Back to Journals » Journal of Pain Research » Volume 16
Association Between Pharmacotherapy and Sleep Quality in Patients with Chronic Orofacial and Chronic Body Pain: A Cross-Sectional Study
Authors Bavia PF ![]() , Khawaja S
, Khawaja S ![]() , Hernández-Nuño de la Rosa MF
, Hernández-Nuño de la Rosa MF ![]() , Tseng LA, Keith DA
, Tseng LA, Keith DA ![]()
Received 15 April 2023
Accepted for publication 23 September 2023
Published 10 October 2023 Volume 2023:16 Pages 3433—3440
DOI https://doi.org/10.2147/JPR.S412459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Paula Furlan Bavia,1 Shehryar Khawaja,2,3 María F Hernández-Nuño de la Rosa,4 Lisa A Tseng,5 David Alexander Keith6
1Private Practice Boca Raton Prosthodontics (Practice Limited to Orofacial Pain), Boca Raton, FL, USA; 2Department of Internal Medicine, Shaukat Khanum Memorial Cancer Hospital & Research Centre, Lahore, Pakistan; 3Craniofacial Pain Center, Department of Diagnostic Sciences, Tufts University School of Dental Medicine, Boston, MA, USA; 4Department of Oral and Maxillofacial Surgery, Tufts University School of Dental Medicine, Boston, MA, USA; 5Pain Medicine, Kaiser Permanente, Redwood City, CA, USA; 6Department of Oral and Maxillofacial Surgery, Massachusetts General Hospital and Harvard School of Dental Medicine, Boston, MA, USA
Correspondence: Paula Furlan Bavia, Email [email protected]
Purpose: Sleep impairment is associated with many chronic pain disorders. While there is an association between chronic pain and sleep disturbances, little is known about the influence of pharmacotherapy for chronic pain conditions, particularly chronic opioid therapy, on sleep. This study aimed to 1) compare the sleep quality (SQ) in patients with two different pain conditions-chronic body pain and chronic orofacial pain; 2) assess the correlation of SQ and pain intensity; and 3) evaluate the association between pharmacotherapy and SQ.
Patients and Methods: The Pittsburgh Sleep Quality Index (PSQI) was used to measure the SQ in subjects with 1) chronic body pain (n = 100) and 2) chronic orofacial pain (n = 100). The visual analogue scale was applied for pain intensity rating. All subjects were adults recruited at Massachusetts General Hospital, United States. The subjects’ demographic data, pain intensity, diagnosis and concurrent use of medications were extracted from their electronic medical records (EMR). Statistical analyses were performed using T-test and Pearson correlation coefficient.
Results: Among 200 subjects (mean age 51.01 ± 15.52 years), 141 (70.5%) were females. PSQI and pain intensity were statistically significantly different between the two groups (p < 0.05 and p < 0.0001, respectively) and higher in subjects with chronic body pain. There was a positive correlation between PSQI and pain intensity (chronic orofacial pain r = 0.3535, p = 0.0004; chronic body pain: r = 0.2247, p < 0.026). PSQI was higher in chronic orofacial pain subjects utilizing opioids and benzodiazepines (PSQI = 15.25).
Conclusion: Chronic pain impairs SQ, which is noticeably worse in subjects with body pain conditions. In addition, pain intensity was correlated with poorer SQ, which in turn was linked to the concomitant use of opioid and benzodiazepine therapy in chronic orofacial pain.
Keywords: sleep quality, chronic pain, pain intensity, pharmacotherapy, opioids, benzodiazepines
Introduction
Sleep plays an essential role in regulating critical mechanisms within the human body. It is well known that sleep regulates brain functions and controls systemic physiological aspects, eg, metabolism, appetite, immune, hormonal and cardiovascular systems.1 A recent cross-sectional study has shown that health status is an important factor affecting sleep and approximately 70.6% of individuals with very good/excellent health reported good/very good sleep quality and only 4.3% rated their sleep quality as poor or very poor.2 In contrast, evidence suggests a strong relationship between sleep and chronic pain, estimating that the prevalence of sleep disturbance ranges between 50% and 80% in patients with chronic pain.3,4 Moreover, a bidirectional association has also been reported,5,6 indicating that in most chronic painful conditions, a night of poor sleep may be followed by increased pain, which in turn may lead to poor sleep.6
Temporomandibular disorders (TMD) are often sources of chronic pain that can alter sleep patterns and lead to comorbid sleep impairments. It is known that painful TMDs significantly impact sleep quality.7,8 Similarly, sleep quality can be progressively worsened prior to the onset of painful TMD.9 It has recently been suggested that disturbed sleep might also be a risk factor for jaw functional limitation in patients with painful TMD.10 In addition, other chronic painful conditions affecting the orofacial region, eg, burning mouth syndrome;11,12 trigeminal neuralgia;13 painful posttraumatic trigeminal neuropathy,13 as well as adults with migraine, particularly those with chronic migraine,14 tension-type headache15 and cervicogenic headaches,16 report worse subjective sleep quality (SQ) than healthy individuals.
