Back to Journals » Clinical Ophthalmology » Volume 20
Ophthalmologists’ Perceptions of the Impact of Patient Mental Status on Clinical Decision-Making: A Cross-Sectional Survey
Authors Kashiwagi K ![]() , Kasai H, Fukuda Y, Hosoda S, Tanabe N
, Kasai H, Fukuda Y, Hosoda S, Tanabe N
Received 28 April 2026
Accepted for publication 1 July 2026
Published 13 July 2026 Volume 2026:20 620562
DOI https://doi.org/10.2147/OPTH.S620562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Kenji Kashiwagi, Hiroshi Kasai, Yoshiko Fukuda, Shuhei Hosoda, Naohiko Tanabe
Department of Ophthalmology, Interdisciplinary Graduate School of Medicine, University of Yamanashi, Yamanashi, Japan
Correspondence: Kenji Kashiwagi, Department of Ophthalmology, Interdisciplinary Graduate School of Medicine, University of Yamanashi, 1110 Shimokato, Chuo City, Yamanashi, 409-3898, Japan, Email [email protected]
Purpose: To investigate ophthalmologists’ perceptions of how patients’ mental status influences ophthalmic clinical practice and to identify ocular diseases perceived by ophthalmologists as having the greatest psychological impact.
Subjects and Methods: This exploratory cross-sectional questionnaire survey included 61 ophthalmologists from a regional ophthalmologists’ association in Japan (41 men and 20 women; mean clinical experience, 26 ± 14 years). Participants rated the extent to which they considered patients’ mental status during treatment selection using a 10-point scale (1 = not considered at all; 10 = maximal consideration). The survey assessed perceived treatment-related changes in patient mental status, clinical domains perceived to be influenced by mental status, experiences of perceived clinical impact due to insufficient psychological consideration, and ocular diseases perceived to impose the greatest psychological burden. Multivariable logistic regression was used to identify factors associated with reporting perceived clinical impact.
Results: The mean mental health attention score was 7.0 ± 1.8 (range, 2– 10). Fifty-five physicians (90.2%) reported experiencing treatment-related changes in patients’ mental status. The clinical domains most frequently selected as being influenced by patient mental status were disease explanation, healthcare-seeking behavior, surgical decision-making, and medication management. Thirty-two physicians (52.5%) reported that insufficient attention to patient mental health had affected clinical care. Higher mental health attention scores were independently associated with reporting perceived clinical impact (odds ratio, 1.45 per 1-point increase; 95% confidence interval, 1.05– 2.01; p = 0.02). Glaucoma was most frequently ranked as the ocular diseases perceived by ophthalmologists as being associated with the greatest psychological burden, followed by retinitis pigmentosa.
Conclusion: Ophthalmologists in this sample perceived patient mental status as relevant to clinical practice, particularly in chronic progressive diseases such as glaucoma and inherited retinal disorders. Because this survey assessed physician perceptions rather than patient-reported mental health or objective clinical outcomes, future studies incorporating validated mental health instruments, patient-reported outcomes, and objective clinical endpoints are needed.
Keywords: mental health, ophthalmology, glaucoma, clinical decision-making, physician perceptions, survey
Introduction
Visual function is important not only for daily activities but also for psychological well-being, autonomy, and social participation. Visual impairment has been associated with depression, anxiety, and reduced quality of life across populations.1–3 Among ophthalmic diseases, chronic progressive and irreversible conditions such as glaucoma and inherited retinal diseases may be particularly associated with psychological distress because of uncertainty regarding prognosis, fear of vision loss, and the need for long-term disease management.4,5
From a behavioral medicine perspective, chronic diseases characterized by unpredictability and limited controllability can generate sustained psychological stress. The stress-coping framework proposed by Lazarus and Folkman emphasizes that perceived threat and lack of control are central determinants of emotional burden.6 Glaucoma, a lifelong and often asymptomatic yet progressive disease, fits this framework and has been linked to anxiety, depressive symptoms, and treatment adherence challenges.7,8 Similarly, retinitis pigmentosa and other inherited retinal degenerations may be associated with uncertainty about future vision, genetic implications, and changes in identity and social participation.9
The Common-Sense Model of illness representation suggests that patients’ beliefs regarding chronicity, severity, controllability, and consequences shape emotional responses and health behaviors.10 Diseases perceived as irreversible and vision-threatening may therefore exert a different psychological impact from treatable conditions such as cataract, in which surgery often offers a high probability of visual improvement.
Psychological influences in ophthalmic care may also be relevant from the clinician’s perspective. Patient distress may alter communication, the perceived difficulty of clinical explanations, follow-up behavior, adherence counseling, and shared decision-making. Conversely, physicians’ awareness of psychological factors may influence whether these issues are recognized and reported in routine care. However, it is important to distinguish among three related concepts: patient psychological burden, physicians’ perceptions of patient mental status, and actual clinical decision-making behaviors. The present study addresses physicians’ perceptions rather than directly measuring patient mental health or objective clinical decisions.
