Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Optimising GLP-1RA Efficacy: A Meta-Analysis of Baseline Age and HbA1c as Predictors of MACE Reduction in T2DM
Received 22 October 2025
Accepted for publication 18 November 2025
Published 26 November 2025 Volume 2025:18 Pages 4347—4358
DOI https://doi.org/10.2147/DMSO.S575790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Samit Ghosal,1 Anuradha Ghosal2
1Nightingale Hospital, Kolkata, India; 2Aston Medical School, Birmingham, UK
Correspondence: Samit Ghosal, Nightingale Hospital, Kolkata, India, Email [email protected]
Background: Type 2 diabetes mellitus (T2DM) increases major adverse cardiovascular event (MACE) risk, requiring effective interventions. Glucagon-like peptide-1 receptor agonists (GLP-1RAs) reduce MACE, but the impact of baseline characteristics on their efficacy is unclear from previous analyses.
Methods: This PRISMA-guided systematic review and meta-analysis included randomised controlled trials (RCTs) comparing GLP-1RAs with placebo in patients with T2DM, sourced from PubMed and Google Scholar. We extracted MACE hazard ratios (HR), 95% confidence intervals (CI), and baseline characteristics (age, BMI, SBP, HbA1c, eGFR, male proportion, diabetes duration, CVD prevalence). A random-effects model estimated pooled HR, with heterogeneity assessed via prediction intervals. Meta-regression identified moderators. Sensitivity analyses and the RoB 2 Tool assessed bias; GRADE evaluated the certainty of evidence.
Results: Across 11 RCTs (83,536 participants), the pooled HR for MACE was 0.87 (95% CI: 0.81– 0.93), indicating a 13% risk reduction with moderate heterogeneity (prediction interval: 0.79– 0.96). After excluding T2DM duration due to multicollinearity, multivariate meta-regression identified age (p = 0.02) and HbA1c (p = 0.03) as significant moderators, which persisted after excluding FREEDOM-CVO (age, p = 0.03; HbA1c, p = 0.04). Baseline CVD prevalence did not moderate outcomes (p = 0.892). Bias was low; evidence certainty was moderate.
Conclusion: GLP-1RAs reduce MACE in T2DM, particularly in older patients with lower baseline HbA1c. This fills a critical gap in prior meta-analyses by identifying actionable pre-treatment predictors that support personalised therapy.
Protocol Registration: Ghosal et al INPLASY protocol 202580045. doi:10.37766/inplasy2025.8.0045 INPLASY202580045.
Keywords: GLP-1 receptor agonists, type 2 diabetes mellitus, major adverse cardiovascular events, meta-analysis, age, HbA1c
Introduction
Type 2 diabetes mellitus (T2DM) is a global health challenge that significantly contributes to cardiovascular morbidity and mortality.1 Major adverse cardiovascular events (MACE), such as myocardial infarction, stroke, and cardiovascular death, are key concerns in T2DM management, with traditional therapies often falling short in adequately reducing this risk.2
Beyond hyperglycaemia, cardiometabolic risk in T2DM is shaped by chronic low-grade inflammation, endothelial dysfunction, and immune–metabolic cross-talk.3 Glutamine-driven macrophage activation and adhesion-molecule polymorphisms such as ICAM-1 rs5498 have been implicated in atherosclerotic progression, highlighting the biological plausibility that anti-inflammatory or pleiotropic metabolic agents could yield cardiovascular benefit.3
At a health-system level, T2DM imposes a substantial burden through avoidable hospitalisations and comorbidities such as anaemia, even among patients with apparently optimal metabolic control.4 These observations reinforce the unmet need for therapies that address residual cardiovascular risk and improve outcomes across diverse populations. Environmental and hepatic metabolic stressors—for example, those mediated by PI3K/AKT/mTOR signalling- further contribute to this complex risk milieu.5,6
Glucagon-like peptide-1 receptor agonists (GLP-1RAs), a class of incretin-based therapies, have shown promise as they lower glucose and may provide cardiovascular benefits.7 Cardiovascular outcome trials (CVOTs) have demonstrated that GLP-1RAs can reduce MACE, but the consistency and extent of this benefit across different patient groups remain unclear.8
The efficacy of GLP-1RAs may depend on baseline patient characteristics, such as body mass index (BMI), systolic blood pressure (SBP), and diabetes duration, which could influence personalised treatment plans.9 Although prior meta-analyses have confirmed the cardiovascular benefits of GLP-1RAs, few have systematically explored baseline patient characteristics—such as age and HbA1c—as potential moderators of MACE reduction. Observed heterogeneity in trial outcomes (eg, HRs ranging from 0.74 to 1.20) suggests variability in treatment effect that cannot be fully explained by drug class or study design alone. This gap limits the ability to identify patients most likely to benefit, particularly in light of moderate evidence certainty and the growing emphasis on precision medicine in T2DM. We therefore conducted a meta-regression to evaluate age and HbA1c as predictors of GLP-1RA efficacy, aiming to inform personalised therapeutic strategies.