There is a clear association between other chronic body pain conditions and sleep disorders. Recent studies have demonstrated poorer SQ in patients with chronic widespread pain;17 fibromyalgia;18,19 symptomatic lumbar spinal stenosis;20 low back pain;21 endometriosis22 and irritable bowel syndrome.23
While it is widely accepted that pain has a negative effect on SQ, little is known about how pharmacotherapy for chronic pain may affect sleep. Specifically, there is a lack of clinical evidence on chronic opioid therapy and a validated SQ metric. Regular, chronic use of opioids is known to interfere with sleep via several mechanisms. It can lead to changes in sleep architecture, including a reduction in sleep efficiency as well as slow wave sleep.24 There also may be a reduction in rapid eye movement (REM) sleep.25 These effects of chronic opioid therapy appear to be dose dependent and lead to poor sleep SQ, resulting in daytime sleepiness.26,27
Given the potential effects of opioids on sleep and the widespread use of opioids in patients with chronic pain, it is clinically relevant to assess sleep in this group of patients. Thus, this study aimed to 1) compare SQ in patients with these two pain conditions; 2) assess the correlation of SQ and pain intensity; and 3) evaluate the association between pharmacotherapy and SQ.
Materials and Methods
Study Sample and Design
This was a cross-sectional study of adult subjects (males and females; age 18–85 years) that had undergone clinical evaluation and management for chronic orofacial pain (n = 100) and chronic body pain (n = 100) in the Department of Oral and Maxillofacial Surgery and Center for Pain Medicine at the Department of Anesthesia, Critical Care and Pain Medicine, at Massachusetts General Hospital, Boston, Massachusetts, United States, between January 2016 and December 2017. All subjects were invited to participate in the study and provided a written consent form approved by the Oral and Maxillofacial Surgery Department Research Committee and Mass General Brigham Human Research Protection Program (HRPP) at Massachusetts General Hospital, Boston, Massachusetts, USA (IRB # 2015P001711). The present study followed the Declaration of Helsinki.
A visual analog scale (VAS) was used to subjectively evaluate pain levels. It was a 100-mm-long horizontal line, anchored by word descriptors at each end, where the left side reads “no pain” and the right side reads “worst pain imaginable.” Patients drew a vertical mark on the line at the point that best represented their perception of their pain level.28 SQ was assessed using the Pittsburgh Sleep Quality Index (PSQI),29 which addresses habitual measures rather than a particular night of sleep, as in laboratory sleep measures. It comprises 19 items and assesses seven components of SQ (subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, hypnotic medication use and daytime dysfunction). Each component is rated on a 0–3 severity scale referring to the frequency of each disturbance and yields a global score with a range of 0–21. A PSQI global score of 5 or greater indicates clinically significant sleep disturbances. For the purposes of this study, the use of sleeping medication, a component of the PSQI, and the global PSQI score were also evaluated.
Clinical Information
The hospital electronic medical records (EMR) were reviewed to extract information regarding subjects’ demographics, pain diagnosis and concurrent use of pharmacological agents such as opioid analgesic medications, non-steroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, triptans, hypnotic and neuropathic agents (eg, anticonvulsants, benzodiazepines, gabapentinoids, and tricyclic antidepressants).
The data regarding pain diagnosis and medication use were extracted from patients’ electronic health records from the most recent primary care physician (PCP) records. Likewise, patient records from other medical providers were reviewed to corroborate the information extracted from PCP’s visit. The medications included were used on a daily basis, however their respective dosages were not taken into account for the current analysis.
Statistical Analyses
The T-test was used for comparison of continuous variables (PSQI) between the two studied groups (chronic orofacial pain vs body pain). Pearson’s correlation coefficient was performed to explore correlations between PSQI and pain intensity in both studied groups. A descriptive analysis was conducted to summarize the PSQI global score of patients concomitantly using the following medications: non-opioids; non-opioids + sleep medicines; opioids + sleep medicines; and opioids + benzodiazepines. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using the BioEstat software (version 5.0, Mamiraua Sustainable Development Institute, Belem, Para, Brazil).