Although a growing body of literature describes psychological burden among patients with ophthalmic disease, less is known about how ophthalmologists perceive the relevance of patient mental status in routine clinical practice. Prior studies have focused mainly on patient-reported psychological outcomes or vision-related quality of life, whereas surveys addressing ophthalmologists’ perceptions of psychosocial factors in everyday ophthalmic care remain limited. Clarifying these perceptions is important because they may shape communication approaches, perceived treatment difficulties, and awareness of patient-centered needs.
Therefore, this exploratory study aimed to investigate ophthalmologists’ perceptions of the influence of patients’ mental status on clinical practice and to identify ocular diseases perceived as having the greatest psychological impact. We also examined factors associated with reporting perceived clinical impact due to insufficient psychological consideration.
Subjects and Methods
Ethics Approval
This study was performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants. The Ethics Committee of the University of Yamanashi School of Medicine approved this study (Approval Code: 2864).
Study Design and Participants
This exploratory cross-sectional survey targeted ophthalmologists who were members of the Yamanashi Ophthalmologists Association, a regional professional organization of ophthalmologists in Yamanashi Prefecture, Japan. The questionnaire was distributed to all 86 members of the association. The survey was designed to assess ophthalmologists’ perceptions of the clinical relevance of patient mental status in ophthalmic care and its perceived influence on clinical decision-making.
A total of 61 ophthalmologists (41 men and 20 women) completed the survey. The mean duration of clinical experience was 26 ± 14 years.
Survey Questionnaire
The questionnaire used in this study is shown in Table 1. It was developed for this exploratory survey and was not adapted from a previously validated instrument. Because the main outcomes relied on subjective physician perceptions, the results should be interpreted as exploratory perception-based findings rather than validated measures of patient mental health or objective clinical decision-making.
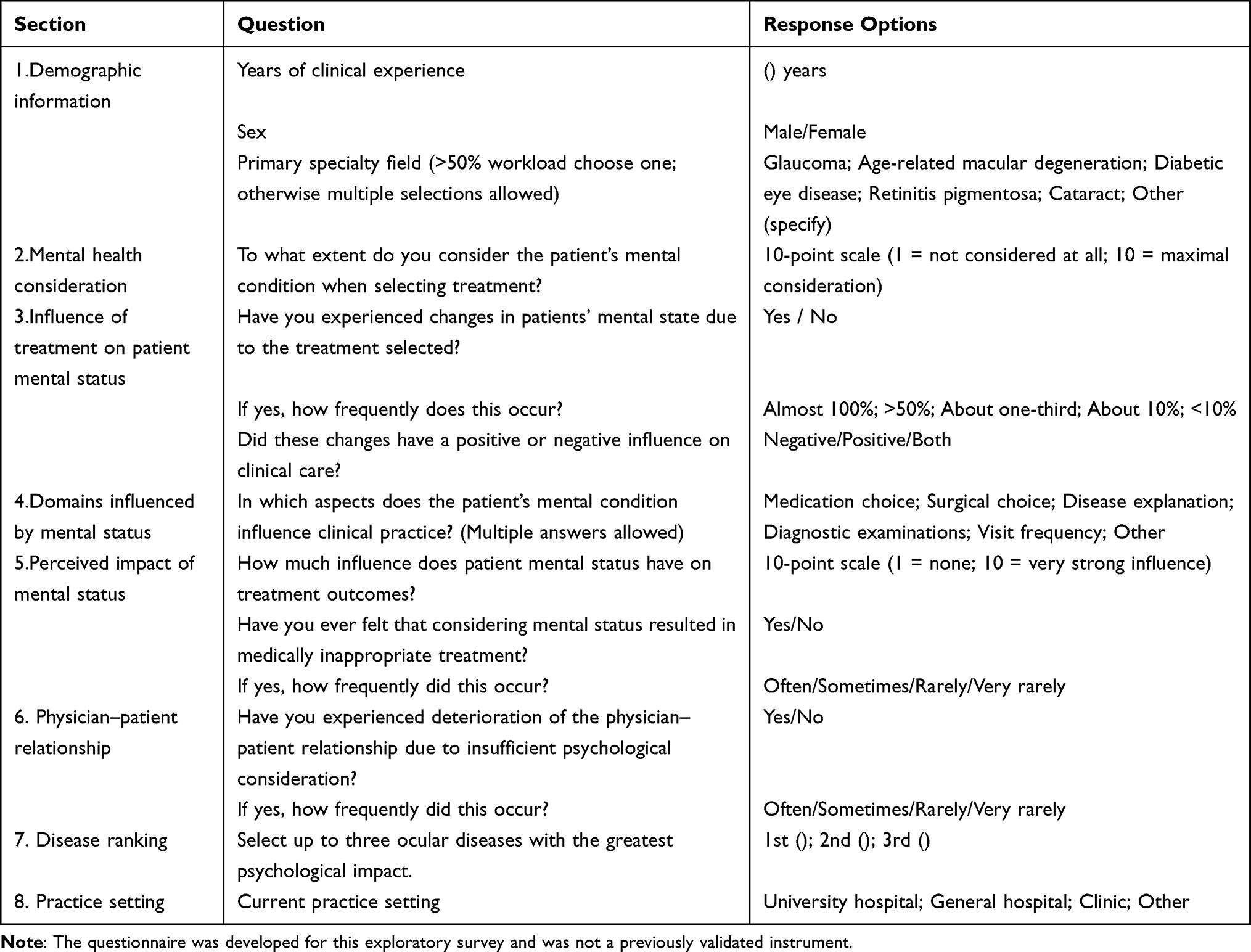 |
Table 1 Survey Questionnaire Used in This Study |
The questionnaire consisted of eight sections assessing demographic characteristics, clinical background, and perceptions regarding the influence of patients’ mental status on ophthalmic practice. Demographic information included years of clinical experience, sex, and primary specialty field. Participants rated the extent to which they considered patients’ mental condition during treatment selection using a 10-point scale (1 = not considered at all; 10 = maximal consideration).
