Back to Journals » Drug Design, Development and Therapy » Volume 20
Oliceridine versus Sufentanil on Postoperative Nausea and Vomiting in Women Undergoing Gynecological Laparoscopic Surgery: A Randomized Double‑Blind Controlled Trial
Authors Liu F ![]() , Liu N
, Liu N ![]() , Wang X
, Wang X ![]() , Liu Z, Tao Z, Yuan Q
, Liu Z, Tao Z, Yuan Q ![]() , Zhang Y, Guan Z
, Zhang Y, Guan Z ![]() , Shen W
, Shen W ![]() , Tang B
, Tang B ![]() , Liu Z
, Liu Z ![]() , Yang L
, Yang L ![]()
Received 1 May 2026
Accepted for publication 2 July 2026
Published 14 July 2026 Volume 2026:20 621409
DOI https://doi.org/10.2147/DDDT.S621409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Feng Liu,1,* Ning Liu,1,* Xin Wang,2,* Zhe Liu,3 Zhirui Tao,4 Qisong Yuan,1 Yi Zhang,1 Zhaoming Guan,1 Wang Shen,1 Bing Tang,1 Zhenyuan Liu,1 Longqiu Yang1
1Department of Anesthesiology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2Department of Anesthesiology, Shengjing Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 3College of Acupuncture and Tuina, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 4Department of Oncology, Tongji Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenyuan Liu, Department of Anesthesiology, Shanghai East Hospital, Tongji University School of Medicine, No. 1800, Yuntai Road, Shanghai, 200120, People’s Republic of China, Email [email protected] Longqiu Yang, Department of Anesthesiology, Shanghai East Hospital, Tongji University School of Medicine, No. 1800, Yuntai Road, Shanghai, 200120, People’s Republic of China, Email [email protected]
Purpose: To evaluate whether oliceridine, a G protein-biased μ-opioid receptor agonist, reduces postoperative nausea and vomiting (PONV) compared with sufentanil in women undergoing gynecological laparoscopic surgery.
Patients and Methods: This prospective, double-blind, randomized controlled trial recruited 260 female patients, ASA physical status I–III, undergoing elective gynecological laparoscopic surgery under general anesthesia at Shanghai East Hospital, Shanghai, People’s Republic of China. Patients were randomized to receive oliceridine (induction 0.05 mg/kg; postoperative infusion 0.4 mg/kg) or sufentanil (induction 0.5 μg/kg; postoperative infusion 2.0 μg/kg), with standardized general anesthesia and prophylactic antiemetics. The primary outcome was 48-hour cumulative PONV incidence. Secondary outcomes included PONV severity, opioid-induced respiratory depression (OIRD), adverse events, pain scores, 15-item Quality of Recovery (QoR-15) score, and patient satisfaction. All analyses were performed on the modified intention-to-treat population.
Results: The 48-hour PONV incidence was significantly lower with oliceridine (22.5% vs 43.0%; odds ratio 0.38; 95% CI 0.22– 0.66; P < 0.001), with consistent findings after multivariate adjustment. The absolute risk reduction was 20.5%, with a relative risk of 0.52, and a number needed to treat of 5, representing a clinically meaningful antiemetic advantage. Severe PONV was reduced (3.9% vs 15.6%, q = 0.02). No significant differences were observed in pain scores or rescue analgesia. Oliceridine patients reported higher QoR-15 scores (median 123 vs 116, q = 0.002) and greater satisfaction (69.0% vs 50.8%, q = 0.02). OIRD and dizziness trended lower but were not significant after multiplicity correction.
Conclusion: Oliceridine significantly reduced PONV incidence and improved recovery quality and patient satisfaction compared with sufentanil, without compromising analgesia, in women undergoing gynecological laparoscopic surgery.
Keywords: oliceridine, opioids, PONV, gynecologic surgery, laparoscopy, QoR-15
Introduction
Postoperative nausea and vomiting (PONV) remains one of the most common and distressing complications after general anesthesia, with an overall incidence of approximately 30% in the general surgical population and up to 80% in untreated high‑risk cohorts.1 Female patients undergoing gynecological laparoscopic surgery (GLS) are particularly susceptible due to the convergence of multiple risk factors, including female sex, non‑smoking status, laparoscopic pneumoperitoneum, and perioperative opioid use.1–4 PONV not only impairs patient satisfaction and recovery quality but also prolongs post‑anesthesia care unit (PACU) stay, increases healthcare costs, and may lead to serious complications such as wound dehiscence, electrolyte imbalance, and aspiration.5–7
Intraoperative opioid administration is a well‑established, dose‑dependent risk factor for PONV, primarily through non‑selective activation of the μ‑opioid receptor (MOR).1 Conventional opioids such as sufentanil and fentanyl engage both the G‑protein signaling pathway (mediating analgesia) and the β‑arrestin pathway, which is strongly associated with opioid‑related adverse events (ORAEs) including nausea, vomiting, sedation, and respiratory depression.8 Oliceridine, a novel G protein‑biased MOR agonist, preferentially activates the G‑protein pathway while substantially reducing β‑arrestin recruitment.9 This biased agonism is hypothesized to preserve analgesic efficacy while mitigating β‑arrestin‑mediated adverse effects.8,10,11 A recent meta‑analysis of randomized controlled trials (RCTs) confirmed that oliceridine, compared with morphine, significantly reduces the incidence of postoperative nausea, vomiting, dizziness, and hypoxemia.12
Recent RCTs have demonstrated the benefits of oliceridine across various surgical settings: it reduces PONV and respiratory depression compared with sufentanil in gastrointestinal endoscopy,13 improves early recovery quality after hysteroscopic surgery,14 and, when compared with morphine in thoracic surgery, achieves faster extubation and superior immediate analgesia.15 Sufentanil is the most frequently used perioperative opioid for GLS at our institution and represents the standard opioid analgesic in this surgical population. However, to our knowledge, few prospective RCTs have directly compared oliceridine with sufentanil for PONV prevention in GLS,16,17 a setting characterized by a uniquely high PONV burden and specific surgical stress.4,7
Therefore, we conducted this prospective, double‑blind, randomized controlled trial to test the hypothesis that oliceridine, compared with sufentanil, reduces the incidence of PONV within 48 hours after GLS, providing head‑to‑head clinical evidence and mechanistic insights into biased opioid signaling in this high‑risk population.
