Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
An Evidence Summary of Health Education in Chronic Obstructive Pulmonary Disease: A Practice-Oriented Assessment with Inter-Rater Reliability
Authors Zhan M, Chen J, Chen C, Zhou J, Zhang H
Received 3 April 2026
Accepted for publication 29 June 2026
Published 15 July 2026 Volume 2026:21 614212
DOI https://doi.org/10.2147/COPD.S614212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Miao Zhan,1,2 Jing Chen,2,3 Changfu Chen,2 Jiali Zhou,2 Hongying Zhang1,2
1Department of Science and Education, The Affiliated Rehabilitation Hospital of Chongqing Medical University, Chongqing, 400084, People’s Republic of China; 2School of Nursing, Chongqing Medical University, Chongqing, 400016, People’s Republic of China; 3Department of Breast and Thyroid Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
Correspondence: Hongying Zhang, Department of Science and Education, The Affiliated Rehabilitation Hospital of Chongqing Medical University, Chongqing, 400084, People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, with a rising burden. Patients are mainly older adults with limited self-management abilities due to low education and cognitive decline. Systematic health education is key to improving disease knowledge and self-management; however, current programs lack standardized content, delivery, and implementation.
Objective: To systematically search, appraise, and synthesize the best evidence on COPD health education, providing healthcare professionals with a rational basis for improving patients’ disease knowledge and home-based self-management.
Methods: This study was registered with the Open Science Framework. Following the “ 6S” evidence pyramid model and a top-down principle, we systematically searched the following databases and websites from inception to November 18, 2025: BMJ Best Practice, UpToDate, Cochrane Library, National Institute for Health and Care Excellence, Registered Nurses’ Association of Ontario, Medlive, Guidelines International Network, American Thoracic Society, European Respiratory Society, Global Initiative for Chronic Obstructive Lung Disease, China National Knowledge Infrastructure, Wanfang Data, VIP Database, Sinomed, PubMed, Embase, and Web of Science. We included clinical practice guidelines, systematic reviews, and expert consensus. Quality was assessed using the AGREE II and JBI checklists. Evidence levels and recommendations were determined using the JBI Pre-grading System (2014).
Results: Twenty-one publications were included (nine guidelines, eight systematic reviews, and four expert consensuses). Thirty-one evidence items were extracted and grouped into seven themes: educational principles, providers, recipients, methods, objectives, core content, and outcome assessment.
Conclusion: Effective COPD health education should shift from one-way knowledge transfer to patient-empowerment-based, interactive models. The content must be tailored to local resources, culture, and health literacy. A closed-loop “education-assessment-feedback” system, multidisciplinary teams, and smart technologies are recommended. Future research should focus on resource-limited settings, multidisciplinary implementation strategies and long-term digital intervention outcomes.
Keywords: chronic obstructive pulmonary disease, health education, self-management, multidisciplinary team, patient empowerment
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, second only to ischemic heart disease and stroke. The global burden of this disease is becoming increasingly severe and is expected to continue growing. According to the Global Burden of Disease Database, the number of patients with COPD is projected to approach 600 million by 2050.1 The increase in prevalence is highly correlated with the trend of population aging, and the majority of patients are elderly individuals. This group often has limited self-management ability due to factors such as low education level and cognitive decline, which poses more severe challenges for disease education and management.2,3
Although drug treatment is the basis for alleviating COPD symptoms, the full clinical efficacy of this treatment largely depends on whether patients correctly master the inhalation technique and maintain good compliance. Systematic patient education plays an irreplaceable role in standardizing inhalation behavior and enhancing compliance. Multiple systematic reviews have confirmed that self-management education can effectively improve the quality of life and disease knowledge of patients, and significantly reduce hospitalizations and emergency visits due to respiratory problems.4–6 Therefore, effective health education strategies have become an indispensable component of comprehensive management plans for patients.
Although the Global Strategy for Chronic Obstructive Pulmonary Disease and the guidelines and statements of the American Thoracic Society/European Respiratory Society on pulmonary rehabilitation emphasize the crucial role of education in COPD management interventions,7,8 existing studies significantly lack homogeneity in terms of intervention content, implementation methods, and interdisciplinary personnel allocation. This is manifested as follows: (1) in terms of educational content, there are complex multidisciplinary plans covering the entire disease cycle, as well as one-sided publicity focusing only on the use of a single inhaler.9,10 (2) in terms of educational methods, from traditional offline oral guidance and paper manuals to digital medical and remote follow-up, the forms are diverse but mostly one-way teaching11,12 and (3) in terms of personnel allocation, the admission standards and responsibilities of multidisciplinary teams are also not clearly defined.13 This heterogeneity not only causes the research evidence for COPD health education to be scattered but also leads to a lack of standardized implementation plans in clinical practice.
Therefore, to compensate for the lack of scattered evidence and standardized implementation plans, this study adopts an evidence-based approach, systematically searches, evaluates, and integrates evidence in the field of COPD health education, aiming to provide a rational educational basis for clinical medical staff, thereby improving patients’ understanding of the disease and enhancing their self-management ability at home.
Materials and Methods
Scheme Registration
The protocol of this study has been registered with the Open Science Framework (OSF). The registration DOI is https://doi.org/10.17605/OSF.IO/UJYRX.
Formulation of the Evidence-Based Question
The PIPOST model was used to frame the evidence-based question:
Population (P): Patients with COPD.
Intervention (I): Health education strategies.
Professionals (P): Healthcare professionals (physicians, nurses, respiratory therapists, pharmacists, nutritionists, etc).
Outcome (O): Disease knowledge level, self-management ability, quality of life, medication adherence, inhalation technique mastery, and acute exacerbation rate.
Setting (S): Hospitals, community health centers, rehabilitation facilities, and home care settings.
Type of evidence (T): Clinical practice guidelines, evidence summaries, systematic reviews and expert consensuses.
