Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Optimizing Treatment for Hospitalized Patients with COPD: A Study on the Impact of a LINE App-Based Multidisciplinary Team Approach Targeting Pharmacological Treatment, Lifestyle Changes, and Smoking Cessation
Authors Huang HY, Chen CL, Lin YL, Chen SC, Lee LC, Dai HM, Chiang CY, Chang YF, Lu H, Lee MR, Yang CC, Su CH, Chiang YZ, Yang MC ![]() , Shyu RY, Lan CC
, Shyu RY, Lan CC ![]()
Received 4 January 2025
Accepted for publication 26 March 2025
Published 18 April 2025 Volume 2025:20 Pages 1149—1159
DOI https://doi.org/10.2147/COPD.S511869
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Hsiang-Yu Huang,1,* Chia-Ling Chen,2,* Yi-Ling Lin,3 Shu-Chuan Chen,4 Li-Chu Lee,4 Huei-Min Dai,4 Cheng-Yang Chiang,5 Yu-Fan Chang,6 Hsiu Lu,7 Mung-Rung Lee,7 Chih-Chiao Yang,8 Chiu-Hui Su,9 Ying-Zhen Chiang,10 Mei-Chen Yang,2,11 Rong-Yaun Shyu,12 Chou-Chin Lan2,11
1Division of Respiratory Therapy, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 2Division of Pulmonary Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 3Department of Planning and Management, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 4Department of Nursing, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 5Department of Nutrition, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 6Department of Pharmacy, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 7Center of Community and Long-term Care Services, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 8Department of Social Services, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 9Center of Chest Medicine Examination, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 10Center of Quality Management, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China; 11School of Medicine, Tzu-Chi University, Hualien, Taiwan, Republic of China; 12Division of Gastroenterology, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Republic of China
*These authors contributed equally to this work
Correspondence: Chou-Chin Lan, Division of Pulmonary Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, 289, Jianguo Road, Xindian City, New Taipei City, 23142, Taiwan, Republic of China, Tel +886-2-6628-9779 ext. 2259, Fax +886-2-6628-9009, Email [email protected] Rong-Yaun Shyu, Division of Gastroenterology, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, 289, Jianguo Road, Xindian City, New Taipei City, 23142, Taiwan, Republic of China, Tel +886-2-6628-9779 ext. 8119, Fax +886-2-6628-9009, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a progressive respiratory condition that significantly impacts patients’ health status. Effective management requires a multidisciplinary team (MDT) to address pharmacological and non- pharmacological treatments. The integration of mobile apps and devices improves COPD management by reducing symptoms and exacerbations. LINE, a commonly used communication app, enhanced team coordination and real-time decision-making. This study explored the effectiveness of LINE-based MDT interventions in hospitalized patients with COPD.
Methods: This retrospective analysis included patients with COPD admitted for exacerbations and compared their outcomes before and after the implementation of LINE-based MDT care. The MDT consisted of pulmonologists, care managers, nurses, dietitians, social workers, pharmacists, respiratory therapists, and long-term care teams. A LINE group coordinated care in real-time, enabling the team to promptly review the patients’ conditions, adjust treatment plans, and provide tailored interventions.
Results: The LINE-based MDT group demonstrated significantly higher intervention rates, including systemic steroids, inhaled corticosteroids, long-acting beta-agonists, long-acting muscarinic antagonists, and pulmonary rehabilitation (p< 0.05). BSRS improvement was greater in the MDT group than the non-MDT group (40.9% vs 29.7%, p = 0.016). However, there were no significant differences between the groups’ readmission rates, emergency room visits, or one year survival (p> 0.05).
Conclusion: Implementing LINE-based MDT care significantly improved the delivery of pharmacological and non-pharmacological interventions, enhanced coordination, and facilitated comprehensive management, leading to better quality of life outcomes, as evidenced by improvements in BSRS scores. This highlights the value of leveraging real-time communication tools like LINE app to optimize COPD care.
Keywords: chronic obstructive pulmonary disease, multidisciplinary team, health-related quality of life, LINE-based
Introduction
Chronic obstructive pulmonary disease (COPD) is a respiratory disease influenced by several risk factors, including smoking, air pollution, occupational exposure, genetic predisposition, and infections during childhood or adulthood.1 According to the World Health Organization (WHO), 3 million deaths are attributed to this disease each year. WHO also predicts that COPD will become the third leading cause of death by 2030.2 COPD poses a significant public health challenge in Taiwan.3 An epidemiological survey revealed a prevalence rate of 6.1% in this population, with many affected individuals experiencing multiple comorbidities.3
COPD is a significant public health issue. It is a progressive condition that worsens over time, leading to health decline, reduced health-related quality of life (HRQL), and diminished endurance in daily activities.4 The symptoms and complications of COPD can severely limit the patient’s ability to perform everyday tasks, greatly affecting their overall well-being. Frequent acute exacerbations and hospitalizations are common in COPD, often resulting in a further decline in HRQL and overall health status.4 Moreover, patients with COPD who experience frequent hospitalization are at a significantly higher risk of mortality.4 As such, effective management of hospitalized COPD patients is crucial.
The management of COPD requires collaborative efforts by multiple healthcare professionals to deliver both pharmacological and non-pharmacological interventions for optimal outcomes.5 There is a growing trend toward an interdisciplinary approach to COPD management.5 A multidisciplinary team (MDT) plays a crucial role in the comprehensive care of COPD, which often involves respiratory complications and comorbid conditions such as cardiovascular disease and malnutrition.6,7 Pulmonologists focus on medical treatment and respiratory care; physiotherapists assist with pulmonary rehabilitation (PR); dietitians offer nutritional support; and psychologists provide mental health care, addressing all aspects of the patient’s treatment.6 MDT also strongly emphasizes patient education and self-management, empowering individuals to manage their symptoms and adhere to treatment plans.7 This collaborative approach has become essential in COPD care, enabling personalized strategies that effectively address both pulmonary and non-pulmonary challenges. However, the effectiveness of these programs remains unclear.5,7
Many studies have highlighted the potential of electronic tools, including electronic monitoring devices, smartphone apps, and web-based platforms, in the management of patients with COPD.8,9 One systematic review suggested that the use of electronic health tools can improve adherence to inhalation therapy.8 myCOPD is a digital application (app) designed by experts to assist healthcare providers and patients in managing COPD.9 It offers education, self-management features, symptom tracking, and PR support. It has been reported to be non-inferior to face-to-face PR in terms of COPD assessment test (CAT) score, walking test performance, anxiety levels, and HRQL.9 The integration of electronic tools in COPD management is growing.8,9 In Taiwan, the use of the LINE app has become widespread, offering a convenient platform to assist with treatment support.
