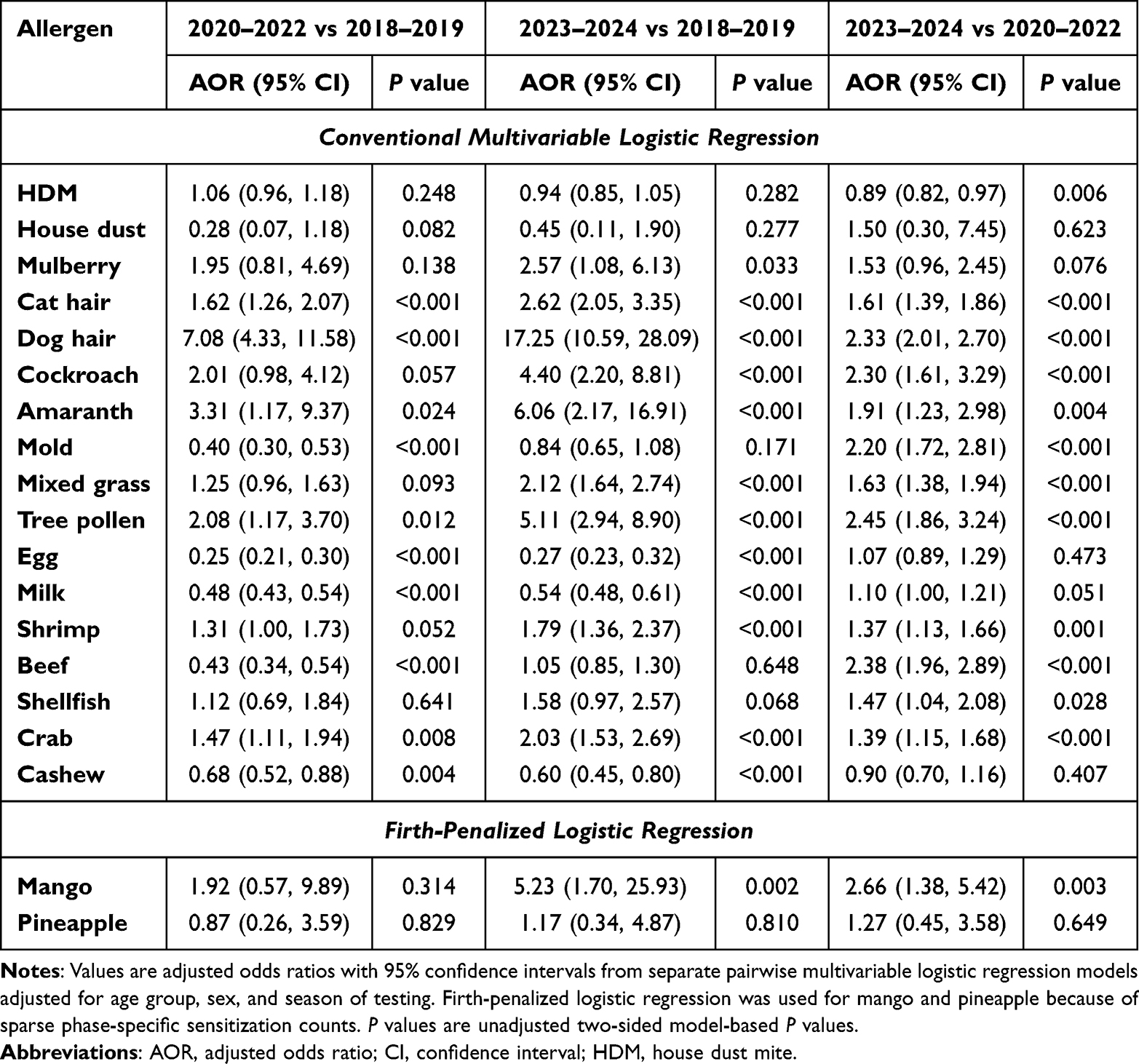 |
Table 3 Adjusted Logistic Regression Analyses of Allergen Sensitization Across Pandemic Phases |
Among pollens, amaranth and tree pollen showed higher adjusted odds in both later phases than in 2018–2019 and in 2023–2024 than in 2020–2022; mulberry was higher in 2023–2024 than in 2018–2019 only; mixed grass was significantly higher only in comparisons involving 2023–2024 (Table 3). For food allergens, egg, milk, and cashew sensitization remained lower in both later phases than in 2018–2019. Shrimp sensitization was significantly higher in 2023–2024 than in both earlier phases, whereas the 2020–2022 versus 2018–2019 contrast was not significant (AOR 1.31, 95% CI 1.00–1.73; P = 0.052). Crab sensitization was higher in all phase contrasts, whereas shellfish was higher only in 2023–2024 than in 2020–2022. Mold and beef showed lower adjusted odds in 2020–2022 than in 2018–2019 and higher adjusted odds in 2023–2024 than in 2020–2022, with no significant difference between 2023–2024 and 2018–2019. In Firth-penalized logistic regression models, mango sensitization was higher in 2023–2024 than in both earlier phases, whereas pineapple showed no clear phase-related difference. Supplementary analyses stratified by sex, age group, and season showed broadly consistent patterns for the main findings (sex-stratified results in Supplementary eTable 1, age-stratified results in Supplementary eTables 2a–2c, and season-stratified results in Supplementary eTables 3a–3d). Univariable estimates are presented in Supplementary eTable 4.
