Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Optimizing Hepatocellular Carcinoma Selection for Liver Transplantation: The Impact of an Integrated MELD-ALBI Score on Post-Transplant Outcomes
Authors Alkhatib A ![]() , Gomaa AI
, Gomaa AI ![]() , Abdel-Razek W
, Abdel-Razek W
Received 6 April 2026
Accepted for publication 10 June 2026
Published 12 June 2026 Volume 2026:13 614920
DOI https://doi.org/10.2147/JHC.S614920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ali Hosni
Alzhraa Alkhatib, Asmaa Ibrahim Gomaa, Wael Abdel-Razek
Department of Hepatology and Gastroenterology, National Liver Institute, Menoufia University, Shebeen El-Kom, Menoufia, Egypt
Correspondence: Alzhraa Alkhatib, Department of Hepatology and Gastroenterology, National Liver Institute, Menoufia University, Shebeen El-Kom, Menoufia, Egypt, Email [email protected]
Background and Aim: Hepatocellular carcinoma (HCC) is the leading cause of cancer-related mortality in Egypt. The model for end-stage liver disease (MELD) score is the standard for prioritizing liver transplantation (LT) candidates but often underestimates hepatic biosynthetic failure in patients with compensated cirrhosis. This study evaluated the utility of an integrated “MELD-ALBI” classification to refine risk stratification in patients undergoing living donor liver transplantation (LDLT).
Patients and Methods: This retrospective study included 76 adult patients with HCC who underwent LDLT between 2010 and 2021. Patients with early postoperative mortality (< 1 month) were excluded. An integrated model was developed stratifying patients into three classes: Class 1 (low risk): ALBI grade 1, or ALBI grade 2 with MELD < 12; Class 2 (intermediate risk): ALBI grade 2 with MELD ≥ 12; and Class 3 (high risk): ALBI grade 3.
Results: The integrated model achieved a numerically higher diagnostic performance for predicting 1-year mortality (AUC=0.625) compared to MELD (AUC=0.611) or ALBI (AUC=0.593). Kaplan-Meier analysis showed significantly superior survival for Class 1 compared to Class 2 (P=0.029). In univariate Cox regression, Class 2 was associated with a threefold increase in mortality risk compared to Class 1 (HR 3.22, 95% CI 1.05– 9.90, P=0.041), whereas survival outcomes for Class 2 and Class 3 were statistically comparable (P=0.27). In multivariate analysis adjusted for age, Class 2 maintained a high hazard ratio (HR 2.59), though statistical significance was attenuated (P=0.101).
Conclusion: The integrated MELD-ALBI classification identifies a “hidden high-risk” subgroup (Class 2) underserved by standard allocation. We propose assigning exception “Z-points” to these patients to align their priority with biological urgency. This framework offers a potential model for refining allocation.
Keywords: hepatocellular carcinoma, liver transplantation, MELD, ALBI, survival
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy and the third leading cause of cancer-related mortality worldwide and the leading cause of cancer deaths in Egypt.1 Liver transplantation (LT) remains the only curative option that simultaneously addresses both the tumor burden and the underlying cirrhosis.2,3 Historically, the model for end-stage liver disease (MELD) score has served as the gold standard for prioritizing candidates based on waitlist mortality risk.4,5 However, the MELD score has significant limitations in the context of HCC; it primarily reflects renal and coagulative dysfunction but often underestimates the severity of hepatic biosynthetic failure in patients with compensated cirrhosis, potentially delaying life-saving transplantation.6,7 To address this disparity, “exception points” are frequently awarded, yet the optimal stratification of these points remains a subject of ongoing debate, particularly in balancing urgency with post-transplant utility.7–9
In recent years, the albumin-bilirubin (ALBI) grade has emerged as a superior, objective alternative to the Child-Pugh classification for assessing liver function in HCC patients.10,11 Unlike Child-Pugh classification, which relies on subjective variables such as ascites and encephalopathy, the ALBI grade is based solely on albumin and bilirubin levels, offering a more granular assessment of hepatic reserve.12,13 While ALBI has been extensively validated for predicting outcomes after resection and locoregional therapies,14,15 its prognostic value in the setting of liver transplantation—specifically when integrated with the MELD score—remains underexplored. Combining the systemic decompensation metric of MELD with the liver-specific biosynthetic marker of ALBI could theoretically identify a “hidden high-risk” subgroup of patients who are currently underserved by standard allocation algorithms.10
This refinement is particularly critical in the context of living donor liver transplantation (LDLT), which constitutes the predominant form of transplantation in Egypt and many Eastern countries due to the scarcity of deceased donor organs.16,17 In the LDLT setting, the decision to proceed involves not only recipient urgency but also the ethical imperative to justify the risk to a healthy donor.18 Therefore, precise risk stratification is essential to avoid futile transplantation in patients with advanced failure while prioritizing those with intermediate dysfunction who would benefit most from early intervention. This study aims to evaluate the impact of a novel “Integrated MELD-ALBI” classification system on the outcomes of HCC patients undergoing LDLT, proposing a new algorithm to standardize exception point prioritization and refine eligibility criteria.
