Back to Journals » Psychology Research and Behavior Management » Volume 16
The Relationship Between Fear Avoidance Belief and Threat Learning in Postoperative Patients After Lung Surgery: An Observational Study
Authors Bao L, Peng C, He J, Sun C, Feng L, Luo Y ![]()
Received 10 May 2023
Accepted for publication 10 August 2023
Published 16 August 2023 Volume 2023:16 Pages 3259—3267
DOI https://doi.org/10.2147/PRBM.S420724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Lihong Bao,1,* Chunfen Peng,2,* Jingting He,2 Chengqin Sun,1 Lijuan Feng,1 Yang Luo1
1Department of Thoracic Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Luo; Jingting He, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Email [email protected]; [email protected]
Background: The role of fear-avoidance beliefs (FAB) in patients with chronic pain has been widely confirmed. However, few conclusions have been drawn about its role in postoperative patients.
Objective: To explore the characteristics of FAB in postoperative patients after lung surgery as well as the effect of threat learning on FAB.
Methods: Between May and September 2022, this study recruited 150 participants who had undergone thoracoscopic surgery. Variables such as age, gender, education, chronic pain, fear of pain, surgery method, pain intensity, FAB, cough, ambulation and threat learning were collected and subjected to correlation analysis and stepwise regression.
Results: The correlation analysis revealed that FAB was associated with age (r = − 0.183, p < 0.05), gender (r = − 0.256, p < 0.01), and preoperative FOP-9 (r = 0.400, p < 0.01). Postoperative variables such as pain intensity (r = 0.574, p < 0.01), initiation day of ambulation (r = 0.648, p < 0.01), total numbers of ambulation (r = − 0.665, p < 0.01), and cough performance (r = − 0.688, p < 0.01) were correlated with FAB. Furthermore, FAB was highly correlated with indicators of threat learning: direct (r = 0.556, p < 0.01), observation (r = 0.655, p < 0.01), and instruction (r = 0.671, p < 0.01). The highest variance explanation model of stepwise regression which explained 52.8% of the variance including instruction (B=1.751; p< 0.01), direct (B=1.245; p< 0.01), observation (B=0.768; p< 0.01), age (B=− 0.085; p< 0.01), and surgery method (B=1.321; p< 0.05).
Conclusion: Patients commonly experience FAB after lung surgery, which can directly affect their recovery behaviors such as ambulation and active coughing. The formation of FAB is influenced by threat learning, which suggests that controlling threat learning is important in preventing postoperative FAB.
Keywords: fear-avoidance, threat learning, fear of pain, postoperative pain, lung surgery
Background
According to global cancer surveillance data,1,2 lung cancer has been the most common type of cancer worldwide for many years in terms of both incidence and mortality rates. Surgical treatment is generally considered the primary treatment option for lung cancer.3 However, surgical treatment can lead to many complications for patients, with pain being one of the most common issues. One study found that among 51 patients who underwent lung surgery, moderate postoperative pain occurred in 36–58% of cases and severe pain occurred in 11–26% of cases; furthermore, 39% of patients experienced more pain than expected.4
Pain is not only an extremely uncomfortable experience but can also lead to a variety of physical and psychological complications such as increased oxygen consumption and pulmonary complications,5 as well as depression, anxiety, sleep disorders, and social disorders.6
Pain also is one of the main factors that affects early ambulation in patients after surgery, which can hinder their rapid recovery.7 Early ambulation is an important nursing intervention that can help prevent postoperative complications and maintain optimal patient outcomes. According to current literature, initiating ambulation early can significantly reduce the risk of postoperative complications, accelerate the recovery of functional walking capacity, positively impact several patient-reported outcomes, and reduce hospital length of stay and care costs.8–10
The definition of pain comprises physical and psychological events.11 However, most recommendations for postoperative pain management12–14 still focus on the patient’s physiological aspects, such as improved surgical procedures and anesthesia, while paying little attention to the impact of the patient’s psychological characteristics on pain perception and behavior. There is still a lot of room for psychological intervention in postoperative pain.