Results
Among 200 subjects, 141 (70.5%) were females. The mean age of study subjects was 51.01 ± 15.52 years. The demographic characteristics of both groups are summarized in Table 1. The etiology of the patients’ orofacial pain was as follows: temporomandibular disorders (84%); painful posttraumatic trigeminal neuropathy (13%); trigeminal neuralgia (3%); burning mouth syndrome (4%); and chronic migraine (3%). The etiology of the patients’ chronic body pain was as follows: low back pain (60%); upper back/shoulder pain (17%); chest/abdominal/pelvic pain (10%); complex regional pain syndrome (3%); neuropathic foot pain (3%); fibromyalgia (2%); cancer-related pain (1%); and post-herpetic neuralgia (1%).
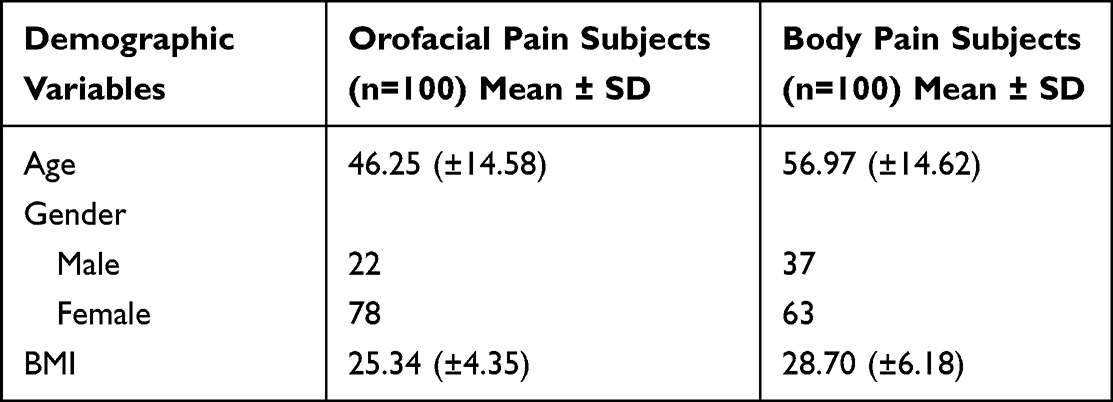 |
Table 1 Summary of Demographic Characteristics of Patients with Chronic Orofacial and Body Pain Conditions |
The pain score was 5.07 in patients with chronic orofacial pain and 6.55 among those with chronic body pain (p < 0.0001) (Table 2). PSQI global score of 5 or greater was reported by 86% and 96% participants with chronic orofacial and body pain, respectively. The mean PSQI score was 9.10 ± 4.55 and 11.44 ± 4.50 for participants with chronic orofacial and body pain, respectively (p = 0.0002) (Figure 1). There was a positive correlation between PSQI and pain intensity (chronic orofacial pain r = 0.3535, p = 0.0004; chronic body pain: r = 0.2247, p < 0.026).
 |
Table 2 Summary of PSQI and Pain Score (VAS) of Patients with Chronic Orofacial and Body Pain Conditions |
 |
Figure 1 Comparison of global PSQI score among patients with chronic orofacial and body pain. |
Of the 100 participants with chronic orofacial pain, only 13 participants were not utilizing any medications and 87 were utilizing at least one pharmacological agent for pain management. Of those, fifty participants (50%) were utilizing non-opioids; 21 (21%) were utilizing non-opioids and sleep medication; twelve (12%) were utilizing opioids and sleep medication; and 4 (4%) participants were concomitantly using opioids and benzodiazepines. The global PSQI was considerably higher in the subjects utilizing the combination of opioids and benzodiazepines (PSQI = 15.25) than in the subjects who were utilizing non-opioid medications (PSQI = 9.60) or the combination of non-opioids + sleep medications (PSQI = 11.43) and opioids and sleep medications (PSQI = 14.80). Similarly, 100% of the participants with chronic body pain were utilizing at least one pharmacological agent for pain management. Of those, fifty-seven participants (57%) were utilizing non-opioids; 6 (6%) were utilizing non-opioids and sleep medication; twenty (20%) were utilizing opioids and sleep medication; and seventeen (17%) participants were concomitantly using opioids and benzodiazepines. The global PSQI was higher in the subjects utilizing the combination of non-opioids + sleep medications (PSQI = 14.50) than in the subjects who were taking a combination of opioids and benzodiazepines (PSQI = 12.24) than in the subjects who were utilizing opioids and sleep medications (PSQI = 11.40) and non-opioid medications (PSQI = 10.53) (Figure 2).