This study aimed to systematically review and perform a meta-analysis of CVOTs to evaluate the effectiveness of GLP-1RAs in reducing MACE in T2DM patients compared to placebo, and to examine the moderating effects of baseline characteristics through multivariate meta-regression. The PICO framework guided the search strategy.
- Population: Adults with T2DM.
- Intervention: GLP-1RA therapy.
- Comparison: Placebo.
- Outcome: MACE (composite of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke).
By addressing these objectives, this analysis aims to provide evidence-based insights into the cardiovascular benefits of GLP-1RAs and to identify patient-specific factors that influence these effects positively or negatively. The protocol was registered with INPLASY (INPLASY202580045, doi: 10.37766/inplasy2025.8.0045).
Methods
Study Design and Search Strategy
This systematic review and meta-analysis followed the guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).6 Two investigators, Dr. Samit Ghosal (MD, FRCP, Consultant Physician at Nightingale Hospital, Kolkata, India) and Miss Anuradha Ghosal (a third-year student at Aston University, Birmingham, UK), independently conducted comprehensive literature searches using PubMed and Google Scholar databases to identify randomized controlled trials (RCTs) comparing glucagon-like peptide-1 receptor agonists (GLP-1RAs) to placebo regarding major adverse cardiovascular events (MACE) among patients with type 2 diabetes mellitus (T2DM). The searches were performed with filters, including the English language and a search period from January 2010 to August 2025, with the final search conducted on August 1, 2025. The keywords used included “GLP-1RA”, “cardiovascular outcome trials”, “MACE”, and “RCT”. Discrepancies between search results were resolved through consensus. An initial total of 537 records were identified from PubMed, of which 153 duplicates were removed. After screening 384 records, 374 were excluded because 221 were not CVOTs, 98 were not RCTs, and 55 did not report MACE. Thus, 10 reports were considered suitable for eligibility assessment. The preliminary Google Scholar search yielded 362 citations, which, after removing duplicates (n=126), irrelevant entries (n=213), and studies not meeting inclusion criteria (n=22), resulted in the inclusion of one additional citation, bringing the total number of studies to 11.10–20 A PRISMA flow diagram illustrating this process is provided in Figure 1. The search was restricted to English-language publications from January 1, 2010, to August 1, 2025. Final searches were conducted on August 1, 2025.
 |
Figure 1 PRISMA flow diagram illustrating the study selection process for randomised controlled trials (RCTs) evaluating glucagon-like peptide-1 receptor agonists (GLP-1RAs) versus placebo in patients with type 2 diabetes mellitus (T2DM), showing the number of records identified, screened, and included (n = 11 trials). |
Eligibility Criteria
Studies were included if they met all of the following criteria (PICO framework):
- Population: Adults (≥18 years) with type 2 diabetes mellitus (T2DM)
- Intervention: GLP-1 receptor agonist (any agent, dose, or duration)
- Comparison: Placebo
- Outcome: Reported major adverse cardiovascular events (MACE) as a 3-point composite (cardiovascular death, non-fatal myocardial infarction, non-fatal stroke) with hazard ratio (HR) and 95% confidence interval (CI)
- Study Design: Randomized controlled trial (RCT)
Studies were excluded if:
- MACE was not reported or not defined as a 3-point composite
- An active comparator was used instead of a placebo
- Population included non-T2DM patients or was restricted to acute coronary syndrome without chronic T2DM
- Only published in abstract form or in a non-English language
- Grey literature (eg, conference abstracts, theses) was not actively searched but included if retrieved and met the criteria
Only full-text peer-reviewed publications were included. No unpublished or grey literature was systematically searched.
MACE Definition Consistency and Standardisation
All included RCTs reported 3-point MACE (cardiovascular death, non-fatal myocardial infarction, non-fatal stroke) as a pre-specified outcome. Although ELIXA and FREEDOM-CVO used 4-point MACE (adding hospitalisation for unstable angina) as their primary endpoint, both trials explicitly reported 3-point MACE hazard ratios (HRs) as secondary outcomes:
- ELIXA: HR = 1.00 (95% CI: 0.87–1.15)
- FREEDOM-CVO: HR = 1.20 (95% CI: 0.88–1.64)
For consistency across all 11 trials, only the 3-point MACE HRs were extracted and used in the meta-analysis. No further adjustment or imputation was required.
Cardiovascular Risk Stratification
No formal thresholds for “moderate” or “high” cardiovascular risk were applied. Inclusion required reporting 3-point MACE as an outcome in T2DM patients, regardless of baseline CV risk. Trials spanned primary prevention (eg, REWIND: 31% CVD) to secondary prevention (eg, ELIXA: 100% CVD).
Data Extraction
Data were independently extracted by two investigators using a standardized form that included trial name, sample size, HR, 95% CI, and baseline characteristics such as age, body mass index (BMI), systolic blood pressure (SBP), glycated haemoglobin (HbA1c), estimated glomerular filtration rate (eGFR), male proportion, diabetes duration, and cardiovascular disease (CVD) prevalence. Discrepancies were resolved through consensus. The baseline characteristics are summarised in Table 1.
