Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Paliperidone Palmitate versus Risperidone Long-Acting Injectable in Patients with Schizophrenia: A Meta-Analysis of Efficacy and Safety
Authors Zhao M, Qin B, Mao Y, Zhang Y, Zhao R, Wang A, Wang H, Zhao J, Wang C
Received 6 February 2023
Accepted for publication 30 March 2023
Published 5 April 2023 Volume 2023:19 Pages 749—757
DOI https://doi.org/10.2147/NDT.S407259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Richard J Porter
Mingjun Zhao,1,* Bin Qin,2,* Yage Mao,3 Yang Zhang,4 Ruisheng Zhao,5 Aiqin Wang,1 Hailing Wang,1 Jianting Zhao,6 Changhong Wang7
1Department of Pharmacy, The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang, People’s Republic of China; 2Department of Neurology, Liuzhou General Hospital, Liuzhou, People’s Republic of China; 3Department of Pharmacy, Maternal and Child Health Care hospital of Xinxiang City, Xinxiang, People’s Republic of China; 4Department of Respiratory, The People’s Hospital of Jiaozuo City, Jiaozuo, People’s Republic of China; 5Department of Pharmacy, The First Affiliated Hospital of Xinxiang Medical University, Xinxiang, People’s Republic of China; 6Department of Neurology, Central Hospital of Xinxiang City, Xinxiang, People’s Republic of China; 7Department of Psychiatry, The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Changhong Wang, Department of Psychiatry, The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), 207# QianJin Road, Xinxiang, Henan, 453000, People’s Republic of China, Tel +86-373-3388798, Fax +86-373-3374082, Email [email protected]
Purpose: The aim of this study was to assess the efficacy and safety of paliperidone palmitate (PP) treatment compared with risperidone long-acting injectable (LAI) treatments for patients with schizophrenia.
Patients and Methods: Data mining was conducted in April 2022 across PubMed, Web of Science, Embase, the Cochrane Library, ClinicalTrials.gov, and PsycINFO. All published randomized controlled trials (RCTs) that assessed the effect of PP treatment for patients with schizophrenia when compared with the risperidone-LAIAs group were included. Relevant data were extracted and synthesized narratively. Results were expressed as standardized mean differences (SMDs) or risk ratios (RRs), with 95% confidence intervals (CIs).
Results: Four RCTs with 2451 patients met all the inclusion and exclusion criteria. Efficacy analyses showed no significant statistical differences in Positive and Negative Syndrome Scale (PANSS) total score changes at the endpoint (SMD = 0.10, P = 0.19), or in response rates (RR = 0.93; P = 0.40). Regarding the safety outcomes, PP treatment showed significantly increased risks of discontinuation rates for any reason (35.7% vs 30.4%; RR = 1.19; 95% CI, 1.03 to 1.39; P = 0.02) and nonsignificantly increased risks of total treatment emergent adverse events (TEAEs) (66.6% vs.64.8%; RR = 1.01; 95% CI, 0.94 to 1.09; P = 0.78) compared with the risperidone-LAIAs-treated group. Furthermore, PP may significantly increase total discontinuation rates compared with risperidone-LAIAs.
Conclusion: Our meta-analysis did not find a more beneficial effect of PP compared to risperidone-LAIAs treatments for schizophrenia. Clinicians should interpret and translate our data with caution, as the meta-analysis was based on a limited number of randomized controlled trials and patients.
Keywords: paliperidone palmitate, risperidone, long-acting injectable, schizophrenia, meta-analysis
Introduction
Schizophrenia is a complex and multifactorial mental disorder characterised by wide variability in both causes and effects on individuals. These can include persistent psychiatric symptoms, high risk of unemployment, and around a 20% reduction in life expectancy.1–3 Symptom expression is highly heterogeneous, but it can include common positive symptoms, including delusions, hallucinations, and thought disorders, as well as negative symptoms, such as emotional withdrawal, passivity, difficulty beginning and sustaining activities; and cognitive deficits, such as impaired executive function, information processing, attention, and memory.4–7 Collectively, these symptoms may disrupt social and occupational functioning and negatively impact overall quality of life.8,9
Antipsychotics represent the cornerstone of current pharmacological treatments for schizophrenia.10 Two main classes of antipsychotics, first-generation (typical) and second-generation (atypical), are used to treat schizophrenia. Most atypical antipsychotics are antagonists of dopamine D2 and serotonin 5-HT2A receptors and can alleviate both positive and negative symptoms10,11 with fewer or less severe adverse effects, such as extrapyramidal symptoms (EPS), hyperprolactinemia, and cardiovascular abnormalities compared to typical antipsychotics.12,13 Although a newer study reported that psychotropic medication non-adherence was high, and was influenced by various factors (such as patients’ individual behavior, social or family support, clinical or illness and treatment-related, and overall health care system-related factors) operating at different levels,14 LAI formulations of paliperidone palmitate 3-monthly (PP3M), aripiprazole, olanzapine, and paliperidone palmitate once-monthly (PP1M) showed the highest effect sizes and certainty of evidence for both relapse prevention and acceptability in the maintenance treatment of adults with nonaffective psychoses.15 Thus, LAI antipsychotics (LAIAs) may promote the development in the later stages of schizophrenia, and introducing the patient to a long-acting formulation for ongoing maintenance therapy while treating acute psychotic episodes,16–19 or nonaffective psychoses15 may assist clinicians in establishing optimal treatment strategies.
