Back to Journals » Drug Design, Development and Therapy » Volume 19
Oxycodone versus Sufentanil for Postoperative Recovery in Obese Patients Undergoing Laparoscopic Bariatric Surgery: A Randomized Controlled Trial
Authors Yao X, Wang Z, Zhang Y, Jia W, Sheng X, Zhou Y, Xu C, Jiao H
Received 19 June 2025
Accepted for publication 10 October 2025
Published 17 October 2025 Volume 2025:19 Pages 9387—9397
DOI https://doi.org/10.2147/DDDT.S548173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Xiangyu Yao,1,* Zeyang Wang,2,* Yu Zhang,1,* Wensen Jia,1 Xinfang Sheng,1 Ye Zhou,1 Chun Xu,1 Hao Jiao3
1School of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Anesthesiology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, People’s Republic of China; 3Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Jiao, Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China, Tel +86 13512560960, Email [email protected]
Purpose: Obese patients undergoing bariatric surgery face unique challenges in postoperative pain management and recovery. Due to altered opioid pharmacokinetics and heightened pain sensitivity in this population, optimizing analgesic regimens is crucial. This study compared the impact of oxycodone- vs sufentanil-based analgesic regimens on postoperative recovery quality in obese patients undergoing bariatric surgery.
Methods: Eighty-four obese patients (BMI ≥ 30 kg/m², ASA II–III) undergoing elective laparoscopic bariatric surgery were randomized into oxycodone (n=42) or sufentanil (n=42) groups. Standardized anesthesia included either oxycodone (0.3 mg/kg at induction, 0.1 mg/kg 10 min before surgery completion) or sufentanil (0.3 μg/kg at induction, 0.1 μg/kg 10 min before surgery completion). The primary outcome was the Quality of Recovery-40 (QoR-40) score at 24 h postoperatively. Secondary outcomes included NRS pain scores, rescue analgesia requirements, adverse events (PONV and hypoxemia), sedation scores, and recovery milestones.
Results: Compared to the sufentanil group, the oxycodone group had significantly higher 24-hour QoR-40 scores (median [IQR]: 187.0 [178.8– 190.3] vs 173.0 [164.8– 184.3]; estimated median difference: 11; 95% CI: 6– 17; P< 0.001), with improved physical comfort, emotional status, physical independence, and pain (all P< 0.05). Oxycodone provided superior analgesia: lower NRS pain scores at 0.5, 2, 6, and 24 h postoperatively (all P≤ 0.003), reduced rescue analgesia in PACU (16.7% vs 50%; P=0.001) and on the ward (23.8% vs 64.3%; P< 0.001), and fewer PACU adverse events—PONV (47.6% vs 69.1%; P=0.046), antiemetic use (14.3% vs 35.7%; P=0.023), and hypoxemia (19.1% vs 50%; P=0.003). Recovery milestones (extubation, first flatus, ambulation) occurred earlier in the oxycodone group (all P< 0.05).
Conclusion: Oxycodone significantly enhanced postoperative recovery quality compared with sufentanil in obese patients undergoing laparoscopic bariatric surgery, providing superior analgesia and reducing opioid-related side effects.
Keywords: oxycodone, obesity, bariatric surgery, postoperative analgesia, quality of recovery, ERAS
Introduction
Bariatric surgery remains the most effective long-term treatment for morbid obesity, significantly reducing obesity-related comorbidities and mortality risks.1,2 However, this population presents unique perioperative challenges, particularly in postoperative pain management and early recovery.3,4 Effective analgesia not only alleviates pain but also directly enhances postoperative recovery quality, which encompasses physical comfort, emotional state, physical independence, psychological support, and pain control—factors particularly critical for obese patients prone to complications such as pulmonary dysfunction, nausea, and vomiting.5,6 Enhanced Recovery After Surgery (ERAS) protocols advocate multimodal analgesia to minimize opioid-related risks, including respiratory depression, exacerbation of obstructive sleep apnea, and sedation-induced delayed mobilization.7–9 Thus, careful analgesic selection and dosing in obese patients are essential for improving overall postoperative recovery.
Obesity significantly affects opioid pharmacokinetics and pharmacodynamics.6,10 Highly lipophilic opioids such as sufentanil demonstrate an increased volume of distribution and prolonged elimination half-life in obese patients, potentially leading to postoperative sedation and respiratory compromise.10 Furthermore, alterations in hepatic enzyme activities (such as CYP2D6 and CYP3A4) have been reported, influencing opioid metabolism and potentially reducing analgesic predictability and safety in obese individuals.11,12 Pain perception may also differ in obese patients, with reports indicating heightened sensitivity and lower pain thresholds.13 These pharmacological and physiological differences highlight the necessity for analgesic strategies tailored specifically to obese populations, underscoring the importance of using appropriate assessment tools such as the Quality of Recovery-40 (QoR-40) questionnaire to comprehensively evaluate postoperative outcomes.14
Despite the goal of multimodal analgesia to reduce opioid utilization, opioids remain essential in the analgesic management of bariatric surgery. Among commonly used perioperative opioids, sufentanil offers rapid onset and short duration of action, contributing to its widespread use in bariatric procedures due to its high potency and ease of titration. Nevertheless, its brief analgesic effect may lead to early postoperative pain recurrence. Oxycodone, acting on both µ- and κ-opioid receptors, potentially provides superior visceral analgesia due to κ-receptor agonism, and a longer analgesic duration, possibly bridging the analgesic gap postoperatively.15 Recent studies comparing oxycodone with other opioids have demonstrated superior analgesic efficacy and improved patient satisfaction across various surgical populations;16 however, existing research specifically addressing obese patients undergoing bariatric surgery remains sparse, often limited by small sample sizes or a lack of comprehensive recovery evaluation. Thus, this randomized controlled trial aimed to determine whether oxycodone could enhance postoperative recovery quality compared to sufentanil in obese patients undergoing laparoscopic bariatric surgery.
Methods
Ethics and Study Design
This study was a prospective, double-blind randomized controlled trial conducted at a single tertiary hospital (the Affiliated Hospital of Xuzhou Medical University, China). Institutional ethics committee approval was obtained (no. XYFY2024-KL475-01) on October 18, 2024, and the trial was registered at ClinicalTrials.gov (Registration no: ChiCTR2500095380; Principal investigator: Xiangyu Yao; Date of registration: January 6, 2025). This trial was conducted in strict compliance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines and adhered to the ethical principles established by the Declaration of Helsinki. All enrolled patients provided written informed consent.
