")
Back to Journals » Patient Preference and Adherence » Volume 17
Diabetes Mellitus and Its Therapy in Brunei Darussalam – A Critical Revisit
Authors Muhammad Haskani NH, Ming LC , Dhaliwal JS, Wee DVT , Goh BH , Ali M , Shaharuddin S, Goh KW, Goh HP
Received 12 March 2022
Accepted for publication 1 November 2022
Published 22 April 2023 Volume 2023:17 Pages 1131—1136
DOI https://doi.org/10.2147/PPA.S366152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Najwa Hazwani Muhammad Haskani,1 Long Chiau Ming,1,2 Jagjit Singh Dhaliwal,1 Daniel Vui Teck Wee,3 Bey Hing Goh,4,5 Majid Ali,6 Shazwani Shaharuddin,3 Khang Wen Goh,7 Hui Poh Goh1
1PAPRSB Institute of Health Sciences, Universiti Brunei Darussalam, Gadong, Brunei Darussalam; 2School of Medical and Life Sciences, Sunway University, Sunway City, Selangor, Malaysia; 3Pharmacy Department, Suri Seri Begawan Hospital, Ministry of Health, Belait, Brunei Darussalam; 4Biofunctional Molecule Exploratory (BMEX) Research Group, School of Pharmacy, Monash University Malaysia, Selangor, Malaysia; 5College of Pharmaceutical Sciences, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 6College of Medicine, Sulaiman Al Rajhi University, Al Bukayriyah, Saudi Arabia; 7Faculty of Data Science and Information Technology, INTI International University, Nilai, Negeri Sembilan, Malaysia
Correspondence: Hui Poh Goh, PAPRSB Institute of Health Sciences, Universiti Brunei Darussalam, Gadong, Brunei Darussalam, Email [email protected]
Introduction: Diabetes is becoming an increasingly common condition across the world including Brunei Darussalam. Bruneian population, although is relatively small, represents a miniature urban community of neighbouring Southeast Asian countries as they share similar dietary and ethnicity patterns. Thus, it would be valuable to examine the findings of studies conducted among Bruneians. This study aimed to identify and review research related to the practice of patients with DM in Brunei Darussalam in order to identify associated factors influencing diabetic medication knowledge and adherence.
Methods: This narrative review analyzed literature related to DM and its therapy in Brunei Darussalam. Other issues consisting of knowledge and adherence related to DM were also explored. Databases (Scopus, PubMed, and Google Scholar) were used to search literature published up to May 2022. Search terms “diabetes mellitus”, “Brunei” combined using Boolean operator were used.
Results and Discussion: Conducting appropriate studies in Brunei Darussalam can benefit the government and policymakers to implement effective measures and programmes to combat the diabetes epidemic. Despite the government’s efforts, additional relevant stakeholders must be included in order to work together and engage in these initiatives in order to increase diabetes awareness, give people the power to make healthy decisions, and ultimately reduce the prevalence of diabetes in Brunei Darussalam. Patients’ medication knowledge proficiency plays a main component of ensuring appropriate and safe use of medication prescribed to them.
Conclusion: Relatively poor medication knowledge and inappropriate diabetes-related practices were observed in studies conducted in Brunei Darussalam. However, no study has been done which directly measures both medication awareness and compliance among Brunei Darussalam T2DM patients. Future studies can focus on the relation between these two factors in different geographical locations of the world that are characterized by different diabetes-related practices and culture.
Keywords: diabetes mellitus, cardiovascular risk factors, healthy lifestyle, education research, health system access
Introduction
Diabetes mellitus (DM) accounted for 10.1% of the total deaths in Brunei Darussalam in 2017. Since 2012, it is the third greatest cause of death in Brunei. It has been reported that the mortality rate from DM was 9.1% in 2016.1 The largest diabetic population of diabetics live in Asia, among the 10 countries to have the most diabetic patients, four are in Asia ie China, India, Indonesia, and Japan. It is assumed that the rapid urbanisation, development and nutritional transition have resulted in Asia being the centre of the global epidemic of DM.2,3 In 2016, diabetes prevalence was 9.7%.1 The study reported it to be a non-communicable disease (NCDs) epidemic in the sultanate, including type 2 DM (T2DM).1 However, it was reported that the prevalence of diabetes was lower in Brunei Darussalam as compared with two other Asian countries including Singapore (11%) and Malaysia (18%).