Paliperidone is a metabolite of risperidone that has been introduced commercially in an oral formulation. Like risperidone, paliperidone blocks both 5HT2A and D2 receptors, α1 and α2 adrenoceptors, and H1 receptors, but not β adrenoceptors, muscarinic cholinoceptors, or peptidergic receptors. Paliperidone palmitate (PP), a second-generation LAIA, has three different formulations: PP1M, PP3M and paliperidone palmitate 6-monthly (PP6M),20 and has been shown to be effective in the treatment of schizophrenia.21 Although the introduction of PP for the treatment of psychotic disorders constitutes a valuable broadening of therapeutic possibilities for patients with a primary diagnosis of schizophrenia, the therapeutic superiority of PP LAIAs over risperidone LAIAs is inconclusive.
To date, there have been several randomized controlled trials (RCTs) on the efficacy and safety of PP vs risperidone LAIA,22–24 but the conclusions from these studies are limited. One previous review investigated the efficacy and safety of PP vs risperidone LAIA and a placebo for schizophrenia.25 The results suggested that PP and risperidone LAI are roughly equivalent in efficacy and safety.
The present study addresses one clinical question not clear answered in the above mentioned studies: Are there differences in efficacy (ie, the Positive and Negative Syndrome Scale (PANSS) scores, response rate, and clinical global impression of severity (CGI-S) scale score), and safety (ie, the discontinuation rate, the incidence of treatment emergent adverse events (TEAEs), and weight gain) between PP and risperidone LAIA for the treatment of schizophrenia?
Given the inconsistencies in the literature mentioned above and two other RCTs23,26 with 473 patients that were not included in the previous review,25 there is an urgent need to compare the effects of PP and risperidone LAIA in patients with schizophrenia. Therefore, we performed the present meta-analysis of controlled trials to evaluate the efficacy and safety of PP and risperidone LAIA in patients with schizophrenia to assist clinicians in making treatment recommendations and establishing optimal treatment strategies.
Materials and Methods
All steps of this review were performed in strict accordance with the Cochrane Handbook for Systematic Reviews of Interventions.27 The Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement guidelines were followed during the meta-analysis and the preparation of this review.28
Search Strategy
Databases including PubMed, Web of Science, Embase, Cochrane Library, ClinicalTrials.gov, and PsycINFO were searched from the date of their inception to December 2022, with no language restrictions. We used the search terms: “paliperidone”, “risperidone”, and “schizophreni*” (Supplementary Table 1). Relevant articles were obtained by scanning the conference summaries and reference lists for all the identified publications and related reviews. The literature search was carried out by two independent authors, and any disagreements were resolved via discussion with another member of the review team to ensure accuracy.
Eligibility Criteria and Study Selection
We included all clinical trials that met the following criteria: (a) all included patients had to be diagnosed with schizophrenia according to standard operationalised diagnostic criteria (DSM-III, DSM-III-R, DSM-IV, DSM-5, and ICD-10); and (b) there were RCTs comparing PP with risperidone LAIA treatment options. We excluded (a) duplicate publications, (b) studies of pooled analysis, (c) post-hoc analyses, (d) non-RCTs, (e) non-relevant interventions, and (f) studies with no relevant results on efficacy or safety. Eligibility screening was performed in two steps, each by two independent reviewers: (a) title and abstract screening for relevance to the study objective and (b) full-text screening for meta-analysis eligibility. Conflicts were resolved by a third reviewer.
Open-label studies were included to evaluate the effect of PP and risperidone LAIA more comprehensively.
Outcome Measures
In this meta-analysis, we assessed both dichotomous and continuous measures of schizophrenia outcomes. Clinical outcomes were recorded based on intent-to-treat analyses, if possible. Our primary outcomes were efficacy as assessed by PANSS total score changes from baseline to the endpoint, and the proportion of patients responding to treatment, total treatment discontinuation ratios, and total TEAEs.
Secondary outcomes were changes from baseline to the endpoint for positive and negative subscale PANSS scores, CGI-S scale score changes, and the ratios of a ≥7% increase in body weight.