Given the complexity of COPD and its associated comorbidities, hospitalized patients with COPD often present with a poor condition and require more comprehensive treatment.10 This makes the MDT approach an ideal strategy for their care.10 To enhance MDT care, our study integrated LINE, a widely used communication app in Taiwan, to improve coordination and real-time communication among team members. Through the LINE-based system, the respiratory care manager promptly notified MDT members upon a patient’s admission, enabling rapid evaluation and collaborative decision-making. This communication platform allowed for seamless updates on patient progress and facilitated the timely delivery of individualized care. By leveraging this tool, MDT care can be delivered more efficiently and effectively, addressing the complexities of hospitalized COPD management. The primary outcomes of this study included hospitalization days, 14-day re-admission rates, emergency room visits within 30 days of discharge, and one-year survival rate. Secondary outcomes included HRQL, adherence to treatment plans, and smoking cessation rates. By analyzing these outcomes, we aimed to assess the value of LINE-based MDT interventions in optimizing treatment and improving outcomes in hospitalized patients with COPD.
Materials and Methods
Patient Recruitment
The study included patients admitted to the Chest Ward for COPD exacerbation between January 1, 2018, and September 20, 2024. We retrospectively analyzed real-world data on COPD diagnoses confirmed by spirometry. The MDT was established on January 1, 2019. Therefore, the period from January 1, 2018, to December 31, 2018, represented care without MDT involvement, whereas the period after January 1, 2019, reflected care under the MDT approach. In this study, we compared patient outcomes before and after the implementation of MDT care. The Ethics Committee of the Taipei Tzu Chi Hospital approved the study protocol and the approval number is 14-IRB-208. We performed this study in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants in the study.
Patient Care
Before MDT Care
The patients received usual care, with the chest physician prescribing medications based on their clinical expertise. The chest physician initiated PR interventions. Ward nurses provided routine care and education. Dietitian intervention was initiated when the patient’s body mass index (BMI) was < 18.5 kg/m². The nurse notified the smoking cessation manager to intervene if the patient was a current smoker. The Brief Symptom Rating Scale (BSRS-5) scores were routinely assessed at admission and discharge. During hospitalization, patient management was typically handled by physicians and nurses based on their individual experiences, without team oversight.
Applying MDT Care
The multidisciplinary team (MDT) consisted of chest physicians, ward nurses, respiratory care managers, smoking cessation managers, respiratory therapists, dietitians, long-term care case managers, social workers, technicians, and other specialists. The entire team communicated through a LINE group, whereupon patient admission for COPD exacerbation, the case manager promptly notified all team members. The respiratory care manager evaluated within one working day, and the team reviewed the patient’s condition and treatment plan collaboratively via LINE. Other team members followed up with assessments and interventions within three working days. The respiratory therapist provided education on breathing exercises and diaphragmatic breathing, and recommended respiratory care. Dietitian intervention was triggered when the patient’s BMI fell below 21 kg/m², and the smoking cessation manager was informed to intervene with the smokers. BSRS assessments were performed at admission and discharge. Each MDT member delivered individualized care, performed comprehensive assessments, developed tailored treatment plans, provided educational interventions, and offered counseling through LINE. The LINE group facilitated real-time collaboration, allowing team members to promptly adjust treatment plans based on ongoing evaluations and ensuring a coordinated and responsive approach to patient care.
Pulmonary Function Test
Pulmonary function tests were performed by a technician following the established guidelines of the American Thoracic Society, employing a spirometer device produced by Medical Graphics Corporation, St. Paul, Minnesota, USA.11 The measurements of forced vital capacity (FVC) and forced expiratory volume in the first second (FEV1) were included. The degree of airflow obstruction was assessed by evaluating the FEV1 percentage.6
Psychological Distress and Health-Related Quality of Life
Psychological distress was assessed using the BSRS-5, which includes items measuring anxiety, depression, hostility, inferiority, and insomnia.12 Additionally, the final item screened for suicidal ideation. Patients rated each symptom on a 5-point scale ranging from 0 (not at all) to 4 (extremely), and the total score was calculated.12 If depression was suspected based on BSRS-5 results, patients were referred to psychologists or social workers for further evaluation and management. BSRS-5 scores were assessed at admission and discharge.
Pharmacological Treatment by Chest Physician
The three main medications most commonly used for COPD exacerbation are bronchodilators, corticosteroids, and antibiotics (if an infection is present).10
Medications were prescribed by chest physicians and evaluated using the MDT within one working day following the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines.6 For acute exacerbations, inhalation was the preferred route of administration, with nebulized Atrovent and Bricanyl being commonly used. Systemic corticosteroids such as hydrocortisone or methylprednisolone were administered as needed. Long-acting beta-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS) were prescribed before discharge. Patients were educated on proper inhaler techniques to ensure effective medication use.6
Education Provided by Ward Nurse
The ward nurses offered education centered on patient care during hospitalization, emphasizing the importance of understanding patients’ conditions and treatment plans.13 The patients were taught about their medications, including dosages and potential side effects, and the significance of maintaining a healthy lifestyle, including nutrition. The nurses also provided information on recognizing early signs of complications and the importance of promptly communicating concerns.13
Education Provided by Respiratory Case Manager
The respiratory case manager provided education focused on managing respiratory conditions, emphasizing the importance of medication adherence, proper inhaler techniques, and self-treatment knowledge.14 Patients were taught to recognize and respond to the symptoms of exacerbations and the significance of regular follow-up appointments. In addition, the case manager offered resources and support for smoking cessation and exercise training.14
Breathing Exercise
The protocol for breathing exercises, such as pursed-lip and diaphragmatic breathing, was taught to the patients.15 Pursed-lip breathing involves slow inhalation through the nose and gentle exhalation through the pursed lips. This technique helps slow the breathing rate, increases oxygenation, and prevents airway collapse by maintaining a positive airway pressure during exhalation. Diaphragmatic breathing encourages deep breathing through engagement with the diaphragm. Patients were instructed to place one hand on their abdomen and the other on their chest, focusing on expanding their abdomen during inhalation.15
Airway Clearance Techniques
Airway clearance techniques, including huffing and oscillating positive expiratory pressure (OPEP) devices, were used in patients with sputum.16 Huffing involves taking a deep breath, followed by a forceful exhalation with an open mouth to help move mucus from the smaller to the larger airways for easier clearance. The patients were also provided with Aerobika, an OPEP device. Respiratory therapists instructed patients on properly performing huffing and used the Aerobika device for optimal airway clearance.16
Nutritional Strategies
Patients with a BMI < 21 kg/m² were referred to a dietician for nutritional counseling. They were advised to limit the intake of simple carbohydrates, including table sugar, candy, cake, and regular soft drinks.17 They should consume 20 to 30 grams of fiber daily, primarily through fruits, vegetables, and whole grains. Basic nutraceutical components such as vitamins and fibers were to be obtained from natural food sources. Additionally, a diet higher in healthy fats (excluding trans and saturated fats), increased protein intake, and reduced carbohydrate intake were suggested.17
Smoking Cessation
The ward nurse evaluated all admitted patients, identified current smokers, and advised them to quit.18 These patients were referred to a smoking cessation case manager. Clear guidance on smoking cessation was provided, highlighting its significant health benefits, particularly for lung function and overall respiratory health. Patients were encouraged to seek assistance from smoking cessation specialists through counseling, nicotine replacement therapy, or medication, as needed, to aid the cessation process.18
Outcomes and Measurements
The primary outcome measures included clinical indicators such as hospitalization days, the occurrence of 14-day re-admission, emergency room visits within 30 days of discharge, and one-year survival.19 Secondary outcome measures included HRQL, adherence to treatment plans, and smoking cessation success rates.20 All outcome measures were compared between patients treated with and without the MDT to evaluate the impact of the MDT approach on patient care.
