Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Humanistic and Economic Burden of COPD Patients in Urban China: A Propensity Score Matching Study
Authors Dou L ![]() , Zheng Y, Feng J, Huang Z, Qin F, Gao M
, Zheng Y, Feng J, Huang Z, Qin F, Gao M ![]() , Li S
, Li S ![]()
Received 20 February 2025
Accepted for publication 13 August 2025
Published 27 August 2025 Volume 2025:20 Pages 2993—3004
DOI https://doi.org/10.2147/COPD.S524028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Fanny Wai San Ko
Lei Dou,1– 4 Yu Zheng,5 Junchao Feng,1– 4 Zhezhou Huang,6 Fei Qin,6 Mingyue Gao,6 Shunping Li1– 4
1Department of Social Medicine and Health Management, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, People’s Republic of China; 2NHC Key Laboratory of Health Economics and Policy Research (Shandong University), Jinan, Shandong, People’s Republic of China; 3Center for Health Management and Policy Research, Shandong University (Shandong Provincial Key New Think Tank), Jinan, Shandong, People’s Republic of China; 4Center for Health Preference Research, Shandong University, Jinan, Shandong, People’s Republic of China; 5Blood Center of Shandong Province, Jinan, Shandong, People’s Republic of China; 6Cerner Enviza, Shanghai, People’s Republic of China
Correspondence: Shunping Li, Department of Social Medicine and Health Management, School of Public Health, Cheeloo College of Medicine, Shandong University, Wenhua Xi Road44, Jinan, Shandong, 250012, People’s Republic of China, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) is a leading cause of death in China. However, few national surveys have comprehensively evaluated the health and economic outcomes among COPD patients in China. The objective of this study was to examine and compare the humanistic and economic burden of COPD patients with a control group.
Patients and Methods: Data from the 2020 National Health and Wellness Survey (NHWS) in China (N=20051), a nationally representative survey targeting urban adults, was used in this study. The propensity score matching (PSM) method was employed to match respondents who reported being diagnosed with COPD by a physician with those who did not have COPD. Differences between COPD patients and matched controls were assessed in terms of quality of life (using EQ-5D-5L and SF-12v2), work productivity loss, healthcare resource utilization over the past 6 months, and estimated annual indirect costs.
Results: COPD patients exhibited significantly worse outcomes compared to non-COPD respondents. The mean scores for MCS, PCS, and health state utility (HSU) were substantially lower in COPD patients than in the control group (47.69 vs 49.49, 47.27 vs 51.71, and 0.90 vs 0.94, respectively; all P < 0.01). Moreover, the score difference between COPD patients and the control group reached minimal clinically important difference (MCID) for both PCS and HSU. Compared to the non-COPD population, COPD patients reported higher rates of absenteeism (6.88% vs 3.74%, P< 0.01), presenteeism (28.02% vs 21.43%, P< 0.01), work productivity loss (31.31% vs 23.57%, P< 0.01) and activity impairment (27.15% vs 19.53%, P< 0.01), resulting in greater indirect cost. The number of hospitalizations was significantly higher among COPD patients than the non-COPD population (2.11 vs 1.96, P< 0.01), while the number of outpatient visits was similar to that of the control group.
Conclusion: These findings highlight the pervasive impact of COPD on health outcomes. The results highlight the substantial burden of COPD compared with the non-COPD population, suggesting that increased attention and targeted interventions are warranted to address the significant health and economic challenges posed by this disease.
Keywords: chronic obstructive pulmonary disease, health-related quality of life, healthcare resource use, work productivity loss, disease costs
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a prevalent and progressive lung disease characterized by persistent respiratory symptoms and airflow limitation.1 It ranks as the third leading cause of death globally, affecting 212.3 million people globally and resulting in 3.3 million deaths annually.2 In China, the overall prevalence of COPD was estimated at 8.6%, impacting approximately 100 million Chinese adults in 2015.3 Notably, China has the largest number of active smokers and a rapidly aging population, which are expected to dramatically increase the incidence of COPD in the coming decades.4 By 2039, it is projected that 103.3 million individuals in China will be affected by this condition.5
COPD patients commonly experience a range of physiological symptoms, including cough, sputum, wheezing and dyspnea, and are often accompanied by psychological symptoms.6 Moreover, compared to the general population, COPD patients face a higher risk of comorbidities.7 Consequently, they often experience poorer health-related quality of life (HRQoL),8–11 increased healthcare resource use (HRU),12 greater work productivity loss,8,11 and higher economic costs.13,14
The detrimental impact of COPD has been well-documented. A multinational survey revealed that COPD has a strong impact on HRQoL, with patients’ quality of life decreasing as the severity of the disease increases.11 Studies have consistently shown that HRQoL is significantly impaired in COPD patients compared to those with other respiratory diseases (eg, allergic rhinitis, asthma, chronic bronchitis) and the non-COPD population.8–10 In addition to its effects on HRQoL, several studies have documented that COPD negatively affects work-related outcomes, such as reduced work productivity while at work (presenteeism),8,11 earlier retirement ages,13 and lower employment rates.15,16 Furthermore, COPD patients experience approximately three times higher HRU than those without this condition,12 resulting in a higher economic burden.13,14 According to a systematic review of the COPD disease burden in China, direct costs caused by HRU range from 499 USD to 1930 USD per capita per year, and indirect costs due to lost work productivity range from 20 USD to 783 USD per capita per year.17
Despite extensive research on the disease burden of COPD, there remains a paucity of research on the humanistic (ie, quality of life) and economic burden of COPD in China, particularly those based on nationally representative samples.12,17 Existing studies have often focused on a limited number of outcomes (eg, HRQoL only, without considering work productivity or costs).17 Moreover, studies assessing the costs of COPD have predominantly been conducted in the USA and Europe, with limited data available for China, especially indirect costs.17–19 Koch et al reported and compared HRQoL, work productivity loss, and HRU between the population with and without COPD using the 2017 China National Health and Wellness Survey (NHWS), but did not focus on the economic burden of COPD.12 The lack of relevant information on the economic burden of COPD is a major reason for the limited attention this disease receives from the government and policymakers. Furthermore, previous studies have exhibited several methodological limitations, including the lack of adjustment for important confounders.20
Therefore, to address these limitations in the existing literature, the present study employed a propensity score matching (PSM) strategy to compare COPD patients with the non-COPD population. The aim was to describe the impact of COPD on a range of humanistic and economic outcomes, including HRQoL, work productivity, HRU, and associated economic costs, thereby providing a comprehensive picture of the burden imposed by COPD in China.