Data Extraction
Two reviewers independently assessed the articles according to the inclusion and exclusion criteria, as well as the completeness of the data abstraction. We abstracted key data using a standardised data extraction form to ensure the consistency of the appraisal for every study. The data were summarised by one investigator and checked by a second reviewer. Any disagreements were resolved by consensus with a third reviewer to ensure that accurate data were obtained.
Risk of Bias Assessment
Methodological quality was assessed using the Risk of Bias Assessment Tool from the Cochrane Handbook for Systematic Reviews of Interventions, and the risk of bias table containing seven dimensions of Random sequence generation (selection bias); Allocation concealment (selection bias); Blinding of participants and personnel (performance bias); Blinding of outcome assessment (detection bias); Incomplete outcome data (attrition bias); Selective reporting (reporting bias); Other bias was generated using Review Manager (RevMan) version 5.3 (http://www.cochrane.org). To reduce reporting biases, we also searched and evaluated unpublished literature and accessed online trial registries. Each domain was rated as either “high risk”, “unclear risk”, or “low risk”.27
Data Analysis
The meta-analysis was performed using Review Manager (RevMan) version 5.3 (http://www.cochrane.org) to estimate the effect sizes and pool estimates for the effects across studies, with analysis of inverse variance models for risk ratios (RR) in dichotomous measures and inverse variance models for standardised mean difference (SMD) in continuous measures, as well as 95% confidence intervals (CIs). The random-effects model of DerSimonian and Laird29 was used for the data pooling, as it is more conservative than typical fixed-effects models; thus, it is more appropriate when there is potential heterogeneity across studies. We also assessed heterogeneity using the Q statistic and the I2 statistic, with Q test P value <0.1 or I2 ≥ 50% indicating significant heterogeneity, and I2 values of 25%, 50%, and 75% signifying mild, moderate, and high heterogeneity, respectively.30,31 Sensitivity analysis or subgroup analysis will be conducted to demonstrate the robustness and heterogeneity of the outcomes when the number of the included trials is enough.
Results
Search Results
A total of 1222 records were identified through a database search (PubMed: 41; Cochrane Library: 211; Embase: 827; Web of Science: 91; ClinicalTrials: 28; PsycINFO: 24). After excluding 156 duplicate records, 1034 potentially relevant studies were retrieved. Of these, 992 papers were excluded because their titles or abstracts did not meet the inclusion criteria. A total of 38 papers were excluded after two reviewers independently read the full-text manuscripts. Finally, four studies (two open-label studies23,26 and two double-blind RCTs)22,24 met our inclusion criteria. These studies concerned 2451 patients who were randomly assigned to receive either PP or risperidone LAIA treatment (Figure 1).
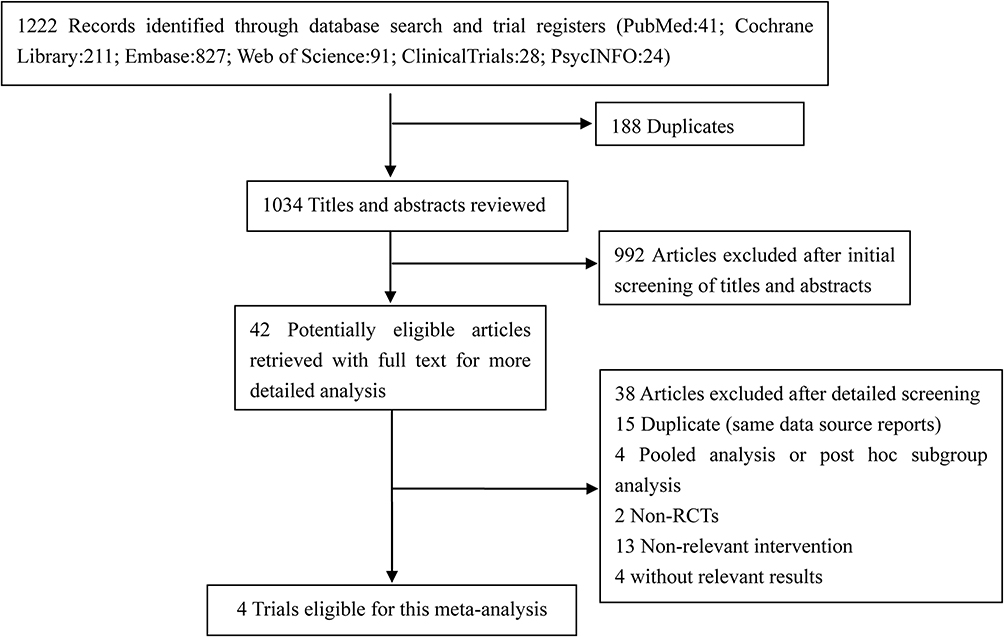 |
Figure 1 Prisma flow chart of the study selection. |
Characteristics of the Included Studies
The patient characteristics and design features for he included trials are summarised in Table 1. The trials were conducted between 2011 and 2016. The PP-LAI formulation of four included trials is PP1M. The sample sizes ranged from 30 to 1220 patients, with a median sample size of 612.75 per trial. The overall male ratio was 54.9% (range, 40.0–59.4%), with no statistically significant difference (P = 0.56) and no heterogeneity (I2 = 48%, P = 0.12). The age range of the participants was 18 to 64 years, with no statistically significant difference (P = 0.68), and no substantial heterogeneity across trials (I2 = 0%, P = 0.79). Mean baseline PANSS total scores ranged from 78.1 to 84.4, with no statistically significant difference (P = 0.82) and mild heterogeneity (I2 = 39%, P = 0.18). This indicated mild-to-moderate levels of schizophrenic symptoms.32 The median study duration was 25.75 weeks (range, 13–53 weeks).