Retrieval Strategy
Following the “6S” pyramid evidence model and a top-down search principle, a comprehensive search strategy using subject headings and free-text terms was employed. Databases and websites searched included:
Evidence-based resources: BMJ Best Practice, UpToDate, Cochrane Library.
Guideline development websites: National Institute for Health and Clinical Excellence (NICE), Registered Nurses’ Association of Ontario (RNAO), Medlive, Guidelines International Network (GIN).
Professional society websites: American Thoracic Society (ATS), European Respiratory Society (ERS), Global Initiative for Chronic Obstructive Lung Disease (GOLD).
General databases: China National Knowledge Infrastructure (CNKI), Wanfang Data, VIP Database, Sinomed, PubMed, Embase, Web of Science.
The search period was from database inception to November 18, 2025. The specific search methods for all databases and websites are detailedin Appendix 1. Additionally, we manually searched the reference lists of all included guidelines, systematic reviews, evidence summaries, and expert consensus.
Literature Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) patients with COPD; (2) focus on COPD health education; (3) study types: clinical practice guidelines, evidence summaries, expert consensus, or systematic reviews (with the most recent version included for guidelines or expert consensus); and (4) published in Chinese or English.
The exclusion criteria were as follows: (1) not in Chinese or English; (2) duplicate publications; and (3) low methodological quality.
Evaluation and Screening Criteria for Literature Quality
Two researchers (MZ and JC) who had received systematic evidence-based medicine training independently conducted literature screening and quality evaluation. Using NoteExpress, they independently evaluated the titles and abstracts based on preset inclusion and exclusion criteria. For the screened literature, full texts were obtained and independently evaluated by the two researchers. Subsequently, the AGREE II tool was used to evaluate the quality of the guidelines, and the Australian JBI standards (2016) were used to evaluate the quality of systematic reviews and expert consensus.
The inter-rater consistency of the title/abstract screening, full-text eligibility assessment, and quality evaluation stages was tested using Cohen’s Kappa coefficient,14 with the Kappa value serving as the effect size. A Kappa value of ≥ 0.81 indicates excellent consistency, 0.61 to 0.80 indicates good consistency, 0.41 to 0.60 indicates moderate consistency, 0.21 to 0.40 indicates average consistency, and ≤ 0.20 indicates poor consistency. Any disagreements that arose during this process were first resolved through consensus discussions; if a consensus could not be reached, the final decision was made by the third senior researcher (HYZ).
Data Synthesis and Classification
During evidence extraction, when the two researchers (MZ and JC) encountered conflicting recommendations, they followed the principle of “prioritizing the most recent, high-quality, evidence-based evidence.”
Subsequently, the Australian JBI Evidence Pre-grading System (2014)15 was used to classify the levels of evidence and determine the strength of recommendations. According to the study design, the evidence was classified into five main levels: Level 1 (experimental designs, including randomized controlled trials), Level 2 (quasi-experimental designs), Level 3 (observational-analytic designs), Level 4 (observational-descriptive designs), and Level 5 (expert opinion or basic research). For each piece of evidence, a corresponding sub-level (eg, 1a, 1b, 5b) was assigned based on the specific document type and original research method. Following the JBI recommendations, after a structured assessment of effectiveness, feasibility, appropriateness, and clinical significance, the strength of recommendation was rated as Grade A (strong recommendation) or Grade B (weak recommendation).
Results
Consistency Test
The Cohen’s Kappa coefficient between the two researchers (MZ and JC) was 0.83 (95% CI: 0.79–0.87) for the title/abstract screening stage, and 0.88 (95% CI: 0.82–0.94) for the full-text eligibility assessment and quality appraisal stage, indicating excellent agreement between the two reviewers.
General Characteristics of the Included Literature
A total of 9,825 records were initially identified through the database searches: CNKI (n=96), Wanfang Data (n=332), VIP (n=659), PubMed (n=1,455), Web of Science (n=1,758), Cochrane Library (n=322), SinoMed (n=310), Embase (n=3,392), BMJ Best Practice (n=272), UpToDate (n=87), NICE (n=60), RNAO (n=5), GIN (n=0), Medlive (n=450), ATS (n=587), ERS (n=20), and GOLD (n=20). Furthermore, all references included in the guidelines, systematic reviews, evidence summaries, and expert consensuses were manually searched, and no other eligible literature was found.