Patients And Methods
Study Design and Population
This retrospective cohort study included adult patients (≥ 18 years) with HCC who underwent LDLT at the National Liver Institute, Menoufia University, Egypt, between January 2010 and December 2021.
The study was approved by the National Liver Institute’s IRB (Protocol No. 00845/2026), which waived informed consent due to the retrospective nature of the data. All procedures followed the Declaration of Helsinki and ICH-GCP guidelines, ensuring strict data confidentiality. All organs were voluntarily donated with documented informed consent, in full compliance with the Declaration of Istanbul.
Diagnosis of HCC was established based on non-invasive imaging criteria (arterial hyper-enhancement with “washout” in portal venous or delayed phases) according to the American Association for the Study of Liver Diseases (AASLD) guidelines prior to LDLT, and was confirmed histologically in the explant in all cases.19
Inclusion and Exclusion Criteria
Patients were included if they had confirmed HCC and underwent LDLT during the study period. Exclusion criteria were: extrahepatic metastasis or macrovascular invasion; combined hepatocellular-cholangiocarcinoma; history of other malignancies; prior solid organ transplantation; and incomplete preoperative data.
To strictly evaluate the prognostic value of the scoring systems and avoid immortal time bias, patients who died within the first postoperative month were excluded from the survival analysis.
Data Collection and Clinical Definitions
Demographic, clinical, and laboratory data were retrieved from medical records. Laboratory parameters included serum bilirubin, albumin, creatinine, sodium (Na), international normalized ratio (INR), and alpha-fetoprotein (AFP).
Liver disease severity was assessed using the Child-Pugh,20 Model for End-Stage Liver Disease (MELD),4 and MELD-Na21 scores. Tumor burden was staged according to the Barcelona Clinic Liver Cancer (BCLC) staging system,22 and the Milan criteria was used to accept patients to undergo transplant.23
Calculation of Prognostic Scores
The ALBI score was calculated using the formula: (log10 bilirubin [μmol/l] x 0.66) + (albumin [g/l] x −0.085) (12). ALBI grades were stratified as:
- Grade 1: Score ≤ −2.60.
- Grade 2: Score > −2.60 to ≤ −1.39.
- Grade 3: Score > −1.39.
Proposed Integrated MELD-ALBI Classification
We developed an integrated risk stratification model combining the ALBI grade (representing hepatic biosynthetic reserve) and the MELD score (representing systemic decompensation). Based on survival analysis, a MELD cutoff of 12 was identified as the optimal discriminator. The optimal MELD cutoff was determined by testing all integer values between 6 and 25 using log-rank survival analysis. A score of 12 was identified as the threshold yielding the most significant separation in survival curves (P=0.032) for this cohort. Patients were stratified into three risk classes:
- Class 1 (low risk): Patients with ALBI grade 1 or 2 with MELD score < 12.
- Class 2 (intermediate risk): Patients with ALBI grade 2 with MELD score ≥ 12.
- Class 3 (high risk): Patients with ALBI grade 3.
Statistical Analysis
Quantitative data were expressed as mean and standard deviation. Categorical variables were expressed as frequencies and percentages. Overall survival (OS) was calculated from the date of transplantation to the date of death or last follow-up. Survival curves were generated using the Kaplan-Meier method and compared using the Log rank test. To compare the predictive performance of the scoring systems for 1-year mortality, receiver operating characteristic (ROC) curve analysis was performed, and the area under the curve (AUC) was calculated. Predictors of post-transplant mortality were identified using univariate and multivariate Cox proportional hazards regression. Variables with a P value < 0.10 in univariate analysis were included in the multivariate model.
All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). A two-tailed p-value < 0.05 was considered statistically significant.
Results
Study Cohort and Baseline Characteristics
Of 88 patients with HCC who underwent LDLT during the study period, 76 patients met the final inclusion criteria. Twelve patients were excluded: 11 due to early postoperative mortality (< 1 month) and one due to combined HCC-cholangiocarcinoma.