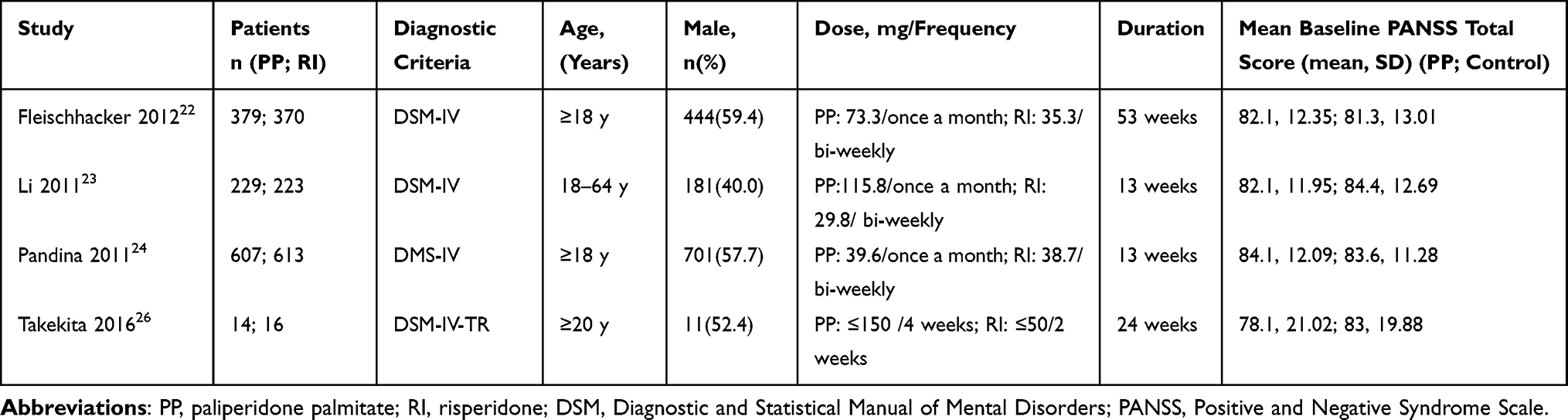 |
Table 1 Characteristics of the Included Studies |
Study Quality
The risk of bias in individual trials and the proportions of trials with low, unclear, and high risk of bias in each of the domains are shown in Figure 2. The overall quality of the studies was rated as moderate, and all four studies described the method of random sequence generation. Allocation concealment was low across all the trials. Three studies reported blinding of the participants, and three studies reported blinding of the assessors. Two trials reported completeness of follow-up as the outcome. Selective reporting was observed in one trial.