The survey also asked whether physicians had experienced treatment-related changes in patients’ mental status, the perceived frequency of such changes, and whether these changes had positive or negative effects on clinical care. In addition, respondents identified clinical domains in which patients’ mental status was perceived to influence practice, including medication choice, surgical decision-making, disease explanation, diagnostic examinations, follow-up frequency, and other domains. Multiple answers were allowed.
Participants evaluated the perceived overall influence of patient mental status on treatment outcomes using a 10-point scale and reported whether consideration of mental status had ever resulted in medically inappropriate treatment decisions. The questionnaire further assessed whether insufficient psychological consideration had affected the physician-patient relationship and, if so, how frequently this occurred. Finally, respondents ranked up to three ocular diseases perceived to have the greatest psychological impact on patients and reported their current practice setting.
Statistical Analysis
All statistical analyses were performed using R software (version 4.5.2). Continuous variables are presented as the mean ± standard deviation, and categorical variables are presented as counts and percentages. Percentages were calculated using the number of valid responses for each item as the denominator. For questions allowing multiple selections, percentages are described as proportions of total selected responses unless otherwise specified.
Because this was an exploratory perception survey with a modest sample size, all inferential analyses were considered exploratory and hypothesis-generating. A two-sided p value < 0.05 was used as a reference threshold for statistical interpretation.
To identify factors associated with reporting perceived clinical impact due to insufficient psychological consideration, multivariable logistic regression analysis was performed. The outcome variable was defined as reporting perceived clinical impact due to insufficient psychological consideration (yes = 1, no = 0). Predictor variables included years of clinical experience, sex, mental health attention score, and practice setting (university hospital, general hospital, or private clinic). Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
Disease ranking was summarized descriptively using first-rank responses. The Bradley–Terry analysis was conducted as an exploratory method to summarize the relative perceived importance of each ophthalmic disease based on ophthalmologists’ ranking responses. Because of the limited sample size and the presence of partial ranking data, the Bradley–Terry results were interpreted descriptively rather than as confirmatory statistical evidence.
Results
Participant Characteristics
Of the 86 ophthalmologists who were members of the Yamanashi Ophthalmologists Association and received the questionnaire, 61 responded, yielding a response rate of 71.0%. Among the respondents, 41 were male (67.2%) and 20 were female (32.8%). The mean duration of clinical experience was 26.0 ± 14.0 years (range, 1–54 years). Regarding practice setting, 30 respondents worked in private clinics (49.2%), 17 in university hospitals (27.9%), and 14 in general hospitals (23.0%). With respect to primary specialty fields, cataract was the most frequently reported specialty (30/61, 49.2%), followed by glaucoma (27/61, 44.3%), macular diseases (9/61, 14.8%), and diabetic retinopathy (9/61, 14.8%).
Perceived Attention to Patient Mental Health
The mean score for attention to patient mental health during clinical practice was 7.0 ± 1.8 (range, 2–10). A total of 55 physicians (90.2%) reported experiencing treatment-related changes in patients’ mental status. Among those reporting such changes, 67.3% reported both positive and negative influences, 19.2% reported only positive effects, and 13.5% reported only negative effects.
Clinical Domains Perceived to Be Influenced by Patient Mental Status
The clinical domains most frequently selected as being influenced by patient mental status were disease explanation and healthcare-seeking behavior, followed by surgical decision-making, medication management, diagnostic examinations, and sleep-related issues (Figure 1). Because multiple responses were allowed, these percentages represent the proportion of total selected responses rather than the proportion of respondents.