In recent years, the Fear-Avoidance Model was designed to identify and explain why chronic pain problems, and associated disability, develop in members of the population suffering from chronic pain conditions.15 This theoretical model to guide pain research and management, explain how threat learning causes fear of pain (FOP) and ultimately result in pain avoidance behavior when individuals experiences pain.16 When a stimulus (such as pain) is considered a threat, we are primed to adapt our behavior according to that threat, aided by stress response systems.16 As pain is considered an emotionally-salient stressor and can be seen as a threat, this can lead to FOP. This threat learning can occur in multiple ways, including through direct experience, by observing others (eg, via facial expressions), and by instruction.17
When individuals have negative beliefs about pain and its consequences, including catastrophic thoughts, they may experience feelings of FOP, avoid daily activities, and become hypervigilant.18 As a result of this misinterpretation, individuals repeatedly avoid activities that cause pain and are likely to overestimate any future pain from such activities and finally lead to disability.19 This disability is associated with several deleterious consequences including physical deconditioning, diminished muscle mass, increased pulmonary complications (atelectasis and pneumonia), and increased risk of venous thrombosis embolism.9
Although the theory of threat learning has been confirmed to some extent in laboratory and chronic pain patients, fewer conclusions have been drawn in acute pain, especially postoperative patients. However, how fear-avoidance beliefs (FAB) is generated and its impact on patient behavior in postoperative pain patients is still unknown. Therefore, this study aims to explore how threat learning affects pain fear from the perspective of threat learning and ultimately affects patient behavior by taking postoperative patients as samples.
Materials and Methods
Participants
This study is a single-center cross-sectional study of thoracic hospitalized patients at Wuhan Union Hospital (a tertiary hospital) in Wuhan, China. Patients were selected based on the following inclusion criteria: (1) patients were at least 18 years old; (2) they underwent lung surgery; and (3) they did not suffer from or have a history of neurological or psychiatric disorders. Exclusion criteria included: (1) patients who were not fully in the ward within three days after surgery due to transfer to ICU or early discharge; (2) patients who were unable to perform early ambulation due to illness; and (3) patients who exhibited uncooperative behavior. All participants provided written and oral informed consent for this research which was approved by both the institutional ethics board of Wuhan Union Hospital of Tongji Medical College, Huazhong University of Science and Technology (NO. 20200351), and by clinical trial registration (NO. ChiCTR2200056651). The study was supported by general program of Hubei Provincial Natural Science Foundation of China (No. 2021CFB588), but the funder did not play any role in designing, conducting, or reporting this study. All patients received the same intravenous anesthesia strategy after surgery.
Measures
Pain Intensity
On the third day after surgery, we will use the numerical pain rating scale (NRS) to assess average pain intensity in the days following surgery. The NRS is a commonly used method for assessing pain intensity in clinical settings. It is a simple and reliable tool that asks patients to rate their pain on a scale of 0–10, with 0 indicating no pain and 10 indicating the worst possible pain.
Fear-Avoidance Beliefs
On the third day after surgery, we used the Physical Activity subscale of the Fear-Avoidance Beliefs Questionnaire (FABQ-PA) to measure patients’ FAB. The FABQ-PA is a self-reported questionnaire consisting of the first five questions of the Fear-Avoidance Beliefs Questionnaire.20 A higher score on this scale indicates higher levels of fear avoidance behaviors.
Threat Learning
We designed three questions to measure direct experience (direct), observation experience (observation), and instruction from others (instruction) regarding threat learning. On the third day after surgery, patients were asked to rate their postoperative experience on a 6-point Likert scale ranging from strongly disagree (0) to strongly agree (5) with the following statements: a) I experienced unbearable pain when I tried to get out of bed after surgery; b) I have often observed that getting out of bed after surgery can be painful; c) others often advise me to rest to avoid pain.
Cough Performance
Active coughing is an essential rehabilitation measure after lung surgery.21 However, this movement can cause pain and reflect the patient’s pain response. Each patient was asked to actively cough after surgery and informed of its importance in postoperative recovery. On the third day after surgery, patients were instructed to cough, and their response was observed within the next 5 seconds after sitting up. The semiquantitative cough strength score (SCSS) was used to evaluate the strength of the cough. The SCSS is graded from 0 to 5 and is a subjective evaluation tool used to evaluate patients’ cough ability.22 In this study the cough was then evaluated as either strong (SCSS ≥3) or weak (SCSS <3), or if the patient refused to perform the action due to pain.