The cohort was predominantly males (94.7%) with a mean age of 48.9 ± 7.6 years. The primary etiology of liver disease was HCV-related cirrhosis (93.4%). The mean MELD score was 13.5 ± 4.2. Regarding tumor burden, 81.6% of patients were within Milan criteria, and 51.3% presented with a single nodule. Thirteen patients (17.1%) were classified as BCLC Stage D; notably, all 13 patients in this subgroup presented with Child-Pugh Class C decompensation. Baseline characteristics are detailed in.Table 1
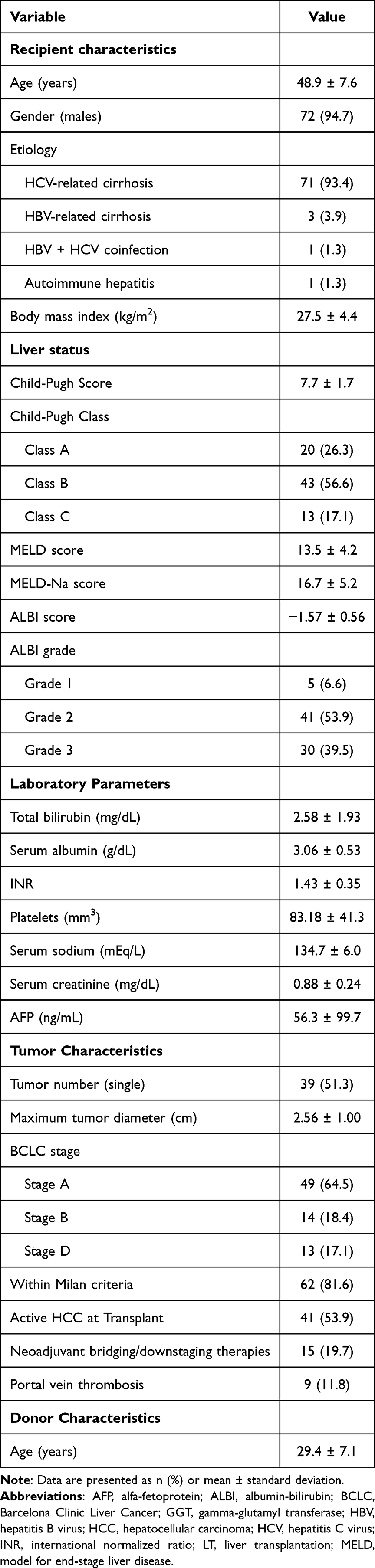 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Cohort |
Survival Analysis
The overall 1-, 3-, and 5-year survival rates were 80.1%, 77.0%, and 70.3%, respectively.
Survival outcomes were stratified by pre-transplant prognostic scores: (Figure 1, panels A–D).
- MELD score: Patients with a MELD score < 12 had significantly superior overall survival compared to those with a MELD score ≥ 12 (P = 0.032) (Figure 1A).
- ALBI grade: Patients with ALBI Grade 2 showed higher 1-year survival compared to ALBI Grade 3 (80.3% vs. 76.7%), though the difference was not statistically significant (P > 0.05) (Figure 1B).
- BCLC stage: There was no statistically significant difference in survival between BCLC Stages A, B, and D (Log-rank P > 0.05 for all pairwise comparisons) (Figure 1C).
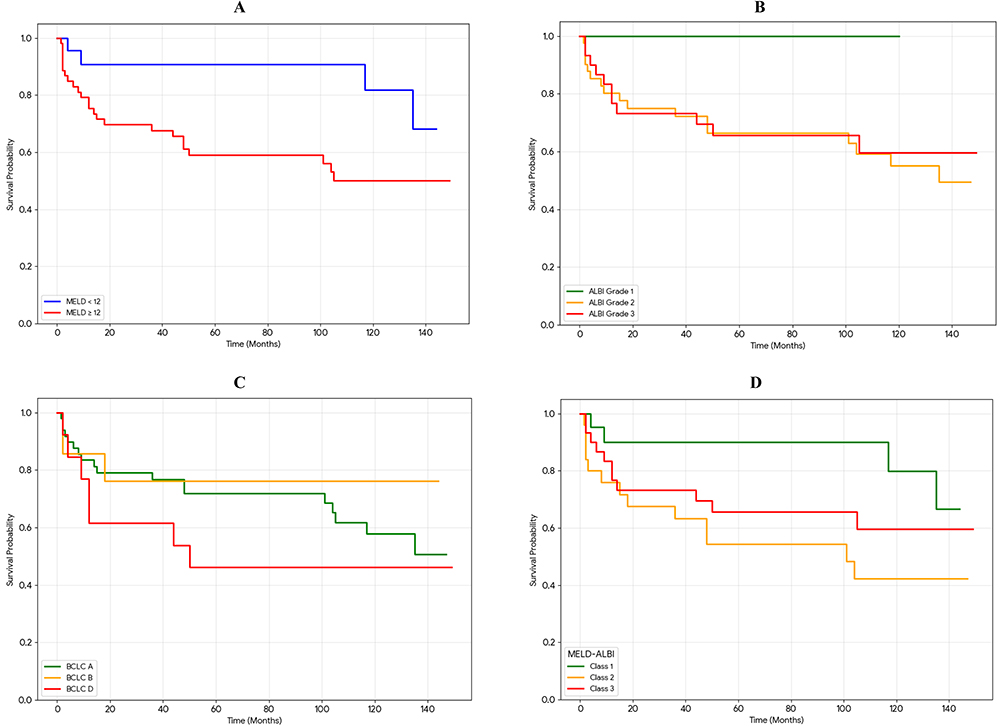 |
Figure 1 Comparative survival stratification: (A), MELD score cutoff 12; (B), ALBI grade; (C), BCLC; (D), Integrated MELD-ALBI classes. |
Diagnostic Performance
ROC curve analysis was performed to predict 1-year mortality. The Integrated MELD-ALBI model yielded an AUC of 0.625 (95% CI: 0.44–0.79). The MELD score alone yielded an AUC of 0.611 (95% CI: 0.43–0.78), and the ALBI score alone yielded an AUC of 0.593 (95% CI: 0.42–0.76) (Figure 2).
