Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Carbon Emissions and Treatment Efficiency in Chronic Obstructive Pulmonary Disease: The Impact of Inhaled Bronchodilators and Corticosteroids
Authors Jao LY, Yang MC ![]() , Lee C
, Lee C ![]() , Wu YK
, Wu YK ![]() , Huang KL, Su WL
, Huang KL, Su WL ![]() , Huang CY, Tzeng IS
, Huang CY, Tzeng IS ![]() , Lan CC
, Lan CC ![]()
Received 16 April 2026
Accepted for publication 18 June 2026
Published 17 July 2026 Volume 2026:21 617602
DOI https://doi.org/10.2147/COPD.S617602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Zijing Zhou
Lun-Yu Jao,1– 3 Mei-Chen Yang,1,2 Chung Lee,1,2 Yao-Kuang Wu,1,2 Kuo-Liang Huang,1,2 Wen-Lin Su,1,2 Chun-Yao Huang,1,2 I-Shiang Tzeng,4 Chou-Chin Lan1,2
1Division of Pulmonary Medicine, Department of Internal Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan; 2School of Medicine, Tzu Chi University, Hualien, Taiwan; 3Division of Hospital Medicine, Department of Internal Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan; 4Department of Research, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan
Correspondence: Chou-Chin Lan, Division of Pulmonary Medicine, Department of Internal Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan, Tel +886-2-6628-9779 ext. 8119, Fax +886-2-6628-9009, Email [email protected]
Background: Inhaled therapies are essential for chronic obstructive pulmonary disease (COPD) management but also contribute to healthcare-related carbon emissions. Real-world evidence linking inhaler-related carbon burden to clinical outcomes remains limited. This study evaluated the relationship between inhaler-related CO2 emissions and clinical effectiveness of different treatment regimens.
Methods: This retrospective single-center observational study included patients with COPD. Patients were categorized into four groups based on the inhaled therapy: long-acting muscarinic antagonists (LAMA) monotherapy, LAMA/long-acting β 2-agonists (LABA), LABA/inhaled corticosteroids (ICS), and triple therapy (LAMA/LABA/ICS). Clinical outcomes, including pulmonary function test (PFT) parameters and health-related quality of life (HRQL), were assessed over one year. Total inhaler-related CO2 emissions were calculated using published conversion factors. Emission-adjusted outcomes were derived to evaluate the clinical benefits per unit of CO2 emission.
Results: Clinical improvements in HRQL and PFT were comparable across groups, with no significant differences in ΔFEV1, ΔFVC, or ΔCAT. However, CO2 emissions differed significantly, being the lowest in the LAMA monotherapy group and the highest in the LABA/ICS and triple therapy groups (p < 0.001). Emission-adjusted analysis demonstrated that lower-intensity regimens, particularly LAMA monotherapy, were associated with more favorable CO2-adjusted treatment efficiency, particularly in ΔmMRC/CO2 (p = 0.001) and ΔFEV1 (%)/CO2 (p = 0.026), indicating higher clinical benefit per unit carbon emission. After adjustment for baseline severity-related variables, including age, sex, smoking status, baseline FEV1, baseline CAT score, and baseline mMRC score, higher-intensity regimens remained associated with lower CO2-adjusted pulmonary function improvement compared with LAMA monotherapy.
Conclusion: High-intensity regimens were associated with substantially increased inhaler-related CO2 emissions. Although major clinical outcomes were generally comparable across groups, lower-emission regimens showed relatively more favorable CO2-adjusted outcomes in this cohort. These findings highlight the importance of balancing clinical effectiveness with environmental considerations while maintaining guideline-based, individualized COPD management according to disease severity and clinical needs.
Keywords: chronic obstructive pulmonary disease, inhaler, carbon emissions, treatment efficiency, pulmonary function, health-related quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health burden and a leading cause of morbidity and mortality worldwide, accounting for approximately 3.7 million deaths each year.1 The disease is characterized by persistent respiratory symptoms and progressive airflow limitation, leading to substantial healthcare utilization and economic burdens.2 COPD profoundly compromises patient outcomes, leading to impaired quality of life, reduced functional capacity, and an increased risk of mortality.3 Management of COPD requires comprehensive and sustained pharmacological therapy, particularly with bronchodilators.2
Bronchodilators constitute the cornerstone of COPD therapy and provide sustained improvement in airflow limitation.2 Long-acting bronchodilators, including long-acting muscarinic antagonists (LAMA) and long-acting β2-agonists (LABA), are the mainstay of maintenance treatment, improve lung function, reduce symptoms, decrease exacerbation risk, and enhance health-related quality of life (HRQL).2,4 In selected patients, inhaled corticosteroids (ICS), typically in combination with LABA or as part of triple therapy (LAMA/LABA/ICS), further reduce exacerbations and provide additional clinical and HRQL benefits.2,5
The environmental impact of healthcare systems has gained increasing attention in recent years.6 Inhaler devices are recognized as contributors to the carbon footprint of respiratory care, with substantial variations in greenhouse gas emissions across device types.6–8 This environmental impact has important public health implications, as inhaler-related emissions contribute to climate change, which is associated with worsening air quality, increased frequency of extreme weather events, and a higher risk of respiratory exacerbations.7 Reflecting these concerns, several guidelines have begun to incorporate environmental considerations into inhaler prescriptions.7,9 This underscores a critical paradox in respiratory care: although inhalers are essential for disease management, their cumulative environmental impact may indirectly contribute to worsening respiratory health outcomes.7,9
Both clinical effectiveness and environmental impact are important considerations when selecting inhaler therapies. However, current evidence is largely based on lifecycle or modeling studies with limited real-world, patient-level data.6–8 Moreover, previous studies have primarily focused on differences between inhaler device types, whereas treatment regimens in COPD often reflect differences in disease severity, medication intensity, and inhaler utilization patterns in real-world clinical practice.6–8 These factors may substantially influence both cumulative carbon emissions and clinical outcomes. Therefore, evaluating carbon emissions across treatment regimens may provide more clinically relevant information regarding the balance between therapeutic benefit and environmental burden in routine COPD management. Accordingly, this study aimed to quantify inhaler-related CO2 emissions in patients with COPD and compare emission profiles across different treatment regimens to evaluate both clinical benefits and carbon burden.