Material and Methods
Data Source and Analysis Sample
This cross-sectional study utilized Cerner Enviza’s existing database from the China National Health and Wellness Survey (NHWS). The NHWS is an internet-based and self-administered nationwide survey of the urban adult population (Tier 1 (large, densely populated urban metropolises such as Shanghai, Beijing, Guanghzhou, etc.) and Tier 2 cities (provincial and sub-provincial capital cities such as Changchun, Changsha, etc.) that provides “real-word” patient-level data on over 200 conditions. Prior publications have summarized the methods of the China NHWS21. It offers a unique perspective on the healthcare market from the viewpoint of the general public. Data were collected annually (or sometimes every other year) from respondents in China and nine other countries (United States, France, Germany, UK, Italy, Spain, Japan, Russia, and Brazil). This study analyzed data from the 2020 China NHWS (N=20051). A stratified random sampling method (stratified by sex and ages) was employed to ensure the sample was representative of the demographic composition of the Chinese urban adult population. All participants were required to be able to read and write Chinese, be aged 18 years or older, reside in China, and provide online written consent. The 2020 NHWS was reviewed by the Pearl Institutional Review Board (Indianapolis, IN) and granted exemption status (Protocol #20-KANT-228).
This study focused on respondents who self-reported a physician diagnosis of COPD. To enhance the specificity of the COPD group, we excluded those patients who self-reported having COPD symptoms but had not been clearly diagnosed by a physician, as well as those at high risk of COPD (ie, respondents with Lung Function Questionnaire scores ranging from 5 and 18). To compare health outcomes, after excluding the aforementioned two categories of respondents, a control group (ie, non-COPD population) was created via propensity score matching (PSM) from the remaining respondents (Figure 1).
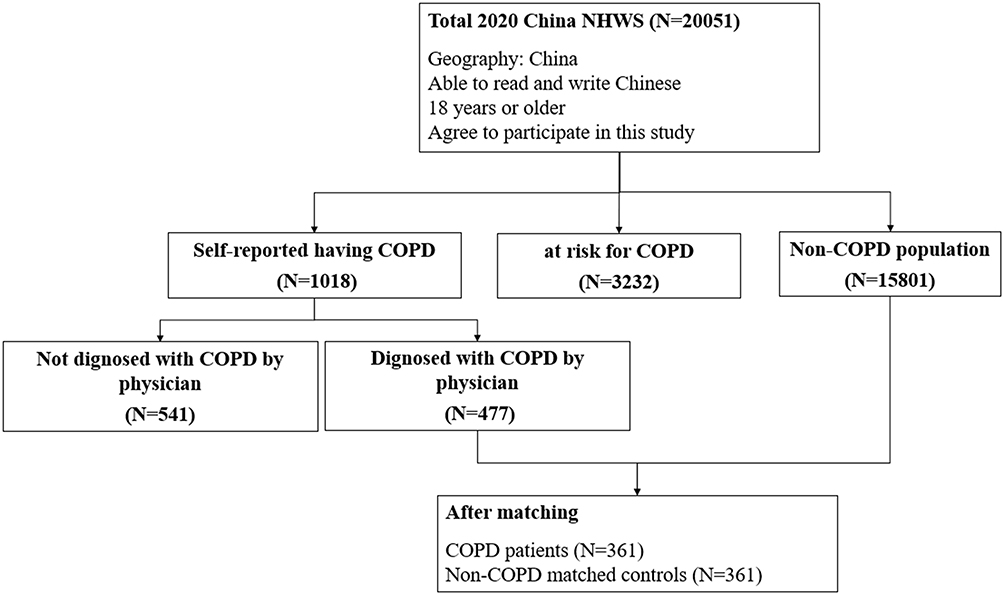 |
Figure 1 Flow chart of sample selection. |
Measures
Demographic and Health Characteristics
The following sociodemographic variables were evaluated: age, gender, marital status, educational level, employment status, monthly household income, and medical insurance status. General health characteristics, including body mass index (BMI), smoking status, alcohol use, exercise behavior, and the Charlson Comorbidity Index (CCI), were collected from all respondents. The CCI is a weighted sum of multiple comorbidities (eg, HIV/AIDS, metastatic tumor, lymphoma), and a higher total CCI score indicating a greater burden from comorbidities.22 Clinical health characteristics were assessed in COPD patients, including frequency of symptoms, exacerbation of symptoms, duration of COPD, and COPD severity.
Health-Related Quality of Life
HRQoL was assessed using the SF-12v2 and EQ-5D-5L. The SF-12v2 consists of 12 items that measure eight health domains, including physical functioning, role physical, bodily pain, general health, vitality, social functioning, emotional role limitations, and mental health, to evaluate both physical and mental health.23 The Physical component summary (PCS) and mental component summary (MCS) scores can be derived from the SF-12v2.23 Higher scores on these scales indicate better quality of life. Previous research has suggested that a differences of 3.0 points on PCS and MCS is considered to be clinically meaningful.24
The EQ-5D-5L comprises a descriptive system based on five dimensions: motility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has a five-point response: no problems, slight problems, moderate problems, severe problems and extreme problems.25 For analysis, health state utility (HSU) was calculated according to the Chinese-specific value set, ranging from −0.391 to 1.000.26 Higher HSU scores indicate better quality of life, while negative HSU represents a certain health status worse than death. Previous studies have suggested that a difference of 0.03 points in HSU is clinically meaningful.27 The validity and reliability of the EQ-5D-5L have been confirmed in Chinese COPD patients.28
Work Productivity and Activity Impairment
Work productivity loss and activity impairment were assessed using the Work Productivity and Activity Impairment (WPAI) questionnaire, a validated 6-item instrument that generates four scores: absenteeism (the percentage of work time missed due to health), presenteeism (the percentage of impairment experienced due to one’s health while at work), overall work productivity loss (a combination of absenteeism and presenteeism), and activity impairment (the percentage of impairment in daily activities due to health). Higher scores indicate greater impairment and reduced productivity over the past 7 days.29 Absenteeism, presenteeism, and overall work impairment were calculated only for respondents who reported being employed full-time or part-time. Data on activity impairment were provided by all respondents.