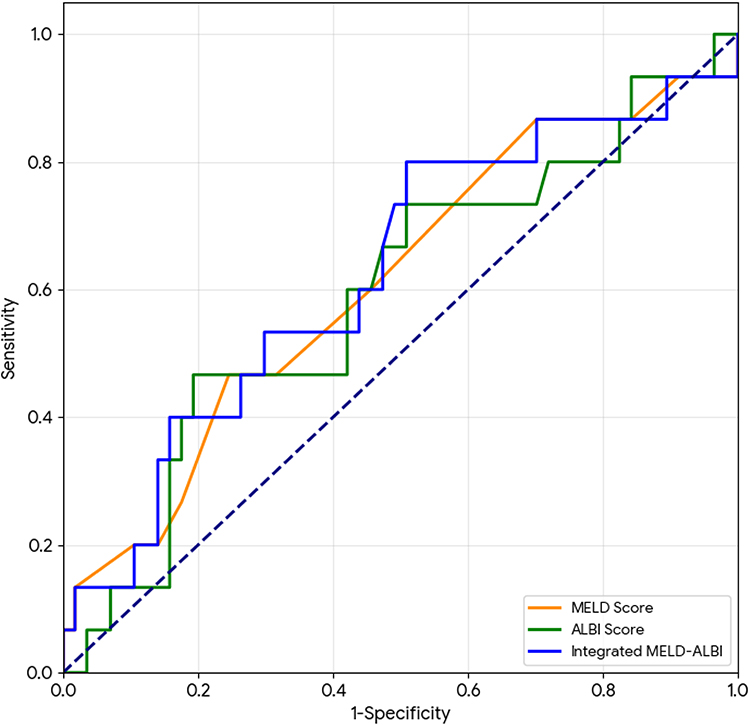 |
Figure 2 Receiver operating characteristic (ROC) curves for 1-year mortality prediction. |
Predictors of Post-Transplant Mortality
Univariate and multivariate Cox proportional hazards regression analyses were performed (Table 2). In univariate analysis, MELD-ALBI Class 2 was significantly associated with increased mortality compared to Class 1 (HR 3.22, 95% CI 1.05–9.90, P=0.041). Other significant predictors included recipient’s age (HR 1.07, P=0.024), serum sodium (HR 0.93, P=0.040), and MELD-Na (HR 1.15, P=0.003).
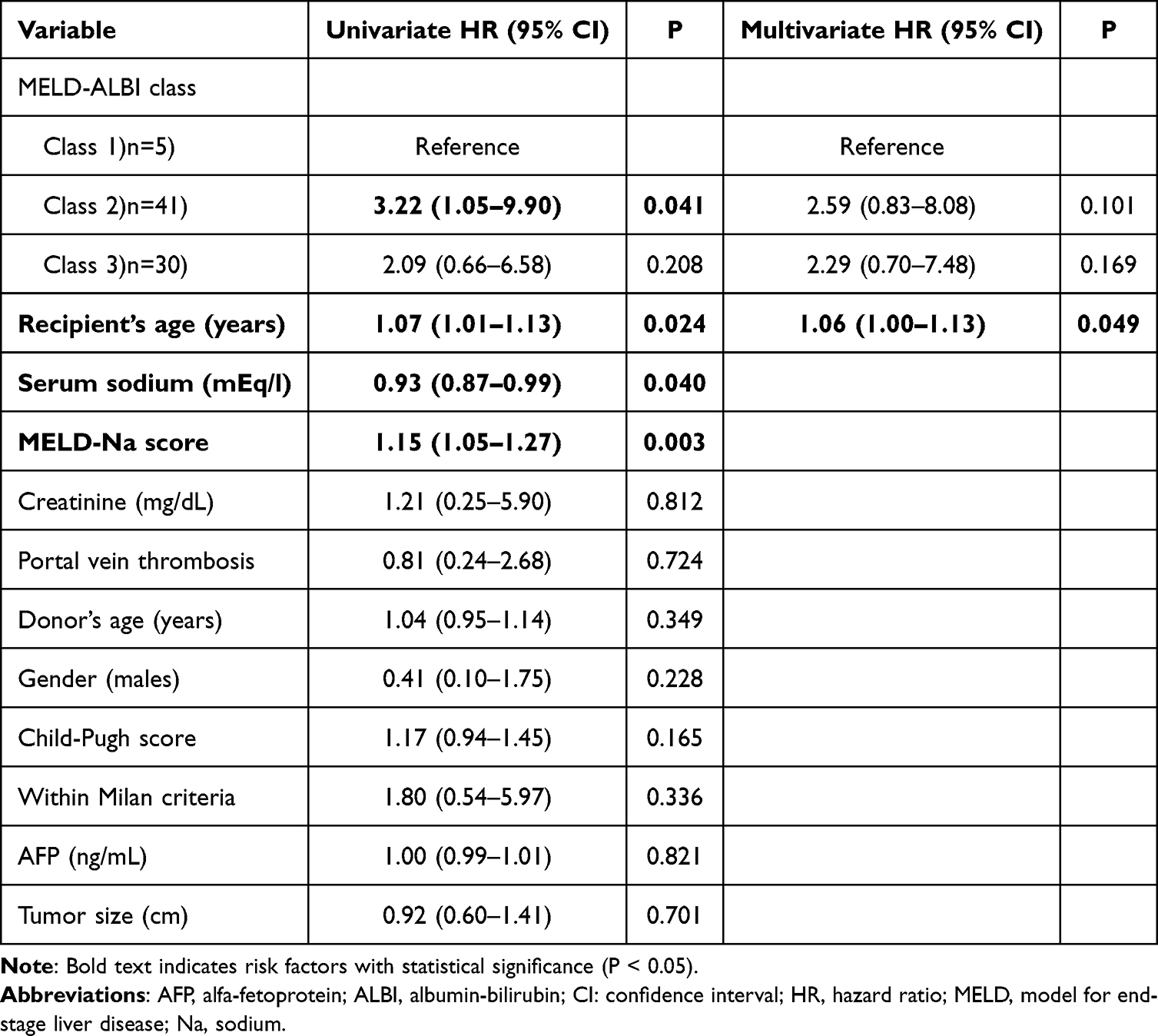 |
Table 2 Univariate and Multivariate Cox Proportional Hazards Regression for Overall Survival |
In the multivariate model adjusted for recipient’s age, MELD-ALBI Class 2 showed a hazard ratio of 2.59 (P=0.101), and recipient’s age remained significant (HR 1.06, P=0.049). Serum Sodium and MELD-Na were excluded from the multivariate analysis due to missing data in 25% of the cohort (n=19). In addition, MELD-Na was excluded to avoid multicollinearity with the MELD-based components of the proposed classification.
Evaluation of the Integrated MELD-ALBI Classification
