Back to Journals » Clinical Ophthalmology » Volume 20
MicroPulse Transscleral Cyclophotocoagulation for Early to Moderate Glaucoma: A Case Series of 11 Eyes with One-Year Follow-Up and Literature Review
Received 8 October 2025
Accepted for publication 22 January 2026
Published 28 January 2026 Volume 2026:20 569880
DOI https://doi.org/10.2147/OPTH.S569880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Liu Li, Yingjie Li
Department of Ophthalmology, Nanchang First Hospital, Nanchang, Jiangxi Province, 330008, People’s Republic of China
Correspondence: Yingjie Li, Department of Ophthalmology, Nanchang First Hospital, Nanchang, 330008, People’s Republic of China, Email [email protected]
Purpose: To assess the efficacy and safety of MicroPulse Transscleral Cyclophotocoagulation (MP-TSCPC) in Chinese patients with early to moderate glaucoma over a one-year follow-up.
Patients and Methods: This retrospective case series included 11 eyes of 11 consecutive Chinese patients with early to moderate glaucoma who underwent MP-TSCPC between November 2023 and March 2024. All patients were aged 18– 80 years, had a baseline intraocular pressure (IOP) ≥ 21 mmHg, and completed at least 12 months of follow-up. MP-TSCPC was performed using an Iridex Cyclo G6 laser with standardized settings (2000 mW power, 31.3% duty cycle, 160 seconds total). Changes in IOP, the number of anti-glaucoma medications, best-corrected visual acuity (BCVA), surgical success rates, and complications were recorded.
Results: At 12 months, mean IOP decreased significantly from 28.64± 12.18 mmHg to 18.09± 7.70 mmHg (P< 0.05), and the mean number of anti-glaucoma medications was reduced from 3.27± 0.91 to 1.64± 1.00 (P< 0.01). BCVA remained stable throughout follow-up. No severe complication occurred, transient mild anterior chamber inflammation resolved with treatment.
Conclusion: Despite the small cohort size, MP-TSCPC demonstrates preliminary efficacy and good safety profile in IOP control in Chinese patients with early to moderate glaucoma, significantly lowering IOP and reducing medication burden without negatively impacting visual acuity or causing serious complications.
Keywords: intraocular pressure reduction, anti-glaucoma medication burden, surgical safety profile, treatment efficacy, Chinese patient cohort
Introduction
Glaucoma is a progressive optic neuropathy that leads to visual field loss and remains a leading cause of irreversible blindness worldwide.1 Reducing intraocular pressure (IOP) is the key strategy for preventing further optic nerve damage and visual impairment.2 Although topical medications and conventional incisional surgeries are standard treatments, limitations remain, including poor patient adherence, medication-related ocular surface complications,3 and postoperative risks such as hypotony.4,5 These limitations highlight the need for innovative and safer therapeutic approaches.
Patients with refractory glaucoma, whose IOP remains uncontrolled despite optimal medical and surgical therapy, may require cyclodestructive procedures such as cyclocryotherapy and continuous-wave transscleral cyclophotocoagulation (CW-TSCPC). However, these interventions carry significant morbidity and are associated with complications—including persistent hypotony, phthisis bulbi, endophthalmitis, loss of vision, and severe pain—which severely limit their clinical utility.6–8
MicroPulse transscleral cyclophotocoagulation (MP-TSCPC) is a non-invasive laser procedure that applies repetitive pulses of diode laser energy to the pigmented ciliary epithelium. In the “on” phase, melanin absorbs the thermal energy, which decreases aqueous humor production and may enhance uveoscleral outflow; the “off” phase allows for tissue cooling and minimizes collateral damage.9 Compared to conventional CW-TSCPC, MP-TSCPC results in less inflammation and fewer postoperative complications.7 Its non-incisional nature, repeatability, and technical ease make MP-TSCPC a promising alternative for IOP control.
Although MP-TSCPC has demonstrated efficacy in refractory glaucoma, its use and long-term outcomes in early to moderate stages—and particularly among Chinese patients—have been inadequately studied. Most available studies focuses on advanced disease or have limited follow-up durations.10 To address this gap, we report a one-year case series of 11 Chinese patients with early to moderate glaucoma treated with MP-TSCPC. We present clinical outcomes in terms of IOP reduction, medication burden, visual acuity, and safety profile, contributing new evidence to guide management in this patient population.