After removing 3,385 duplicate records using NoteExpress, 6,440 records remained eligible for screening. Following title and abstract screening, 6,267 records were excluded, leaving 173 records for full text assessment. After a full text review, 144 records that did not meet the inclusion criteria were excluded, 5 records could not be obtained in full text, and 3 records were excluded because they were not published in Chinese or English. Ultimately, 21 records were included (Figure 1), comprising eight systematic reviews,5,6,16–21 nine clinical practice guidelines,22–30 and four expert consensuses (Table 1).31–34
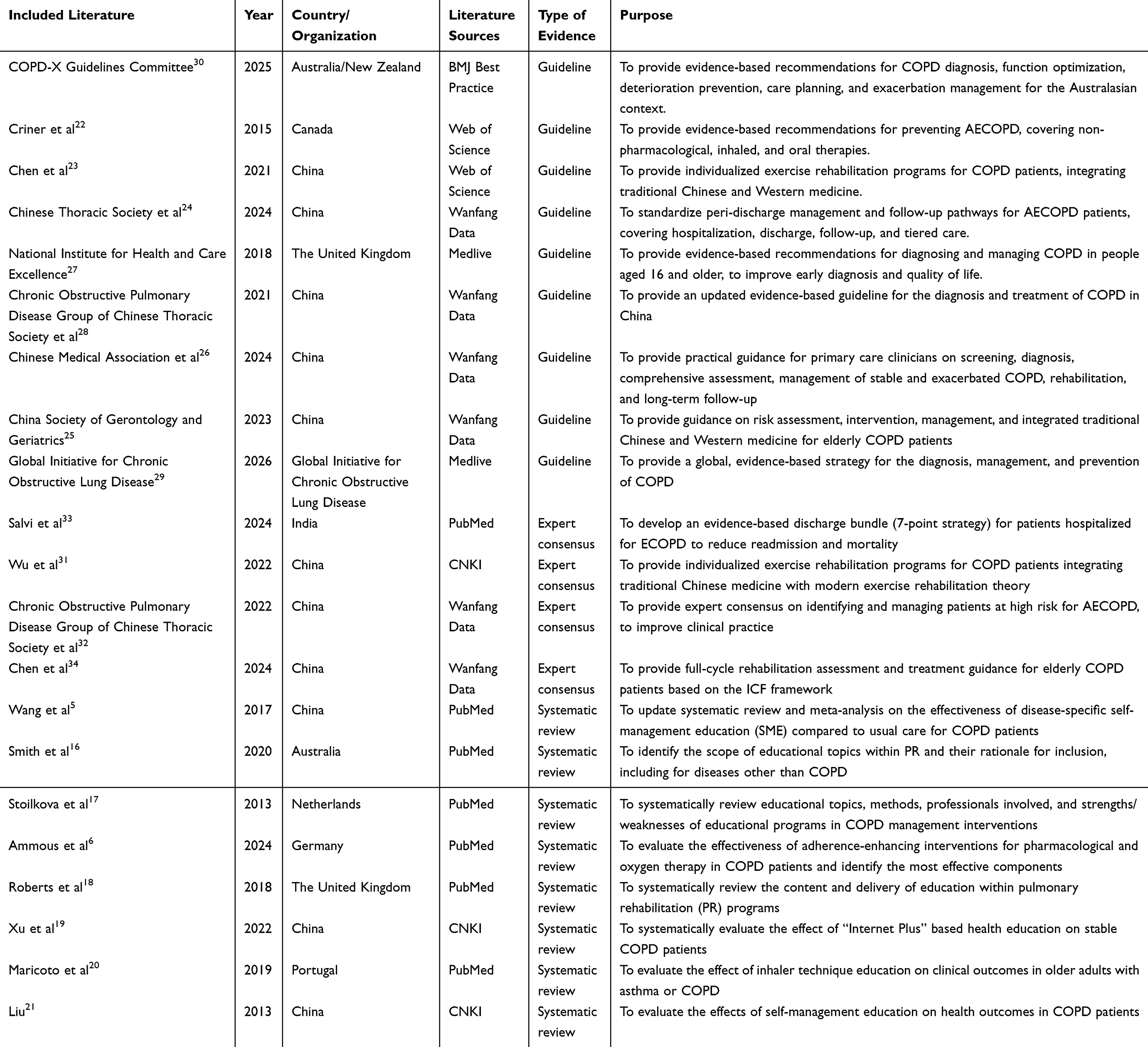 |
Table 1 Basic Characteristics of Included Articles (n=21) |
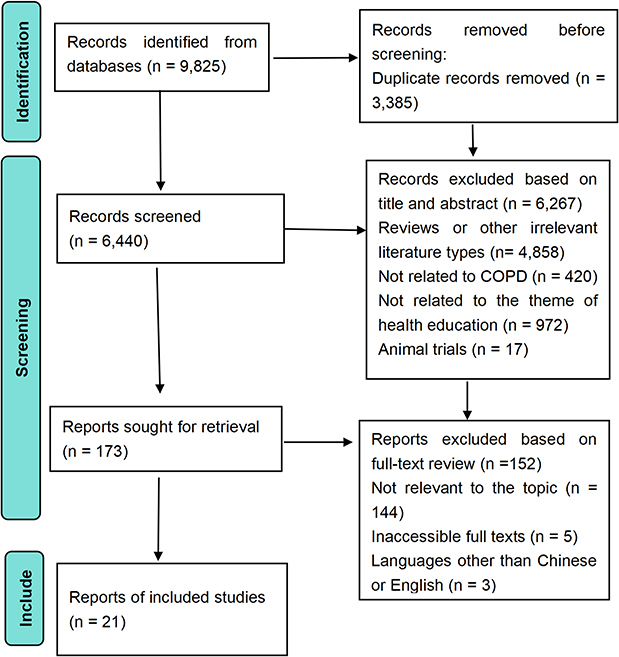 |
Figure 1 Flow diagram of the article selection process. |
Quality Evaluation Results of the Included Literature
Guideline
A total of nine clinical practice guidelines were included, among which two22,23 were from Web of Science, four24–26,28 from Wanfang Data, one27 from Medlive, one29 from GOLD, and one30 from BMJ Best Practice The overall quality was good. In addition to Chen et al23 and Criner et al22 were grade B recommendations. The rest were recommended at grade A and included. (Table 2).