Furthermore, prevalence of obesity is 28%, which ranks highest amongst Southeast Asian countries and it is a major risk factor for T2DM. In Brunei, smoking and obesity were linked to risk of non-communicable diseases. The standardised methods used in this study are significant for public health interventions surveillance. It may give policymakers the opportunity to more accurately assess the needs of public health, establish priority settings, and create pertinent and appropriate goals. Due to the high prevalence of T2DM in the sultanate, the government has been implementing several initiatives to curtail the disease prevalence.4 The rising obesity issue among youth in Brunei also triggered alarm to nip the problem in the bud before it leads to metabolic syndromes such as DM.5,6
These programmes use a variety of strategies, including health promotion and health education campaigns, in an effort to increase public knowledge of diabetes prevention. A government-run health programme called the Health Screening Effectiveness (3PK) Programme has been put in place for risk assessment and early identification of NCDs, including diabetes. Despite the government’s efforts, additional important stakeholders must be included in order to work together and engage in these initiatives in order to increase diabetes awareness, provide people the power to make healthy decisions, and eventually reduce the prevalence of DM in Brunei Darussalam.7 This review aimed to explore the current diabetes-related practices and associated factors among diabetes mellitus patients in Brunei Darussalam.
Methods
This narrative review focused on two aspects of DM; studies conducted in Brunei Darussalam and/or targeting the residents of Brunei Darussalam and related to its therapy. The published reports were searched through online databases: Scopus, and PubMed. Google Scholar was also used to find reports published in non-indexed journals from inception till 31 May 2022.
Search terms “diabetes mellitus” and “Brunei Darussalam” were used along with Boolean search strategy “AND.” A total of 32 articles were found. After screening for relevance, only five articles were included in the review.
Results and Discussion
Diabetes Studies Done in Brunei Darussalam
Five relevant diabetes-related studies that had been conducted in Brunei Darussalam were found and these studies had several emphases as shown in Table 1.
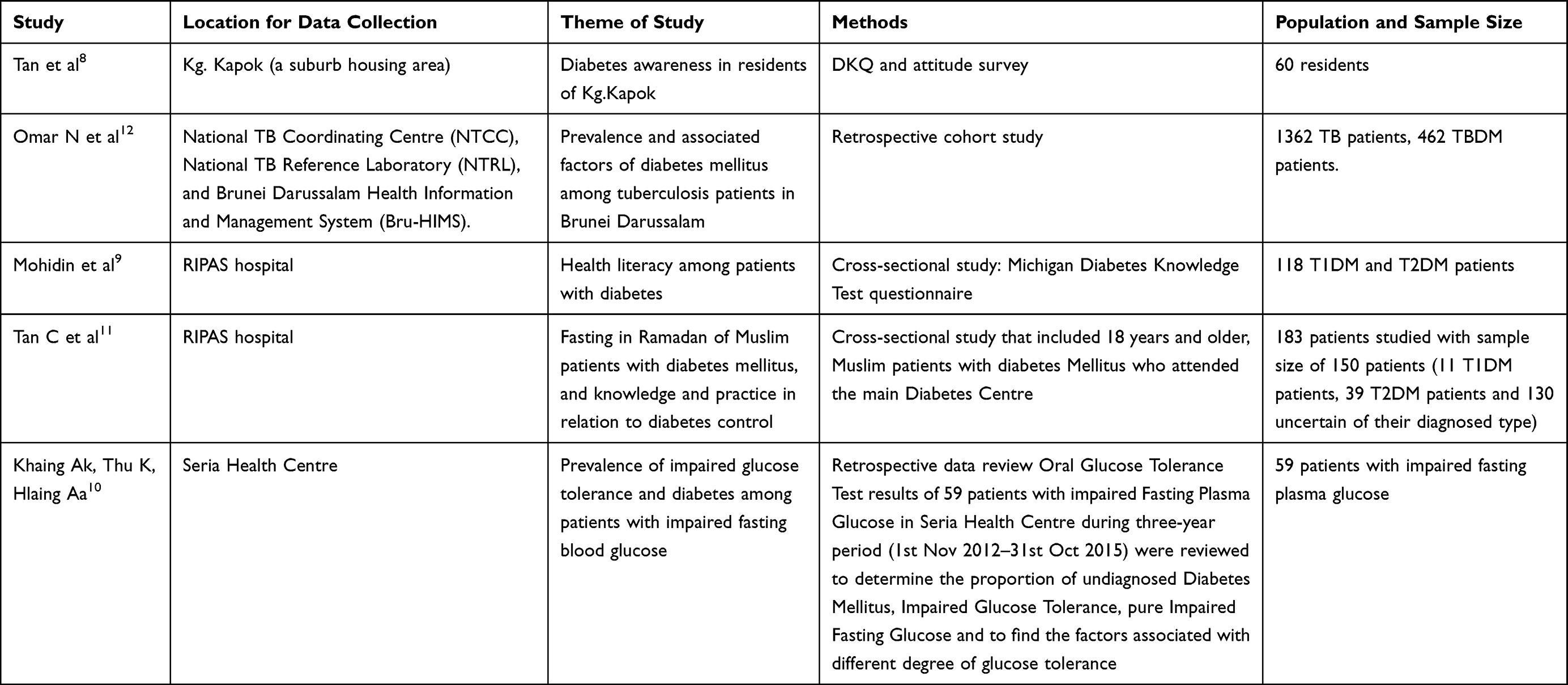 |
Table 1 Summary of Diabetes Studies Done in Brunei Darussalam |
The study done in Kg. Kapok area had evaluated the residents’ knowledge on diabetes, which was generally poor, and introduced an intervention to improve their awareness on diabetes. Education and monthly income levels were considerably linked to knowledge about diabetes.8,9 Researchers assessed knowledge, attitudes, and practices related to DM in a small sample. The issues surrounding DM were highlighted in small group discussions, and a talk was given. Participants’ knowledge was assessed for any changes after the event through questionnaires.8 In a more recently conducted study, patients attending a diabetes outpatient clinic of the main tertiary hospital of the capital city were also tested for knowledge of their condition, and the level of glycaemic control using Michigan Diabetes Knowledge Test and correlated with HbA1c.9 However, this test has not been validated for assessing the diabetes knowledge in Brunei Darussalam.9
