Back to Journals » Journal of Pain Research » Volume 19
Outcomes of Single versus Repeated High-Voltage Pulsed Radiofrequency for Thoracic Herpes Zoster Neuralgia in Patients with Diabetes Mellitus: A Retrospective Study
Authors Shen Q, Zhang H ![]() , Yu J
, Yu J ![]() , Wang B
, Wang B ![]()
Received 20 April 2026
Accepted for publication 23 June 2026
Published 29 June 2026 Volume 2026:19 618445
DOI https://doi.org/10.2147/JPR.S618445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Andrea Tinnirello
Qianqian Shen,1 Hua Zhang,2 Jianming Yu,2 Bo Wang2
1Department of Dermatology, Hangzhou Third People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Pain Medicine, Hangzhou Third People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Jianming Yu, Department of Pain Medicine, Hangzhou Third People’s Hospital, No. 38 West Lake Road, Hangzhou, Zhejiang, 310009, People’s Republic of China, Tel +86 15068180821, Email [email protected] Bo Wang, Department of Pain Medicine, Hangzhou Third People’s Hospital, No. 38 West Lake Road, Hangzhou, Zhejiang, 310009, Tel +86 15158185787, Email [email protected]
Background: Patients with herpes zoster neuralgia (HZN) and comorbid diabetes mellitus (DM) often experience persistent pain that markedly undermines quality of life. Most of these patients respond poorly to oral anticonvulsants or conventional pulsed radiofrequency (PRF). Repeated application of high-voltage PRF may offer superior clinical benefits and improve patient satisfaction.
Objective: This retrospective study aimed to analyze the outcomes of single versus repeated high-voltage PRF for thoracic HZN in patients with DM.
Patients and Methods: We retrospectively analyzed data from 109 thoracic HZN patients with DM who underwent CT-guided high-voltage PRF targeting the thoracic selective dorsal root ganglia (DRG) during a one-week hospitalization period. Outcome measures included the incidence of clinically meaningful postherpetic neuralgia (PHN) and the HbA1c level at 12 weeks post-PRF, Numeric Rating Scale (NRS) score, Pittsburgh Sleep Quality Index (PSQI) score at baseline (pre-PRF) and 1, 4, 8, and 12 weeks following PRF (post-PRF), and the adverse events associated with PRF.
Results: 56 patients received the single high-voltage PRF group (one PRF session, Group SHV-PRF) and 53 patients received the repeated high-voltage PRF group (two PRF sessions, Group RHV-PRF). The incidence of clinically meaningful PHN at 12 weeks post-PRF was lower in group RHV-PRF than in group SHV-PRF (20.8%vs 41.1%, P < 0.05). NRS and PSQI scores were lower in group RHV-PRF than in group SHV-PRF at 1, 4, 8, and 12 weeks post-PRF (P < 0.05). The HbA1c level at 12 weeks post-PRF was lower in group RHV-PRF than in group SHV-PRF (P< 0.05). No severe adverse events were recorded in either group.
Conclusion: Repeated high-voltage pulsed radiofrequency confers favorable therapeutic outcomes for thoracic herpes zoster neuralgia in patients with diabetes mellitus, with an acceptable safety profile.
Keywords: repeated, high-voltage, pulsed radiofrequency, diabetes mellitus, herpes zoster neuralgia
Introduction
Herpes zoster (HZ) is an acute, painful dermatomal vesicular eruption caused by reactivation of latent varicella-zoster virus (VZV).1 In China, the pooled incidence of HZ is 4.28 per 1000 person-years overall and 11.69 per 1000 person-years among individuals aged ≥60 years.2 Herpes zoster neuralgia (HZN) represents the most common and distressing symptom, typically described as lancinating, burning, or electric-shock-like pain restricted to the affected dermatome.3 When neuralgia persists for 90 days or more after rash onset, it is defined as postherpetic neuralgia (PHN).4 The pathophysiology of PHN is multifactorial and remains incompletely elucidated; consequently, treatment responses are often unsatisfactory, resulting in significant deterioration of patients’ physical and psychological well-being.5
Diabetes mellitus (DM) is a prevalent chronic metabolic disorder. In 2021, approximately 521 million people worldwide and 141 million individuals in China were living with DM, with global prevalence projected to reach 1.31 billion by 2050.6 Patients with DM carry a significantly elevated risk of HZ development (84–164%),7,8 and a 23–31% higher likelihood of progression to PHN.9,10 Given the considerable age-related overlap between DM and HZ, the co-occurrence of DM and HZN often leads to more severe and refractory clinical presentations, posing substantial therapeutic dilemmas. A dual-focused strategy is typically advocated: optimization of glycemic control alongside prompt and effective pain relief.