Materials and Methods
Study Design
This prospective, randomized, double‑blind controlled trial was conducted at a single center in Shanghai East Hospital. The study was performed in strict accordance with the ethical principles of the Declaration of Helsinki and is reported in compliance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Ethical Considerations
Ethical approval was granted by the Medical Ethics Committee of Shanghai East Hospital (approval number: 2025YS-085) on March 31, 2025. The trial was prospectively registered with the Chinese Clinical Trial Registry (registration number: ChiCTR2500110250) on October 11, 2025, prior to the enrollment of the first participant. Written informed consent was obtained from all patients before any study‑related procedures and retained by the investigators.
Participants
Eligible patients were recruited from October 18, 2025, to April 6, 2026. Inclusion criteria were female sex, age 18 years or older, American Society of Anesthesiologists (ASA) physical status I to III, and scheduled elective gynecological laparoscopic surgery under general anesthesia. Exclusion criteria were severe hepatic or renal dysfunction, known allergy or contraindication to oliceridine or sufentanil, preoperative use of antiemetic medications, pregnancy or lactation, anticipated postoperative tracheal intubation with intensive care unit (ICU) admission, psychiatric disorders or communication difficulties, and any other condition deemed by the investigators to render the patient ineligible for study participation. For this study, female was defined as female sex assigned at birth. All participants provided written informed consent prior to enrollment.
Randomization and Blinding
Eligible patients were randomly assigned in a 1:1 ratio to either the oliceridine group or the sufentanil group. Randomization was stratified by type of surgery and Apfel PONV risk score (2 vs ≥ 3) using permuted blocks with randomly varying sizes of 4 and 6. The allocation sequence was generated by an independent statistician using an online randomization tool (Sealed Envelope Ltd., London, UK) and concealed in sequentially numbered, opaque, sealed envelopes.
To maintain blinding, an anesthesia nurse not otherwise engaged in the care or evaluation of study participants prepared all investigational drugs. For each patient, the assigned opioid was diluted in normal saline to an identical final volume and placed in indistinguishable syringes labeled exclusively with the randomization number and the intended phase of administration (induction or postoperative infusion). The postoperative analgesic solution was prepared in identical reservoirs and administered via a mechanical infusion pump without revealing the identity of the study drug. All patients, attending anesthesiologists, surgeons, and personnel responsible for postoperative follow‑up and data collection remained unaware of group allocation throughout the study.
Intervention
Preoperative Management
All patients underwent a standardized general anesthesia protocol combined with preoperative regional analgesia. Before induction of anesthesia, ultrasound‑guided transversus abdominis plane (TAP) block was performed bilaterally using liposomal bupivacaine.
Intraoperative Care
Upon arrival in the operating room, standard monitoring was established, including electrocardiography, noninvasive blood pressure, pulse oximetry, end‑tidal carbon dioxide (ETCO2) monitoring, and Bispectral Index (BIS) measurement. Invasive arterial blood pressure monitoring was employed at the discretion of the attending anesthesiologist. Anesthesia was induced with intravenous remimazolam 0.1 mg/kg, propofol 1.5 mg/kg, rocuronium 1.0 mg/kg, and the assigned study drug. According to group allocation, patients in the oliceridine group received oliceridine 0.05 mg/kg, whereas those in the sufentanil group received sufentanil 0.5 μg/kg. The doses of oliceridine and sufentanil were selected based on their known analgesic potency relative to morphine, with an approximate potency ratio of 1:100 to 1:200. After tracheal intubation, mechanical ventilation was initiated with a tidal volume of 6–8 mL/kg, and a respiratory rate adjusted to maintain ETCO2 between 35 and 45 mmHg.
Anesthesia was maintained with sevoflurane inhalation at an end‑tidal concentration of 0.7–1.0 minimum alveolar concentration (MAC), propofol infusion at 2–6 mg/kg/h, and remifentanil infusion at 0.1–0.3 μg/kg/min. Additional boluses of rocuronium were administered at the discretion of the anesthesiologist based on neuromuscular monitoring. The doses of sevoflurane, propofol, and remifentanil were titrated to maintain the BIS between 40 and 60 and to keep blood pressure and heart rate within ±20% of preoperative baseline values. Approximately 20 minutes before the anticipated completion of surgery, sevoflurane inhalation was discontinued, and ondansetron 4 mg was administered intravenously. Ten minutes before the end of surgery, propofol infusion was stopped, and a final dose of the assigned study drug (oliceridine 0.5 mg or sufentanil 5 μg) was given. Remifentanil infusion was terminated at the conclusion of surgery. Neuromuscular blockade was antagonized with sugammadex 2 mg/kg, and the trachea was extubated after confirmation of adequate spontaneous ventilation and recovery of consciousness.
Postoperative Protocol
For postoperative analgesia, a mechanical intravenous infusion pump was connected immediately after surgery. Patients in the oliceridine group received oliceridine 0.4 mg/kg diluted in normal saline to a total volume of 100 mL, and patients in the sufentanil group received sufentanil 2.0 μg/kg similarly diluted. Both solutions also contained ondansetron 8 mg for additional PONV prophylaxis. The pump was programmed to deliver a continuous background infusion at a rate of 2.5 mL/h. Pain intensity was evaluated using a numerical rating scale (NRS) ranging from 0 (no pain) to 10 (worst imaginable pain). Rescue analgesia with intravenous flurbiprofen axetil 50 mg was permitted if the NRS pain score exceeded 4 at rest. For persistent nausea or vomiting, metoclopramide 10 mg was administered intravenously as rescue antiemetic therapy.
Outcomes
Primary Outcome
The primary outcome was the cumulative incidence of PONV within 48 hours after surgery. PONV was defined as any episode of nausea, retching, or vomiting occurring during the 48-hour postoperative period, consistent with the Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting.6 PONV was assessed at six timepoints after surgery: 0–30 min (T1), > 30 min-2 h (T2), > 2–6 h (T3), > 6–12 h (T4), > 12–24 h (T5), and > 24–48 h (T6). These intervals were chosen to reflect distinct recovery phases: the early emergence period (T1-T2), the expected peak incidence window (T3-T4), and the later phase of delayed PONV (T5-T6). PONV events were assessed through direct patient interviews conducted by trained outcome assessors blinded to group allocation.
Secondary Outcomes
Secondary outcomes included PONV severity, postoperative adverse events, as well as pain and recovery measures. PONV severity was assessed using a visual analog scale (VAS) ranging from 0 to 10, and categorized as mild (VAS 1–3), moderate (VAS 4–6), or severe (VAS 7–10).