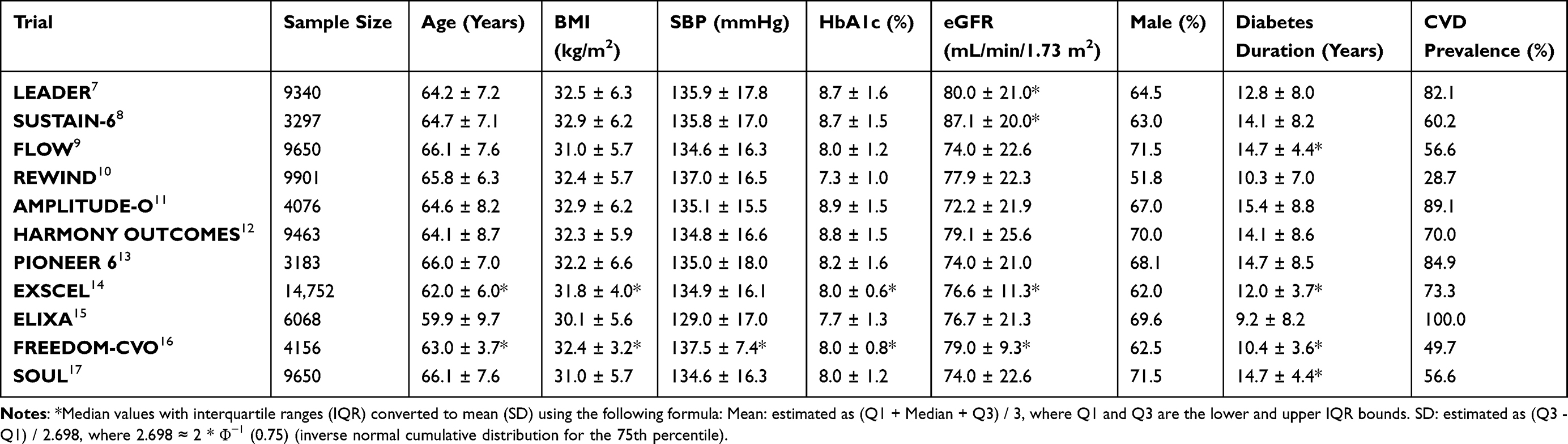 |
Table 1 Baseline Characteristics of 11 RCTs Comparing GLP-1RAs with Placebo in T2DM Patients, Including Sample Size, Mean Age (Years), Body Mass Index (BMI, kg/M2), Systolic Blood Pressure (SBP, mmHg), Glycated Haemoglobin (HbA1c, %), Estimated Glomerular Filtration Rate (eGFR, mL/min/1.73 M2), Male Proportion (%), Diabetes Duration (Years), and Cardiovascular Disease (CVD) Prevalence (%) |
Risk of Bias and Certainty of Evidence
The potential for bias was evaluated utilising the Revised Cochrane Risk-of-Bias Tool for Randomised Trials (RoB 2), which examines domains including random sequence generation, allocation concealment, blinding, and selective reporting. The certainty of evidence was appraised employing the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) methodology, taking into account risk of bias, inconsistency, imprecision, indirectness, and publication bias.
Statistical Analysis
A random-effects model was used to estimate the pooled HR for MACE across the included trials, employing the DerSimonian and Laird method to account for between-study heterogeneity. Heterogeneity was evaluated using the prediction interval. Univariate meta-regression was planned to identify potential moderators among baseline characteristics (age, BMI, SBP, HbA1c, eGFR, male proportion, diabetes duration, and CVD prevalence) using the metafor package in R (version 4.4.3). The significance level was set at p < 0.05, with the QM statistic used to test the overall contribution of moderators and R2 to estimate the proportion of heterogeneity explained.
Following univariate meta-regression (Supplementary Table 2), age, HbA1c, and diabetes duration were significant moderators (p < 0.05). An initial multivariate model including all three showed loss of significance, prompting a formal assessment of multicollinearity. A correlation matrix and approximate variance inflation factors (VIF) were computed using a linear model fitted to logHR and the moderators. Diabetes duration had the highest VIF (4.87), driven by its moderate correlations with age (r = 0.67) and HbA1c (r = 0.66), indicating redundancy in the multivariate model (Supplementary Table 4). It was therefore excluded. The refined multivariate model with age and HbA1c restored significance (p = 0.02 and 0.03, respectively; Table 2) and explained nearly all heterogeneity (R2 = 99.83%, I2 = 0.0%). To evaluate whether baseline cardiovascular risk influenced the meta-regression results, the prevalence of established CVD (%) was included as an additional covariate in an extended multivariate model.