Pulsed radiofrequency has emerged as a well-established neuromodulatory technique for HZN management.11 High-voltage pulsed radiofrequency (HV-PRF) has been shown to provide superior analgesic efficacy in HZN.12,13 however, its efficacy in patients DM complicated by HZN remains suboptimal.14 As such, the efficacy of HV-PRF in this high-risk population has become a key research focus. Recent studies suggest that repeated HV-PRF (RHV-PRF) can significantly improve clinical outcomes in patients with HZN and PHN;15,16 Nevertheless, whether RHV-PRF yields meaningful long-term benefits specifically for thoracic HZN in patients with DM is still unclear. In this study, we retrospectively observed the clinical efficacy and safety of RHV-PRF for thoracic HZN in patients with DM, and compare the outcomes with a single HV-PRF treatment.
Patients and Methods
Study Patients
This study received approval from the Ethics Committee of Hangzhou Third People’s Hospital (2026KA026) and registered with the Chinese Clinical Trial Registry (ChiCTR2600119064) conducted in accordance with the Declaration of Helsinki. Patients were informed and signed the informed consent forms. We collected clinical data from the hospital database and analyzed the records of thoracic HZN patients with DM who underwent HV-PRF in the pain department from March 2022 to October 2025.
Inclusion criteria: (1) Age >18 years; (2) Diagnosed with thoracic HZN; (3) Duration of HZN <1 month; (4) Established diagnosis of type 2 diabetes mellitus;17 (5) Numeric Rating Scale (NRS) score >5 on a 0–10 numerical pain scale.
Exclusion criteria: (1) Unable to reliably report pain intensity or characteristics due to language barriers, neuropsychiatric disorders, or other cognitive impairments; (2) History of preexisting chronic neuralgia unrelated to the HZN; (3) Concomitant ketoacidosis or diabetic hyperosmolar coma; (4) Contraindications to percutaneous needle procedures, including coagulopathy, local infection at the intended puncture site, or underlying malignancy; (5) Loss to follow-up or failure to complete scheduled postoperative assessments.
At admission, patients were informed that they could receive either a single session or repeated sessions of HV-PRF treatment during the one-week hospitalization. The treatment modality was selected by patients based on considerations such as concerns about surgical risks and treatment costs. Accordingly, patients were divided into two groups: the single HV-PRF group (one PRF session; Group SHV-PRF) and the repeated HV-PRF group (two PRF sessions were performed two consecutive days, Group RHV-PRF).
Clinical Procedure
Patients were positioned prone on the treatment bed. Blood pressure, heart rate, pulse oximetry, and electrocardiography were monitored continuously throughout the intervention. The target thoracic dorsal root ganglion (DRG) was identified based on the distribution of cutaneous hyperpigmentation corresponding to the herpes zoster (HZ) dermatome. Using thin-slice (2-mm) CT guidance, the image plane containing the upper-middle portion of the corresponding intervertebral foramen was selected as the optimal puncture plane. The puncture path was designed on this plane image, the upper-middle portion of the corresponding intervertebral foramen was designated as the puncture target, and a line was drawn from this target to avoid the lung; the intersection of this line with the skin served as the puncture point. The distance between the puncture point and the target (the needle penetration depth) and the angle between the line and the sagittal plane (the puncture angle) were measured using the software tools provided by the CT, thereby determining the optimal puncture angle and depth. Following local anesthetic infiltration, a PRF trocar (22gauge, 10 cm electrode with a 10 mm active tip, PMF-22-100-10, Baylis Medical Inc., Montreal, QC, Canada) was advanced under intermittent CT guidance until CT image confirmed that the radiofrequency needle tip was positioned at the upper-middle segment of the intervertebral foramen (Figure 1).