Postoperative adverse events were recorded within 48 hours after surgery and included opioid‑induced respiratory depression (OIRD), hypotension, hypertension, bradycardia, tachycardia, dizziness, headache, pruritus, shivering, and dry mouth. OIRD was defined as a respiratory rate < 8 breaths/min or oxygen saturation < 90% requiring intervention. Hypotension was defined as a decrease in mean arterial pressure > 30% from baseline, and hypertension as an increase > 30% from baseline. Bradycardia was defined as a heart rate < 50 beats/min, and tachycardia as a heart rate > 100 beats/min.
The maximum NRS pain score during the 48‑hour period and the proportion of patients with an NRS pain score ≥ 4 were recorded. The need for rescue analgesia was documented. Recovery outcomes included time to first flatus, hospital length of stay, quality of recovery assessed by the 15-item Quality of Recovery (QoR‑15) score, and patient satisfaction. Patient satisfaction was evaluated using a 5‑point Likert scale, and high satisfaction was defined as a score of 4 or 5.
Sample Size
Based on a pilot study of 25 patients per group, the observed PONV incidence was 36.0% (9/25) in the sufentanil group and 20.0% (5/25) in the oliceridine group, corresponding to an absolute risk reduction of 16.0 percentage points in favor of oliceridine. Assuming a two‑sided significance level of 0.05, a power of 0.80, and a 1:1 allocation ratio, a two‑proportions z‑test (unpooled) indicated that 120 patients per group would be required. Based on institutional experience with similar elective surgical procedures, an anticipated dropout rate of 5% was considered appropriate. Accordingly, the planned enrollment was 127 patients per group, for a total of 254 patients. Sample size calculation was performed using PASS software version 2021 (NCSS, LLC, Kaysville, UT, USA). All assumptions regarding the anticipated effect size, significance level, power, and dropout rate were prespecified before the start of the main trial. The pilot patients were not included in the final analysis.
Statistical Analyses
All statistical analyses were performed using R version 4.3.2 (R Foundation of Statistical Computing). Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation (SD) and compared between groups using the independent samples t‑test. Non‑normally distributed data were presented as median with interquartile range (IQR) and analyzed using the Mann–Whitney U-test. Categorical variables were expressed as numbers (percentages) and compared using the chi‑square test or Fisher exact test, as appropriate. For each baseline characteristic, the standardized mean difference (SMD) was calculated to assess balance between groups, with an SMD > 0.10 considered indicative of meaningful imbalance.
All analyses were performed on the modified intention-to-treat (mITT) population, defined as all randomized patients who received the assigned study intervention and had available primary outcome data. The primary outcome was analyzed using logistic regression, with results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). To adjust for potential confounding, two prespecified multivariate logistic regression models were fitted. Model 1 included established high‑risk factors for PONV: Apfel PONV risk score, duration of surgery, and total remifentanil consumption. Model 2 additionally adjusted for variables with a SMD greater than 0.10 at baseline: age, BMI, and sevoflurane consumption.
For secondary outcomes, P values were adjusted using the Benjamini-Hochberg procedure to control the false discovery rate, and the resulting adjusted P values are reported as q values. Prespecified subgroup analyses of the primary outcome were performed according to age (< 60 vs ≥ 60 years), BMI (< 25 vs ≥ 25 kg/m2), ASA physical status (I–II vs III), Apfel PONV risk score (2 vs ≥ 3), history of hypertension, and type of surgery. Interaction terms between treatment group and each subgroup variable were included in logistic regression models to evaluate effect modification. All tests were two‑sided, and statistical significance was set at P < 0.05 for the primary outcome and q < 0.05 for secondary outcomes after false discovery rate correction. All analyses of PONV incidence at individual time points (T1–T6) were considered exploratory and were not adjusted for multiple comparisons.
Results
Of 272 patients screened for eligibility, 260 were randomly assigned to receive either oliceridine or sufentanil. After randomization, 1 patient in the oliceridine group and 2 patients in the sufentanil group were transferred to the ICU with tracheal intubation. Consequently, the mITT analysis included 129 patients in the oliceridine group and 128 patients in the sufentanil group. The flowchart of participant enrollment and allocation is presented in Figure 1.
 |
Figure 1 Flowchart of participant enrollment and allocation. |
Demographic and baseline characteristics, as well as intraoperative measurements, are presented in Table 1. Imbalances between groups were observed in age (SMD, 0.20), BMI (SMD, 0.18), and sevoflurane consumption (SMD, 0.23). Other baseline variables, including height, weight, ASA physical status, Apfel PONV risk score, comorbidities, duration of surgery, duration of anesthesia, remifentanil consumption, intravenous fluids, blood transfusion, use of vasopressors, type of surgery, and conversion to laparotomy, were well balanced between the two groups.