Statistical Analysis
Patients were divided into two groups: those without and those with MDT support. Continuous variables with a normal distribution are presented as means ± SD, while continuous variables with a skewed distribution are presented as medians (interquartile range, IQR). Categorical variables are presented as counts (percentages). An independent samples t-test was used to compare continuous variables between the two groups, whereas Pearson’s chi-square and Fisher’s exact test were used for categorical variables. The propensity score matching (PSM) was performed with age, body height, smoking, FEV1/FVC, and FEV1 as the matching variables using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The matching process followed a one-to-many approach. The method prioritizes “best” matches first and then proceeds with “next-best” matches until no more can be made. Statistical analyses except for PSM were conducted using SPSS (version 24.0; SPSS Inc., Chicago, IL, USA).
Results
Demographic and Clinical Differences Between Patients without and with MDT Before Matching
Table 1 presents the demographic and clinical characteristics of all patients before matching. The non-MDT and MDT groups included 83 and 406 patients, respectively. MDT patients were younger on average (75.8 vs 78.9 years, p = 0.015) but had a lower median FEV1/FVC ratio (49.0% vs 56.0%, p = 0.026) and FEV1% (50.0% vs 55.0%, p = 0.036). The non-MDT group had a higher proportion of nonsmokers than the MDT group (50.6% vs 25.9%, p < 0.001). BMI, body weight, COPD stage, FVC, and FVC% were not significantly different between the groups (all p > 0.05).
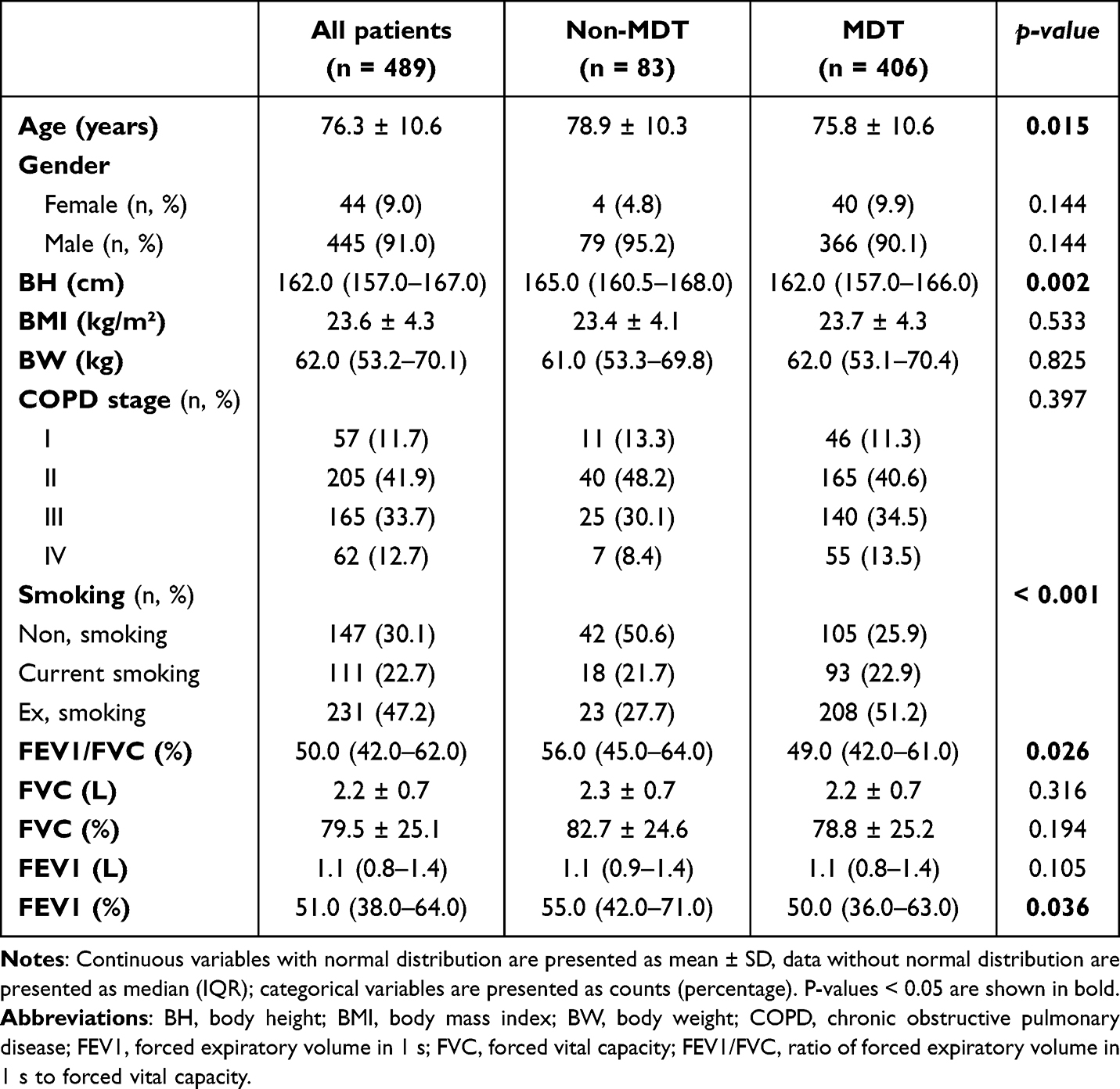 |
Table 1 Demographic and Clinical Differences Between Patients Without and With Multidisciplinary Team |
Demographic and Clinical Differences Between Patients without and with MDT After Matching
Table 2 shows that after propensity matching, there were no significant differences between the MDT and non-MDT groups. Age, height, BMI, body weight, FVC, FEV1, COPD stage, and smoking status were comparable, with similar distributions across all variables (all p > 0.05).