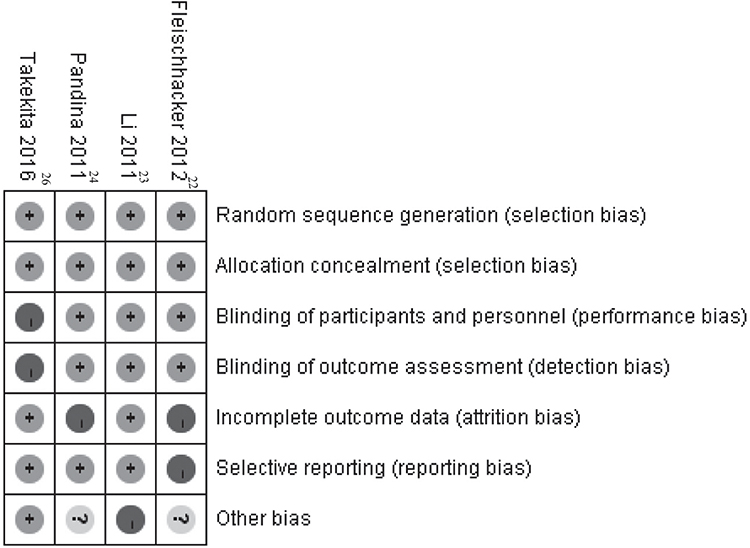 |
Figure 2 Risk of bias of the included studies. |
Primary Outcomes
In the overall pooled population, there were no statistically significant differences in PANSS total score changes at the endpoint between the PP-treated group and the risperidone LAIA-treated group, with an SMD of 0.10 (95% CI, −0.05 to 0.25; P = 0.19) and moderate heterogeneity (I2 = 50%, P = 0.11) (Figure 3A). There was no statistically significant difference between the PP-treated group (53.6%) and the risperidone LAIA-treated group (56.7%) in terms of response rate (RR = 0.93; 95% CI, 0.79 to 1.10; P = 0.40), and there was significant heterogeneity (I2 = 78%, P = 0.01) (Figure 3B). The PP-treated group showed a statistically significant increased risk of discontinuation of treatment for any reason compared with the risperidone LAIA-treated group. The RR value was 1.19 (35.7% vs 30.4%; 95% CI, 1.03 to 1.39; P = 0.02), with mild heterogeneity (I2 = 31%, P = 0.23) (Figure 3C). We also analysed the safety outcomes based on total TEAEs during the double-blind trial (DBT) period. Although the difference was nonsignificant, more patients receiving PP therapy had TEAEs than those who received risperidone LAIA (66.6% vs 64.8%; RR = 1.01; 95% CI, 0.94 to 1.09; P = 0.78), with statistically nonsignificant mild heterogeneity (I2 = 48%, P = 0.15) (Figure 3D).
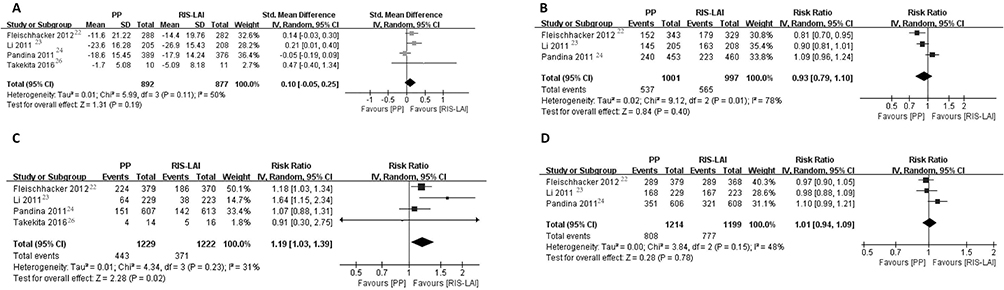 |
Figure 3 Forest plot of the primary outcomes of paliperidone palmitate (PP) and risperidone long-acting injectable (RIS-LAI) for (A) Standardized mean differences (SMDs) and 95% confidence intervals (CIs) for changed Positive and Negative Syndrome Scale (PANSS) total scores. (B) Risks ratios (RRs) and 95% confidence intervals (CIs) of the response rates. (C) Risks ratios (RRs) and 95% confidence intervals (CIs) of the discontinuation of treatment due to any reason. (D) Risks ratios (RRs) and 95% confidence intervals (CIs) of the total treatment emergent adverse events (TEAEs). |
Secondary Outcomes
Relative treatment effects for changes from the baseline to the endpoint in positive and negative subscale PANSS scores and CGI-S scores are shown by forest plots. PP-treated patients showed no difference compared to risperidone LAIA-treated patients in terms of the overall pooled effect size, with an SMD of 0.12 (95% CI, −0.15 to 0.39; P = 0.39) and a statistically significant heterogeneity (I2 = 73%, P = 0.03) for the PANSS positive score changes (Figure 4A). An SMD of 0.04 (95% CI, −0.09 to 0.16; P = 0.56) with mild heterogeneity (I2 = 12%, P = 0.32) was found for the PANSS negative score change (Figure 4B). No significant difference was found between the PP and risperidone LAIA-treated groups, with an SMD of 0.10 (95% CI, −0.02 to 0.21; P = 0.10) and a mild heterogeneity (I2 = 39%, P = 0.19) regarding CGI-S score changes (Figure 4C).