Ambulation Performance
All patients were advised to begin ambulating at least once a day starting from the day after surgery and informed of the benefits of postoperative ambulation. However, no emphasis was placed on the duration or times of ambulation. In this study, ambulation was defined as the voluntary act of upright walking outside of the ward or bed unit, excluding activities that require leaving the bed such as going to the bathroom or for check-ups. On the third postoperative day, we investigated the initiation day of ambulation (ie, the first day of ambulation) and the total number of ambulations (ie, the number of times ambulated within three days).
Sample Size
In multivariate statistics, it is generally recommended that the sample size be greater than 10 events per variable.23 In our study, the regression analysis included no more than 13 observational variables. Therefore, the sample size should be at least 130 people.
Statistics
The analyses were performed using SPSS version 25.0 for Windows (Chicago, IL, USA). All participants who provided data were included in the analysis. Descriptive data were presented as counts and percentages for categorical data and as means and standard deviations or medians and interquartile ranges for continuous normally distributed data or data with skewed distribution. Correlations between study variables were analyzed using Spearman correlation analyses. Stepwise multiple linear regression was used to predict or estimate the relationship between variables. The confidence interval (CI) level was set at 95%, and that of the tests was set at 5%. All p-values were two-sided.
Results
Participants
Between May and September 2022, 176 patients met the inclusion criteria. Of these, 26 patients were excluded from the final sample: 12 due to transfer to the ICU after surgery, 9 due to unstable vitals that prevented them from getting out of bed, 4 due to uncooperative behavior, and 1 due to early discharge. Finally, we included 150 participants in our analysis. Baseline characteristics are listed in Table 1.