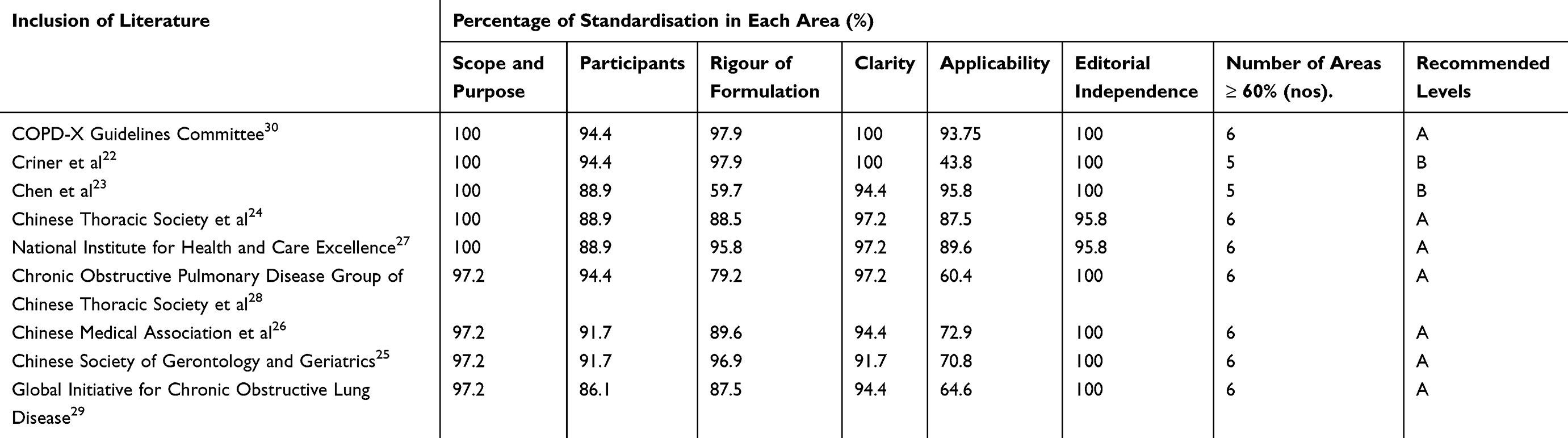 |
Table 2 Results of the Quality Evaluation of the Guidelines (n=9) |
Systematic Review
A total of eight systematic reviews were included, among which six5,6,16–18,20 were from PubMed and two19,21 from CNKI. Among them, all entries in the three articles19–21 were marked as “yes.” Wang et al,5 Smith et al,16 Stoilkova et al,17 Liu et al,21 and Roberts et al18 only had the entry “Was the possibility of publication bias evaluated?”, which were evaluated as “no” or “unclear”, the rest of the items were all “yes”, and the overall quality was acceptable Therefore, all high-quality systematic reviews were included (Table 3).
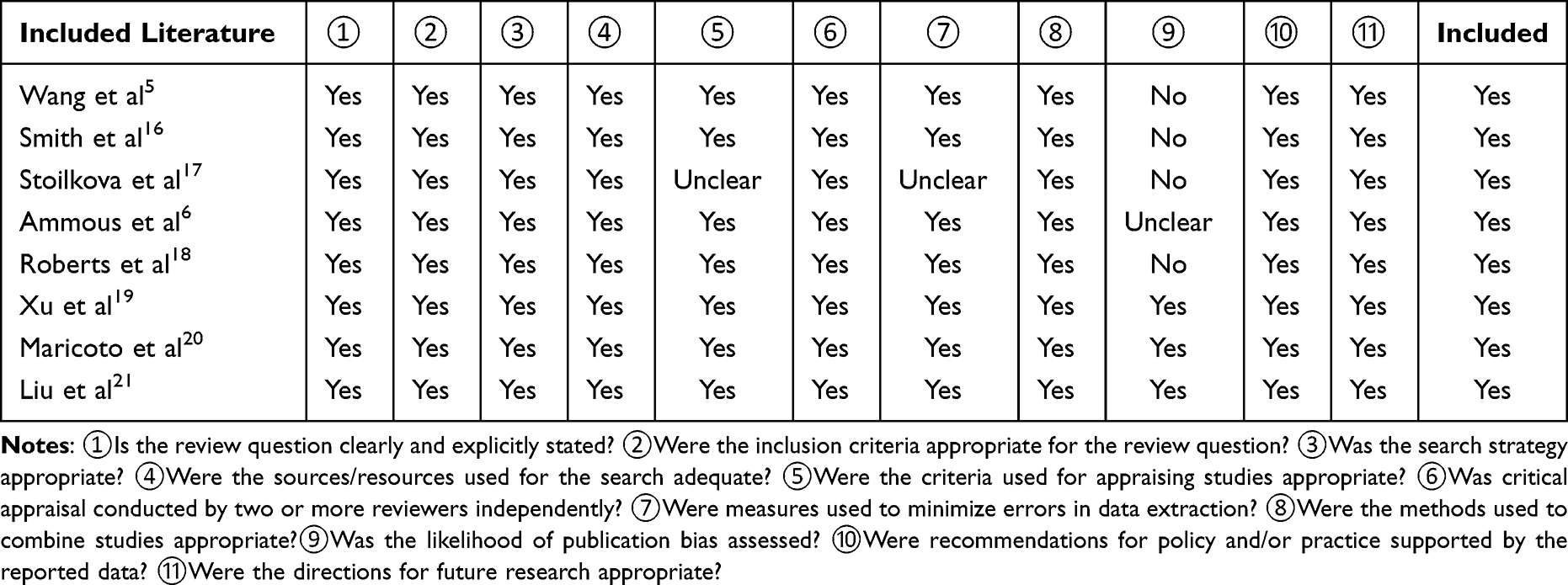 |
Table 3 Quality Appraisal results of Systematic Reviews (n = 8) |
Expert Consensus
A total of four expert consensuses were included, among which one33 was from PubMed, one31 from CNKI, and two32,34 from Wanfang Data. The evaluation results of all entries were “yes,” indicating high quality of the literature, and all were included(Table 4).
 |
Table 4 Quality Appraisal Results of Expert Consensuses (n = 4) |
Evidence Summary and Description
A total of 31 evidence items related to COPD health education were extracted in this study (Table 5) and categorized into seven themes: (1) principles, (2) providers, (3) recipients, (4) methods, (5) objectives, (6) core content, and (7) outcome assessment. The Cohen’s Kappa coefficient for the two researchers’ agreement (MZ and JC) on theme assignment was 0.82 (95% CI: 0.73–0.91), indicating a good inter-rater agreement.
 |
Table 5 Summary of Best Evidence for Health Education for Patients with COPD |
Discussion
Through systematic search and quality evaluation, this study ultimately included 21 articles, extracted 31 pieces of evidence, and summarized them into seven themes. The following section discusses this evidence and analyzes the challenges and prospects of clinical application.
Consensus and Differences in Core Topics of Health Education for COPD
Effective health education themes should be determined based on the available evidence, and individualized strategies should be developed by integrating patients’ preferences and specific circumstances.