Strong Sensitization Among Sensitized Children
Among children sensitized to the corresponding allergen (sIgE ≥0.35 IU/mL), the proportion with strong sensitization (sIgE ≥3.51 IU/mL; Grades 3–6) differed across phases for selected allergens (Tables 4 and 5). Strong sensitization for HDM increased from 25.9% pre-pandemic to 38.2% during lockdown and 44.1% post-lockdown (P <0.001). Cat hair also showed a post-lockdown increase (6.2% to 6.3% to 13.2%, respectively; P = 0.002).
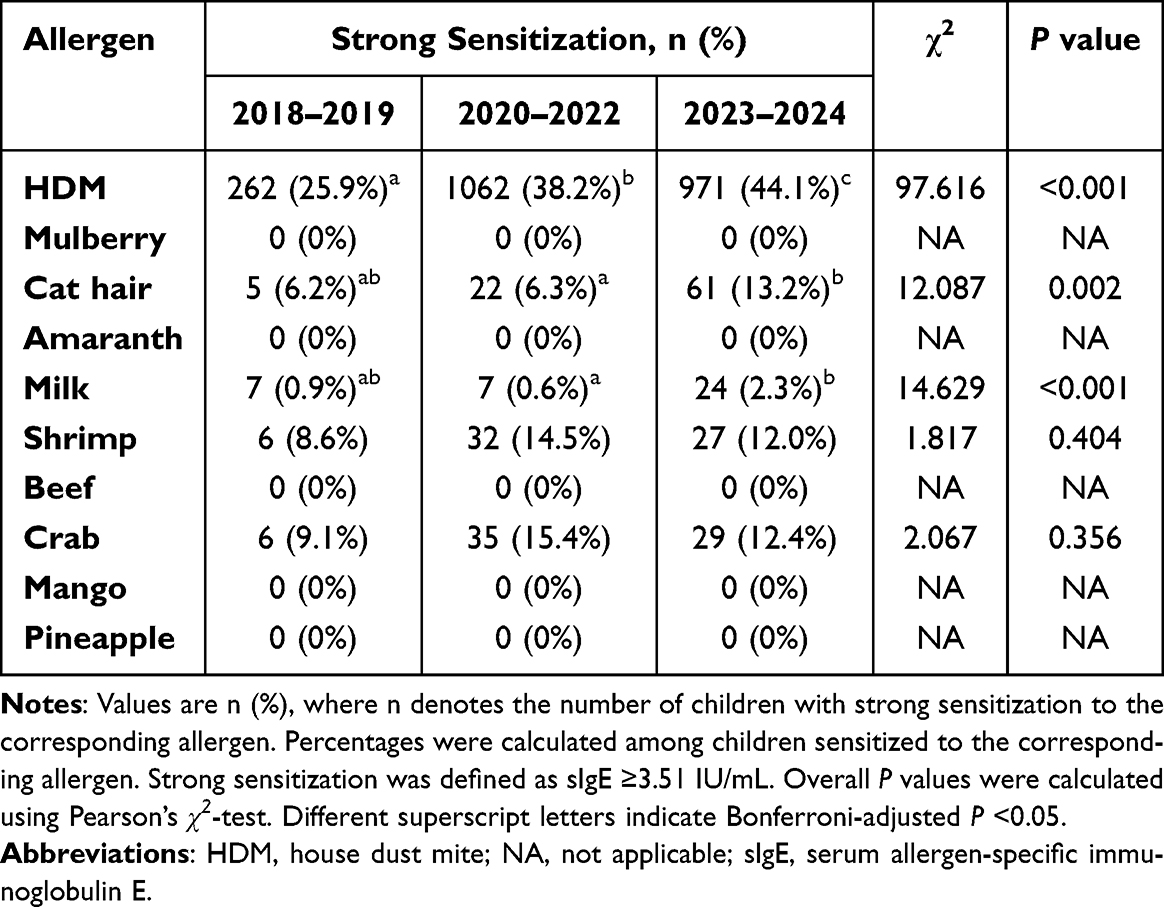 |
Table 4 Strong Sensitization Among Sensitized Children Across Pandemic Phases (Pearson’s χ2-Test) |
 |
Table 5 Strong Sensitization Among Sensitized Children Across Pandemic Phases (Fisher’s Exact Test) |
For food allergens, the proportion of strong sensitization was highest in the post-lockdown phase for milk (0.9%, 0.6%, and 2.3%, respectively; P <0.001) and increased across phases for egg (0.3%, 1.8%, and 3.2%, respectively; Fisher’s exact P = 0.006). For cashew, the overall test was significant (1.1% to 1.3% to 6.7%; Fisher’s exact P = 0.028), although no individual pairwise comparison reached significance after Bonferroni correction. Strong sensitization for shellfish varied across the phases (9.1% to 0% to 16.9%, respectively; Fisher’s exact P <0.001).