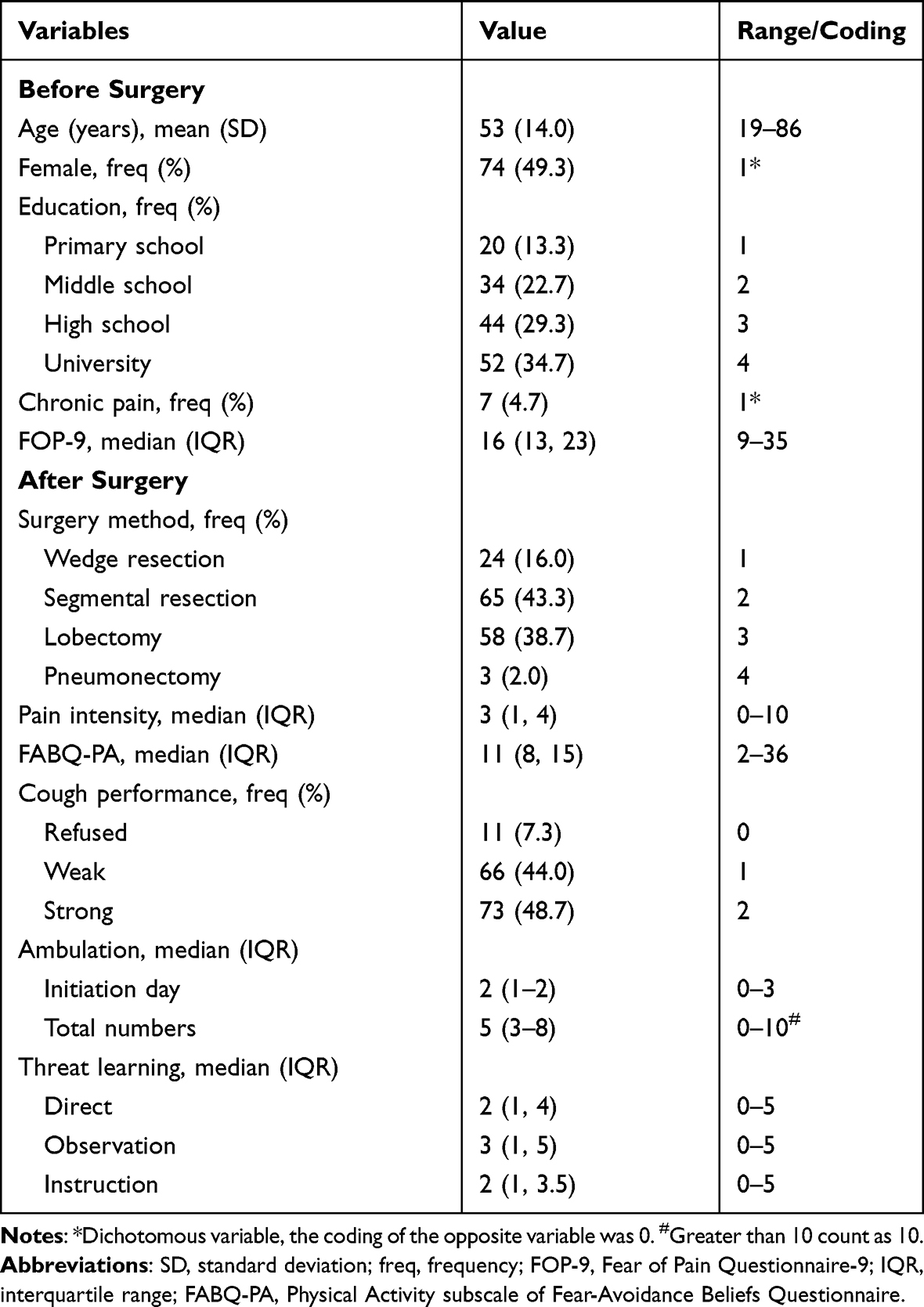 |
Table 1 Baseline Characteristics of Participants (n=150) |
Correlation
Table 2 presents the correlations between the variables. The correlation analysis revealed that FABQ-PA was associated with age (r = −0.183, p < 0.05), gender (r = −0.256, p < 0.01), and preoperative FOP-9 (r = 0.400, p < 0.01). This suggests that younger age, female, and high preoperative FOP may be risk factors for postoperative FAB. Postoperative variables such as pain intensity (r = 0.574, p < 0.01), initiation day of ambulation (r = 0.648, p < 0.01), total numbers of ambulation (r = −0.665, p < 0.01), and cough performance (r = −0.688, p < 0.01) were correlated with FABQ-PA which indicates that postoperative FAB may affect higher pain reporting and negative pain avoidance behavior after surgery. Furthermore, FABQ-PA was highly correlated with indicators of threat learning: direct (r = 0.556, p < 0.01), observation (r = 0.655, p < 0.01), and instruction (r = 0.671, p < 0.01). This suggests that FAB formation may be related to threat learning.
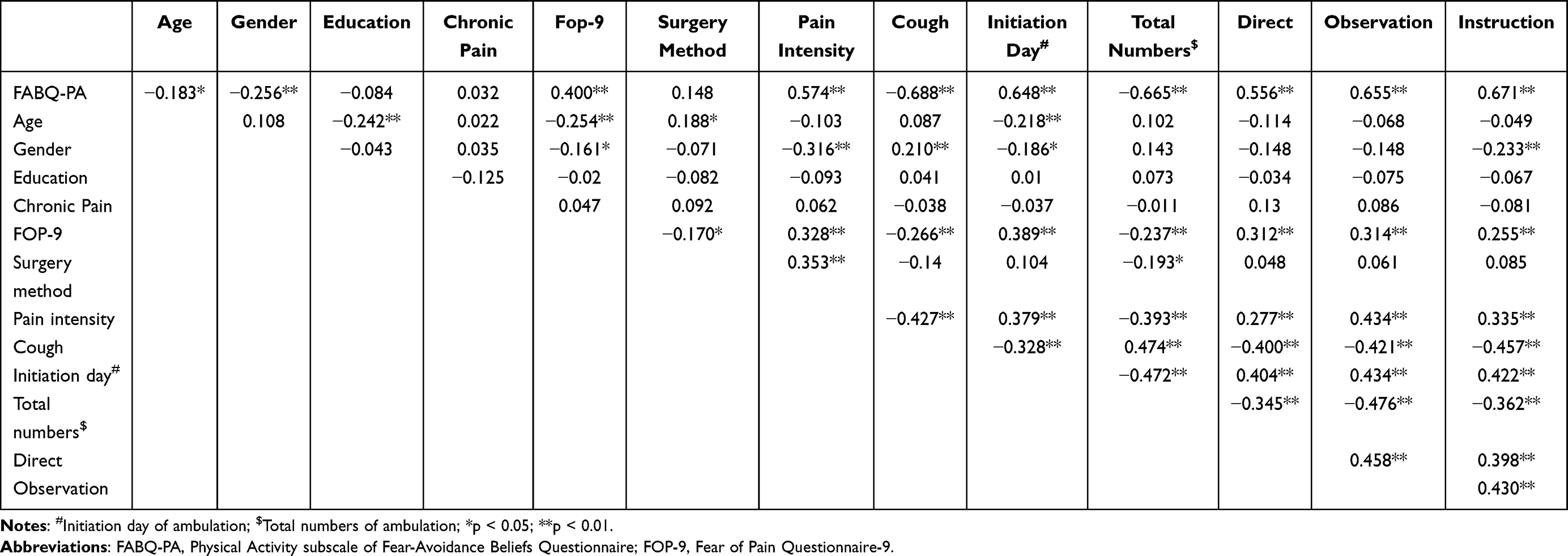 |
Table 2 Correlation Coefficients Between Variables (n=150) |
Regression
The results of the stepwise multiple linear regression are displayed in Table 3. Because FABQ-PA may affect ambulation performance, cough performance, and pain intensity, we excluded these variables from the selection of input variables in the stepwise regression process. We set FABQ-PA as the dependent variable and age, gender, education, chronic pain, FOP-9, surgery method and threat learning (direct, observational and instruction) as independent variables. Five models were statistically significant (p<0.05), with the highest variance explanation including instruction (B=1.751; p<0.01), direct (B=1.245; p<0.01), observation (B=0.768; p<0.01), age (B=−0.085; p<0.01), and surgery method (B=1.321; p<0.05). These independent variables explained 52.8% of the variance in the model’s results. Combining the results in Table 2, it can be inferred that age and threat learning are independent risk factors for FAB.