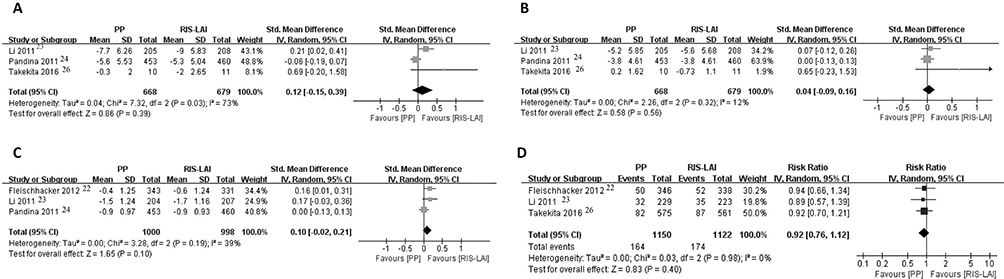 |
Figure 4 Forest plot of the secondary outcomes of paliperidone palmitate (PP) and risperidone long-acting injectable (RIS-LAI) for (A) Standardized mean differences (SMDs) and 95% confidence intervals (CIs) for changed Positive and Negative Syndrome Scale (PANSS) positive scores. (B) Standardized mean differences (SMDs) and 95% confidence intervals (CIs) for changed PANSS negative scores. (C) Standardized mean differences (SMDs) and 95% confidence intervals (CIs) for changed clinical global impression of severity (CGI-S) scale score. (D) Risks ratios (RRs) and 95% confidence intervals (CIs) of the rates of a ≥7% increase in body weight. |
Because the ratio of ≥ a 7% increase in body weight is a standard regulatory metric, we also analysed the incidence of a ≥ 7% increase in body weight, which was not analysed in a previous review.25 The difference did not reach significance (14.3% and 15.5% for PP and risperidone LAIA, respectively; RR = 0.92; 95% CI, 0.76 to 1.12; P = 0.40), and there was no heterogeneity (I2 = 0%, P = 0.98) (Figure 4D).
Discussion
We conducted this meta-analysis to critically evaluate the efficacy and safety of PP compared with risperidone LAIA. Two23,26 of the four relevant RCTs included were not analysed in a previous review.25 In addition to the PANSS total score change, CGI-S score change, and total discontinuation rate, we examined factors not looked at in previous studies, such as response rate, changes in positive and negative subscale PANSS scores, total TEAEs, and the ≥7% increase in body weight.
As was the case with the previous review,25 no statistically significant differences were found between the PP-treated group and the risperidone LAIA-treated patients in terms of PANSS total score and CGI-S score changes at endpoint.
Clinical trials of antipsychotics for use with effective schizophrenia suggest a 64–84% discontinuation rate for various antipsychotic treatments.33,34 All-cause discontinuation has previously been used as a measure of treatment acceptability because it encompasses efficacy and tolerability.35 Inconsistent with the conclusions of previous research,25 our analyses showed that significantly higher numbers of PP-treated patients discontinued treatment compared with the risperidone LAI-treated groups. This finding may alert psychiatrists to the risk of PP being associated with increased discontinuation compared to risperidone-LAIA.
Response rate, one of the primary outcomes in our study, can clearly demonstrate patient symptom improvement and is of high clinical value.36 A previous study25 did not analyse response rate. Interestingly, we found that there was a nonsignificant decrease in response rate among the PP-treated group compared to the risperidone-LAIA group (53.6% vs 56.7%).
Weight gain is a risk factor not only for obesity, which is associated with a reduced quality of life, but also for metabolic syndrome, which leads to increased morbidity and mortality in psychiatric patients.33 Interestingly, we identified no difference between the PP and risperidone-LAIA-treated participants in terms of the incidence of a ≥ 7% increase in body weight. This may indicate that patients who are receiving PP are not significantly at risk for increased body weight gain compared with those receiving risperidone-LAIA.
In summary, we found that PP may not be either safer or more effective than risperidone-LAIA treatment, except in terms of total discontinuation rates.
This study had several limitations. First, we included only four randomized controlled trials (RCTs), which may have influenced the reliability of the results. Second, the sample sizes were generally small. Only 2451 patients were included; thus, conclusions based on certain study populations might not be generalisable to the wider public. Third, the PANSS positive scores change and response rate showed significant heterogeneity, but the sensitivity analysis or subgroup analysis should not be performed because only four RCTs (two open-label studies and two double-blind RCTs) were included. More studies will need to be conducted to demonstrate these results further. Finally, owing to the limited number of studies included in our meta-analysis, we did not compare time of onset between groups treated with PP-LAIs and risperidone-LAIA.