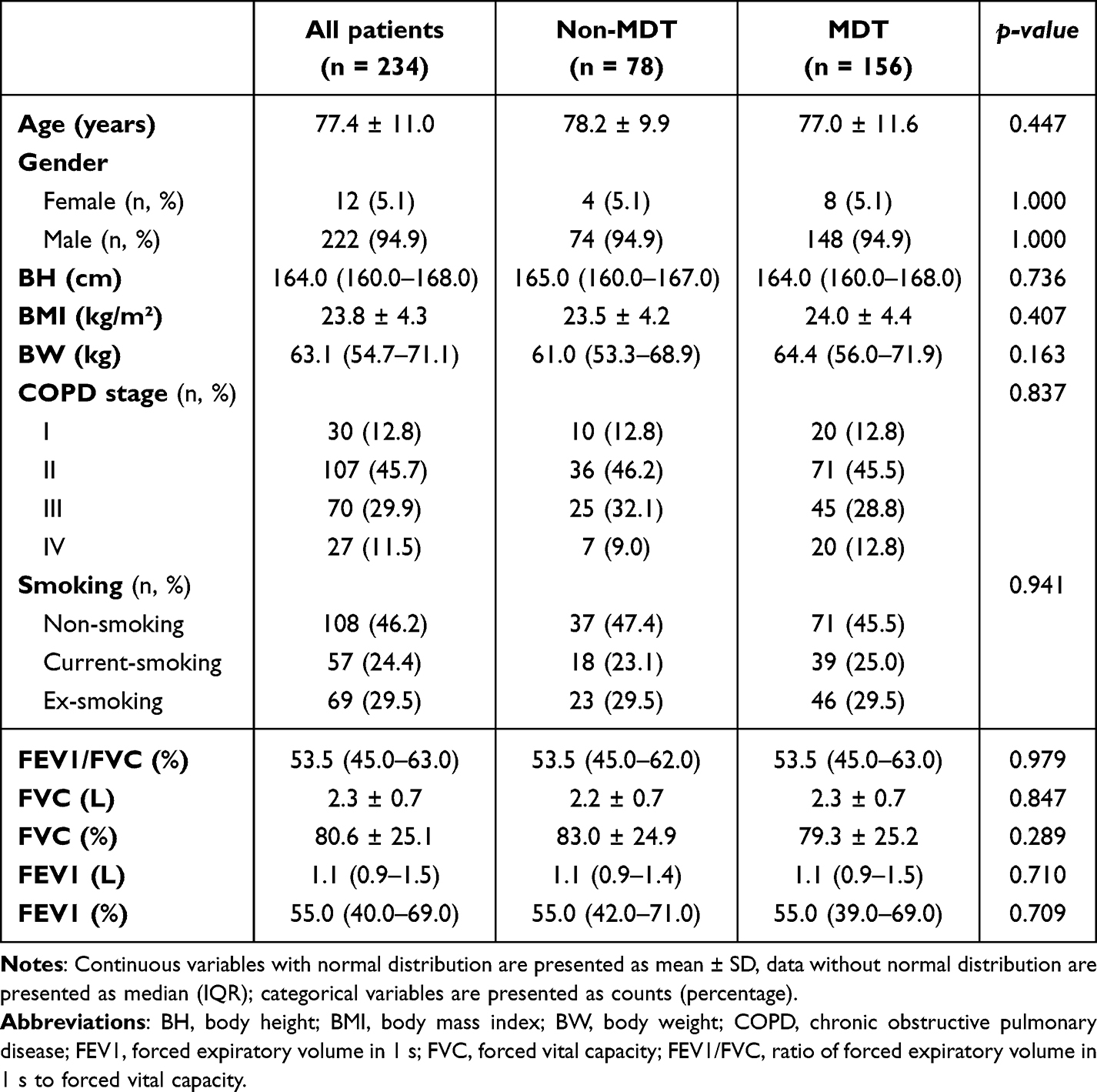 |
Table 2 Demographic and Clinical Differences Between Patients Without and With Multidisciplinary Team (MDT) After Matching |
Comparison of Treatment and Intervention Usage Between Patients Treated without and with MDT After Matching
Table 3 compares treatment and intervention usage between the MDT and non-MDT groups. A higher proportion of patients in the MDT group received inhaled steroids (80.0% vs 59.0%, p = 0.001), overall steroids (96.8% vs 87.2%, p = 0.005), LABA (94.9% vs 71.8%, p < 0.001), LAMA (85.3% vs 61.5%, p < 0.001), and PR (80.8% vs 50.0%, p < 0.001) compared to the non-MDT group. No significant differences were observed between the groups regarding SABA, SAMA, smoking cessation interventions, successful smoking cessation, or influenza vaccination (all p > 0.05). Nutritional intervention usage varied, with a higher percentage of MDT patients with a BMI < 21 kg/m² receiving nutritional intervention than those without (22.2% vs 9.0%, p < 0.001).