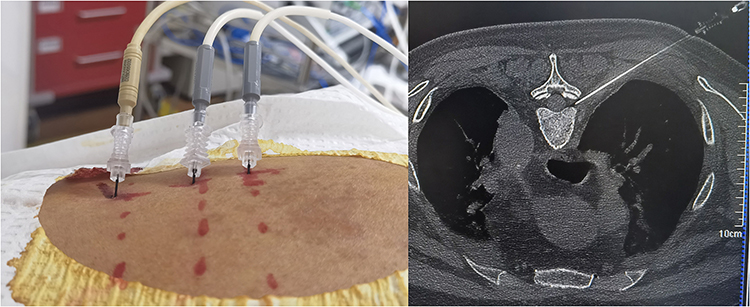 |
Figure 1 Image of puncture and CT shows the needle to the target position. |
Connected to an RFE4 radiofrequency generator in sensation-testing mode, sensory paresthesia (including pain, numbness, thermal sensation, and occasional twitching or tingling) in the cutaneous territory innervated by the target nerve could be evoked at a stimulation voltage within 0.5 V, and in motor-testing mode, no muscle twitching was observed in the corresponding innervated region at stimulation voltages exceeding 1.0 V, verified that the needle tip was accurately positioned at the target dorsal root ganglion (DRG). High voltage was defined as an initial PRF output voltage of 50 V, which was gradually increased until the patient’s tolerable upper limit of abnormal sensation (eg, burning pain) was reached.12 The manual PRF mode was employed with the following basic settings: pulse width 20 ms, pulse frequency 2 Hz, PRF duration 600 seconds, pulse temperature limit 42 °C, and impedance range 150–300 Ω, the initial PRF voltage was set to 50 V and increased in 5–10 V increments until the high voltage was achieved, and treatment was then delivered. Impedance remained stable (variation <10%) throughout the procedure, so automatic adjustment was not required.
In both groups, pregabalin was tapered and discontinued within two weeks after treatment. Rescue tramadol (100 mg) was permitted when NRS >6. Glycemic management was overseen by the same endocrinologist; basal insulin was adjusted based on fasting glucose, and prandial insulin was modified according to post-prandial glucose excursions every 1–3 days. Oral hypoglycemic agents were individually adjusted. After discharge, patients continued their regular medications and attended scheduled follow-ups.
Outcomes
Demographic and disease-related information, including age, gender, disease duration, affected side, hemoglobin A1c (HbA1c) level, fasting blood glucose, dose of pregabalin before PRF and PRF voltage were retrieved from the electronic medical record system. The NRS ranges from 0 to 10, and the Pittsburgh Sleep Quality Index (PSQI) total score ranges from 0 to 21.
The primary outcome was the incidence of clinically meaningful PHN at 12 weeks post-PRF4(clinically meaningful PHN, dermatomal pain persisting at least 90 days after the appearance of the acute herpes zoster rash, usually a NRS score of 3 or higher on a scale ranging from 0 (no pain) to 10 (worst possible pain)). Secondary outcomes included the NRS and PSQI scores at pre-PRF, 1, 4, 8, and 12 weeks post-PRF, the HbA1c level at 12 weeks post-PRF, and the adverse events associated with PRF (eg, nerve damage, hemopneumothorax, hematoma, and local infections).
Statistical Analysis
SPSS 20.0 software (SPSS, Illinois, United States) was used for data analysis. Enumeration data were presented as counts, and rates were compared using the χ2 test, odds ratio with 95% CI was provided. All quantitative data were evaluated for normality with the Shapiro–Wilk test and assessed for homogeneity of variance using Levene’s test. Data followed a normal distribution were presented as mean ± standard deviation and compared using the t-test, and to assess variable data at different time points, a repeated measures analysis of variance (RM-ANOVA) was conducted, and the mean difference with its 95% confidence interval (CI) was reported. Data did not follow a normal distribution were presented as median (interquartile range) and compared using the Mann–Whitney U-test. P < 0.05 was considered statistically significant.
Results
A total of 119 patients were enrolled in this study. Among them, 6 patients were lost to follow-up, and 4 patients withdrew (Figure 2). Ultimately, 109 patients were included in the analysis. 56 patients received the SHV-PRF group and 53 patients received the repeated RHV-PRF group.