Co-Sensitization and Sensitization Burden
The prevalence of several selected co-sensitization pairs changed across phases (Table 6). Among indoor allergen pairs, HDM–cat hair co-sensitization increased from 2.3% in 2018–2019 to 4.5% in 2020–2022 and 7.3% in 2023–2024, while HDM–dog hair increased from 0.5% to 3.5% and 7.2%, respectively (both P <0.001). HDM–cockroach co-sensitization also increased across phases (0.3%, 0.7%, and 1.8%; P <0.001), as did cat hair–dog hair co-sensitization (0.3%, 1.1%, and 2.7%; P <0.001). Among pollen-related pairs, mulberry–tree pollen and mulberry–mixed grass co-sensitization both rose from 0.1% pre-pandemic to 0.6% post-lockdown (P = 0.002 and P = 0.001, respectively). Among food-related and cross-group pairs, shrimp–crab co-sensitization increased from 2.6% to 3.5% and 4.5% (P <0.001), whereas egg–milk co-sensitization decreased markedly from 9.8% to 1.8% and 2.1% (P <0.001). HDM–shrimp co-sensitization increased modestly across phases (2.6%, 3.2%, and 3.8%; P = 0.043), whereas HDM–egg co-sensitization declined from 9.7% pre-pandemic to 2.7% during lockdown and 2.6% post-lockdown (P <0.001). In contrast, shellfish–shrimp co-sensitization did not differ significantly across phases (0.8%, 0.8%, and 1.1%; P = 0.165).
 |
Table 6 Selected Co-Sensitization Pairs Across Pandemic Phases |
Descriptive within-phase pairwise analyses yielded OR point estimates above 1 for all selected allergen pairs (Table 7). The HDM–cockroach association appeared stronger in later phases, with ORs of 2.42 (95% CI 0.51–14.97), 9.17 (95% CI 3.62–29.74), and 24.71 (95% CI 9.28–93.07) across the three periods. Shrimp–crab showed very large descriptive within-phase ORs (ORs 1518.54, 1848.42, and 2206.36), whereas cat hair–dog hair remained positively associated but was less pronounced in later phases (ORs 20.16, 5.24, and 3.70). HDM–shrimp also remained positively