The findings of Khaing et al study draw our attention to an important issue related to clinical practices in Brunei Darussalam. They reported that almost half of sample population should be classified as diabetic were not properly diagnosed. Khaing et al reported that repeating fasting blood glucose test alone at patients' follow-up clinic visits is a gold standard test. Fasting blood glucose testing alone has its own inherent weakness because this method does not fully quantify the recommended diagnosis of T2DM and caused delay of treatment. However, the results should be interpreted with caution as the study was only done in one health-care centre with a small sample size.10
Another study examined the fasting of pattern of DM patients with Islamic faith in Brunei Darussalam, along with other information such as fasting activities and knowledge and practice in DM control. The study reported that 93.4% of the participants had observed fasting for about 24.1 days during the Islamic fasting month of Ramadan. Interestingly, those with age 55 years and above had observed significantly higher number of fasting days than the younger group (p=0.010), yet less than half of them had consulted the physician before fasting and performed home monitoring of blood glucose levels during the fasting month.11 However, it must be noted that validation of the research instrument was not performed and there was also the possibility of potential recall bias.11
Meanwhile, the prevalence and related factors of DM in patients with tuberculosis (TB) in Brunei Darussalam were established in 2021. This retrospective study reviewed medication data of TB patients with DM up to 6 years and determined their prevalence and associated factors. However, the limitations of this study were that the researcher did not check the exact duration of having DM for each TB case, status of DM management, missing data and inconvenience in gathering information on the etiology of deaths among TB patients.12
In Brunei Darussalam, patient medication counselling is a major contributor to medication knowledge.13 The counselling is given by either a pharmacist or a dispenser who has been trained to conduct such medication counseling. There is no other known method of providing medication knowledge to patients. The set of facts a patient must have in order to utilise their drug correctly, including the therapeutic objective, dosage, time to take it, safety, and ways for preserving it, as well as any potential interactions and side effects, can be referred to as their knowledge of their medications.14 Unexpected clinical outcomes, the onset of secondary health problems, misuse of medications, and adverse effects related to medications are all possible repercussions of inadequate medication knowledge.15,16 Due to the high incidence, it is regarded as a significant public health issue.