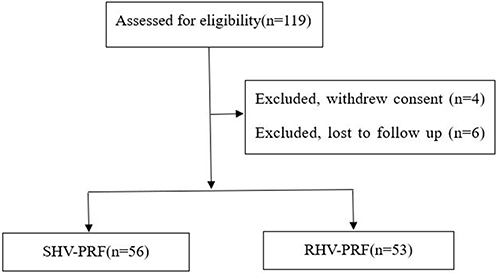 |
Figure 2 Flow diagram of the study patients. Abbreviations: SHV-PRF, single high-voltage pulsed radiofrequency; HVR-PRF, repeated high-voltage pulsed radiofrequency. |
The baseline characteristics of patients, including age, gender, duration of HZN and DM, affected side, pre-PRF HbA1c level, dose of pregabalin, fasting blood glucose, and PRF voltage exhibited no significant differences between the two groups (P > 0.05, Table 1).
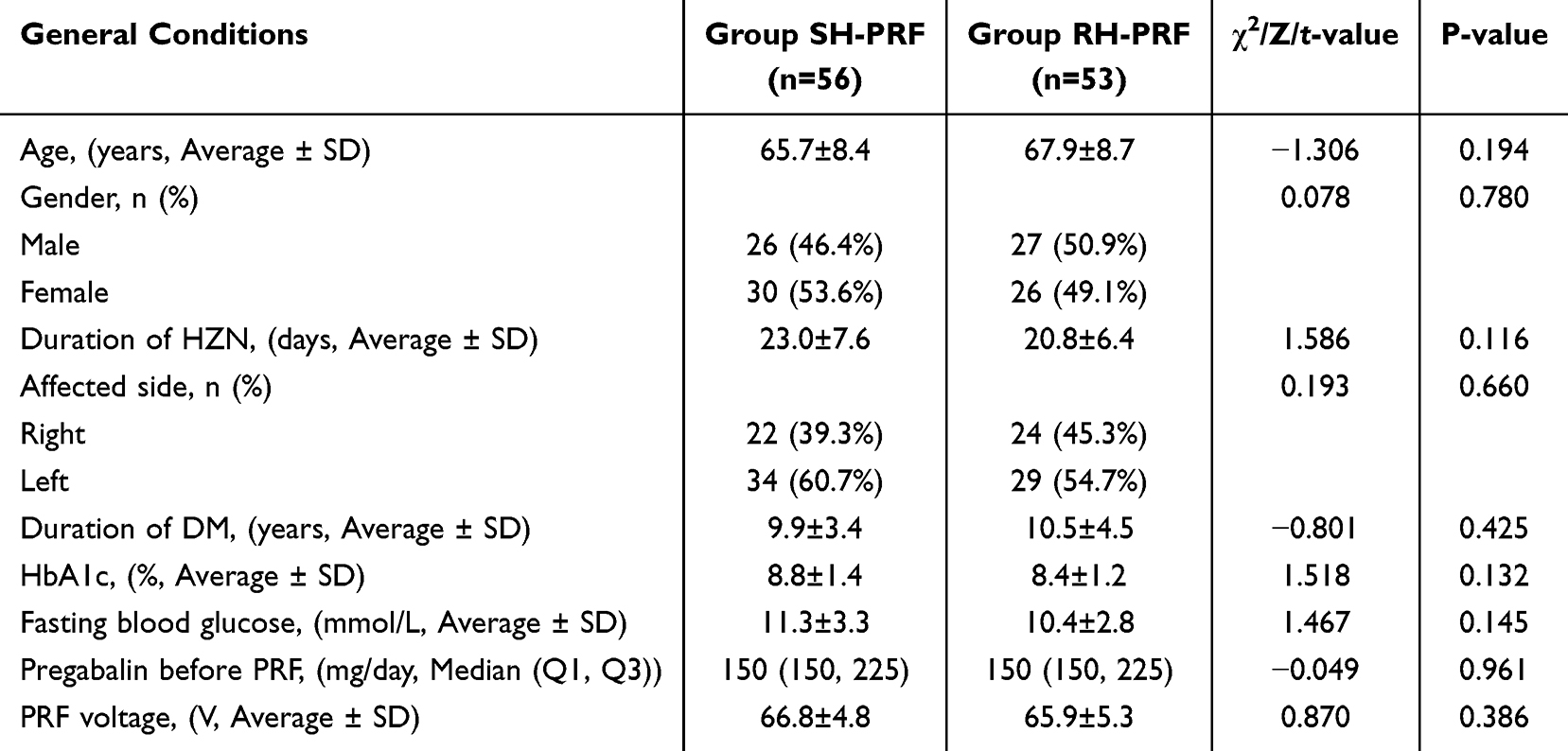 |
Table 1 Basic Characteristics of the Participants |
The incidence of clinically meaningful PHN at 12 weeks post-PRF was lower in group RHV-PRF than in group SHV-PRF (20.8%vs 41.1%, OR=2.661 (1.136, 6.232), P < 0.05). Moreover, NRS scores were lower in group RHV-PRF than in group SHV-PRF at 1, 4, 8, and 12 weeks post-PRF (mean difference: 1.710, 1.601, 1.700, and 1.566; 95% CI: 1.316 −2.104, 1.260–1.943, 1.297–2.103, and 1.185 −1.946; P < 0.05) (Table 2), and PSQI scores were lower in group RHV-PRF than in group SHV-PRF at 1, 4, 8, and 12 weeks post-PRF (mean difference: 3.080, 2.413, 2.152, and 2.278; 95% CI: 2.401–3.759, 1.893–2.934, 1.681–2.623, and 1.844–2.712; P < 0.05) (Table 3). The HbA1c level at 12 weeks post-PRF was lower in group RHV-PRF than in group SHV-PRF (mean difference: 1.548, CI: 1.102–1.994, P<0.05) (Table 4). Additionally, no serious adverse events and no rescue analgesic measure were reported in either group.