Patient Selection
Eligible participants were adults aged 18–60 years, classified as American Society of Anesthesiologists (ASA) physical status II–III, with obesity defined as a body mass index (BMI) ≥30 kg/m², who were scheduled for elective laparoscopic bariatric surgery (including sleeve gastrectomy or sleeve gastrectomy with transit bipartition). Exclusion criteria included severe cardiovascular disease or hepatic/renal dysfunction, history of open abdominal surgery, psychiatric disorders, chronic opioid or alcohol abuse, known allergy to the study drugs, inability or unwillingness to comprehend the scoring scales or refusal to participate, and severe obstructive sleep apnea-hypopnea syndrome (OSAHS).
Randomization and Blinding
Patients were randomized in a 1:1 ratio into either the oxycodone group (Group O) or sufentanil group (Group S) using a computer-generated randomization sequence. Random allocation was concealed using opaque, sealed envelopes opened immediately before anesthesia induction by an anesthesia provider who did not participate in patient care or outcome assessment. This unblinded provider prepared the assigned study drugs (oxycodone or sufentanil) in identical syringes to ensure that the appearance and volumes were indistinguishable. Patients, surgeons, anesthesiologists (except the drug-preparing provider), outcome assessors, and postoperative nursing staff were all blinded to group allocation throughout the study. All surgical procedures were performed by the same surgical team.
Anaesthesia Protocol
All patients underwent a standardized anesthesia protocol, differing only in the opioid administered (oxycodone or sufentanil). Upon entering the operating room, standard monitoring was established, including electrocardiography (ECG), pulse oximetry (SpO2), invasive arterial blood pressure, bispectral index (BIS), and train-of-four (TOF) monitoring. After adequate preoxygenation (FiO2 100% for 3 min), anesthesia induction was performed using intravenous propofol (2 mg/kg), rocuronium bromide (0.9 mg/kg), and dexamethasone (8 mg). Analgesic induction differed between groups: patients in the oxycodone group (Group O) received oxycodone (0.3 mg/kg), whereas the sufentanil group (Group S) received sufentanil (0.3 µg/kg). Five minutes after induction, tracheal intubation was performed.
Mechanical ventilation was initiated with pressure-controlled ventilation–volume guaranteed (PCV-VG) mode, characterized by a tidal volume of 6 to 8 mL/kg, an inspiratory-to-expiratory (I:E) ratio of 1:2, an initial inspired oxygen fraction (FiO2) of 80%, a positive end-expiratory pressure (PEEP) of 5 cm H2O, and an airway pressure limit of < 30 cm H2O. The respiratory rate was adjusted to maintain end-tidal CO2 (PETCO2) between 35 and 45 mm Hg. After intubation, bilateral ultrasound-guided transverse abdominis plane (TAP) blocks (20 mL of 0.375% ropivacaine each side) and rectus sheath blocks (10 mL of 0.375% ropivacaine each side) were performed on all patients.
Anesthesia maintenance consisted of intravenous infusions of propofol and remifentanil combined with inhaled sevoflurane (1–2%). Rocuronium infusion was titrated based on quantitative TOF monitoring to maintain a TOF ratio of 0. Hemodynamic stability was maintained by adjusting the infusion rates of propofol and remifentanil and administering vasoactive drugs as needed, ensuring mean arterial pressure (MAP) fluctuations remained within 30% of baseline values and heart rate (HR) between 45–100 beats/min.17
Approximately 20 minutes before the anticipated end of surgery, sevoflurane and rocuronium infusions were discontinued, and tropisetron (2 mg IV) was administered. Propofol infusion was discontinued at the beginning of skin closure. The skin closure procedure generally takes approximately 10 minutes to complete. Group O received oxycodone (0.1 mg/kg IV) and Group S received sufentanil (0.1 µg/kg IV). At the end of skin closure, remifentanil was discontinued, and neuromuscular blockade was reversed with sugammadex (2 mg/kg IV). The tracheal tube was removed once standard extubation criteria were met, and patients received supplemental oxygen via face mask for at least 5 minutes before transfer to the post-anesthesia care unit (PACU).
Intervention and Postoperative Management
Patients in Group O received intravenous oxycodone (0.3 mg/kg at anesthesia induction, supplemented with 0.1 mg/kg 10 min before surgery completion). Group S received intravenous sufentanil (0.3 μg/kg at induction, supplemented with 0.1 μg/kg 10 min before surgery completion). Upon arrival in the PACU, patients continued to receive supplemental oxygen to maintain SpO2 >94%. Pain intensity was routinely assessed using the Numeric Rating Scale (NRS), ranging from 0 (no pain) to 10 (worst imaginable pain). If moderate-to-severe pain occurred (NRS >4), intravenous fentanyl (100 µg) was administered as rescue analgesia and documented. Postoperative nausea and vomiting (PONV) were treated with intravenous metoclopramide (10 mg) and recorded as necessary. Intravenous infusions of flurbiprofen axetil (routine analgesia) and tramadol (100 mg; rescue for NRS >4 breakthrough pain) were administered in the surgical ward.
All medication dosages, expressed in mg/kg or µg/kg, were calculated based on corrected body weight (CBW), where ideal body weight (IBW) was defined as height (cm) minus 100 for males or height (cm) minus 105 for females, and CBW was calculated as IBW + [0.4 × (actual weight – IBW)].18
Outcome Measures
Primary Outcome
The primary endpoint was the quality of postoperative recovery assessed by the 40-item Quality of Recovery questionnaire (QoR-40) at 24 h after surgery. QoR-40 is a validated instrument widely used to measure patient-reported recovery quality across dimensions including physical comfort, emotional state, physical independence, psychological support, and pain.14,19 Higher QoR-40 scores indicate better recovery quality.
Secondary Outcomes
Secondary endpoints included postoperative pain intensity, functional recovery milestones, sedation, analgesic requirements, and adverse events. Postoperative pain intensity was assessed using the numeric rating scale (NRS, ranging from 0 = no pain to 10 = worst imaginable pain) at 0.5, 2, 6, and 24 h post-surgery. Functional recovery milestones recorded were awakening time (defined as the duration from anesthetic discontinuation to patient responsiveness) and extubation time (interval from anesthetic discontinuation to removal of the endotracheal tube). Additionally, postoperative sedation was evaluated using the Ramsay sedation scale upon arrival in the PACU. The rates of rescue analgesia, PONV, administration of rescue antiemetics, and hypoxemia (defined as SpO2 <90% persisting for more than 10 seconds) were documented. Duration of PACU stay, time to first flatus, time to first ambulation, and length of postoperative hospital stay were also recorded and compared between groups.
All outcome data were collected by an investigator blinded to group allocation. Pain and sedation scores were directly obtained from patient self-reports and nursing assessments, while clinical events and recovery milestones were recorded from medical charts and anesthesia records.