Materials and Methods
Study Design and Population
This retrospective observational study was conducted at Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan. Patients were enrolled during the study period from January 1, 2025 to December 31, 2025. The patient selection process is summarized in Supplementary Figure 1. Adult patients (aged ≥18 years) with COPD were included in this study. Patients were eligible for inclusion if they had a confirmed diagnosis of COPD based on clinical evaluation and spirometric criteria, with available medical records including treatment details, HRQL assessments, and pulmonary function test (PFT) data during the study period. Patients were excluded if they had incomplete clinical data, no follow-up assessments, or were receiving long-term mechanical ventilation or palliative care at baseline. Patients were categorized into four groups based on their inhaled pharmacological regimens: Group 1, LAMA monotherapy; Group 2, combined LAMA and LABA; Group 3, combined LABA and ICS; and Group 4, triple therapy (LAMA/LABA/ICS). Patient grouping was based on the inhaled treatment regimen that was maintained for the majority of the follow-up period rather than solely on the baseline regimen. Specifically, patients were classified into the treatment group corresponding to the inhaled regimen used for more than two-thirds of the one-year follow-up period (ie, >8 months). Treatment escalation, de-escalation, or switching during follow-up was allowed in real-world clinical practice. However, all inhalers used during the study period were included in the calculation of cumulative CO2 emissions regardless of subsequent treatment changes.
The study protocol was approved by the Institutional Review Board of Taipei Tzu Chi Hospital (IRB No. 14-IRB 106) and all procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients for review of their medical records and use of anonymized clinical data for research purposes. All patient information was de-identified prior to analysis, and confidentiality of patient data was strictly maintained throughout the study. This study was implemented as part of the Disease Specific Care–Chronic Obstructive Pulmonary Disease certification program, reflecting real-world quality improvement practices in COPD management.
Patients were followed for one year to assess outcomes. Follow-up assessments in this retrospective study were conducted as part of routine clinical care and the Disease Specific Care–Chronic Obstructive Pulmonary Disease certification program at our institution. Patients were regularly followed at outpatient clinics according to standard management practice, including scheduled clinical evaluations, inhaler prescription records, HRQL assessments, and pulmonary function testing. Clinical data were retrospectively collected from the electronic medical record system. Patients without sufficient follow-up data during the study period were excluded from the analysis.
Changes in clinical outcomes, including PFT parameters and HRQL scores, were assessed by comparing baseline and one-year follow-up data within each treatment group. Total CO2 emissions were calculated for each patient during the study period. Between-group differences in outcome changes were also analyzed to evaluate the relative effectiveness of the different inhaled regimens.
Data Collection
Demographic and clinical data, including age, sex, height, weight, body mass index, smoking status, and HRQL, were collected from electronic medical records. HRQL was assessed using the COPD Assessment Test (CAT), modified Medical Research Council (mMRC) dyspnea scale, and Brief Symptom Rating Scale (BSRS-5), along with PFT recorded at baseline and follow-up. The CAT is an 8-item questionnaire that assesses the impact of COPD on health status, with higher scores indicating worse symptoms.10 The mMRC dyspnea scale grades the severity of breathlessness from 0 to 4 based on functional limitations, with higher scores indicating a greater severity of dyspnea.11 The BSRS-5 is a 5-item instrument evaluating psychological distress, including anxiety, depression, hostility, inferiority, and insomnia, with higher scores indicating greater distress.12 PFTs were performed by trained technicians in accordance with the guidelines of the American Thoracic Society using a spirometer (Medical Graphics Corporation, St. Paul, Minnesota, USA).13 Measurements included forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and the FEV1/FVC ratio. The severity of airflow obstruction was assessed based on the FEV1 percentage (FEV1%) of predicted values.13 Patients were classified into Global Initiative for Chronic Obstructive Lung Disease (GOLD) Groups A, B, and E according to symptom burden and exacerbation history, with Group A representing low symptoms and low exacerbation risk, Group B representing higher symptom burden, and Group E representing frequent exacerbations.2
Estimation of Inhaler-Related Carbon Emissions
Inhaler-related carbon dioxide equivalent (CO2-eq) emissions were estimated based on patient inhaler use over the preceding year. Total CO2 emissions were calculated as the cumulative sum of all inhalers used during this period. Emission estimates were derived using previously published conversion factors for inhaler-related carbon footprint.14–17 Berotec® pressurized metered-dose inhaler (pMDI, 200 puffs) has a carbon footprint of 16.484 kg CO2-eq per inhaler.14 Among ICS+LABA combination therapies, Symbicort® pMDI (MDI, 120 puffs) generates 34.400 kg CO2-eq per inhaler, whereas Foster® pMDI and Seretide® Evohaler (pMDI, 120 puffs) generate 14.153 and 19.000 kg CO2-eq, respectively.14 Trimbow® pMDI (MDI, 120 puffs) has emissions of 14.5 kg CO2-eq.13 Dry Powder Inhaler (DPI) devices such as Relvar® Ellipta (30–60 puffs), Anoro® Ellipta (30 puffs), Trelegy® Ellipta (30 puffs), and Ultibro® Breezhaler (30 puffs) have lower emissions of approximately 0.4–0.8 kg CO2-eq per inhaler.14–16 Soft mist inhalers (SMIs), including Spiriva® Respimat and Spiolto® Respimat (both 60 puffs), have emissions of approximately 0.775 kg CO2-eq per inhaler.14,17
Clinical and Pulmonary Outcomes
Treatment-related outcomes were evaluated by assessing changes in HRQL and PFT, calculated as the difference between follow-up and baseline values (Δ). To evaluate treatment efficiency relative to environmental impact, CO2 emission–adjusted outcomes were calculated by normalizing clinical changes to total CO2 emissions, expressed as ratios such as ΔCAT/CO2 emission, ΔmMRC/CO2 emission, and ΔFEV1/CO2 emission. In this study, “treatment efficiency” refers to the magnitude of clinical or pulmonary function improvement achieved per unit of inhaler-related CO2 emission. For symptom-related scores, including CAT, mMRC, and BSRS-5, more negative values indicate greater clinical improvement per unit of CO2 emission, whereas for pulmonary function parameters, higher positive values indicate greater pulmonary improvement per unit of CO2 emission.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation, and categorical variables as counts and percentages. Comparisons across groups were performed using one-way analysis of variance for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables, as appropriate. When significant differences were detected, post hoc comparisons were conducted using the Games–Howell test. To control for potential confounding factors, multivariable linear regression analysis was additionally performed, adjusting for age, sex, smoking status, baseline FEV1, baseline CAT score, and baseline mMRC score. Adjusted associations between inhaled treatment groups and clinical outcomes were evaluated using regression coefficients with corresponding 95% confidence intervals and p-values. Statistical significance was defined as a two-sided p-value of < 0.05. Statistical analyses were performed using the SPSS software (IBM Corp., Armonk, NY, USA).