Conclusion
In conclusion, our meta-analysis showed no significant statistical differences in PANSS total scores, PANSS positive scores, PANSS negative scores, CGI-S endpoint score changes, response rates, ratios of total TEAEs, or a ≥ 7% increase in body weight. Furthermore, the total discontinuation rate may be significantly higher for PP compared to risperidone-LAIA. In other words, our study did not find a more beneficial effect of PP compared to risperidone-LAIA treatment for schizophrenia, which were similar to the results of the previous study.25 Although this study is likely to be of interest to clinicians and patients, clinicians should interpret and translate our data with caution because the meta-analysis was based on a limited number of RCTs and patients. Therefore, in the future, there is an urgent need to conduct more high-quality RCTs comparing PP-LAI and risperidone-LAIA treatments for schizophrenia. Additionally, more relevant meta-analyses will need to be carried out to assist clinicians in making treatment recommendations and establishing optimal treatment strategies.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This study was supported by the Central Plains Talent Programme (Yucai Series), Henan Collaborative Innovation Center of Prevention and Treatment of Mental Disorder.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Chesney E, Goodwin G, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. 2014;13(2):153–160. doi:10.1002/wps.20128
2. Owen M, Sawa A, Mortensen P. Schizophrenia. Lancet. 2016;388(10039):86–97. doi:10.1016/s0140-6736(15)01121-6
3. Samara MT, Dold M, Gianatsi M, et al. Efficacy, acceptability, and tolerability of antipsychotics in treatment-resistant schizophrenia: a network meta-analysis. JAMA Psychiatr. 2016;73(3):199–210. doi:10.1001/jamapsychiatry.2015.2955
4. Messias E, Chen C, Eaton W. Epidemiology of schizophrenia: review of findings and myths. Psychiatr Clin North Am. 2007;30(3):323–338. doi:10.1016/j.psc.2007.04.007
5. McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. 2008;30:67–76. doi:10.1093/epirev/mxn001
6. Volavka J, Citrome L. Oral antipsychotics for the treatment of schizophrenia: heterogeneity in efficacy and tolerability should drive decision-making. Expert Opin Pharmacother. 2009;10(12):1917–1928. doi:10.1517/14656560903061309
7. Rössler W, Salize H, van Os J, Riecher-Rössler A. Size of burden of schizophrenia and psychotic disorders. Eur Neuropsychopharmacol. 2005;15(4):399–409. doi:10.1016/j.euroneuro.2005.04.009
8. Browne S, Clarke M, Gervin M, Waddington J, Larkin C, O’Callaghan E. Determinants of quality of life at first presentation with schizophrenia. Br J Psychiatr. 2000;176:173–176. doi:10.1192/bjp.176.2.173
9. Hayhurst K, Massie J, Dunn G, Lewis S, Drake R. Validity of subjective versus objective quality of life assessment in people with schizophrenia. BMC Psychiatry. 2014;14:365. doi:10.1186/s12888-014-0365-x
10. Miyamoto S, Duncan GE, Marx CE, Lieberman JA. Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry. 2005;10(1):79–104. doi:10.1038/sj.mp.4001556
11. Mauri MC, Paletta S, Maffini M, et al. Clinical pharmacology of atypical antipsychotics: an update. Excli J. 2014;13:1163–1191.
12. Miyamoto S, Miyake N, Jarskog LF, Fleischhacker WW, Lieberman JA. Pharmacological treatment of schizophrenia: a critical review of the pharmacology and clinical effects of current and future therapeutic agents. Mol Psychiatry. 2012;17(12):1206–1227. doi:10.1038/mp.2012.47
13. Uçok A, Gaebel W. Side effects of atypical antipsychotics: a brief overview. World Psychiatry. 2008;7(1):58–62. doi:10.1002/j.2051-5545.2008.tb00154.x
14. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
15. Ostuzzi G, Bertolini F, Del Giovane C, et al. Maintenance treatment with long-acting injectable antipsychotics for people with nonaffective psychoses: a network meta-analysis. Am J Psychiatry. 2021;178(5):424–436. doi:10.1176/appi.ajp.2020.20071120
16. Tiihonen J, Haukka J, Taylor M, Haddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168(6):603–609. doi:10.1176/appi.ajp.2011.10081224
17. Stahl S. Long-acting injectable antipsychotics: shall the last be first? CNS Spectr. 2014;19(1):3–5. doi:10.1017/s1092852913001016