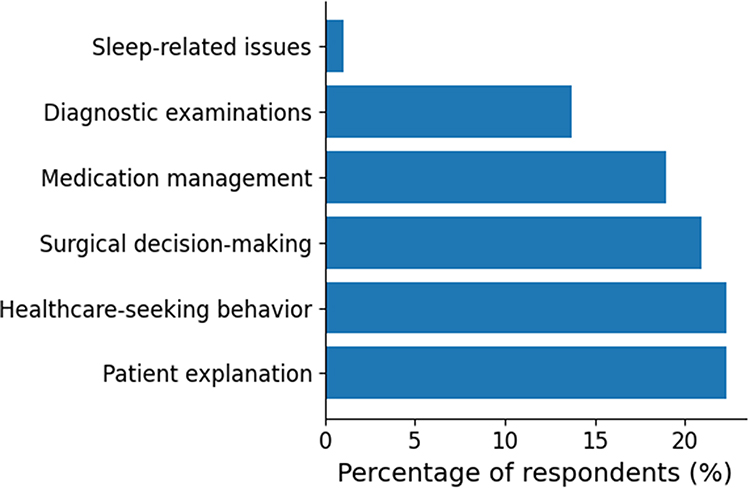 |
Figure 1 Clinical domains perceived to be influenced by patient mental status. Values represent the proportion of total selected responses because multiple answers were allowed. |
Perceived Clinical Impact of Insufficient Attention to Mental Health
Overall, 32 of 61 physicians (52.5%) reported that insufficient attention to patient mental health had affected clinical care, whereas 29 physicians (47.5%) reported no such experience. Approximately half of respondents reported experiencing deterioration in the physician-patient relationship because of inadequate psychological consideration.
Multivariable Logistic Regression Analysis
Multivariable logistic regression analysis was performed to identify factors associated with reporting perceived clinical impact due to insufficient psychological consideration (Table 2). A higher mental health attention score was independently associated with reporting perceived clinical impact (OR, 1.45 per 1-point increase; 95% CI, 1.05–2.01; p = 0.02). In contrast, years of clinical experience and sex were not significantly associated with reporting perceived clinical impact. Practice setting showed a nonsignificant tendency toward higher reporting among physicians working in university hospitals compared with those working in private clinics (Figure 2).
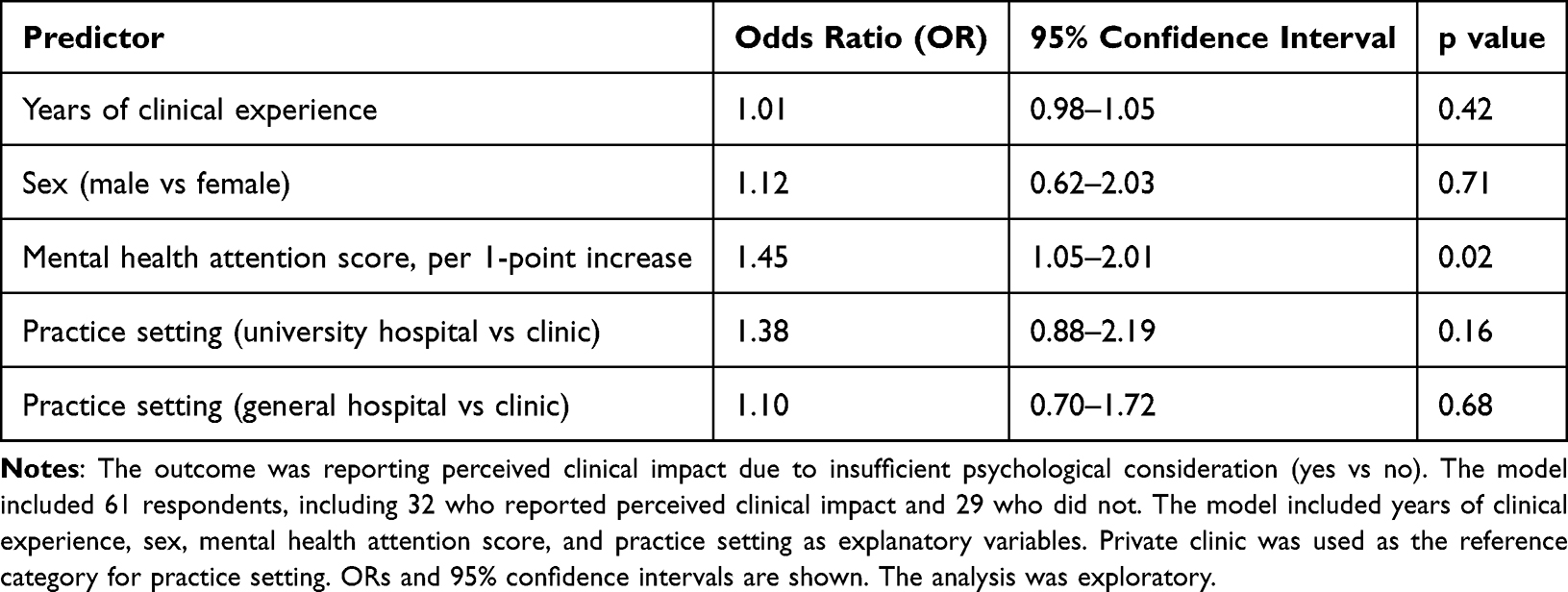 |
Table 2 Multivariable Logistic Regression Analysis Identifying Factors Associated with Reporting Perceived Clinical Impact Due to Insufficient Psychological Consideration |
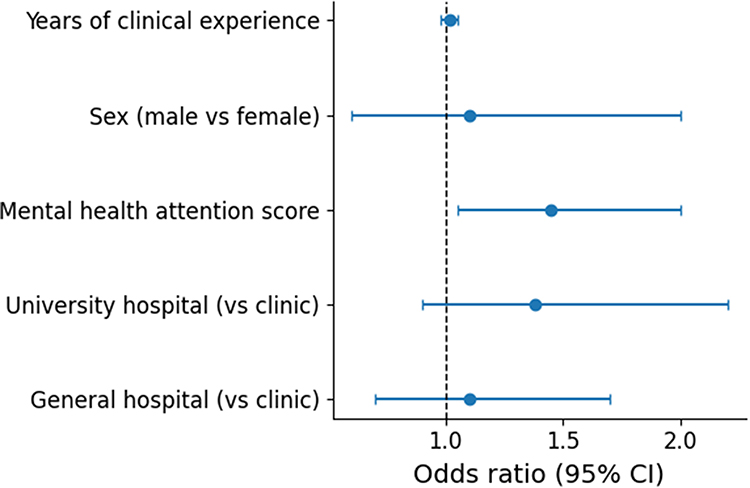 |