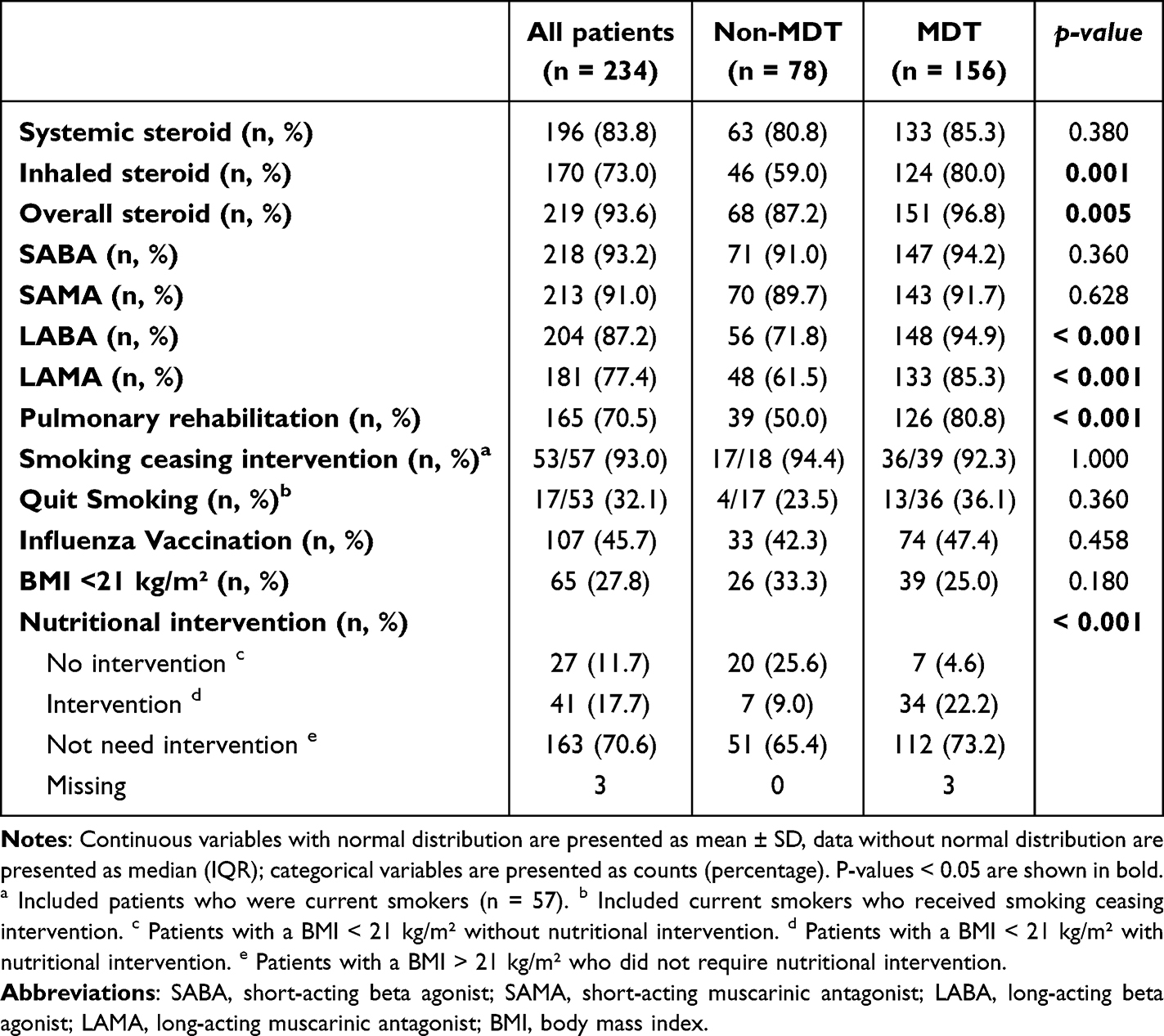 |
Table 3 Comparison of Treatment and Intervention Usage Between Patients Treated Without and With a Multidisciplinary Team After Matching |
Comparison of Clinical Outcomes Between Patients Treated without and with MDT After Matching
Table 4 presents the clinical outcomes of the patients managed with and without MDT. The proportion of BSRS improvement was higher in patients in the MDT group compared to the non-MDT group (40.9% vs 29.7%, p = 0.016). No significant differences were observed in the length of stay, 14-day readmission rates, 30-day emergency visits, or one year survival rates between the two groups (all p > 0.05).
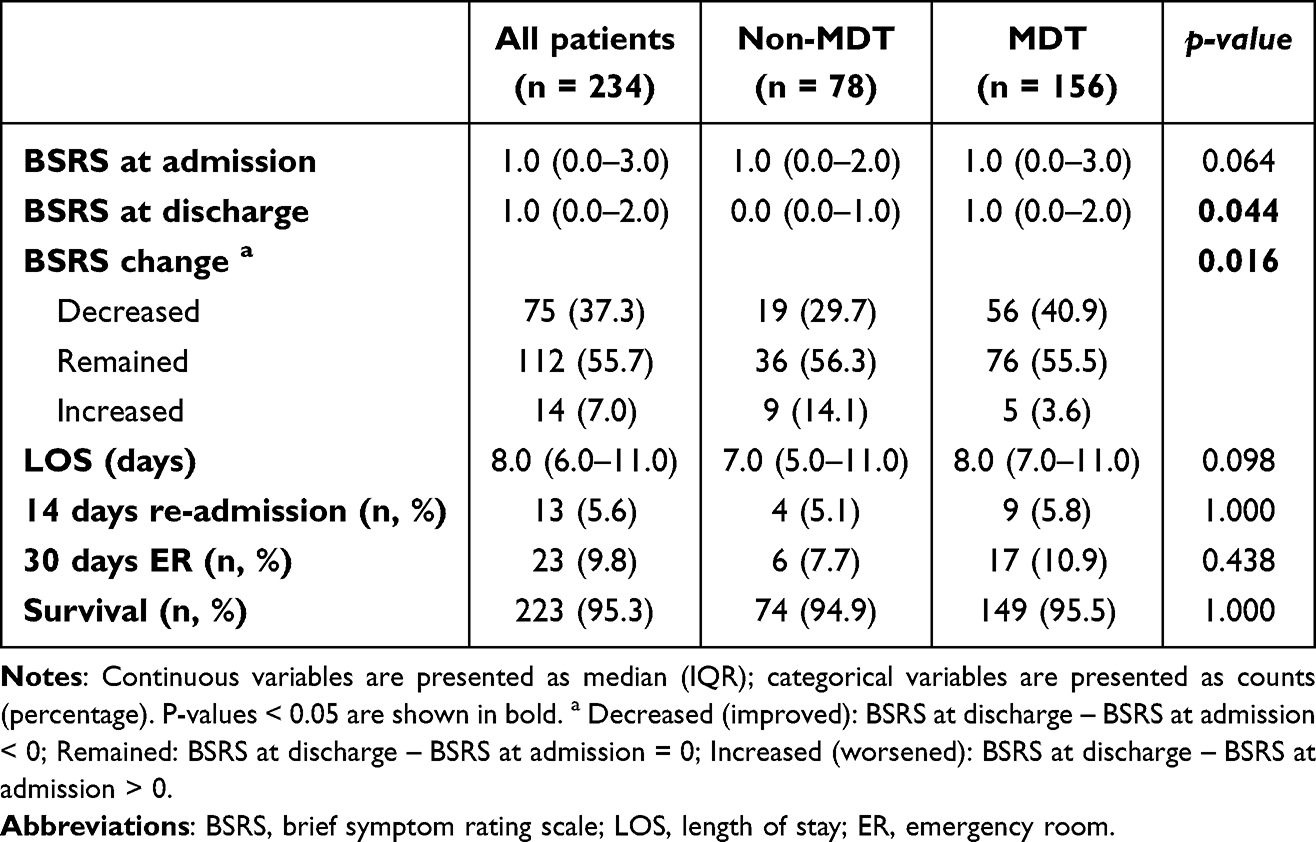 |
Table 4 Comparison of Clinical Outcomes Between Patients Treated Without and With a Multidisciplinary Team After Matching |
Discussion
This study yielded several important and novel findings. The MDT group, supported by a LINE-based communication platform, demonstrated significantly higher rates of standard pharmacological and non-pharmacological treatments, including systemic steroids, ICS, LABA, LAMA, and PR. Furthermore, the MDT group exhibited greater improvement in the BSRS than the non-MDT group. However, no significant differences between the groups were observed in the readmission rates, emergency room visits, or one year survival. These findings emphasize the effectiveness and novelty of the LINE-based MDT model, which represents a significant advancement in optimizing COPD management through enhanced communication and collaboration. The integration of LINE enabled real-time coordination among team members, ensuring timely, tailored interventions that directly addressed each patient’s needs. To our knowledge, this is the first study to show a LINE-based communication platform for COPD management within a MDT setting, marking an important step forward in the use of digital tools.