Healthcare Resource Use
Healthcare resource use (HRU) was evaluated using two distinct items. Specifically, respondents reported the number of outpatient visits, including visits to primary care provider and respiratory specialist, as well as the number of hospitalizations over the past 6 months.
Direct and Indirect Costs
To calculate the direct costs of COPD patients, we projected annual data by multiplying the number of outpatient visits and hospitalizations by two. We then multiplied these figures by per-unit costs of outpatient visits and hospitalizations, respectively, which were obtained from a previous study measuring COPD costs.
The total indirect cost was estimated using the human capital method. We integrated the 2020 provincial average wage data from the National Bureau Statistics30 with data from the WPAI questionnaire. Notably, we accounted for wage differences across various provinces in China by multiplying the average wage of the province where each patient is resides by the number of missed work hours to calculate the indirect cost more accurately. Specifically, for each respondent, we calculated the number of hours missed due to absenteeism and presenteeism over the past week and multiplied this by their estimated hourly wage based on the province where they are located. The indirect cost was then annualized by multiplying the weekly estimates by 50 (the number of work weeks in a year).
Statistical Analysis
Descriptive Analyses
Descriptive analyses were conducted to summarize sociodemographic and health characteristics of the COPD patients and non-COPD population before and after matching, as well as the health outcomes of those two groups matching. Continuous variables were presented as means and standard deviations (SD), while categorical variables were presented as numbers and percentages (%).
Bivariate Analyses
To determine significant differences in characteristic and health outcomes between COPD patients and the non-COPD population, chi-square tests were used for categorical variables. For continuous variables, t-tests (or ANOVA, in the case of more than two groups) were used for those with normal distributions, while Mann–Whitney tests or Kruskal–Wallis H-tests were used for those with skewed distributions. For variables with more than two groups (eg, analyzed by ANOVA or Kruskal–Wallis H-test), if the overall test indicated a statistically significant difference (p < 0.05), post-hoc pairwise comparisons were performed. To account for multiple testing in these post-hoc comparisons, the Bonferroni correction was applied by adjusting the significance level to α divided by the number of possible pairwise comparisons (k) for that specific variable (adjusted α = 0.05/k).