Figure 2 Multivariable logistic regression analysis showing factors associated with reporting perceived clinical impact due to insufficient psychological consideration. Odds ratios and 95% confidence intervals are presented. The outcome was reporting perceived clinical impact due to insufficient psychological consideration. |
Disease Ranking Analysis
Participants ranked up to three ocular diseases according to the perceived psychological burden associated with each disease. Among available first-rank responses, glaucoma was most frequently ranked as the disease associated with the greatest perceived psychological burden (34/58), followed by retinitis pigmentosa (7/58), cataract (4/58), diabetic retinopathy (2/58), dry eye disease (2/58), and macular disease (1/58) (Figure 3). The distribution of diseases across first-, second-, and third-rank responses is shown in Table 3.
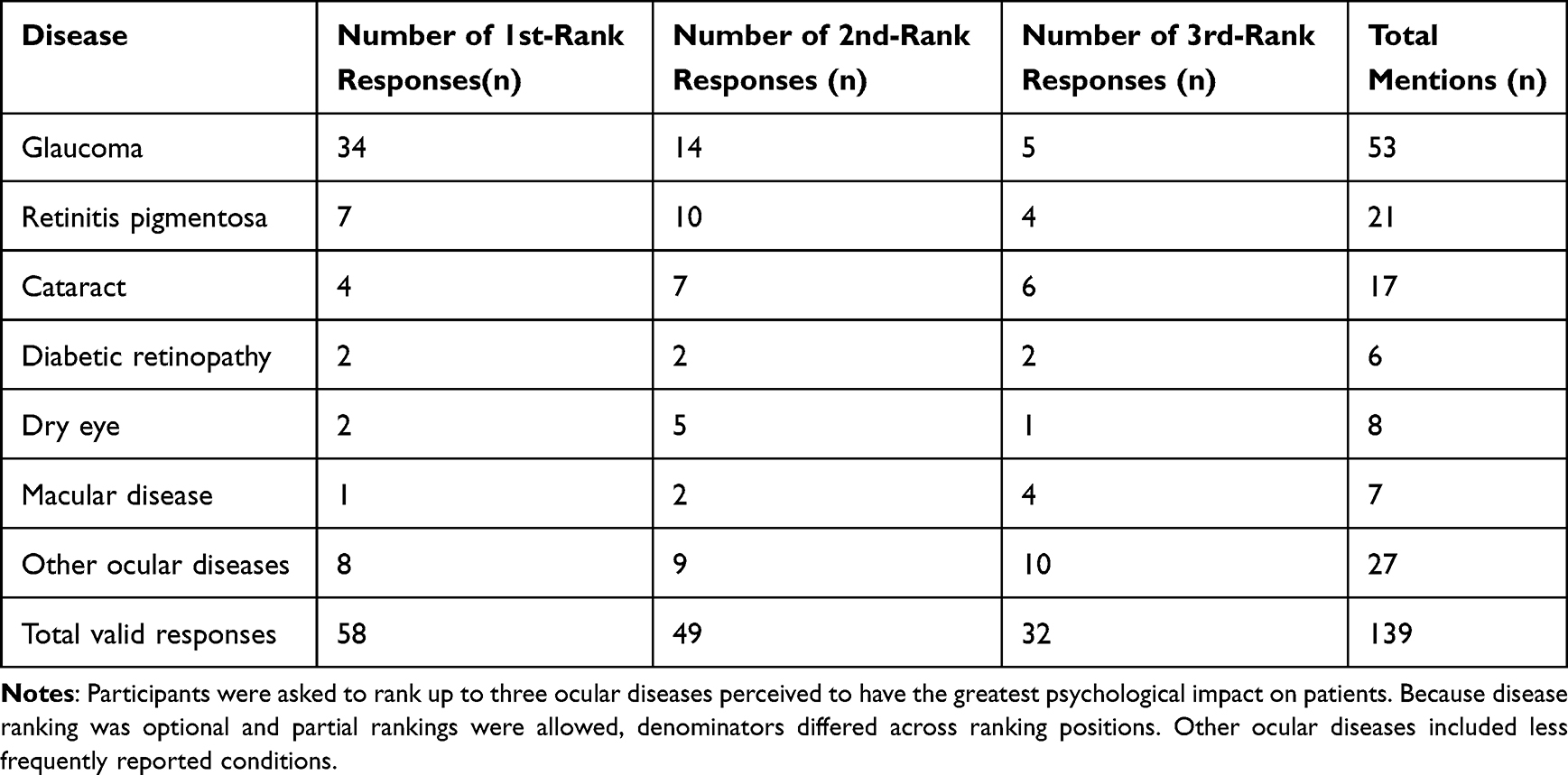 |
Table 3 Distribution of Ocular Diseases Ranked as Having the Greatest Perceived Psychological Impact |
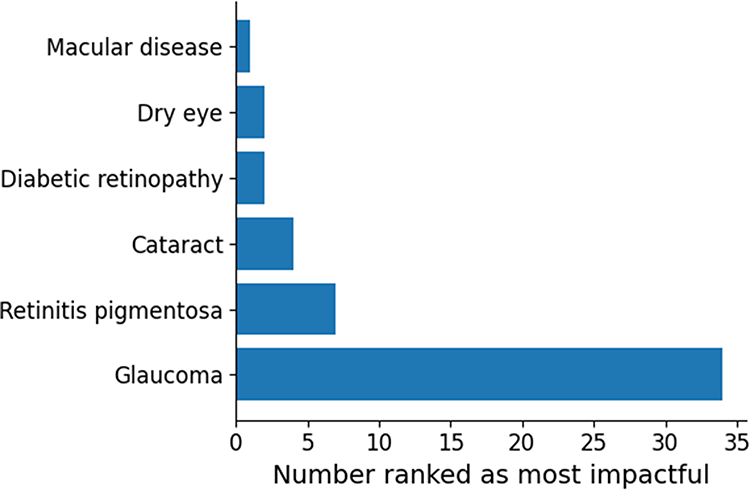 |
Figure 3 Ocular diseases ranked as having the greatest perceived psychological impact. Bars represent the number of respondents who ranked each disease first. Glaucoma was most frequently selected. |
When all available ranking positions were considered, glaucoma remained the most frequently mentioned disease (53 total mentions), followed by other ocular diseases (27 mentions), retinitis pigmentosa (21 mentions), cataract (17 mentions), dry eye disease (8 mentions), macular disease (7 mentions), and diabetic retinopathy (6 mentions). In the exploratory Bradley–Terry model, glaucoma showed the highest relative ranking strength, followed by retinitis pigmentosa (Figure 4). These findings indicate that, within this sample, glaucoma was ranked highest by ophthalmologists in