Sample Size Calculation
Sample size estimation was based on a preliminary study demonstrating a standard deviation of 15 for the QoR-40 total score at 24 h postoperatively. A difference of 10 points on the QoR-40 scale represents a clinically meaningful improvement in recovery quality following surgery.20 Assuming an α-error of 0.05 and β-error of 0.20 (power = 80%), the calculated required sample size was 37 patients per group. To account for a potential dropout rate of approximately 10%, we planned to enroll 42 patients in each group, resulting in a total of 84 patients.
Statistical Analysis
All statistical analyses were performed using SPSS software (version 25.0, IBM Corp., Armonk, NY, USA). Data distribution normality was assessed by the Kolmogorov–Smirnov test. Continuous data with normal distribution were presented as mean (standard deviation, SD) and analyzed using independent-samples t-tests. Non-normally distributed continuous data were expressed as median (interquartile range, IQR) and analyzed with Mann–Whitney U-tests. Categorical variables were reported as numbers and percentages (%) and compared using Chi-square tests or Fisher’s exact tests, as appropriate. For repeated measures data (such as postoperative NRS scores at multiple time points), generalized estimating equations (GEE) were applied. A two-tailed p-value < 0.05 was considered statistically significant.
Results
Patient Enrollment and Baseline Characteristics
Between January and September 2025, 100 patients scheduled for elective laparoscopic bariatric surgery were screened. Among these, 84 met eligibility criteria, provided informed consent, and were randomized equally to the oxycodone group (n = 42) or sufentanil group (n = 42). All patients received the assigned interventions, completed the study protocol and were discharged uneventfully, with no instances of loss to follow-up (Figure 1). Baseline demographic and clinical characteristics were comparable between groups with no statistically significant differences (Table 1).
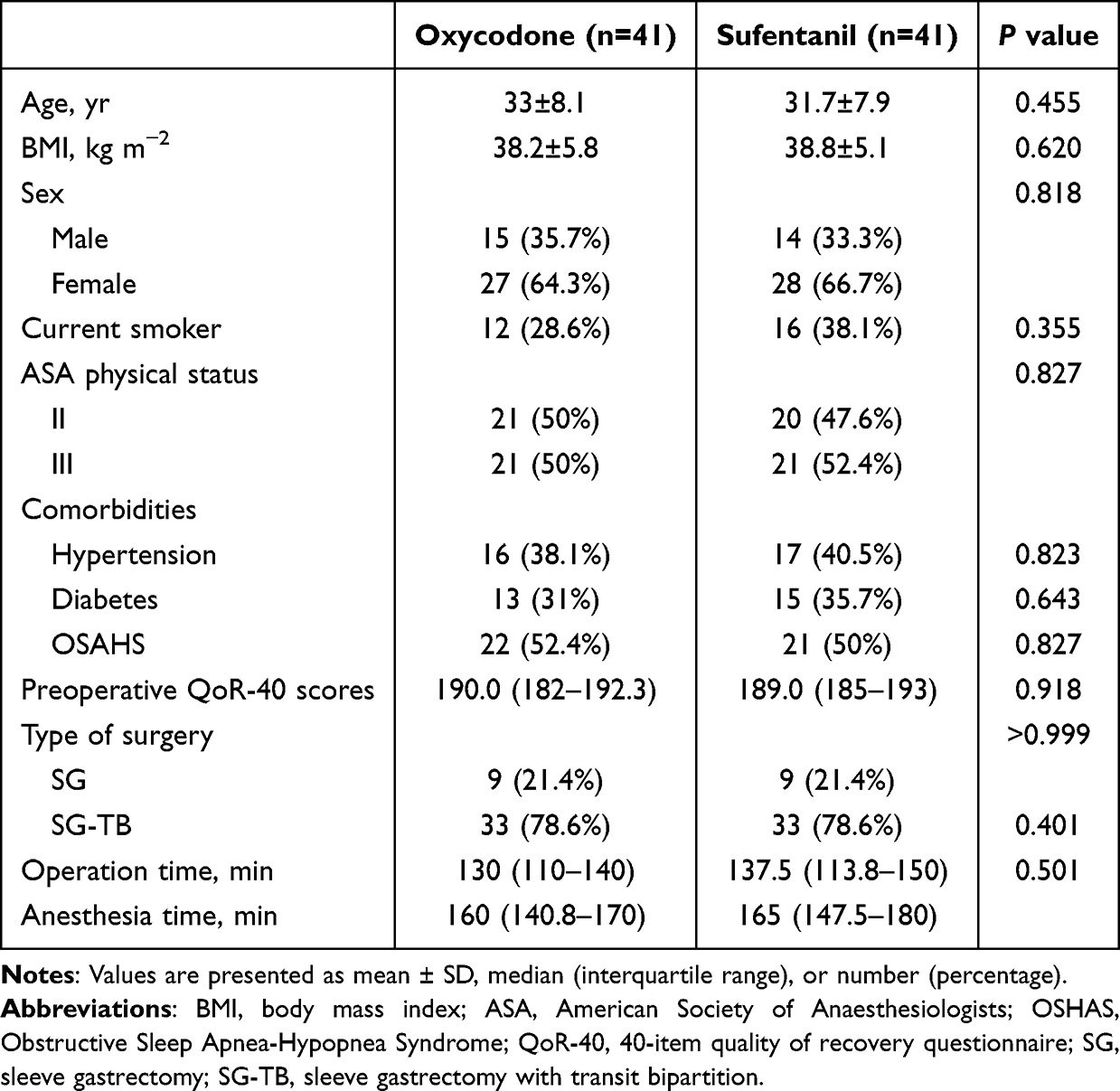 |
Table 1 Patient Characteristics |
 |
Figure 1 Study flow diagram. Abbreviations: BMI, body mass index; OSHAS, Obstructive Sleep Apnea-Hypopnea Syndrome. |
Primary Outcome
The oxycodone group demonstrated significantly higher global QoR-40 scores at 24 hours postoperatively compared to the sufentanil group (median [IQR]: 187.0 [178.8–190.3] vs 173.0 [164.8–184.3]; estimated median difference: 11; 95% CI: 6–17; P<0.001), indicating a clinically and statistically significant improvement in recovery quality. Specifically, patients in the oxycodone group had significantly better scores in physical comfort (P < 0.001), emotional status (P = 0.006), physical independence (P = 0.033), and pain control dimensions (P < 0.001). Psychological support scores showed no significant difference (Table 2).