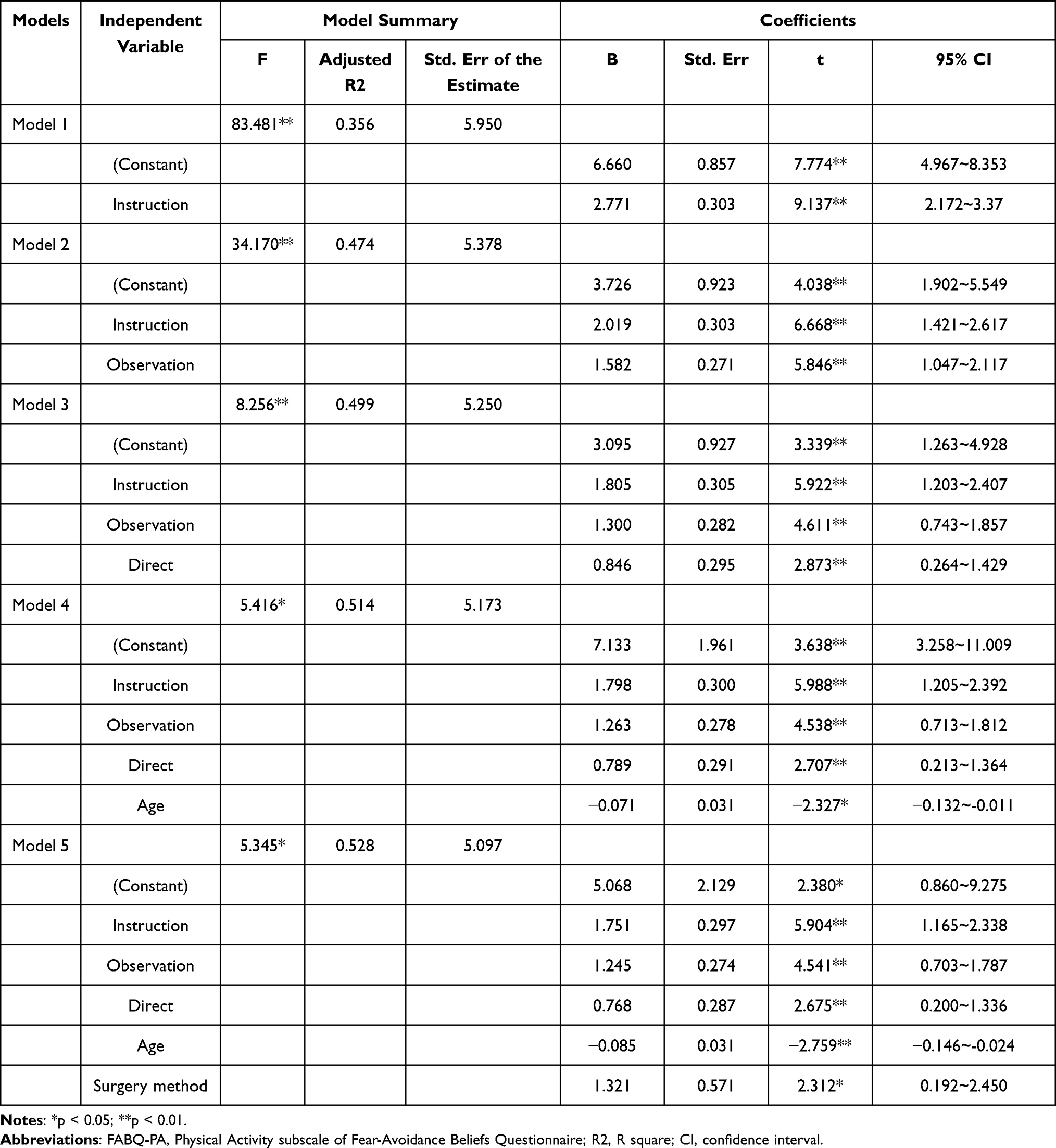 |
Table 3 Stepwise Regression Analysis of FABQ-PA as the Dependent Variable (n=150) |
Discussion
The fear-avoidance model is a widely used theoretical framework that explains the psychological factors involved in pain experience and the development of chronic pain and disability. Negative beliefs, such as FAB about pain or negative illness information, may lead to an exaggerated negative mental response where the worst possible outcome is imagined.24 FAB have been shown to play an important role in the occurrence and maintenance of chronic pain.24 This study showed that FAB about physical activity also appeared in post-operative patients, with a median of 11 (full score is 36).
The risk factors for FAB include age, gender, employment status, anxiety, quality of sleep, and health locus of control.25 Our study found that FAB are correlated with gender, age, and trait FOP. These personal factors may predispose individuals to FAB.
FAB represent cognitions and emotions that underpin concerns and fears about physical activities’ potential to produce pain and further harm.26 As a result of these beliefs, individuals repeatedly avoid pain-inducing activities and are likely to overestimate any future pain from such activities.27 Our results also show that patients’ FAB are highly correlated with delayed activity and inefficient coughing. This may be because FAB lead patients to avoid behaviors that cause pain. However, these activities are important for rapid recovery in patients who underwent modern lung surgery.9,14 Therefore, it is necessary to intervene in postoperative patients’ fear-avoidance behavior.