 |
Table 2 The NRS of the Patients in the Two Groups |
 |
Table 3 The PSQI of the Patients in the Two Groups |
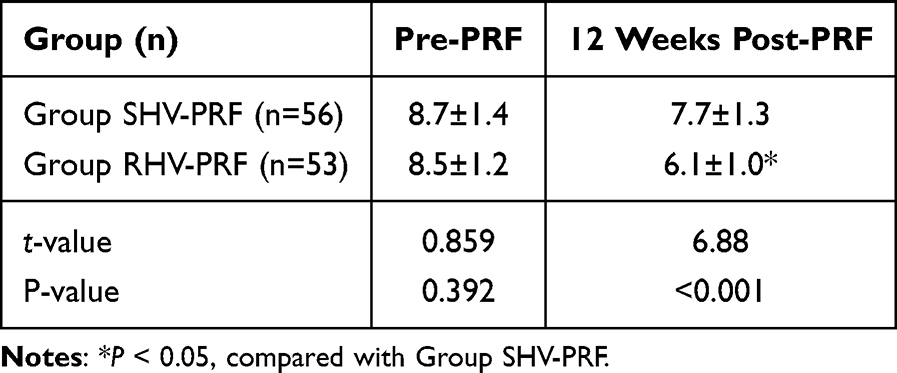 |
Table 4 The HbA1c Level of the Patients in the Two Groups |
Discussion
Diabetes mellitus impairs glucose metabolism, activating the polyol pathway, compromising cellular immunity, and promoting microangiopathy, all of which increase susceptibility to VZV reactivation.18,19 Furthermore, neuralgia and infection trigger elevations in counter-regulatory hormones (glucocorticoids, glucagon, catecholamines),20 exacerbating hyperglycemia. Hyperglycemia, in turn, upregulates pro-inflammatory cytokines (NF-κB, TNF-α, IL-6)21,22 and enhances oxidative stress via nitric oxide and superoxide production, leading to nitrosative damage and neuronal injury.23,24 These pathological cascades worsen demyelination and axonal degeneration in sensory fibers, intensifying pain and establishing a bidirectional vicious cycle of “neuralgia–hyperglycemia”. Consequently, managing both pain and glucose control becomes extremely challenging for thoracic HZN in patients with DM.