Results
Clinical and demographic variables were compared across the four treatment groups among the 148 patients included in the final analysis: Group 1 (n = 9), Group 2 (n = 51), Group 3 (n = 15), and Group 4 (n = 73). The baseline characteristics are summarized in Table 1. Significant differences were observed in terms of age, sex, and smoking status. Group 4 patients were older (73.42 ± 9.27 years), while Group 3 had the lowest mean age (65.67 ± 12.49 years; p = 0.035). Male predominance was highest in Group 4 (95.9%) and lowest in Group 3 (66.7%, p = 0.008). Smoking status showed a higher proportion of current smokers in Group 3 (40.0%, p = 0.020). No significant differences were found in height, weight, or body mass index (all p > 0.05). Group 4 had lower FEV1/FVC and FEV1 values than Groups 1–3 (both p < 0.001). GOLD stage distribution also differed across groups, with Group 4 showing a higher proportion of patients classified as GOLD Stage E (27.4%), whereas no patients in Group 1 were classified as Stage E. In addition, prior exacerbation-related emergency room visits within 1 year were more frequent in Group 4 (30.1%) than in the other groups (p = 0.001). In Group 1, all patients received Spiriva Respimat (9, 100%). In Group 2, DPI devices were predominant, with Anoro Ellipta DPI (29, 56.9%) and Ultibro Breezhaler DPI (9, 17.6%) accounting for 74.5% of prescriptions, while Spiolto Respimat accounted for 25.5% (13 patients). In Group 3, pMDI therapies were predominant (86.7%), mainly Symbicort pMDI (7, 46.7%) and Foster pMDI (5, 33.3%), whereas Relvar Ellipta DPI was used in 13.3% of patients (2 patients). In Group 4, pMDI-containing regimens accounted for 65.7% of prescriptions, including Trimbow pMDI (27, 37.0%), Seretide pMDI plus Spiriva Respimat (10, 13.7%), Symbicort pMDI plus Spiriva Respimat (10, 13.7%), and Anoro Ellipta plus Seretide pMDI (1, 1.4%), while DPI-only regimens accounted for 34.3%, primarily Trelegy Ellipta DPI (24, 32.9%) and Relvar Ellipta plus Spiriva Respimat (1, 1.4%).
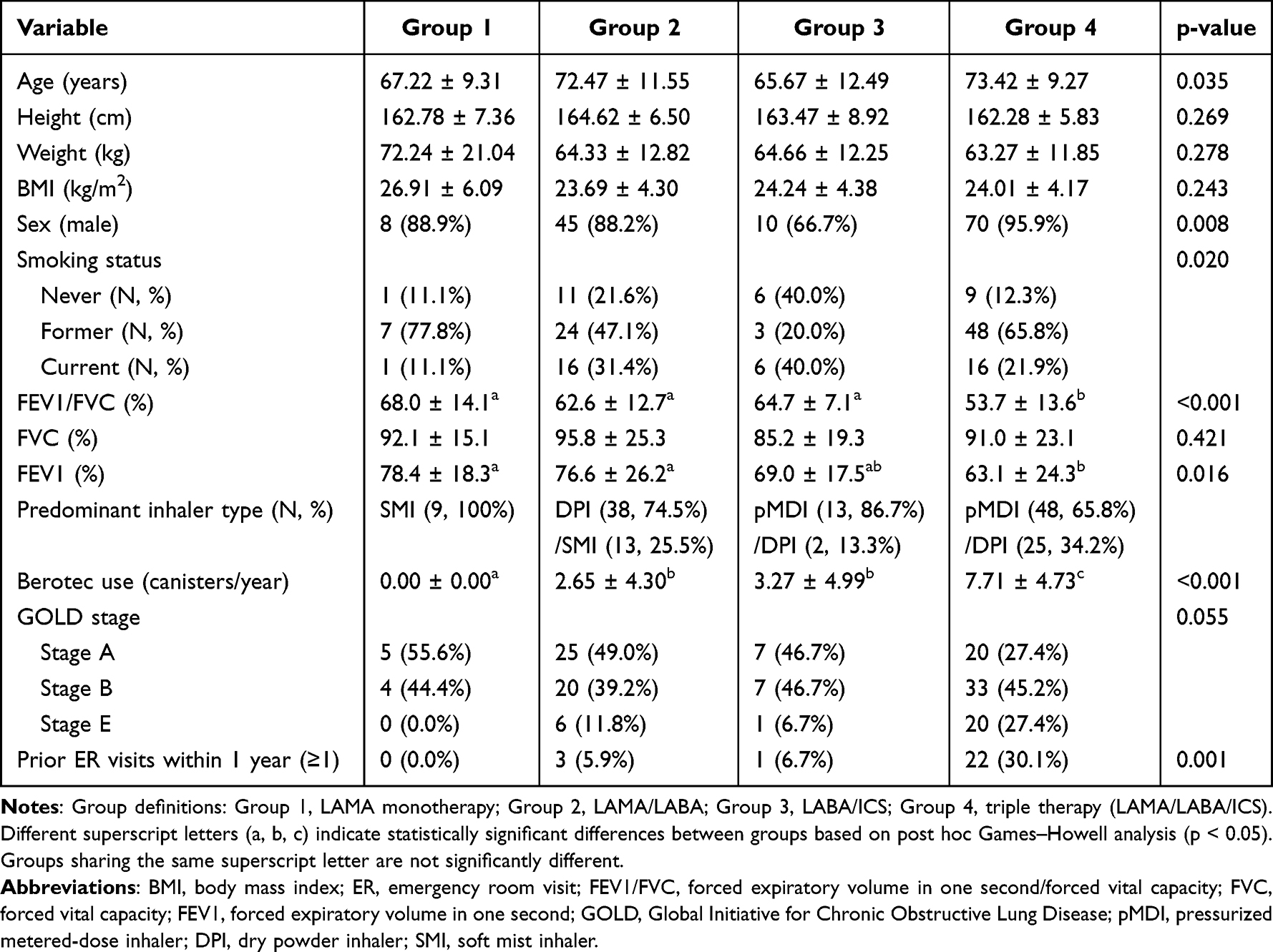 |
Table 1 Baseline Characteristics Across Groups |
The HRQL outcomes are presented in Table 2. CAT and BSRS-5 scores showed no significant differences among groups at baseline, follow-up, or in change (Δ) (all p > 0.05). In contrast, mMRC scores differed significantly at both baseline and follow-up (p < 0.001), with Group 4 showing greater dyspnea severity; however, the magnitude of improvement (ΔmMRC) was similar across groups.