associated across phases (ORs 6.79, 6.06, and 4.46). Because some within-phase ORs were very large, particularly for shrimp–crab and selected pollen-related pairs, these estimates should be interpreted as descriptive measures of association rather than stable or precise biological effect-size estimates. The distribution of sensitization burden changed across phases, with the proportion of children showing single sensitization decreasing from 35.2% in 2018–2019 to 30.4% in 2023–2024, and the proportion with ≥4 sensitizations increasing from 6.7% to 9.5% (Table 8).
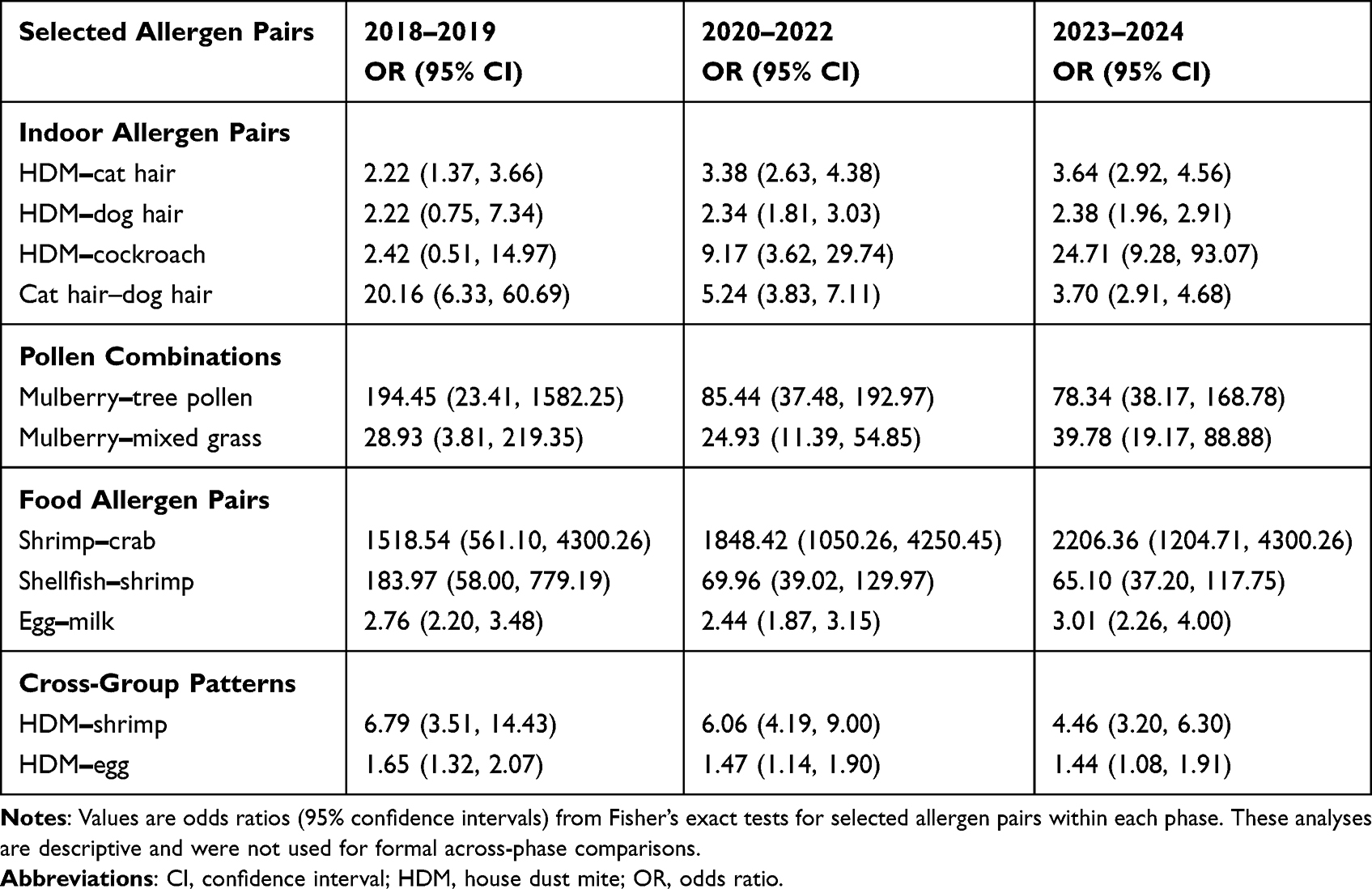 |
Table 7 Descriptive Within-Phase Associations for Selected Allergen Pairs |
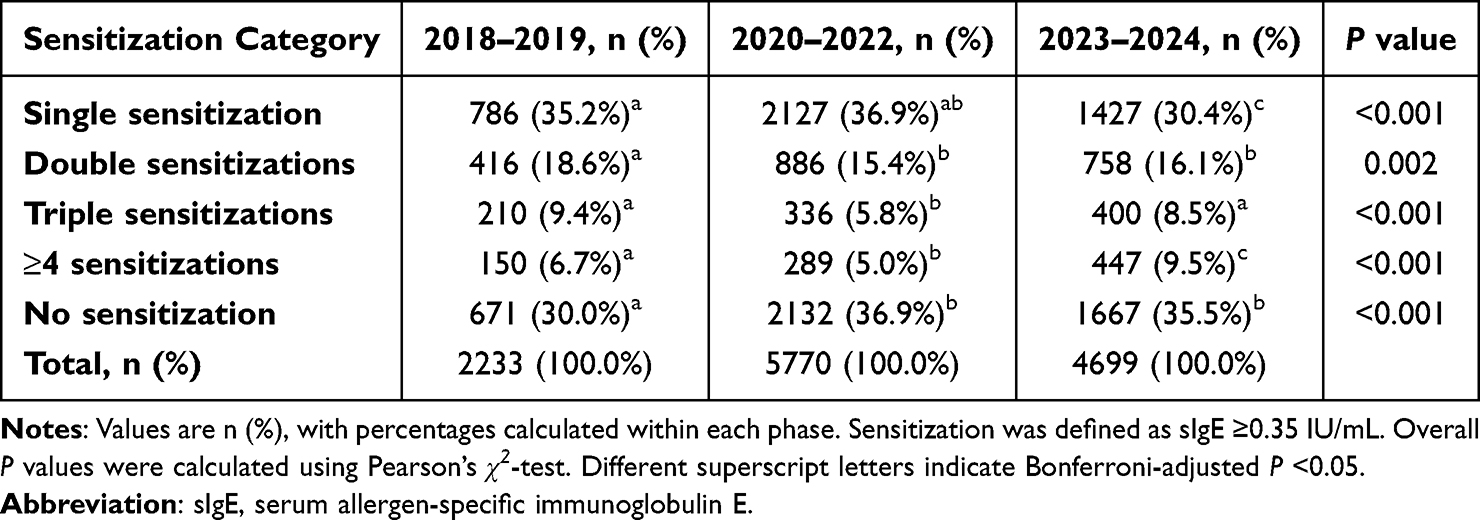 |
Table 8 Distribution of Sensitization Burden Across Pandemic Phases |
Discussion
Our analysis of 12,702 Chinese children with AR showed phase-stratified shifts in sIgE sensitization between 2018 and 2024. Few studies have examined allergen sensitization across the pre-pandemic and lockdown periods, and even fewer have extended these comparisons into the post-lockdown period in Chinese children with AR.16,17 During China’s prolonged control period, children’s exposures may have shifted toward indoor environments,27,28 whereas reopening may have reintroduced a broader mix of indoor and outdoor exposures.29 In our cohort, phase-specific comparisons showed higher sensitization to several inhalant allergens, especially pet dander and selected pollens, whereas selected food sensitizations were lower during and after the lockdown phase. Furthermore, post-lockdown profiles showed greater sensitization intensity and a higher proportion of children with ≥4 sensitizations. Changes in the age distribution and seasonality of testing (Table 1) may also have influenced the observed phase-specific patterns and should be considered when interpreting temporal trends.