Medication knowledge has been shown to be favourably connected with improved quality of life, treatment adherence, and accomplishment of desired pharmacological outcomes. As a result, medication knowledge is critical in illness management and reducing the occurrence of adverse drug responses.17,18 Proper medication knowledge is one of the criteria for a patient’s participation in decreasing medication mistakes.19 Despite this, there is little research that examines drug awareness, particularly in T2DM patients and in hospital settings. Polypharmacy is used on a significant number of outpatients, which can increase the risk of other health complications such as drug interactions and toxicity.20 Extant literature have generally demonstrated poor medication knowledge, especially with reference to potential side effects and how their medications work. Factors affecting medication knowledge include age, educational level, and number of medications taken daily.21–24 As for age, those of younger age are associated with having better medication knowledge.25,26 This is supported with studies published by Al-Qazaz et al,27 McPherson et al28 and Sweileh et al. These studies included patients with mean age older than 50 years, which may play a role in contributing to the general consensus of poor patient medication knowledge. Education level has also been thought to have a positive correlation with patient medication knowledge.29 In comparison with study conducted outside Brunei Darussalam, Al-Qazaz et al27 and Karaoui et al29 have demonstrated the significance of educational level in patient medication knowledge and diabetes knowledge (P < 0.05 and P < 0.01).27,30 However, studies by McPherson et al28 and Gangwar et al31 have shown no significant link between literacy and patient medication knowledge. Polypharmacy has been associated with poor patient medication knowledge. However, a study by McPherson et al28 discovered that 9 out of 10 (90%) patients on 2 medications scored 5 and above on medication knowledge, but this was achieved in only 18 out of 34 (52.9%) patients on one medication.26,32 The difference in the number of people on one or two medications is huge; therefore, the comparison should be evaluated with caution. McPherson et al had also revealed that patient medication knowledge had a significant inverse correlation with the patient’s glycemic control (r = −0.61, P < 0.01).28 Better knowledge on disease is associated with higher medication adherence as supported by Al-Qazaz et al in which the study had shown that higher diabetes knowledge was significantly linked to better adherence.27,33,34 However, Karaoui et al had found that better diabetes knowledge was not significantly associated with better adherence (r = 0.456, P < 0.01).30
These studies have conveyed the significance of patient medication knowledge and its inverse association to glycemic control.28 Conducting a study to assess the patient medication knowledge and medication adherence can contribute to a better understanding of the factors, which may affect a patient’s medication adherence and their health outcomes. Furthermore, the prevalence of comorbidities is high in patients with T2DM, thus taking multiple medications is common in these patients.35 Patient medication knowledge can play a significant role in ensuring appropriate and safe use of medications prescribed to patients.36
Conclusion
This review concludes that a relatively poor medication knowledge and inappropriate diabetes-related practices were observed among the findings of the studies conducted in Brunei Darussalam. Based on the theory that medication knowledge significantly correlates to medication adherence, it can be inferred that poor medication adherence also exists in T2DM patients in Brunei Darussalam. Studies that evaluated medication knowledge focussed on glycemic control and other factors, which may also influence medication knowledge and thus medication adherence. However, no study has reported both medication knowledge and medication adherence measurement among T2DM patients in Brunei Darussalam. Future studies can focus on the relationship between these two factors in different geographical locations of the world exhibiting different diabetes-related practices and culture.