There have been previous studies on MDT care for patients with stable COPD. A recent Cochrane review of MDT programs for COPD suggested improvements in disease-specific QoL, exercise capacity, hospital admissions, and hospital stay.7 Statistically significant improvements were observed in the MRC Dyspnea Scale at short- and medium-term follow-ups but not at long-term follow-ups.7 No differences were observed in terms of mortality.7 MDT management programs have positively affected PR attendance, self-reported daily activities, and disease knowledge.21 However, there were no significant differences between groups in HRQL, exacerbation rates, or length of hospital stay.21 A study on MDT in primary care led by general practitioners for COPD found no statistically significant differences in the St. George’s Respiratory Questionnaire (SGRQ) and CAT score changes between the MDT and non-MDT groups. The proportion of participants showing improvements in hospital anxiety and depression scale (HADS) scores and modified Medical Research Council (mMRC) grades was also not significantly different between the groups, and the smoking cessation success rates were similar.5 Previous studies on MDT care have shown improvements in disease-specific quality of life, exercise capacity, and hospital admissions; however, findings regarding long-term outcomes, HRQL, exacerbation rates, and hospitalized acute exacerbations remain inconclusive. Although some studies have explored MDT care in patients with stable COPD, research focusing specifically on hospitalized patients with acute exacerbations remains limited.
Only a few review articles have suggested implementing MDT care for hospitalized patients with COPD.10,22 One study showed that daily MDT meetings significantly reduced the hospital stay duration for COPD patients from 5.6 to 3.4 days.22 However, this study excluded patients with known or suspected heart failure and those with a febrile temperature (> 38°C), despite secondary infections being a common cause of COPD exacerbations. Furthermore, the study reported only the length of hospital stay and did not assess any other outcomes.22 Therefore, these results only apply to patients with COPD without heart failure or infection.22 One study showed that patients’ 30-day all-cause readmission rate dropped from 22.7% without bundled care to 14.7% with bundled care.23 In a previous study, we implemented a COPD care bundle for hospitalized patients with reduced readmission rates.24 The 30-day rate dropped from 38.3% to 22.4% post-intervention, with similar reductions at 60 days (40.3% to 13.7%) and 90 days (32.2% to 10.1%).24 Studies suggest that MDT and COPD care bundles significantly reduce hospital stay duration and readmission rates.
This study is the first to explore the use of LINE-based MDT in treating patients with COPD. The COPD Foundation highlighted the importance of digital adaptation in improving usability and enabling healthcare providers to access critical COPD management resources more efficiently.25 Another prior study also revealed the effectiveness of smartphone applications in enhancing COPD management, improving the quality of life, and increasing patients’ knowledge about the disease and its nonpharmacological management.26 A recent review emphasized that integrating simple, scalable, affordable, and future-proof digital solutions into healthcare systems could transform global chronic disease management and optimize patient care and healthcare resources.27 Our study contributes to the growing body of evidence by providing comprehensive insights into the application of LINE-based MDT for COPD care.
Management of COPD is complex and requires both pharmacological and non-pharmacological treatments for comprehensive care.6 The GOLD guidelines recommend long-acting bronchodilators (LABA or LAMA) as first-line therapy, with short-acting bronchodilators (SABA or SAMA) used for immediate relief. ICS was administered to patients with frequent exacerbations or higher eosinophil counts. Triple therapy (LAMA, LABA, and ICS) is recommended for patients with persistent symptoms or frequent exacerbations.6 However, before the introduction of MDT care, we observed low utilization of LABA, LAMA, and ICS. The application of LINE-based MDT significantly improved the use of standard pharmacological treatments. Relying solely on pharmacological agents is insufficient for treating patients with COPD, necessitating several non-pharmacological interventions to enhance treatment options, such as PR.28 One meta-analysis revealed that inpatient PR improved the 6-minute walk distance, quality of life, and lower limb muscle strength, although it did not affect the length of hospital stay.29 Another meta-analysis showed early PR in patients hospitalized for acute exacerbations of COPD. Early PR significantly improved readmission rates, 6-minute walk distance, SGRQ scores, and mMRC dyspnea scale results.30 However, a low participation rate in PR has been observed in patients with acute exacerbations of COPD.31 In the current study, the application of Line-based MDT significantly increased the rates of bronchodilator and steroid use during COPD exacerbation, which are often necessary in these situations. Additionally, there has been an increase in the use of non-pharmacological treatments such as PR.