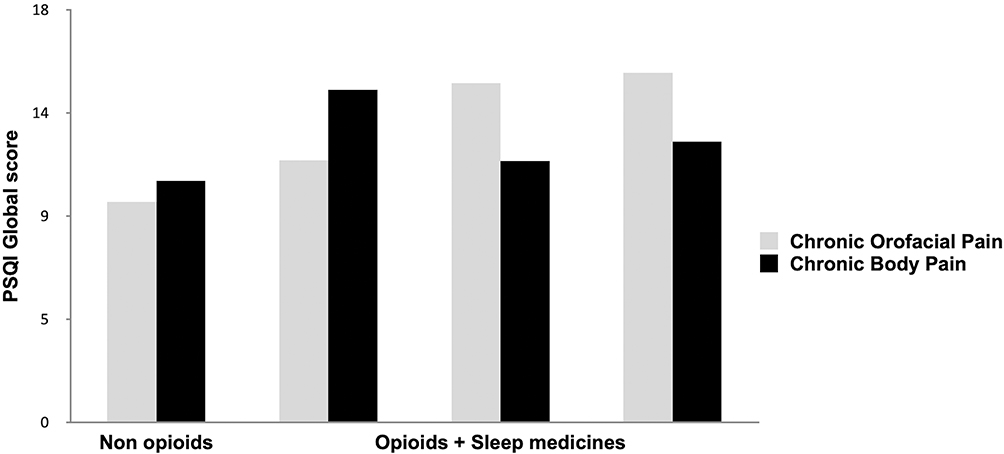 |
Figure 2 PSQI global score according to concurrent use of opioid and non-opioid medications. |
Discussion
To the authors’ knowledge, this is the first study to directly contrast the sleep quality in patients with chronic orofacial and body pain. Poor SQ (PSQI > 5) was observed in 86% and 96% percent of patients with chronic orofacial and body pain, respectively. The findings of this study suggest that sleep disruption is common in all chronic pain conditions and, in accordance with previous studies, which have demonstrated poor SQ ranging from 86.4% to 92.9% in individuals with different chronic pain conditions.30–32 Moreover, the present study revealed that patients with chronic body pain reported worse PSQI parameters compared to chronic orofacial pain patients. Thus, poorer SQ was observed in patients with chronic body pain, with a mean global PSQI score of 11.44. Likewise, previous studies demonstrated similar global PSQI scores of 11.9631 and 12.130 indicating clinically significant sleep impairment and emphasizing the importance of evaluating SQ while treating chronic pain.
In both groups in the present study, most patients with chronic pain were females. This could be attributed to the fact that chronic pain conditions are considerably more prevalent in the female than male population.33 Low back pain and temporomandibular disorders (TMD) were the most common conditions affecting 60% of the chronic body pain group and 84% of the chronic orofacial pain group, respectively. Likewise, low back pain and TMD are highly prevalent among chronic pain conditions and are in turn also more common in women.34,35
This study shows that individuals with chronic body pain reported higher pain scores (6.55) when compared to chronic orofacial pain patients (5.07) and that a moderate positive correlation exists between pain intensity and SQ for both groups. In the studied cohort, the higher the pain score, the higher the global PSQI score, suggesting that pain intensity may interfere with SQ. These results are consistent with previous studies32,36,37 which also identified that the greater the intensity of pain according to the VAS, the higher the PSQI global score. Moreover, those who considered their sleep as “poor quality” have significantly elevated pain intensity, suggesting that the intensity of pain plays a role in the quality of sleep.32 As previously reported, the relationship between chronic pain and sleep has been described as a “circular model” where a night of poor sleep is followed by a day with more intense pain, which is then followed by a night of nonrestorative sleep and morning-related complaints of unrefreshed sleep.38 In addition to this “vicious cycle”, poor sleep heightens pain sensitivity,39 resulting in the requirement for more medications in an attempt to control pain symptoms and improve sleep.