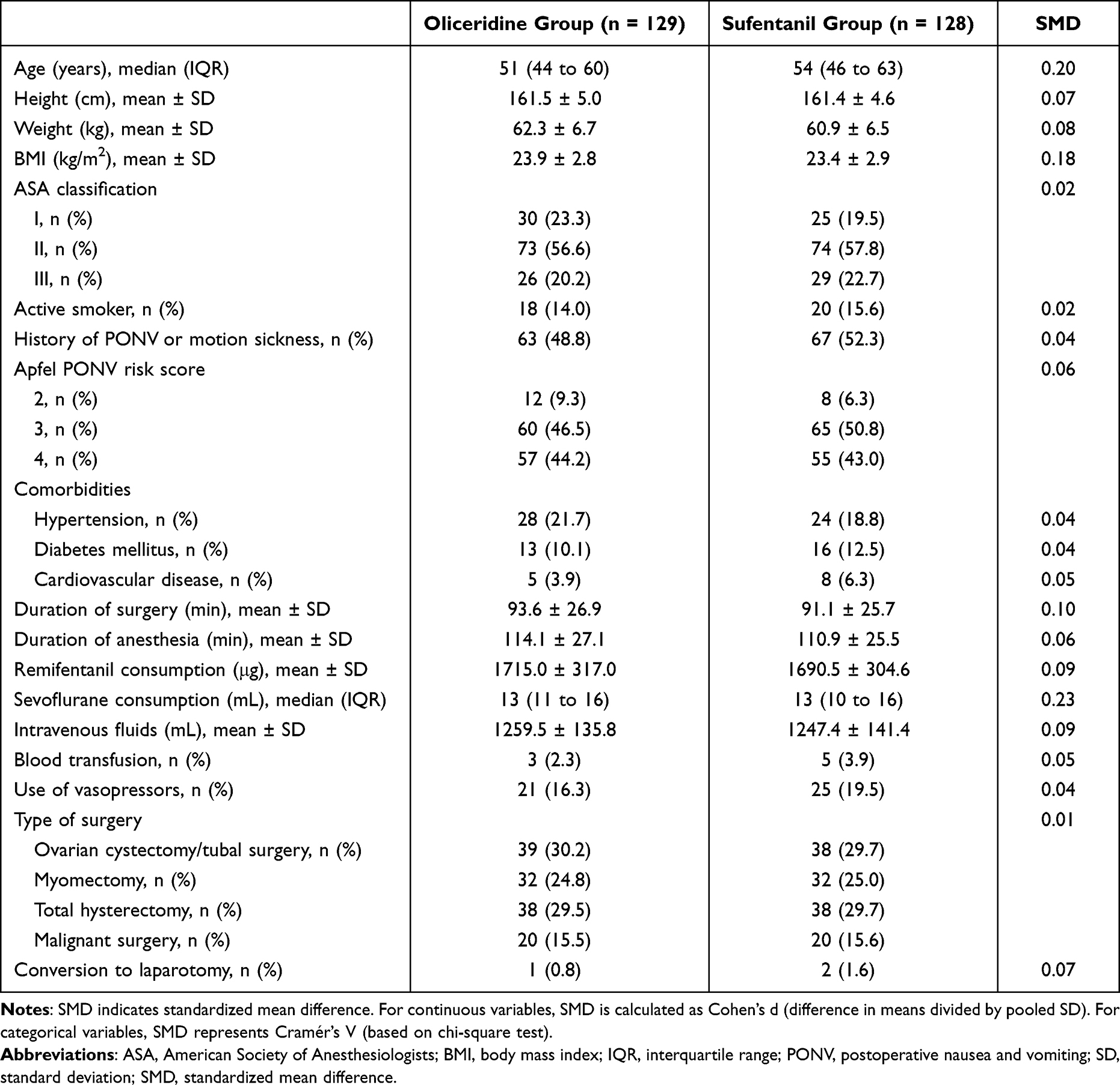 |
Table 1 Baseline Characteristics and Intraoperative Measurements |
Primary Outcome
The incidence of PONV within 48 hours after surgery was significantly lower in the oliceridine group compared with the sufentanil group (22.5% vs 43.0%; OR, 0.38; 95% CI, 0.22 to 0.66; P < 0.001) (Table 2). This difference remained statistically significant after adjustment for Apfel PONV risk score, duration of surgery, and total remifentanil consumption in Model 1 (OR, 0.37; 95% CI, 0.21 to 0.64; P < 0.001), and after further adjustment for age, BMI, and sevoflurane consumption in Model 2 (OR, 0.36; 95% CI, 0.20 to 0.67; P = 0.001). When analyzed by postoperative time intervals (T1-T6), the oliceridine group showed consistently lower PONV rates at all time points, with nominal statistical significance observed from T2 to T6 in these exploratory analyses (all P < 0.05).
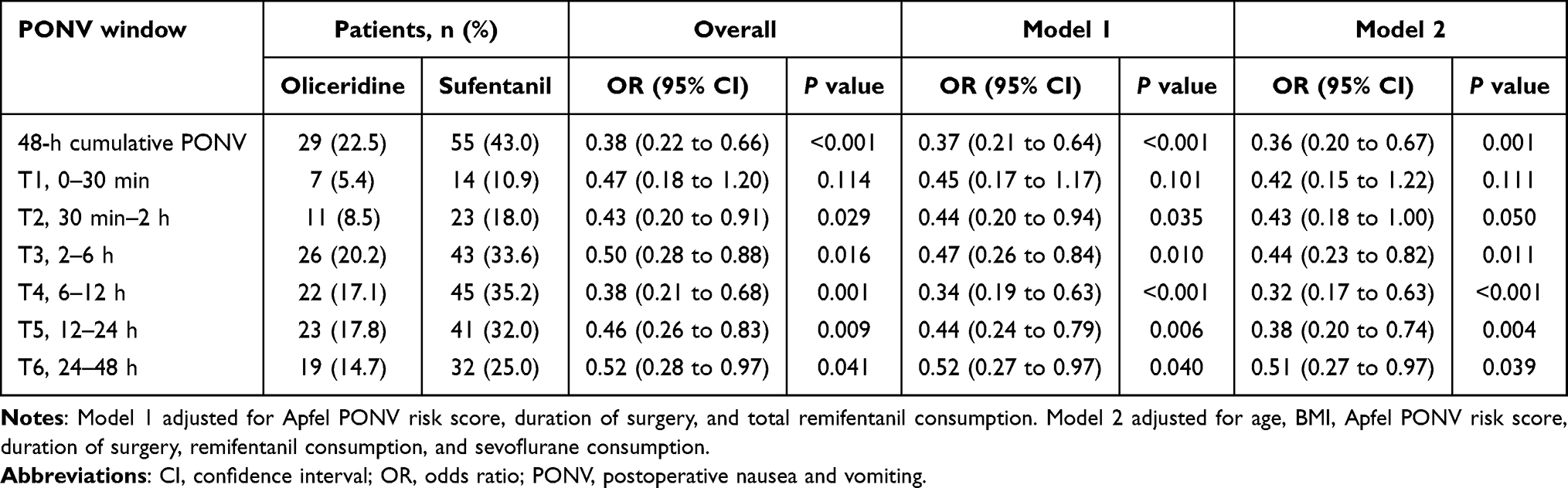 |
Table 2 Primary Outcome and Time‑Point Analyses of PONV |
Based on crude 48‑hour PONV incidence (22.5% for oliceridine vs 43.0% for sufentanil), the absolute risk reduction (ARR) was 20.5%, with a relative risk (RR) of 0.52 and a number needed to treat (NNT) of 5. This NNT value demonstrates a clinically meaningful preventive effect of oliceridine on postoperative nausea and vomiting.