Patients were stratified into three classes according to the proposed algorithm (Figure 3). Kaplan-Meier survival analysis (Figure 1D) demonstrated that Class 1 (low risk) patients had significantly better survival compared to Class 2 (intermediate risk) (P=0.029). There was no statistically significant difference in survival between Class 2 and Class 3 (high risk) (P=0.27).
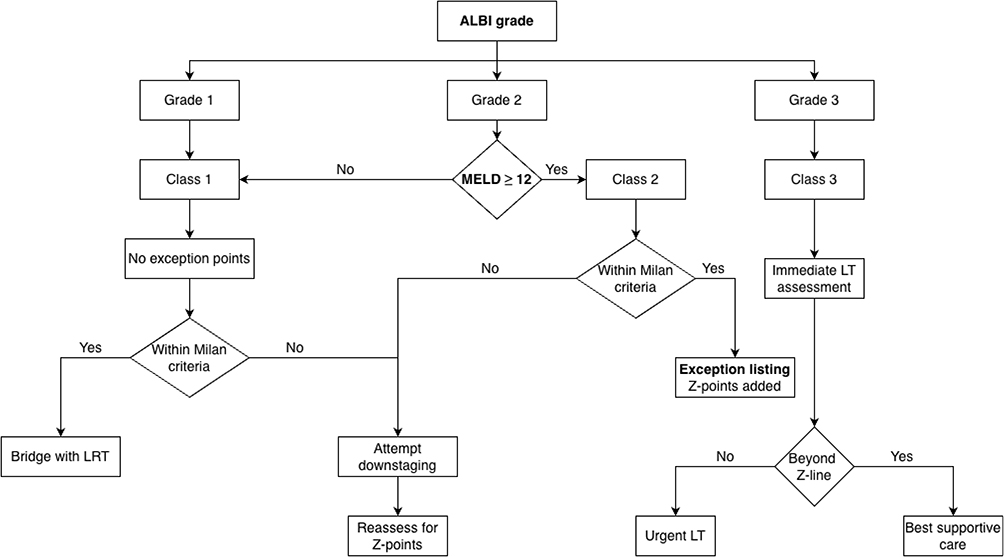 |
Figure 3 Proposed Integrated MELD-ALBI selection algorithm for HCC transplantation. |
Discussion
The primary challenge in allocating liver grafts for HCC is balancing urgency with utility. While the MELD score effectively prioritizes candidates with decompensated cirrhosis, it frequently underestimates the mortality risk in HCC patients who may suffer from “biological decompensation”—a decline in hepatic biosynthetic reserve captured by albumin and bilirubin—before they develop the renal or coagulative failure driving the MELD score.7,12 This discrepancy is particularly acute in Egypt, where the reliance on LDLT necessitates a precise justification of risk to healthy donors.16 In this study, we proposed and evaluated an “Integrated MELD-ALBI” classification. Our principal finding is that patients with “Intermediate Risk” (Class 2: ALBI Grade 2 and MELD ≥ 12) represent a distinct, high-risk subgroup with a threefold increase in post-transplant mortality compared to low-risk candidates, justifying their prioritization for exception points.