terms of perceived disease-related psychological burden. However, this result should be interpreted cautiously because the respondent sample included a relatively high proportion of glaucoma specialists and because the ranking analysis assessed physician perceptions rather than patient-reported psychological burden. Because the Bradley–Terry analysis was exploratory and included partial ranking data, these results are interpreted descriptively as relative indicators of physicians’ perceived disease importance.
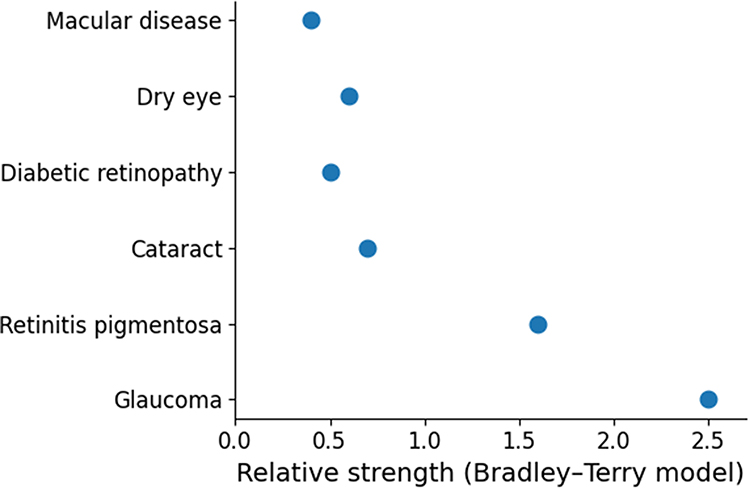 |
Figure 4 Exploratory Bradley-Terry relative ranking strength parameters for the perceived psychological impact of ocular diseases. Higher values indicate stronger perceived psychological impact. The analysis should be interpreted descriptively because of the modest sample size and optional partial ranking format. |
Discussion
Principal Findings
In this exploratory survey of Japanese ophthalmologists, patient mental status was perceived to be relevant to ophthalmic clinical practice. More than half of respondents reported that insufficient attention to patients’ psychological states had affected clinical care, and approximately half reported deterioration in the physician-patient relationship related to inadequate psychological consideration.
Higher physician attention to patient mental health was independently associated with reporting perceived clinical impact. This association should not be interpreted as evidence that attention to mental health causes greater clinical impact. Rather, it may reflect perception bias: physicians who are more attentive to psychological factors may be more likely to notice and report their influence in clinical practice.