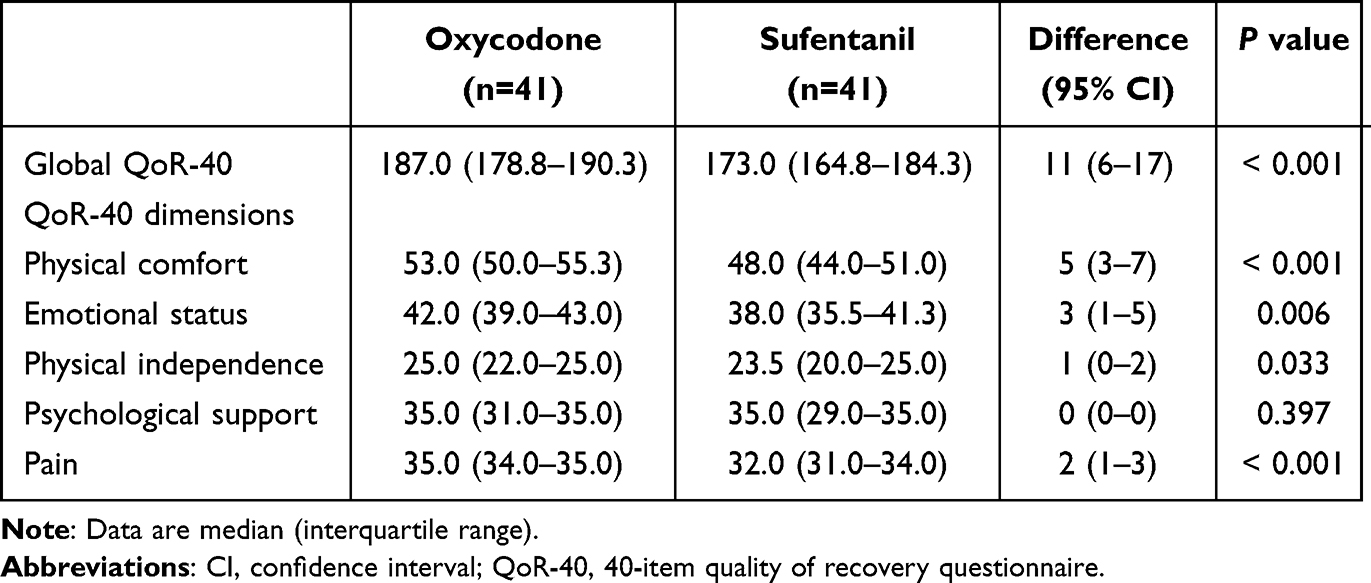 |
Table 2 Postoperative QoR-40 Scores at 24 Hours |
Secondary Outcomes
Patients receiving oxycodone reported lower postoperative NRS pain scores compared with sufentanil at 0.5 h, 2 h, 6 h (all P < 0.001), and 24 h (P = 0.003) after surgery. The rate of rescue analgesia was lower in the oxycodone group than in the sufentanil group both in the PACU (16.7% vs 50%; P = 0.001) and on the ward (23.8% vs 64.3%; P < 0.001). Incidences of PONV (47.6% vs 69.1%; P = 0.046), antiemetic usage (14.3% vs 35.7%; P = 0.023), and hypoxemia events (19.1% vs 50%; P = 0.003) were also lower in the oxycodone group. The oxycodone group demonstrated earlier extubation time (P=0.048), first flatus (P=0.024), and first ambulation (P=0.040) compared to the sufentanil group. Patients in the oxycodone group required lower intraoperative total doses of propofol (P = 0.025) and remifentanil (P < 0.001) compared to those in the sufentanil group (Tables 3 and 4).
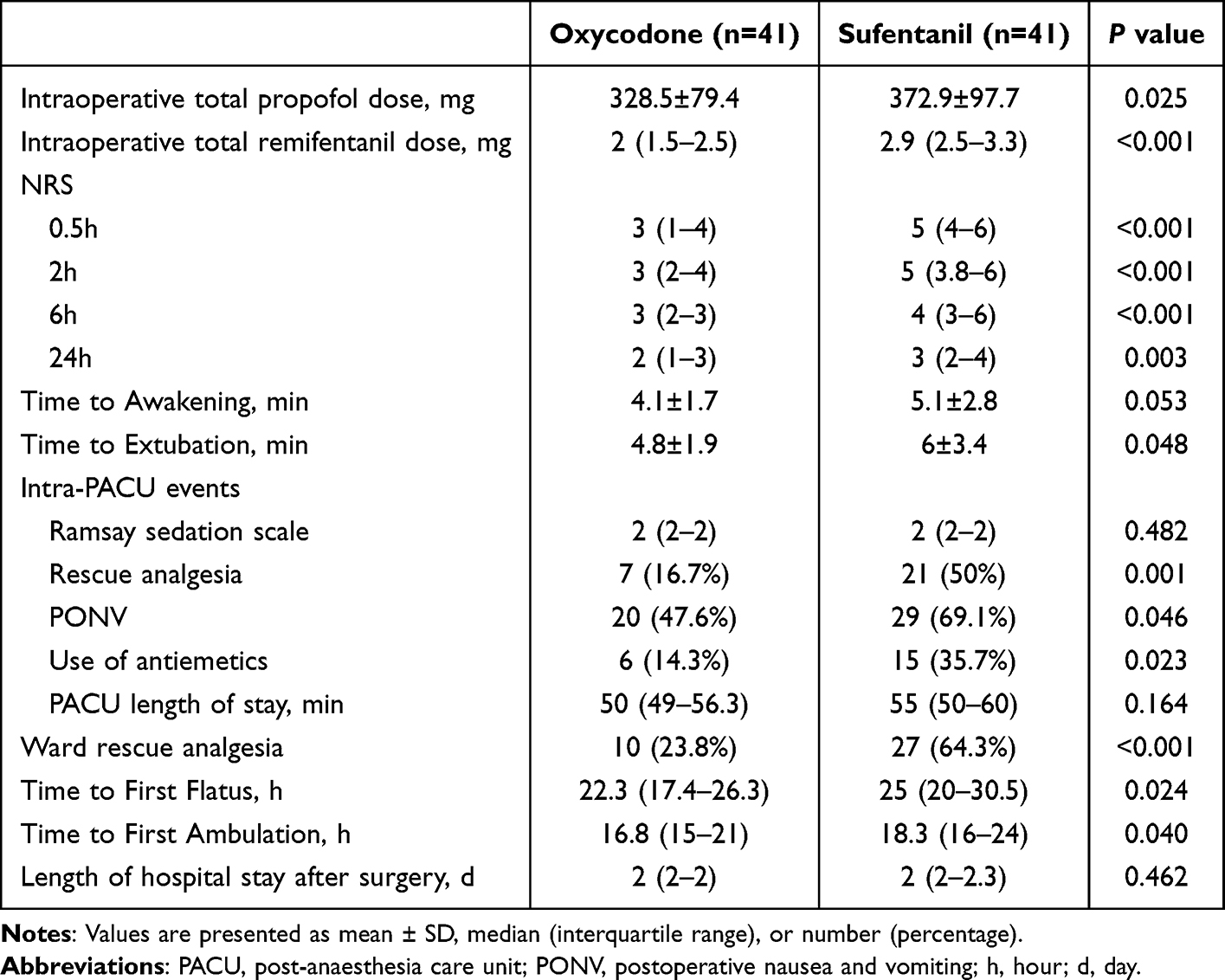 |
Table 3 Postoperative Outcomes |
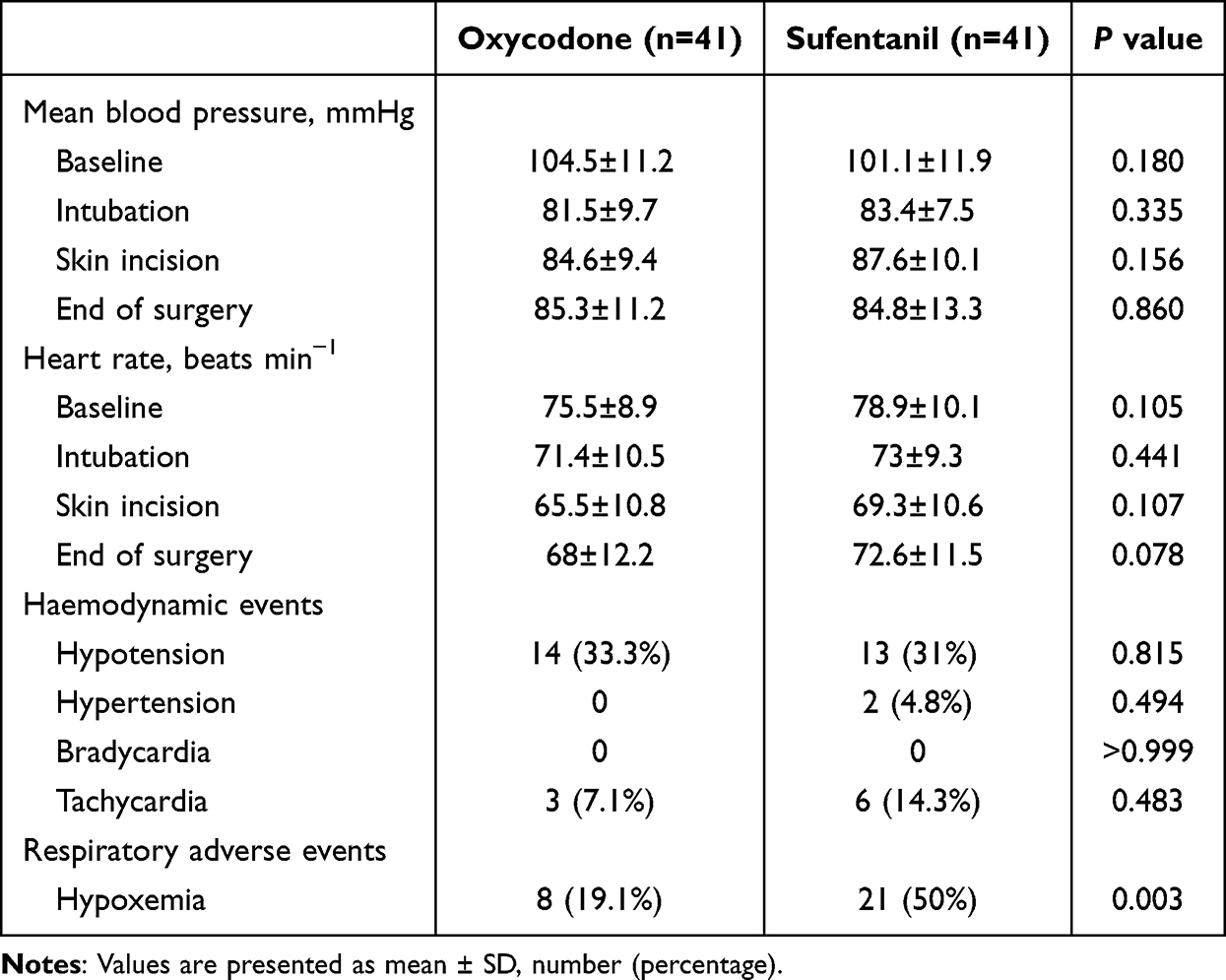 |
Table 4 Hemodynamic Data and Respiratory Adverse Events |
Hemodynamic Outcomes
No significant differences in mean arterial pressure (MAP) or heart rate (HR) were observed between the two groups. (P > 0.05). (Table 4).
Discussion
In this randomized trial, we found that an oxycodone-based analgesic regimen improved postoperative pain control and recovery outcomes compared with sufentanil in obese patients undergoing laparoscopic bariatric surgery. Patients receiving oxycodone exhibited lower pain scores, reduced total opioid consumption, and achieved earlier recovery milestones, such as first ambulation and return of bowel function. These benefits were attained without an increase in opioid-related complications and were reflected in significantly higher QoR-40 scores, representing clinically meaningful improvements in the quality of recovery.
With the increasing adoption of multimodal analgesia and ERAS protocols in bariatric surgery, postoperative complications have decreased. Consequently, the assessment of postoperative recovery quality has shifted its focus toward patient-centered self-evaluation.21 The QoR-40, as a comprehensive and validated instrument, is widely used as an outcome measure in clinical trials.19 In this study, the total QoR-40 score on