Optimal glycemic management in these patients requires reassessment by an endocrinologist, adjustment of the medication regimen, and efforts to maintain a stable glycemic range. The use of continuous glucose monitoring system is recommended to dynamically and accurately monitor glucose level, allowing for the timely implementation of precise glycemic management strategies.25 Pharmacological management of thoracic HZN in patients with DM presents unique clinical challenges, as these patients often exhibit reduced drug tolerance and increased susceptibility to adverse reactions associated with anticonvulsants and analgesics. Consequently, achieving therapeutic doses becomes difficult, leading to poor treatment response and delayed disease resolution. This, coupled with prolonged disease duration and severe pain that necessitates the combination of multiple treatment modalities, increases healthcare resource utilization and cost burden.26
Our study demonstrated significant improvements in NRS and PSQI scores from baseline in both groups, corroborating the effectiveness and precision of HV-PRF therapy for HZN. PRF delivers an intermittent high-frequency current that acts on nerve tissue for short durations, inhibiting excitatory afferent input from dorsal root C-fibers, upregulating c-fos gene expression in dorsal root neurons, and modulating neural synapses.27 These mechanisms contribute to the peripheral long-term analgesic effects of pain modulation. Increasing the PRF voltage, and thereby the electric field strength, induces changes in neural plasticity and significantly enhances its efficacy.28
Our findings indicate that repeated HV-PRF resulted in significantly lower NRS and PSQI scores at all follow-up timepoints and lower incidence of clinically meaningful PHN at 12 weeks post-PRF. HZN is a complex neuropathic pain condition, and patients frequently experience multiple types of pain simultaneously, therefore, a single PRF has a limited regulatory effect on the nervous system and cannot fully address all pain signals. Repeated PRF stimulation can act on injured nerves multiple times, promoting neurorepair, resolving neuroinflammation, normalizing aberrant discharges, and enhancing neuroplasticity while reducing central sensitization.29 Two sessions within one week deliver cumulative, prolonged DRG stimulation, consolidating therapeutic effects and enabling more thorough modulation of residual pain, thus offering a stepwise, individualized management approach.
The HbA1c level at 12 weeks post-PRF was lower in group RHV-PRF than in group SHV-PRF, though confounding factors (eg, baseline glycemic severity, medication changes) were not rigorously controlled, so this result should be interpreted cautiously. However, the difference in this indicator between the two groups represents an important finding. Severe and persistent pain acts as a chronic stressor, activating the sympathoadrenal and hypothalamic-pituitary-adrenal (HPA) axis, which leads to surges in counterregulatory hormones (cortisol and catecholamines) that induce peripheral insulin resistance and glucose volatility. We speculate that RHV-PRF, by providing superior analgesia and restorative sleep, may interrupt this deleterious feedback loop, thereby promoting better autonomic balance and metabolic stability. This “analgesic-metabolic” benefit is especially important for diabetic patients, in whom glycemic management serves both as a therapeutic goal and a prerequisite for neural repair.
In this study, no adverse events associated with PRF, including puncture site infection, hematoma, bleeding, or pneumothorax occurred in either group. The puncture angle and trajectory were designed based on preoperative CT scans, and real-time CT guidance was used during the procedure to ensure full visualization and precise execution throughout the entire surgical process. Furthermore, the unique mechanism of PRF generates temperatures that do not damage nerves or surrounding tissues.
Despite these encouraging results, we advocate preventive measures for diabetic patients, including regular glucose monitoring, immune assessment, health education, and HZ vaccination,30 especially in those with a family history.
The study has several limitations that should be addressed in future research. First, the study was non-randomized and retrospective in design, it cannot avoid confounders that may independently influence outcomes. Second, patients were recruited from a single center, resulting in a relatively small sample size, expanding the sample size and engaging in multicenter collaboration would be beneficial. Third, the decision to administer two treatment sessions within one week of hospitalization was based on inpatient logistical considerations and a previous study on trigeminal neuralgia,15 the optimal interval and number of repeated treatments remain to be determined. Fourth, we did not include a separate standard PRF or non-PRF treatment (eg, pharmacological optimization alone) control group, the inclusion of a control group would enhance the significance of this study. Finally, glucose-related indicators were exploratory endpoints, and confounding factors such as diet, exercise and medication regimen were not strictly controlled, the causal relationship should be interpreted with caution, yet it warrants further investigation.
Conclusion
In this retrospective study, repeated high-voltage pulsed radiofrequency was associated with a lower incidence of clinically meaningful PHN and superior pain and sleep outcomes compared with a single session for thoracic HZN in patients with DM. However, treatment session assignment was not randomized, these results should be interpreted as exploratory associations. A well-designed prospective randomized controlled trial is warranted to confirm the therapeutic advantage of repeated HV-PRF in this population.
Data Sharing Statement
Data used to support the findings of this study are available from the corresponding author (Bo Wang) upon request.