Sensitization patterns varied across inhalant allergen categories. HDM sensitization remained relatively stable compared with the pre-pandemic phase but was modestly lower post-lockdown than during lockdown (AOR = 0.89). Previous pediatric studies have reported heterogeneous HDM sensitization patterns across regions and periods, which may reflect regional differences in allergen exposure, climate, and analytic methods.16,30–33 Sensitization to cat hair and dog hair was higher in later phases, which may be consistent with increased indoor contact time or changes in household pet exposure during the pandemic-control period;17,25 however, pet ownership and pet allergen levels were not available in this record-based dataset. Mold sensitization decreased during lockdown (AOR = 0.40) and returned toward pre-pandemic levels thereafter. Such transient fluctuations are consistent with the variability in mold sensitization patterns reported in recent pediatric studies and may reflect unmeasured phase-specific shifts in microenvironmental exposures.27,30 Several pollens, including amaranth, mixed grass pollen, and tree pollen, showed higher odds during lockdown and/or after reopening (Table 3). Pollen can enter homes through ventilation or on clothing even when outdoor activity is reduced, and may accumulate indoors when air exchange is limited;34,35 greater outdoor contact may also have contributed to the persistence of these patterns.36 House dust showed a non-monotonic pattern in crude sensitization rates (Table 2), but the adjusted pairwise comparisons were not statistically significant (Table 3). This discrepancy suggests that the crude pattern should be interpreted cautiously and may partly reflect differences in age distribution, seasonality, healthcare access, or sparse positive counts rather than a stable biologic change. House dust is a heterogeneous indoor matrix, and dust-related allergenic components may vary by season and indoor environmental conditions.37,38
Food and inhalant sensitization showed divergent phase-specific trajectories. Egg, milk, and cashew sensitization decreased during lockdown and remained below pre-pandemic levels post-lockdown, whereas several inhalant allergens, particularly pet dander and selected pollens, showed higher sensitization in later phases (Tables 2 and 3). In contrast, shrimp and crab sensitization increased progressively across phases, a pattern that may be consistent with changes in seafood exposure, home-cooking practices, or cross-reactivity with mite allergens (Table 2).39,40 At the same time, food-related findings were not uniform across analytic dimensions: although overall sensitization to egg, milk, and cashew decreased across phases, strong sensitization to some of these foods increased post-lockdown (Table 5). In addition, shrimp–crab co-sensitization became more common (Table 6), whereas the very large descriptive within-phase shrimp–crab ORs (Table 7) may reflect shared allergenic components and cross-reactivity,40 as well as sparse cell counts, or correlated sensitization patterns, rather than stable effect-size estimates. Therefore, food-related sIgE findings in children with AR should be interpreted in clinical context, together with dietary exposure, reaction history, and potential cross-reactivity.9,10,40
By jointly examining sensitization intensity (strong positivity), co-sensitization patterns, and overall sensitization burden, we observed a post-lockdown profile characterized by greater sensitization intensity and selected features of greater sensitization complexity. Strong-positive sIgE responses (≥3.51 IU/mL; Grades 3–6) to selected indoor allergens, including HDM and cat hair, were more common post-lockdown (Table 4). In parallel, the prevalence of HDM–cat hair, HDM–dog hair, and HDM–cockroach co-sensitization increased (Table 6), and descriptive within-phase HDM–cockroach associations appeared stronger in later phases (Table 7). These descriptive patterns may be consistent with shared indoor exposures during and after the pandemic-control period,16,17,25,41 although exposure data were not directly measured. Cross-reactive arthropod allergens, such as tropomyosin,42,43 may also have contributed to the observed mite–cockroach and shrimp–crab patterns (Tables 6 and 7), although these mechanisms cannot be confirmed in this record-based study. In addition, the higher proportion of children with ≥4 sensitizations post-lockdown (Table 8) suggests greater overall sensitization complexity after reopening. Clinically, these findings may help refine post-pandemic risk stratification and follow-up priorities. Children with strong-positive indoor inhalant allergen sensitization, multiple sensitizations, or recurrent HDM-related co-sensitization patterns may warrant closer follow-up, more focused environmental counseling, and consideration of inhalant immunotherapy evaluation when clinically appropriate.4–6 For highly associated pairs, such as shrimp–crab, mulberry–tree pollen, and HDM–cockroach (Table 7), component-resolved diagnostics may be helpful in selected children when cross-reactivity is suspected.32,44 The rising prevalence of HDM–cat hair, HDM–dog hair, and HDM–cockroach co-sensitization (Table 6) also supports considering evidence-based indoor allergen mitigation, such as bedding encasements and targeted cleaning or filtration, when clinically appropriate.45,46 The very large ORs observed for some pairs, particularly shrimp–crab and selected pollen-related pairs (Table 7), should be interpreted as descriptive measures of within-phase association rather than precise effect-size estimates. Overall, these findings suggest that post-pandemic pediatric AR may involve greater sensitization intensity and complexity, which may help inform testing priorities, counseling, and follow-up in clinical practice.
This retrospective, single-center study has several limitations. First, generalizability is limited because the data were derived from a single pediatric center in Eastern China, where climate and urbanization patterns may differ from those in other regions. Second, because of the record-based design, we could not capture individual-level environmental and behavioral factors (eg, household environment, ventilation, pet ownership, dietary exposure, and symptom severity) or care-related factors (eg, healthcare access, referral pathways, healthcare-seeking behavior, and changes in testing indications or practices over time). These unmeasured factors may have contributed to the observed phase-specific differences independently of true changes in sensitization profiles, thereby limiting inference regarding specific mediating factors. In addition, because AR diagnosis required evidence of allergen sensitization, the cohort represented children with sensitized AR, and selection related to testing indications and care pathways may have varied across phases. Third, we did not perform mechanistic profiling or biomarker-based analyses; therefore, the observed phase-related differences should be interpreted as associative rather than causal. Fourth, the post-lockdown window (2023–2024) was relatively short, and longer follow-up is needed to assess the durability of these patterns. In addition, although 2020–2022 was grouped as the lockdown phase to capture the prolonged COVID-19 control period in China, public health restrictions, healthcare access, and testing behavior may have varied within this period; therefore, the phase-based comparisons should be interpreted as broad temporal contrasts rather than year-specific effects. Finally, some analyses involved sparse outcomes and very large ORs. These estimates may be unstable and may partly reflect cross-reactivity rather than independent co-sensitization.