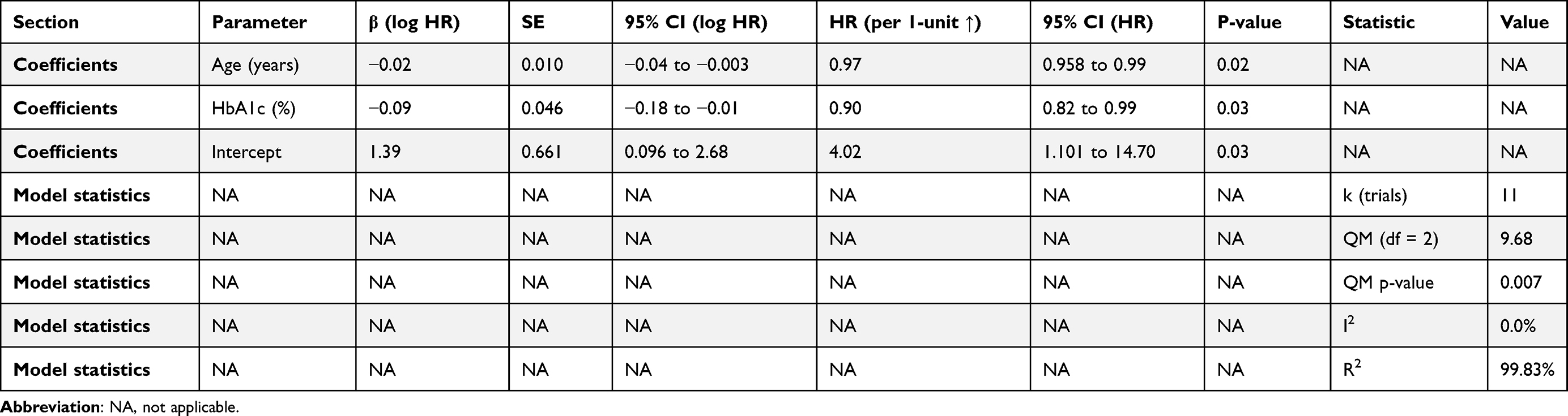 |
Table 2 Multivariate Meta-Regression Results for the Association of Baseline Age (Years) and HbA1c (%) with MACE HR in 11 RCTs of GLP-1RAs versus Placebo in T2DM Patients, Presenting Estimates, Standard Errors (SE), p-values, and Model Statistics (k, QM, QM p-value, I2, R2) for the Entire Model |
Exploration of Other Potential Confounders
All eight baseline characteristics (age, BMI, SBP, HbA1c, eGFR, male proportion, diabetes duration, CVD prevalence) were evaluated in univariate meta-regression (Supplementary Table 2). Only age, HbA1c, and diabetes duration reached p < 0.05 and were entered into multivariate modelling. After excluding diabetes duration due to high VIF (4.87), an extended multivariate model tested CVD prevalence as an additional confounder. It was non-significant (p = 0.892) and did not alter the effects of age or HbA1c. No other variables warranted inclusion based on univariate significance or clinical plausibility within the collinearity framework.
GLP-1RA Class-Effect Assumption
All GLP-1RAs were pooled under a class-effect assumption, consistent with prior CVOT meta-analyses. No subgroup analyses by agent, molecule type (human vs exendin-based), or dose were conducted due to limited power (k = 11) and high heterogeneity in trial designs. However, FREEDOM-CVO (ITCA 650 mini-pump) was included in the sensitivity analysis due to its unique delivery method; its exclusion did not alter the conclusions (see Results). This supports the robustness of the class-level findings.
Sensitivity analysis was planned to evaluate the robustness of the final multivariate model by excluding the trial with the most extreme HR (FREEDOM-CVO, HR = 1.20) based on its potential influence, as determined by influence diagnostics (Cook’s distance, hat values, and standardised residuals) computed using the influence.rma function from the metafor package. All analyses were to be conducted in R, with data and code made available on Figshare (https://doi.org/10.6084/m9.figshare.29918414.v2), accessible publicly with an embargo until the publication date.
Management of Heterogeneity from Baseline Characteristics
Heterogeneity arising from differences in baseline participant characteristics (eg, age, HbA1c, CVD prevalence) was addressed through univariate and multivariate meta-regression using the metafor package in R. This approach directly modelled the influence of each baseline variable on the log hazard ratio (logHR), allowing quantification of their moderating effects. A random-effects model (DerSimonian-Laird) was used to account for residual between-study heterogeneity. Multicollinearity was assessed using correlation matrices and variance inflation factors (VIF); variables with high VIF (>4) were excluded (eg, diabetes duration, VIF = 4.87). Sensitivity analysis excluding influential trials (eg, FREEDOM-CVO) confirmed robustness.