Threat learning explains how FAB are learned and reinforced. It is a behavioral paradigm that has been successfully utilized to define the mechanisms underlying threat (fear) memory formation.28 Threat learning can occur through direct experience, observation of others (eg, via facial expressions), and instruction.16 Direct experience refers to Pavlovian threat conditioning which is based on the formation of predictive associations between personally experienced stimuli.29 Observational learning occurs through the observation of the emotional responses of others.30 Instructional learning occurs through verbal instruction.29 Our research shows that all three methods are highly correlated with FAB. The results of linear regression showed that instruction from others had the largest absolute value regression coefficient among included independent variables, indicating its importance in generating patients’ fear belief.
The results of our research suggest that threat learning plays an important role in the formation of fear-avoidance beliefs (FAB), which may directly affect positive postoperative recovery behaviors. Interventions on three aspects of threat learning may be a way to promote early postoperative recovery. Firstly, patients can be guided to perform activities (including turning over, coughing and even getting out of bed) in a safe and comfortable environment (such as the use of analgesics) as early as possible (within 4 hours after surgery) by associating activity with safety. Secondly, patients with high FAB scores should not be placed in the same ward because threat learning will reinforce their negative views of activities by observing each other. Instead, it is better to place patients with low FAB and patients with high FAB in the same ward. We believe that patients with high FAB are less likely to be influenced by patients with low FAB, while the latter can be influenced by the former. Thirdly, patients’ and caregivers’ concepts of postoperative pain and recovery behaviors are also important factors leading to the formation of FAB. Therefore, healthcare providers should not only educate patients but also caregivers.