In the present investigation information regarding medication use was obtained from EMR and included non-opioid (NSAIDs, analgesics, muscle relaxants, antidepressants, anticonvulsants, tricyclic antidepressants), non-benzodiazepines prescribed as sleeping aid agents, benzodiazepines and opioids. In this sample, at least one pharmacological agent was being used for pain management in 100% and 87% of chronic body pain and orofacial pain groups, respectively. In the chronic body pain group, 20% of individuals were utilizing opioids, and 17% of individuals were concomitantly using opioids and benzodiazepines. In the chronic orofacial pain group, 12% of individuals were utilizing opioids, and 4% of individuals were concomitantly using opioids and benzodiazepines. The global PSQI was considerably higher in the subjects utilizing the combination of opioids and benzodiazepines than in the subjects who were utilizing non-opioid medications or a combination of non-opioids/opioids and sleep medications. Thus, results from this study suggest that patients with chronic orofacial pain who are prescribed opioids report more sleep impairment than patients with chronic pain who are not prescribed opioid medications. Evidence indicates that chronic use of opioids significantly disrupts sleep via several mechanisms. Previous studies have shown that opioid use affects sleep architecture.26,27 Normal sleep architecture consists of cycles of non-rapid eye movement (NREM) and rapid eye movement (REM) sleep, with NREM predominating in the first part of the night and REM at the final sleep stages. NREM sleep is divided in NREM 1, 2 and 3 stages, with 3 characterized as the deepest stage, essential for restorative sleep.40 It has been shown that opioids suppress rapid-eye-movement (REM) sleep and deep non-rapid-eye-movement (NREM) and increase light NREM sleep,26,27 thus interfering with the restorative aspect of sleep. Furthermore, the use of opioid medications has been associated with increased incidence of sleep apnea41 and hazardous respiratory depression that can lead to hypercapnic respiratory failure, leading to serious morbidity or death.42 Similarly, long-term opioids may play a role in the exacerbation of central sleep apneic events43 and opioid-induced hyperalgesia,44 which could contribute to additional sleep impairment in individuals with chronic pain. Interestingly, impaired sleep quality is a critical comorbidity in patients with opioid use disorder45 and suicidal ideation,46 therefore highlighting the importance of sleep assessment in patients on chronic opioid therapy. Given the deleterious association between opioid use, sleep, and pain, long-term opioid should be cautiously recommended for chronic pain. Furthermore, prior to considering long-term opioid therapy, clinicians should perform individualized benefit–risk assessments; opioid selection, dose initiation/titration/monitoring/mitigation strategies; and consideration of alternative, non-opioid therapies.47 In addition, despite the use of benzodiazepines to address sleep issues, they are also known to interfere with sleep quality by reducing deep NREM sleep and resurgence of insomnia,48 and a poorer sleep quality has been associated with prolonged use of benzodiazepines;49–51 therefore, the chronic and indiscriminate use of these medications should also be avoided when treating chronic pain conditions.
Our results suggest that clinicians who manage patients with chronic pain should focus on interventions that relieve pain, as well as assessing and treating sleep disturbance. However, there are limitations to the conclusions that can be drawn from this study. First, possible associations between gender and sleep quality were not addressed in this research. Second, due to the observational nature of the cross-sectional study design, the results cannot be used to determine causality. In addition, even though the PSQI has been widely used as a validated questionnaire to detect possible sleep problems, the PSQI uses retrospective self-report to measure SQ and the scores could be impacted by other pain- and sleep-related factors, such as depression or anxiety, which were not accounted for in the present investigation. Future research should consider the use of objective measures such as polysomnography along with the self-reported subjective assessments to improve the accuracy of overall sleep impairments. Moreover, data regarding pharmacotherapy was extracted from the EMR, thus it was not possible to verify whether medications were taken as prescribed. Lastly, different types of non-opioid and opioid medications were prescribed, and it was not determined if a particular medication was associated with the outcome variables; therefore, additional prospective research is suggested to precisely evaluate the impact of opioids on sleep and pain outcomes.
Conclusion
This study has shown that chronic pain impairs sleep quality, which is noticeably worse in subjects with chronic body pain. It also suggests that the concomitant use of opioid and benzodiazepine medications is linked to a lower sleep quality in chronic orofacial pain.
Acknowledgments
The authors hereby express their gratitude to Dr. Steven John Scrivani for initiating this study. This study was supported by the Massachusetts General Hospital – Oral and Maxillofacial Surgery Education and Research Fund (IRB Protocol: 2015P001711).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Colten HR, Altevogt BM. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington (DC): National Academies Press; 2006.