Materials and Methods
Study Design and Patient Selection
This retrospective case series was conducted at Nanchang First Hospital in China and included 11 eyes from 11 consecutive patients with early to moderate glaucoma who underwent MP-TSCPC between November 2023 and March 2024. Eligible patients were aged 18–80 years, had a baseline intraocular pressure (IOP) of ≥21 mmHg, and demonstrated visual field loss consistent with early to moderate glaucoma according to the Hodapp-Parrish-Anderson classification.11 Exclusion criteria were neovascular or advanced glaucoma, prior cyclodestructive procedures, significant ocular comorbidities, or follow-up less than 12 months.
All procedures and data collection adhered to the principles of the Declaration of Helsinki principles, and ethical approval was obtained from the Ethics Committee of Nanchang First Hospital. Written informed consent was obtained from all participants prior to their inclusion in the study.
MP-TSCPC Procedure
All interventions were performed by a single experienced glaucoma specialist (Yingjie Li). MP-TSCPC was performed using the Iridex Cyclo G6 diode laser (IRIDEX Corporation, USA) with standardized parameters: 2000 mW power, 31.3% duty cycle, and total application time of 160 seconds per eye. The laser was applied 360 degrees of the limbal area, sparing the 3 and 9 o’clock and any existing filtering blebs to protect vital structures (eg, ciliary nerves) and prevent scleral thinning. Topical anesthesia was administered prior to the procedure. After surgery, all patients received topical corticosteroids and antibiotics for 1 to 2 weeks.
Clinical Assessment
Outcomes were assessed at baseline and at 1, 3, 6, and 12 months postoperatively. Both preoperative and postoperative intraocular pressure (IOP) measurements were obtained using non-contact tonometry (NCT). The number of prescribed anti-glaucoma medications was documented at each follow-up visit. Best-corrected visual acuity (BCVA) was measured using Snellen charts and subsequently converted to LogMAR units for statistical analysis. For patients with subnormal visual acuity, standardized LogMAR values were applied as follows: counting fingers = 2.6, hand motion = 2.9, light perception (LP) = 3.2, and no light perception (NLP) = 3.5.12,13 Any postoperative complications were also recorded.
Outcome Measures
The primary outcome was the change in mean intraocular pressure (IOP) from baseline to 12 months postoperatively. Secondary outcomes included the reduction in the number of anti-glaucoma medications, changes in BCVA, surgical success rate, and incidence of adverse events.
Surgical Success was defined as achieving a postoperative IOP ≤ 21 mmHg, regardless of medication use. Complete success was defined as an IOP of ≤ 21 mmHg without anti-glaucoma medications, while qualified success was defined as an IOP of ≤ 21 mmHg with or without medication. The surgical success rate was calculated as the percentage of eyes meeting these criteria.
Complication assessed included anterior chamber inflammation, hypotony (IOP < 6 mmHg), corneal pathology, choroidal detachment, and phthisis bulbi.
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA). Data are expressed as mean ± standard deviation. Differences between baseline and follow-up measures were assessed using paired Student’s t-test. A P-value < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of the Patients
As summarized in Table 1, a total of 11 patients (unilateral cases) were enrolled in this study, including 6 males and 5 females, with a mean age of (51.18±15.63) years and an average disease duration of (3.92±2.97) years. Prior to the current procedure, patients had undergone an average of 0.91±0.54 glaucoma surgeries. Based on medical history and gonioscopic examination, 5 eyes (45.45%) were diagnosed with primary open-angle glaucoma (POAG), 4 eyes (36.36%) with primary angle-closure glaucoma (PACG), and 2 eyes (18.18%) with secondary open-angle glaucoma (1 case due to corticosteroid use, and 1 case due to angle recession). Glaucoma was staged as early in 2 eyes (18.18%) and moderate in 9 eyes (81.82%). Details are listed in Table 1.