Limitations
The most important limitation of this study is that there may be an interaction between the dependent variable and independent variables. For instance, postoperative pain and FAB. It is unclear whether the post-operative pain caused the FAB or whether the FAB caused the post-operative pain report. Furthermore, it should be noted that this study is of a cross-sectional nature and therefore further investigation is required to establish any causal relationships between the variables.
Conclusion
FAB are common among patients after lung surgery and can directly affect their recovery behaviors such as ambulation and active coughing. Threat learning plays an important role in the formation of FAB. The control of the threat learning path may aid in the reduction of pain FAB.
Data Sharing Statement
The individual deidentified participant data of this study can be requested from the corresponding author ([email protected]) upon reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
3. Montagne F, Guisier F, Venissac N, Baste JM. The role of surgery in lung cancer treatment: present indications and future perspectives-state of the art. Cancers. 2021;13(15). doi:10.3390/cancers13153711
4. Frödin M, Stomberg MW. Pain management after lung surgery. Nurs Rep. 2014;4(1):3225.
5. Julliard W, Krupnick AS. Improving pain after video-assisted thoracoscopic lobectomy-advantages of a wound retractor camera port. J Thorac Dis. 2019;11(2):341–344. doi:10.21037/jtd.2018.11.42
6. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet Lond Engl. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
7. Wainwright TW, Burgess L. Early ambulation and physiotherapy after surgery. In: Ljungqvist O, Francis NK, Urman RD, editors. Enhanced Recovery After Surgery: A Complete Guide to Optimizing Outcomes. Springer International Publishing; 2020:211–218. doi:10.1007/978-3-030-33443-7_23
8. Tazreean R, Nelson G, Twomey R. Early mobilization in enhanced recovery after surgery pathways: current evidence and recent advancements. J Comp Eff Res. 2022;11(2):121–129. doi:10.2217/cer-2021-0258
9. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardio Thorac Surg. 2019;55(1):91–115. doi:10.1093/ejcts/ezy301
10. Talec P, Gaujoux S, Samama CM. Early ambulation and prevention of post-operative thrombo-embolic risk. J Visc Surg. 2016;153(6):S11–S14. doi:10.1016/j.jviscsurg.2016.09.002
11. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
12. Marshall K, McLaughlin K. Pain management in thoracic surgery. Thorac Surg Clin. 2020;30(3):339–346. doi:10.1016/j.thorsurg.2020.03.001
13. Li JW, Ma YS, Xiao LK. Postoperative pain management in total knee arthroplasty. Orthop Surg. 2019;11(5):755–761. doi:10.1111/os.12535
14. Joshi GP, Kehlet H. Postoperative pain management in the era of ERAS: an overview. Best Pract Res Clin Anaesthesiol. 2019;33(3):259–267. doi:10.1016/j.bpa.2019.07.016