postoperative day 1 was significantly higher in the oxycodone group compared to the sufentanil group, with notable improvements in physical comfort, emotional state, activity independence, and pain management. This suggests that oxycodone-based multimodal analgesia may enhance early postoperative recovery. A similar trend has been observed in other surgical populations: Hao et al reported higher QoR-15 scores in the oxycodone group after thoracic surgery, and Wang et al found superior early recovery in the oxycodone group following Da Vinci robot-assisted nephrectomy.22,23 These findings support the potential of oxycodone to improve early postoperative recovery. Our study extends this by focusing on a high-risk group—obese patients undergoing bariatric surgery, a population less studied in the existing literature. To our knowledge, this is one of the few studies in this field using QoR-40 as the primary outcome measure, providing a more comprehensive assessment of recovery quality than the QoR-15. Higher QoR-40 scores not only align with the ERAS concept but also indirectly reflect better patient recovery experiences, enhanced overall satisfaction, and increased confidence in their rehabilitation.24
Accumulating evidence indicates κ-opioid receptor activation as a peripherally restricted strategy for visceral pain management, mechanistically mediated through heightened nociceptive thresholds and suppression of afferent pain transmission.25–27 The superior analgesia observed with oxycodone aligns with its pharmacological profile, characterized by dual µ- and κ-opioid receptor agonism, providing robust visceral pain relief. This is particularly relevant in laparoscopic bariatric surgery, where pneumoperitoneum and visceral traction contribute significantly to postoperative discomfort. Consistent with previous studies, oxycodone provided effective relief from postoperative visceral pain, thereby encouraging deep breathing and early ambulation.28–30 By comparison, sufentanil primarily exerts its analgesic effects through μ-opioid receptors in the central nervous system. Its relatively short duration of action, combined with rapid redistribution and elimination, contributes to higher early postoperative pain scores. Therefore, the intraoperative use of sufentanil may require supplemental analgesia to achieve effective postoperative pain control.