Subgroup Analyses
Subgroup analyses for the primary outcome are presented in Figure 2. The direction of the treatment effect favored oliceridine across most prespecified subgroups, including age (< 60 vs ≥ 60 years), BMI (< 25 vs ≥ 25 kg/m2), ASA physical status (I–II vs III), Apfel PONV risk score (2 vs ≥ 3), and history of hypertension, although the interaction tests for these subgroups were not statistically significant (P for interaction > 0.05 for all). A significant interaction was observed for the type of surgery (P for interaction = 0.047). In patients undergoing ovarian cystectomy/tubal surgery, oliceridine was associated with a significantly lower incidence of PONV compared with sufentanil (15.4% vs 50.0%; OR, 0.18; 95% CI, 0.06 to 0.53). A statistically significant benefit was also observed for total hysterectomy (23.7% vs 50.0%; OR, 0.31; 95% CI, 0.12 to 0.83). For myomectomy, a similar numerical trend was observed (25.0% vs 43.8%; OR, 0.43; 95% CI, 0.15 to 1.24), but the confidence interval crossed 1, indicating a non-significant result. In contrast, among patients undergoing malignant surgery, the point estimate favored sufentanil, though the difference was not statistically significant (30.0% vs 15.0%; OR, 2.43; 95% CI, 0.51 to 11.51).
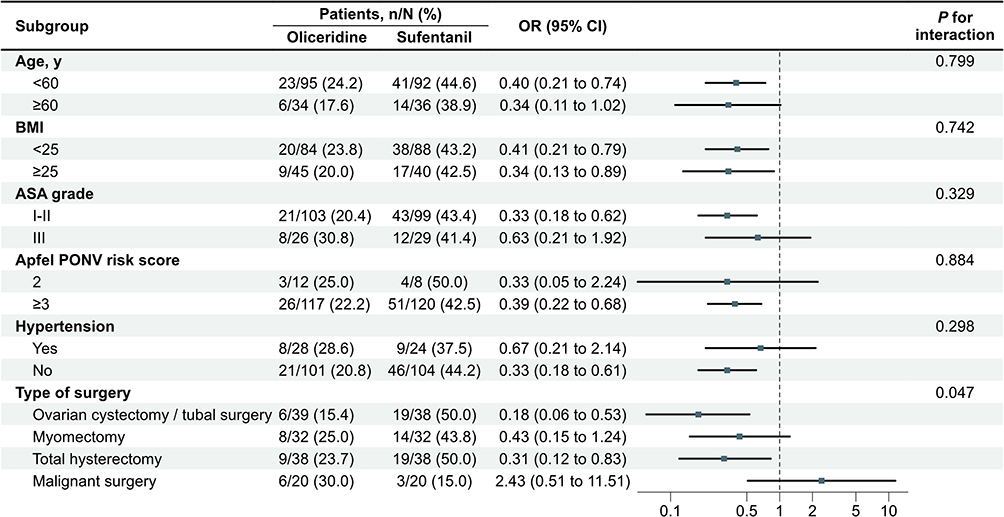 |
Figure 2 Subgroup analyses of the primary outcome. Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; OR, odds ratio; PONV, postoperative nausea and vomiting. Notes: Odds ratios and 95% confidence intervals are shown for each prespecified subgroup. The beneficial effect of oliceridine was consistent across most subgroups, with a significant interaction observed only for type of surgery (P for interaction = 0.047). |
Secondary Outcomes
The distribution of PONV severity, assessed by VAS categories, differed between groups, as summarized in Table 3. The incidence of severe PONV (VAS 7–10) was significantly lower in the oliceridine group compared with the sufentanil group (3.9% vs 15.6%; OR, 0.22; 95% CI, 0.08 to 0.60; q = 0.02). A similar trend was observed for moderate PONV (VAS 4–6), although the difference did not meet the significance threshold after correction for multiple comparisons (7.0% vs 16.4%; OR, 0.38; 95% CI, 0.17 to 0.87; q = 0.07). The incidence of mild PONV (VAS 1–3) was comparable between groups (11.6% vs 10.9%; OR, 1.07; 95% CI, 0.49 to 2.32; q = 0.86).
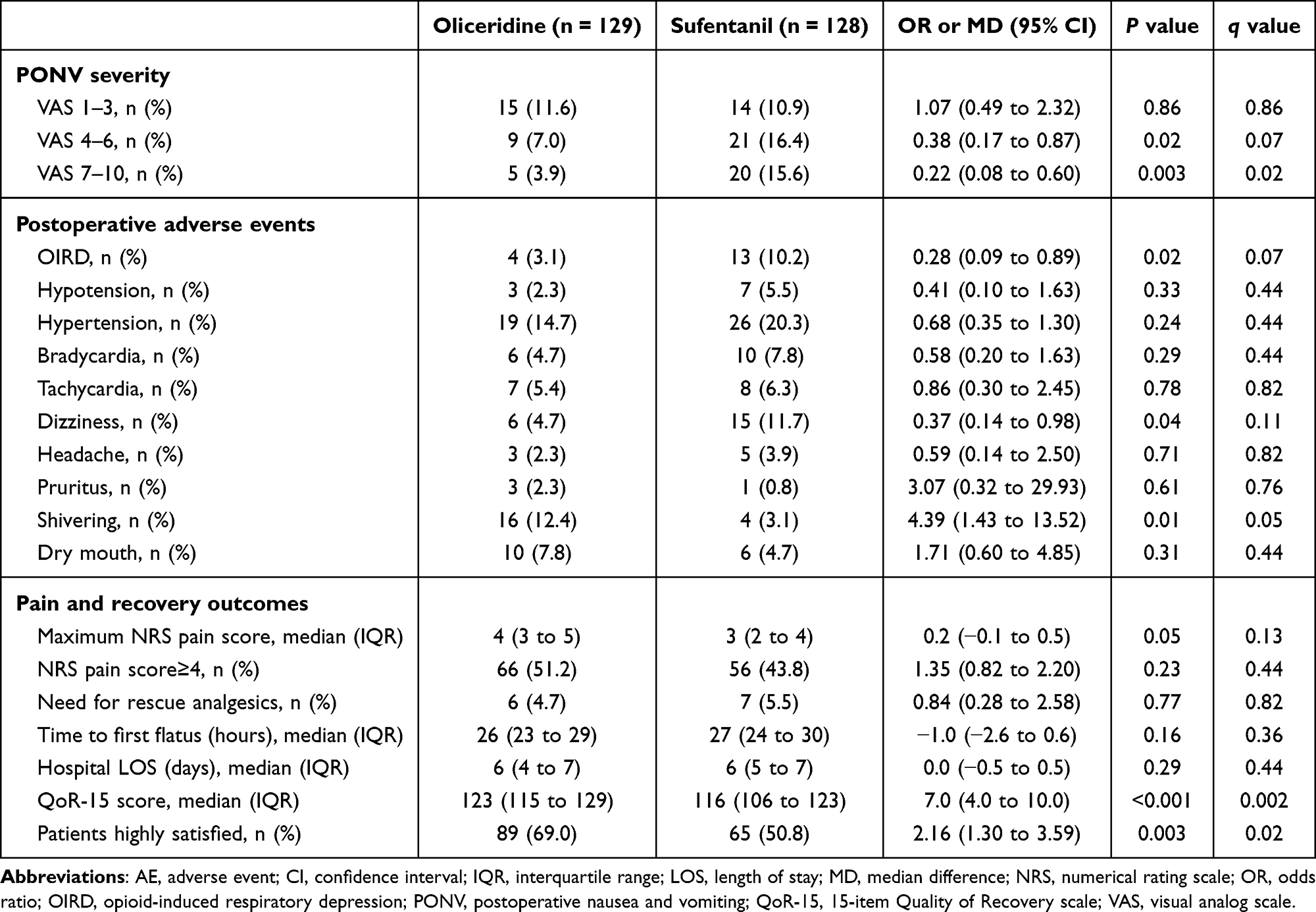 |
Table 3 Summary of Secondary Outcomes |
Among postoperative adverse events, the oliceridine group showed numerically lower rates of dizziness (4.7% vs 11.7%; OR, 0.37; 95% CI, 0.14 to 0.98; q = 0.11) and OIRD (3.1% vs 10.2%; OR, 0.28; 95% CI, 0.09 to 0.89; q = 0.07), although these differences did not reach statistical significance after false discovery rate correction. The incidence of shivering was higher in the oliceridine group (12.4% vs 3.1%; OR, 4.39; 95% CI, 1.43 to 13.52; q = 0.05), but this difference did not reach statistical significance after multiplicity correction. No significant differences between groups were observed for hypotension, hypertension, bradycardia, tachycardia, headache, pruritus, or dry mouth (all q > 0.05).