Propensity Score Matching (PSM) Analyses
To properly isolate the burden specific to COPD, the PSM method was used in this study. PSM was employed to control for the unbalanced characteristics between COPD patients and the non-COPD population, including age, gender, marital status, educational level, employment status, insurance status, BMI, smoking status, alcohol use, exercise behavior, and CCI. The 1:1 PSM yielded matched pairs of 361 COPD patients and 361 non-COPD individuals, resulting in no significant differences in sociodemographic, general health characteristics, and CCI between the two groups.
Statistical analysis was conducted using SAS software (version 9.4, SAS Institute, Inc., Cary, NC). All the statistical tests were two-tailed, with a significance level set at 0.05.
Results
Characteristics of COPD Patients After PSM
Before PSM, all potential sociodemographic and general health characteristics, except for monthly household income, significantly differed between respondents with and without COPD (Table 1). The matching process successfully eliminated all significant differences between the two groups. After matching, we obtained 361 COPD patients and 361 individuals without COPD (Figure 1).
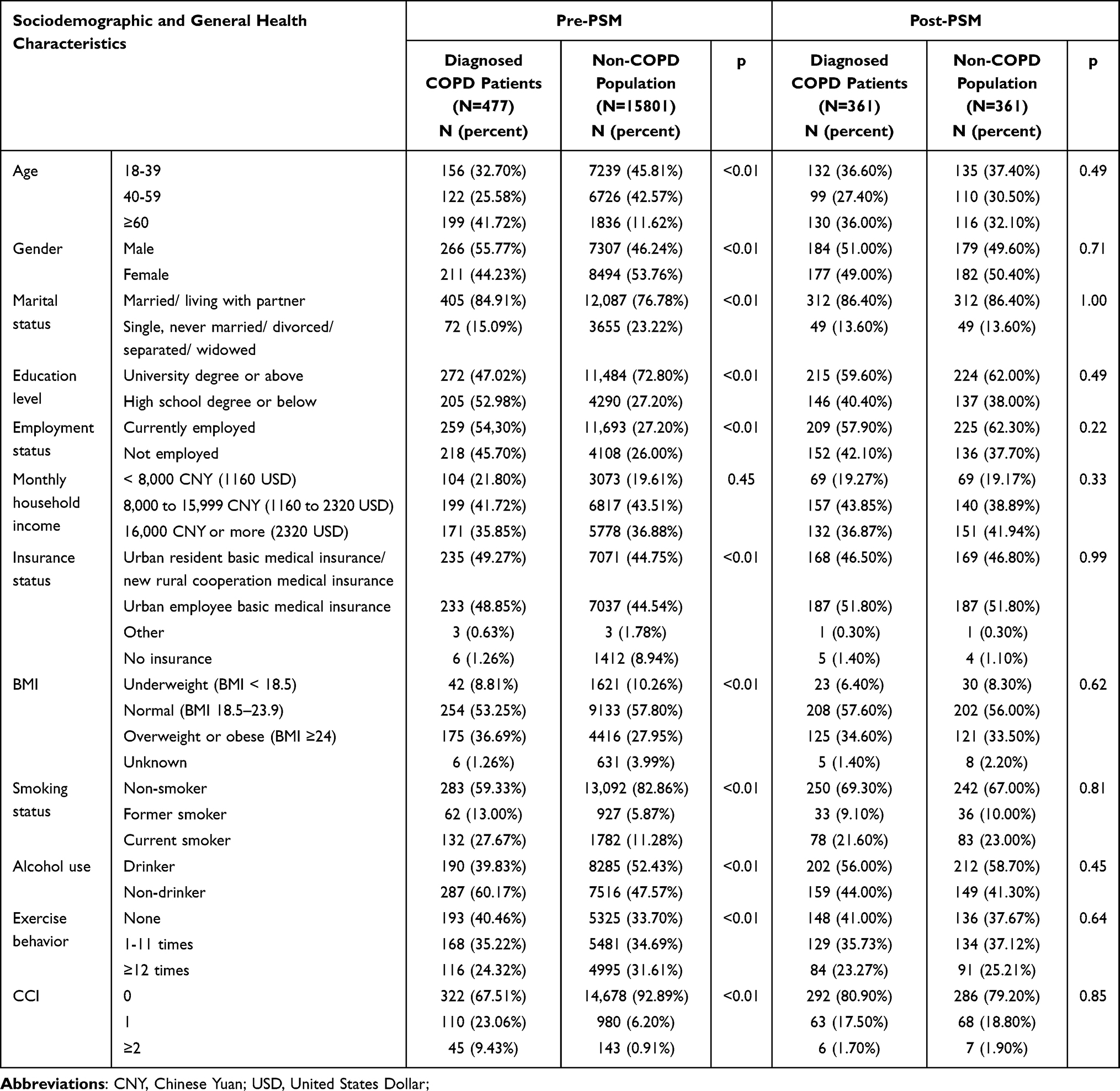 |
Table 1 Comparisons of Sociodemographic and General Health Characteristics Between COPD Patients and Non-COPD Population Pre- and Post-PSM |
Table 1 presents the sociodemographic and general health characteristics of COPD patients after PSM. The majority reported being male (51.00%), married or living with a partner (86.40%), having a university degree or higher (59.60%), and being currently employed (57.90%). Among the 361 COPD patients, the percentages reporting never having experienced dyspnea, fits of coughing, infection, mucous production, and wheezing were 14.96%, 4.99%, 28.81%, 11.63%, and 10.80%, respectively. Most patients (90.30%) did not experience exacerbation of symptoms, and approximately half of the patients had a disease duration of less than 5 years (Table 2).
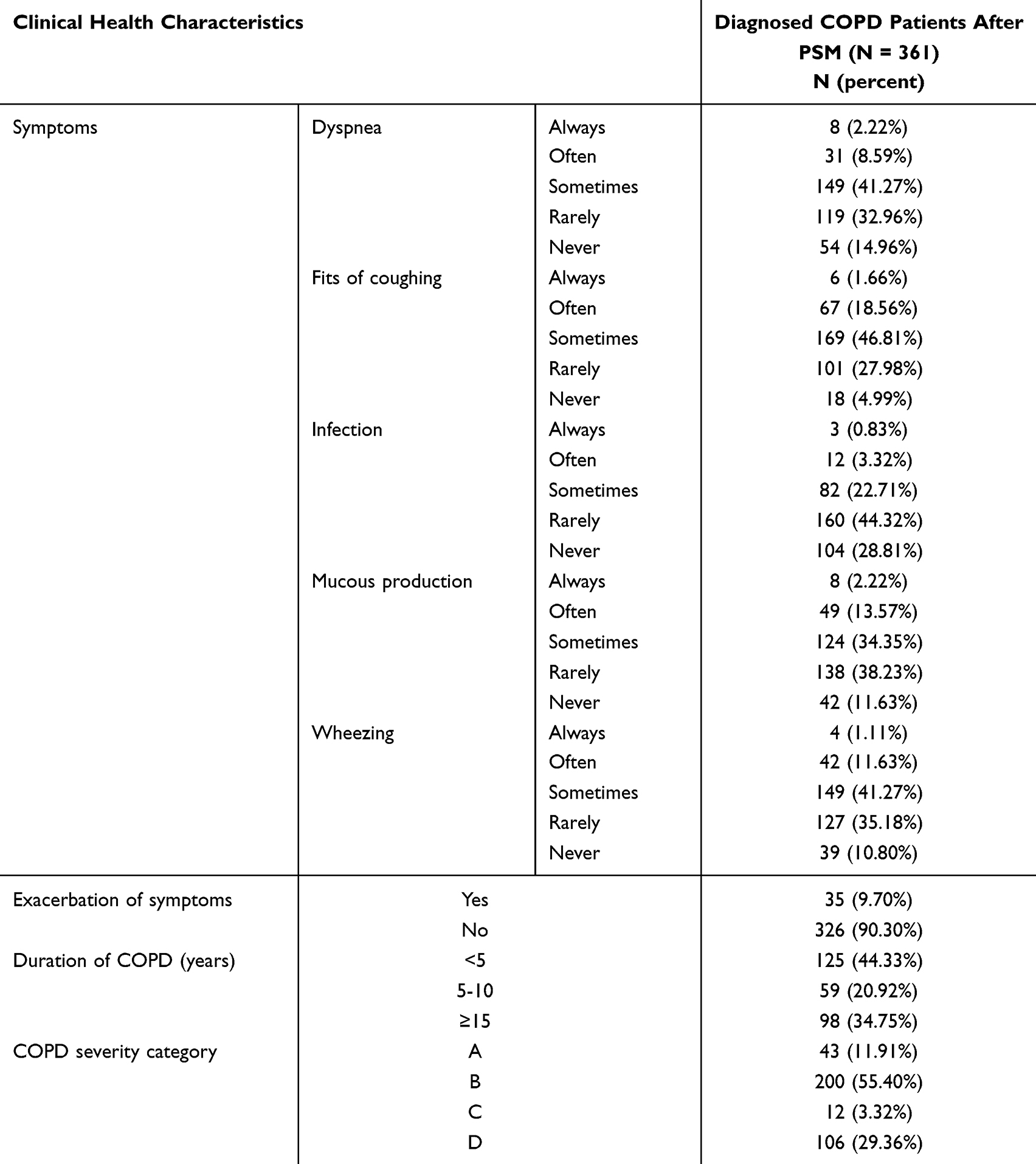 |
Table 2 Clinical Health Characteristics of COPD Patients After PSM |
We also illustrated histogram of the propensity score distributions for the two groups before and after PSM. Supplementary Figure 1A shows the unbalanced distribution of propensity scores for two groups before the PSM. Supplementary Figure 1B displays the balanced propensity score distribution after the PSM.