Abbreviations
DM, Diabetes Mellitus; T2DM, Type II Diabetes Mellitus; T1DM, Type I Diabetes Mellitus; PKM, Patient’s knowledge of their medications; NRM, Negative results related to medication; NCD, Non-communicable diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ong SK, Lai DTC, Wong JYY, et al. Cross-sectional STEPwise approach to surveillance (STEPS) population survey of noncommunicable diseases (NCDs) and risk factors in Brunei Darussalam 2016. Asia Pac J Public Health. 2017;29(8):635–648. doi:10.1177/1010539517738072
2. Jia W. Diabetes: a challenge for China in the 21st century. Lancet Diabetes Endocrinol. 2014;2(4):e6–e7. doi:10.1016/S2213-8587(14)70027-0
3. Zimmet PZ, Magliano DJ, Herman WH, Shaw JE. Diabetes: a 21st century challenge. Lancet Diabetes Endocrinol. 2014;2(1):56–64. doi:10.1016/S2213-8587(13)70112-8
4. Muhammad Haskani NH, Goh HP, Wee DVT, Hermansyah A, Goh KW, Ming LC. Medication Knowledge and Adherence in Type 2 Diabetes Mellitus Patients in Brunei Darussalam: A Pioneer Study in Brunei Darussalam. Int J Environ Res Public Health 18. 2022;19(12):7470. doi:10.3390/ijerph19127470
5. Zhu X, Hu J, Guo H, et al. Effect of metabolic health and obesity phenotype on risk of diabetes mellitus: a population-based longitudinal study. Diabetes Metab Syndr Obes. 2021;14:3485–3498. doi:10.2147/DMSO.S317739
6. Al-Goblan AS, Al-Alfi MA, Khan MZ. Mechanism linking diabetes mellitus and obesity. Diabetes Metab Syndr Obes. 2014;7:587–591. doi:10.2147/DMSO.S67400
7. Ministry of Health Brunei Darussalam. Latest news - World Health Day: beat Diabetes; 2022. Available from: http://www.moh.gov.bn/Lists/Latest%20news/NewDispForm.aspx?ID=37&ContentTypeId=0x0104009A3003A09F8D6E42981D262E322516A22016.
8. Shi Ying T, Shazli AAH, Abd Wahab A, Rahman AA, Idris F. Diabetes awareness in Kampong Kapok, Brunei Maura district, Brunei Darussalam. Brunei Int Med J. 2015;11(5):247–250.
9. Mohidin AMAA, Chong PL, Shyh Poh T, et al. Health literacy among patients with diabetes in ripas hospital, Brunei. Brunei Int Med J. 2020;16:36–41.
10. Khaing A, K THU, Hlaing A. Prevalence of impaired glucose tolerance and diabetes among patients with impaired fasting blood sugar in Seria Health Centre. Brunei Int Med J. 2017;13(3):5.
11. Tan C, Yong AML, Haji Mohamad MA, Abdul Rahman H, Naing L. Fasting in Ramadan of Muslim patients with diabetes Mellitus, and knowledge and practice in relation to diabetes control in Brunei. Diabetes Res Clin Pract. 2018;144:171–176. doi:10.1016/j.diabres.2018.09.004
12. Omar N, Wong J, Thu K, Alikhan MF, Chaw L. Prevalence and associated factors of diabetes mellitus among tuberculosis patients in Brunei Darussalam: a 6-year retrospective cohort study. Int J Infect Dis. 2021;105:267–273. doi:10.1016/j.ijid.2021.02.064
13. Nasir HHA, Dhaliwal JS, Goh HP, et al. Patient’s own medication use during hospitalization. Prog Microb Mol Biol. 2022;5(1):1.
14. Eva JJ, Kassab YW, Neoh CF, et al. Self-care and self-management among adolescent T2DM patients: a review. Front Endocrinol (Lausanne). 2018;9:489. doi:10.3389/fendo.2018.00489
15. Abdullah IS, Chaw LL, Koh D, et al. Over-the-counter medicine attitudes and knowledge among university and college students in Brunei Darussalam: findings from the first national survey. Int J Environ Res Public Health. 2022;19(5):2658. doi:10.3390/ijerph19052658
16. Tan CS, Hassali MAA, Neoh CF, Ming LC. Beliefs about medicine and medication adherence among hypertensive patients in the community setting. Drugs Ther Perspect. 2020;36(8):358–367. doi:10.1007/s40267-020-00744-8
17. Long CS, Kumaran H, Goh KW, et al. Online pharmacies selling prescription drugs: systematic review. Pharmacy. 2022;10(2):42. doi:10.3390/pharmacy10020042
18. Elkalmi RM, Al-Worafi YM, Alseragi WM, Ming LC, Siddique A. Drug safety in Malaysia. In: Drug Safety in Developing Countries. Elsevier; 2020:245–253.