Conclusions
This study provides a phase-stratified assessment of sIgE-defined sensitization in Chinese children with AR across the pre-pandemic, lockdown, and post-lockdown periods. We observed phase-specific differences in sensitization profiles, including higher sensitization to several inhalant allergens, particularly pet dander and selected pollens, lower sensitization to selected food allergens during and after the lockdown phase, and greater post-lockdown sensitization intensity, co-sensitization, and overall sensitization complexity. These observed differences should be interpreted as associations rather than causal pandemic effects and may partly reflect temporal shifts in environmental and dietary exposures, care-related factors, and the characteristics of the tested population. Although mechanistic inferences cannot be confirmed in this record-based study, these findings may help inform interpretation of contemporary sensitization profiles in children with AR, especially with respect to indoor inhalant allergens, multiple sensitizations, selected co-sensitization patterns, and cautious interpretation of food sIgE positivity in clinical context.
Abbreviations
AR, allergic rhinitis; IgE, immunoglobulin E; sIgE, serum allergen-specific immunoglobulin E; COVID-19, coronavirus disease 2019; LIS, Laboratory Information System; HDM, house dust mite; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio.
Data Sharing Statement
The datasets analyzed during the current study are not publicly available because of patient privacy considerations and institutional regulations. De-identified data may be available from the corresponding author on reasonable request, subject to institutional review board approval where required.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Hangzhou Children’s Hospital (approval no. IRB-2025-022 (IIT)). Because this study used de-identified data extracted from existing electronic medical records, the requirement for informed consent was waived by the Ethics Committee of Hangzhou Children’s Hospital. All data were anonymized, kept confidential, and used solely for research purposes. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the Declaration of Helsinki. Clinical trial registration was not applicable.
Acknowledgments
The authors thank all participants, the research team, the medical laboratory technicians, and the clinicians at Hangzhou Children’s Hospital for their support. No writing or editing assistance was used, and no third-party submission services were involved.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cheng M, Dai Q, Liu Z, Wang Y, Zhou C. New progress in pediatric allergic rhinitis. Front Immunol. 2024;15:1452410. doi:10.3389/fimmu.2024.1452410
2. Yang T, Wang HR, Mou YK, et al. Mutual influence between allergic rhinitis and sleep: factors, mechanisms, and interventions—a narrative review. Nat Sci Sleep. 2024;16:1451–12. doi:10.2147/NSS.S482258
3. Lam K, Au E, Ip W, Tam J, Leung P. Inhalant mediated allergy: immunobiology, clinical manifestations and diagnosis. Clin Rev Allergy Immunol. 2025;68:43. doi:10.1007/s12016-025-09053-2
4. Coppens K. Diagnosis and management of allergic rhinitis in children. Belg J Paediatr. 2024;25(4):272–276.
5. Migueres M, Dávila I, Frati F, et al. Types of sensitization to aeroallergens: definitions, prevalences and impact on the diagnosis and treatment of allergic respiratory disease. Clin Transl Allergy. 2014;4(1):16. doi:10.1186/2045-7022-4-16
6. Izmailovich M, Semenova Y, Abdushukurova G, et al. Molecular aspects of allergen-specific immunotherapy in patients with seasonal allergic rhinitis. Cells. 2023;12(3):383. doi:10.3390/cells12030383
7. Zhao Z, Chen L, Huang C, et al. Allergen sensitization patterns in children with allergic rhinitis: insights from a four-year retrospective study in Shenzhen, China. BMC Pediatr. 2025;25:544. doi:10.1186/s12887-025-05885-1
8. Hu Z, Xue J, Pan M, et al. Prevalence of allergen sensitization among children with allergic rhinitis in Changzhou, China: a retrospective observational study. BMC Pediatr. 2023;23(1):466. doi:10.1186/s12887-023-04291-9
9. Wasserman RL. A diagnostic approach to IgE-mediated food allergy: a practical algorithm. J Food Allergy. 2024;6(1):15–20. doi:10.2500/jfa.2024.6.240007
10. Manea I, Ailenei E, Deleanu D. Overview of food allergy diagnosis. Med Pharm Rep. 2016;89(1):5–10. doi:10.15386/cjmed-513
11. Cudowska B, Pawłowicz M, Lebensztejn D. Pollen-related food allergy in children with seasonal allergic rhinitis. Postepy Dermatol Alergol. 2021;38(2):96–101. doi:10.5114/ada.2021.104284
12. Hou Z, Song S, Du F, et al. The influence of the COVID-19 epidemic on prevention and vaccination behaviors among Chinese children and adolescents: cross-sectional online survey study. JMIR Public Health Surveill. 2021;7(5):e26372. doi:10.2196/26372