Humanistic and Economic Burden in Patients with COPD
Table 3 provides a detailed comparison of health outcomes of COPD patients and the control group. Compared to the matched control group, COPD patients exhibited lower quality of life (Table 3). Specifically, COPD patients reported significantly lower mean HSU of EQ-5D-5L (0.90 vs 0.94, P<0.01), MCS scores (47.69 vs 49.49, P<0.01), and PCS scores (47.27 vs 51.71, P<0.01). The percentage of individuals reporting at least a slight problem in each dimension of the EQ-5D-5L was higher among COPD patients than in the control group (Figure 2). Among COPD patients, pain/discomfort was the most frequently reported problem, followed by anxiety/depression.
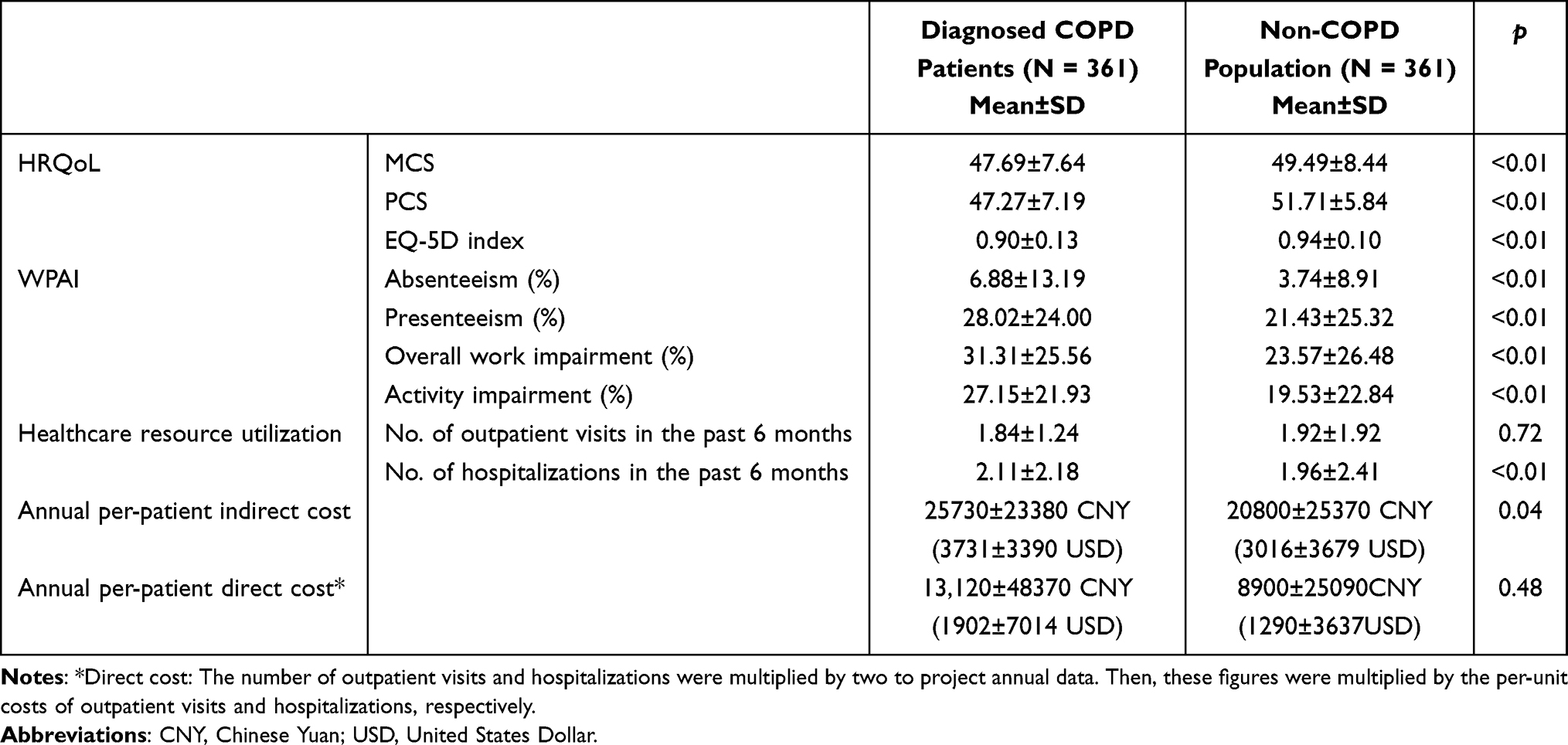 |
Table 3 Comparisons of Post-PSM Disease Burden Between COPD Patients and Non-COPD Population in China |
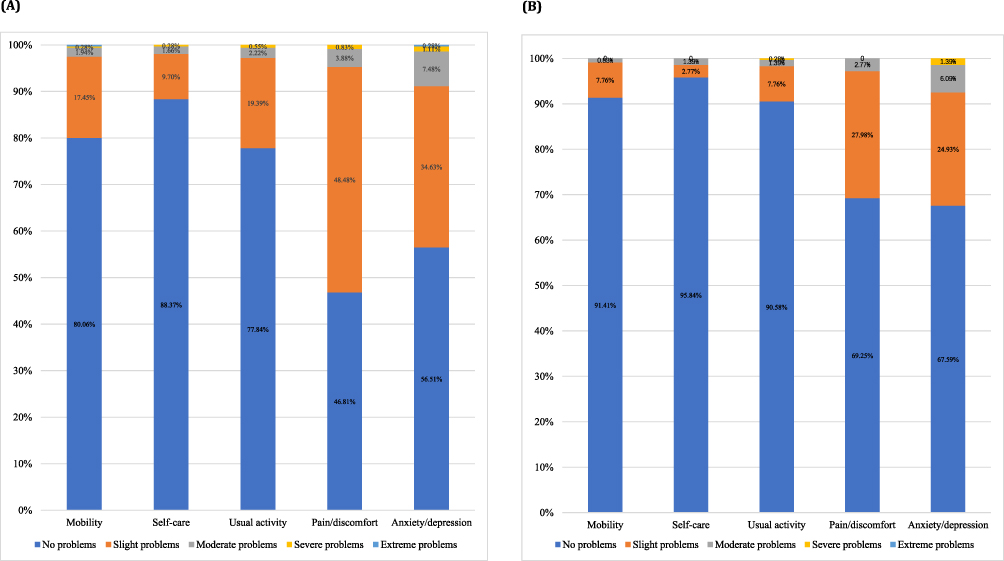 |
Figure 2 Health problems reported by COPD patients and non-COPD population.(A) is health problems reported by 361 COPD patients in each dimension of EQ-5D-5L (B) is health problems reported by 361 control population in each dimension of EQ-5D-5L. |
Work productivity loss was significantly higher among COPD patients compared to their control counterparts (Table 3). COPD patients reported significantly higher mean percentages of absenteeism, presenteeism, overall work impairment, and activity impairment (all P<0.01), indicating greater work productivity loss and activity impairments. Notably, COPD patients reported approximately twice as much absenteeism as the non-COPD population.