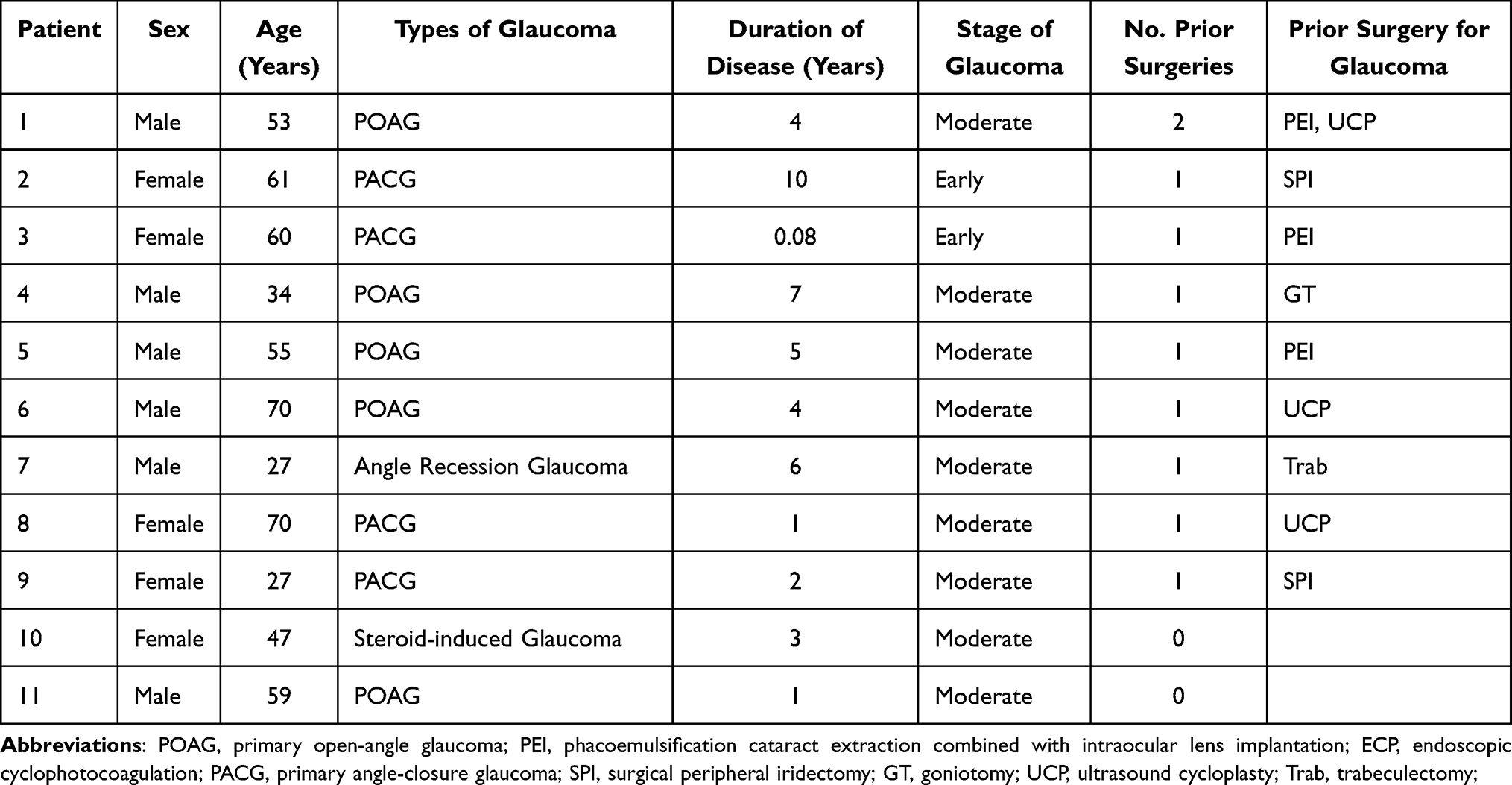 |
Table 1 Baseline Demographics and Characteristics of the Study Participants |
Changes in IOP
Preoperative IOP ranged from 21 to 57 mmHg, with a mean of 28.64±12.18 mmHg. At 12 months postoperatively, IOP significantly decreased to 18.09±7.70 mmHg (P<0.05, Table 2).
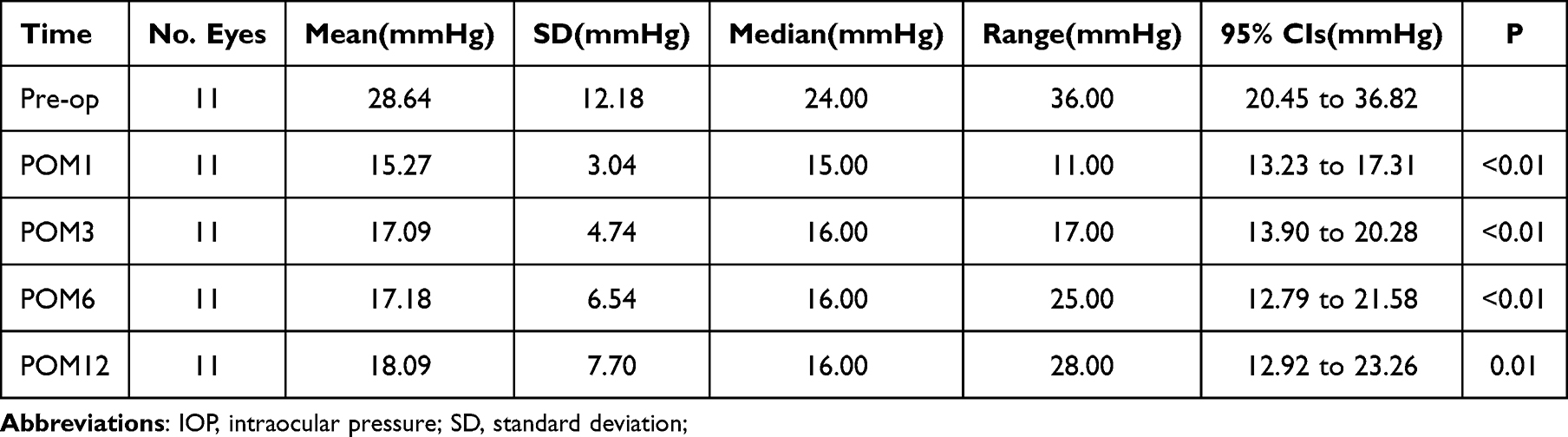 |
Table 2 Changes in IOP of the Study Participants |
Changes in Anti-Glaucoma Medications
The number of anti-glaucoma medications decreased from 3.27±0.91 at baseline to 1.64±1.00 at 12 months (P<0.01, Table 3).