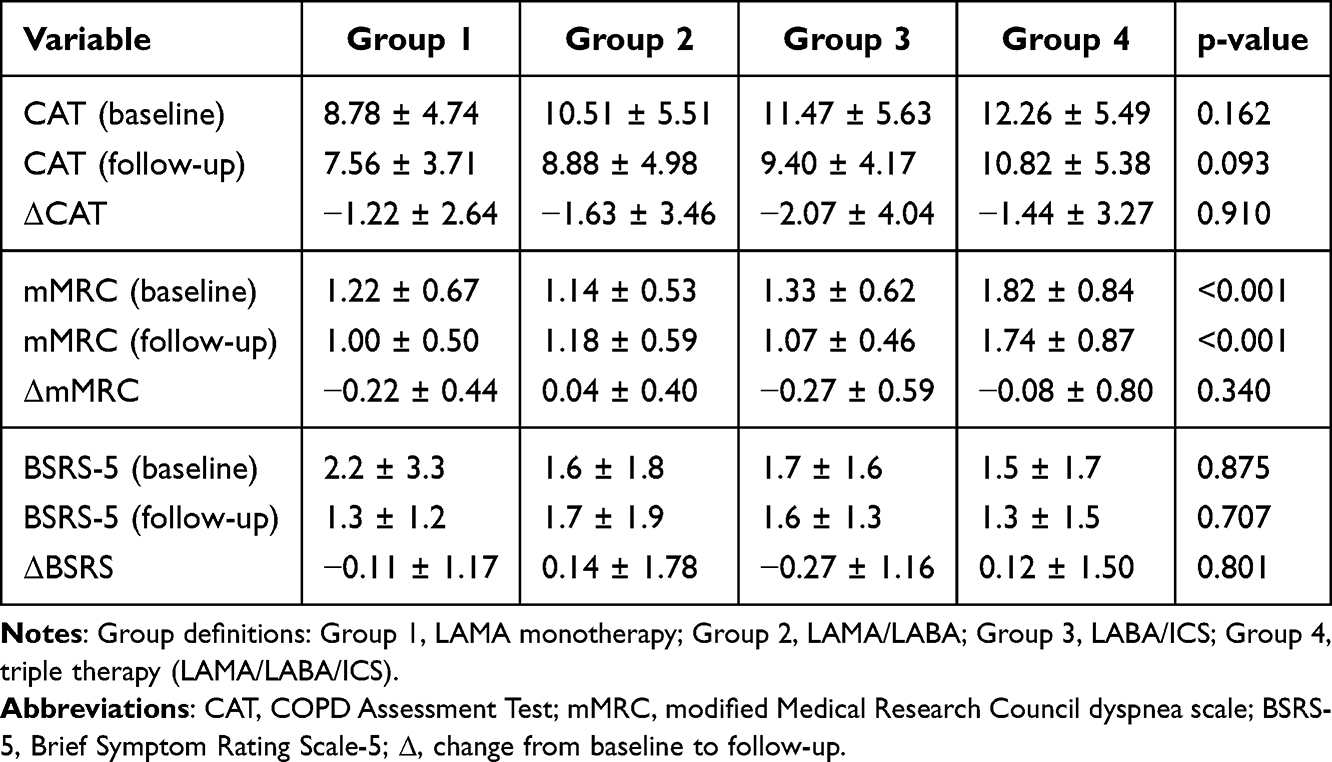 |
Table 2 HRQL Outcomes Across Groups |
PFT outcomes are presented in Table 3. At baseline, Group 4 had lower FEV1/FVC, FVC, and FEV1 values (all p < 0.05). After treatment, Group 4 continued to exhibit significantly lower FEV1/FVC, FEV1, and FEV1 (%) than the other groups (p < 0.05). Regarding changes over time, no significant between-group differences were observed in ΔFEV1/FVC, ΔFVC, or ΔFEV1.