With respect to pain and recovery outcomes, no significant differences were detected between groups for maximum NRS pain score (median, 4 vs 3; median difference, 0.2; 95% CI, −0.1 to 0.5; q = 0.13), the proportion of patients with NRS pain score ≥4 (51.2% vs 43.8%; OR, 1.35; 95% CI, 0.82 to 2.20; q = 0.44), or the need for rescue analgesics (4.7% vs 5.5%; OR, 0.84; 95% CI, 0.28 to 2.58; q = 0.82). Recovery profiles were similar with respect to time to first flatus (median, 26 h vs 27 h; median difference, −1.0 h; 95% CI, −2.6 to 0.6; q = 0.36) and hospital length of stay (median, 6 days in both groups; median difference, 0.0 days; 95% CI, −0.5 to 0.5; q = 0.44). However, patients in the oliceridine group reported a significantly higher median QoR‑15 score (123 vs 116; median difference, 7.0; 95% CI, 4.0 to 10.0; q = 0.002) and a greater proportion of patients were highly satisfied with their anesthesia care (69.0% vs 50.8%; OR, 2.16; 95% CI, 1.30 to 3.59; q = 0.02).
Discussion
In this randomized trial of women undergoing GLS, oliceridine significantly reduced the 48‑hour incidence of PONV compared with sufentanil (22.5% vs 43.0%; OR, 0.38; P < 0.001), with consistent findings after multivariate adjustment. The NNT of 5 indicates that approximately five patients need to be treated with oliceridine instead of sufentanil to prevent one episode of PONV, underscoring the clinically meaningful benefit of this opioid in this high-risk population. The oliceridine group also had less severe PONV, higher QoR‑15 scores, and greater patient satisfaction. This is the first randomized trial to designate PONV as the primary outcome in a head‑to‑head comparison of oliceridine and sufentanil in GLS, and the largest to date in this surgical population.
The 48‑hour incidence of PONV was significantly lower in the oliceridine group than in the sufentanil group, which is consistent with the results of Duan et al, who reported PONV rates of 175% vs 40.0% in a smaller RCT of oliceridine versus sufentanil patient-controlled intravenous analgesia (PCIA) after total laparoscopic hysterectomy (P = 0.026).16 Meng et al demonstrated a comparable reduction in thoracoscopic surgery (323% vs 50.8%; P = 0.033),17 and a large retrospective cohort of thoracoscopic lung resection found a lower PONV incidence with oliceridine than with conventional opioids (15.5% vs 19.7%; P < 0.001).18 These consistent findings across surgical populations support the reproducibility of oliceridine’s antiemetic advantage. Notably, the absolute PONV incidence in our sufentanil group (43.0%) is substantially higher than that in the endoscopy trial (10.1%),13 which reflects the uniquely high emetogenic burden of gynecological laparoscopic surgery, where female sex, pneumoperitoneum, and pelvic manipulation converge to amplify PONV risk.4 From a pharmacological perspective, the observed PONV reduction is mechanistically plausible. Conventional opioids such as sufentanil activate the MOR non‑selectively, engaging both the G‑protein pathway (mediating analgesia) and the β‑arrestin pathway, which stimulates 5‑HT3 and D2 receptors in the area postrema and nucleus tractus solitarius—key nuclei in the central emetogenic circuitry.19–22 Oliceridine, by preferentially activating G‑protein signaling while substantially reducing β‑arrestin recruitment, may attenuate this central emetogenic activation while preserving analgesic efficacy.9 Furthermore, the sustained antiemetic benefit observed across all prespecified time intervals (T2-T6) suggests that oliceridine’s pharmacological advantage is not limited to the immediate postoperative period but extends throughout the 48‑hour observation window.