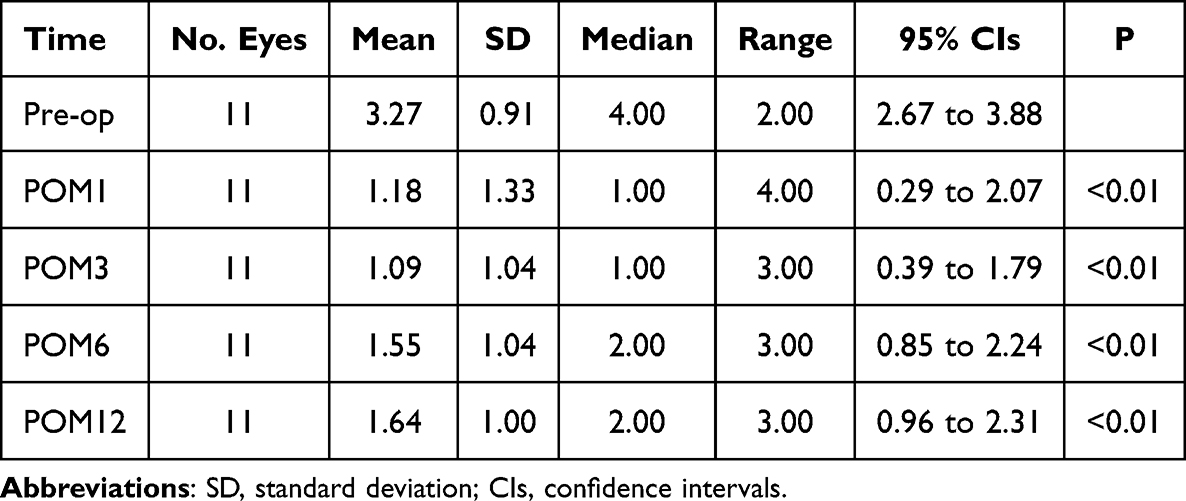 |
Table 3 Changes in Number of Medications of the Study Participants |
Changes in Best-Corrected Visual Acuity (BCVA)
There was no significant change in BCVA compared to baseline over the follow-up period (P > 0.05, Table 4). A change of more than two lines on the Snellen chart was defined as improvement or deterioration. At 1 month, BCVA improved in 2 patients (18.18%), with no significant change in the others. At 3 months, 3 patients (27.27%) showed improvement, while the remainder exhibited no change. At 6 months, improvement was observed in 2 patients (18.18%). At 1 year, BCVA improved in 3 patients (27.27%), declined in 2 patients (18.18%), and remained stable in the rest.