Evidence items 6–30 (Table 5) systematically synthesized the consensus reached in the included literature, clarifying the core content of basic COPD health education, including disease basics, medication and inhalation techniques, recognition and management of acute exacerbations, pulmonary rehabilitation, smoking cessation, vaccination, nutrition, psychological support, and oxygen therapy. However, there are differences in the coverage and emphasis on educational themes across regions.
In high-income countries and international guidelines, while retaining the above basic themes, the scope of health education has been further extended to more advanced and strategic topics, such as advance care directives and end-of-life care,29 travel advice,30 and environmental exposure reduction.27 These themes reflect the relatively well-developed healthcare infrastructure in these regions, as well as an emphasis on holistic care, patient dignity, and quality of life. In contrast, in low- and middle-income countries, the selection of health education themes is often constrained by practical conditions such as healthcare resource allocation and patients’ basic health literacy,19,26,28 with a greater focus on fundamental and accessible content, such as basic disease concepts and correct use of inhalation devices. This heterogeneity may not reflect a flaw in the study quality but rather differences in healthcare systems, cultural backgrounds, resource accessibility, and disease management philosophies across countries. Taking China as an example, incorporating traditional exercises such as Tai Chi and Ba Duan Jin into education programs as low-cost, culturally adapted alternatives within the pulmonary rehabilitation theme demonstrates a pragmatic orientation under resource-limited conditions.
Therefore, future health education strategies should, on an evidence-based foundation, fully consider regional characteristics, healthcare resource allocation, and individual patient preferences to achieve truly individualized education.
Establishing Patient-Centered COPD Health Education
However, a personalized theme list is only the first step in the educational process. Translating this content into patients’ actual actions requires targeted strategies, which is also an inevitable requirement for practicing a “patient-centered” approach.
Evidence item 4 (Table 5) indicates that common methods of health education include verbal instruction, printed materials, video demonstrations, health lectures, and Internet-based remote education.35 In clinical practice, verbal instructions and printed handouts still dominate. However, Giguère et al36 conducted a systematic review of 23 high-quality studies and concluded that printed educational materials as a standalone intervention did not significantly improve patient clinical outcomes. Muijsenberg et al37 clearly pointed out that traditional didactic education struggles to meet patients’ real needs, providing a strong rationale for shifting health education toward personalized and multimodal approaches. Furthermore, approximately 40–80% of medical information is forgotten by patients immediately after consultation; during a 5-minute routine education session, the effective information retention rate is only 20%, and nearly half of that is misunderstood.38 This phenomenon is known as the “knowledge transmission inverted triangle,” where information continuously attenuates as it is transferred from healthcare providers to patients, highlighting the fundamental limitation of traditional one-way educational models.
Therefore, based on patient empowerment theory, the core goal of health education should not remain at the level of knowledge transmission but should shift toward promoting patient behavioral change and ultimately enhancing patients’ self-management abilities. The teach-back method has been confirmed by multiple studies to be an effective two-way interactive strategy.39–41 Notably, although the teach‑back method does not appear as an independent item in the evidence presented in this study (Table 3), its concept is highly consistent with Evidence item 5 (Table 5) and can serve as an important supplement for clinical translation. Its core advantage lies in transforming one-way information delivery into a two-way interactive cycle of “explain - repeat - correct” between healthcare providers and patients, ensuring that patients truly understand and master the information. This method not only effectively identifies and corrects patient misunderstandings, reducing the risk of medication errors or disease deterioration caused by incorrect understanding, but also enhances patient engagement and adherence to treatment. Simultaneously, it provides healthcare professionals with immediate feedback to evaluate educational effectiveness. Theoretically, the effectiveness of the teach-back method can be supported by the Knowledge-Attitude-Practice (KAP) model and the Health Belief Model (HBM). The KAP model points out that knowledge is the foundation of behavioral change, attitude is the driving force, and behavior is the ultimate goal. By repeatedly verifying patients’ understanding of information, the teach-back method ensures the accuracy of knowledge acquisition, lays the premise for forming correct attitudes, and ultimately promotes stable behavioral establishment. The HBM emphasizes that whether an individual adopts a health behavior depends on their perception of disease threat, recognition of behavioral benefits, and level of self-efficacy. During the “repeat-correct” process, the teach-back method helps patients clearly understand the specific risks of non-adherent behavior, reinforces the benefits of correct performance, and builds the confidence of “I can do it” through repeated successful repetition, thereby effectively translating health beliefs into daily health actions.
With “Internet + Healthcare” becoming a hot topic in research and practice, inefficient educational models are undergoing profound transformations.42 The teach-back method focuses on interaction quality, while digital technology focuses on resource accessibility, and the two can complement one another. Increasingly, researchers are leveraging remote platforms to deliver online education to patients, driving health education toward digitalization, personalization, and systematization.43,44 Many platforms have achieved Internet interoperability, supporting patients in autonomously retrieving customized health knowledge.45 These technologies not only expand the accessibility of educational resources but also empower patients with greater confidence to actively participate in health management processes.
Multidisciplinary Collaboration is the Structural Prerequisite for Achieving Personalized Education
Given that COPD is a chronic disease with multiple comorbidities, patients often suffer from various physical and psychological complications, such as cardiovascular disease, diabetes, osteoporosis, anxiety, and depression. This pathological characteristic determines that the self‑management skills that patients need to master are not limited to respiratory rehabilitation or medication adherence but rather span a complex knowledge system across multiple domains, including respiratory, cardiovascular, metabolic, musculoskeletal, and psychological health. This inherent complexity requires a multidisciplinary team (MDT) to provide leadership and support for individualized education.46,47
As Anne stated,48 MDT is not simply a collection of individuals but a collaborative network that organically integrates the roles of physicians, respiratory nurses, physiotherapists, dietitians, psychological counselors, and pharmacists. However, multiple studies have consistently indicated that the clinical implementation rate of MDT is far lower than expected.49 Even in the context of strong guideline recommendations for MDT effectiveness,30 real-world data remain discouraging. Henoch et al,50 based on data from 7,810 patients with COPD in the Swedish National Airway Registry, found that less than 20% of patients had ever been in contact with a physiotherapist or dietitian. This means that although guidelines advocate for multidimensional, interdisciplinary comprehensive care, the vast majority of patients with COPD do not receive these core support services during routine clinical visits.