13. Xie F, Cai T, Jin B, et al. Investigation and analysis of children’s behavior and outpatient number of respiratory diseases in Shanghai before and after the COVID-19 pandemic. Heliyon. 2023;9(9):e19592. doi:10.1016/j.heliyon.2023.e19592
14. Wan L, Liu Y, Tan S, et al. Prevalence and factors of COVID-19 among children in Hunan, China, following the deregulation of epidemic control: an observational study in epidemiology. BMJ Open. 2025;15(3):e089651. doi:10.1136/bmjopen-2024-089651
15. Schreiner GZ, Nascimento JS, Araujo LML. Effects of social distancing during the COVID-19 pandemic on childhood rhinitis. Arq Asma Alerg Imunol. 2023;7(3):273–283. doi:10.5935/2526-5393.20230040-en
16. Li Y, Hu H, Zhang T, et al. Increase in indoor inhalant allergen sensitivity during the COVID-19 pandemic in South China: a cross-sectional study from 2017 to 2020. J Asthma Allergy. 2021;14:1185–1195. doi:10.2147/JAA.S322034
17. Zhang Y, Fu X, Chen Y, et al. Divergent sensitization kinetics to indoor allergens in children: early dust mite surges vs delayed cat dander peaks during COVID-19 lockdowns. J Asthma Allergy. 2025;18:1539–1549. doi:10.2147/JAA.S556457
18. Li X, Li T, Chen N, Wang X, Yang J, Bi L. Influence of COVID-19 pandemic on inhaled allergens in children with allergic diseases, Henan, China. J Med Virol. 2023;95(1):e28409. doi:10.1002/jmv.28409
19. Wu L, Luo W, Hu H, et al. A multicenter study assessing risk factors and aeroallergens sensitization characteristics in children with self-reported allergic rhinitis in China. J Asthma Allergy. 2021;14:1453–1462. doi:10.2147/JAA.S342495
20. Choi HG, Kim SY, Joo YH, Cho HJ, Kim SW, Jeon YJ. Incidence of asthma, atopic dermatitis, and allergic rhinitis in Korean adults before and during the COVID-19 pandemic using data from the Korea National Health and Nutrition Examination Survey. Int J Environ Res Public Health. 2022;19(21):14274. doi:10.3390/ijerph192114274
21. Brakspear L, Boules D, Nicholls D, Burmester V. The impact of COVID-19-related living restrictions on eating behaviours in children and adolescents: a systematic review. Nutrients. 2022;14(17):3657. doi:10.3390/nu14173657
22. Nakano A, Maeta A, Takaoka Y, et al. Parents’ fears about hospital visits and trait anxiety in the COVID-19 pandemic. Healthcare. 2023;11(8):1080. doi:10.3390/healthcare11081080
23. Krishna MT, Beck SC, Gribbin N, et al. The impact of COVID-19 pandemic on adult and pediatric allergy & immunology services in the UK National Health Service. J Allergy Clin Immunol Pract. 2021;9(2):709–722.e2. doi:10.1016/j.jaip.2020.11.038
24. Chen H, Li J, Cheng L, et al. China consensus document on allergy diagnostics. Allergy Asthma Immunol Res. 2021;13(2):177–205. doi:10.4168/aair.2021.13.2.177
25. Evcen R, Çölkesen F, Yıldız E, et al. Increasing prevalence of sensitization to cat/dog allergens in the COVID-19 pandemic. Int Arch Allergy Immunol. 2024;185(2):133–141. doi:10.1159/000534173
26. Subspecialty Group of Rhinology, Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery, Subspecialty Groups of Rhinology and Pediatrics, Society of Otorhinolaryngology Head and Neck Surgery, Chinese Medical Association. Guideline for diagnosis and treatment of pediatric allergic rhinitis (2022, revision). Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022;57(4):392–404. doi:10.3760/cma.j.cn115330-20220303-00092
27. Cheng Z, Zhan Z, Xue M, et al. Public health measures and the control of COVID-19 in China. Clin Rev Allergy Immunol. 2023;64(1):1–16. doi:10.1007/s12016-021-08900-2
28. Zhang Y, Zhao J, Yu Z, et al. Changes in home environment, lifestyles, and mental health among preschoolers who experienced lockdown during the first wave of COVID-19 in Shanghai. Child Youth Serv Rev. 2024;161:107654. doi:10.1016/j.childyouth.2024.107654
29. Ge J. The COVID-19 pandemic in China: from dynamic zero-COVID to current policy. Herz. 2023;48(3):226–228. doi:10.1007/s00059-023-05183-5
30. Huang X, Yang M, Ye M, Qiu J, Chen Y. Impact of the COVID-19 epidemic on inhalant allergen sensitization in children. J Immunol Res. 2024;2024(1):5641948. doi:10.1155/2024/5641948
31. Shao W, Shao Q. Impact of COVID-19 restrictions on childhood allergic sensitization: a three-phase comparative study. Sci Rep. 2025;15(1):39800. doi:10.1038/s41598-025-23547-1
32. Lis K, Bartuzi Z. Selected technical aspects of molecular allergy diagnostics. Curr Issues Mol Biol. 2023;45(7):5481–5493. doi:10.3390/cimb45070347
33. Zeng Q, Yang C, Li J, Qiu X, Liu W. Aeroallergen sensitization patterns and related factors in children with allergic rhinitis in Guangzhou. Mediators Inflamm. 2025;2025:5887915. doi:10.1155/mi/5887915
34. Wang W, Ooka R, Kikumoto H, Oh W, Han M. Influence of various factors on indoor/outdoor pollen concentration ratio based on experimental research: a review. Build Environ. 2022;219:109154. doi:10.1016/j.buildenv.2022.109154
35. Takahashi Y, Takano K, Suzuki M, et al. Two routes for pollen entering indoors: ventilation and clothes. J Investig Allergol Clin Immunol. 2008;18(5):382–388.