Results
Baseline Characteristics and Comparability
The 11 included RCTs enrolled 83,536 participants with T2DM, but baseline characteristics varied considerably (Table 1). Mean age ranged from 60.3 to 66.3 years, HbA1c from 7.3% to 8.7%, BMI from 28.8 to 33.8 kg/m2, diabetes duration from 8.5 to 15.0 years, and established CVD prevalence from 31% to 100%. These differences reflect diverse trial populations, from primary prevention (eg, REWIND) to high-risk secondary prevention (eg, ELIXA). Such heterogeneity in baseline risk and glycaemic control was expected and was explicitly addressed through meta-regression to identify moderators of treatment effect.
Study Selection and Characteristics
The systematic search identified 11 randomised controlled trials (RCTs) meeting the inclusion criteria, involving a total of 83,536 participants with type 2 diabetes mellitus (T2DM). (Table 1) These trials, conducted across diverse populations, reported major adverse cardiovascular events (MACE) as a primary or secondary outcome, with hazard ratios (HRs) and 95% confidence intervals (CIs) extracted for meta-analysis. Baseline characteristics, including age, body mass index (BMI), systolic blood pressure (SBP), glycated haemoglobin (HbA1c), estimated glomerular filtration rate (eGFR), proportion of males, diabetes duration, and cardiovascular disease (CVD) prevalence, varied across trials, with FREEDOM-CVO showing a notable outlier HR of 1.24. The study selection process is detailed in the PRISMA flow diagram (Figure 1).
Risk of Bias
Risk of bias assessment using the RoB 2 Tool showed low risk across the included trials, with no major issues related to random sequence generation, allocation concealment, blinding, or selective reporting. (Supplementary Figure 1) All five RoB 2 domains (randomisation, deviations, missing data, outcome measurement, and reporting) were rated low risk across all 11 trials, with no single domain contributing concern (Supplementary Figure 1).
GRADE Assessment of Evidence Certainty
The overall certainty of evidence was rated moderate using the GRADE framework (Supplementary Table 1). No downgrading was required for risk of bias (all trials low risk via RoB 2), indirectness (direct evidence from T2DM CVOTs), or publication bias (Egger’s p = 0.72). The evidence was downgraded one level for inconsistency due to moderate heterogeneity (I2 = 36.5%) and one level for imprecision because the prediction interval (0.79–0.96) approached the null value of 1.0. Despite these limitations, the consistent direction of effect and the exclusion of no-benefit support robust clinical confidence.
Pooled Effect Estimate
The random-effects meta-analysis of the 11 trials showed a pooled HR for MACE of 0.87 (95% CI: 0.81–0.93), indicating a 13% risk reduction with GLP-1RA therapy compared to placebo. Moderate heterogeneity was present, with a prediction interval of 0.79–0.96, implying variability in treatment effects across studies (Figure 2).
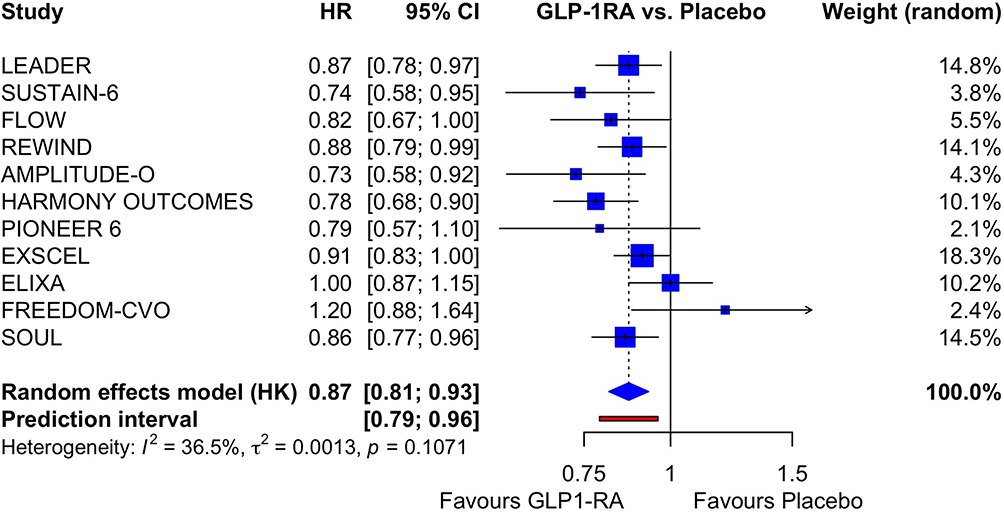 |
Figure 2 Forest plot of hazard ratios (HRs) for major adverse cardiovascular events (MACE) in 11 RCTs comparing GLP-1RAs with placebo in T2DM patients, with 95% confidence intervals (CI) and heterogeneity measures, highlighting the overall effect estimate. |
Publication Bias
Egger’s linear regression test for funnel plot asymmetry was conducted to assess publication bias, yielding a non-significant p-value, indicating no evidence of asymmetry (Supplementary Figure 2).