Disease ranking analyses identified glaucoma as the condition most frequently perceived to impose the greatest psychological burden, followed by retinitis pigmentosa. This result is clinically plausible because glaucoma and inherited retinal diseases are chronic, progressive, and potentially irreversible. Nevertheless, the observed ranking may also reflect the specialty distribution of respondents, because glaucoma was one of the most common specialty fields in this sample.
Psychological Mechanisms Underlying Perceived Disease Burden
The predominance of glaucoma as the disease most strongly associated with perceived psychological burden may be interpreted within established behavioral medicine frameworks. According to the stress-coping model proposed by Lazarus and Folkman,6 chronic progressive diseases characterized by uncertainty and limited controllability can generate sustained psychological stress. Glaucoma, a lifelong and often asymptomatic disease with potential irreversible visual loss, fits this profile and may contribute to anticipatory anxiety regarding future vision.
From the perspective of the Common-Sense Model of illness representation,10 diseases perceived as chronic, severe, and difficult to control are more likely to generate psychological distress. Glaucoma and retinitis pigmentosa share these characteristics, which may partly explain why they were frequently selected by ophthalmologists as psychologically burdensome diseases.
However, the present study did not directly assess patient anxiety, depression, quality of life, adherence, or objective clinical outcomes. Therefore, these mechanisms should be regarded as plausible explanatory frameworks rather than findings directly demonstrated by the present survey.
Disease-Specific Considerations
Glaucoma is associated with fear of blindness, lifelong treatment, uncertainty regarding disease progression, and adherence challenges. Previous studies have reported anxiety, depressive symptoms, and reduced quality of life among patients with glaucoma.11,12 The present findings suggest that ophthalmologists also perceive glaucoma as a disease with substantial psychosocial relevance.
Inherited retinal diseases such as retinitis pigmentosa may affect younger individuals and can have genetic implications. Qualitative and clinical studies have described uncertainty regarding future vision, identity disruption, and unmet needs among patients with inherited retinal disease.13 These features may explain why retinitis pigmentosa ranked highly in perceived psychological impact.
Cataract was less frequently ranked as having the greatest psychological impact, possibly because it is generally treatable and patients may perceive a higher degree of controllability. Diabetic retinopathy, although vision-threatening, may be cognitively integrated within the broader context of systemic diabetes management and may therefore be perceived differently by ophthalmologists.
Physician Awareness and Clinical Consequences
Physicians who reported greater attention to patients’ mental health were more likely to report that psychological factors affected clinical care. This finding may indicate greater psychosocial awareness, but it may also reflect reporting or recognition bias. Thus, the association should be interpreted as a relationship between awareness and recognition of perceived clinical impact rather than as evidence of a causal effect.
Respondents most frequently reported that mental status influenced disease explanation, healthcare-seeking behavior, surgical decision-making, and medication management. These domains are clinically relevant because anxiety may affect patients’ understanding during explanations, whereas depressive symptoms may reduce motivation for follow-up or treatment persistence. Nevertheless, the present survey did not directly evaluate adherence, consultation behavior, or treatment outcomes.
Clinical Implications
The findings suggest a perceived need for psychosocial awareness in ophthalmic care, especially for chronic progressive and vision-threatening diseases. Potential practical approaches include improved communication training, structured inquiry regarding patient concerns, and multidisciplinary collaboration when psychological distress is suspected.
These implications are consistent with the broader biopsychosocial model of medicine,14 which emphasizes the integration of biological, psychological, and social factors in healthcare. However, whether structured psychosocial approaches improve adherence, satisfaction, shared decision-making, or clinical outcomes in ophthalmology remains to be tested in future studies.
Strengths and Limitations
This study addresses an understudied area by focusing on ophthalmologists’ perceptions of patient mental status in clinical practice. The inclusion of disease ranking allowed us to explore which ocular diseases clinicians perceive as being associated with greater psychological burden.
Several limitations should be considered. First, this study assessed physicians’ perceptions rather than patient-reported psychological outcomes, objectively measured mental health status, or actual clinical decision-making behaviors. Therefore, the findings should be interpreted as ophthalmologists’ subjective perceptions and not as direct evidence of the psychological status of patients or its objective impact on clinical care.
Second, although the response rate was relatively high at 71.0%, the study population was limited to members of the Yamanashi Ophthalmologists Association, a regional professional organization in Yamanashi Prefecture, Japan. Therefore, the findings may not be fully generalizable to all ophthalmologists in Japan or to ophthalmologists practicing in other countries or healthcare systems. In addition, because participation was voluntary, selection bias cannot be excluded; ophthalmologists with greater interest in patient mental status or psychosocial aspects of ophthalmic care may have been more likely to respond.
Third, the questionnaire was developed for this exploratory survey and was not formally validated. Therefore, its measurement reliability, reproducibility, and construct validity remain uncertain. Future studies should use or develop validated instruments to assess ophthalmologists’ perceptions of patient mental status in clinical settings.