The reasons for this are as follows: First, there is a shortage of interdisciplinary staff. Effective MDT operation for COPD requires the joint participation of respiratory physicians, nurses, physiotherapists, pharmacists, and other professionals. Such professionals are severely lacking in most healthcare institutions, even in developed countries (eg, Ireland), and especially in low- and middle-income countries. Lim et al51 conducted a cross‑sectional survey of consultant respiratory physicians in the Republic of Ireland and found that only 31% of respondents reported having a dedicated COPD multidisciplinary team in their institution, and approximately 30% felt that adequate pulmonary rehabilitation resources were unavailable. Moreover, up to 71.4% of nurses reported a lack of specialized health-education training.52 Nurses are the main executors of education, and their insufficient knowledge base and lack of training opportunities are the deeper reasons why MDT implementation is difficult.
Therefore, we strongly recommend: (1) Strengthen the core staffing of MDT. Each tertiary hospital respiratory department should be equipped with at least one respiratory nurse, one physiotherapist, and one pharmacist as permanent core members of the MDT. For institutions with staffing shortages, assistance should be provided to lower-level hospitals through tertiary hospital Internet platforms. Simultaneously, systematically trained respiratory nurses should be allowed to take on multiple expanded roles (eg, basic pulmonary rehabilitation guidance, rapid nutritional risk assessment, and psychological support) so that limited staffing can cover the core functions of the MDT. (2) Improving the education and certification systems for respiratory nurses. Pre-service and in-service education for all respiratory nurses should adopt a model combining simulated cases and standardized patients, and MDT qualification should be certified through objective structured clinical examinations (OSCEs). Healthcare institutions should make passing this certification a mandatory requirement for nurses responsible for COPD patient follow-up, and regular re-evaluations should be conducted.
Limitations
This study has the following limitations: (1) the literature search was limited to Chinese and English databases, which may introduce language bias; (2) some of the included literature was not specifically focused on COPD health education, so its applicability may be limited; and (3) the existing evidence originates from studies conducted in multiple countries, with insufficient consideration given to specific cultural backgrounds, health literacy levels, and social support systems. Therefore, when health education programs are applied in local contexts, adaptive adjustments and innovations are needed; (4) the researchers performed the extraction, grading, and synthesis of evidence. Although we used independent assessments by two reviewers and Kappa consistency tests, some subjective judgments may still exist, potentially affecting the robustness of the evidence synthesis.
Conclusion
This study systematically retrieved and synthesized 31 evidence items on health education in COPD, covering seven themes: educational principles, providers, recipients, methods, objectives, core content, and outcome assessment. The evidence indicates that effective health education should shift from traditional one-way knowledge transmission to an interactive model centered on patient empowerment. Educational content should be tailored based on regional resources, cultural backgrounds, and patients’ health literacy levels, and a closed loop of “education – assessment – feedback” should be established to continuously optimize outcomes. Relying on multidisciplinary teams and intelligent technologies, health education can achieve systematic, personalized, and interactive delivery. Future research should focus on the development and validation of localized education programs in low‑resource settings, implementation strategies for multidisciplinary team collaboration, and long‑term intervention outcome evaluations supported by digital technologies.
Data Sharing Statement
The datasets supporting the conclusions of this article are included within the article and its additional file.
Ethics Statement
This systematic review did not involve direct patient contact or primary data collection. All included studies had obtained appropriate ethical approval and informed consent as reported in their original publications. No further ethical approval or informed consent was required for this review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Graduate Innovation Fund of theAffiliated Rehabilitation Hospital of Chongqing Medical University (Grant No. KFS2025001) and the Project of Chongqing Municipal Bureau of Disease Control and Prevention (Grant No. 2026JKXM043).
Disclosure
The authors declare no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
2. Muijsenberg AJL, Houben-Wilke S, Spruit MA, Janssen DJA. Education for people with serious chronic respiratory diseases and their informal caregivers: how to address challenges that impact learning. Curr Opin Support Palliat Care. 2024;18(4):206–17. doi:10.1097/SPC.0000000000000719
3. Ho CC, Chan CWH, Li C, Xiao J, Ng MS. Literature review and development of pictorial action plan to promote self-management of chronic obstructive pulmonary disease. Patient Educ Couns. 2023;115:107923. doi:10.1016/j.pec.2023.107923
4. Schrijver J, Lenferink A, Brusse-Keizer M, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1(1):CD002990. doi:10.1002/14651858.CD002990.pub4
5. Wang T, Tan JY, Xiao LD, Deng R. Effectiveness of disease-specific self-management education on health outcomes in patients with chronic obstructive pulmonary disease: an updated systematic review and meta-analysis. Patient Educ Couns. 2017;100(8):1432–1446. doi:10.1016/j.pec.2017.02.026