Moderator Analysis
Univariate meta-regression identified Age, HbA1c, and duration of T2DM as significant moderators (p < 0.05). (Supplementary Table 2) A multivariate meta-regression with these three moderators initially showed no significant effects, prompting an assessment of multicollinearity. (Supplementary Table 3) The correlation matrix and variance inflation factors (VIF) revealed moderate multicollinearity, with the duration of T2DM exhibiting the highest VIF (4.8730), leading to its exclusion. (Supplementary Table 4) A re-analysed multivariate meta-regression with Age and HbA1c restored significance, with Age (p = 0.02) and HbA1c (p = 0.03) showing effects consistent with univariate findings (Table 2).
Sensitivity Analysis and Justification for FREEDOM-CVO Exclusion
FREEDOM-CVO was identified as an influential outlier based on formal diagnostics: HR = 1.20 (the only trial showing no MACE benefit), Cook’s distance = 0.0198 (highest), hat value = 0.0956, and standardised residual = 0.4456 (Supplementary Table 6). It tested a novel ITCA 650 exenatide mini-pump, distinct from injectable or oral GLP-1RAs in other trials. Excluding it in sensitivity analysis maintained significance for age (p = 0.03) and HbA1c (p = 0.04), with improved model fit (R2 = 100.0%, I2 = 0.0%; Supplementary Table 5). Exclusion did not materially alter conclusions; age and HbA1c remained significant moderators supporting robustness across delivery methods.
Discussion
Summary of Key Findings
This meta-analysis of 11 cardiovascular outcome trials (CVOTs) involving 83,536 participants with type 2 diabetes mellitus (T2DM) showed a significant 13% reduction in major adverse cardiovascular events (MACE) with glucagon-like peptide-1 receptor agonists (GLP-1RAs) compared to placebo (pooled HR = 0.87, 95% CI: 0.81–0.93), with moderate heterogeneity (prediction interval 0.79–0.96). (Figure 2) Univariate meta-regression identified age, HbA1c, and duration of T2DM as significant moderators, but multivariate analysis revealed a loss of significance, likely due to moderate multicollinearity (eg, VIF = 4.87 for duration of T2DM). Refining the model by excluding the duration of T2DM restored significance for age (p = 0.02) and HbA1c (p = 0.03). Sensitivity analysis excluding FREEDOM-CVO, an outlier with HR = 1.20 and Cook’s distance = 0.0198, maintained significance for age (p = 0.03) and was borderline for HbA1c (p = 0.04), with a stable model fit (R2 = 100.0%, I2 = 0.0%) (Table 2).
Comparison with Prior Research
The pooled HR is consistent with previous meta-analyses, strengthening the evidence for GLP-1RAs’ cardiovascular benefits in T2DM.8 The notable moderation by Age and HbA1c contrasts with some studies that did not account for multicollinearity, which may have obscured these effects.21,22 The exclusion of FREEDOM-CVO, due to its outlier HR, emphasises the importance of sensitivity analyses, differing from Kristensen et al,20 which included all trials without such adjustments. The initial consideration of the duration of T2DM, despite its nearly significant univariate effect (p = 0.0034), highlights the necessity for multicollinearity checks, a step often missed in earlier meta-analyses.21,22
Strengths and Limitations
Strengths of this study include the comprehensive analysis of 11 CVOTs with 83,536 participants, a PRISMA-guided approach, and the use of random-effects models with meta-regression to explore moderators. The GRADE assessment rated the evidence as moderate, downgraded for inconsistency (I2 = 26.7%) and imprecision (prediction interval including 1), with no significant publication bias (Egger’s p = 0.7171). Limitations include the moderate heterogeneity, which the two final moderators may not fully address, and the risk of overfitting in the initial multivariate model with three predictors across 11 trials. The focus on FREEDOM-CVO exclusion, while justified by influence diagnostics, may limit generalizability to trials with similar outlier profiles. Comorbidities beyond extracted baseline characteristics (eg, heart failure, atrial fibrillation, advanced CKD) were not uniformly reported and could not be analysed. Their potential influence on GLP-1RA efficacy remains unexplored and warrants future individual-patient-data meta-analyses.
What This Study Adds
This study builds on our previous meta-analysis, which identified HbA1c reduction as a key factor influencing the effectiveness of GLP-1RA in reducing MACE, by shifting the focus to baseline characteristics before starting GLP-1RA treatment.23 The strong link between older age and lower baseline HbA1c with greater MACE reduction suggests a personalised treatment approach, pinpointing a specific group of T2DM patients—older individuals with better pre-treatment glycaemic control—who may benefit most from GLP-1RA. Conversely, younger patients or those with higher baseline HbA1c might see less benefit, possibly due to different cardiovascular risk profiles or stages of disease. This interaction between age-related risk and glycaemic status complements the effect of HbA1c reduction, providing a new criterion for pre-treatment selection. The marginal significance of HbA1c after excluding data from FREEDOM-CVO (p = 0.0490) and the moderate heterogeneity indicate that caution is needed in interpretation and that further research is required.