Our analysis identified a MELD score of 12 as the optimal cutoff for risk stratification in this cohort, which is lower than the traditional cutoff of 15 often cited in western deceased-donor liver transplant literature.24 This lower threshold likely reflects the specific dynamics of LDLT. In a living donor setting, the “waitlist” is theoretical; the timing of surgery is determined by donor availability and the transplant team’s assessment of futility. Consequently, patients are often transplanted earlier in their disease course than those on deceased donor lists. We demonstrated that even at this lower MELD threshold, adding the ALBI grade significantly refines prognosis. Patients with MELD scores ≥ 12 who also had compromised biosynthetic function (ALBI Grade 2) had significantly worse survival (P=0.029) than those with preserved function, proving that MELD alone is insufficient to capture the full spectrum of risk.
A striking finding of our study was the “survival paradox” observed between Class 2 and Class 3 patients. While Class 2 was a significant predictor of mortality (HR 3.22), Class 3 (High Risk) did not reach statistical significance compared to Class 1. This seemingly counterintuitive result might be explained by the stringent selection bias inherent to LDLT, where recipients with marginal physiological reserves are frequently excluded to minimize donor risk, a practice well-documented in LDLT selection protocols.17 Patients with ALBI Grade 3 (advanced decompensation) undergo rigorous multidisciplinary screening; only those with the most favorable anatomical and biological profiles are cleared for living donor transplantation to avoid futile outcomes. In contrast, Class 2 patients—who occupy a “grey zone” of intermediate dysfunction—may be perceived as “safe enough” for transplant, yet they harbor underestimated physiological instability that manifests as increased post-transplant mortality. This identifies Class 2 as a “hidden high-risk” phenotype that requires more aggressive prioritization (via Z-points) to prevent waitlist dropout or post-transplant deterioration.
Regarding diagnostic performance, the Integrated MELD-ALBI model achieved an AUC of 0.625 for predicting 1-year mortality. While this value falls below the traditional threshold of 0.70 often used to denote “good” discrimination, it must be interpreted within the unique context of HCC allocation, where discrimination is notoriously difficult due to competing risks ranging from tumor recurrence to graft failure.25,26 Although the integrated model achieved a numerically higher AUC than MELD (0.611) or ALBI (0.593) alone, the overlapping confidence intervals indicate that this improvement did not reach statistical significance. Nevertheless, in this setting, even incremental gains in predictive accuracy can meaningfully impact waitlist equity. Crucially, the true value of the MELD-ALBI model lies not in its raw diagnostic superiority, but in its ability to categorize patients into actionable risk strata (Class 2 vs. Class 1)—a granular distinction that MELD alone fails to capture. Thus, the integrated model serves as a valuable complementary decision aid for candidates with identical MELD scores who carry vastly different biological risks.
To operationalize these findings, we propose the assignment of “Z-points” (Zone-points) to Class 2 candidates. Conceptually, Z-points would function similarly to standard HCC exception points but are triggered by biological instability (ALBI Grade) rather than tumor size. For a patient with a MELD score of 13 but ALBI Grade 2 (Class 2), the addition of Z-points would elevate their priority to match that of a patient with biochemical decompensation (eg., MELD 18–20). This adjustment aims to bridge the gap between their static MELD score and their true mortality risk (HR 3.22), ensuring they are offered transplantation before crossing the “Z-line” into futility.
We also evaluated standard prognostic systems. Consistent with recent literature, traditional morphological staging (BCLC) failed to stratify survival in our cohort.22 In our cohort, BCLC Stage D reflected decompensated liver function (Child-Pugh C) rather than extensive tumor burden, making transplantation the only curative rescue therapy. Consequently, these patients, otherwise limited to palliative care, achieved survival rates comparable to early-stage patients after transplantation. This confirms that in the era of transplant oncology, “terminal” liver function (Child-Pugh C) should not preclude curative treatment if the tumor biology is favorable. Furthermore, while MELD-Na showed a strong statistical correlation with mortality (P=0.003), its continuous nature lacks the actionable “categorization” needed for allocation policy. The MELD-ALBI Classes offer a practical advantage by grouping patients into clear actionable strata (Low, Intermediate, High) that can be directly linked to policy decisions like assigning exception points.