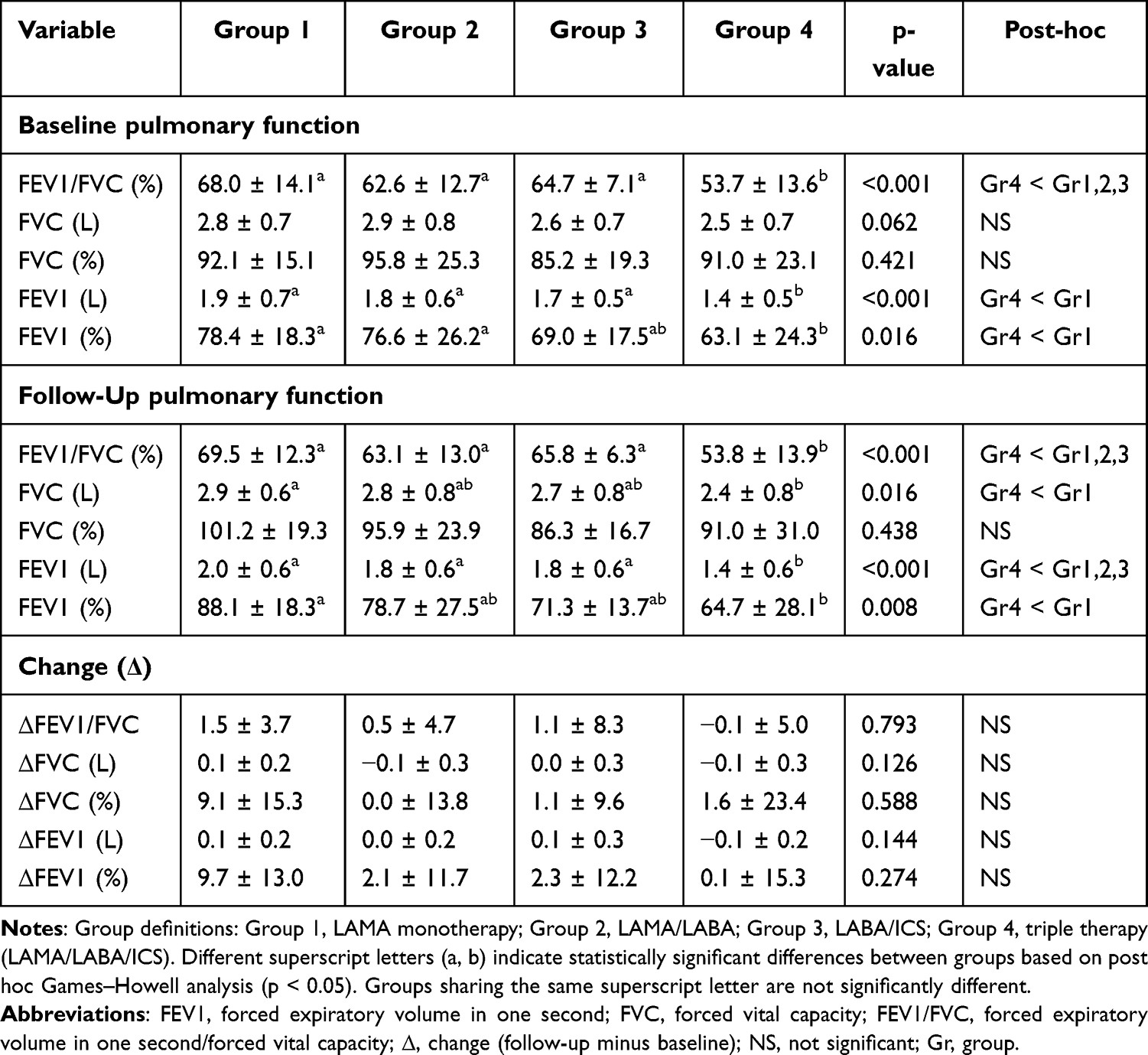 |
Table 3 Pulmonary Function Across Groups |
Figure 1 illustrates CO2 emissions across the four groups. Total CO2 emissions differed significantly (8.78 ± 0.87 kg CO2-eq in Group 1, 63.11 ± 86.55 kg CO2-eq in Group 2, 322.89 ± 174.79 kg CO2-eq in Group 3, and 271.55 ± 127.10 kg CO2-eq in Group 4; p < 0.001), with Group 3 and Group 4 showing markedly higher levels than Group 1 and Group 2. Berotec-related CO2 emissions also differed significantly (0.00 ± 0.00 kg CO2-eq in Group 1, 43.63 ± 70.85 kg CO2-eq in Group 2, 53.85 ± 82.29 kg CO2-eq in Group 3, and 128.09 ± 77.92 kg CO2-eq in Group 4; p < 0.001), with the highest levels observed in Group 4. Non-Berotec CO2 emissions also differed significantly, with Group 3 showing the highest levels, followed by Group 4 (8.78 ± 0.87 kg CO2-eq in Group 1, 19.47 ± 34.68 kg CO2-eq in Group 2, 269.04 ± 139.17 kg CO2-eq in Group 3, and 142.73 ± 118.07 kg CO2-eq in Group 4; p < 0.001).
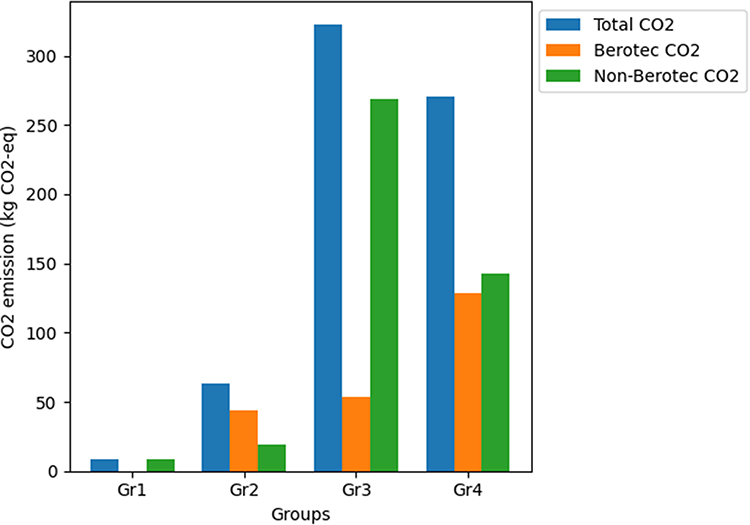 |
Figure 1 Carbon dioxide emissions across treatment groups. Groups 3 and 4 demonstrates markedly higher levels compared with Gr1 and Gr2 (p < 0.001). Berotec-related CO2 emissions were highest in Gr4, indicating a substantial contribution from short-acting bronchodilator use. In contrast, non-Berotec CO2 emissions were highest in Gr3, followed by Gr4, suggesting that non-bronchodilator sources were the primary drivers of elevated emissions in Gr3. Data are presented as mean ± standard deviation. Statistical comparisons were performed using a one-way analysis of variance. Abbreviations: CO2, carbon dioxide; Gr, group. |
CO2 emission–adjusted clinical and PFT responses are presented in Table 4. Among symptom-related outcomes, ΔmMRC/CO2 differed significantly across groups (−0.028 ± 0.056 in Group 1, 0.008 ± 0.029 in Group 2, −0.007 ± 0.027 in Group 3, and −0.0002 ± 0.0026 in Group 4; p = 0.001), whereas ΔCAT/CO2 and ΔBSRS/CO2 showed no significant between-group differences. For PFT responses, most parameters, including ΔFEV1/FVC/CO2, ΔFVC/CO2, and ΔFEV1/CO2, did not differ significantly across groups. However, ΔFEV1 (%)/CO2 showed a significant difference (p = 0.026), with Group 1 showing greater improvement per unit CO2 emission compared with Groups 3 and 4.