6. Ammous O, Kampo R, Wollsching-Strobel M, et al. Adherence-enhancing interventions for pharmacological and oxygen therapy in patients with COPD: a systematic review and component network meta-analyses. Eur Respir Rev. 2024;33(173):240011. doi:10.1183/16000617.0011-2024
7. Nici L, Donner C, Wouters E, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173(12):1390–1413. doi:10.1164/rccm.200508-1211ST
8. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
9. Mendes MA, Rodrigues G, Janssen DJA, Spruit MA, Marques A. Understanding the determinants and outcomes of education in pulmonary rehabilitation: moving toward person-centered care. Chest. 2025;167(6):1615–1627. doi:10.1016/j.chest.2025.01.005
10. Heijmans M, Poortvliet R, Van der Gaag M, et al. Using a taxonomy to systematically identify and describe self-management interventions components in randomized trials for COPD. Int J Environ Res Public Health. 2022;19(19):12685. doi:10.3390/ijerph191912685
11. Aung H, Tan R, Flynn C, et al. Digital remote maintenance inhaler adherence interventions in COPD: a systematic review and meta-analysis. Eur Respir Rev. 2024;33(174):240136. doi:10.1183/16000617.0136-2024
12. Song J, Wang Q, Zhao C, Wang L, Li L, Kang D. Comparative efficacy of pulmonary rehabilitation delivery models on dyspnoea, exercise capacity and health-related quality of life in chronic respiratory disease: a systematic review and network meta-analysis. NPJ Prim Care Respir Med. 2025;36(1):8. doi:10.1038/s41533-025-00472-4
13. Siu DCH, Gafni-Lachter L. Addressing Barriers to Chronic Obstructive Pulmonary Disease (COPD) care: three innovative evidence-based approaches: a review. Int J Chron Obstruct Pulmon Dis. 2024;19:331–341. doi:10.2147/COPD.S426050
14. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174. doi:10.2307/2529310
15. Pearson A, Wiechula R, Court A, Lockwood C. The JBI model of evidence-based healthcare. Int J Evid Based Healthc. 2005;3(8):207–215. doi:10.1111/j.1479-6988.2005.00026.x
16. Smith R, Osadnik CR, Lee AL. Educational topics and their rationale for inclusion within pulmonary rehabilitation - a systematic review. Patient Educ Couns. 2020;103(10):1997–2008. doi:10.1016/j.pec.2020.04.009
17. Stoilkova A, Janssen DJ, Wouters EF. Educational programmes in COPD management interventions: a systematic review. Respir Med. 2013;107(11):1637–1650. doi:10.1016/j.rmed.2013.08.006
18. Roberts NJ, Kidd L, Kirkwood K, Cross J, Partridge MR. A systematic review of the content and delivery of education in pulmonary rehabilitation programmes. Respir Med. 2018;145:161–181. doi:10.1016/j.rmed.2018.11.002
19. Xu B, Wei QG, Chen SF, et al. Systematic evaluation of the efficacy of health education based on “Internet Plus” on stable phase of chronic obstructive pulmonary disease. China Med Pharm. 2023;13(4):47–51.
20. Maricoto T, Monteiro L, Gama JMR, Correia-de-Sousa J, Taborda-Barata L. Inhaler technique education and exacerbation risk in older adults with asthma or chronic obstructive pulmonary disease: a meta-analysis. J Am Geriatr Soc. 2019;67(1):57–66. doi:10.1111/jgs.15602
21. Liu XL, Tan JY, Liu F, Zhang M, Yao LQ . Meta-analysis of the impact of self-management education on the health of patients with chronic obstructive pulmonary disease. Chin J Nurs. 2013;48(3):263–266.
22. Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015;147(4):894–942. doi:10.1378/chest.14-1676
23. Chen X, Gong D, Huang H, Wang K, Zhang W, Li S. Expert consensus and operational guidelines on exercise rehabilitation of chronic obstructive pulmonary disease with integrating traditional Chinese medicine and Western medicine. J Thorac Dis. 2021;13(6):3323–3346. doi:10.21037/jtd-21-431
24. Chinese Thoracic Society; Respiratory Disease Prevention and Control Specialty Societies of Chinese Preventive Medicine Association. Chronic Obstructive Pulmonary Disease Committee of Chinese Association of Chest Physician; County Respiratory Professional Committee of China Association of Health Promotion and Education. [Peri-discharge management and follow-up of acute exacerbations of COPD]. Zhonghua Jie He He Hu Xi Za Zhi. 2024;47(11):1048–1068. doi:10.3760/cma.j.cn112147-20240816-00488.
25. Chinese Society of Gerontology and Geriatrics. Guidelines for the management of chronic obstructive pulmonary disease in the elderly. J Integr Tradit Chin West Med Res. 2023;15(3):154–164.
26. Chinese Medical Association, et al. Guidelines for the primary care diagnosis and management of chronic obstructive pulmonary disease in China (2024). Chin J Gen Pract. 2024;23(6):578–602.
27. National Institute for Health and Care Excellence. Chronic Obstructive Pulmonary Disease in Over 16s: Diagnosis and Management. NICE guideline NG115. London: NICE;2019.
28. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society, et al. Guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease (2021 revised edition). Chin J Tuberc Respir Dis. 2021;44(3):170–205.
29. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2026 report. 2026.
30. Yang IA, George J, McDonald CF, et al. The COPD-X plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease 2025. version 2.78. 2025. Available from: https://copdx.org.au/copd-x-plan/.
31. Wu XD, Chen X, Li SQ, Zhang W, Wu QH . Expert consensus on the application of traditional Chinese medicine in exercise rehabilitation for chronic obstructive pulmonary disease. World Clin Drugs. 2022;43(3):211–221.
32. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society, et al. Chinese expert consensus on the identification and management of patients at high risk for acute exacerbation of chronic obstructive pulmonary disease. Int J Respir. 2022;42(24):1845–1863.