The integration of mobile apps or devices in chronic lung disease management is expanding.32–36 A randomized trial (RCT) using myCOPD app in patients with COPD showed improvements in CAT scores and inhaler technique, along with trends toward fewer exacerbations and lower readmission risk.32 Another RCT in Germany and Switzerland found that app users with higher adherence had greater exercise capacity gains.33 Additionally, a study using the MyTatva app’s algorithm demonstrated significant improvements in FEV1, body weight, and six-minute walk test performance.34 A real-world study showed that physical activity, tracked via a wearable device, was inversely associated with CAT scores and acute exacerbations.35 A systematic review suggests that wearable interventions significantly improve daily step count and exercise capacity, with the greatest benefits from multi-component interventions combining wearable technology with health coaching or pulmonary rehabilitation.36 Furthermore, previous studies suggested mobile apps beneficial for asthma management in both patients and healthcare professionals.37 These studies underscore the growing potential of mobile apps in improving the management of chronic respiratory diseases. In the context of communication tools, the integration of the LINE app within a MDT for COPD management holds significant potential, as demonstrated by our current study. The use of LINE in this study facilitated real-time communication and coordination among healthcare professionals, leading to higher intervention rates, optimized pharmacological treatment, and enhanced non-pharmacological care.
Limitations of This Study
This study had several limitations. This study was conducted at a single center, which may limit the generalizability of the results to broader clinical settings and diverse patient populations. Moreover, the potential impact of the COVID-19 pandemic on the before-and-after results was not fully accounted in this study. The pandemic significantly disrupted healthcare delivery, leading to changes in patient care practices, treatment protocols, and follow-up schedules, which could have influenced both the management and outcomes of COPD patients.38 The additional strain on healthcare systems, reduced patient access to rehabilitation programs, and delays in elective procedures may have affected the clinical results.38 Furthermore, there was a relatively large number of patients who received the intervention compared to those who did not, which may have introduced selection bias. These factors could have influenced the outcomes and may not have been fully controlled for by the statistics. Despite these limitations, this real-world analysis provides valuable insights into the clinical benefits of a LINE-based MDT approach for managing COPD.
Conclusions
The management of COPD is complex and necessitates a comprehensive approach that integrates both pharmacological and non-pharmacological interventions. The LINE-based MDT, comprising physicians, nurse practitioners, nurses, respiratory therapists, social workers, dietitians, physiotherapists, disease managers, and smoking cessation managers, facilitates a holistic care plan. This study demonstrates that the LINE-based MDT significantly improved adherence to standard pharmacological treatments, including steroids, LABA, LAMA, and PR. Furthermore, the MDT group exhibited notable improvements in BSRS scores. The use of the LINE app also contributed to improved discharge processes and more effective medication management, highlighting its potential in enhancing clinical outcomes. These findings suggest that the LINE-based MDT model has potential to optimize COPD management by improving coordination, communication, and patient care, ultimately fostering better clinical outcomes.
Acknowledgments
This study was supported by grants from Taipei Tzu Chi Hospital and Buddhist Tzu Chi Medical Foundation (TCRD-TPE-111-RT-3(3/3)).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
3. Cheng SL, Chan MC, Wang CC, et al. COPD in Taiwan: a national epidemiology survey. Int J Chron Obstruct Pulmon Dis. 2015;10:2459–2467. doi:10.2147/copd.S89672
4. Jarab AS, Al-Qerem W, Alzoubi KH, et al. Health-related quality of life and its associated factors in patients with chronic obstructive pulmonary disease. PLoS One. 2023;18(10):e0293342. doi:10.1371/journal.pone.0293342
5. Liang J, Abramson MJ, Russell G, et al. Interdisciplinary COPD intervention in primary care: a cluster randomised controlled trial. Eur Respir J. 2019;53(4):1801530. doi:10.1183/13993003.01530-2018
6. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–e8. doi:10.1016/s2213-2600(24)00413-2
7. Poot CC, Meijer E, Kruis AL, Smidt N, Chavannes NH, Honkoop PJ. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;9(9):Cd009437. doi:10.1002/14651858.CD009437.pub3
8. Xu H, Jiang X, Zeng Q, Li R. Application of e-Health tools in the assessment of inhalation therapy adherence in patients with chronic obstructive pulmonary disease: scoping review coupled with bibliometric analysis. Respir Med. 2025;236:107898. doi:10.1016/j.rmed.2024.107898
9. Davies H, Chappell M, Wang Y, et al. myCOPD app for managing chronic obstructive pulmonary disease: a NICE medical technology guidance for a digital health technology. Appl Health Econ Health Policy. 2023;21(5):689–700. doi:10.1007/s40258-023-00811-x
10. Amin AN, Cornelison S, Woods JA, Hanania NA. Managing hospitalized patients with a COPD exacerbation: the role of hospitalists and the multidisciplinary team. Postgrad Med. 2022;134(2):152–159. doi:10.1080/00325481.2021.2018257
11. Culver BH, Graham BL, Coates AL, et al. Recommendations for a standardized pulmonary function report. An official American thoracic society technical statement. Am J Respir Crit Care Med. 2017;196(11):1463–1472. doi:10.1164/rccm.201710-1981ST
12. Yang HF, Chang WW, Chou YH, et al. Impact of background music listening on anxiety in cancer patients undergoing initial radiation therapy: a randomized clinical trial. Radiat Oncol. 2024;19(1):73. doi:10.1186/s13014-024-02460-3
13. Hindelang M, Kirsch F, Leidl R. Effectiveness of non-pharmacological COPD management on health-related quality of life - a systematic review. Expert Rev Pharmacoecon Outcomes Res. 2020;20(1):79–91. doi:10.1080/14737167.2020.1734455
14. Cross AJ, Thomas D, Liang J, Abramson MJ, George J, Zairina E. Educational interventions for health professionals managing chronic obstructive pulmonary disease in primary care. Cochrane Database Syst Rev. 2022;5(5):Cd012652. doi:10.1002/14651858.CD012652.pub2
15. Yang Y, Wei L, Wang S, et al. The effects of pursed lip breathing combined with diaphragmatic breathing on pulmonary function and exercise capacity in patients with COPD: a systematic review and meta-analysis. Physiother Theory Pract. 2022;38(7):847–857. doi:10.1080/09593985.2020.1805834
16. Belli S, Prince I, Savio G, et al. Airway clearance techniques: the right choice for the right patient. Front Med Lausanne. 2021;8:544826. doi:10.3389/fmed.2021.544826
17. Mekal D, Czerw A, Deptala A. Dietary behaviour and nutrition in patients with COPD treated with long-term oxygen therapy. Int J Environ Res Public Health. 2021;18(23):12793. doi:10.3390/ijerph182312793
18. Wang Z, Qiu Y, Ji X, Dong L. Effects of smoking cessation on individuals with COPD: a systematic review and meta-analysis. Front Public Health. 2024;12:1433269. doi:10.3389/fpubh.2024.1433269
19. Guerrero M, Crisafulli E, Liapikou A, et al. Readmission for acute exacerbation within 30 days of discharge is associated with a subsequent progressive increase in mortality risk in COPD patients: a long-term observational study. PLoS One. 2016;11(3):e0150737. doi:10.1371/journal.pone.0150737
20. Schrijver J, Lenferink A, Brusse-Keizer M, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1(1):Cd002990. doi:10.1002/14651858.CD002990.pub4
21. Kruis AL, Boland MR, Assendelft WJ, et al. Effectiveness of integrated disease management for primary care chronic obstructive pulmonary disease patients: results of cluster randomised trial. BMJ. 2014;349(sep10 11):g5392. doi:10.1136/bmj.g5392
22. Sagana RL, Wesorick DH, Byrne BT, et al. Michigan Medicine Clinical Care Guidelines. Care of the Hospitalized Patient With Acute Exacerbation of COPD. Michigan Medicine University of Michigan© Regents of the University of Michigan.; 2022.