The need for higher intraoperative remifentanil and propofol doses in the sufentanil group, as observed in our study, suggests that sufentanil’s shorter duration may lead to compensatory increases in other anesthetics. This could contribute to postoperative hyperalgesia or delayed recovery.31 In contrast, oxycodone, administered at induction and skin closure, provided sustained analgesia and helped reduce the need for additional intraoperative opioids and hypnotics.
Reduced opioid requirements (less rescue analgesia) observed with oxycodone treatment are consistent with prior literature and reinforce the clinical significance of its opioid-sparing effects. Wang et al similarly reported that oxycodone decreased total opioid consumption compared to sufentanil after abdominal surgery.32 This opioid reduction translated into fewer adverse effects and facilitated an earlier return of gastrointestinal function, a critical ERAS milestone.
Additionally, patients in the oxycodone group demonstrated lower rates of postoperative nausea and vomiting (PONV), aligning with previous studies.33,34 This observed advantage may be attributed to reduced supplemental opioid use and oxycodone’s milder emetogenic potential compared to sufentanil.
Opioid-induced respiratory depression represents a primary safety concern. Previous studies observed a numerically lower incidence of respiratory depression with oxycodone compared to sufentanil. However, this difference lacked statistical significance due to limited event numbers, suggesting comparable safety profiles between these opioids.22,30,33,35 However, this statistically non-significant difference may potentially magnify in higher-risk cohorts such as obese populations where postoperative respiratory depression risk is elevated. Our study demonstrated a significantly lower incidence of hypoxemia in the oxycodone group compared to the sufentanil group—a critical advantage for obese patients. Respiratory depression, primarily mediated by μ-opioid receptor activation, was attenuated with oxycodone due to its low lipophilicity (reducing central nervous system penetration) and reduced μ-receptor affinity.28,36,37 Furthermore, oxycodone’s superior visceral analgesia facilitated sustained deep breathing, improving respiratory mechanics and thereby counterbalancing partial respiratory depression effects.
An intriguing finding was the shorter extubation time in the oxycodone group, which is consistent with findings reported in previous studies of other surgical procedures.22,30 This seemingly counterintuitive finding may be associated with the lower total burden of intraoperative sedative and analgesic medications in the oxycodone group, as well as the milder respiratory depression associated with oxycodone. Although both sufentanil and oxycodone exert some sedative effects at the time of extubation, the sedative effects of opioids at conventional doses typically do not impede extubation when adequate neuromuscular blockade reversal with sugammadex is achieved.38 The less pronounced central respiratory depression induced by oxycodone likely constitutes a key contributing factor to its shorter extubation time.
It is also worth comparing our opioid-based approach with the emerging concept of opioid-free anesthesia (OFA) in bariatric surgery. OFA typically uses alternatives like infusions of dexmedetomidine, ketamine, lidocaine, etc., to avoid opioids entirely.39–41 Studies and meta-analyses on OFA in bariatric patients have shown mixed results: some report improved immediate postoperative pain scores and reduced PONV, while others find no difference in overall opioid consumption postoperatively.42,43 In practice, many OFA patients still require opioids for postoperative pain, so total avoidance is challenging.44 Our trial was not an OFA study, but the strong performance of oxycodone raises an argument that a carefully managed opioid-inclusive strategy can be just as effective for recovery.
These findings support the integration of oxycodone into multimodal analgesia protocols within ERAS pathways for bariatric surgery. Although current anesthetic and analgesic approaches for bariatric surgery increasingly favor ultra-short-acting opioids or opioid-free multimodal regimens to minimize the risk of opioid-induced respiratory depression, an optimal analgesic strategy should balance efficacy with safety. Our results demonstrate that the prudent use of potent, long-acting opioids like oxycodone not only effectively alleviates postoperative pain in obese patients but also reduces postoperative opioid requirements and related adverse events. This approach accelerates patient recovery and significantly enhances the early postoperative experience for bariatric surgery patients.
Several limitations warrant acknowledgment. This single-center study had a moderate sample size, limiting generalizability. Patients with severe obstructive sleep apnea or chronic opioid use were excluded, so findings may not extend to these high-risk subgroups. Additionally, our analysis focused on in-hospital recovery outcomes; longer-term endpoints such as chronic pain development or persistent opioid use were not assessed.
Conclusion
In conclusion, oxycodone provided superior visceral pain relief, reduced opioid requirements, enhanced recovery quality metrics, and demonstrated a more favorable safety profile compared with sufentanil in obese patients undergoing laparoscopic bariatric surgery. These findings support using oxycodone as the primary opioid within multimodal analgesic regimens for this high-risk surgical population to enhance recovery outcomes in bariatric surgical patients undergoing ERAS pathways.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding authors on reasonable request.