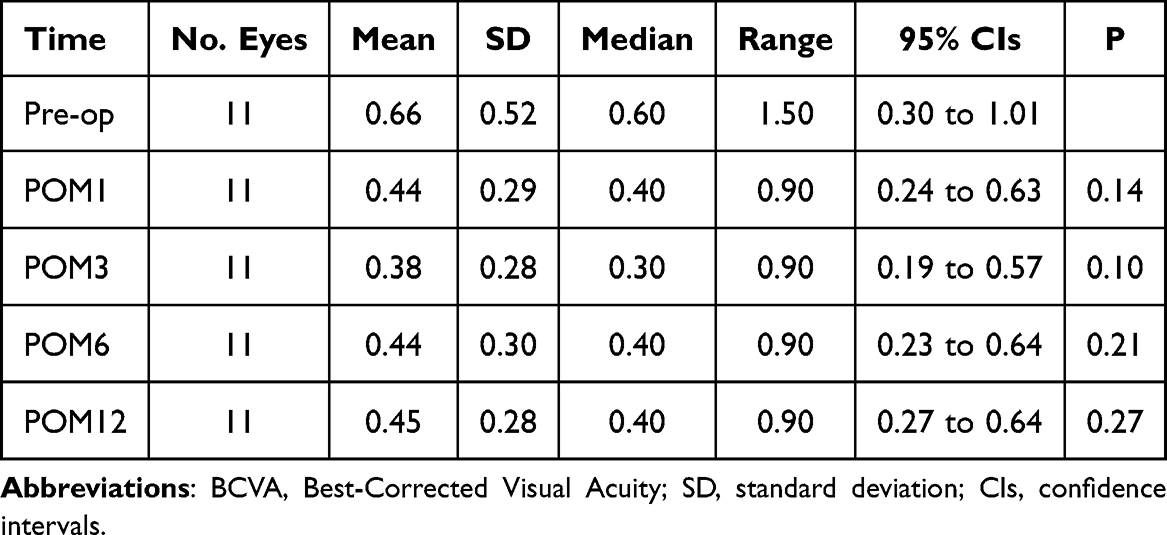 |
Table 4 Changes in BCVA of the Study Participants |
Success Rate
At 12 months, the complete success rate and qualified success rate were 9.09% (1/11 eyes) and 90.91% (10/11 eyes), respectively.
Complications
Post-operatively, one patient developed a conjunctival hemorrhage, which resolved spontaneously within one week. Mild anterior chamber inflammation (1+ flare) occurred in three cases and subsided within three days following topical steroid therapy.14 No severe complications (eg, choroidal detachment or phthisis bulbi) were observed.
Discussion
This retrospective case series reports one-year follow-up data of 11 consecutive patients with early to moderate glaucoma who underwent MicroPulse Transscleral Cyclophotocoagulation (MP-TSCPC). The results indicate that MP-TSCPC, a non-invasive glaucoma therapy, effectively reduced intraocular pressure (IOP) in this cohort, with IOP control remained over the one-year period. This outcome is consistent with the overarching goals of non-invasive glaucoma procedures: non-invasive, safety, and efficacy. Compared with traditional incisional glaucoma surgeries, which are associated with greater invasiveness and higher risk of complications, MP-TSCPC’s offers several advantages, including a non-penetrating approach, repeatability, and preservation of ocular surface. These attributes contribute to improved patient outcomes. This case series, while limited in sample size, provides valuable insights into the mid-term efficacy and safety of MP-TSCPC in Chinese patients with early to moderate glaucoma—a patient group which remains understudied in existing literature.
The significant IOP-lowering observed in this study aligns with findings from previous reports.15–17 However, most studies conducted in Chinese populations have primarily focused on refractory or advanced glaucoma, and follow-up has generally been ≤ 6 months.10,18–20 Studies from Hong Kong have not clearly distinguished glaucoma stage and typically provided outcomes at only one month post-treatment.21 Similarly, reports from Taiwan mainly included refractory cases, with one study restricting its cohort to primary open-angle glaucoma (POAG) and about 10% of cases being end-stage.22–24 In contrast, our cohort was composed exclusively of patients with early to moderate glaucoma and followed for 12 months, supplying preliminary evidence for sustained IOP control by MP-TSCPC in this underrepresented group.
Internationally, research on MP-TSCPC in early to moderate glaucoma is still limited. Murtaza et al treated 153 eyes, including 46 with early and 35 with moderate POAG, showing mean preoperative IOPs of 19.37 ± 4.91 mmHg and 18.31 ± 3.70 mmHg, respectively, which decreased to 15.74 ± 4.33 mmHg and 16.00 ± 6.01 mmHg after surgery.17 Despite adequate IOP reduction, there was no significant decrease in medication use, and reported surgical success rates (58.7% for early and 45.7% for moderate glaucoma) were lower than those observed in our series—possibly reflecting differences in success criteria. Bernardi et al described 47 eyes (mostly POAG, pseudoexfoliation, and angle-closure glaucoma), reporting a mean IOP reduction from 22.0 ± 7.2 mmHg to 15.7 ± 4.8 mmHg and an 87.5% success rate, comparable to the 90.91% observed in our study, likely owing to similar definitions of surgical success.25 Taken together, existing international literature supports the efficacy of MP-TSCPC in lowering IOP among patients with early to moderate glaucoma.