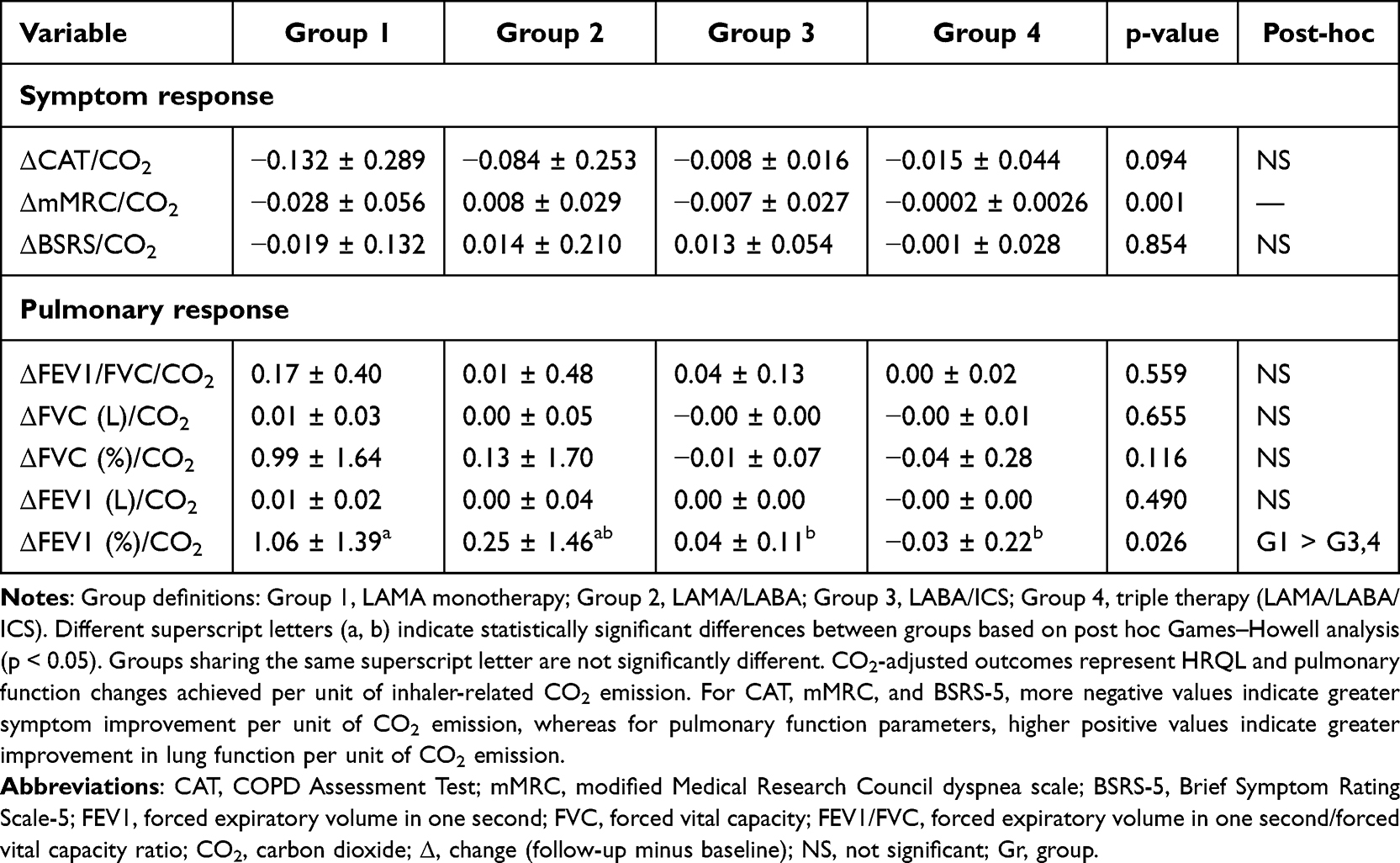 |
Table 4 CO2 Emission-Adjusted Clinical and Pulmonary Responses Across Groups |
To control for potential confounding factors and baseline disease severity differences among groups, multivariable linear regression analyses were additionally performed adjusting for age, sex, smoking status, baseline FEV1, baseline CAT score, and baseline mMRC score. After adjustment, Groups 2, 3, and 4 remained independently associated with lower ΔFEV1 (%)/CO2 compared with Group 1. The regression coefficients compared with Group 1 were −0.89 for Group 2 (p = 0.018), −1.08 for Group 3 (p = 0.013), and −1.23 for Group 4 (p = 0.001), respectively. Similarly, for ΔmMRC/CO2, Groups 2, 3, and 4 remained independently associated with higher ΔmMRC/CO2 compared with Group 1. The regression coefficients compared with Group 1 were 0.032 for Group 2 (p = 0.001), 0.022 for Group 3 (p = 0.033), and 0.028 for Group 4 (p = 0.002), respectively. Detailed regression results are presented in Supplementary Table 1.
Discussion
This study provides novel real-world evidence highlighting the balance between clinical effectiveness and environmental impact in COPD management. Despite comparable improvements in HRQL and PFT across treatment groups, substantial differences in CO2 emissions were observed, with higher-intensity regimens, particularly LABA/ICS and triple therapy, associated with markedly greater carbon burden. CO2 emission–adjusted outcomes suggested that LAMA monotherapy was associated with greater clinical improvement per unit of carbon emitted in this cohort, particularly in ΔmMRC/CO2 and ΔFEV1%/CO2. These associations remained significant after adjustment for age, sex, smoking status, baseline FEV1, baseline CAT score, and baseline mMRC score, supporting the robustness of the observed associations despite baseline differences among groups.