Acknowledgments
No funding was received for this study. The authors extend their sincere gratitude to all study participants for their valuable contributions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: a review. JAMA. 2020;324(9):879. doi:10.1001/jama.2020.12567
2. Perdomo CM, Cohen RV, Sumithran P, Clément K, Frühbeck G. Contemporary medical, device, and surgical therapies for obesity in adults. Lancet. 2023;401(10382):1116–1130. doi:10.1016/S0140-6736(22)02403-5
3. Bamgbade OA, Oluwole O, Khaw RR. Perioperative analgesia for fast-track laparoscopic bariatric surgery. Obes Surg. 2017;27(7):1828–1834. doi:10.1007/s11695-017-2562-4
4. Iamaroon A, Tangwiwat S, Nivatpumin P, Lertwacha T, Rungmongkolsab P, Pangthipampai P. Risk factors for moderate to severe pain during the first 24 hours after laparoscopic bariatric surgery while receiving intravenous patient-controlled analgesia. Anesthesiol Res Pract. 2019;2019:1–7. doi:10.1155/2019/6593736
5. Bamgbade OA, Oluwole O, Khaw RR. Perioperative antiemetic therapy for fast-track laparoscopic bariatric surgery. Obes Surg. 2018;28(5):1296–1301. doi:10.1007/s11695-017-3009-7
6. Alvarez A, Singh PM, Sinha AC. Postoperative analgesia in morbid obesity. Obes Surg. 2014;24(4):652–659. doi:10.1007/s11695-014-1185-2
7. Thorell A, MacCormick AD, Awad S, et al. Guidelines for perioperative care in bariatric surgery: enhanced Recovery After Surgery (ERAS) society recommendations. World J Surg. 2016;40(9):2065–2083. doi:10.1007/s00268-016-3492-3
8. Riley CL. Anesthesia and enhanced recovery after surgery in bariatric surgery. Anesthesiol Clin. 2022;40(1):119–142. doi:10.1016/j.anclin.2021.11.006
9. Ingrande J, Lemmens HJM. Dose adjustment of anaesthetics in the morbidly obese. Br J Anaesth. 2010;105:i16–i23. doi:10.1093/bja/aeq312
10. Casati A, Putzu M. Anesthesia in the obese patient: pharmacokinetic considerations. J Clin Anesth. 2005;17(2):134–145. doi:10.1016/j.jclinane.2004.01.009
11. Brill MJE, Diepstraten J, van Rongen A, van Kralingen S, van den Anker JN, Knibbe CAJ. Impact of obesity on drug metabolism and elimination in adults and children. Clin Pharmacokinet. 2012;51(5):277–304. doi:10.2165/11599410-000000000-00000
12. Olkkola KT, Kontinen VK, Saari TI, Kalso EA. Does the pharmacology of oxycodone justify its increasing use as an analgesic? Trends Pharmacol Sci. 2013;34(4):206–214. doi:10.1016/j.tips.2013.02.001
13. Okifuji A, Hare B. The association between chronic pain and obesity. J Pain Res. 2015;8:399–408. doi:10.2147/JPR.S55598
14. Myles PS, Weitkamp B, Jones K, Melick J, Hensen S. Validity and reliability of a postoperative quality of recovery score: the QoR-40. Br J Anaesth. 2000;84(1):11–15. doi:10.1093/oxfordjournals.bja.a013366
15. Li Y, Dou Z, Yang L, Wang Q, Ni J, Ma J. Oxycodone versus other opioid analgesics after laparoscopic surgery: a meta-analysis. Eur J Med Res. 2021;26(1):4. doi:10.1186/s40001-020-00463-w
16. Raff M, Belbachir A, El-Tallawy S, et al. Intravenous oxycodone versus other intravenous strong opioids for acute postoperative pain control: a systematic review of randomized controlled trials. Pain Ther. 2019;8(1):19–39. doi:10.1007/s40122-019-0122-4
17. Yang GW, Cheng H, Song XY, et al. Effect of oxycodone-based multimodal analgesia on visceral pain after major laparoscopic gastrointestinal surgery: a randomised, double-blind, controlled trial. Drug Des Devel Ther. 2024;18:1799–1810. doi:10.2147/DDDT.S464518
18. Benevides ML, Ssds O, De Aguilar-Nascimento JE. The combination of haloperidol, dexamethasone, and ondansetron for prevention of postoperative nausea and vomiting in laparoscopic sleeve gastrectomy: a randomized double-blind trial. Obes Surg. 2013;23(9):1389–1396. doi:10.1007/s11695-013-0923-1
19. Gornall BF, Myles PS, Smith CL, et al. Measurement of quality of recovery using the QoR-40: a quantitative systematic review. Br J Anaesth. 2013;111(2):161–169. doi:10.1093/bja/aet014
20. Yao Y, Fu S, Dai S, et al. Impact of ultrasound-guided erector spinae plane block on postoperative quality of recovery in video-assisted thoracic surgery: a prospective, randomized, controlled trial. J Clin Anesth. 2020;63:109783. doi:10.1016/j.jclinane.2020.109783
21. Léger M, Campfort M, Cayla C, Lasocki S, Rineau E. Postoperative quality of recovery measurements as endpoints in comparative anaesthesia studies: a systematic review. Br J Anaesth. 2021;126(6):e210–e212. doi:10.1016/j.bja.2021.03.008
22. Wang T, Wang QB, Hou ZJ, et al. Effect of serratus anterior plane block combined with oxycodone for transition analgesia on preventing emergence agitation after video-assisted thoracoscopic surgery: a randomized controlled trial. Sci Rep. 2024;14(1):30016. doi:10.1038/s41598-024-81801-4
23. Wang H, Qiu Y, Zheng Q, Chen Y, Ma L. Application of oxycodone in anesthesia induction and overall management of Da Vinci robot-assisted nephrectomy: a randomized controlled trial. Medicine. 2022;101(32):e29893. doi:10.1097/MD.0000000000029893
24. Hao C, Xu H, Du J, et al. Impact of opioid-free anesthesia on postoperative quality of recovery in patients after laparoscopic cholecystectomy-a randomized controlled trial. Drug Des Devel Ther. 2023;17:3539–3547. doi:10.2147/DDDT.S439674
25. Staahl C, Christrup LL, Andersen SD, Arendt-Nielsen L, Drewes AM. A comparative study of oxycodone and morphine in a multi-modal, tissue-differentiated experimental pain model. Pain. 2006;123(1):28–36. doi:10.1016/j.pain.2006.02.006
26. Rivière PJM. Peripheral kappa-opioid agonists for visceral pain. Br J Pharmacol. 2004;141(8):1331–1334. doi:10.1038/sj.bjp.0705763
27. Arendt-Nielsen L, Olesen AE, Staahl C, et al. Analgesic efficacy of peripheral kappa-opioid receptor agonist CR665 compared to oxycodone in a multi-modal, multi-tissue experimental human pain model: selective effect on visceral pain. Anesthesiology. 2009;111(3):616–624. doi:10.1097/ALN.0b013e3181af6356