The number of hospitalizations of COPD patients in the past 6 months had a substantially higher than matched controls (2.11 vs 1.96, P<0.01). However, COPD patients had fewer outpatient visits than matched controls, although the difference was not statistically significant (1.84 vs 1.92, P=0.72).
Using the aforementioned work productivity loss and healthcare resource data, we derived the indirect and direct costs associated with COPD. COPD patients incurred higher indirect costs (3731 USD vs 3016 USD, P=0.04) compared to the non-COPD population, while the direct cost of COPD patients was 1902 USD.
Discussion
This nationwide real-world survey of adults with and without COPD provided valuable insights into the multifaceted humanistic and economic burden of COPD in China. This population-based comparative study revealed that COPD patients experienced lower HRQoL, higher work productivity loss and activity impairment, a greater number of hospitalizations, higher indirect costs compared to controls without COPD, and the per capita annual direct costs of 1902 USD for COPD patients.
Our study found that individuals with COPD reported significantly lower scores in MCS, PCS and HSU compared to those without COPD.12,31 Notably, the difference in PCS and HSU between COPD patients and controls exceeded the clinically meaningful threshold (ie, PCS difference of over 3 points and HSU difference of over 0.03 points), further confirming the poorer physical health status experienced by COPD patients. However, although a statistically significant difference in MCS was observed between respondents with and without COPD, the meaningful difference cutoff was not reached.24 Moreover, the difference in PCS between the COPD group and the control group was higher than the difference in MCS between the two groups, indicating that COPD generally impacts physical status more than mental status. Therefore, we recommend regular physical training for all COPD patients, as it may significantly improve their physical health status and exercise tolerance.
According to the EQ-5D-5L results, anxiety/depression was the dimension with a higher number of reported problems by COPD patients. This pattern differs from prior studies by Lin et al and Merino et al, which identified mobility as the most problematic dimension.32,33 Potential explanations for this discrepancy may include the younger age profile of our study (64.0% ≤60 years vs predominantly >60 years in prior studies). Supporting this observation, one study used the EQ-5D-5L to assess the health status of China’s urban population and showed that younger individuals experienced more problems with anxiety/depression and fewer problems with mobility compared to older individuals.34 While age distribution may be a contributing factor, other population-specific characteristics (eg, cultural context, comorbidities) could also play a role. Urban environments expose residents to elevated air pollution, a well-established risk factor for airway inflammation and COPD exacerbations,3 which may compound psychological distress in younger urban COPD patients who face disease management. Our findings highlight the necessity to prioritize the mental health of COPD patients, particularly in addressing common comorbidities such as anxiety and depression.
In this study, COPD patients were often accompanied by dyspnea, cough, infection, mucous, and wheezing. These symptoms were associated with significant work productivity loss. The results demonstrated that COPD patients reported higher presenteeism, absenteeism, overall work impairment, and activity impairment compared to non-COPD group, aligning with previously studies.12,31 Consistent with existing literature, absenteeism in COPD patients was nearly twice that of the non-COPD.12 Additionally, presenteeism exceeded absenteeism (28.02% vs 6.88%).This pattern may reflect the impact of symptom burden on workplace performance despite attendance. It is crucial to contextualize these findings within the unique circumstances of 2020, during which the COVID-19 pandemic significantly altered healthcare access, health behaviors, and work patterns globally. The significant increase in presenteeism, which traditionally reflects working while impaired at the workplace, indicates in the context of widespread remote work that the symptom burden experienced by COPD patients is substantial enough to significantly affect their work productivity even when working from home. Moreover, absenteeism may be underestimated in the context of remote work.
In addition to impaired HRQoL, higher work productivity loss and activity impairment, COPD imposed a greater burden on society and the healthcare system due to an increased healthcare resources consumption. We found that COPD patients reported a significantly higher number of hospitalizations than those without COPD, consistent with previous studies.12,35 However, the number of outpatient visits did not significantly differ between COPD and non-COPD populations. One possible reason is that during the pandemic, people more strictly adhered to mask-wearing and social distancing measures, which may have reduced non-COVID respiratory infections that are common triggers for COPD exacerbations. This may partially explain the lack of differences in outpatient visits. Moreover, due to the pandemic impact, patients who were limited by symptoms and had low expectations of their disease may have postponed medical visits.36 The predominantly young cohort with short disease duration may have been more inclined to adopt a “watch and wait” approach, especially when healthcare access was perceived as risky or limited.
Our study revealed that COPD patients reported higher costs compared to the control group. To our knowledge, few prior studies have reported costs arising from work productivity loss and healthcare resource use associated with COPD in China. In this study, we estimated the per capita annual direct cost of COPD patients to be 1902 USD. This estimation was derived by doubling the costs observed over a 6-month period. However, it is important to acknowledge that this approach may not fully capture the seasonal variation in COPD exacerbations, particularly for patients with moderate-to-severe disease, where exacerbations are more frequent and often peak during colder months. Consequently, while our estimate appears similar to the result reported by Chen et al (1853 USD) in a survey conducted across four urban cities in China,37 direct comparability should be interpreted with caution due to potential methodological differences in capturing annual costs. According to the 2020 China Health Statistical Yearbook, the per capita health expenditure of Chinese individuals was 5112.3 CNY (741.3 USD; 1 CNY: 0.145 USD). Our estimated annual direct cost for COPD patients is higher than this national average, indicating that COPD patients likely face elevated direct costs compared to the general population, though the precise magnitude is subject to the methodological limitation noted above. Furthermore, the current study reported per-patient annual indirect costs of 3731 USD for COPD patients, higher than in previous studies.38–40 A possible reason for this may be related to the difference in income of the study population, as Lou et al and Cai et al surveyed rural patients,38,40 while our study focused on urban patients who typically have higher incomes. Additionally, methodological differences may contribute to this variation, as Lou et al used patients’ life expectancy and average income to compute indirect cost,40 while our study used time loss due to health problems. Given the current cost burden of COPD, early screening and investments in effective interventions against COPD may help reduce economic costs and provide substantial economic returns in the foreseeable future.