This study has limitations inherent to its single-center, retrospective design. First, the sample size (N=76), while representative of a specialized LDLT center, limited the statistical power of multivariate sub-analyses. Specifically, this necessitated the exclusion of serum sodium and MELD-Na from the final model to preserve cohort size, potentially underestimating their prognostic value. Second, we acknowledge that the significant association between Class 2 and mortality observed in univariate analysis was attenuated in the multivariate model (P=0.101). Given the likely underpowering to detect independent effects in a small cohort, these findings should be considered hypothesis-generating and require validation in larger, multi-center studies. Third, the specific cutoffs identified, such as MELD 12, require external validation to confirm their generalizability. Finally, and most critically, this study was conducted exclusively in an LDLT cohort. The waitlist dynamics, pre-transplant attrition rates, and selection criteria in LDLT differ fundamentally from deceased donor liver transplantation (DDLT). Therefore, the “MELD-ALBI” classes and the proposed “Z-points” must be rigorously validated in DDLT populations before being considered for national deceased donor allocation policies.
In conclusion, the Integrated MELD-ALBI classification successfully identifies a “hidden high-risk” subgroup of HCC patients (Class 2) who harbor significant biological instability despite intermediate MELD scores. While this model was developed in a living donor cohort, the biological principle likely transcends the graft source. Prioritizing these patients with exception points could optimize allocation in both LDLT settings—where donor risk must be justified—and DDLT waitlists, ensuring that scarce organs are directed toward candidates whose physiological urgency exceeds their biochemical MELD score.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this research.
Disclosure
The authors declare no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–10. doi:10.3322/caac.21834
2. Martin P, DiMartini A, Fallon M, et al. Evaluation for liver transplantation in adults: 2013 practice guideline by the AASLD and AST. Hepatology. 2014;59:1144–1165. doi:10.1002/hep.26972
3. European association for the study of the liver. EASL clinical practice guidelines: liver transplantation. J Hepatol. 2016;64(2):433–485. doi:10.1016/j.jhep.2015.10.006
4. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33(2):464–470. doi:10.1053/jhep.2001.22172
5. Wiesner R, Edwards E, Freeman R, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124(1):91–96. doi:10.1053/gast.2003.50016
6. Guo G, Yang W, Sun C, et al. The development and appraisal of meld 3.0 in liver diseases. J Clin Transl Hepatol. 2025;13(1):62–68. doi:10.14218/JCTH.2024.00303
7. Kensinger CD, Feurer ID, Karp SJ. An outcome-based approach to assign meld exception points for HCC. Transplantation. 2017;101(9):2056–2061. doi:10.1097/TP.0000000000001812
8. Habib S, Berk B, Chang CCH, et al. MELD and prediction of post–liver transplantation survival. Liver Transpl. 2006;12(3):440–447. doi:10.1002/lt.20721
9. Mehta N, Heimbach J, Lee D, et al. Wait time and HCC recurrence after LT. Transplantation. 2017;101:2071–2078. doi:10.1097/TP.0000000000001752
10. Toyoda H, Johnson PJ. The ALBI score: from liver function in HCC to a general measure. JHEP Rep. 2022;4(10):100557. doi:10.1016/j.jhepr.2022.100557
11. Demirtas CO, D’Alessio A, Pinato DJ, et al. ALBI grade: improved model for liver function estimation in HCC. JHEP Rep. 2021;3(5):100347. doi:10.1016/j.jhepr.2021.100347
12. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol off J Am Soc Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
13. Fragaki M, Sifaki-Pistolla D, Kouroumalis E, et al. Comparative evaluation of ALBI, MELD, and Child-Pugh. Ann Gastroenterol. 2019;32(6):626–632. doi:10.20524/aog.2019.0417
14. Chen PC, Chiu NC, Lin HC, et al. ALBI grade and outcomes after RFA in early HCC. J Chin Med Assoc. 2019;82:2–10. doi:10.1097/JCMA.0000000000000001
15. Hiraoka A, Kumada T, Michitaka K, et al. Prognostic use of ALBI grade in 2584 HCC patients. J Gastroenterol Hepatol. 2016;31(5):1031–1036. doi:10.1111/jgh.13250
16. Bhavsar R, Das SAP, Mehta NN. Transplantation in hepatocellular carcinoma – controversies and recommendations. Int J Adv Med Health Res. 2021;8(2):49–56. doi:10.4103/ijamr.ijamr_220_21
17. Goldaracena N, Barbas AS, Ghanekar A, et al. Living donor liver transplantation: current status and recent trends. Curr Opin Organ Transplant. 2015;20(2):226–231.