28. An Y, Zhao L, Wang T, et al. Preemptive oxycodone is superior to equal dose of sufentanil to reduce visceral pain and inflammatory markers after surgery: a randomized controlled trail. BMC Anesthesiol. 2019;19(1):96. doi:10.1186/s12871-019-0775-x
29. Lin C, Xu Z, XinLiang W, Wang X, Wang X. A randomized controlled trial to compare the effect of oxycodone and sufentanil on postoperative analgesia and immune function for laparoscopic resection of colorectal cancer. BMC Anesthesiol. 2025;25(1):1–8. doi:10.1186/s12871-025-02922-5
30. Dang SJ, Li RL, Wang J, et al. Oxycodone vs sufentanil in patient-controlled intravenous analgesia after gynecological tumor operation: a randomized double-blind clinical trial. J Pain Res. 2020;13:937–946. doi:10.2147/JPR.S236933
31. Fletcher D, Martinez V. Opioid-induced hyperalgesia in patients after surgery: a systematic review and a meta-analysis. Br J Anaesth. 2014;112(6):991–1004. doi:10.1093/bja/aeu137
32. Wang N, Zhou H, Song X, Wang J. Comparison of oxycodone and sufentanil for patient-controlled intravenous analgesia after laparoscopic radical gastrectomy: a randomized double-blind clinical trial. Anesth Essays Res. 2016;10(3):557–560. doi:10.4103/0259-1162.186603
33. Feng X, Yang P, Liao Z, Zhou R, Chen L, Ye L. Comparison of oxycodone and sufentanil in patient-controlled intravenous analgesia for postoperative patients: a meta-analysis of randomized controlled trials. Chin Med J (Engl). 2023;136(1):45–52. doi:10.1097/CM9.0000000000002259
34. Tao B, Liu K, Wang D, Ding M, Zhao P. Effect of intravenous oxycodone versus sufentanil on the incidence of postoperative nausea and vomiting in patients undergoing gynecological laparoscopic surgery. J Clin Pharmacol. 2019;59(8):1144–1150. doi:10.1002/jcph.1408
35. Zhang J, Tu Q, Gan J, et al. Preemptive anti-stress response effects of oxycodone versus sufentanil for patients undergoing cardiac valve replacement-a randomized controlled trial. Clin Pharmacol Drug Dev. 2020;9(3):321–329. doi:10.1002/cpdd.764
36. Pöyhiä R, Hynynen M, Seppälä T, Roine RO, Verkkala K, Olkkola KT. Pharmacodynamics and pharmacokinetics of high-dose oxycodone infusion during and after coronary artery bypass grafting. J Cardiothorac Vasc Anesth. 2004;18(6):748–754. doi:10.1053/j.jvca.2004.08.013
37. nan YZ, Juan XY, Wei LD, et al. Comparison of oxycodone hydrochloride and flurbiprofen axetil on analgesia in mechanically ventilated patients with respiratory failure in a multicenter study. Sci Rep. 2025;15(1):5012. doi:10.1038/s41598-025-85119-7
38. Sun Y, Wu Z, Wang Q, Chen R, Sun S, Lin Y. Sugammadex, the guardian of deep muscle relaxation during conventional and robot-assisted laparoscopic surgery: a narrative review. Drug Des Devel Ther. 2021;15:3893–3901. doi:10.2147/DDDT.S328682
39. Hung KC, Wu SC, Chang PC, et al. Impact of Intraoperative ketamine on postoperative analgesic requirement following bariatric surgery: a meta-analysis of randomized controlled trials. Obes Surg. 2021;31(12):5446–5457. doi:10.1007/s11695-021-05753-8
40. Hung KC, Chang YJ, Chen IW, Chang YP, Chiu SF, Sun CK. Efficacy of intraoperative intravenous lidocaine for postoperative analgesia following bariatric surgery: a meta-analysis of randomized controlled studies. Surg Obes Relat Dis off J Am Soc Bariatr Surg. 2022;18(1):135–147. doi:10.1016/j.soard.2021.08.014
41. Beloeil H, Garot M, Lebuffe G, et al. Balanced opioid-free anesthesia with dexmedetomidine versus balanced anesthesia with remifentanil for major or intermediate noncardiac surgery: the Postoperative and Opioid-free Anesthesia (POFA) randomized clinical trial. Anesthesiology. 2021;134(4):541–551. doi:10.1097/ALN.0000000000003725
42. Hung KC, Chiu CC, Hsu CW, et al. Impact of opioid-free anesthesia on analgesia and recovery following bariatric surgery: a meta-analysis of randomized controlled studies. Obes Surg. 2022;32(9):3113–3124. doi:10.1007/s11695-022-06213-7
43. Berlier J, Carabalona JF, Tête H, et al. Effects of opioid-free anesthesia on postoperative morphine consumption after bariatric surgery. J Clin Anesth. 2022;81:110906. doi:10.1016/j.jclinane.2022.110906
44. Campbell S, Chin R, Liu WM, Siddiqui U, Kastanias P, Chin KJ. Postoperative pain trajectory and opioid requirements after laparoscopic bariatric surgery: a single-centre historical cohort study. Can J Anesth Can Anesth. 2024;71(11):1505–1517. doi:10.1007/s12630-024-02795-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Retrospective Evaluation of Pregnancy Outcomes Following Bariatric Surgery: A Single-Center Experience
Wang X, Liu J, He A, Dong Z, Chen X, Yu S, Gao L, Wang H, Chen W, Hu R, Jiang S, Wang J, Chen Y, Wang C, Yang W, Li R
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3669-3678
Published Date: 25 November 2022
An Assessment of the Effect of Bariatric Surgery on Cardiovascular Disease Risk in the Chinese Population Using Multiple Cardiovascular Risk Models
Xu G, Wang Z, Yu C, Amin B, Du D, Li T, Chen G, Wang L, Li Z, Chen W, Tian C, Wuyun Q, Sang Q, Shang M, Lian D, Zhang N
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1029-1042
Published Date: 12 April 2023
Bariatric Surgery and Gut-Brain-Axis Driven Alterations in Cognition and Inflammation
Custers E, Franco A, Kiliaan AJ
Journal of Inflammation Research 2023, 16:5495-5514
Published Date: 22 November 2023
Comparing Lifestyle and Behavior of Post-Bariatric Surgery and Participants with Obesity: A Community-Based Cross-Sectional Study
Althumiri NA, BinDhim NF, Aldabaeab AE, AlMousa N, Aljabbary RA, Alumran A
Diabetes, Metabolic Syndrome and Obesity 2024, 17:31-44
Published Date: 3 January 2024
Cost-Utility Analysis of Metabolic Bariatric Surgery for Individuals with Obesity in Saudi Arabia
Nagi MA, Turongkaravee S, Almalki ZS, Thavorncharoensap M, Sangroongruangsri S, Chaikledkaew U, Alqahtani AM, AlSharif LS, Alsubaihi IA, Alzarea AI, Alsultan MM
ClinicoEconomics and Outcomes Research 2025, 17:519-533
Published Date: 23 July 2025