36. Sözener ZÇ, Öztürk BÖ, Aydın Ö, et al. Coincidence of pollen season and coronavirus disease 2019 pandemic: less time outdoors - lesser allergy symptoms in 2020. Asia Pac Allergy. 2021;11(2):e16. doi:10.5415/apallergy.2021.11.e16
37. Araki A, Bamai YA, Ketema R, Kishi R. House dust and its adverse health effects. Nihon Eiseigaku Zasshi. 2018;73(2):130–137. doi:10.1265/jjh.73.130
38. Cochran SJ, Acosta L, Divjan A, et al. Spring is associated with increased total and allergenic fungal concentrations in house dust from a pediatric asthma cohort in New York City. Build Environ. 2022;226:109711. doi:10.1016/j.buildenv.2022.109711
39. Tian X, Zhou Y, Wang H. The impact of COVID-19 on food consumption and dietary quality of rural households in China. Foods. 2022;11(4):510. doi:10.3390/foods11040510
40. Giannetti A, Pession A, Bettini I, Ricci G, Giannì G, Caffarelli C. IgE mediated shellfish allergy in children—a review. Nutrients. 2023;15(14):3112. doi:10.3390/nu15143112
41. Sun BQ, Lai XX, Gjesing B, Spangfort MD, Zhong NS. Prevalence of sensitivity to cockroach allergens and IgE cross-reactivity between cockroach and house dust mite allergens in Chinese patients with allergic rhinitis and asthma. Chin Med J. 2010;123(24):3540–3544. doi:10.3760/cma.j.issn.0366-6999.2010.24.007
42. Yang Y, Zhang Y, He X, et al. An overview of seafood allergens: structure–allergenicity relationship and allergenicity elimination processing techniques. Foods. 2025;14(13):2241. doi:10.3390/foods14132241
43. Reina R, Acevedo N, Caballero MÁ, Gil I, Lopez-Salgueiro R, Caraballo L. IgE sensitization to house dust mite and cockroach allergens in asthmatic and allergic patients in the tropics. Front Allergy. 2025;6:1727880. doi:10.3389/falgy.2025.1727880
44. Turkalj M, Banić I, Fressl Juroš G. Component-resolved and multiplex-specific IgE diagnostics: utility in anaphylaxis and beyond. Children. 2025;12(7):933. doi:10.3390/children12070933
45. Beheshti R, Grant TL, Wood RA. Minimizing indoor allergen exposure: what works? Curr Allergy Asthma Rep. 2024;25(1):3. doi:10.1007/s11882-024-01185-3
46. Li Y, Lin C, Wang Q, et al. Inhalant-specific IgE profiles to guide the clinical management and prevention of children with respiratory allergies in Fuzhou: a cross-sectional cohort study based on ImmunoCAP. J Asthma Allergy. 2025;18:1847–1856. doi:10.2147/JAA.S549970
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exosomes Derived hsa-miR-4669 as a Novel Biomarker for Early Predicting the Response of Subcutaneous Immunotherapy in Pediatric Allergic Rhinitis
Jiang S, Xie S, Fan R, Tang Q, Zhang H, Wang F, Xie S, Gao K, Zhang J, Xie Z, Jiang W
Journal of Inflammation Research 2022, 15:5063-5074
Published Date: 3 September 2022
Epidemiology and Clinical Characteristics of Seasonal Human Coronaviruses in Children Hospitalized in Hebei Province, China Before and During the COVID-19 Pandemic
Zhao MC, Wen C, Sun L, Duan SX, Zang KX, Wang L, Cui XW
Risk Management and Healthcare Policy 2023, 16:1801-1807
Published Date: 8 September 2023
Association of Mite Molecular Sensitization Profiles with Respiratory Allergies and Asthma Control in Children from East China
He J, Lin N, Jin T, Lin M, Huang Z, Li S, Liu J, Su L, Ye X, Wu L, Song Z, Xu H, Chen Z
Journal of Asthma and Allergy 2024, 17:965-975
Published Date: 7 October 2024
Correlations of Nasal Microbiome with Allergic Rhinitis and Its Symptoms Severity in Children Progression
Teng Z, Li Q, Shen XF
Journal of Asthma and Allergy 2024, 17:1187-1196
Published Date: 16 November 2024
Trends and Characteristics of Pertussis Epidemic in Pediatric Patients During and After the COVID-19 Pandemic in East China
Wang L, Gao M, Chen Y, Gu Q, Guan L, Sun L, George AS, Rafay A, Yang Y, Bai G
Infection and Drug Resistance 2025, 18:4351-4361
Published Date: 26 August 2025