2. Gordon NP, Yao JH, Brickner LA, Lo JC. Prevalence of sleep-related problems and risks in a community-dwelling older adult population: a cross-sectional survey-based study. BMC Public Health. 2022;22(1):2045. doi:10.1186/s12889-022-14443-8
3. Cole JC, Dubois D, Kosinski M. Use of patient-reported sleep measures in clinical trials of pain treatment: a literature review and synthesis of current sleep measures and a conceptual model of sleep disturbance in pain. Clin Ther. 2007;29:2580–2588. doi:10.1016/j.clinthera.2007.12.005
4. Sun Y, Laksono I, Selvanathan J, et al. Prevalence of sleep disturbances in patients with chronic non-cancer pain: a systematic review and meta-analysis. Sleep Med Rev. 2021;57:101467. doi:10.1016/j.smrv.2021.101467
5. Schutz TC, Andersen ML, Tufik S. The influence of orofacial pain on sleep pattern: a review of theory, animal models and future directions. Sleep Med. 2009;10(8):822–828. doi:10.1016/j.sleep.2008.09.018
6. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539–1552. doi:10.1016/j.jpain.2013.08.007
7. Vilanova LS, Goncalves TM, Pimentel MJ, Bavia PF, Rodrigues Garcia RC. Mastication movements and sleep quality of patients with myofascial pain: occlusal device therapy improvements. J Prosthet Dent. 2014;112(6):1330–1336. doi:10.1016/j.prosdent.2014.07.008
8. Lei J, Yap AU, Zhang M, Fu KY. Temporomandibular disorder subtypes, emotional distress, impaired sleep, and oral health-related quality of life in Asian patients. Community Dent Oral Epidemiol. 2021;49(6):543–549. doi:10.1111/cdoe.12643
9. Sanders AE, Akinkugbe AA, Bair E, et al. Subjective Sleep quality deteriorates before development of painful temporomandibular disorder. J Pain. 2016;17(6):669–677. doi:10.1016/j.jpain.2016.02.004
10. Kim HK, Kim ME. Disturbed sleep may be a core risk factor for jaw functional limitation in patients with painful temporomandibular disorders. J Oral Rehabil. 2021;48(9):1013–1024. doi:10.1111/joor.13217
11. Lopez-Jornet P, Lucero-Berdugo M, Castillo-Felipe C, Zamora Lavella C, Ferrandez-Pujante A, Pons-Fuster A. Assessment of self-reported sleep disturbance and psychological status in patients with burning mouth syndrome. J Eur Acad Dermatol Venereol. 2015;29(7):1285–1290. doi:10.1111/jdv.12795
12. Lee GS, Kim HK, Kim ME. Relevance of sleep, pain cognition, and psychological distress with regard to pain in patients with burning mouth syndrome. Cranio. 2022;40(1):79–87. doi:10.1080/08869634.2019.1681621
13. Haviv Y, Zini A, Etzioni Y, et al. The impact of chronic orofacial pain on daily life: the vulnerable patient and disruptive pain. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017;123(1):58–66. doi:10.1016/j.oooo.2016.08.016
14. Stanyer EC, Creeney H, Nesbitt AD, Holland PR, Hoffmann J. Subjective sleep quality and sleep architecture in patients with migraine: a meta-analysis. Neurology. 2021;97(16):e1620–e1631. doi:10.1212/WNL.0000000000012701
15. Andrijauskis D, Ciauskaite J, Vaitkus A, Pajediene E. Primary Headaches and Sleep Disturbances: a Cause or a Consequence? J Oral Facial Pain Headache. 2020;34(1):61–66. doi:10.11607/ofph.2405
16. Mingels S, Dankaerts W, van Etten L, Bruckers L, Granitzer M. Exploring multidimensional characteristics in cervicogenic headache: relations between pain processing, lifestyle, and psychosocial factors. Brain Behav. 2021;11(10):e2339. doi:10.1002/brb3.2339
17. de Rooij A, van der Leeden M, Roorda LD, Rinkema M, Beuving W, Dekker J. Factors associated with sleep quality in patients with chronic widespread pain attending multidisciplinary treatment. Pain Pract. 2020;20(5):471–479. doi:10.1111/papr.12873
18. Cetin B, Sunbul EA, Toktas H, Karaca M, Ulutas O, Gulec H. Comparison of sleep structure in patients with fibromyalgia and healthy controls. Sleep Breath. 2020;24(4):1591–1598. doi:10.1007/s11325-020-02036-x