23. Gentene AJ, Guido MR, Woolf B, et al. Multidisciplinary team utilizing pharmacists in multimodal, bundled care reduce chronic obstructive pulmonary disease hospital readmission rates. J Pharm Pract. 2021;34(1):110–116. doi:10.1177/0897190019889440
24. Kendra M, Mansukhani R, Rudawsky N, et al. Decreasing hospital readmissions utilizing an evidence-based COPD care bundle. Lung. 2022;200(4):481–486. doi:10.1007/s00408-022-00548-9
25. Thomashow B, Crapo JD, Drummond MB, et al. Introducing the new COPD pocket consultant guide app: can a digital approach improve care? A statement of the COPD foundation. Chronic Obstr Pulm Dis. 2019;6(3):210–220. doi:10.15326/jcopdf.6.3.2018.0167
26. Adida F, Pandia P, Pradana A, et al. Effectiveness of smartphone application in increasing knowledge on COPD and its non-pharmacological management in COPD patients. Narra J. 2023;3(3):e412. doi:10.52225/narra.v3i3.412
27. Watson A, Wilkinson TMA. Digital healthcare in COPD management: a narrative review on the advantages, pitfalls, and need for further research. Ther Adv Respir Dis. 2022;16:17534666221075493. doi:10.1177/17534666221075493
28. Mansoor S, Obaida Z, Ballowe L, et al. Clinical impact of multidisciplinary outpatient care on outcomes of patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:33–42. doi:10.2147/copd.S225156
29. Moecke DP, Zhu K, Gill J, et al. Safety and efficacy of inpatient pulmonary rehabilitation for patients hospitalized with an acute exacerbation of chronic obstructive pulmonary disease: systematic review and meta-analyses. Ann Am Thorac Soc. 2023;20(2):307–319. doi:10.1513/AnnalsATS.202206-545OC
30. Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC. Effects of early pulmonary rehabilitation on hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:881–893. doi:10.2147/copd.S397361
31. Gueçamburu M, Verdy G, Cuadros J, et al. Insufficient pulmonary rehabilitation uptake after severe exacerbation of COPD: a multicentre study in the south west region of France. Int J Chron Obstruct Pulmon Dis. 2024;19:1579–1589. doi:10.2147/copd.S460991
32. North M, Bourne S, Green B, et al. A randomised controlled feasibility trial of E-health application supported care vs usual care after exacerbation of COPD: the RESCUE trial. NPJ Digit Med. 2020;3(1):145. doi:10.1038/s41746-020-00347-7
33. Gloeckl R, Spielmanns M, Stankeviciene A, et al. Smartphone application-based pulmonary rehabilitation in COPD: a multicentre randomised controlled trial. Thorax. 2024. doi:10.1136/thorax-2024-221803
34. Sharma P, Gharia M, Aswal D, et al. Development of an algorithm impacting COPD care through personalized nutrition and IoT-based monitoring. J Health Popul Nutr. 2025;44(1):14. doi:10.1186/s41043-024-00727-9
35. Boesch M, Baty F, Bilz S, Brutsche MH, Rassouli F. Tracking real-world physical activity in chronic obstructive pulmonary disease over one year: results from a monocentric, prospective, observational cohort study. Int J Chron Obstruct Pulmon Dis. 2024;19:1921–1929. doi:10.2147/copd.S469984
36. Shah AJ, Althobiani MA, Saigal A, Ogbonnaya CE, Hurst JR, Mandal S. Wearable technology interventions in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. NPJ Digit Med. 2023;6(1):222. doi:10.1038/s41746-023-00962-0
37. Alladina J, Moschovis PP, Gandhi HN, et al. Observational study of the Amaze™ asthma disease management platform. Digit Health. 2024;10:20552076241282380. doi:10.1177/20552076241282380
38. Fekadu G, Bekele F, Tolossa T, et al. Impact of COVID-19 pandemic on chronic diseases care follow-up and current perspectives in low resource settings: a narrative review. Int J Physiol Pathophysiol Pharmacol. 2021;13(3):86–93.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characteristics and Quality of Life of Patients with COPD with Different Degrees of Exercise-Induced Desaturation on Six-minute Walk Test
Gao B, Wang S, Zhao L, Liao H, Qumu S, Wang P, Yang T, Jiang S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2381-2391
Published Date: 14 July 2025
The Humanistic and Economic Burden of COPD Patients in Urban China: A Propensity Score Matching Study
Dou L, Zheng Y, Feng J, Huang Z, Qin F, Gao M, Li S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2993-3004
Published Date: 27 August 2025
An Evidence Summary of Health Education in Chronic Obstructive Pulmonary Disease: A Practice-Oriented Assessment with Inter-Rater Reliability
Zhan M, Chen J, Chen C, Zhou J, Zhang H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:614212
Published Date: 15 July 2026
Carbon Emissions and Treatment Efficiency in Chronic Obstructive Pulmonary Disease: The Impact of Inhaled Bronchodilators and Corticosteroids
Jao LY, Yang MC, Lee C, Wu YK, Huang KL, Su WL, Huang CY, Tzeng IS, Lan CC
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:617602
Published Date: 17 July 2026