Ethical Approval
The Ethics Committee of Hangzhou Third People’s Hospital (2026KA026) and Chinese Clinical Trial Registry (ChiCTR2600119064) approved this research.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
All authors had complete access to the data and were involved in all analyses. The corresponding author reviewed and approved the final version and has final responsibility for the decision to submit this manuscript for publication. We would like to thank the editorial board for their review and criticism in improving this manuscript.
Funding
This research provided financial support in the form of the Hangzhou Joint Funds of Zhejiang Provincial Natural Science Foundation of China under Grant No. LHZY24H090001. The sponsor had no role in the design or conduct of this research.
Disclosure
The authors declare that they have no competing interests in this research.
References
1. Gnann JJW, Whitley RJ. Clinical practice. Herpes zoster. N Engl J Med. 2002;347(5):340–8. doi:10.1056/nejmcp013211
2. Zhang ZJZ, Liu XN, Suo LD, et al. The incidence of herpes zoster in China: a meta-analysis and evidence quality assessment. Hum Vaccines Immunother. 2023;19(2):2228169. doi:10.1080/21645515.2023.2228169
3. Patil A, Goldust M, Wollina U. Herpes zoster: a review of clinical manifestations and management. Viruses. 2022;14(2):192. doi:10.3390/v14020192
4. Johnson RW, Rice AS. Clinical practice. Postherpetic neuralgia. New Engl J Med. 2014;371(16):1526–1533. doi:10.1056/NEJMcp1403062
5. Adriaansen EJM, Jacobs JG, Vernooij LM, et al. Herpes zoster and post herpetic neuralgia. Pain Pract. 2024;11(04). doi:10.1111/papr.13423
6. GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the global burden of disease study 2021. Lancet. 2023;402(10397):203–234. doi:10.1016/S0140-6736(23)01301-6.
7. Huang CT, Lee CY, Sung HY, et al. Association between diabetes mellitus and the risk of herpes zoster: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2022;107(2):586–597. doi:10.1210/clinem/dgab675
8. Queenan JA, Farahani P, Ehsani-Moghadam B, et al. The prevalence and risk for herpes zoster infection in adult patients with diabetes mellitus in the Canadian primary care sentinel surveillance network. Can J Diab. 2018;42(5):465469. doi:10.1016/j.jcjd.2017.10.060
9. Lan HN, Ai ZG, Xu SC, et al. Genetically predicted amino acids related to neural regulation mediate the association between diabetes mellitus and postherpetic neuralgia: a Mendelian randomization study. Diabetol Metab Syndr. 2025;17(1):104. doi:10.1186/s13098-025-01672-1
10. Yang XY, Li DR, Chen YQ, et al. Exploring the link between diabetes, herpes zoster, and post-herpetic neuralgia: insights from mendelian randomization. J Pain Res. 2025;18(3):1479–1489. doi:10.2147/JPR.S501674
11. Kim KH, Jo DH, Kim ED. Pulsed radiofrequency to the dorsal root ganglion in acute herpes zoster and postherpetic neuralgia. Pain Phys. 2017;20(3):E411–418. PMID: 28339440.
12. Wang B, Du ZJ, Xia JR, et al. Efficacy of high-voltage pulsed radiofrequency for the treatment of elderly patients with acute herpes zoster neuralgia. Revista da Associacao Medica Brasileira. 2021;67(4):585–589. doi:10.1590/1806-9282.20201124
13. Song YH, Yu ZH, Guan JJ, et al. Efficacy of gasserian ganglion high-voltage, long-duration pulsed radiofrequency combined with block on acute/subacute zoster-related trigeminal neuralgia. Pain Res Manag. 2024;2024:1992483. doi:10.1155/2024/1992483
14. Yang J, Liu RG, Feng SX, et al. The influence analysis of diabetes on the treatment of postherpetic neuralgia by high-voltage pulsed radiofrequency. Chin J Pain Med. 2021;27(07):505–509. doi:10.3969/j.issn.1006-9852.2021.07.005
15. Wang B, Xia JR, Li JY, et al. Effect of repeated pulsed radiofrequency for trigeminal herpes zoster neuralgia: a retrospective study. J Pain Res. 2026;19:557560. doi:10.2147/JPR.S557560
16. Wen HC, Wang Y, Cheng H, et al. Outcomes of twice-repeated high-voltage long-duration pulsed radiofrequency treatment in subacute postherpetic neuralgia: a retrospective single-center analysis. J Pain Res. 2024;17:2043–2050. doi:10.2147/JPR.S465251
17. American Diabetes Association Professional Practice Committee. 2. Diagnosis and classification of diabetes: standards of care in diabetes-2024. Diab Care. 2024;47(Suppl 1):S20–S42. doi:10.2337/dc24-S002.