33. Salvi S, Ghorpade D, Nair S, et al. A 7-point evidence-based care discharge protocol for patients hospitalized for exacerbation of COPD: consensus strategy and expert recommendation. NPJ Prim Care Respir Med. 2024;34(1):44. doi:10.1038/s41533-024-00378-7
34. Chen X, Jia J, Ding YP, et al. Respiratory and rehabilitation expert consensus on full-cycle rehabilitation assessment and treatment for elderly patients with chronic obstructive pulmonary disease. Rehabil Med. 2024;34(6):544–555. doi:10.3724/SP.J.1329.2024.06003
35. Elnasieh AM, Alturki AT, Alhadlaq R, et al. Health education resources favored by out-patients attending King Saud Medical City, Riyadh. Cureus. 2024;16(8):e67089. doi:10.7759/cureus.67089
36. Giguère A, Légaré F, Grimshaw J, et al. Printed educational materials: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2012;10(10):CD004398. doi:10.1002/14651858.CD004398.pub3
37. Muijsenberg AJ, Houben-Wilke S, Tatousek J, Lacroix J, Spruit MA, Janssen DJ. Educational needs of people with COPD or asthma entering pulmonary rehabilitation and their significant others: a cross-sectional study. Chron Respir Dis. 2025;22:14799731251316891. doi:10.1177/14799731251316891
38. Geleta TA, Deriba BS. Exploring enablers and barriers to utilize printed information, education, and communication materials among healthcare providers of North Shoa Zone, Oromia, Ethiopia. Risk Manag Healthc Policy. 2022;15:1303–1313. doi:10.2147/RMHP.S360417
39. Hasanpour Dehkordi A, Ebrahimi-Dehkordi S, Banitalebi-Dehkordi F, Salehi Tali S, Kheiri S, Soleimani Babadi A. The effect of teach-back training intervention of breathing exercise on the level of dyspnea, six-minutes walking test and FEV1/FVC ratio in patients with chronic obstructive pulmonary disease; a randomized controlled trial. Expert Rev Respir Med. 2021;15(1):161–169. doi:10.1080/17476348.2020.1822740
40. Ji Q, Han M, Xu K, Liu T, Yang J, Wang T. Research on the application of feedback method combined with diversified health education in elderly patients with COPD complicated with dysphagia. Sci Rep. 2025;16(1):3658. doi:10.1038/s41598-025-33757-2
41. Vázquez-González N, Leiva-Fernández J, Cotta-Luque VM, et al. Effectiveness of an educational intervention about inhalation technique in healthcare professionals in primary care: a cluster randomized trial. Front Pharmacol. 2023;14:1266095. doi:10.3389/fphar.2023.1266095
42. Yang K, Hu Y, Qi H. Digital health literacy: bibliometric analysis. J Med Internet Res. 2022;24(7):e35816. doi:10.2196/35816
43. Sun C, Dai H, Van der Kleij MJJR, et al. Digital health education for chronic lung disease: scoping review. J Med Internet Res. 2025;27:e53142. doi:10.2196/53142
44. Sarker MHR, Moriyama M, Rashid HU, et al. Chronic kidney disease awareness campaign and mobile health education to improve knowledge, quality of life, and motivation for a healthy lifestyle among patients with chronic kidney disease in Bangladesh: randomized controlled trial. J Med Internet Res. 2022;24(8):e37314. doi:10.2196/37314
45. Zhao L, Liu Y, Li J, Li P, Zhao X, Zhang S. Effects of internet-based health education on patients with acute intermittent porphyria. Orphanet J Rare Dis. 2024;19(1):428. doi:10.1186/s13023-024-03440-2
46. Shi Y, Li H, Yuan B, Wang X. Effects of multidisciplinary teamwork in non-hospital settings on healthcare and patients with chronic conditions: a systematic review and meta-analysis. BMC Prim Care. 2025;26(1):110. doi:10.1186/s12875-025-02814-0
47. Miguel-Díez JD, Fernández-Villar A, Doña Díaz E, et al. Chronic obstructive lung disease: treatment guidelines and recommendations for referral and multidisciplinary continuity of care. J Clin Med. 2024;13(2):303. doi:10.3390/jcm13020303
48. Kuzma AM, Meli Y, Meldrum C, et al. Multidisciplinary care of the patient with chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):567–571. doi:10.1513/pats.200708-125ET
49. Houben-Wilke S, Vaes AW, Cuijpers M, et al. An overview of the importance of allied healthcare for patients with COPD. Expert Rev Respir Med. 2026. doi:10.1080/17476348.2026.2629007
50. Henoch I, Strang S, Löfdahl CG, Ekberg-Jansson A. Management of COPD, equal treatment across age, gender, and social situation? A register study. Int J Chron Obstruct Pulmon Dis. 2016;11:2681–2690. doi:10.2147/COPD.S115238
51. Lim J, O’Brien H, McCarthy J, McCarthy C, Franciosi AN. Current practices, perceptions and future challenges in the management of moderate to severe COPD: a cross-sectional survey of respiratory consultants in the Republic of Ireland. BMJ Open Respir Res. 2025;12(1):e003520. doi:10.1136/bmjresp-2025-003520
52. Pueyo-Garrigues M, Pardavila-Belio MI, Canga-Armayor A, Esandi N, Alfaro-Díaz C, Canga-Armayor N. NURSES’ knowledge, skills and personal attributes for providing competent health education practice, and its influencing factors: a cross-sectional study. Nurse Educ Pract. 2022;58:103277. doi:10.1016/j.nepr.2021.103277
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Multivariable Exercise Adherence Prediction Model for Patients with COPD: A Prospective Cohort Study

Ricke E, Bakker EW
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:385-398
Published Date: 22 March 2023
Factors Associated with Non-Adherence to Self-Management Among Patients with Chronic Obstructive Pulmonary Disease: A Survey Using the Delphi Technique and Analytic Hierarchy Process
Choi JY, Ryu EJ
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1247-1259
Published Date: 4 June 2024
Optimizing Treatment for Hospitalized Patients with COPD: A Study on the Impact of a LINE App-Based Multidisciplinary Team Approach Targeting Pharmacological Treatment, Lifestyle Changes, and Smoking Cessation
Huang HY, Chen CL, Lin YL, Chen SC, Lee LC, Dai HM, Chiang CY, Chang YF, Lu H, Lee MR, Yang CC, Su CH, Chiang YZ, Yang MC, Shyu RY, Lan CC
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1149-1159
Published Date: 18 April 2025
The Cost-Effectiveness of a Personalised Early Warning Decision Support System (The COPDPredict™ System) to Predict and Prevent Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Hall JA, Turner AM, Gkini E, Mehta R, Spiteri M, Patel N, Jowett S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1693-1710
Published Date: 25 May 2025
Global Trends in COPD Self-Management Research: A Dual-Perspective Bibliometric Analysis (January 2005–July 2025)
Huang X, Feng J, Gan X, Wu R, Su C, Zheng L, Deng R
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:563718
Published Date: 6 January 2026