The observed differences in carbon emissions are largely attributable to the inhaler device characteristics. The MDI-containing regimens, which were more prevalent in Group 3, contributed substantially to higher emissions owing to propellant-related greenhouse gas release, whereas the DPI and SMI devices had lower lifecycle emissions.14–17 In addition, higher reliance on short-acting bronchodilators in Group 4 further increased carbon burden. These results are consistent with previous lifecycle and modeling studies but extend existing knowledge by demonstrating these differences in a real-world clinical setting.14–17
According to the current treatment guidelines, patients with more severe symptoms or frequent exacerbations are more likely to receive intensified therapy, including ICS-containing regimens.2 In this study, patients receiving triple therapy had worse baseline lung function, higher dyspnea scores and more exacerbation, consistent with more advanced disease. Therefore, these findings should be interpreted cautiously because baseline disease severity differed across treatment groups. These patients exhibited a more severe baseline status, the magnitude of clinical improvement was not significantly greater than that in the other groups, suggesting that the observed clinical improvements were not proportionally greater despite increased baseline disease severity. In contrast, patients in Group 1, who had milder disease and did not require short-acting bronchodilators such as Berotec®, achieved favorable CO2-adjusted outcomes, including ΔmMRC/CO2 and ΔFEV1 (%)/CO2. These findings may suggest that, in clinically stable patients with milder disease, lower-emission treatment strategies may still provide acceptable clinical outcomes in selected patients with milder disease. This highlights the importance of individualized treatment strategies that balance disease severity, expected clinical benefits, and environmental impact.
Climate change and healthcare-related greenhouse gas emissions have emerged as important public health concerns, particularly in patients with chronic respiratory diseases.18 Healthcare systems are estimated to contribute approximately 5% of global greenhouse gas emissions, and inhaler therapies represent a notable component of the respiratory care carbon footprint.18,19 Increased greenhouse gas emissions contribute to climate change, worsening air pollution, rising ambient temperatures, and more frequent extreme environmental events, all of which have been associated with increased respiratory symptoms, exacerbations, and healthcare utilization in patients with asthma and COPD.20 Optimizing inhaler strategies may therefore provide dual benefits by maintaining disease control while simultaneously reducing environmental burden. In particular, carbon-conscious prescribing approaches, including appropriate selection of lower-emission inhaler devices and reduction of unnecessary rescue inhaler overuse, may help decrease avoidable healthcare-related emissions without compromising patient care.10 From a broader population-health perspective, improving respiratory disease control may itself reduce downstream environmental impact by lowering exacerbations, emergency visits, and hospitalizations, which are associated with substantially greater healthcare-related carbon emissions.21
From clinical and policy perspectives, these findings underscore the importance of integrating environmental considerations into COPD management.22 While pharmacological intensification remains essential for patients with more severe diseases, optimizing inhaler selection and avoiding unnecessary high-emission devices may improve carbon efficiency without compromising clinical outcomes.23 This aligns with the emerging recommendations that advocate environmentally sustainable prescription practices. Such efforts are critical for developing carbon-conscious, patient-centered treatment strategies in respiratory medicine.24 These findings support consideration of environmental impact during inhaler selection in COPD management. Treatment decisions should remain individualized according to disease severity, symptom burden, and exacerbation risk. Appropriate use of lower-emission inhaler devices may help reduce healthcare-related carbon emissions in selected patients.
Limitations of the Study
This study has some limitations. First, this was a single-center retrospective study, which may limit the generalizability of the findings and introduce potential selection bias. Second, CO2 emission estimates were derived from published conversion factors rather than direct measurements and therefore may not fully capture real-world variability in inhaler use, adherence, and disposal patterns, or other healthcare-related sources of carbon burden, such as exacerbation-related emergency visits and hospitalizations. Third, treatment allocation was not randomized, and baseline differences in disease severity across groups, particularly in lung function and dyspnea severity, may have influenced both clinical outcomes and emission profiles, resulting in potential residual confounding. Although additional multivariable analyses adjusting for age, sex, smoking status, baseline FEV1, baseline CAT score, and baseline mMRC score were performed, unmeasured confounding factors may still exist. In addition, the relatively small sample size in certain groups, particularly the LAMA monotherapy group, may have limited statistical power and affected the stability of between-group comparisons. Finally, the one-year follow-up period limited the assessment of long-term clinical outcomes and environmental impact. Therefore, the findings of this study should be interpreted as exploratory and hypothesis-generating.
Conclusions
In patients with COPD, high-intensity regimens, particularly those involving greater use of MDIs, were associated with increased CO2 emissions. Treatment efficiency, defined as clinical improvement per unit of CO2 emission, appeared to be more favorable in patients with milder disease receiving lower-intensity regimens, particularly LAMA monotherapy. These findings highlight the importance of balancing clinical effectiveness with the environmental impact of treatment selection. Incorporating carbon-conscious prescribing strategies may help optimize patient outcomes while reducing the environmental burden of respiratory care.
Funding
This study was funded by institutional research grants (grant numbers TCRD-TPE-114-RT-3(2/3) and TCRD-TPE-115-31).
Disclosure
No potential conflicts of interest are reported by the authors.