18. Katsuda Y, Sasase T, Tadaki H, et al. Contribution of hyperglycemia on diabetic complications in obese type 2 diabetic SDT fatty rats: effects of SGLT inhibitor phlorizin. Exp Animals. 2015;64(2):161–169. doi:10.1538/expanim.14-0084
19. Thallas-Bonke V, Jha JC, Gray SP, et al. Nox-4 deletion reduces oxidative stress and injury by PKC-α-associated mechanisms in diabetic nephropathy. Physiol Rep. 2014;2(11):e12192. doi:10.14814/phy2.12192
20. Munoz-Quiles C, Lopez-Lacort M, Ampudia-Blasco FJ, et al. Risk and impact of herpes zoster on patients with diabetes: a population-based study, 2009-2014. Hum Vaccin Immunother. 2017;13(11):2606–2611. doi:10.1080/21645515.2017.1368600
21. Rahman MH, Jha MK, Suk K. Evolving insights into the pathophysiology of diabetic neuropathy: implications of malfunctioning glia and discovery of novel therapeutic targets. Targets Current Pharmaceut Design. 2016;22(6):738–757. doi:10.2174/1381612822666151204001234
22. Mu ZP, Wang YG, Li CQ, et al. Association between tumor necrosis factor-α and diabetic peripheral neuropathy in patients with type 2 diabetes: a meta-analysis. Mol Neurobiol. 2017;54(2):983–996. doi:10.1007/s12035-016-9702-z
23. Vincent AM, Backus C, Mclean LL, et al. Short-term hyperglycemia produces oxidative damage and apoptosis in neurons. Fed Am Soc Exp Biol. 2005;19(6):638–640. doi:10.1096/fj.04-2513fje
24. Vinik AI, Park TS, Stansberry KB. Diabetic neuropathies. Diabetologia. 2000;43(8):957–973. doi:10.1007/s001250051477
25. Danne T, Nimri R, Battelino T, et al. International consensus on use of continuous glucose monitoring. Diab Care. 2017;40(12):1631–1640. doi:10.2337/dc17-1600
26. Poirrier JE, Meyers JL, Nagar SP, et al. Herpes zoster incidence and burden in adults with type 2 diabetes in the U.S.: a retrospective database analysis. Diab Care. 2022;45(11):2585–2593. doi:10.2337/dc21-2053
27. Ojango C, Raguso M, Fiori R, et al. Pulse-dose radiofrequency treatment in pain management-initial experience. Skel Radiol. 2018;47(5):609–618. doi:10.1007/s00256-017-2854-8
28. Wan CF, Liu Y, Dong DS, et al. Bipolar high-voltage, long-duration pulsed radiofrequency improves pain relief in postherpetic neuralgia. Pain Phys. 2016;19(5):E721–E728. doi:10.202207/article.27389115
29. Vallejo R, Tilley DM, Williams J, et al. Pulsed radiofrequency modulates pain regulatory gene expression along the nociceptive pathway. Pain Phys. 2013;16(5):E601–E613. doi:10.36076/ppj.2013/16/e601
30. Silverii GA, Clerico A, Fornengo R, et al. Efficacy and effectiveness of herpes zoster vaccination in adults with diabetes mellitus: a systematic review and meta-analysis of clinical trials and observational studies. Acta Diabetolog. 2023;60(10):1343–1349. doi:10.1007/s00592-023-02127-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of High-Voltage Pulsed Radiofrequency versus Standard-Voltage Pulsed Radiofrequency for Patients with Neuropathic Pain: A Literature Review and Meta-Analysis
Wang Y, Jia Y, Wang Z, Feng G, Ma Y, Fan Z, Liu M, Feng K, Wang T
Journal of Pain Research 2024, 17:851-863
Published Date: 4 March 2024
Effect of Repeated Pulsed Radiofrequency for Trigeminal Herpes Zoster Neuralgia: A Retrospective Study
Wang B, Xia JR, Li JY, Du ZJ, Yu JM
Journal of Pain Research 2026, 19:557560
Published Date: 9 January 2026