Patients in the oliceridine group reported a significantly higher median QoR‑15 score (123 vs 116; median difference, 7.0; q = 0.002). Improved recovery quality was accompanied by higher patient satisfaction (69.0% vs 50.8%; q = 0.02), findings consistent with existing comparative trials.16,17 This multifaceted benefit likely reflects not only reduced PONV but also the numerically lower rates of dizziness and OIRD, with the latter trend aligning with oliceridine’s known respiratory safety profile.23,24 A numerically higher incidence of shivering was observed in the oliceridine group (12.4% vs 3.1%; q = 0.05), although this difference did not reach statistical significance after multiplicity correction. Sufentanil is known to suppress postoperative shivering through μ‑receptor‑mediated thermoregulatory mechanisms;25,26 oliceridine’s G‑protein‑biased signaling may confer a less pronounced anti-shivering effect at equianalgesic doses. Whether this numerical trend represents a genuine pharmacological difference or a chance finding warrants further investigation.
Importantly, no significant differences were observed in maximum NRS pain scores, the proportion of patients with NRS ≥ 4, or rescue analgesic requirements, confirming that oliceridine’s antiemetic and recovery benefits were achieved without compromising analgesic efficacy.16 The comparable analgesic outcomes, together with the favorable recovery profile, suggest that oliceridine may offer a more balanced risk‑benefit ratio than sufentanil in this high‑risk surgical population. However, the failure of OIRD and dizziness to reach statistical significance after correction for multiple comparisons indicates that larger studies are needed to definitively establish these safety advantages.
The design and methodology of this study provide robust support for interpreting the benefits of oliceridine over sufentanil in reducing PONV and improving recovery quality. First, the guideline-based definition of PONV combined with six pre-specified assessment windows over 48 hours ensured a comprehensive evaluation of both early and delayed nausea and vomiting.6 Second, moving beyond traditional efficacy endpoints, the inclusion of patient-reported outcomes such as QoR-15 scores and satisfaction ratings directly addresses the modern perioperative focus on patient-centered care.27,28 Methodologically, we applied the Benjamini-Hochberg procedure to control the false discovery rate when testing multiple secondary outcomes. This approach mitigates the risk of false-positive findings that would otherwise arise from multiple comparisons, thereby ensuring the rigor and reliability of inferences drawn from secondary outcomes.29 Furthermore, although exploratory and underpowered individually, the pre-specified subgroup analyses with interaction testing offered initial insights into potential effect modifiers.30,31 Finally, the consistency of the primary outcome across adjusted and unadjusted analyses further strengthens the robustness of our conclusions.
Several limitations should be acknowledged. First, this single‑center trial has limited generalizability. Second, the sample size may be insufficient to detect significant differences in less frequent outcomes such as OIRD and dizziness after multiplicity correction. Third, the estimated equianalgesic doses may not have been fully equivalent. Fourth, the 48‑hour observation period precludes evaluation of longer‑term recovery outcomes. Finally, prespecified subgroup analyses were exploratory and not powered for definitive subgroup comparisons; the observed interaction for type of surgery should be interpreted with caution.
Conclusion
In conclusion, oliceridine significantly reduced the 48‑hour incidence of PONV compared with sufentanil in women undergoing gynecological laparoscopic surgery, while improving recovery quality and patient satisfaction without compromising analgesia. These findings support oliceridine as a valuable alternative to sufentanil for perioperative analgesia in this high‑risk population. Further multicenter trials are warranted to confirm these results and evaluate cost‑effectiveness in broader surgical populations.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Longqiu Yang ([email protected]), upon reasonable request.
Acknowledgments
We thank the anesthesia team and the operating room staff at Shanghai East Hospital, Tongji University School of Medicine for their invaluable support during the data collection phase of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Stoops S, Kovac A. New insights into the pathophysiology and risk factors for PONV. Best Pract Res Clin Anaesthesiol. 2020;34(4):667–12. doi:10.1016/j.bpa.2020.06.001
2. Qiu Z, Guo Y, Zhong W, et al. The Comparison of the Efficacy of Esketamine Over Sufentanil to Reduce Postoperative Nausea and Vomiting in Gynecological Laparoscopic Surgery: a Prospective, Double-Blind, Randomized Controlled Trial. Drug Des Devel Ther. 2025;19:8919–8929. doi:10.2147/DDDT.S533198
3. Shen Y, Wu Y, Tang Q, Wang Y, Ma W, Wang J. Efficacy of opioid-free anesthesia in reducing postoperative nausea and vomiting following gynecological laparoscopic surgery: a randomized controlled trial. Front Med. 2025;12:1606383. doi:10.3389/fmed.2025.1606383
4. Zhu Y, Jiang L, Sun C, Li Y, Xie H. A Prediction Model for Postoperative Nausea and Vomiting After Laparoscopic Surgery for Gynecologic Cancers. Clin Ther. 2025;47(2):143–147. doi:10.1016/j.clinthera.2024.11.018
5. Arslan HN, Çelik S. Nonpharmacological Nursing Interventions in Postoperative Nausea and Vomiting: a Systematic Review. J Perianesth Nurs. 2024;39(1):142–154. doi:10.1016/j.jopan.2023.06.096