18. Miller CM. Ethical issues in living donor liver transplantation. Liver Transpl. 2000;6(6 Suppl 2):S85–8. doi:10.1002/lt.500060516
19. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
20. Pugh RNH, Murray-Lyon IM, Williams R, et al. Transection of oesophagus for variceal bleeding. Br J Surg. 1973;60(8):646–649. doi:10.1002/bjs.1800600817
21. Kim WR, Biggins SW, Kremers WK, et al. Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med. 2008;359(10):1018–1026. doi:10.1056/NEJMoa0801209
22. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
23. Mazzaferro V, Regalia E, Gennari L, et al. Liver transplantation for small HCC in cirrhosis. N Engl J Med. 1996;334:693–699. doi:10.1056/NEJM199603143341104
24. Merion RM, Schaubel DE, Wolfe RA, et al. Survival benefit of liver transplantation. Am J Transplant. 2005;5:307–313. doi:10.1111/j.1600-6143.2004.00703.x
25. Noordzij M, Leffondré K, van Stralen KJ, et al. When do we need competing risks in nephrology? Nephrol Dial Transpl. 2013;28:2670–2677. doi:10.1093/ndt/gft355
26. Lai Q, Vitale A, Iesari S, et al. ITT survival benefit of LT in HCC. Hepatology. 2017;66:1910–1919. doi:10.1002/hep.29342
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low MARCO Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma Following Liver Transplantation
Zhang Q, Wei Y, Li Y, Jiao X
Cancer Management and Research 2022, 14:1935-1944
Published Date: 11 June 2022
Delayed Hepatocellular Carcinoma Recurrence After Liver Transplantation: Comprehensive Clinical Characterization of Case Series
Wong TH, Ho CM, Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
Journal of Hepatocellular Carcinoma 2022, 9:1081-1091
Published Date: 17 October 2022
Prognostic Significance of Hemoglobin, Albumin, Lymphocyte and Platelet (HALP) Score in Hepatocellular Carcinoma
Zhou J, Yang D
Journal of Hepatocellular Carcinoma 2023, 10:821-831
Published Date: 2 June 2023
A Novel Four-Gene Signature Based on Nonsense-Mediated RNA Decay for Predicting Prognosis in Hepatocellular Carcinoma: Bioinformatics Analysis and Functional Validation
Zhao J, Wang C, Zhao L, Zhou H, Wu R, Zhang T, Ding J, Zhou J, Zheng H, Zhang L, Kong T, Zhou J, Hu Z
Journal of Hepatocellular Carcinoma 2024, 11:747-766
Published Date: 23 April 2024
Portal Venous and Hepatic Arterial Coefficients Predict Post-Hepatectomy Overall and Recurrence-Free Survival in Patients with Hepatocellular Carcinoma: A Retrospective Study
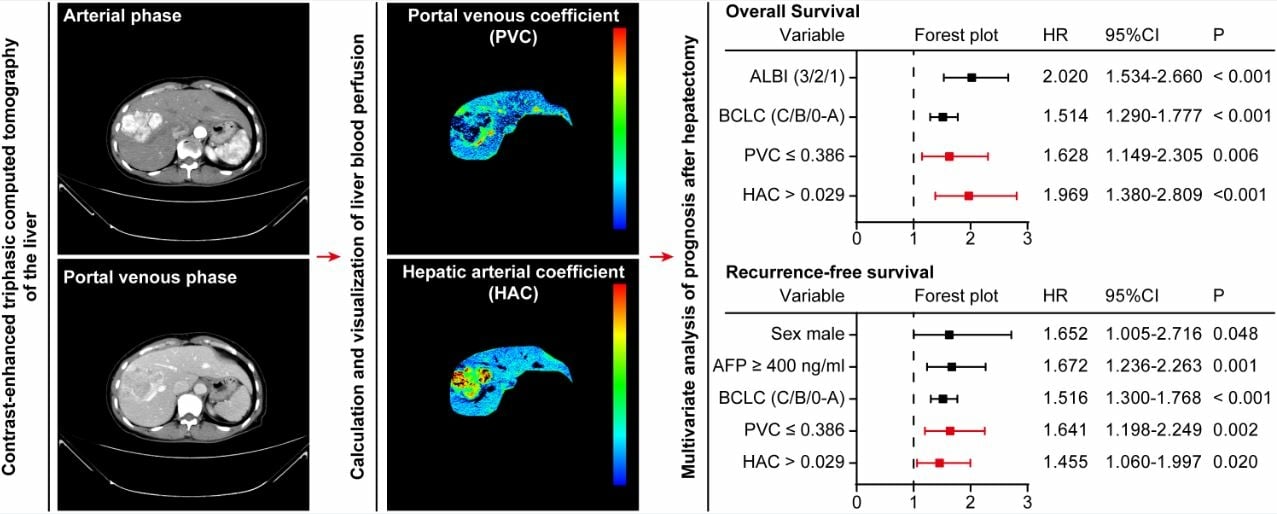
Li YK, Wu S, Wu YS, Zhang WH, Wang Y, Li YH, Kang Q, Huang SQ, Zheng K, Jiang GM, Wang QB, Liang YB, Li J, Lakang Y, Yang C, Li J, Wang JP, Kui X, Ke Y
Journal of Hepatocellular Carcinoma 2024, 11:1389-1402
Published Date: 9 July 2024