A notable finding of this series is the significant reduction in anti-glaucoma medication use following MP-TSCPC. The mean number of medications decreased from 3.27±0.91 at baseline to 1.64±1.00 at 12 months (P < 0.01), demonstrating that MP-TSCPC can not only lower IOP but also reduce medication dependency. Prolonged use of topical anti-glaucoma therapy is associated with ocular surface disorders, such as dry eye, allergic conjunctivitis, and corneal epithelial abnormalities.26–28 which negatively impact patient comfort, quality of life, and tolerance for ongoing therapy. Reducing medication reliance may alleviate these adverse effects, thereby improving overall patient quality of life. Additionally, lifelonged use of multiple medications can generate substantial financial burden, particularly for patients in low-resource settings. By decreasing medication requirements, MP-TSCPC may offer economic benefits and improved treatment accessibility, which is especially relevant in developing countries.
The safety profile of MP-TSCPC was favorable. Only one case of conjunctival hemorrhage (resolved spontaneously) and three cases of mild anterior chamber inflammation (resolved within 3 days of topical steroid treatment) were recorded with no severe complications such as choroidal detachment or phthisis bulbi. These observations are consistent with prior reports, which have described lower rates of complications with MP-TSCPC compared to conventional TSCPC, such as conjunctival burns, hyphema, choroidal detachment, and cataract.29–32 Micropulse technology, by delivering energy in short, controlled pulses, minimizes collateral thermal injury, thus reducing inflammation and other complications.7 This advantage is particularly important for preservation of visual function in early to moderate glaucoma.
With respect to visual outcomes, two patients experienced a decrease in visual acuity at one year, though no evidence of glaucoma progression was found based on IOP, cup-to-disc ratio, or visual fields; cataract progression was considered the likely cause. Conversely, three patients had improved visual acuity postoperatively. Notably, two of these had high baseline IOPs (>45 mmHg), suggesting that restoration of retinal perfusion and relief of axoplasmic stasis contributed to visual improvement after IOP reduction. Another patient who benefited had a reduction in the number of topical medications postoperatively, likely resulting in stabilization of the tear film and improvement of vision, as multiple medications are known to negatively affect the ocular surface.33 Overall, these findings suggest that MP-TSCPC may stabilize, and in select cases improve, visual function by mechanisms both related and unrelated to IOP reduction.
As a retrospective case series, this study has inherent limitations. The small sample size limits statistical power and generalizability, and increases susceptibility to selection bias. Lack of a control group precludes direct comparison with other treatments. An uneven distribution of glaucoma subtypes within this small cohort may further affect generalizability. Although the 12-month follow-up provides mid-term data, long-term efficacy and safety remain to be determined and warrant further prospective research. While Goldmann applanation tonometry was used at initial diagnosis to ensure accuracy, all follow-up IOP measurements in this study were assessed with non-contact tonometry (NCT), chosen for its convenience, patient comfort, and acceptable accuracy in this early to moderate glaucoma cohort.34,35
Given these limitations, the results should be regarded as exploratory and preliminary. The aim of this study is not to provide definitive conclusions, but rather to offer initial clinical observations and reference data to inform future research. Despite these constraints, our findings suggest that MP-TSCPC is a promising option for early to moderate glaucoma in Chinese patients, supporting further large-scale, prospective, longer investigations.
Conclusion
This exploratory study provides promising evidence for the mid-term effectiveness and safety of MP-TSCPC in Chinese patients with early to moderate glaucoma, based on one-year follow-up data. Nevertheless, these results should be considered preliminary because of the study’s small sample size and retrospective nature. To confirm and expand upon these findings, future prospective studies with larger, more diverse cohorts—preferably employing randomized controlled designs—are warranted. Such research will offer more robust data regarding the long-term efficacy and safety of MP-TSCPC.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
All experimental protocols were approved by the Ethics Committee of Nanchang First Hospital. Informed consent was obtained from all participants.