The study has several limitations. First, data were collected by self-reported, so diagnoses were not validated through objective means and some potential corresponding biases (eg, recall bias) may present in health outcomes. In this study, we excluded patients who self-reported having COPD but were not diagnosed by a physician. Future validation of the study results could be enhanced by incorporating objective indicators, such as spirometry data. Second, the study was based on a cross-sectional investigation, and therefore it was not possible to examine any causal relationships. The longitudinal data are needed to explore the temporal relationship between COPD and prognosis in the future study. Third, we were unable to stratify the analysis by COPD disease severity (eg, using GOLD staging) due to limitations in the available dataset. Consequently, our findings represent an average burden across the severity spectrum and cannot provide specific insights into how the humanistic and economic burden evolves with disease progression. Fourth, although PSM was employed to balance observed baseline characteristics (including demographics, socioeconomic status, and clinical factors like the CCI), this approach cannot account for unmeasured or unobserved confounders. Residual confounding bias remains a fundamental limitation of this observational study, the direction and magnitude of any potential bias introduced by unbalanced factors are unknown. Additionally, while the CCI provides a valuable composite measure of comorbidity burden, its use during matching may not fully account for the differential impact of specific, individual comorbidities on the outcomes studied. Fifth, the respondents of the NHWS are mainly individuals with internet access, who may differ from the broader population. The study data lacks a detailed breakdown of the respondents’ occupations, such as distinguishing between retirees and employed individuals. This may lead to an underestimation of the true economic burden of the disease on patients when interpreting indirect costs and work absenteeism. Finally, the sample of this study only represents the urban adult population in China, and the total national humanistic and economic burden of COPD needs to be verified in the future studies.
Conclusions
The results from this analysis indicate that adult patients with COPD experience a substantial burden relative to matched controls. Specifically, COPD poses a significant burden on patients, including a decline in HRQoL, higher work productivity loss, greater hospitalization use, and leading to higher direct and indirect costs. Strengthening the standardized management of COPD, early screening and identification of COPD can effectively prevent disease progression and reduce the health and economic burden of COPD.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; HRQoL, Health-Related Quality of Life; HRU, Healthcare Resource Use; NHWS, National Health and Wellness Survey; PSM, Propensity Score Matching; BMI, Body Mass Index; CCI, Charlson Comorbidity Index; PCS, Physical Component Summary; MCS, Mental Component Summary; HSU, Health State Utility; WPAI, Work Productivity and Activity Impairment questionnaire; SD, Standard Deviations; MCID, Minimal Clinically Important Difference; CNY, Chinese Yuan; USD, United States Dollar.
Data Sharing Statement
The data that support the findings of this study are available from Cerner Enviza but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Cerner Enviza.
Ethics Approval and Informed Consent
The NHWS received Pearl Institutional Review Board (Indianapolis, IN, USA) approval (No. Protocol #20-KANT-228), and all respondents were informed about confidentiality in the statement of informed consent. Respondents provided written consent to participate.
Author Contributions
LD, SL and JF conceptualized the rationale and design of the study. LD and YZ draws the original manuscript. ZH, FQ, and MG performed data analysis. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
2. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
4. Yin P, Wu J, Wang L, et al. The Burden of COPD in China and its provinces: findings from the global burden of disease study 2019. Front Public Health. 2022;10:859499. doi:10.3389/fpubh.2022.859499
5. Park JE, Zhang L, Ho YF, et al. Modeling the health and economic burden of chronic obstructive pulmonary disease in China from 2020 to 2039: a simulation study. Value Health Reg Issues. 2022;32:8–16. doi:10.1016/j.vhri.2022.06.002
6. Tsiligianni I, Kocks JWH. Daytime symptoms of chronic obstructive pulmonary disease: a systematic review. NPJ Prim Care Respir Med. 2020;301:6. doi:10.1038/s41533-020-0163-5
7. García-Olmos L, Alberquilla A, Ayala V, et al. Comorbidity in patients with chronic obstructive pulmonary disease in family practice: a cross sectional study. BMC Fam Pract. 2013;14:11. doi:10.1186/1471-2296-14-11
8. DiBonaventura M, Paulose-Ram R, Su J, et al. The impact of COPD on quality of life, productivity loss, and resource use among the elderly United States workforce. Copd. 2012;9(1):46–57. doi:10.3109/15412555.2011.634863
9. Bentsen SB, Rokne B, Wahl AK. Comparison of health-related quality of life between patients with chronic obstructive pulmonary disease and the general population. Scand J Caring Sci. 2013;27(4):905–912. doi:10.1111/scs.12002
10. Cappa V, Marcon A, Di Gennaro G, et al. Health-related quality of life varies in different respiratory disorders: a multi-case control population based study. BMC Pulm Med. 2019;19(1):32. doi:10.1186/s12890-019-0796-8
11. Fletcher MJ, Upton J, Taylor-Fishwick J, et al. COPD uncovered: an international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age population. BMC Public Health. 2011;11:612. doi:10.1186/1471-2458-11-612
12. Koch M, Butt T, Guo W, et al. Characteristics and health burden of the undiagnosed population at risk of chronic obstructive pulmonary disease in China. BMC Public Health. 2019;19:1727. doi:10.1186/s12889-019-8071-8