Clinical Implications and Future Research
The findings indicate that GLP-1RAs are most effective in older T2DM patients with lower HbA1c, supporting age- and glycaemic-specific therapy. The model’s stability after excluding FREEDOM-CVO shows robustness against outliers, but the borderline HbA1c effect suggests the need for further validation. Future research should examine additional factors such as drug-specific effects and comorbidities, and utilise individual patient data to address heterogeneity and confirm this tailored subgroup in longer-term studies.
Emerging research using continuous glucose monitoring (CGM) with machine learning has demonstrated predictive value for diabetic retinopathy in type 1 diabetes, while integrated genetic and glycemic profiling is improving immunological risk stratification. Such multimodal strategies may complement GLP-1RA therapy to advance precision medicine in diabetes management.24,25
Clinical Interpretation of Heterogeneity and Prediction Interval
The moderate heterogeneity reflects expected variation in trial populations, designs, and GLP-1RA agents. The prediction interval (0.79–0.96) indicates that in 95% of future similar T2DM populations, GLP-1RA therapy would reduce MACE by 4% to 21%. This excludes no benefit (HR = 1.0) and supports consistent clinical efficacy across diverse settings. The meta-regression findings further refine applicability: older patients and those with lower baseline HbA1c are likely to experience the most significant benefit, enabling personalised treatment selection.
Conclusion
GLP-1RAs reduce 3-point MACE by 13% in T2DM patients (HR = 0.87, 95% CI: 0.81–0.93), with greater benefit in older patients and in those with lower baseline HbA1c (meta-regression p = 0.02 and 0.03, respectively). Clinicians should prioritise GLP-1RAs in this subgroup. Evidence certainty is moderate due to inconsistency and imprecision, but findings are robust across sensitivity analyses. Further studies should validate the pre-treatment selection criteria based on age and HbA1c.
Use of Artificial Intelligence/LLM
Grammarly was used to correct grammatically wrong statements. All other aspects of the paper preparation and the conduction of statistical analysis were done by the authors.
Data Sharing Statement
Data and code supporting this study, including the PubMed search strategy and R scripts used for meta-analysis, are available on Figshare. Ghosal, Samit; Ghosal, Anuradha (2025). Optimising GLP-1RA Efficacy: A Meta-Analysis of Baseline Age and HbA1c as Predictors of MACE Reduction in T2DM. figshare. Dataset. https://doi.org/10.6084/m9.figshare.29918414.v2.
Author Contributions
Dr Samit Ghosal: Conceptualisation, Formal Analysis, Investigation, Methodology, Validation, Visualisation, Writing – original draft, Writing – review & editing.
Miss. Anuradha Ghosal: Data Curation, Investigation, Resources, Writing – review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this paper.
Disclosure
The authors declare no conflicts of interest.
References
1. Siam NH, Snigdha NN, Tabasumma N, Parvin I. Diabetes mellitus and cardiovascular disease: exploring epidemiology, pathophysiology, and treatment strategies. Rev Cardiovasc Med. 2024;25(12):436. doi:10.31083/j.rcm2512436
2. American Heart Association Diabetes Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Clinical Cardiology; and Council on Hypertension; Joseph JJ, Deedwania P, Acharya T, et al. Comprehensive management of cardiovascular risk factors for adults with type 2 diabetes: a scientific statement from the American heart association. Circulation. 2022;145(9):e722–e759. doi:10.1161/CIR.0000000000001040
3. Ren W, Xia Y, Chen S, et al. Glutamine metabolism in macrophages: a novel target for obesity/type 2 diabetes. Adv Nutr. 2019;10(2):321–330. doi:10.1093/advances/nmy084
4. Loutradis C, Skodra A, Georgianos P, et al. Diabetes mellitus increases the prevalence of anemia in patients with chronic kidney disease: a nested case-control study. World J Nephrol. 2016;5(4):358–366. doi:10.5527/wjn.v5.i4.358
5. Yarahmadi A, Azarpira N, Mostafavi-Pour Z. Role of mTOR complex 1 signaling pathway in the pathogenesis of diabetes complications; A mini review. Int J Mol Cell Med. 2021;10(3):181–189. doi:10.22088/IJMCM.BUMS.10.3.181
6. Chu H, Du C, Yang Y, et al. MC-LR aggravates liver lipid metabolism disorders in obese mice fed a high-fat diet via PI3K/AKT/mTOR/SREBP1 signaling pathway. Toxins. 2022;14(12):833. doi:10.3390/toxins14120833
7. Marx N, Husain M, Lehrke M, Verma S, Sattar N. GLP-1 receptor agonists for the reduction of atherosclerotic cardiovascular risk in patients with type 2 diabetes. Circulation. 2022;146(24):1882–1894. doi:10.1161/CIRCULATIONAHA.122.059595