References
1. Cao Z, Tong X, He L, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2021: results from the global burden of disease study 2021. BMJ Public Health. 2026;4(1):e002489. doi:10.1136/bmjph-2024-002489
2. Venkatesan P. GOLD COPD report: 2026 update. Lancet Respir Med. 2025;12(1):15–10. doi:10.1016/s2213-2600(25)00432-1
3. Ren X, Li F, Gao T, et al. A phenomenological qualitative study of primary informal caregiver of Chinese patients with advanced stage COPD: an in-depth exploration of experiences and needs. Int J Chron Obstruct Pulmon Dis. 2026;21:514685. doi:10.2147/copd.S514685
4. Buhl R, Miravitlles M, Anzueto A, Brunton S. Long-acting muscarinic antagonist and long-acting β(2)-agonist combination for the treatment of maintenance therapy-naïve patients with chronic obstructive pulmonary disease: a narrative review. Ther Adv Respir Dis. 2024;18:17534666241279115. doi:10.1177/17534666241279115
5. Tashkin DP, Strange C. Inhaled corticosteroids for chronic obstructive pulmonary disease: what is their role in therapy? Int J Chron Obstruct Pulmon Dis. 2018;13:2587–2601. doi:10.2147/copd.S172240
6. Parsekar K, Xydopoulos G, Yousef A, et al. Carbon dioxide equivalent emissions and cost impact of non-clinically driven inhaler initiation or switch for COPD. Curr Med Res Opin. 2026;42(1):49–59. doi:10.1080/03007995.2026.2628120
7. Tirumalasetty J, Miller SA, Prescott HC, et al. Greenhouse gas emissions and costs of inhaler devices in the US. JAMA. 2024;332(12):1017–1019. doi:10.1001/jama.2024.15331
8. Arslan IG, Vervloet M, de Bekker-Grob EW, et al. The role of environmental impact in healthcare providers’ choices of inhalers for treatment of asthma and COPD: a discrete choice experiment. BMC Prim Care. 2025;26(1):278. doi:10.1186/s12875-025-02941-8
9. Kazda L, Schlub TE, Guppy M, et al. Impact of carbon footprint information on inhaler prescribing intentions by general practitioners: protocol for an online factorial randomised experiment. Respir Med. 2026;252:108657. doi:10.1016/j.rmed.2026.108657
10. Huang CY, Hsieh MS, Wu YK, et al. Chronic obstructive pulmonary disease assessment test for the measurement of deterioration and recovery of health status of patients undergoing lung surgery. Thorac Cancer. 2022;13(4):613–623. doi:10.1111/1759-7714.14306
11. Lai XM, Xie XY, Zhang JC. Association between peripheral blood NLR, PLR, and EXACT-PRO scores in patients with acute exacerbations of chronic obstructive pulmonary disease: a prospective observational cohort study. Int J Chron Obstruct Pulmon Dis. 2026;21:578000. doi:10.2147/copd.S578000
12. Huang HY, Chen CL, Lin YL, et al. Optimizing treatment for hospitalized patients with COPD: a study on the impact of a LINE app-based multidisciplinary team approach targeting pharmacological treatment, lifestyle changes, and smoking cessation. Int J Chron Obstruct Pulmon Dis. 2025;20:1149–1159. doi:10.2147/copd.S511869
13. Culver BH, Graham BL, Coates AL, et al. Recommendations for a standardized pulmonary function report. An official american thoracic society technical statement. Am J Respir Crit Care Med. 2017;196(11):1463–1472. doi:10.1164/rccm.201710-1981ST
14. Chen C-H, Lin IC, Lai -C-C, et al. The carbon footprint associated with the overuse of short-acting β2-agonists in asthma patients. Environ Res Commun. 2024;6(12):125009. doi:10.1088/2515-7620/ad9818
15. Janson C, Hernando Platz J, Soulard S, Langham S, Nicholson L, Hartgers-Gubbels ES. Reducing carbon footprint by switching to reusable soft-mist inhalers. ERJ Open Res. 2023;9(3):00543–2022. doi:10.1183/23120541.00543-2022
16. Janson C, Henderson R, Löfdahl M, Hedberg M, Sharma R, Wilkinson AJK. Carbon footprint impact of the choice of inhalers for asthma and COPD. Thorax. 2020;75(1):82–84. doi:10.1136/thoraxjnl-2019-213744
17. Hänsel M, Bambach T, Wachtel H. Reduced environmental impact of the reusable Respimat(®) Soft Mist™ inhaler compared with pressurised metered-dose inhalers. Adv Ther. 2019;36(9):2487–2492. doi:10.1007/s12325-019-01028-y
18. Andersen ZJ, Vicedo-Cabrera AM, Hoffmann B, Melén E. Climate change and respiratory disease: clinical guidance for healthcare professionals. Breathe. 2023;19(2):220222. doi:10.1183/20734735.0222-2022
19. Or Z, Seppänen A-V. The role of the health sector in tackling climate change: a narrative review. Health Policy. 2024;143:105053. doi:10.1016/j.healthpol.2024.105053
20. Agusti A, Kirk A, Panigone S, Crasto De Stefano I, Levy ML. Climate change and respiratory health: implications for respiratory clinicians in primary and specialist care. Npj Primary Care Respiratory Med. 2026;36(1):20. doi:10.1038/s41533-026-00494-6
21. Usmani OS, Levy ML. Effective respiratory management of asthma and COPD and the environmental impacts of inhalers. NPJ Prim Care Respir Med. 2023;33(1):24. doi:10.1038/s41533-023-00346-7
22. Urrutia-Pereira M, Chong-Neto HJ, Winders TA, Solé D. Environmental impact of inhaler devices on respiratory care: a narrative review. J Bras Pneumol. 2023;48(6):e20220270. doi:10.36416/1806-3756/e20220270
23. Alzaabi A, Bell JP, Montero-Arias F, et al. Greenhouse gas emissions from respiratory treatments: results from the SABA CARBON international study. Adv Ther. 2023;40(11):4836–4856. doi:10.1007/s12325-023-02663-2
24. Wilkinson A, Maslova E, Janson C, et al. Environmental sustainability in respiratory care: an overview of the healthCARe-based envirONmental cost of treatment (CARBON) programme. Adv Ther. 2022;39(5):2270–2280. doi:10.1007/s12325-022-02076-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lung Ultrasound Assessment of Lung Hyperinflation in Patients with Stable COPD: An Effective Diagnostic Tool
Chen Y, Li J, Zhu Z, Lyu G
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:319-330
Published Date: 27 January 2024
Nurses’ Reports of Inhaler Use Errors in Patients with Chronic Obstructive Pulmonary Disease in Hong Kong
Ng SW, Lit MP, Lai AY
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2775-2785
Published Date: 31 December 2024
Optimizing Treatment for Hospitalized Patients with COPD: A Study on the Impact of a LINE App-Based Multidisciplinary Team Approach Targeting Pharmacological Treatment, Lifestyle Changes, and Smoking Cessation
Huang HY, Chen CL, Lin YL, Chen SC, Lee LC, Dai HM, Chiang CY, Chang YF, Lu H, Lee MR, Yang CC, Su CH, Chiang YZ, Yang MC, Shyu RY, Lan CC
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1149-1159
Published Date: 18 April 2025
Characteristics and Quality of Life of Patients with COPD with Different Degrees of Exercise-Induced Desaturation on Six-minute Walk Test
Gao B, Wang S, Zhao L, Liao H, Qumu S, Wang P, Yang T, Jiang S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2381-2391
Published Date: 14 July 2025
The Humanistic and Economic Burden of COPD Patients in Urban China: A Propensity Score Matching Study
Dou L, Zheng Y, Feng J, Huang Z, Qin F, Gao M, Li S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2993-3004
Published Date: 27 August 2025