Funding
This work was supported by the Natural Science Foundation of Jiangxi Province (Grant No. 20212BAG70033), and the Health Commission of Jiangxi Province (Grant No. 2026L1003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jonas JB, Aung T, Bourne RR, et al. Glaucoma. Lancet. 2017;390(10108):2183–8. doi:10.1016/S0140-6736(17)31469-1
2. Ofri R. Intraocular pressure and glaucoma. Vet Clin North Am Exot Anim Pract. 2002;5(2):391–406. doi:10.1016/S1094-9194(01)00004-4
3. Kim S, Tong B, Lee J, et al. Lifestyle counseling for medication adherence in glaucoma. Clin Ophthalmol. 2021;15:3521–3529. doi:10.2147/OPTH.S321351
4. Chai C, Loon SC. Meta-analysis of viscocanalostomy versus trabeculectomy in uncontrolled glaucoma. J Glaucoma. 2010;19(8):519–527. doi:10.1097/IJG.0b013e3181ca7694
5. Leung DY, Tham CC. Management of bleb complications after trabeculectomy. Semin Ophthalmol. 2013;28(3):144–156. doi:10.3109/08820538.2013.771199
6. Kim BS, Kim YJ, Seo SW, et al. Long-term results from cyclocryotherapy applied to the 3 o’clock and 9 o’clock positions in blind refractory glaucoma patients. Korean J Ophthalmol. 2015;29(1):47–52. doi:10.3341/kjo.2015.29.1.47
7. Abdelrahman AM, El Sayed YM. Micropulse versus continuous wave transscleral cyclophotocoagulation in refractory pediatric glaucoma. J Glaucoma. 2018;27(10):900–905. doi:10.1097/IJG.0000000000001053
8. Maestrini HA, Russ HHA, Seixas RCS, et al. Continuous wave transscleral cyclophotocoagulation with the slow-cooking protocol to treat refractory glaucomas. Eur J Ophthalmol. 2025;35(5):1654–1665. doi:10.1177/11206721251335381
9. Sanchez FG, Peirano-Bonomi JC, Grippo TM. Micropulse transscleral cyclophotocoagulation: a hypothesis for the ideal parameters. Med Hypothesis Discov Innov Ophthalmol. 2018;7(3):94–100.
10. Cheng FC. Efficacy analysis of micropulse laser transscleral cyclophotocoagulation in the treatment of advanced glaucoma. Medical Diet Health. 2020;18(10):64–65.
11. Wm H Jr, Becker B. The onset and evolution of glaucomatous visual field defects. Ophthalmology. 1982;89(3):268–279. doi:10.1016/S0161-6420(82)34798-3
12. Shaarawy TM, Sherwood MB, Grehn F, editors. World Glaucoma Association Guidelines on Design and Reporting of Glaucoma Surgical Trials. Amsterdam: Kugler Publications; 2009.
13. Li L, Li Y, Hong L, et al. Twelve-month outcomes of ultrasound cycloplasty after failed glaucoma surgery: a prospective study. J Glaucoma. 2025;34(11):959–963. doi:10.1097/IJG.0000000000002621
14. Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516.
15. Vig N, Ameen S, Bloom P, et al. Micropulse transscleral cyclophotocoagulation: initial results using a reduced energy protocol in refractory glaucoma. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):1073–1079. doi:10.1007/s00417-020-04611-0
16. Sivasubramanian R, Siddharth K, Senthilkumar VA, et al. Safety and efficacy of micropulse in pediatric eyes with refractory glaucoma. Indian J Ophthalmol. 2025;73(Suppl 2):S227–S231. doi:10.4103/IJO.IJO_1066_24
17. Murtaza F, Kaba Q, Somani S, et al. Micropulse transscleral cyclophotocoagulation in non-incisional eyes with ocular hypertension and primary open-angle glaucoma. Clin Ophthalmol. 2024;18:1295–1312. doi:10.2147/OPTH.S447875
18. Lin FB, Hu BY, Lin QY, et al. Efficacy and safety of micropulse transscleral cyclophotocoagulation in the treatment of refractory glaucoma: a prospective multicenter observational study. Chin J Exp Ophthalmol. 2024;42(06):527–531.
19. Guo Q, Chen B, Ji Y, et al. Clinical efficacy of micropulse transscleral cyclophotocoagulation in the treatment of refractory glaucoma in Qinghai region. J High Altitude Med. 2025;35(03):10–14.
20. Man XF, Zhao PQ. Efficacy of micropulse laser transscleral cyclophotocoagulation in refractory pediatric claucoma: a six-month follow-up study. Chin J Ophthalmol Otorhinolaryngol. 2025;25(06):498–501+509.