19. Choy EH. The role of sleep in pain and fibromyalgia. Nat Rev Rheumatol. 2015;11(9):513–520. doi:10.1038/nrrheum.2015.56
20. Lee NK, Jeon SW, Heo YW, et al. Sleep disturbance in patients with lumbar spinal stenosis: association with disability and quality of life. Clin Spine Surg. 2020;33(4):E185–E190. doi:10.1097/BSD.0000000000000944
21. Marty M, Rozenberg S, Duplan B, et al. Quality of sleep in patients with chronic low back pain: a case-control study. Eur Spine J. 2008;17(6):839–844. doi:10.1007/s00586-008-0660-7
22. Facchin F, Buggio L, Roncella E, et al. Sleep disturbances, fatigue and psychological health in women with endometriosis: a matched pair case-control study. Reprod Biomed Online. 2021;43(6):1027–1034. doi:10.1016/j.rbmo.2021.08.011
23. Zargar A, Gooraji SA, Keshavarzi B, Haji Aghamohammadi AA. Effect of irritable bowel syndrome on sleep quality and quality of life of inflammatory bowel disease in clinical remission. Int J Prev Med. 2019;10:10. doi:10.4103/ijpvm.IJPVM_364_17
24. Xiao L, Tang YL, Smith AK, et al. Nocturnal sleep architecture disturbances in early methadone treatment patients. Psychiatry Res. 2010;179(1):91–95. doi:10.1016/j.psychres.2009.02.003
25. Teichtahl H, Prodromidis A, Miller B, Cherry G, Kronborg I. Sleep-disordered breathing in stable methadone programme patients: a pilot study. Addiction. 2001;96(3):395–403. doi:10.1046/j.1360-0443.2001.9633954.x
26. Shaw IR, Lavigne G, Mayer P, Choiniere M. Acute intravenous administration of morphine perturbs sleep architecture in healthy pain-free young adults: a preliminary study. Sleep. 2005;28(6):677–682. doi:10.1093/sleep/28.6.677
27. Dimsdale JE, Norman D, DeJardin D, Wallace MS. The effect of opioids on sleep architecture. J Clin Sleep Med. 2007;3(1):33–36.
28. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. doi:10.1016/0304-3959(83)90126-4
29. Buysse DJ, Reynolds CF, Monk TH, Hoch CC, Yeager AL, Kupfer DJ. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep. 1991;14(4):331–338.
30. Harrison L, Wilson S, Heron J, Stannard C, Munafo MR. Exploring the associations shared by mood, pain-related attention and pain outcomes related to sleep disturbance in a chronic pain sample. Psychol Health. 2016;31(5):565–577. doi:10.1080/08870446.2015.1124106
31. Naughton F, Ashworth P, Skevington SM. Does sleep quality predict pain-related disability in chronic pain patients? The mediating roles of depression and pain severity. Pain. 2007;127(3):243–252. doi:10.1016/j.pain.2006.08.019
32. Covarrubias-Gomez A, Mendoza-Reyes JJ. Evaluation of sleep quality in subjects with chronic nononcologic pain. J Pain Palliat Care Pharmacother. 2013;27(3):220–224. doi:10.3109/15360288.2013.816405
33. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
34. Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA. Epidemiology of low back pain in adults. Neuromodulation. 2014;17(Suppl 2):3–10. doi:10.1111/ner.12018
35. Manfredini D, Guarda-Nardini L, Winocur E, Piccotti F, Ahlberg J, Lobbezoo F. Research diagnostic criteria for temporomandibular disorders: a systematic review of axis I epidemiologic findings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(4):453–462. doi:10.1016/j.tripleo.2011.04.021
36. Marin R, Cyhan T, Miklos W. Sleep disturbance in patients with chronic low back pain. Am J Phys Med Rehabil. 2006;85(5):430–435. doi:10.1097/01.phm.0000214259.06380.79
37. Bintang AKS, Aulina S, Aulina S, Aulina S, Aulina S. Relationship between sleep quality and pain intensity in patients with chronic low back pain. Med Clin Pract. 2021;4:100208. doi:10.1016/j.mcpsp.2021.100208
38. Lavigne GJ, Sessle BJ. The neurobiology of orofacial pain and sleep and their interactions. J Dent Res. 2016;95(10):1109–1116. doi:10.1177/0022034516648264
39. Roehrs T, Hyde M, Blaisdell B, Greenwald M, Roth T. Sleep loss and REM sleep loss are hyperalgesic. Sleep. 2006;29(2):145–151. doi:10.1093/sleep/29.2.145