18. Simpson GM. A brief history of depot neuroleptics. J Clin Psychiatry. 1984;45(5 Pt 2):3–4.
19. Cameron C, Zummo J, Desai DN, et al. Aripiprazole lauroxil compared with paliperidone palmitate in patients with schizophrenia: an indirect treatment comparison. Value Health. 2017;20(7):876–885. doi:10.1016/j.jval.2017.03.010
20. Bramante S, Di Salvo G, Maina G, Rosso G. Paliperidone palmitate: a breakthrough treatment for schizophrenia? A review on patient adherence levels, healthcare resource utilization and costs. Neuropsychiatr Dis Treat. 2023;19:519–530. doi:10.2147/ndt.s374696
21. Whale R, Pereira M, Cuthbert S, Fialho R. Effectiveness and predictors of continuation of paliperidone palmitate long-acting injection treatment: a 12-month naturalistic cohort study. J Clin Psychopharmacol. 2015;35(5):591–595. doi:10.1097/jcp.0000000000000385
22. Fleischhacker WW, Gopal S, Lane R, et al. A randomized trial of paliperidone palmitate and risperidone long-acting injectable in schizophrenia. Article. Int J Neuropsychopharmacol. 2012;15(1):107–118. doi:10.1017/S1461145711001076
23. Li H, Rui Q, Ning X, Xu H, Gu N. A comparative study of paliperidone palmitate and risperidone long-acting injectable therapy in schizophrenia. Comparative Study; Journal Article; Randomized Controlled Trial. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(4):1002–1008. doi:10.1016/j.pnpbp.2011.02.001
24. Pandina G, Lane R, Gopal S, et al. A double-blind study of paliperidone palmitate and risperidone long-acting injectable in adults with schizophrenia. Journal Article; Randomized Controlled Trial; Research Support, Non‐U.S. Gov’t. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):218–226. doi:10.1016/j.pnpbp.2010.11.008
25. Nussbaum AM, Stroup TS. Paliperidone palmitate for schizophrenia. Cochrane Database Syst Rev. 2012;(6). doi:10.1002/14651858.CD008296.pub2
26. Takekita Y, Koshikawa Y, Fabbri C, et al. Cognitive function and risperidone long-acting injection vs. paliperidone palmitate in schizophrenia: a 6-month, open-label, randomized, pilot trial. Article. BMC Psychiatry. 2016;16(1):172. doi:10.1186/s12888-016-0883-9
27. Higgins J, Thompson SG, Deeks JJ, Altman DG. Cochrane handbook for systematic reviews of interventions version 5.1.0. the Cochrane collaboration. Naunyn Schmiedebergs Archiv für Experimentelle Pathologie und Pharmakologie. 2008;5(2):S38.
28. Moher D, Liberati A, Tetzlaff J, Altman D. Reprint--preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89(9):873–880. doi:10.1093/ptj/89.9.873
29. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. doi:10.1016/0197-2456(86)90046-2
30. Higgins J, Thompson S, Deeks J, Altman D. Statistical heterogeneity in systematic reviews of clinical trials: a critical appraisal of guidelines and practice. J Health Serv Res Policy. 2002;7(1):51–61. doi:10.1258/1355819021927674
31. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
32. Leucht S, Kane J, Kissling W, Hamann J, Etschel E, Engel R. What does the PANSS mean? Schizophr Res. 2005;79:231–238. doi:10.1016/j.schres.2005.04.008
33. Stroup TS, Lieberman JA, Mcevoy JP, et al. Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am J Psychiatry. 2006;163(4):611–622. doi:10.1176/ajp.2006.163.4.611
34. Lieberman JA, Stroup TS, McEvoy JP, et al.Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. Revista Colombiana De Psiquiatría. 2005;353(12):1209–1223.
35. Cipriani A, Furukawa T, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009;373(9665):746–758. doi:10.1016/S0140-6736(09)60046-5
36. Cai S, Lu H, Bai Z, Wu R, Zhao J. Paliperidone extended-release tablets in Chinese patients with schizophrenia: meta-analysis of randomized controlled trials. Neuropsychiatr Dis Treat. 2015;11:1817–1834. doi:10.2147/NDT.S84833
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Personal and Social Functioning and Health-Related Quality of Life in Patients with Schizophrenia Treated with the Long-Acting Injectable Antipsychotic Risperidone ISM
Litman R, Naber D, Anta L, Martínez J, Filts Y, Correll CU
Neuropsychiatric Disease and Treatment 2023, 19:219-232
Published Date: 25 January 2023
The Effect of Longer Dosing Intervals for Long-Acting Injectable Antipsychotics on Outcomes in Schizophrenia
Milz R, Benson C, Knight K, Antunes J, Najarian D, Lopez Rengel PM, Wang S, Richarz U, Gopal S, Kane JM
Neuropsychiatric Disease and Treatment 2023, 19:531-545
Published Date: 7 March 2023
Aripiprazole Plasma Concentrations Delivered from Two 2-Month Long-Acting Injectable Formulations: An Indirect Comparison
Harlin M, Chepke C, Larsen F, Bell Lynum KS, Chumki SR, Fitzgerald H, Such P, Madera-McDonough J, Yildirim M, Panni M, Saklad SR
Neuropsychiatric Disease and Treatment 2023, 19:1409-1416
Published Date: 8 June 2023
A Meta-Analysis on the Efficacy of Acupuncture as an Adjuvant Therapy for Schizophrenia
Huang C, Zhang P, Dong Y, Chang R, Lao J, Li Z, Lan D
Neuropsychiatric Disease and Treatment 2023, 19:2381-2400
Published Date: 7 November 2023
Treatment Patterns and Outcomes from OASIS: A Prospective Observational Study of Long-Acting Injectables in Schizophrenia
Weiden PJ, Strand LN, Doane MJ, Arevalo C, McGrory JA, Achtyes ED, Harvey PD, Kane JM, Saklad SR, Trotter J, Velligan DI
Neuropsychiatric Disease and Treatment 2025, 21:2165-2181
Published Date: 23 September 2025