19. Rodziewicz TL, Houseman B, Hipskind JE. Medical Error Reduction and Prevention. StatPearls; 2022.
20. Ramia E, Zeenny RM, Hallit S, Salameh P. Assessment of patients’ knowledge and practices regarding their medication use and risks in Lebanon. Int J Clin Pharm. 2017;39(5):1084–1094. doi:10.1007/s11096-017-0517-4
21. Mwangasha FM, Nyamu DG, Tirop LJ. Factors impacting on diabetes knowledge, medication adherence and glycemic control among adult diabetics visiting a county teaching and referral hospital in Kenya: a cross-sectional study. Pan Afr Med J. 2021;40:5. doi:10.11604/pamj.2021.40.5.21848
22. Rahmawati R, Bajorek B. Factors affecting self-reported medication adherence and hypertension knowledge: a cross-sectional study in rural villages, Yogyakarta Province, Indonesia. Chronic Illn. 2018;14(3):212–227. doi:10.1177/1742395317739092
23. Kelly M, McCarthy S, Sahm LJ. Knowledge, attitudes and beliefs of patients and carers regarding medication adherence: a review of qualitative literature. Eur J Clin Pharmacol. 2014;70(12):1423–1431. doi:10.1007/s00228-014-1761-3
24. Salmasian H, Tran TH, Chase HS, Friedman C. Medication-indication knowledge bases: a systematic review and critical appraisal. J Am Med Inform Assoc. 2015;22(6):1261–1270. doi:10.1093/jamia/ocv129
25. Moosa A, Bezuidenhout S, Meyer JC, Godman B. Knowledge regarding medicines management of type 2 diabetes amongst patients attending a Community Health Centre in South Africa. J Pharm Health Serv Res. 2019;10(1):13–28. doi:10.1111/jphs.12283
26. Bosch-Lenders D, Maessen DW, Stoffers HE, Knottnerus JA, Winkens B, van den Akker M. Factors associated with appropriate knowledge of the indications for prescribed drugs among community-dwelling older patients with polypharmacy. Age Ageing. 2016;45(3):402–408. doi:10.1093/ageing/afw045
27. Al-Qazaz H, Sulaiman SA, Hassali MA, et al. Diabetes knowledge, medication adherence and glycemic control among patients with type 2 diabetes. Int J Clin Pharm. 2011;33(6):1028–1035. doi:10.1007/s11096-011-9582-2
28. McPherson ML, Smith SW, Powers A, Zuckerman IH. Association between diabetes patients’ knowledge about medications and their blood glucose control. Res Social Adm Pharm. 2008;4(1):37–45. doi:10.1016/j.sapharm.2007.01.002
29. Lemmens-Gruber R, Hahnenkamp C, Gössmann U, et al. Evaluation of educational needs in patients with diabetes mellitus in respect of medication use in Austria. Int J Clin Pharm. 2012;34(3):490–500. doi:10.1007/s11096-012-9636-0
30. Karaoui LR, Deeb ME, Nasser L, Hallit S. Knowledge and practice of patients with diabetes mellitus in Lebanon: a cross-sectional study. BMC Public Health. 2018;18(1):1–9. doi:10.1186/s12889-018-5416-7
31. Ahmad A. Assessment of medication knowledge and counseling in type 2 diabetes mellitus patients attending community pharmacy in rural North India. Afr J Pharm Pharmacol Pharm. 2013;4:1–11.
32. Beuscart JB, Petit S, Gautier S, et al. Polypharmacy in older patients: identifying the need for support by a community pharmacist. BMC Geriatr. 2019;19(1):277. doi:10.1186/s12877-019-1276-y
33. Garcia-Perez LE, Alvarez M, Dilla T, Gil-Guillen V, Orozco-Beltran D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175–194. doi:10.1007/s13300-013-0034-y
34. Mekonnen GB, Gelayee DA. Low medication knowledge and adherence to oral chronic medications among patients attending community pharmacies: a cross-sectional study in a low-income country. Biomed Res Int. 2020;2020:4392058. doi:10.1155/2020/4392058
35. Iglay K, Hannachi H, Joseph Howie P, et al. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(7):1243–1252. doi:10.1185/03007995.2016.1168291
36. Gudeta T, Mechal D. Patient knowledge of correct dosage regimen; the need for good dispensing practice. J Prim Care Community Health. 2019;10:2150132719876522. doi:10.1177/2150132719876522
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.