Fourth, the sample included a relatively high proportion of glaucoma specialists, which may have influenced the disease-ranking results. The finding that glaucoma was perceived as one of the diseases most strongly associated with psychological burden should therefore be interpreted in light of the specialty composition of the respondents.
Fifth, the study did not account for patient-level clinical factors, such as disease severity, duration of visual impairment, patient age, treatment history, adherence, or socioeconomic background, all of which may influence psychological burden and physicians’ perceptions of its clinical relevance. Sixth, the cross-sectional design precludes causal inference. Finally, because several statistical analyses, including the Bradley–Terry analysis, were performed in a modest sample with partial ranking data, the results should be interpreted as exploratory, descriptive, and hypothesis-generating.
Conclusion
Ophthalmologists in this sample perceived patient mental status as relevant to clinical practice, particularly in chronic progressive diseases such as glaucoma and inherited retinal disorders. Greater physician attention to psychological factors was associated with increased recognition of their perceived clinical impact. These findings support the need for further research on psychosocial awareness in ophthalmic care. Future studies should incorporate patient-reported outcomes, validated mental health instruments, and objective clinical endpoints to determine whether structured psychosocial approaches improve ophthalmic care.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Yamanashi School of Medicine (Approval Code: 2864).
Acknowledgments
The authors thank all participating ophthalmologists for their valuable contributions to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhang X, Bullard KM, Cotch MF, et al. Association between glaucoma and depressive symptoms among US adults. Am J Ophthalmol. 2017;178:111–10.
2. Evans JR, Fletcher AE, Wormald RPL. Depression and anxiety in visually impaired older people. Ophthalmology. 2007;114:283–288. doi:10.1016/j.ophtha.2006.10.006
3. Evans JR. Depression, anxiety and quality of life in visually impaired people. Curr Opin Ophthalmol. 2010;21:441–446.
4. Ribeiro MV, Hasten-Reiter HN, Menegat L, Ribeiro EA. Association between glaucoma and quality of life: a systematic review. Clinics. 2015;70:446–453. doi:10.6061/clinics/2015(06)11
5. Skalicky SE, Goldberg I. Depression and quality of life in patients with glaucoma. J Glaucoma. 2012;21:546–551.
6. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York: Springer; 1984.
7. Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmology. 2015;122:1308–1316. doi:10.1016/j.ophtha.2015.03.026
8. Sleath B, Blalock SJ, Covert D, et al. The relationship between glaucoma medication adherence, eye drop technique, and visual field defect severity. Ophthalmology. 2011;118:2398–2402. doi:10.1016/j.ophtha.2011.05.013
9. Bittner AK, Edwards L, George M. Coping strategies to manage stress related to vision loss and fluctuations in retinitis pigmentosa. Optometry. 2010;81:461–468. doi:10.1016/j.optm.2010.03.006
10. Leventhal H, Meyer D, Nerenz D. The common-sense model of illness danger. In: Medical Psychology. New York: Pergamon Press; 1980.
11. Mabuchi F, Yoshimura K, Kashiwagi K, et al. High prevalence of anxiety and depression in patients with primary open-angle glaucoma. J Glaucoma. 2012;21:435–440.
12. McKean-Cowdin R, Wang Y, Wu J, Azen SP, Varma R. Impact of visual field loss on health-related quality of life in glaucoma. Ophthalmology. 2008;115(6):941–948. doi:10.1016/j.ophtha.2007.08.037
13. Cross N, Rubin G, Kleinman M. Retinitis pigmentosa: burden of disease and unmet needs. Ophthalmol Ther. 2022;11:127–144.
14. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129–136. doi:10.1126/science.847460
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disease Burden of Glaucoma in China: Findings from the Global Burden of Disease 2019 Study
Sun Y, Chen A, Zou M, Liu Z, Young CA, Zheng D, Jin G
Clinical Epidemiology 2022, 14:827-834
Published Date: 4 July 2022
The Link Between Gastrointestinal Microbiome and Ocular Disorders
Alfuzaie R
Clinical Ophthalmology 2023, 17:2133-2140
Published Date: 25 July 2023
Awareness, Beliefs, and Psychological Impact of Patients with Alopecia Areata in Saudi Arabia: A Multi-Center Study
Almulhim NA, Alojail HY, Aljughayman MA, Almarri FH, Alsultan NH, Albash LA, Almukhaimar SK, Alkhamis AA, Albaqshi MA, Alkhawajah AA
Patient Preference and Adherence 2024, 18:2597-2607
Published Date: 20 December 2024
Trends in Glaucoma Fellowship Surgical Experience
Creagmile J, Chen N, Yee P, Lin K, Fox A, Smith A, Kwan C, Mosaed S
Clinical Ophthalmology 2025, 19:2719-2727
Published Date: 12 August 2025
MicroPulse Transscleral Cyclophotocoagulation for Early to Moderate Glaucoma: A Case Series of 11 Eyes with One-Year Follow-Up and Literature Review
Li L, Li Y
Clinical Ophthalmology 2026, 20:569880
Published Date: 28 January 2026