21. Wong HM, Tsui LY, Poon SY, et al. In vivo confocal microscopy (IVCM) analysis of corneal sub-basal nerve plexus (SNP) and corneal sensitivity after micropulse transscleral cyclophotocoagulation (MP-TSCPC) in glaucoma patients. Int Ophthalmol. 2025;46(1):4. doi:10.1007/s10792-025-03862-2
22. Chen HS, Yeh PH, Yeh CT, et al. Micropulse transscleral cyclophotocoagulation in a Taiwanese population: 2-year clinical outcomes and prognostic factors. Graefes Arch Clin Exp Ophthalmol. 2022;260(4):1265–1273. doi:10.1007/s00417-021-05468-7
23. Chen KY, Chang SHL. Comparison of the efficacy of micropulse diode laser transscleral cyclophotocoagulation using different energy protocols. Taiwan J Ophthalmol. 2024;14(3):414–421. doi:10.4103/tjo.TJO-D-23-00129
24. Chang HL, Chao SC, Lee MT, et al. Micropulse transscleral cyclophotocoagulation as primary surgical treatment for primary open angle glaucoma in Taiwan during the COVID-19 pandemic. Healthcare. 2021;9(11):1563. doi:10.3390/healthcare9111563
25. Bernardi E, Töteberg-Harms M. MicroPulse transscleral laser therapy demonstrates similar efficacy with a superior and more favorable safety profile compared to continuous-wave transscleral cyclophotocoagulation. J Ophthalmol. 2022;2022:8566044. doi:10.1155/2022/8566044
26. Chen HY, Lin CL, Tsai YY, et al. Association between glaucoma medication usage and dry eye in Taiwan. Optom Vis Sci. 2015;92(9):e227–32. doi:10.1097/OPX.0000000000000667
27. Tanihara H, Yamamoto T, Aihara M, et al. Long-term intraocular pressure-lowering efficacy and safety of ripasudil-brimonidine fixed-dose combination for glaucoma and ocular hypertension: a multicentre, open-label, Phase 3 study. Graefes Arch Clin Exp Ophthalmol. 2024;262(8):2579–2591. doi:10.1007/s00417-024-06388-y
28. Pinheiro R, Panfil C, Schrage N, et al. The impact of glaucoma medications on corneal wound healing. J Glaucoma. 2016;25(1):122–127. doi:10.1097/IJG.0000000000000279
29. Gupta V, Sony P, Sihota R. Inadvertent sclerostomy with encysted bleb following trans-scleral contact diode laser cyclophotocoagulation. Clin Exp Ophthalmol. 2006;34(1):86–87. doi:10.1111/j.1442-9071.2006.01125.x
30. Kermani O, Mons B, Kirchhof B, et al. Contact cw-Nd:YAG laser cyclophotocoagulation for treatment of refractory glaucoma. Ger J Ophthalmol. 1992;1(2):74–78.
31. Sheheitli H, Persad PJ, Feuer WJ, et al. Treatment outcomes of primary transscleral cyclophotocoagulation. Ophthalmol Glaucoma. 2021;4(5):472–481. doi:10.1016/j.ogla.2020.12.014
32. Tan AM, Chockalingam M, Aquino MC, et al. Micropulse transscleral diode laser cyclophotocoagulation in the treatment of refractory glaucoma. Clin Exp Ophthalmol. 2010;38(3):266–272. doi:10.1111/j.1442-9071.2010.02238.x
33. Kaido M. Functional Visual Acuity. Invest Ophthalmol Vis Sci. 2018;59(14):DES29–DES35. doi:10.1167/iovs.17-23721
34. Yildiz A, Yasar T. Comparison of Goldmann applanation, non-contact, dynamic contour and tonopen tonometry measurements in healthy and glaucomatous eyes, and effect of central corneal thickness on the measurement results. Med Glas. 2018;15(2):152–157. doi:10.17392/960-18
35. Chaglasian M, Hou H, Tafreshi M, et al. Clinical assessment of automated non-contact tonometer: interchangeability with Goldmann applanation tonometry and repeatability. J Clin Med. 2025;14(8):2726. doi:10.3390/jcm14082726
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Link Between Gastrointestinal Microbiome and Ocular Disorders
Alfuzaie R
Clinical Ophthalmology 2023, 17:2133-2140
Published Date: 25 July 2023
Trends in Glaucoma Fellowship Surgical Experience
Creagmile J, Chen N, Yee P, Lin K, Fox A, Smith A, Kwan C, Mosaed S
Clinical Ophthalmology 2025, 19:2719-2727
Published Date: 12 August 2025
Micropulse Transscleral Cyclophotocoagulation for the Management of Diverse Glaucoma Types: A Multicenter Short-Term Real-World Study

Lima NVDA, Lopes NLV, Maestrini HA, Giacometti HHAR, Rodrigues Neto TDS, Mario LPD, Fernandes TAP, Balbino M, Seixas RCS, Moreira LP
Clinical Ophthalmology 2026, 20:555181
Published Date: 8 January 2026
Ophthalmologists’ Perceptions of the Impact of Patient Mental Status on Clinical Decision-Making: A Cross-Sectional Survey
Kashiwagi K, Kasai H, Fukuda Y, Hosoda S, Tanabe N
Clinical Ophthalmology 2026, 20:620562
Published Date: 13 July 2026