40. Marshansky S, Mayer P, Rizzo D, Baltzan M, Denis R, Lavigne GJ. Sleep, chronic pain, and opioid risk for apnea. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):234–244. doi:10.1016/j.pnpbp.2017.07.014
41. Chung F, Wong J, Bellingham G, et al. Predictive factors for sleep apnoea in patients on opioids for chronic pain. BMJ Open Respir Res. 2019;6(1):e000523. doi:10.1136/bmjresp-2019-000523
42. Nagappa M, Weingarten TN, Montandon G, Sprung J, Chung F. Opioids, respiratory depression, and sleep-disordered breathing. Best Pract Res Clin Anaesthesiol. 2017;31(4):469–485. doi:10.1016/j.bpa.2017.05.004
43. Jungquist CR, Flannery M, Perlis ML, Grace JT. Relationship of chronic pain and opioid use with respiratory disturbance during sleep. Pain Manag Nurs. 2012;13(2):70–79. doi:10.1016/j.pmn.2010.04.003
44. Higgins C, Smith BH, Matthews K. Evidence of opioid-induced hyperalgesia in clinical populations after chronic opioid exposure: a systematic review and meta-analysis. Br J Anaesth. 2019;122(6):e114–e126. doi:10.1016/j.bja.2018.09.019
45. Baldassarri SR, Beitel M, Zinchuk A, et al. Correlates of sleep quality and excessive daytime sleepiness in people with opioid use disorder receiving methadone treatment. Sleep Breath. 2020;24(4):1729–1737. doi:10.1007/s11325-020-02123-z
46. Brudern J, Hallensleben N, Holler I, et al. Sleep disturbances predict active suicidal ideation the next day: an ecological momentary assessment study. BMC Psychiatry. 2022;22(1):65. doi:10.1186/s12888-022-03716-6
47. Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113–130. doi:10.1016/j.jpain.2008.10.008
48. Staner L. Comorbidity of insomnia and depression. Sleep Med Rev. 2010;14(1):35–46.
49. Bastien CH, Fortier-Brochu E, Rioux I, LeBlanc M, Daley M, Morin CM. Cognitive performance and sleep quality in the elderly suffering from chronic insomnia. Relationship between objective and subjective measures. J Psychosom Res. 2003;54(1):39–49. doi:10.1016/S0022-3999(02)00544-5
50. Beland SG, Preville M, Dubois MF, et al. Benzodiazepine use and quality of sleep in the community-dwelling elderly population. Aging Ment Health. 2010;14(7):843–850. doi:10.1080/13607861003781833
51. Beland SG, Preville M, Dubois MF, et al. The association between length of benzodiazepine use and sleep quality in older population. Int J Geriatr Psychiatry. 2011;26(9):908–915. doi:10.1002/gps.2623
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cohort Description: Preventing an Opioid Epidemic in Norway – Focusing on Treatment of Chronic Pain (POINT) – A National Registry-Based Study
Hamina A, Odsbu I, Borchgrevink PC, Chen LC, Clausen T, Espnes KA, Gjesdal K, Handal M, Hartikainen S, Hjellvik V, Holter MTS, Høibø T, Kurita GP, Langaas HC, Lid TG, Nøst TH, Sjøgren P, Skurtveit S
Clinical Epidemiology 2022, 14:1477-1486
Published Date: 8 December 2022
Tapentadol: A Review of Experimental Pharmacology Studies, Clinical Trials, and Recent Findings
Alshehri FS
Drug Design, Development and Therapy 2023, 17:851-861
Published Date: 21 March 2023
Engagement in Integrative and Nonpharmacologic Pain Management Modalities Among Adults with Chronic Pain: Analysis of the 2019 National Health Interview Survey
Rodgers-Melnick SN, Trager RJ, Love TE, Dusek JA
Journal of Pain Research 2024, 17:253-264
Published Date: 16 January 2024
Pharmacological Prescribing and Satisfaction with Pain Treatment Among Non-Hispanic Black Men with Chronic Pain
Oloruntoba O, Bergeron CD, Zhong L, Merianos AL, Sherman LD, Kew CL, Goidel RK, Smith ML
Patient Preference and Adherence 2024, 18:187-195
Published Date: 19 January 2024
Enhanced Recovery After Surgery (ERAS) Protocols in Orthopaedic Surgery: Opioids or Not Opioids?
Grossi P
Journal of Pain Research 2025, 18:1683-1695
Published Date: 28 March 2025