15. Vlaeyen JWS, Crombez G, Linton SJ. The fear-avoidance model of pain. PAIN. 2016;157(8):1588–1589.
16. Timmers I, Quaedflieg CWEM, Hsu C, Heathcote LC, Rovnaghi CR, Simons LE. The interaction between stress and chronic pain through the lens of threat learning. Neurosci Biobehav Rev. 2019;107:641–655. doi:10.1016/j.neubiorev.2019.10.007
17. den Hollander M, de Jong JR, Volders S, Goossens MEJB, Smeets RJEM, Vlaeyen JWS. Fear reduction in patients with chronic pain: a learning theory perspective. Expert Rev Neurother. 2010;10(11):1733–1745. doi:10.1586/ern.10.115
18. Atkinson-Jones K, Jacobs K, Lau JYF. Associations between biased threat interpretations, fear and avoidance of pain and pain-linked disability in adolescent chronic pain patients. Eur J Pain Lond Engl. 2021;25(5):1031–1040. doi:10.1002/ejp.1724
19. van Vliet CM, Meulders A, Vancleef LMG, Vlaeyen JWS. The perceived opportunity to avoid pain paradoxically increases pain-related fear through increased threat appraisals. Ann Behav Med Publ Soc Behav Med. 2021;55(3):216–227. doi:10.1093/abm/kaaa045
20. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–168. doi:10.1016/0304-3959(93)90127-B
21. Lin R, Chen W, Zhu L, Pan X. Comparison of postoperative cough-related quality of life and recovery between sublobectomy and lobectomy for early-stage non-small cell lung cancer patients: a longitudinal study. BMC Pulm Med. 2022;22(1):154. doi:10.1186/s12890-022-01954-8
22. Ibrahim AS, Aly MG, Abdel-Rahman KA, Mohamed MA, Mehany MM, Aziz EM. Semi-quantitative cough strength score as a predictor for extubation outcome in traumatic brain injury: a prospective observational study. Neurocrit Care. 2018;29(2):273–279. doi:10.1007/s12028-018-0539-3
23. Tabachnick BG, Fidell LS. Using Multivariate Statistics. Pearson Education; 2013. Available from: https://books.google.com.sg/books?id=ucj1ygAACAAJ.
24. Burgstaller JM, Wertli MM, Steurer J, Kessels AGH, Held U, Gramke HF. The influence of pre- and postoperative fear avoidance beliefs on postoperative pain and disability in patients with lumbar spinal stenosis: analysis of the Lumbar Spinal Outcome Study (LSOS) Data. Spine. 2017;42(7):E425–E432. doi:10.1097/BRS.0000000000001845
25. Agnus Tom A, Rajkumar E, John R, Joshua George A. Determinants of quality of life in individuals with chronic low back pain: a systematic review. Health Psychol Behav Med. 2022;10(1):124–144. doi:10.1080/21642850.2021.2022487
26. Rainville J, Smeets RJEM, Bendix T, Tveito TH, Poiraudeau S, Indahl AJ. Fear-avoidance beliefs and pain avoidance in low back pain--translating research into clinical practice. Spine J off J North Am Spine Soc. 2011;11(9):895–903. doi:10.1016/j.spinee.2011.08.006
27. Wong WS, Lam HMJ, Chen PP, et al. The fear-avoidance model of chronic pain: assessing the role of neuroticism and negative affect in pain catastrophizing using structural equation modeling. Int J Behav Med. 2015;22(1):118–131. doi:10.1007/s12529-014-9413-7
28. Sears RM, Schiff HC, LeDoux JE. Molecular mechanisms of threat learning in the lateral nucleus of the amygdala. Prog Mol Biol Transl Sci. 2014;122:263–304. doi:10.1016/B978-0-12-420170-5.00010-6
29. Lindström B, Golkar A, Jangard S, Tobler PN, Olsson A. Social threat learning transfers to decision making in humans. Proc Natl Acad Sci. 2019;116(10):4732–4737. doi:10.1073/pnas.1810180116
30. Kaźmierowska AM, Szczepanik M, Wypych M, et al. Learning about threat from friends and strangers is equally effective: an fMRI study on observational fear conditioning. NeuroImage. 2022;263:119648. doi:10.1016/j.neuroimage.2022.119648
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Personality and Pain Catastrophizing on Postoperative Analgesia Following Cesarean Section: A Prospective Cohort Study
Ren Y, Guo Y, Tang J, He L, Li M, Huang X, Lu Q, Sun B, Feng H, Liu H, Du J, Li J
Journal of Pain Research 2024, 17:11-19
Published Date: 3 January 2024
A Randomized Controlled Trial of Clinical Hypnosis as an Opioid-Sparing Adjunct Treatment for Pain Relief in Adults Undergoing Major Oncologic Surgery
Rosenbloom BN, Slepian PM, Azam MA, Aternali A, Birnie KA, Curtis K, Thaker S, Ladak S, Waisman A, Clarke H, Katz J, Weinrib AZ
Journal of Pain Research 2024, 17:45-59
Published Date: 4 January 2024
Pain Catastrophizing After Early-Stage Lung Cancer Surgery: The Mediating Effects of Interoceptive Awareness, Negative Attentional Bias, and Social Support
Bian G, Sun X, Chang Q, Liu L, Zhang C
Journal of Pain Research 2026, 19:569494
Published Date: 13 January 2026