13. Wacker ME, Jörres RA, Schulz H, et al. Direct and indirect costs of COPD and its comorbidities: results from the German COSYCONET study. Respir Med. 2016;111:39–46. doi:10.1016/j.rmed.2015.12.001
14. Woo L, Smith HE, Sullivan SD. The economic burden of chronic obstructive pulmonary disease in the Asia-Pacific Region: a systematic review. Value Health Reg Issues. 2019;18:121–131. doi:10.1016/j.vhri.2019.02.002
15. de Oca M M, Halbert RJ, Talamo C, et al. Paid employment in subjects with and without chronic obstructive pulmonary disease in five Latin American cities: the PLATINO study. Int J Tuberc Lung Dis. 2011;15(9):1259–1264. doi:10.5588/ijtld.10.0508
16. Sin DD, Stafinski T, Ng YC, Bell NR, Jacobs P. The impact of chronic obstructive pulmonary disease on work loss in the United States. Am J Respir Crit Care Med. 2002;165(5):704–707. doi:10.1164/ajrccm.165.5.2104055
17. Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease burden of COPD in China: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:1353–1364. doi:10.2147/COPD.S161555
18. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of Chronic Obstructive Pulmonary Disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
19. R AU, Ahmad Hassali MA, Muhammad SA, et al. The economic burden of chronic obstructive pulmonary disease (COPD) in the USA, Europe, and Asia: results from a systematic review of the literature. Expert Rev Pharmacoecon Outcomes Res. 2020;20(6):661–672. doi:10.1080/14737167.2020.1678385
20. Rai KK, Adab P, Ayres JG, Jordan RE. Systematic review: chronic obstructive pulmonary disease and work-related outcomes. Occup Med. 2018;68(2):99–108. doi:10.1093/occmed/kqy012
21. Langley PC, Mu R, Wu M, et al. The impact of rheumatoid arthritis on the burden of disease in urban China. J Med Econ. 2011;14(6):709–719. doi:10.3111/13696998.2011.611201
22. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
23. Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
24. Jain S, Gupta S, Li VW, Suthoff E, Arnaud A. Humanistic and economic burden associated with depression in the United States: a cross-sectional survey analysis. BMC Psychiatry. 2022;22(1):542. doi:10.1186/s12888-022-04165-x
25. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20((10):1727–1736. doi:10.1007/s11136-011-9903-x
26. Luo N, Liu G, Li M, Guan H, Jin X, Rand-Hendriksen K. Estimating an EQ-5D-5L Value Set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
27. Bae E, Choi SE, Lee H, Shin G, Kang D. Validity of EQ-5D utility index and minimal clinically important difference estimation among patients with chronic obstructive pulmonary disease. BMC Pulm Med. 2020;20(1):73. doi:10.1186/s12890-020-1116-z
28. Chen J, Wong CK, McGhee SM, Pang PK, Yu WC. A comparison between the EQ-5D and the SF-6D in patients with chronic obstructive pulmonary disease (COPD). PLoS One. 2014;9(11):e112389. doi:10.1371/journal.pone.0112389
29. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
30. National Bureau of Statistics of China. Available from: http://www.stats.gov.cn/sj/ndsj/2021/indexch.htm.
31. Dhamane AD, Witt EA, Su J. Associations between COPD severity and work productivity, health-related quality of life, and health care resource use: a cross-sectional analysis of national survey data. J Occup Environ Med. 2016;58(6):e191–7. doi:10.1097/JOM.0000000000000735
32. Lin FJ, Pickard AS, Krishnan JA, et al. Measuring health-related quality of life in chronic obstructive pulmonary disease: properties of the EQ-5D-5L and PROMIS-43 short form. BMC Med Res Methodol. 2014;14:78. doi:10.1186/1471-2288-14-78
33. Merino M, Villoro R, Á H-V, Carmona C. Health-related quality of life of patients diagnosed with COPD in Extremadura, Spain: results from an observational study. Health Qual Life Outcomes. 2019;17(1):189. doi:10.1186/s12955-019-1244-4
34. Yang Z, Busschbach J, Liu G, Luo N. EQ-5D-5L norms for the urban Chinese population in China. Health Qual Life Outcomes. 2018;16(1):210. doi:10.1186/s12955-018-1036-2
35. D’Souza AO, Shah M, Dhamane AD, Dalal AA. Clinical and economic burden of COPD in a medicaid population. Copd. 2014;11(2):212–220. doi:10.3109/15412555.2013.836168
36. So JY, Nn O, Kenaa B, Williams JG, deBorja CL, Slejko JF. Population decline in COPD admissions during the COVID-19 pandemic associated with lower burden of community respiratory viral infections. Am J Med. 2021;134(10):1252–1259. doi:10.1016/j.amjmed.2021.05.008
37. Chen X, Wang N, Chen Y, Xiao T, Fu C, Xu B. Costs of chronic obstructive pulmonary disease in urban areas of China: a cross-sectional study in four cities. Int J Chron Obstruct Pulmon Dis. 2016;11:2625–2632. doi:10.2147/COPD.S118523
38. Cai L, Wang XM, Liu L, Zhao Y, Golden AR. Socioeconomic differentials of trends in the prevalence and economic burden of chronic obstructive pulmonary disease in rural southwest China. BMC Public Health. 2023;23(1):141. doi:10.1186/s12889-023-15096-x
39. Xu DB, Li HC, M AX. Study on the costs of chronic obstructive pulmonary disease (in Chinese). Chin J Pharm Econ. 2011;6:18–26.
40. Lou P, Zhu Y, Chen P, et al. Vulnerability, beliefs, treatments and economic burden of chronic obstructive pulmonary disease in rural areas in China: a cross-sectional study. BMC Public Health. 2012;12:287. doi:10.1186/1471-2458-12-287
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimizing Treatment for Hospitalized Patients with COPD: A Study on the Impact of a LINE App-Based Multidisciplinary Team Approach Targeting Pharmacological Treatment, Lifestyle Changes, and Smoking Cessation
Huang HY, Chen CL, Lin YL, Chen SC, Lee LC, Dai HM, Chiang CY, Chang YF, Lu H, Lee MR, Yang CC, Su CH, Chiang YZ, Yang MC, Shyu RY, Lan CC
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1149-1159
Published Date: 18 April 2025
Characteristics and Quality of Life of Patients with COPD with Different Degrees of Exercise-Induced Desaturation on Six-minute Walk Test
Gao B, Wang S, Zhao L, Liao H, Qumu S, Wang P, Yang T, Jiang S
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:2381-2391
Published Date: 14 July 2025