8. Rivera FB, Cruz LLA, Magalong JV, et al. Cardiovascular and renal outcomes of glucagon-like peptide 1 receptor agonists among patients with and without type 2 diabetes mellitus: a meta-analysis of randomized placebo-controlled trials. Am J Prev Cardiol. 2024;18:100679. doi:10.1016/j.ajpc.2024.100679
9. Melo M, Gavina C, Silva-Nunes J, Andrade L, Carvalho D. Heterogeneity amongst GLP-1 RA cardiovascular outcome trials results: can definition of established cardiovascular disease be the missing link? Diabetol Metab Syndr. 2021;13(1):81. doi:10.1186/s13098-021-00698-5
10. LEADER Steering Committee; LEADER Trial Investigators; Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–322. doi:10.1056/NEJMoa1603827
11. SUSTAIN-6 Investigators; Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141
12. FLOW Trial Committees and Investigators; Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. 2024;391(2):109–121. doi:10.1056/NEJMoa2403347
13. REWIND Investigators; Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394(10193):121–130. doi:10.1016/S0140-6736(19)31149-3
14. AMPLITUDE-O Trial Investigators; Gerstein HC, Sattar N, Rosenstock J, et al. Cardiovascular and renal outcomes with efpeglenatide in type 2 diabetes. N Engl J Med. 2021;385(10):896–907. doi:10.1056/NEJMoa2108269
15. Harmony Outcomes committees and investigators; Hernandez AF, Green JB, Janmohamed S, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-controlled trial. Lancet. 2018;392(10157):1519–1529. doi:10.1016/S0140-6736(18)32261-X
16. PIONEER 6 Investigators; Husain M, Birkenfeld AL, Donsmark M, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841–851. doi:10.1056/NEJMoa1901118
17. EXSCEL Study Group; Holman RR, Bethel MA, Mentz RJ, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228–1239. doi:10.1056/NEJMoa1612917
18. ELIXA Investigators; Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373(23):2247–2257. doi:10.1056/NEJMoa1509225
19. Ruff CT, Baron M, Im K, O’Donoghue ML, Fiedorek FT, Sabatine MS. Subcutaneous infusion of exenatide and cardiovascular outcomes in type 2 diabetes: a non-inferiority randomized controlled trial. Nat Med. 2022;28(1):89–95. doi:10.1038/s41591-021-01584-3
20. SOUL Study Group; McGuire DK, Marx N, Mulvagh SL, et al. Oral semaglutide and cardiovascular outcomes in high-risk type 2 diabetes. N Engl J Med. 2025;392(20):2001–2012. doi:10.1056/NEJMoa2501006
21. Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20(1):189. doi:10.1186/s12933-021-01366-8
22. Kristensen SL, Rørth R, Jhund PS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019;7(10):776–785. doi:10.1016/S2213-8587(19)30249-9
23. Ghosal S, Sinha B. The cardiovascular benefits of GLP1-RAs are related to their positive effect on glycemic control: a meta-regression analysis. Diabet Res Clin Pract. 2022;186:109824. doi:10.1016/j.diabres.2022.109824
24. Montaser E, Shah VN. Prediction of incident diabetic retinopathy in adults with type 1 diabetes using machine learning approach: an exploratory study. J Diabetes Sci Technol. 2024;19322968241292369. doi:10.1177/19322968241292369
25. Montaser E, Farhy LS, Rich SS. Enhancing type 1 diabetes immunological risk prediction with continuous glucose monitoring and genetic profiling. Diabetes Technol Ther. 2025;27(4):292–300. doi:10.1089/dia.2024.0496
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relation of Red Cell Distribution Width to Glucose Metabolism and Adverse Long-Term Prognosis in Patients with Acute Coronary Syndrome
Xiong K, Xu C, Shou X, Dong M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:61-70
Published Date: 11 January 2023
Diabetes Mellitus and Its Therapy in Brunei Darussalam – A Critical Revisit
Muhammad Haskani NH, Ming LC, Dhaliwal JS, Wee DVT, Goh BH, Ali M, Shaharuddin S, Goh KW, Goh HP
Patient Preference and Adherence 2023, 17:1131-1136
Published Date: 22 April 2023
Effect of Preoperative Level of Glycemic Control with Pulsed Radiofrequency on the Incidence of Postherpetic Neuralgia in Patients with Herpes Zoster Combined with Type 2 Diabetes Mellitus: A Cohort Study
Hua B, An M, Chen L, Ni H, Ni C, Yao M
Diabetes, Metabolic Syndrome and Obesity 2024, 17:3975-3987
Published Date: 24 October 2024
Evaluating the Overall Safety of Glucokinase Activators in Patients with Type 2 Diabetes Mellitus
Liang TT, Cao MJ, Wang Q, Zou JS, Yang XM, Gu LF, Shi FH
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4539-4552
Published Date: 28 November 2024
Molecular Pharmacology of Glucagon-Like Peptide 1-Based Therapies in the Management of Type Two Diabetes Mellitus and Obesity
Alzahrani AM, Alshobragi GA, Alshehri AM, Alzahrani MS, Alshehri HA, Alzhrani RM, Basudan S, Alkatheeri AA, Almutairi SA, Alzahrani YA
Integrated Pharmacy Research and Practice 2025, 14:59-72
Published Date: 6 April 2025