6. Gan TJ, Belani KG, Bergese S, et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth Analg. 2020;131(2):411–448.
7. Liu J, Fang S, Cheng L, et al. A web-based dynamic predictive model for postoperative nausea and vomiting in patient receiving gynecological laparoscopic surgery. J Obstet Gynaecol Res. 2024;50(7):1216–1228. doi:10.1111/jog.15956
8. Lambert D, Calo G. Approval of oliceridine (TRV130) for intravenous use in moderate to severe pain in adults. Br J Anaesth. 2020;125(6):e473–e474. doi:10.1016/j.bja.2020.09.021
9. Moss L, Hijma H, Demitrack M, et al. Neurocognitive Effect of Biased µ-Opioid Receptor Agonist Oliceridine, a Utility Function Analysis and Comparison with Morphine. Anesthesiology. 2023;139(6):746–756. doi:10.1097/ALN.0000000000004758
10. Singla NK, Skobieranda F, Soergel DG, et al. APOLLO-2: a Randomized, Placebo and Active-Controlled Phase III Study Investigating Oliceridine (TRV130), a G Protein-Biased Ligand at the μ-Opioid Receptor, for Management of Moderate to Severe Acute Pain Following Abdominoplasty. Pain Pract. 2019;19(7):715–731. doi:10.1111/papr.12801
11. Viscusi ER, Skobieranda F, Soergel DG, Cook E, Burt DA, Singla N. APOLLO-1: a randomized placebo and active-controlled phase III study investigating oliceridine (TRV130), a G protein-biased ligand at the µ-opioid receptor, for management of moderate-to-severe acute pain following bunionectomy. J Pain Res. 2019;12:927–943. doi:10.2147/JPR.S171013
12. Liu Y, Zhu Y, Fu H. Tolerability of different doses of oliceridine versus traditional opioids in acute pain management: a systematic review and meta-analysis. Sci Rep. 2025;15(1):11470. doi:10.1038/s41598-025-95978-9
13. Ma B, Li Y, Leng C, et al. A Comparative Evaluation of the Safety and Efficacy of Oliceridine and Sufentanil in Gastrointestinal Endoscopy: a Single-Center, Randomized Controlled Trial. Drug Des Devel Ther. 2025;19:5111–5121. doi:10.2147/DDDT.S512529
14. Ke Z, He Y, Hu Q, Zheng D, Yao Z, Zhou W. A comparison of the effects of oliceridine and sufentanil on the quality of recovery after hysteroscopic surgery: a prospective double-blind randomized controlled trial. J Anesth. 2026;40(2):235–244. doi:10.1007/s00540-025-03578-8
15. Na X, Chen Y, Liu X, et al. Effect of oliceridine versus morphine on the quality of early recovery after thoracoscopic surgery: a randomized, controlled clinical trial. BMC Anesthesiol. 2026;26(1):178. doi:10.1186/s12871-026-03674-6
16. Duan J, Liu N, Lu Q, et al. Comparison of Postoperative Analgesic Efficacy of Oliceridine and Sufentanil in Total Laparoscopy Hysterectomy, a Clinical Double-Blind Controlled Trial. Drug Des Devel Ther. 2026;20:582143. doi:10.2147/DDDT.S582143
17. Meng Y, Yuan S, Zhang H, et al. Comparison of oliceridine and sufentanil in patient - controlled intravenous analgesia for post - thoracoscopic nausea and vomiting: a prospective, double - blind, randomized controlled trial. Front Pharmacol. 2025;16:1576154. doi:10.3389/fphar.2025.1576154
18. Huang C, Liu B, Xie S, et al. Evaluating the Opioid-Related Adverse Events of Oliceridine Versus Conventional Opioids in Patient-Controlled Analgesia After Thoracoscopic Lung Resection: a Retrospective Cohort Study. Drug Des Devel Ther. 2025;19:5929–5939. doi:10.2147/DDDT.S532778
19. DeWire SM, Yamashita DS, Rominger DH, et al. A G protein-biased ligand at the μ-opioid receptor is potently analgesic with reduced gastrointestinal and respiratory dysfunction compared with morphine. J Pharmacol Exp Ther. 2013;344(3):708–717. doi:10.1124/jpet.112.201616
20. Feenstra ML, Jansen S, Eshuis WJ, van Berge Henegouwen MI, Hollmann MW, Hermanides J. Opioid-free anesthesia: a systematic review and meta-analysis. J Clin Anesth. 2023;90:111215. doi:10.1016/j.jclinane.2023.111215
21. Fiore JF, El-Kefraoui C, Chay MA, et al. Opioid versus opioid-free analgesia after surgical discharge: a systematic review and meta-analysis of randomised trials. Lancet. 2022;399(10343):2280–2293. doi:10.1016/S0140-6736(22)00582-7
22. Smith HS, Laufer A. Opioid induced nausea and vomiting. Eur J Pharmacol. 2014;722:67–78. doi:10.1016/j.ejphar.2013.09.074
23. Dahan A, van Dam CJ, Niesters M, et al. Benefit and Risk Evaluation of Biased μ-Receptor Agonist Oliceridine versus Morphine. Anesthesiology. 2020;133(3):559–568. doi:10.1097/ALN.0000000000003441
24. Simons P, van der Schrier R, van Lemmen M, et al. Respiratory Effects of Biased Ligand Oliceridine in Older Volunteers: a Pharmacokinetic-Pharmacodynamic Comparison with Morphine. Anesthesiology. 2023;138(3):249–263. doi:10.1097/ALN.0000000000004473
25. Dinges HC, Al-Dahna T, Rücker G, et al. Pharmacologic interventions for the therapy of postanesthetic shivering in adults: a systematic review and network meta-analysis. Minerva Anestesiol. 2023;89(10):923–935. doi:10.23736/S0375-9393.23.17410-4
26. Kranke P, Eberhart LH, Roewer N, Tramèr MR. Single-dose parenteral pharmacological interventions for the prevention of postoperative shivering: a quantitative systematic review of randomized controlled trials. Anesth Analg. 2004;99(3):718–727. doi:10.1213/01.ANE.0000130589.00098.CD
27. Kleif J, Waage J, Christensen KB, Gögenur I. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
28. Myles PS, Shulman MA, Reilly J, Kasza J, Romero L. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. Br J Anaesth. 2022;128(6):1029–1039. doi:10.1016/j.bja.2022.03.009
29. Armstrong RA. When to use the Bonferroni correction. Ophthalmic Physiol Opt. 2014;34(5):502–508. doi:10.1111/opo.12131
30. Rothwell PM. Treating individuals 2. Subgroup analysis in randomised controlled trials: importance, indications, and interpretation. Lancet. 2005;365(9454):176–186. doi:10.1016/S0140-6736(05)17709-5
31. Schnell PM. Controlling the false-discovery rate when identifying the subgroup benefiting from treatment. Clin Trials. 2023;20(4):394–404. doi:10.1177/17407745231169300
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Opioid-Free Anesthesia on the Quality of Recovery After Gynecological Laparoscopy: A Prospective Randomized Controlled Trial
Choi H, Song JY, Oh EJ, Chae MS, Yu S, Moon YE
Journal of Pain Research 2022, 15:2197-2209
Published Date: 3 August 2022
Compare the Effects of Transversalis Fascia Plane Block versus Intravenous Lidocaine Infusion on the Quality of Early Postoperative Recovery in Patients Undergoing Gynecologic Laparoscopic Surgery
Zhang P, Zhao Y, Mu H, Zhang J, Zhang F, Wang S
Journal of Pain Research 2025, 18:7019-7027
Published Date: 23 December 2025
The Satisfactory Analgesia and Minimal Emesis of Elderly Patients After Thoracoscopic Lung Surgery: Oliceridine versus Sufentanil in a Randomized Controlled Trial
Cai Y, Jiang Y, Zhang Q, Yang J, Wang Z, Sun H
Drug Design, Development and Therapy 2026, 20:593306
Published Date: 7 May 2026